
Abstract
Background:
Quantitative magnetic resonance imaging (qMRI) methods were developed to establish the integrity of healing anterior cruciate ligaments (ACLs) and grafts. Whether qMRI variables predict risk of reinjury is unknown.
Purpose:
To determine if qMRI measures at 6 to 9 months after bridge-enhanced ACL restoration (BEAR) can predict the risk of revision surgery within 2 years of the index procedure.
Study Design:
Cohort study; Level of evidence, 2.
Methods:
Originally, 124 patients underwent ACL restoration as part of the BEAR I, BEAR II, and BEAR III prospective trials and had consented to undergo an MRI of the surgical knee 6 to 9 months after surgery. Only 1 participant was lost to follow-up, and 4 did not undergo MRI, leaving a total of 119 patients for this study. qMRI techniques were used to determine the mean cross-sectional area; normalized signal intensity; and a qMRI-based predicted failure load, which was calculated using a prespecified equation based on cross-sectional area and normalized signal intensity. Patient-reported outcomes (International Knee Documentation Committee subjective score), clinical measures (hamstring strength, quadriceps strength, and side-to-side knee laxity), and functional outcomes (single-leg hop) were also measured at 6 to 9 months after surgery. Univariate and multivariable analyses were performed to determine the odds ratios (ORs) for revision surgery based on the qMRI and non-imaging variables. Patient age and medial posterior tibial slope values were included as covariates.
Results:
In total, 119 patients (97%), with a median age of 17.6 years, underwent MRI between 6 and 9 months postoperatively. Sixteen of 119 patients (13%) required revision ACL surgery. In univariate analyses, higher International Knee Documentation Committee subjective score at 6 to 9 months postoperatively (OR = 1.66 per 10-point increase; P = .035) and lower qMRI-based predicted failure load (OR = 0.66 per 100-N increase; P = .014) were associated with increased risk of revision surgery. In the multivariable model, when adjusted for age and posterior tibial slope, the qMRI-based predicted failure load was the only significant predictor of revision surgery (OR = 0.71 per 100 N; P = .044).
Conclusion:
Quantitative MRI-based predicted failure load of the healing ACL was a significant predictor of the risk of revision within 2 years after BEAR surgery. The current findings highlight the potential utility of early qMRI in the postoperative management of patients undergoing the BEAR procedure.
Keywords
Anterior cruciate ligament (ACL) injuries are common in the young active population. For these patients, the desire to regain function and to return to sports is high, and clinical outcomes with nonoperative management are uniformly poor; thus, surgical treatments such as ACL reconstruction (ACLR) are commonly performed. 28 However, only about half of the patients after ACLR are able to return to their preinjury activity level, with an estimated 1 in 4 having a second ACL injury within the first year after surgery.21,28 Numerous factors, such as age, activity level, anatomic features, and graft type, are associated with increased risk of reinjury after ACLR. 24 Given the shortcomings of ACLR (ie, comorbidities due to graft harvest, risk of posttraumatic osteoarthritis), new surgical methods to repair or restore the native ACL have been introduced.17,20,33,48 One such approach, bridge-enhanced ACL restoration (BEAR), is a surgical procedure that stimulates ACL healing by placing an extracellular matrix–based implant within the injury site and using it to hold the patient’s blood in the space between the torn ends of the ligament.32-34,51 The blood-collagen scaffold composite subsequently creates an environment that is biologically conducive to ligament healing. As the BEAR technique is relatively new, postoperative outcome measures that can predict risk factors for reinjury and subsequent revision surgery remain unknown in patients who undergo the BEAR procedure.
Younger age 24 and steeper posterior tibial slope9,44,52 have been identified as risk factors for an ACL graft retear. Moreover, postoperative patient-reported outcomes (eg, International Knee Documentation Committee [IKDC] subjective score),23,36,43 clinical outcomes (eg, arthrometer-based knee laxity testing), 50 and asymmetry in joint function (eg, single-leg hop test) 43 have also been used to track ACLR recovery and to approximate reinjury risk. However, studies have shown that patient-reported outcome measures (eg, IKDC) introduce bias and inconsistency when compared with more objective methods.1,2 Furthermore, these discrepancies become more apparent when comparing various validated knee outcome scores.1,22 Most important, none of these commonly used outcome measures directly assesses the structural integrity of the healing ACL or ACL graft.1,2
To supplement the existing patient-reported, clinical, and functional assessments, noninvasive imaging methods have been developed to evaluate graft maturity and to estimate the structural properties of the surgically treated ACL using quantitative magnetic resonance imaging (qMRI).6,8,25,26,46,49 Studies have determined that changes in qMRI parameters, such as signal intensity (SI), volume, and cross-sectional area (CSA) of the ligament or graft, can be used to determine the integrity of the healing structures, as these parameters have been shown to reflect the biomechanical and histologic properties of the healing tissues.4,6,8,54 Despite promising preclinical and clinical evidence on the utility of qMRI for the noninvasive assessment of the healing ACL structural properties and postoperative remodeling, these techniques have not yet become mainstream. Possible reasons for this include technical challenges in standardizing image acquisition parameters or post hoc harmonization for consistent qMRI results,16,49 as well as the lack of high-quality evidence on the relative performance of qMRI metrics in predicting ACL surgery outcomes and reinjury risk.
