
Abstract
Background:
Recent studies have reported that lateral hinge fracture (LHF) has a negative effect on bone healing at the osteotomy site after medial closing wedge distal femoral osteotomy (MCDFO). However, limited evidence exists in the literature regarding the predictive factors for LHF in MCDFO.
Hypothesis:
A large medial closing gap and a lateral hinge position in the supracondylar area would increase plain radiography–based and/or computed tomography (CT)–based LHF in MCDFO.
Study Design:
Case control study; Level of evidence, 3.
Methods:
We retrospectively evaluated 67 knees of 53 patients (mean age, 37.4 ± 16.9 years) who underwent MCDFO between May 2009 and June 2021. The surgical indications for MCDFO were genu valgum deformity combined with either lateral compartment osteoarthritis or recurrent patellar dislocation. The presence of LHF was evaluated based on immediate postoperative plain radiography and CT scans. The predictive factors for LHF in MCDFO were investigated using multivariate logistic regression analysis.
Results:
LHFs were identified in 21 knees (31.3%) through plain radiography and in 40 knees (59.7%) through CT. Multivariate logistic regression analysis showed that the medial closing gap and lateral hinge position were predictive factors for plain radiography– and CT-based LHF after MCDFO. Controlling for other variables, we found that an increase in the medial opening gap by 1 mm increased the likelihood of plain radiography–based LHF by a factor of 1.805 (95% CI, 1.291-2.525; P = .001) and CT-based LHF by 1.333 (95% CI, 1.003-1.772; P = .048). Moreover, a lateral hinge position in the supracondylar area increased the likelihood of plain radiography–based LHF by a factor of 9.870 (95% CI, 2.179-44.720; P = .003) and CT-based LHF by 5.686 (95% CI, 1.124-28.754; P = .036).
Conclusion:
A large medial closing gap and lateral hinge position in the supracondylar area are associated with LHF in MCDFO. Care should be taken to prevent LHF in MCDFO with a large medial closing gap. Moreover, a lateral hinge position in the supracondylar area should be avoided to decrease the incidence of LHF in MCDFO.
Keywords
Medial closing wedge distal femoral osteotomy (MCDFO) is a well-described treatment option for genu valgum deformity combined with either lateral compartment osteoarthritis1,2,25,26 or recurrent patellar dislocation.3,9,20 Previous studies on MCDFO have reported excellent clinical outcomes with high patient-reported outcomes and survival rates.6,22,25 The complications, however, include fracture, delayed union, nonunion, correction loss, infection, hematoma, hardware failure, plate discomfort, and stiffness. 24
Lateral hinge fracture (LHF) at the osteotomy site is another frequent complication of MCDFO, and its incidence on postoperative radiographs has been reported to be as high as 34.5%.18,21 Recent clinical studies have reported that LHF has negative effects on bone healing at the osteotomy site after MCDFO, such as delayed union, nonunion, or loss of reduction.7,21,23 However, limited evidence exists in the literature regarding the predictive factors for LHF in MCDFO.
This study aimed to investigate the predictive factors for LHF in MCDFO. We hypothesized that a large medial closing gap and lateral hinge position in the supracondylar area would increase the incidence of LHF in MCDFO.
Methods
After obtaining approval from our institutional review board, we retrospectively evaluated patients who underwent MCDFO between May 2009 and June 2021. The surgical indications for MCDFO were (1) genu valgum deformity combined with either lateral compartment osteoarthritis 1 or recurrent patellar dislocation,9,20 (2) absence of osteoarthritic changes in the medial compartment, (3) flexion contracture <15°, (4) lateral collateral laxity of grade 2 or lower (<5 mm),15,17 and (5) a required angle of correction <20°. The inclusion criteria were as follows: (1) patients who underwent primary MCDFO; (2) patients who underwent knee anteroposterior, lateral, and whole-leg standing radiography pre- and postoperatively; and (3) patients who underwent postoperative computed tomography (CT) scans. The exclusion criteria were as follows: (1) revision MCDFO, (2) insufficient medial or radiological data, and (3) need for additional operations due to postoperative complications such as surgical-site infection or ipsilateral distal femoral fracture.
Surgical Technique
All operations were performed by a single experienced surgeon (K.W.N.) using the same surgical technique.20,21 Preoperative planning was performed using whole-leg standing radiographs. The extent of correction was calculated in preoperative planning using the method described by Miniaci et al. 16 The target point of the weightbearing line was planned to be located at the medial spine of the tibial plateau. All radiological measurements and preoperative planning were performed using a picture archiving and communication system (Marotech).
The patient was placed in the supine position on an operating table, and a sterile tourniquet was applied to the thigh. Diagnostic arthroscopy was performed to evaluate the combined intra-articular pathologies. Then, a 10-cm longitudinal skin incision was made on the anteromedial side of the distal femur. The anteromedial aspect of the supracondylar area of the femur was exposed using a subvastus approach. After incision of the muscle fascia, the vastus medialis was stripped from the intermuscular septum and retracted using a Hohmann retractor. Distal femoral osteotomy was planned as an MCDFO on a plane beginning approximately 2 cm superior to the adductor tubercle in the medial supracondylar area and ending in the lateral supracondylar area. The starting point was marked under fluoroscopic guidance on the medial supracondylar area by electrocauterization, with a fixation plate as a reference. The target angle of correction was then marked with 2 Kirschner wires under fluoroscopic guidance (Figure 1A). In biplanar osteotomy, the axial part of the osteotomy involved the posterior two-thirds of the femur and was performed up to 5 mm from the lateral femoral cortex for its preservation. A medial wedge was created along the inner margins of the 2 Kirschner wires previously applied, by using a small oscillating saw (Figure 1B). Electrocauterization marked the direction of the frontal plane from the superior margin of the axial osteotomy to the anterior femoral cortex; the direction was angled at approximately 110° from the axial osteotomy. Subsequently, the medial bone wedge was removed, and the medial osteotomy was carefully closed by applying consistent pressure. Alignment of the leg axis was evaluated and confirmed using fluoroscopy. The osteotomy was stabilized with 1 of 3 locking compression plates: distal femoral locking compression plate (DePuy Synthes; Johnson & Johnson), TomoFix plate (DePuy Synthes), or OhtoFix plate (Ohtomedical) (Figure 1C).
