
Abstract
Background:
Significant controversy surrounds ideal tunnel position for medial patellofemoral ligament (MPFL) reconstruction (MPFLR) in the pediatric setting. The start point for femoral tunnel positioning (the Schöttle point) relative to the distal medial femoral physis is not well defined. Previous studies provide conflicting data regarding position of the MPFL origin and the Schöttle point relative to the distal femoral physis.
Hypothesis:
The Schöttle point would be consistently distal to the distal medial femoral physis.
Study Design:
Descriptive laboratory study.
Methods:
The institutional picture archiving and communication system was queried for computed tomography (CT) imaging studies of pediatric knees. Data were imported to an open-source image computing platform. True lateral digitally reconstructed radiographs and 3-dimensional (3D) renderings were generated, and the Schöttle point was registered in 3D space. Then, 3D distance measurements were obtained from the Schöttle point to the distal medial femoral physis.
Results:
A total of 49 pediatric knee CT scans were included. Mean age was 13.0 ± 2.3 years. Mean minimum distance from the medial physis to the Schöttle point was 9.9 ± 3.0 mm (range, 3.4-16.1 mm). In 49 of 49 cases (100%), the Schöttle point was distal to the physis. Using a 6-mm reaming diameter would result in 3 of 49 (6%) femurs having violation of the distal medial femoral physis. Moving the start point 3 mm distally would result in 0 of 49 (0%) sustaining physeal injury.
Conclusion/Clinical Relevance:
The Schöttle point is consistently distal to the distal medial femoral physis. The mean minimum distance from the Schöttle point to the physis on the medial cortex is 9.9 mm. The Schöttle point provides a safe and reliable radiographic landmark for pediatric MPFLR, although reaming diameter should be considered.
Keywords
Rates of patellar instability, and subsequent rates of medial patellofemoral ligament (MPFL) reconstruction (MPFLR), have been steadily increasing in the United States, especially in the active adolescent population. 9 Patellar dislocation occurs at a 3 to 5 times higher rate in 10- to 19-year-old patients compared with the general population. 25 Female adolescents 10 to 17 years of age experience the highest incidence (108/100,000 person-years) of patellar dislocation and the highest risk (36.8%) of recurrent instability. 6 Younger age at initial injury also increases the risk of recurrent instability. 5 Because of the increasing need for adolescent and pediatric MPFLR, substantial interest has arisen in identifying optimally safe and effective surgical techniques.
A key technical aspect of MPFLR is appropriate placement of the femoral tunnel for graft insertion.13,15 The femoral tunnel must be positioned such that there is favorable anisometry. For a successful surgery, the graft must provide sufficient restraint to patellar lateral movement from full extension through the first 70° of flexion.13,14 During deep flexion, the graft should loosen slightly to minimize graft tension and medial patellofemoral joint overload while the patella is constrained within the trochlear groove, under significant quadriceps tension.1,22 Establishing the femoral tunnel to create such anisometry is technically demanding; however, the ease and accuracy of this task have been greatly improved with the technique described by Schöttle et al. 15 Despite these advancements in MPFLR femoral tunnel technique, the placement of this tunnel in the pediatric patient remains increasingly challenging because of the risk of physeal injury.16,18,23
In the pediatric knee, not only does the graft femoral insertion point require careful attention (anisometry), but so does the entire tunnel position relative to the open distal femoral physis (physeal injury avoidance).10,11,17 The literature reporting the investigation of the relationship of the MPFL femoral attachment to the distal medial femoral physis is widely varied, with many studies providing conflicting results.2,11,17-19 Some studies have provided evidence that the MPFL femoral insertion lies consistently proximal to the distal medial femoral physis, whereas others have argued that the MPFL insertion is consistently distal to the physis.10,17 More recently, some data have indicated that the MPFL has a variable insertion regarding its relationship to the physis and that this relationship may change with growth and increase with age. 18 Given such substantial variation in previous anatomic studies, it remains challenging to define the optimal technique.