The purpose of this preliminary study was to analyze the prospectively collected data from the BEAR clinical trials to determine if early qMRI parameters (eg, those obtained at 6 months or 9 months after ACL surgery) were associated with the risk of revision surgery during the 2 years after the BEAR procedure. The 6- to 9-month window was selected as it corresponds to the time that patients are typically cleared to go back to sports. We also assessed the ability of common patient-reported (eg, IKDC), clinical (eg, anteroposterior knee laxity), and functional (eg, single-leg hop ratio for distance, isometric quadriceps, and hamstring strength) outcomes, all collected at 6 to 9 months postoperatively, to predict the 2-year revision risk in the same cohort. We hypothesized that (1) qMRI-based measures of the healing ACL structural properties (eg, mean CSA, normalized ligamentous SI, and predicted failure load) at 6 to 9 months would predict the risk of ipsilateral revision within 2 years of the BEAR procedure and (2) qMRI-based measures could improve the ability to predict the risk of ipsilateral revision after considering baseline variables (eg, age, medial posterior tibial slope)9,13,44,52 and patient-reported, clinical, and functional outcomes at 6 to 9 months in the multivariable regression analyses.23,36,43,50
Methods
Participants
Data were acquired from patients enrolled in the BEAR I (NCT02292004; IRB-P00012985), 34 BEAR II (NCT02 664545; IRB-P00021470), 33 and BEAR III (NCT03348995; IRB-P00026162) 45 clinical trials between February 2015 and January 2019. The 3 trials were approved by the institutional review boards, and all participants granted their informed consent before participating. BEAR I was a nonrandomized controlled cohort study with 10 patients in the BEAR arm, 34 BEAR II was a randomized controlled trial with 65 patients in the BEAR arm, 33 and BEAR III was a prospective dual-center cohort study with 49 patients in the BEAR arm (Figure 1). 45 Patients were excluded from these trials if they had a history of knee surgery; knee infection; or potentially adverse risk factors, including a history of nicotine use, corticosteroid use, chemotherapy, diabetes, inflammatory arthritis, sickle cell anemia, or anaphylaxis. Patients with concomitant injury to the posterolateral corner, grade III medial collateral ligament injury, or complete patellar dislocation were also excluded. Of the 124 patients who underwent the BEAR procedure, 119 had imaging data to carry out the analysis (97%) (Figure 1), and revision surgery data were available for the 119 patients at 2 years (100%). A complete description of the inclusion and exclusion criteria has been previously published.33,34
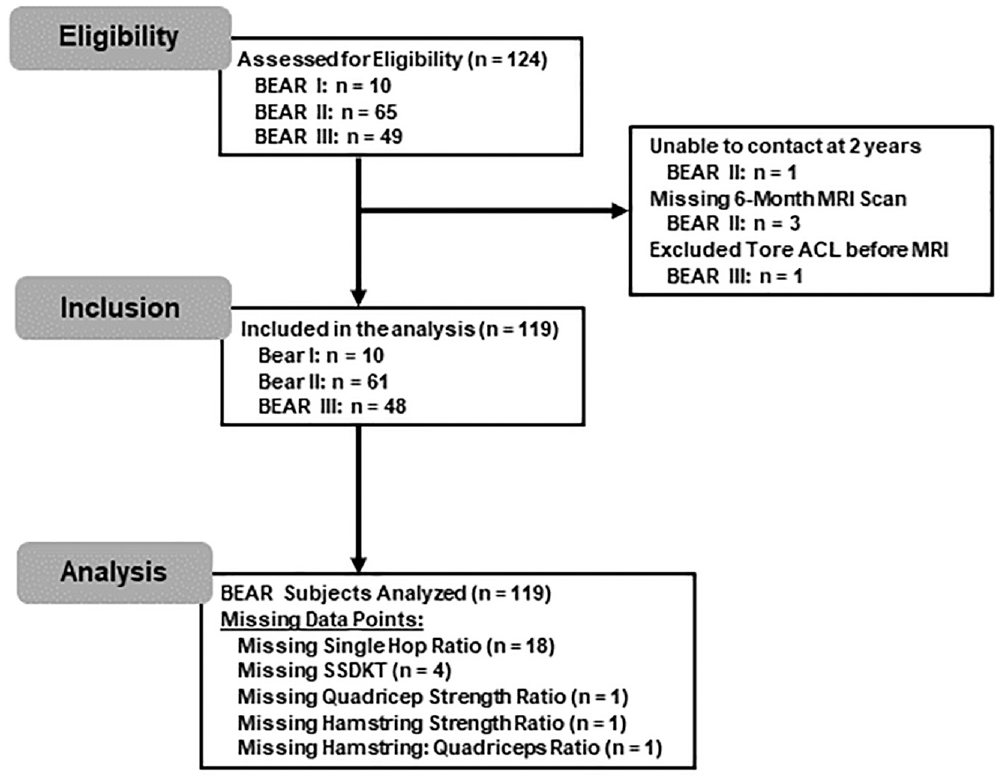
STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) diagram detailing the flow of patients through the analysis. BEAR, bridge-enhanced anterior cruciate (ACL) ligament restoration; SSDKT, side-to-side difference in KT knee laxity. MRI, magnetic resonance imaging.
