
Abstract
Background:
Femoroacetabular impingement (FAI) in patients with dysplasia presents a unique challenge to surgeons. Short-term outcomes are conflicting, while longer term follow-up data are only emerging.
Purpose:
To quantify midterm (minimum 5-year follow-up) outcomes after the arthroscopic correction of FAI in the presence of lateral rim dysplasia compared with a matched control group with FAI with normal acetabular coverage.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
Prospective outcome data, collected in a consecutive series of patients undergoing arthroscopic FAI correction with lateral rim dysplasia (lateral center-edge angle [LCEA] of 13°-25°), were reviewed (N = 75 cases). An age- and sex-matched control group of 120 cases was also formed (LCEA >25°). Survivorship was defined as the avoidance of total hip replacement and assessed using a Kaplan-Meier curve with the log-rank test. Survival rates and patient-reported outcome measure (PROM) scores (modified Harris Hip Score [mHHS], University of California, Los Angeles [UCLA], 36-Item Short Form Health Survey [SF-36], and Western Ontario and McMaster Universities Osteoarthritis Index [WOMAC] preoperatively and at 5 years postoperatively) were compared between the groups. The proportion of patients across groups achieving the minimal clinically important difference (MCID) was compared for each PROM. The dysplasia group was also analyzed independently to identify any factors that may indicate a less favorable outcome using regression analysis. The group was divided into 2 subgroups: borderline dysplasia (LCEA of 20°-25°) and severe dysplasia (LCEA <20°).
Results:
The survival rate in the dysplasia group was 97%. There was no statistical difference with respect to survival rates or any PROM scores (P > .05 for all) between the groups. There were similar rates of achieving the MCID between the groups for the mHHS, UCLA, and WOMAC. The FAI control group had a higher rate of achieving the MCID for the SF-36 (P = .012; effect size = 0.274 [small]). Subgroup analysis indicated a lower survival rate (78% vs 100%, respectively; P < .001) in female cases in the dysplasia group (n = 9) compared with male cases in the dysplasia group (n = 66). The UCLA score in female cases in the dysplasia group at 5 years was statistically lower compared with that in male cases in the dysplasia group (6 vs 10, respectively; P = .003; effect size = 0.378 [medium]), but no other outcome revealed any differences between the sexes. There were also no variables identified on regression analysis that accurately predicted a poorer outcome in the dysplasia group. When stratified by severity, there was no difference in survivorship or outcomes between those with severe dysplasia (LCEA <20°; n = 11) and those with borderline dysplasia (LCEA of 20°-25°; n = 64).
Conclusion:
An arthroscopic intervention was a successful treatment option for FAI in the presence of lateral rim dysplasia at midterm follow-up. Irrespective of the severity of dysplasia, patients can expect similar improvements to those in patients with normal femoral head coverage.
Hip preservation surgery is an established treatment option for causes of nonarthritic hip pain including femoroacetabular impingement (FAI). Arthroscopic surgery removes impinging bony deformities, preserving and repairing soft tissue damage where possible, and results in improved outcomes in patients in the short and medium to longer term.5,15,27,28,33,35,36 The contraindications for hip preservation surgery are increasingly recognized, as are potential predictors of poorer outcomes, namely, evidence of osteoarthritis at the time of patient presentation.21,22,31 Despite the advancement in our understanding of FAI and contraindications for hip preservation, uncertainty remains as to the optimal treatment approach for patients with FAI and concomitant dysplasia. Hip dysplasia is characterized by malalignment and osseous insufficiency of the acetabulum, which can be diagnosed using anteroposterior (AP) radiography. 8 Numerous radiological parameters have been described to detect acetabular undercoverage. The lateral center-edge angle (LCEA) and acetabular index, also known as the Sharp angle, are recommended measures for young adults with hip pain. An LCEA of <25° on AP radiographs is most often used to confirm the presence of dysplasia and is frequently further subcategorized into severe (<20°) and borderline (20° to 25°). 6 Acetabular index values of >42° and >45° have been reported as indicative of dysplasia.25,40
Increased loading on the labrum because of insufficient acetabular coverage as a result of dysplasia has been demonstrated previously. 18 This is further compounded by the presence of pincer and cam deformities. Arthroscopic surgery alone is not sufficient to address undercoverage fully. Some relief from symptomatic FAI may be gained by removing abnormal cam and pincer morphology and repairing the unstable or torn labrum. 13 Some investigations have been conducted with short-term follow-up with conflicting results. Larson et al 23 quantified 2-year outcomes after hip arthroscopic surgery for FAI in patients with dysplasia, comparing them with a purely FAI group. The authors reported that although improvements were noted in patients of the dysplasia group, they had statistically poorer outcomes compared with the FAI group, with higher failure rates. Failure in this instance was defined as a modified Harris Hip Score (mHHS) of <70 and/or conversion to arthroplasty, although it was not possible to differentiate between them from the article. 22 Alternatively, Beck et al 2 did not observe any difference between outcomes in those with borderline dysplasia and those without, with a similar sex distribution.