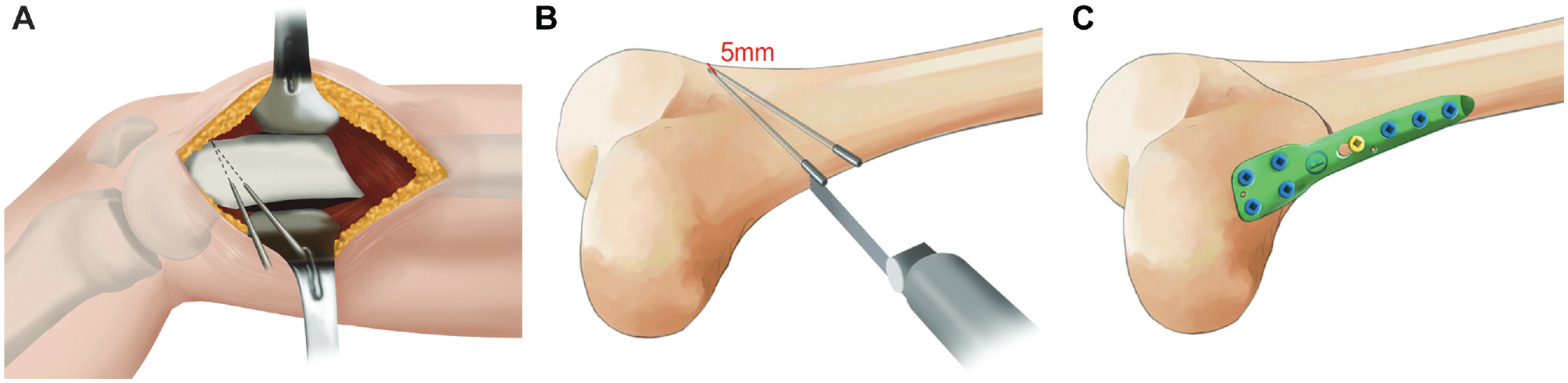
Surgical procedures for medial closing-wedge distal femoral osteotomy. (A) After the vastus medialis was retracted with a Hohmann retractor, the target angle of correction was marked with 2 Kirschner wires under fluoroscopic guidance. (B) A medial wedge was created along the inner margins of the 2 Kirschner wires previously applied, by using a small oscillating saw. (C) The osteotomy was stabilized with a locking compression plate.
Evaluation of the Patient Characteristics and Radiological Parameters
Two orthopaedic residents (H.S.K., D.U.J.), who were blinded to the study design, reviewed all of the medical records and radiological data of the enrolled patients. Demographic data (sex, age, body mass index, and side of operation) and medial closing gaps were collected from medical records. Preoperative and postoperative plain radiographs and postoperative CT scans were also reviewed to evaluate the radiological parameters. Postoperative multislice CT scanning was performed on postoperative day 3 using 2-mm coronal, sagittal, and axial slices of the knee joint. The obtained image data sets were imported into a 3-dimensional software (Aquaris; Tera-Recon) for analysis.