Surgical Procedure
The BEAR procedure uses a resorbable implant to provide a platform on which the patient’s blood can stimulate the torn ACL to heal. 39 The implant is a scaffold composed of bovine extracellular matrix proteins, primarily collagen, which acts to hold autologous blood between the torn ligament ends. The scaffolds were manufactured at Boston Children’s Hospital. 40 Investigational device exemptions for use of the implant in the 3 trials were granted by the US Food and Drug Administration.
Details of the BEAR procedure have been previously described.33,34 In brief, a whipstitch (Vicryl; Ethicon) was placed in the tibial stump. A cortical button combined with a polyester suture stent (Ethibond; Ethicon) was passed through the femoral tunnel and secured to the proximal femoral cortex. The polyester sutures were threaded through the BEAR scaffold and a tibial tunnel and secured in place using an extracortical button. The scaffold was then saturated with 5 to 10 mL of the patient’s blood, and the tibial stump was pulled into the saturated scaffold to repair the ACL.33,34
Magnetic Resonance Imaging
MRI was performed 6 to 9 months after surgery on a 3T scanner (Tim Trio or Prisma; Siemens) using a 15-channel transmit/receive knee coil (Siemens). For the BEAR I and II clinical trials, the Constructive Interference in Steady State sequence was acquired for the surgical limb on the Tim Trio (Table 1). For the BEAR III trial, both the Tim Trio and the Prisma were used (Table 1). Harmonization to standardize the images between the 2 scanners was performed as previously described. 16 The Prisma scans were scaled to the Tim Trio scans due to hardware-necessitated differences in the sequence acquisition parameters (Table 1). The ACL was then segmented from the MRI stack by an observer with >8 years of experience in ACL segmentation (A.M.K.) using commercial imaging software (Mimics; Materialise).
MRI Acquisition Parameters for Constructive Interference in Steady-State Sequence on Tim Trio and Prisma Scanners a
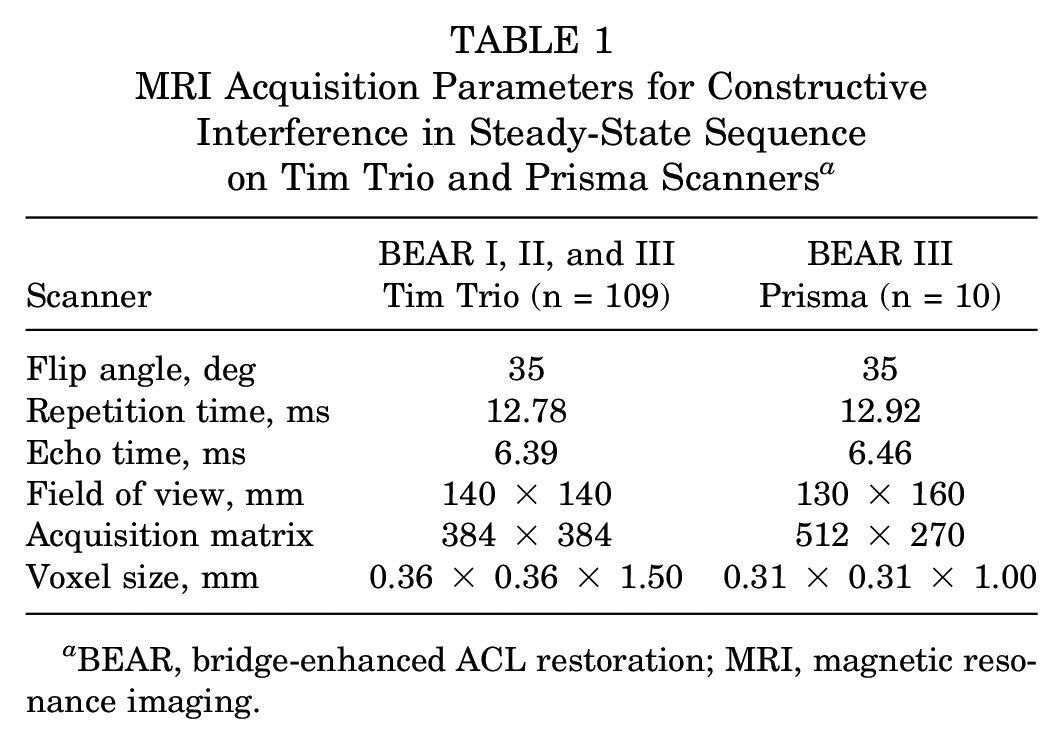
BEAR, bridge-enhanced ACL restoration; MRI, magnetic resonance imaging.
qMRI Outcome Measures
Postoperative MRI scans obtained at 6 to 9 months were used to determine the normalized SI and mean CSA of the ACL. The normalized SI was calculated from the values of each voxel within the segmented ACL, normalized to the SI of the anterior cortex of the femur, and log base-2 transformed as the data were not normally distributed (equation 1). 5 The anterior cortex of the femur was selected because it is consistently near the noise floor. The difference in background noise texture between scanners was used as a scaling term to harmonize the scanners (ΔNoise). 5 The mean CSA was calculated by dividing the ACL volume by the ACL length. The qMRI prediction model of ACL failure load was previously determined using a porcine model of ACL repair, from which qMRI and tensile failure data were available. 5 The models were scaled to humans by exchanging the ligament volume parameter of the previous study with the mean CSA to account for ligament size differences between pigs and humans. The updated model used normalized SI and CSA as independent variables to predict the failure load of the ACL (Fmax) (equation 2). All measurements were completed within 1 month of imaging and values were stored until the 2-year outcomes were measured. The imaging examiner (A.M.K.) was blinded to the postoperative outcomes.