In conjunction with conflicting results across studies, most of the existing literature has published a short-term follow-up. The aim of this study was to determine the midterm (minimum 5-year follow-up) outcomes of arthroscopic surgery for FAI in the presence of lateral rim dysplasia (dysplasia group) and compare them with those of a matched control group with FAI only (FAI control group). A secondary aim was to determine any characteristics that would predict failure in patients with lateral rim dysplasia, including the severity of dysplasia. We hypothesized that patients with lateral rim dysplasia, in the absence of other contraindications, would have comparable survival rates and experience similar improvements in patient-reported outcome measure (PROM) scores to those with normal coverage.
Methods
Study Design
Our prospective institutional hip arthroscopic registry was reviewed. All 1651 hip arthroscopic procedures undertaken between January 2009 and March 2016 were considered for the study. Indications for surgery were a radiographic diagnosis of FAI and clinical signs with appropriate patient history in keeping with FAI. 16 Patients were considered for surgery if they had undergone ≥3 months of nonoperative treatment without relief.
An a priori power analysis was conducted using G*Power software (Version 3.1). 11 The mHHS is one of the most commonly used outcome measures in hip arthroscopic literature and formed the basis of our sample size calculation. An alpha level of .05 and statistical power of 80% to detect a moderate effect were used to determine the sample size. We calculated that a sample of 26 dysplasia cases would be required with 52 matched FAI controls. Assuming a 20% loss to follow-up in both groups, our sample size was therefore adjusted to include a minimum of 31 dysplasia cases and 62 FAI control cases.
Inclusion criteria for the current study consisted of patients undergoing primary hip arthroscopic surgery for FAI with evidence of lateral rim dysplasia. Those diagnosed with an LCEA of ≤25° on AP radiographs were also included. Patients were excluded from the study population if they had evidence of osteoarthritis (Tönnis grade >1), avascular necrosis, underlying hip abnormalities including Perthes disease and slipped capital femoral epiphysis, or previous hip surgery. Those who underwent labral excision rather than preservation were also excluded. This study group was matched to an FAI control group without dysplasia using the same inclusion and exclusion criteria (Figure 1). The groups were further matched using a distribution method for age, Tönnis grade, and alpha angle on both Dunn and AP views. To avoid potential selection bias, a random number generator was used to match dysplasia cases to FAI-only cases.