The hip-knee-ankle (HKA) angle and mechanical lateral distal femoral angle (mLDFA) were measured on preoperative and postoperative whole-leg standing radiographs (Figure 2). Coronal osteotomy angle and lateral hinge position were evaluated using immediate postoperative anteroposterior radiography. The coronal osteotomy angle was defined as the angle formed by the osteotomy line and the distal femoral articular line (Figure 3). Based on previous studies,12,21 the lateral hinge position was classified into the supracondylar area and the lateral epicondyle (Figure 4). The presence of LHF was evaluated based on plain radiographs or CT scans. It was diagnosed if fracture of the lateral cortex was visible on plain radiographs or CT scan (Figure 5).
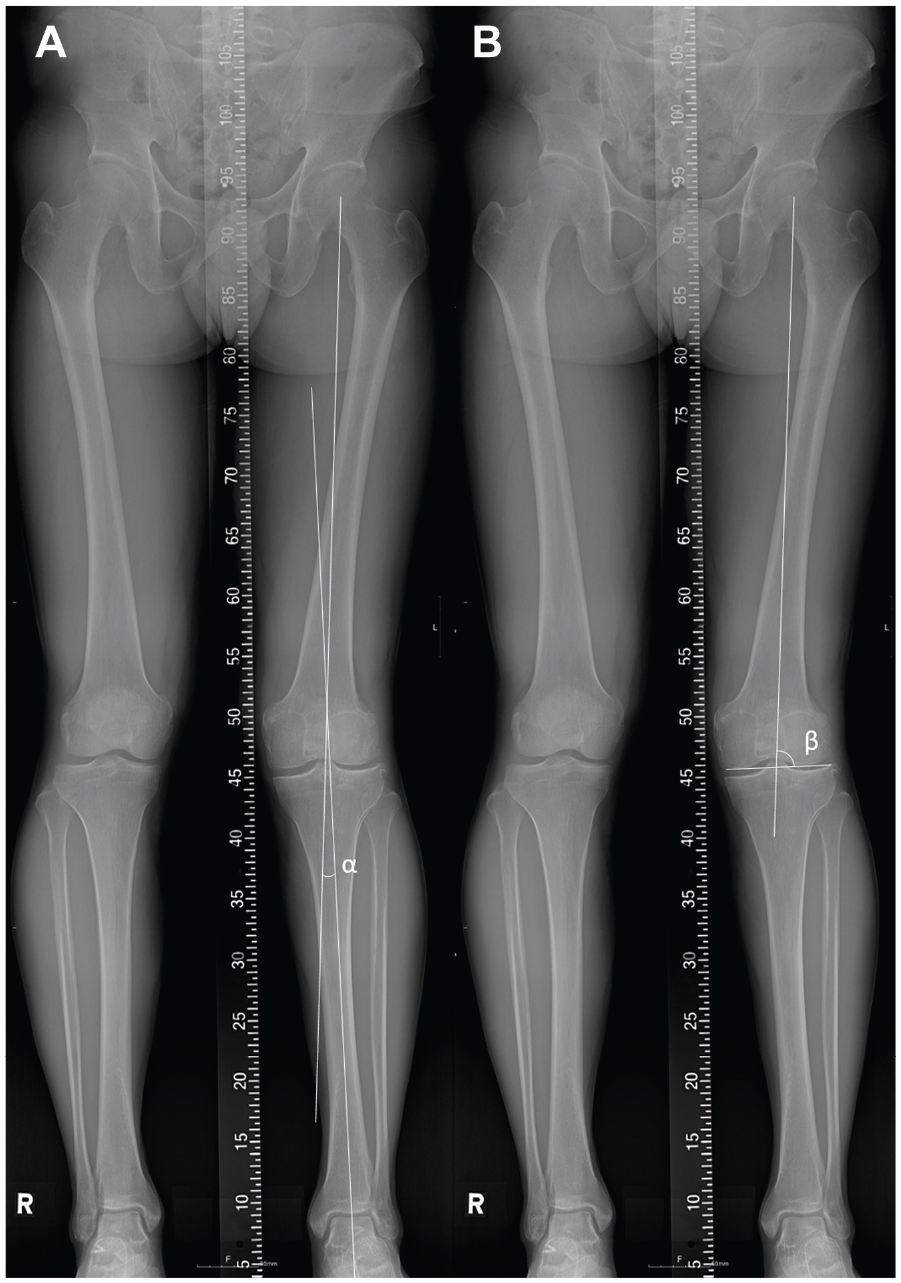
Measurements of radiological parameters on preoperative whole-leg standing radiographs. (A) Hip-knee-ankle angle (α) formed by the mechanical femoral axis and the mechanical tibial axis. (B) Mechanical lateral distal femoral angle (β) formed by the mechanical femoral axis and the distal femoral joint line.
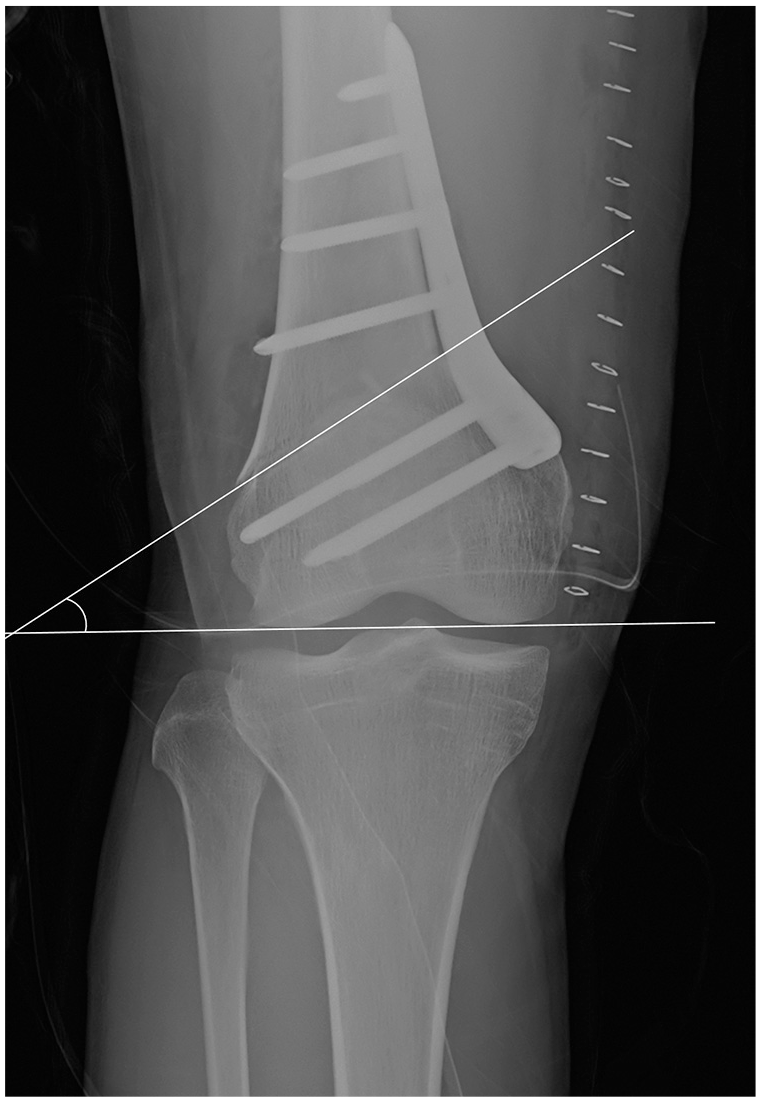
Measurement of the coronal osteotomy angle.