Because of the technical challenge of establishing femoral tunnel position, as well as the conflicting evidence regarding relative physis position, several techniques for localizing the femoral tunnel during MPFLR have been described. Shea and colleagues 17 initially described the position of the MPFL origin relative to the distal femoral physis on radiographs. Some authors have described the location of the MPFL origin relative to palpable bony landmarks on the distal medial femur.8,24 Others have proposed using the radiographic landmarks of the Schöttle point, providing evidence that this method does not result in physeal injury.10,11,15,17 Other studies have proposed idealized distally and anteriorly angulated trajectories to minimize risk of physeal injury.3,12 Last, techniques that do not use bone tunnels have been suggested, and these may further minimize physeal injury risk. 21 Despite these described techniques and detailed anatomic dissection studies, uncertainty remains regarding the ideal femoral tunnel start point and its proximity to the physis.
The purpose of the present study was to determine the proximity of the Schöttle point to the distal medial femoral physis and the medial epicondyle using digitally reconstructed radiographs (DRRs) and 3-dimensional (3D) computed tomography (CT) models. We hypothesized that the Schöttle point would be consistently distal to the distal medial femoral physis and would provide a reliable and safe start point for femoral tunnel positioning in pediatric MPFLR.
Methods
Patient Selection
The picture archiving and communication systems at 2 tertiary care centers were queried for pediatric knee CT scans from December 2011 to July 2021. Inclusion criteria were age <18 years, open or partially open distal femoral physis, and a high-resolution CT scan. CT scans were excluded if the distal femur demonstrated bony injury or deformity. Patient information was collected from the electronic medical record, including the patient’s sex and age at the time of imaging. Approval was obtained from our institutional review board, and an exempt status was determined for this study (No. 145922).
Digitally Reconstructed Radiographs