Preoperative MR images were used to measure the posterior slope of the tibial plateau in the medial compartment (ie, medial posterior tibial slope) as previously described.25,26 The medial posterior tibial slope was measured in a sagittal slice at the center of the medial plateau as the angle between a line that joined the peak points on the anterior and posterior rims of the plateau and as a line perpendicular to the longitudinal axis of the tibia. Measurements were performed based on established techniques by an experienced member (A.M.K.) using a commercially available image viewer (Osirix Viewer Version 8.5; Pixmeo SARL).25,26
Patient Follow-up and Nonimaging Outcome Measures
Six patient-reported, clinical, and functional outcomes were assessed between 6 and 9 months after surgery: (1) the IKDC subjective score,23,36 (2) the side-to-side difference in KT knee laxity, 12 (3) the quadriceps strength ratio (% surgical/contralateral), 3 (4) the hamstring strength ratio (% surgical/contralateral), 3 (5) quadriceps-hamstring strength ratio of the surgical leg, 3 and (6) single-leg hop ratio (% surgical/contralateral). 43 The IKDC subjective score was calculated based on patients’ responses to the IKDC questionnaire.23,36 The arthrometer measurements (KT-1000 arthrometer; MEDMetric) were performed by an experienced independent examiner, who was blinded to surgical laterality and treatment using knee sleeves. Hamstring and quadriceps isometric muscle strength was measured using a handheld dynamometer (Microfet 2; Hoggan Scientific, LLC). All measures were performed on each knee in duplicate, and the duplicates were averaged. 3 During the single-leg hop test, patients wore a brace on the surgically treated knee.
Patients were assessed for initial eligibility (n = 124). Patients missing a 6- or 9-month MRI scan were excluded (n = 4), and 1 patient was lost to follow-up at 2 years (n = 1). The final cohort of participants with BEAR who returned 2 years after surgery for clinical assessment and to verify repair status included 119 patients (Figure 1).
Statistical Analysis
Logistic regression analyses were performed (G.J.B.) to identify outcomes obtained at 6 to 9 months postoperatively, including qMRI; patient-reported, clinical, and functional outcomes; and baseline variables that were significant predictors of revision surgery before the 2-year assessment. First, unadjusted odds ratios were estimated for each variable using univariate logistic regression (ie, 1 predictor at a time). Next, a multivariable logistic regression model using a forward stepwise procedure was implemented to determine the best set of predictors of subsequent revision and their associated adjusted odds ratios. To limit the number of potential predictors, we only considered variables with P < .20 for their bivariate relationship with 2-year revision as candidates for the multivariable model. Two baseline variables, age at surgery and medial posterior tibial slope, were forced into the multivariable stepwise model (ie, step 0), as they have been previously shown to be predictive of revision. 45 Because listwise deletion of cases due to incomplete data on candidate clinical variables (Figure 1) adversely affects the sample size used for the stepwise multivariable regression model, a multiple imputation procedure was used (n = 5 iterations) to allow the use of all cases in the multivariable analyses. 57 All analyses were conducted using SAS Statistical Software Version 9.4 (SAS Institute) with statistical significance based on P < .05.
Results
Baseline Characteristics, qMRI, and Nonimaging Outcomes
The mean ± SD age of the patients in the 3 studies was 17.6 ± 7.1 years; 64 (54%) of the patients were female; 98 (82%) of the patients were White (non-Hispanic). The mean ± SD of the body mass index was 23.9 ± 3.4. The mean ± SD of the medial posterior tibial slope was 5.2°± 2.4°. Table 2 presents the qMRI, patient-reported, clinical, and functional outcomes recorded at 6 to 9 months postoperatively, considered potential predictors of revision surgery.