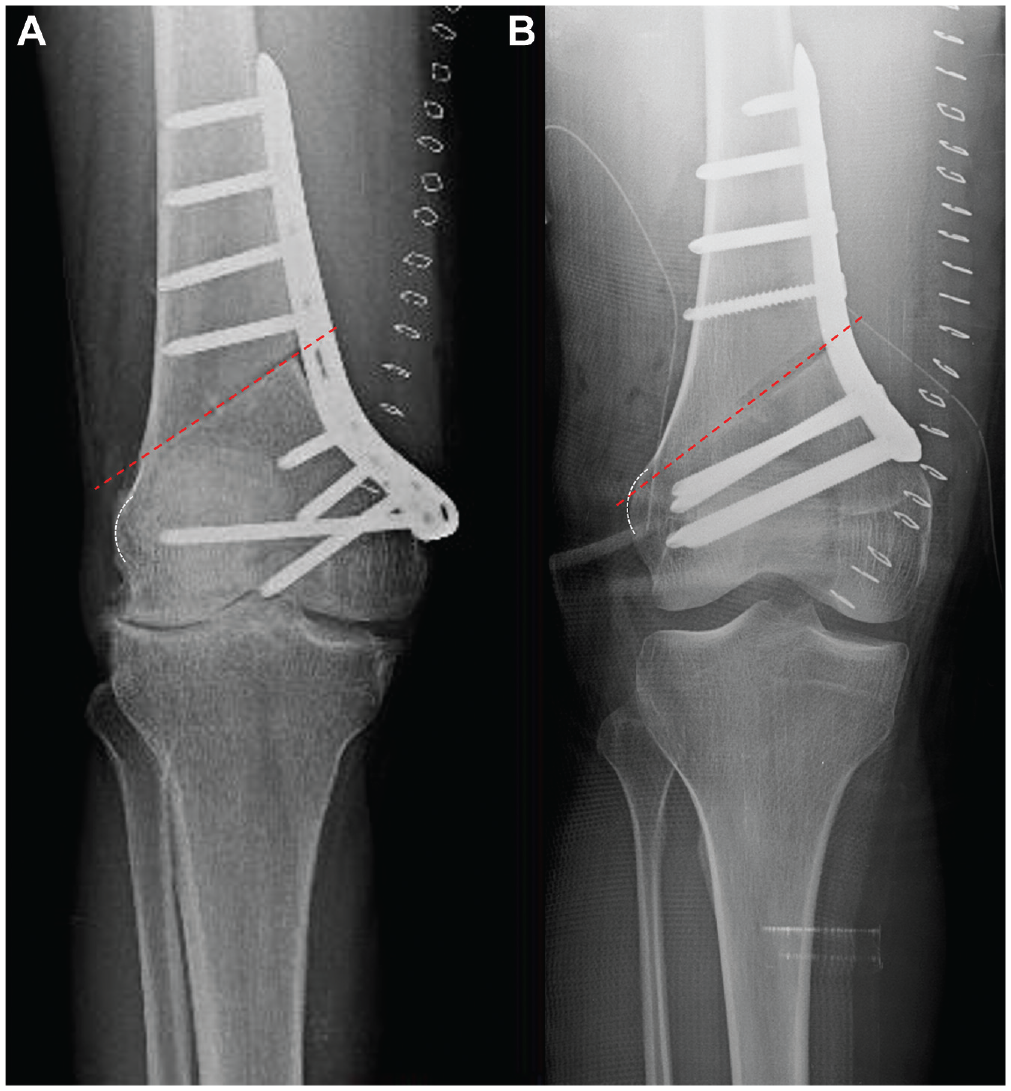
Evaluation of the lateral hinge position after medial closing distal femoral osteotomy. The position of lateral hinge was classified into the (A) supracondylar area and (B) lateral epicondyle. The transverse dotted line indicates the osteotomy line, and the white dotted outline indicates the lateral epicondyle of the distal femur.
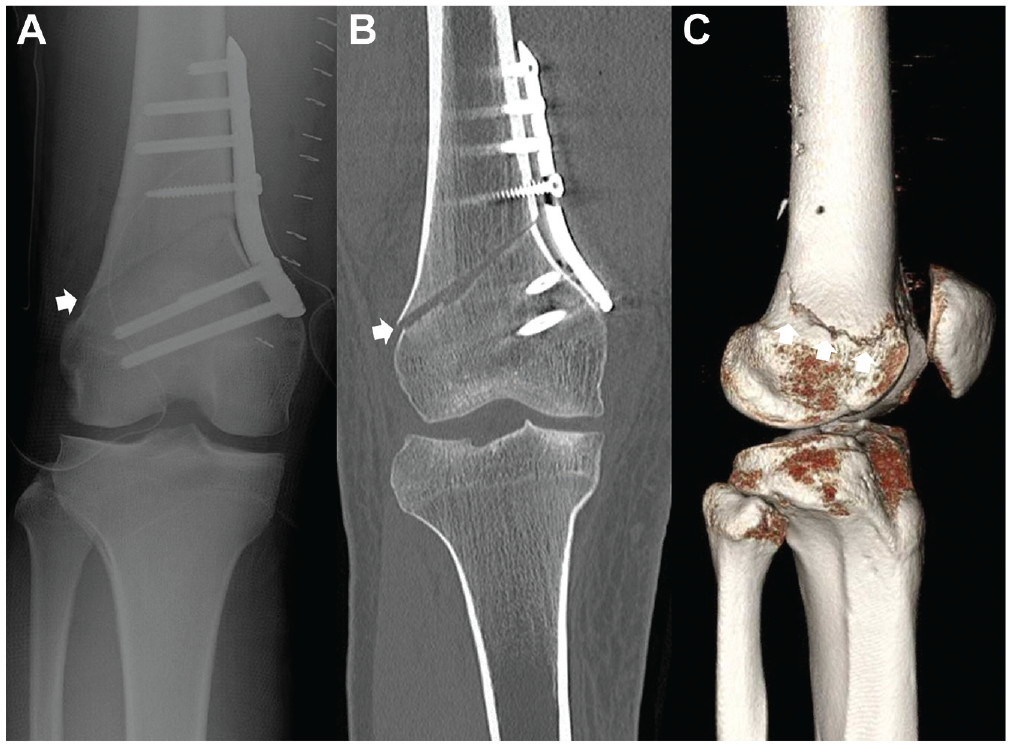
Evaluation of lateral hinge fracture (white arrow) after medial closing distal femoral osteotomy on (A) plain radiograph, (B) coronal sectioned computed tomography (CT) scan, and (C) 3-dimensional reconstructed CT image.