Digital Imaging and Communications in Medicine (DICOM) files of the pediatric knee CT scans were extracted from the picture archiving and communication system and were imported into 3D Slicer Image Computing Platform (Version 4.11.2; SlicerCommunity).4,7 DRRs were generated using the 3D Slicer rendering module. The medial epicondyle was used as the center of the projection field, and the DICOM data were rotationally transformed to create a perfect lateral view of the knee based on alignment of the posterior aspects of the femoral condyles. 15
Schöttle Point Fiducial Marking
The Schöttle point was marked with a fiducial axis as previously described using femoral reference points on the DRR. Reference lines (Figure 1) included a line extending from the posterior femoral cortex (line 1), a line perpendicular to line 1 drawn through the intersection of the posterior femoral cortex at the origin of the femoral condyle (line 2), and a line perpendicular to line 1 and intersecting the posterior-most point of the Blumensaat line (line 3). 15 The Schöttle point was then marked with a fiducial axis perpendicular to the sagittal plane originating 1 mm anterior to line 1 and midway between lines 2 and 3. The Schöttle point was assessed on the DRR as being proximal to the physis, on the physis, or distal to the physis.
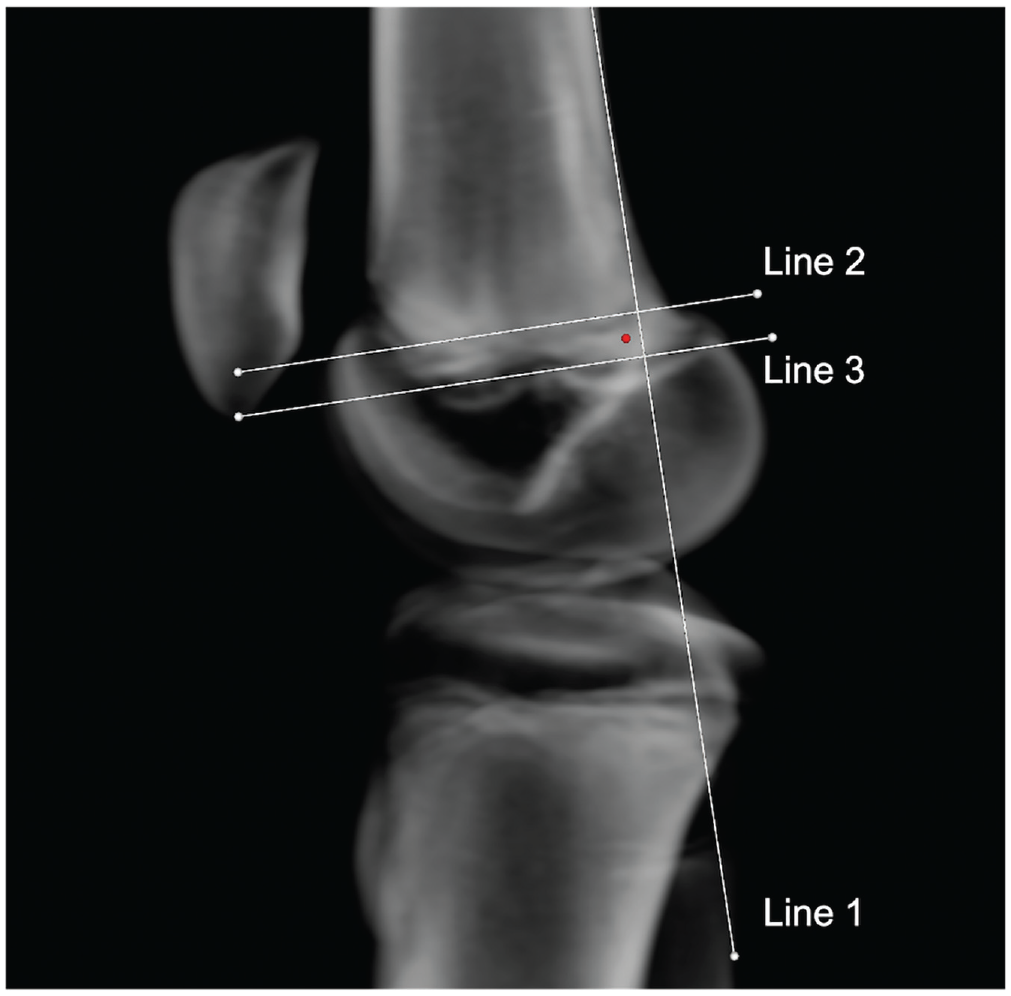
Digitally reconstructed radiograph from available computed tomography data of a pediatric right knee. A lateral view was established to localize the Schöttle point similar to the method used intraoperatively. Line 1 demonstrates the extension of the posterior femoral cortex, line 2 demonstrates the intersection of the posterior femoral cortex with the origin of the femoral condyle, and line 3 demonstrates the intersection of the posterior-most point of the Blumensaat line. The Schöttle point (dot) was then assessed anterior to line 1 and midway between lines 2 and 3.
Measurements of the Schöttle Point Relative to the Distal Medial Femoral Physis
After the Schöttle point was established, a 3D volume rendering was generated using the 3D Slicer rendering module (Figure 2). Distance from the Schöttle point to the distal medial femoral physis within the coronal plane, along the medial cortex, was measured in the CT scan multiplanar reconstruction. Minimal distance from the Schöttle point to the distal medial femoral physis along the medial femoral cortex was also measured using fiducial lines on the 3D reconstruction view. Last, distances from the Schöttle point to the medial epicondyle in the anteroposterior and the superoinferior directions were measured and tabulated.