qMRI and Nonimaging Outcome Measures (N = 119) a
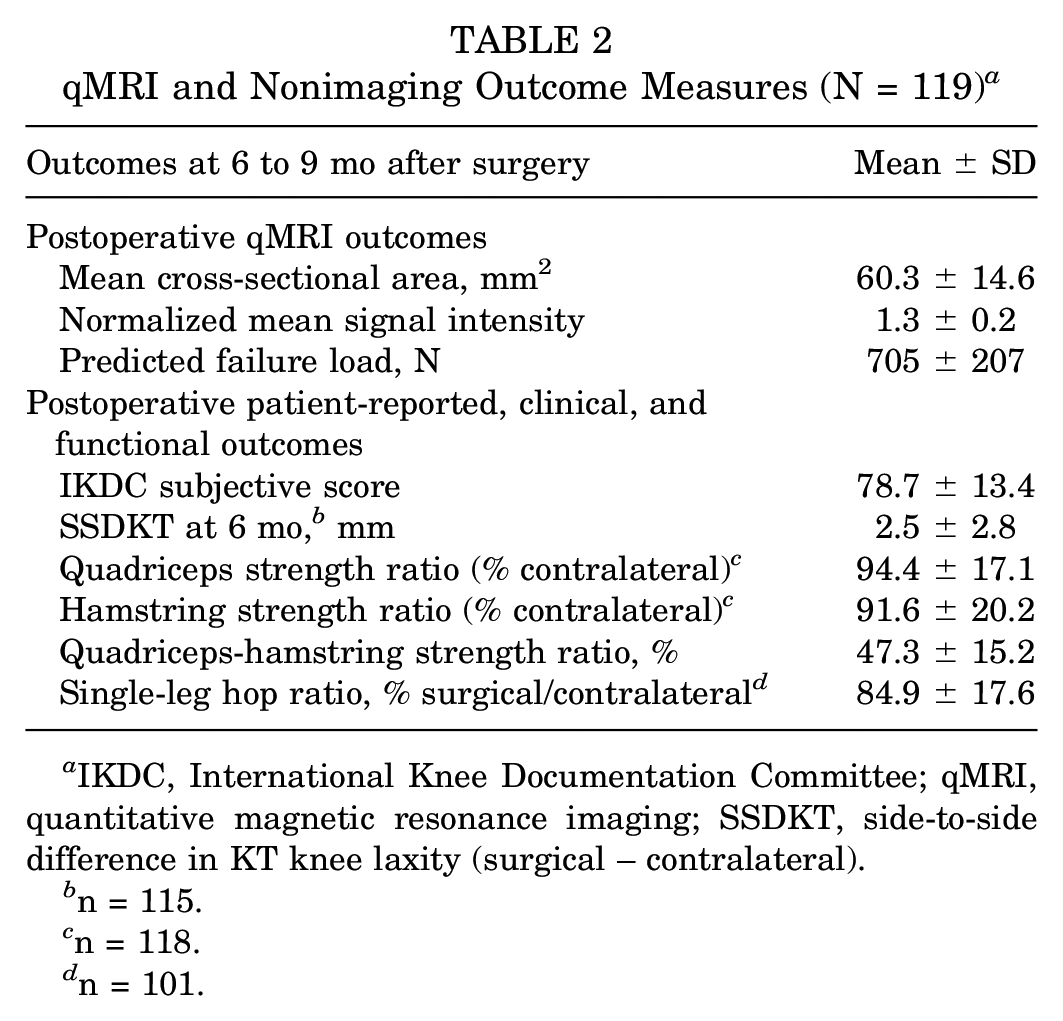
IKDC, International Knee Documentation Committee; qMRI, quantitative magnetic resonance imaging; SSDKT, side-to-side difference in KT knee laxity (surgical – contralateral).
n = 115.
n = 118.
n = 101.
Univariate Predictors of 2-Year Revision
Sixteen (13%) of the 119 analyzed patients required revision surgery before the 2-year follow-up visit. Outcomes significantly associated with increased risk of revision at 2 years were higher IKDC subjective score at 6 to 9 months postoperatively (P = .035) and lower predicted failure load on the 6- to 9-month postoperative qMRI outcomes (P = .014) (Table 3). Each 10-unit increase in IKDC subjective score (total range 100 points) corresponded to a 66% increase in the odds of revision ACL surgery. Additionally, a 100-N increase in qMRI-predicted failure load corresponded to a 34% decrease in the odds of revision. The mean CSA and normalized SI on the 6- to 9-month qMRI outcomes were marginally associated with increased odds of revision (P < .06), with lower mean CSA and higher normalized SI associated with increased risk of 2-year revision (Table 3).
Unadjusted Odds Ratios Associated With Revision by 2-y Follow-up a
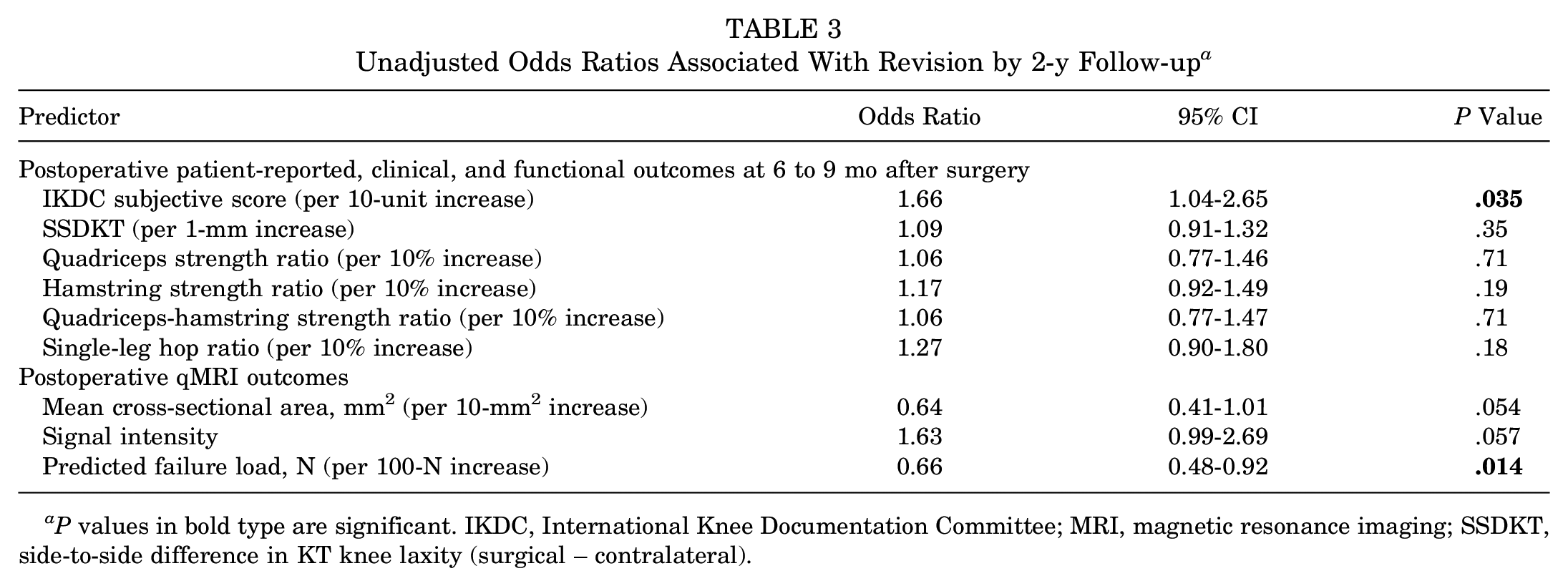
P values in bold type are significant. IKDC, International Knee Documentation Committee; MRI, magnetic resonance imaging; SSDKT, side-to-side difference in KT knee laxity (surgical – contralateral).