Data Analysis and Statistical Methods
All statistical analyses were performed using SPSS Version 21.0 (SPSS Inc). Quantitative variables were presented as mean values and standard deviations with ranges. Chi-square test was used to compare categorical variables such as sex and the lateral hinge position. Continuous variables, such as age and body mass index, were compared using the independent t test for normally distributed continuous variables or the Mann-Whitney U test for nonnormally distributed data.
Predictors of LHF were evaluated using multivariate logistic regression analysis of the odds ratio (OR), with the presence of LHF considered as the dependent variable and patient sex, age, body mass index, preoperative coronal osteotomy angle, medial opening closing, and lateral hinge position as independent variables. The ORs and 95% CIs were calculated.
Univariate logistic regression analysis was used to identify the potential predictors of LHF in MCDFO. The potential predictors identified as significant in the univariate analysis were entered into multivariate logistic regression models, with the exclusion of highly correlated factors, using backward elimination methods with an entry criterion of 0.1 and an exit criterion of 0.05.
Intraobserver and interobserver reliabilities were determined by calculating the intraclass correlation coefficients (ICCs) for radiological outcome parameters such as the HKA angle, mLDFA, coronal osteotomy angle, lateral hinge position, and the absence or presence of LHF. An ICC of <0.40 was considered poor, whereas ICCs of 0.40-0.59, 0.60-0.74, and 0.75-1.00 were considered fair, good, and excellent, respectively. 5 A P value <.05 was considered statistically significant.
Results
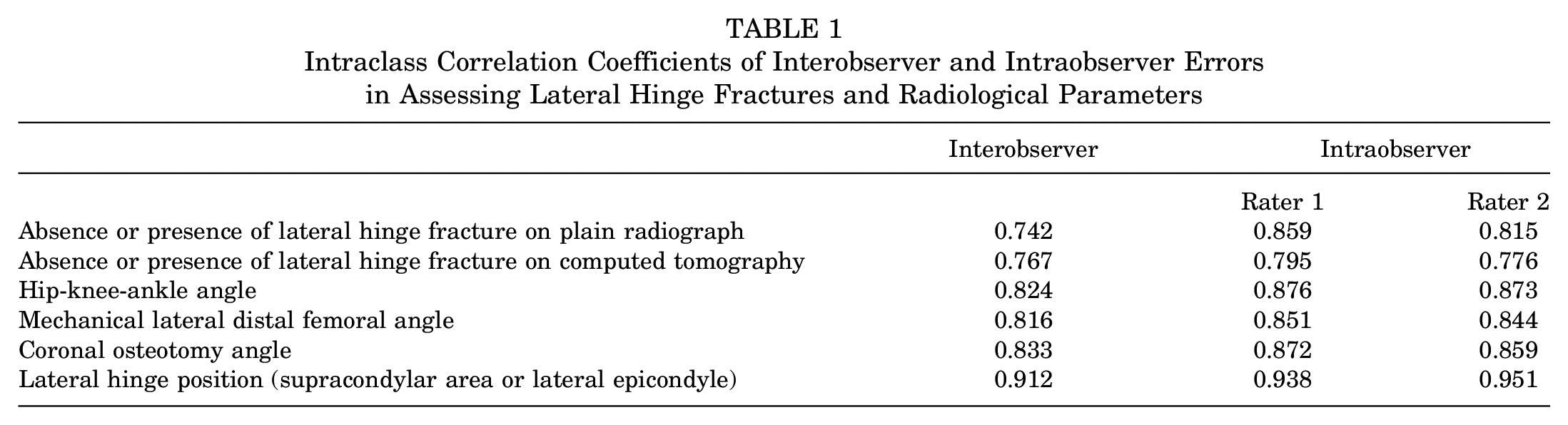
Intraobserver and interobserver reliabilities (ICC values) in determining the absence or presence of LHF and lateral hinge position indicated good to excellent reliability. Moreover, all ICC values for radiological measurements (HKA angle, mLDFA, coronal osteotomy angle, and lateral hinge position) were >0.8 (Table 1).
Intraclass Correlation Coefficients of Interobserver and Intraobserver Errors in Assessing Lateral Hinge Fractures and Radiological Parameters
In total, 74 knees of 59 patients who underwent MCDFO between May 2009 and June 2021 were initially enrolled in this study. A total of 7 knees of 6 patients were excluded because they did not undergo postoperative CT scanning (n = 3 knees) or they underwent additional operations due to postoperative complications, surgical-site infection (n = 2 knees), or postoperative ipsilateral femoral fracture (n = 2 knees). Finally, 67 knees of 53 patients (mean age, 37.4 ± 16.9 years) were enrolled in this study (32 knees of 30 patients with lateral compartment osteoarthritis and 35 knees of 23 patients with recurrent patellar dislocation).
Of the 67 knees, LHFs were identified in 21 knees (31.3%) on plain radiographs and 40 knees (59.7%) on CT scans. The detection rate of LHFs was significantly higher on CT scans than on plain radiographs (P = .001). The demographic and radiological data of the non-LHF and LHF groups are summarized in Table 2. Preoperative demographic (sex, age, affected side, and body mass index) and radiological (HKA angle, mLDFA, and coronal osteotomy angle) data were not significantly different between the non-LHF and LHF groups.
Difference in Preoperative Demographic and Radiological Data Between Non-LHF and LHF Groups a

Values are presented mean ± SD (minimum, maximum) unless otherwise noted. BMI, body mass index; HKA, hip-knee-ankle; LE, lateral epicondyle; LHF, lateral hinge fracture; LOA, lateral osteoarthritis; mLDFA, mechanical lateral distal femoral angle; RPD, recurrent patellar dislocation; SC, supracondylar area.