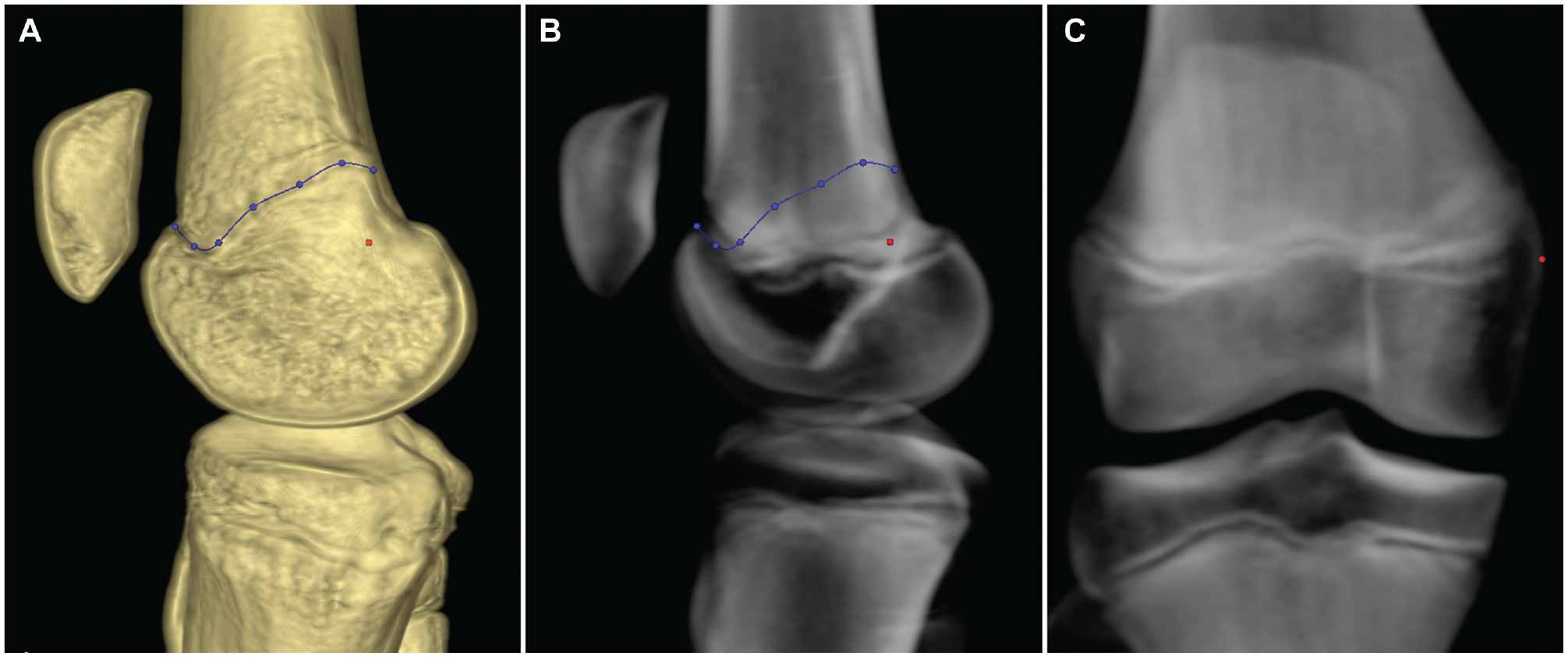
Three-dimensional (3D) rendering and digitally reconstructed radiographs of computed tomography data from a pediatric right knee. (A) A 3D rendering of the knee with markers placed on the distal medial femoral physis (line) and the Schöttle point (point). (B) A digitally reconstructed radiograph of the same knee from the same patient, again with markers placed on the distal medial femoral physis (line) and the Schöttle point (point). (C) An anteroposterior digitally reconstructed radiograph with a marker on the Schöttle point (point), demonstrating this position relative to the upstroke of the distal medial femoral physis.
Statistical Analysis
All patient characteristics and 3D measurements were compiled in a spreadsheet using Excel software (Excel 2016; Microsoft Corp). Descriptive statistics were calculated using Microsoft Excel.
Results
A total of 49 pediatric knee CT scans in 46 patients were included from 71 reviewed scans (Figure 3).