Multivariable Predictors of 2-Year Revision
After adjusting for patient age and medial posterior tibial slope in the multivariable analysis, the 6- to 9-month postoperative qMRI-predicted failure load was the only significant predictor of 2-year revision risk after BEAR (Table 4). Each 100-N increase in predicted failure load at 6 to 9 months corresponded to a 29% decrease in the odds of revision ACL surgery by 2 years postoperatively (Table 4).
Adjusted Odds Ratios Associated With Revision Surgery on Multivariable Stepwise Logistic Regression a
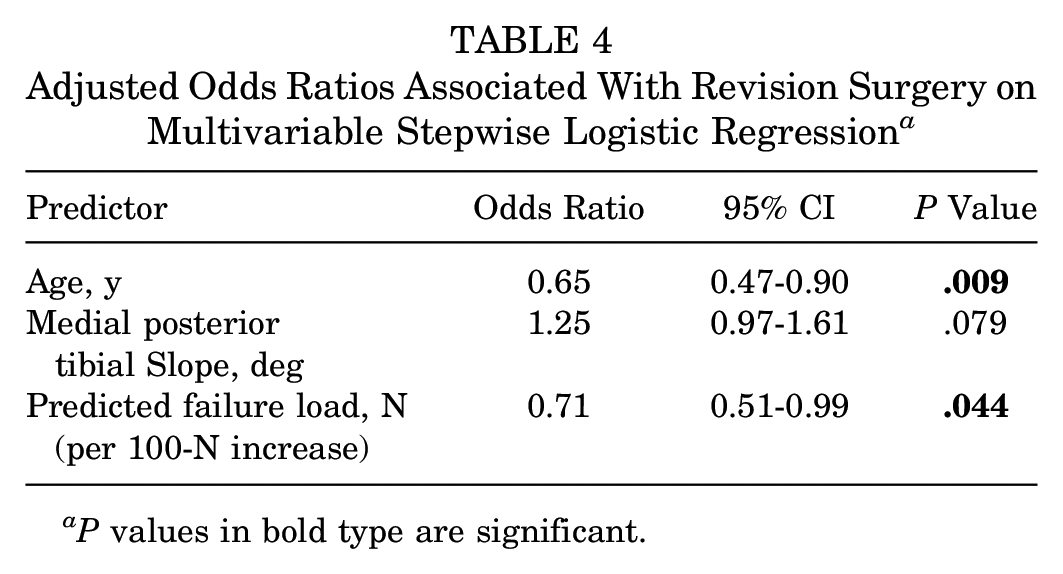
P values in bold type are significant.
Discussion
The significant finding of the study was that an increase in predicted failure load of the healing ACL, as measured via qMRI at 6 to 9 months after surgery, was associated with decreased odds of revision surgery by 2 years. Predicted failure load remained a significant predictor after adjusting for baseline variables (ie, age, medial posterior tibial slope). Patient-reported, clinical, and functional outcomes at 6 to 9 months did not contribute to the predictive ability of revision in the multivariable model.
Traditionally, return-to-sports decisions are based on time, with athletes typically being returned to sports at 6 to 9 months after surgery. 58 More recently, some surgeons have also included a battery of patient-reported, clinical, and functional outcomes to guide the postoperative care plan—in particular, the time for safe return to sports.7,8,53 Acceptable scores on assessments, such as subjective rating scales, knee laxity tests, and functional hop testing, have been used to determine a patient’s readiness to return to play. 8 These outcomes remain controversial as studies have shown reinjuries occurring shortly after using these assessments to decide if a patient is ready to return to sports.11,38,42,55 Moreover, these assessments lack sufficient resolution to directly assess the healing ligament and are often influenced by factors unrelated to the ACL structure. For example, physical examinations of the knee (eg, the Lachman and pivot-shift tests) can be influenced by the injury or hypertrophy of secondary stabilizers of the knee,19,47 as well as by age, 29 sex, 29 and bony anatomy, 35 and are also prone to observer bias. Functional testing (eg, hop testing and balance testing) can be influenced by the quality of the rehabilitation program, patient compliance, and/or fear of reinjury.10,37 Likewise, patient-reported outcomes after ACL surgery have been shown to be influenced by self-esteem levels, 10 body mass index, 30 and smoking. 30 All of these support the need to improve current clearance protocols, including the addition of noninvasive qMRI approaches to directly assess the healing ligament. These techniques have been shown to identify detailed structural changes in the healing ligament and provide an objective evaluation of ligament maturation and remodeling after surgery.25,26,49 Our current observations are in agreement with a recent study that focused on signal intensity, indicating an increased risk of hamstring autograft failure in patients with a higher signal intensity ratio at 1 year. 41 The current study used a combination of SI and CSA to measure failure load to predict the risk of revision surgery, which was evaluated in both univariate and multivariable settings.