On plain radiographs, the medial closing gap was found to be significantly larger in the LHF group (8.3 ± 2.6 mm) than in the non-LHF group (6.0 ± 1.6 mm) (P < .001). Moreover, the proportion with the lateral hinge position in the supracondylar area was higher in the LHF group than in the non-LHF group (47.6% vs 10.9%; P = .001). On CT images, the medial closing gap was significantly larger in the LHF group (7.2 ± 2.4 mm) than in the non-LHF group (6.0 ± 1.8 mm) (P = .026). As well, the ratio of the lateral hinge position in the supracondylar area was higher in the LHF group than in the non-LHF group (32.5% vs 7.4%; P = .016).
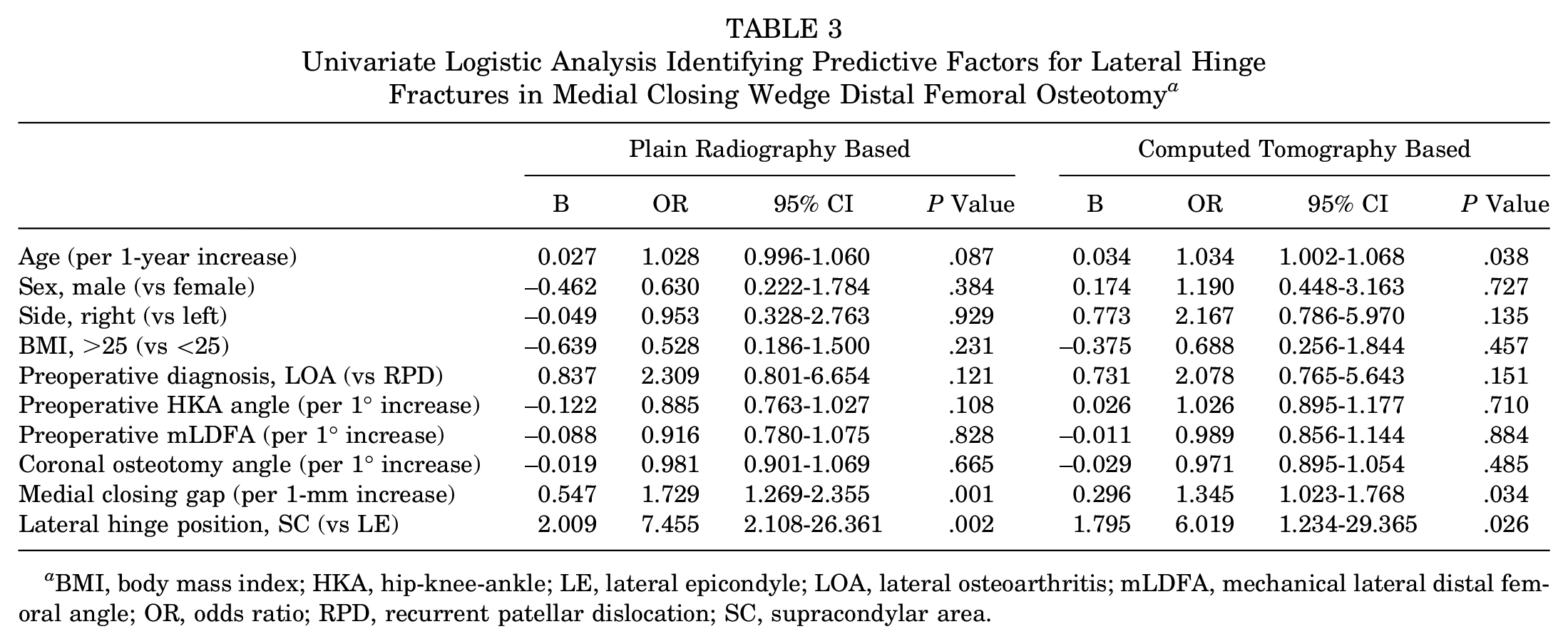
In univariate regression analysis, the medial closing gap (unadjusted OR per 1-mm increase, 1.729; 95% CI, 1.269-2.355; P = .001) and lateral hinge position in the supracondylar area (unadjusted OR, 7.455; 95% CI, 2.108-26.361; P = .002) were identified to be possible predictive factors for plain radiography–based LHF in MCDFO (P < .05) (Table 3). In contrast, age (unadjusted OR per 1-year increase, 1.034; 95% CI, 1.002-1.068; P = .038), medial closing gap (unadjusted OR per 1-mm increase, 1.345; 95% CI, 1.023-1.768; P = .034), and lateral hinge position in the supracondylar area (unadjusted OR, 6.019; 95% CI, 1.234-29.365; P = .026) were identified as possible predictive factors for CT-based LHF in MCDFO (P < .05) (Table 3).
Univariate Logistic Analysis Identifying Predictive Factors for Lateral Hinge Fractures in Medial Closing Wedge Distal Femoral Osteotomy a
BMI, body mass index; HKA, hip-knee-ankle; LE, lateral epicondyle; LOA, lateral osteoarthritis; mLDFA, mechanical lateral distal femoral angle; OR, odds ratio; RPD, recurrent patellar dislocation; SC, supracondylar area.