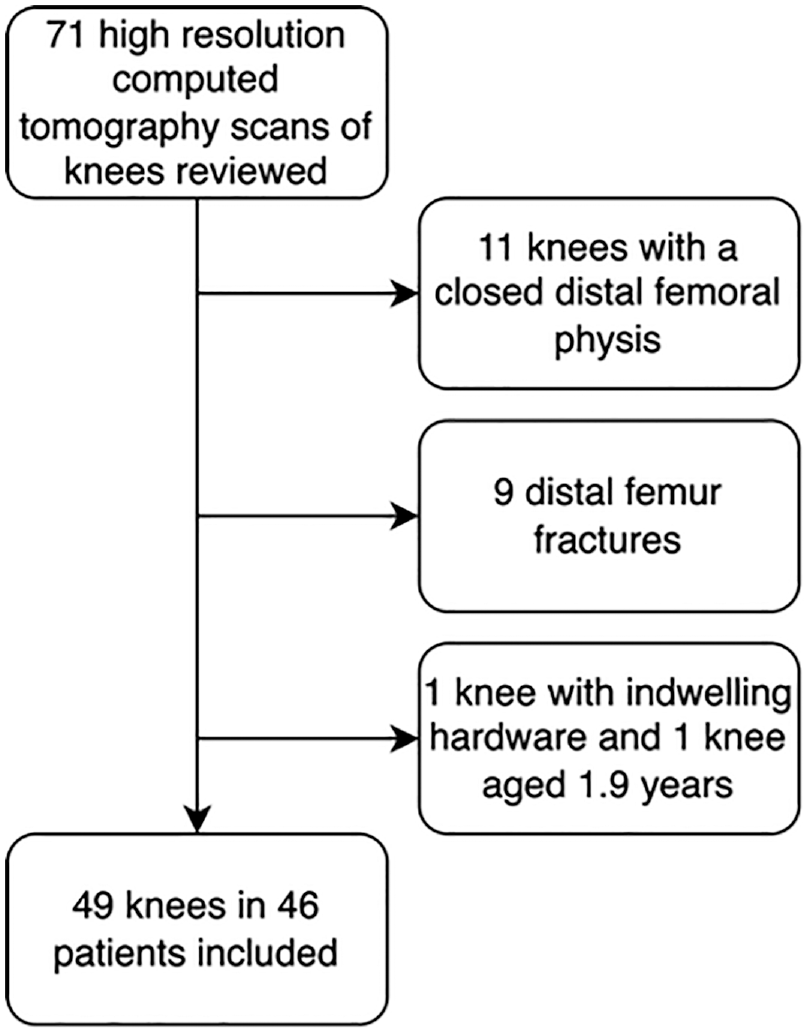
Flow diagram of patient selection. Initial review identified 71 studies with the final patient cohort composed of 49 separate knees after application of exclusion criteria.
In total, 26 (53%) of the CT scans were of right knees, and 19 (39%) were acquired from female patients. The mean ± SD patient age was 13.0 ± 2.3 years: 12 ± 2.6 years (range, 6-17 years) for girls and 13 ± 2.0 years (range, 6-16 years) for boys (Table 1). The most common indications for obtaining the included CT scans were tibial fractures (n = 23; 47%) and patellar instability (n = 7; 14%).
Cohort Characteristics a
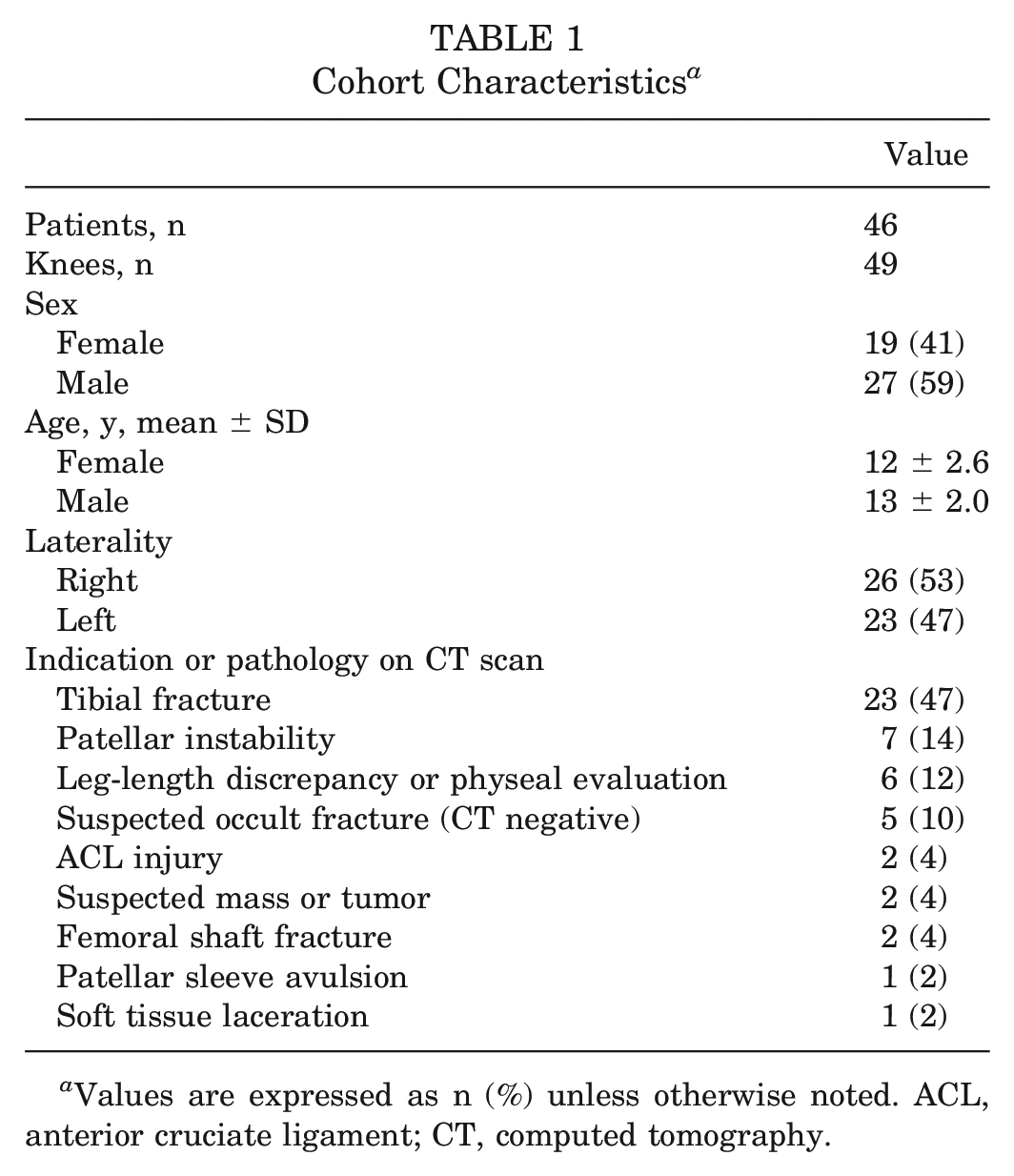
Values are expressed as n (%) unless otherwise noted. ACL, anterior cruciate ligament; CT, computed tomography.
The mean minimum distance from the Schöttle point to the physis along the medial femoral cortex was 9.9 ± 3.0 mm (range, 3.4-16.1 mm). In the majority of knees, the Schöttle point on the DRR was observed to appear either proximal to or at the level of the distal medial femoral physis (44.9% for both positions). In 49 of 49 cases (100%), the Schöttle point was distal to the physis on 3D volume rendering. The Schöttle point was localized at a mean distance of 7.5 ± 3.14 mm posterior to the medial epicondyle and 6.2 ± 2.9 mm superior to the medial epicondyle. Using a 6-mm reaming diameter would result in 3 of 49 (6%) femurs having a violation of the distal medial femoral physis. Moving the start point 3 mm distally would result in 0 of 49 (0%) femurs sustaining physeal injury (Table 2).