In the current study, among all the patient-reported, clinical, and functional outcomes, only the IKDC subjective outcome score at 6 to 9 months was associated with subsequent failure in a univariate analysis. Interestingly, the results of this study demonstrated that a higher IKDC subjective score was predictive of a higher risk of revision after BEAR, while previous work has demonstrated the opposite for patients with ACLR, in whom a higher IKDC score has been associated with a lower risk of revision surgery.10,31,56 One possible explanation for this finding is that patients with a higher IKDC score felt better sooner and may have returned to activities earlier as a result. 10 Further work to better quantify postoperative activity levels in patients with BEAR is planned and should verify or invalidate this hypothesis.
A previous porcine study, 5 which used a similar sequence to that used in the current study, demonstrated that size (volume) and normalized SI were independent predictor variables of the maximum failure load and that an increase in tissue volume and a decrease in normalized SI were related to a higher maximum failure load. Furthermore, it was determined in the porcine study that the combination of both variables in the maximum failure load prediction model provided a significant improvement in the prediction of the maximum failure load (R2 = 0.73), compared with either variable by itself (R2≤ 0.56). 5 These previous findings align with those of the current study, as it would be expected that an increase in the healing ACL failure load would lessen the risk of revision surgery. These findings complement previous reports of temporal changes in ACL or graft-normalized SI within 2 years after surgery, corresponding to tissue healing,25,26 and those associated with high graft SI corresponding to incomplete healing and integration,18,27,41 as well as graft rupture within 1 year after ACLR. 41
To our knowledge, postoperative qMRI parameters have not been used to measure the risk of ACL revision surgery in patients with BEAR. This study, therefore, provides new insight by suggesting that the predicted failure load, as calculated using qMRI techniques at 6 to 9 months, is associated with the risk of revision by 2 years after surgery. This result indicates that for every 100-N increase in predicted failure load measured at 6 to 9 months, the odds of revision by 2 years significantly decrease by 29%. This result provides evidence that a direct assessment of ACL integrity provides valuable data to predict the risk of ACL restoration failure. Future prospective studies are needed to assess whether the use of qMRI assessment can reduce ACL revision surgery when making return-to-sports decisions. A strength of this study was the small number of patients lost to follow-up, with 120 of the original 124 patients receiving the 6- to 9-month MRI and 119 patients providing information on revision surgery at the 2-year follow-up. An additional strength of this study was that the qMRI assessor was blinded to postoperative outcomes and did not know which patients had reinjured their ACL at the time of the analysis. The qMRI data were collected at the 6- to 9-month time point and analyzed before obtaining the revision data for all patients.
This study also has limitations. The total sample size (N = 119) of this cohort and the number of revisions (n = 16) were relatively small. Accordingly, derived confidence intervals for the estimated odds ratios were quite wide. A larger study would lead to more precise point estimates and may potentially identify additional factors with smaller effect sizes that may also be associated with failure. Nonetheless, both the univariate and multivariable analyses showed that the qMRI-predicted failure load was associated with subsequent revision surgery. In addition, this study only evaluated the outcomes of patients undergoing the BEAR procedure. However, the qMRI methods used in this study could potentially be applied to patients with ACLR or primary repair as well. Therefore, it would be interesting to determine the relationships between the qMRI parameters and graft failure after ACLR or primary repair in future studies. While patients with ACLR were included in the BEAR I and II trials, the sample size of the ACLR patients (n = 10 and n = 35, respectively) was too small to be considered for this analysis.33,34 Another limitation was that the MR images were only acquired using scanners by 1 manufacturer. Future studies should explore if these same equations and qMRI methods would be applicable when different manufacturer magnets are used. Last, the imaging was performed using a Tim Trio scanner in the single-site BEAR I and II trials, while both the Tim Trio and Prisma scanners were used in the BEAR III trial. However, a recently validated harmonization procedure was used to standardize the qMRI images between scanners. 16 Future large-scale prospective studies are needed to confirm the current findings and assess the utility of qMRI in revision prediction after ACLR.
The current study provides an example of how qMRI parameters can be used to assess the integrity of a healing ACL after the BEAR procedure. Several hurdles, including cost, must be overcome to translate qMRI in routine clinical practice to predict the integrity of the healing ligament or graft. To aid in translation, we have developed harmonization procedures to standardize qMRI results between scanners. 16 We have also engineered automatic ACL segmentation techniques to reduce the segmentation time from hours to seconds to obtain the qMRI parameters required for the prediction.14,15 An automatic pipeline that includes image harmonization, ACL segmentation, and the predicted equations to determine the failure properties of the healing ligament is under development. We intend to extend the postprocessing pipeline to include ACL grafts to increase generalizability and to help facilitate the clinical translation of qMRI. Quantitative MRI provides a tool to evaluate rehabilitation progress and assist with return-to-sports decisions when needed in light of the additional costs of an MRI.