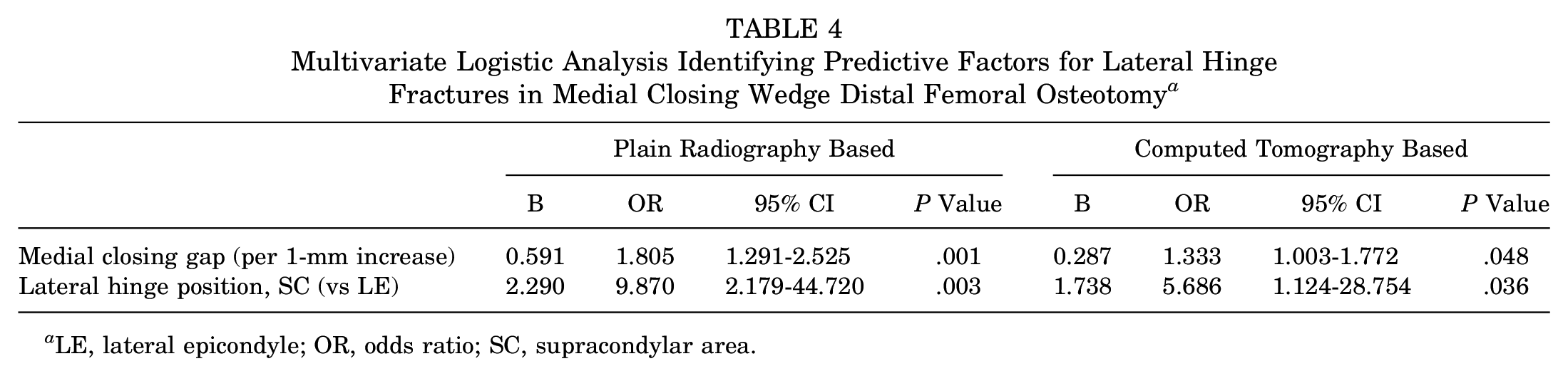
Multivariate logistic regression analysis showed that the medial closing gap and lateral hinge position were predictive factors for plain radiography– and CT-based LHF after MCDFO. Controlling for other variables, we found that a medial opening gap increase of 1 mm increased the likelihood of plain radiography–based LHF by a factor of 1.805 (95% CI, 1.291-2.525; P = .001) and CT-based LHF by 1.333 (95% CI, 1.003-1.772; P = .048) (Table 4). Moreover, a lateral hinge position in the supracondylar area increased the likelihood of plain radiography–based LHF by a factor of 9.870 (95% CI, 2.179-44.720; P = .003) and CT-based LHF by 5.686 (95% CI, 1.124-28.754; P = .036) (Table 4). The incidence of LHF according to medial opening gap and lateral hinge position is summarized in Table 5.
Multivariate Logistic Analysis Identifying Predictive Factors for Lateral Hinge Fractures in Medial Closing Wedge Distal Femoral Osteotomy a
LE, lateral epicondyle; OR, odds ratio; SC, supracondylar area.
Incidence of Lateral Hinge Fractures According to Medial Opening Gap and Lateral Hinge Position a
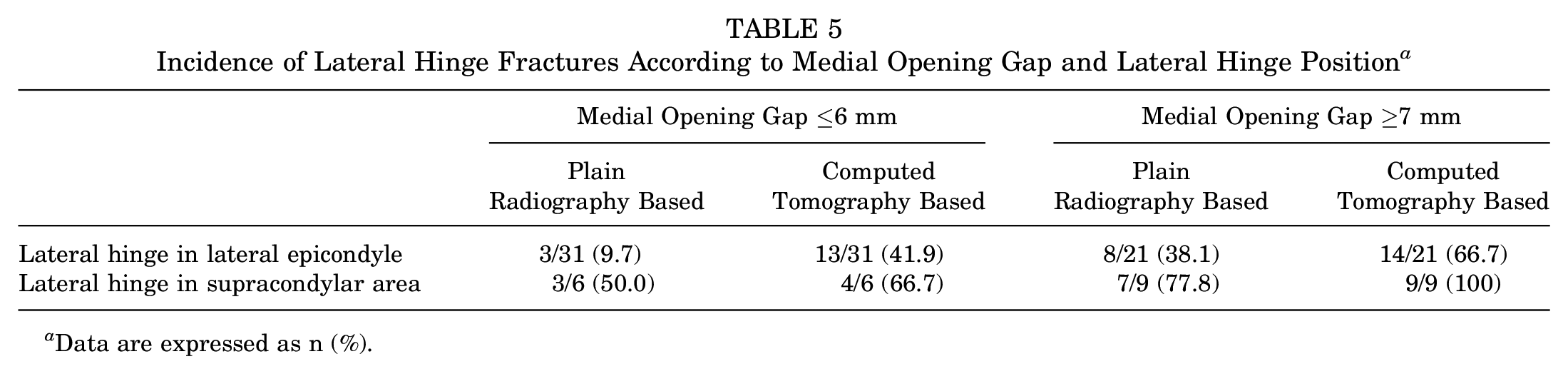
Data are expressed as n (%).
Discussion
The most important finding of this study was that a large medial closing gap and lateral hinge position in the supracondylar area increased the likelihood of LHF in MCDFO. Medial closing gap was significantly larger in the LHF group than in the non-LHF group (plain radiography based, 8.3 ± 2.6 vs 6.0 ± 1.6 mm, respectively; P < .001) (CT based, 7.2 ± 2.4 vs 6.0 ± 1.8 mm, respectively; P = .026). Moreover, the ratio of the lateral hinge position in the supracondylar area was higher in the LHF group than in the non-LHF group (plain radiography based, 47.6% vs 10.9%; P = .001) (CT based, 32.5% vs 7.4%; P = .016). Multivariate logistic regression analysis showed that the adjusted ORs of the medial opening gap (per 1-mm increase) and lateral hinge position in the supracondylar area were 1.805 and 9.870 for plain radiography–based LHF and 1.333 and 5.686 for CT-based LHF, respectively. Therefore, the results of this study suggest that the medial closing gap and lateral hinge position are predictive factors for LHF in MCDFO.
In this study, the detection rate of LHF was significantly higher on CT than on plain radiography (59.7% vs 31.3%, respectively; P < .001), which is consistent with the results of previous clinical studies. Kim et al 11 reported that the detection rate of LHF was higher on CT than on plain radiography after various types of distal femoral osteotomy (41.9% vs 29%, respectively). Nakayama et al 18 compared the incidence of medial hinge fractures after lateral closing wedge distal femoral osteotomy and reported that the incidence of medial hinge fractures was higher on CT scans than on plain radiographs (30.6% vs 19.4%, respectively). Recently, Nha et al 21 also demonstrated that the detection rate of LHF was significantly higher on CT scans than on plain radiography (60% vs 34.5%, respectively; P = .008). Therefore, CT is a more accurate method for detecting hinge fractures, and such imaging is recommended before deciding on a postoperative rehabilitation protocol after MCDFO.