Schöttle Point Anatomic Measurements a
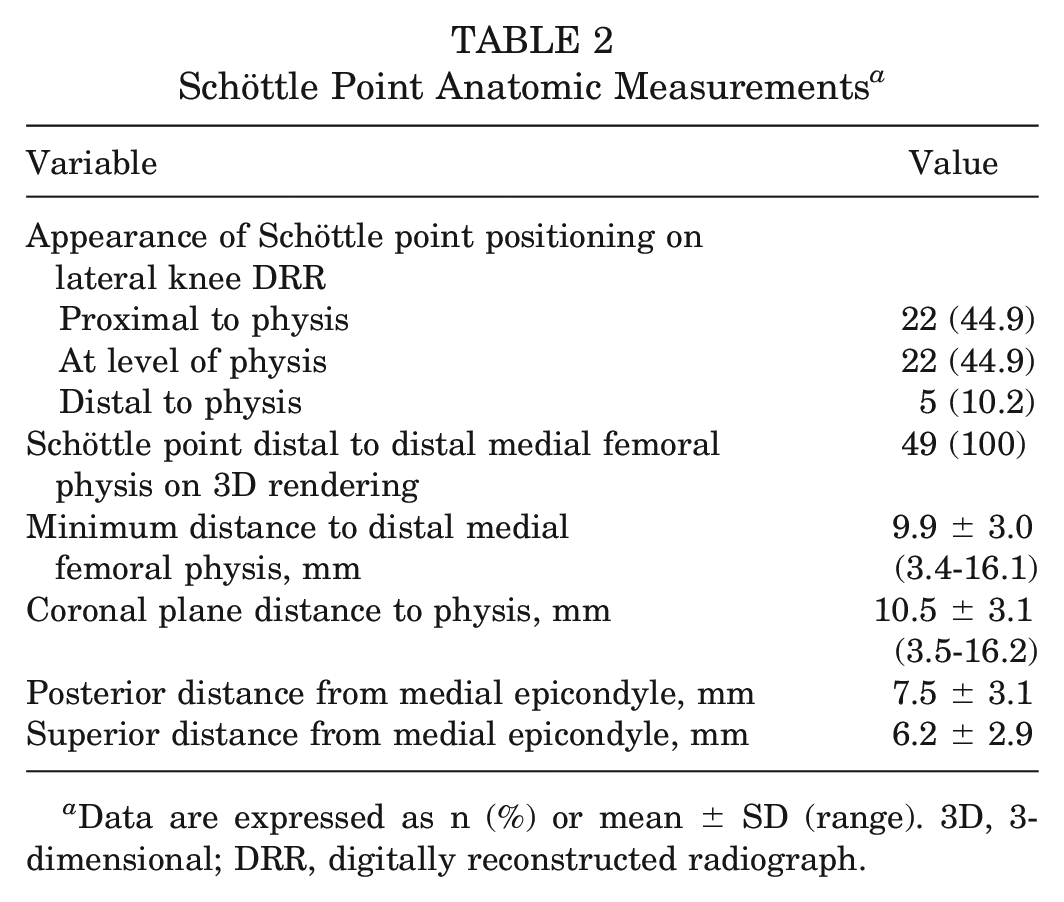
Data are expressed as n (%) or mean ± SD (range). 3D, 3-dimensional; DRR, digitally reconstructed radiograph.
Discussion
Using CT scan data from 49 pediatric knees, the present study demonstrated that in all cases (49/49 knees; 100%), the Schöttle point localized distal to the physis. This study links an established, reliable surgical technique to physeal anatomy, providing intraoperative confidence and technique guidance to the pediatric sports surgeon. As such, the Schöttle point may be used as the radiographic start point for pediatric MPFLR in the vast majority of patients without violation of the distal medial femoral physis, although some caution should be exercised with large reamer size.
The insertion of the MPFL relative to the distal medial femoral epiphysis has been a subject of some confusion. Early work on the MPFL femoral origin found the Schöttle point to be a mean of 2.7 ± 1.1 mm proximal to the physis in female patients (aged 12-13 years) and 4.6 ± 2.4 mm proximal in male patients (aged 14-15 years). 17 This initially raised concerns regarding possible physeal injury during MPFLR, particularly when the Schöttle point technique is used. Subsequently, Nelitz et al, 10 using both anteroposterior and lateral radiographs, demonstrated that the undulating nature of the distal femoral physis made assessment of true physeal position unreliable on a single lateral radiographic view. This group also went on to publish a series of 21 pediatric MPFLRs using the Schöttle point technique without physeal injury or growth disturbance. 11 The present study helps solidify the conclusions of Nelitz and colleagues, 10 as it demonstrates the Schöttle point to be distal to the distal medial femoral physis in a larger cohort of patients, and the present 3D radiographic technique also eliminates confusion caused by misleading radiographic projections.
Previous cadaveric studies have suggested that the MPFL femoral insertion demonstrates significant variation and originates proximal to the physis in younger patients (<7 years). 18 Other recent cadaveric studies have challenged this idea, finding the bony landmarks of the MPFL origin to be distal to the physis. 12 Although these detailed cadaveric studies are essential for elucidation of this anatomic feature, they are limited by small numbers of specimens and may be difficult to translate to intraoperative technique because the native MPFL footprint may not be appreciable intraoperatively among traumatized tissues. As such, practical, repeatable intraoperative landmarks are needed to optimize surgical technique. The present study addresses this need by demonstrating that the Schöttle point, a repeatable and widely used radiographic landmark, is consistently distal to the distal medial femoral physis. The present study complements previous anatomic work by aiding surgeons in translating anatomic knowledge to reliable surgical technique.