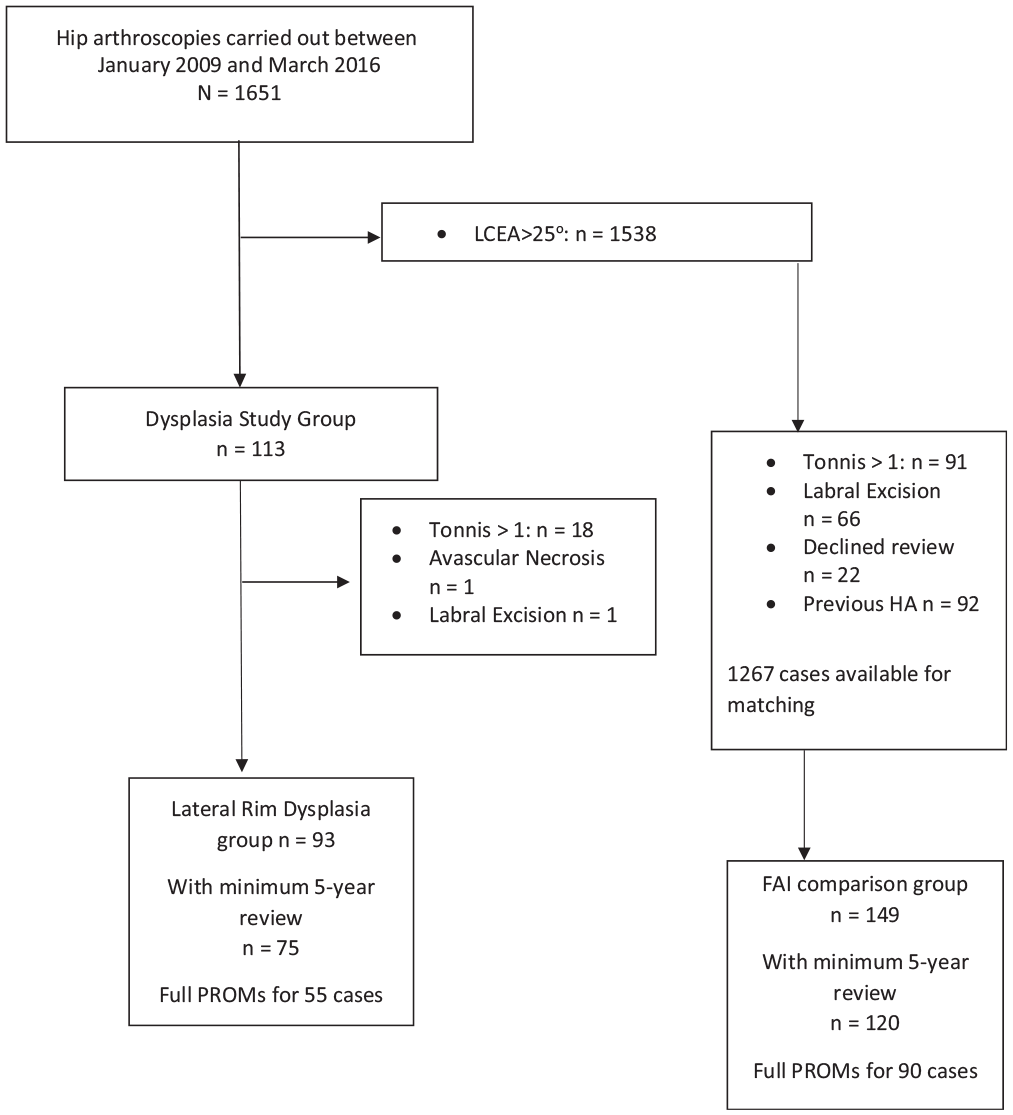
Patient recruitment. FAI, femoroacetabular impingement; HA, hip arthroscopy; LCEA, lateral center-edge angle; PROM, patient-reported outcome measure.
Surgical Procedure
All surgical procedures were carried out by the senior author (P.C.) and have been detailed previously. 4 After distraction, anterolateral and modified anterior portals were used to access the hip joint, and limited interportal capsulotomy was performed. An intraoperative inspection of acetabular cartilage was performed using the Outerbridge grade. The correction of pincer deformities was carried out initially. This was achieved by surgically reflecting the acetabular labrum from the rim and resecting the abnormal underlying bone using a 4.5-mm mechanical bur under radiographic guidance. In cases with dysplasia, care was exercised for any rim recession undertaken to ensure that bony stability was preserved. In the senior author’s experience, an anterior bony prominence is a classic feature observed in conjunction with a hypertrophic, degenerative, and detached labrum, originating secondary to anterior instability. Carefully removing this prominence while maintaining the natural acetabular rim and repairing and stabilizing the labrum are critical steps for surgical success in these cases. The labrum was refixed to the rim using 2 suture anchors. 4 Microfracture was not undertaken in any case. Cam deformities were resected using a 5.5-mm mechanical bur. Capsular repair was not undertaken at the beginning of this hip registry and only became routine in 2013, and thus, not all patients underwent capsular repair. Postoperative radiographic imaging was conducted on day 1 after surgery before discharge.