Recent clinical studies have reported that LHFs can lead to problematic bone healing (nonunion, delayed union, or loss of correction) at the osteotomy site after MCDFO. Nha et al 21 reported that the incidence of problematic bone healing was significantly higher in knees with LHF than in those without LHF, as shown by plain radiography (36.8% vs 8.3%, respectively; P = .001) and CT (30.3% vs 0%, respectively; P = .004). Moreover, Fujita et al 7 demonstrated that LHF and displacement caused slow healing and loss of correction after MCDFO (67% in displaced LHF, 40% in nondisplaced LHF, and 11% in non-LHF). However, few studies have investigated the predictive factors for LHF in MCDFO. We investigated the factors affecting the occurrence of LHF after MCDFO and consequently found that the medial closing gap and lateral hinge position were predictive factors for LHF in MCDFO.
In our study, a large medial closing gap was a predictive factor for LHF in MCDFO. Few clinical studies have investigated the correlation between the lateral closing gap and the incidence of LHF in MCDFO. Previous studies reported that a large opening gap was associated with LHF in medial opening wedge high tibial osteotomy (MOHTO).8,10,14 Lee et al 14 reported that a large opening gap was a risk factor for LHF in MOHTO (OR, 1.615; 95% CI, 1.232-2.118; P = .001). Han et al 8 demonstrated that the osteotomy gap height was the only predictor of LHF (adjusted OR, 1.831; P = .016). The results of these studies may be attributable to the fact that the plastic deformation of the lateral cortical hinge is limited in cases with large closing gaps. Therefore, careful attention and subtle adjustments are required to prevent hinge fractures during the opening or closing of the osteotomy site. Moreover, precise evaluation of hinge fractures and conservative rehabilitation protocols should be performed after osteotomy around the knee.
Although few clinical studies have investigated the relationship between the lateral hinge position and LHF in MCDFO, several cadaveric studies have investigated the ideal location of the lateral hinge to prevent LHF in MCDFO.12,19 Nha et al 19 found that 8 of 10 cadaveric knees with supracondylar hinge had LHFs during closure of the osteotomy gap, and all fractured knees were unstable. In contrast, only 2 of 10 knees with lateral condylar hinges had LHFs. The investigators explained that the lower incidence of LHF may be attributed to the superior capacity of plastic deformation of the metaphysis compared with that of the diaphysis or to the fact that the lateral condylar hinge has an intact posterior bony bridge in the posterior condyle of the distal femur. Moreover, Kim et al 12 compared the incidence of LHF during MCDFO in knees where the lateral hinge was located either inside or outside of the femoral attachment of the gastrocnemius lateral head. The investigators reported that the incidence of unstable LHF during MCDFO significantly decreased when the lateral hinge was positioned inside the femoral attachment of the gastrocnemius lateral head versus outside (0% vs 50%, respectively; P = .01). Kim et al 12 further explained that the femoral attachment of the gastrocnemius lateral head serves as a soft tissue stabilizer during MCDFO. In their cadaveric study, the footprint of the lateral head of the gastrocnemius was located in the metaphyseal area of the lateral femoral condyle. In the present clinical study, we found that the ratio of the lateral hinge position in the supracondylar area was higher in the LHF group than in the non-LHF group. Therefore, the findings of the present study are consistent with those of the previous cadaveric studies.
Previous studies have reported that a steep coronal osteotomy angle affects the development of LHF in MOHTO. Lee et al 13 reported that the coronal osteotomy slope was significantly larger in the LHF group than in the non-LHF group (20.3°± 5.1° vs 16.7°± 4.2°, respectively; P = .001). Choi et al 4 also reported that coronal osteotomy angle was one of the significant modifiable factors to prevent LHF in MOHTO. Lee et al 13 explained that if osteotomy is performed with an abrupt angle on the coronal plane in MOHTO, the thickness of the posterolateral bony bridge would be reduced and the risk of developing LHF would be increased. Based on the results of these studies, we considered the coronal osteotomy angle to be an independent variable causing LHF in MCDFO. Consequently, there was no significant correlation between the coronal osteotomy angle and LHF in MCDFO.
This study has several limitations. First, it was a retrospective study. Therefore, a selection bias may have influenced our results. Second, MCDFOs were performed for 2 indications, lateral osteoarthritis and recurrent patellar dislocation, and therefore the patient cohorts were different; lateral osteoarthritis mainly occurs in older patients, whereas recurrent patellar dislocation occurs in younger patients. However, the mean age of the LHF and non-LHF groups was not significantly different, and patient age was considered an independent variable in the multivariate logistic regression analysis. Third, this study evaluated only the predictive factors for LHF in MCDFO. Therefore, the effects of LHF on bone healing at the osteotomy site and clinical outcomes could not be investigated in this study.
The strength of this study is that it comprehensively analyzed the predictive factors for LHF. We found that a large medial closing gap and lateral hinge position in the supracondylar area are predictive factors for LHF in MCDFO. Therefore, care should be taken to prevent LHF in MCDFO with a large medial closing gap. Moreover, a lateral hinge position in the supracondylar area should be avoided in order to decrease the incidence of LHF in MCDFO.
Conclusion
A large medial closing gap and lateral hinge position in the supracondylar area are associated with LHF in MCDFO. Care should be taken to prevent LHF in MCDFO with a large medial closing gap. Moreover, a lateral hinge position in the supracondylar area should be avoided in order to decrease the incidence of LHF in MCDFO.
Footnotes
Submitted February 24, 2022; accepted August 24, 2022.
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.