A few previous studies have used innovative 3D techniques derived from osteological specimens in efforts to establish optimal femoral tunnel trajectories. 12 These studies showed that the MPFL femoral attachment was a mean of 8.5 mm distal to the medial aspect of the distal femoral physis and that tunnel angulation 15° distally and 20° anteriorly may minimize risk of damage to the physis, femoral cartilage, and elements of the intercondylar notch.3,12 However, in these studies, the start point of the femoral tunnel was identified using precise locations of the medial epicondyle and the abductor tubercle in a 3D computer model, which is not available during routine MPFLR. As such, these studies do not assess the reaming path relative to the commonly used radiographically identified start point, the Schöttle point. The present study complements these 3D modeling studies, as well as previous cadaveric work, by finding that the distance of the Schöttle point from the physis is relatively consistent with the femoral tunnel start point identified by Farrow et al 3 (9.9 vs 8.5 mm, respectively).
Last, the present study offers some unique methodological advantages to previous studies. Pediatric cadaveric studies are limited by availability and size of specimens.18-20 The current study leverages readily available and copious institutional CT data to overcome previous limitations posed by cost and specimen availability. The use of an open source, widely validated image computing platform allows for ease of replication or building upon the findings in the study.4,7 This method—, by integrating CT data, DRRs, and 3D rendering and modeling capability—, provides a foundation for complete digital simulation of the surgical technique.
Limitations
This study has several limitations. First, in this study we analyzed the Schöttle point as a single point on the medial femoral cortex; we did not investigate how angular variations in trajectory would affect physeal penetration. Despite this, the present study, which characterizes the radiographic start point, may be combined with data from previous studies that suggest a distal and anterior trajectory for the femoral tunnel to provide a more complete tunnel reaming technique. Second, the study sample was not confined to individuals undergoing MPFLR, and thus subtle anatomic differences in patellar instability may exist in these patients, particularly those with distal femoral deformity. Third, CT scans of patients <6 years of age were not available, and so the findings of the present study may not be appropriate to extrapolate to this population. However, the present study covers the typical age range of patients who have patellar instability. Fourth, although our study demonstrates that the Schöttle point is consistently distal to the medial distal femoral physis in pediatric patients, enabling precise surgical technique, the present study does not provide insight into the exact geometry and dimensions of the native MPFL footprint. As such, the present study complements, rather than supplants, previous cadaveric dissection work.
Future Work
A number of further investigations could improve understanding of physeal-sparing MPFLR. Three-dimensional modeling techniques, along with DRRs, could be used to fully simulate tunnel placement to optimize angulation and tunnel depth to avoid physeal injury. Cadaveric studies using radio-opaque marker placement at the MPFL footprint with subsequent CT scans, 3D model rendering, and DRRs could investigate the exact relationship of the pediatric MPFL footprint to the Schöttle point. Further, with collection of more CT scan data, additional measurements of distal femoral morphology and skeletal maturity may be used to create statistical models or nomograms for predicting physeal violation.
Conclusion
The radiographically defined surgical start point for MPFL tunnel placement (the Schöttle point) was consistently distal to the distal medial femoral epiphysis. The mean minimum distance from the Schöttle point to the physis on the medial cortex was 9.9 mm. The Schöttle point can provide a safe and reliable radiographic landmark for pediatric MPFLR, although reaming diameter should be considered.
Footnotes
Submitted March 29, 2022; accepted August 16, 2022.
Presented at the annual meeting of the AOSSM, Colorado Springs, Colorado, July 2022.
One or more of the authors has declared the following potential conflict of interest or source of funding: J.J.E. has received consulting fees from Johnson & Johnson Depuy Mitek Sports Medicine and educational support and grants from Arthrex, Smith & Nephew, Gemini Mountain Medical, and Medical Device Business Services. T.G.M. has received consulting fees from Arthrex. S.K.A. has received consulting fees from Stryker Corporation. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.