In conclusion, qMRI outcomes obtained at 6 to 9 months after bridge-enhanced ACL restoration surgery determined that the predicted failure load at that time point was a significant predictor of revision ACL surgery within 2 years of the BEAR procedure. Taken together, these data suggest that a direct measure of the structural properties of the healing ligament using qMRI techniques may be beneficial to assess rehabilitation progress and inform return-to-sports decisions.
Authors
Dominique A. Barnes, BS (Department of Orthopaedics, Warren Alpert Medical School of Brown University/Rhode Island Hospital, Providence, Rhode Island, USA); Gary J. Badger, MS (Department of Medical Biostatistics, Larner College of Medicine, University of Vermont, Burlington, Vermont, USA);Yi-Meng Yen, MD, PhD (Department of Orthopaedic Surgery, Boston Children’s Hospital, Harvard Medical School, Boston, Massachusetts, USA); Lyle J. Micheli, MD (Department of Orthopaedic Surgery, Boston Children’s Hospital, Harvard Medical School, Boston, Massachusetts, USA); Dennis E. Kramer, MD (Department of Orthopaedic Surgery, Boston Children’s Hospital, Harvard Medical School, Boston, Massachusetts, USA); Paul D. Fadale, MD (Department of Orthopaedics, Warren Alpert Medical School of Brown University, Providence, Rhode Island, USA); Michael J. Hulstyn, MD (Department of Orthopaedics, Warren Alpert Medical School of Brown University, Providence, Rhode Island, USA); Brett D. Owens, MD (Department of Orthopaedics, Warren Alpert Medical School of Brown University, Providence, Rhode Island, USA); The BEAR Trial Team (Sean W. Flannery, PhD [Department of Orthopaedics, Warren Alpert Medical School of Brown University/Rhode Island Hospital, Providence, Rhode Island, USA]; Kirsten Ecklund, MS [Department of Orthopaedic Surgery, Boston Children’s Hospital, Harvard Medical School, Boston, Massachusetts, USA]; Ryan M. Sanborn, BA [Department of Orthopaedic Surgery, Boston Children’s Hospital, Harvard Medical School, Boston, Massachusetts, USA]; Meggin Q. Costa, BA [Department of Orthopaedics, Warren Alpert Medical School of Brown University/Rhode Island Hospital, Providence, Rhode Island, USA]; Cynthia Chrostek, BS [Department of Orthopaedics, Warren Alpert Medical School of Brown University/Rhode Island Hospital, Providence, Rhode Island, USA]; Benedikt L. Proffen, MD [Department of Orthopaedic Surgery, Boston Children’s Hospital, Harvard Medical School, Boston, Massachusetts, USA]; Nicholas Sant, BS [Department of Orthopaedic Surgery, Boston Children’s Hospital, Harvard Medical School, Boston, Massachusetts, USA]); Martha M. Murray, MD (Department of Orthopaedic Surgery, Boston Children’s Hospital, Harvard Medical School, Boston, Massachusetts, USA); Braden C. Fleming, PhD (Department of Orthopaedics, Warren Alpert Medical School of Brown University/Rhode Island Hospital, Providence, Rhode Island, USA); and Ata M. Kiapour, PhD (Department of Orthopaedic Surgery, Boston Children’s Hospital, Harvard Medical School, Boston, Massachusetts, USA).
Footnotes
Submitted June 9, 2022; accepted October 17, 2022.
One or more of the authors has declared the following potential conflict of interest or source of funding: This study was funded by the Translational Research Program at Boston Children’s Hospital, the Children’s Hospital Orthopaedic Surgery Foundation, the Children’s Hospital Sports Medicine Foundation, the National Institutes of Health (R01-AR065462, P30-GM122732), RIH Orthopaedic Foundation, the Lucy Lippitt Endowment of Brown University, and the Football Players Health Study at Harvard University. The Football Players Health Study is funded by a grant from the National Football League Players Association. The content is solely the responsibility of the authors and does not necessarily represent the official views of Harvard Medical School, Harvard University or its affiliated academic health care centers, the National Football League Players Association, or Boston Children’s Hospital. M.M.M. is a founder and equity holder in Miach Orthopaedics, which was formed to upscale production of the BEAR scaffold. A.M.K. is a paid consultant of Miach Orthopaedics. Y.-M.Y. is a paid consultant for Smith & Nephew and receives education support from Kairos Surgical and travel funds from Steris. D.E.K. is a paid consultant for Miach Orthopaedics and Johnson & Johnson and receives education support from Kairos Surgical. P.D.F. and M.J.H. have received travel support from Arthrex. B.D.O. has received royalties from Linvatec Corp and consulting fees from Linvatec, DePuy Synthes Products, Vericel, Medical Device Business Services, and Musculoskeletal Transplant Foundation. B.L.P. is an equity holder and consultant for Miach Orthopaedics. B.C.F. and B.D.O. are associate editors for the American Journal of Sports Medicine. B.C.F. is a founder of Miach Orthopaedics and the spouse of M.M.M., who has the conflicts listed above. Conflict-of-interest management plans are in place for all by their respective institutions. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.