As part of a postoperative rehabilitation program, patients were encouraged to fully weight bear as tolerated with crutches for up to 5 days (after which crutches were no longer required), initiate stationary cycling bicycle on day 1, and commence hydrotherapy once incisions had healed. Extension and external rotation were restricted until week 4, but all other hip movements were permitted as tolerated. Low-intensity running was reintroduced at week 8, with sprinting at week 10 and return-to-sports training, if applicable, at week 12.
Assessments and Follow-up
Patients were contacted at a minimum of 5 years after surgery and invited for a clinical follow-up. In cases in which patients declined, copies of the PROMs were mailed to them. The primary outcome in this study was survivorship. Survivorship was defined as the avoidance of total hip replacement (THR); the rates of cases converting to THR and the time to THR were recorded. Reoperation rates were also reported. Secondary outcomes consisted of PROM scores, which were assessed preoperatively and at a minimum of 5 years postoperatively and were composed of the mHHS 38 ; University of California, Los Angeles (UCLA), activity scale39,42; 36-Item Short Form Health Survey (SF-36)17,24,37; and Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC). 26 The mHHS and SF-36 are calculated on a scale of 0 to 100, with 100 considered the maximal score. Conversely, the WOMAC is measured on a scale of 0 to 100, with 100 indicating the most dysfunction and worst score. The UCLA scale is calculated on a scale of 1 to 10, with 1 indicating wholly inactive and 10 representing habitual involvement in impact sports. The minimal clinically important difference (MCID) was calculated relative to each outcome measure.
Statistical Analysis
All statistical analyses were performed using SPSS software (Version 25; IBM). For each analysis an alpha level of 0.05 was applied.
Primary Study Aim
Kaplan-Meier survival analysis was performed with a test of equality of survival distributions between the dysplasia and FAI control groups using the log-rank (Mantel-Cox) test. Patients who underwent bilateral operative procedures were instructed to complete the PROM relative to each hip, and as such each hip was treated as an independent case. 30 Data were assessed for normality using the Shapiro-Wilk test, which indicated that the PROM scores were not normally distributed. The Wilcoxon signed rank test was therefore used to analyze the difference between baseline and postoperative PROM scores for both groups. Group comparisons between PROM scores at baseline and 5-year follow-up were conducted using the nonparametric Mann-Whitney U test. A distribution-based technique was used to determine the MCID (0.5 times the SD of the change in the score). 34
Secondary Study Aim
Regression analysis was conducted to determine if any characteristics were predictive of failure in the group with dysplasia. All potential variables likely to predict success or failure were included in a bivariate regression analysis, and any statistically significant variables were then included in a multivariate forward stepwise regression analysis. The variables included in the analysis were age, LCEA, alpha angle, range of motion, sex, and Tönnis grade. The Mann-Whitney U test was used to compare outcomes in subgroups within the dysplasia group. The Pearson correlation was also used to determine relationships between preoperative radiological parameters and 5-year PROM scores. In cases of statistically significant differences, the relevant effect size was calculated to determine magnitude. 12
Results
A total of 81 patients, amounting to 93 dysplasia cases, met the inclusion criteria for the current study (Table 1). Overall, 82 cases were male cases, and 11 were female cases, with a mean age of 31.1 years (range, 15.8-59.4 years). Additionally, 56 cases involved the right hip and 37 the left hip, with 74 hips rated as Tönnis grade 0 and 19 as Tönnis grade 1. A matched control group of 149 cases was included, with no significant differences between the groups for baseline characteristics apart from internal rotation and the expected differences in LCEA and Sharpe angle. The dysplasia group had higher internal rotation (Table 1) and Sharpe angles and lower LCEA angles compared to the control group. 81% of cases were followed up in both groups for the primary outcome (survivorship) of the study (75 dysplasia cases and 120 FAI control cases). For transparency, the number of responses for each outcome is stated in the tables. A comparison of baseline characteristics between those who were followed up and those who were not is presented in the Appendix (available in the online version of this article). Changes in radiographic parameters are presented in Table 2.
Patient Characteristics a
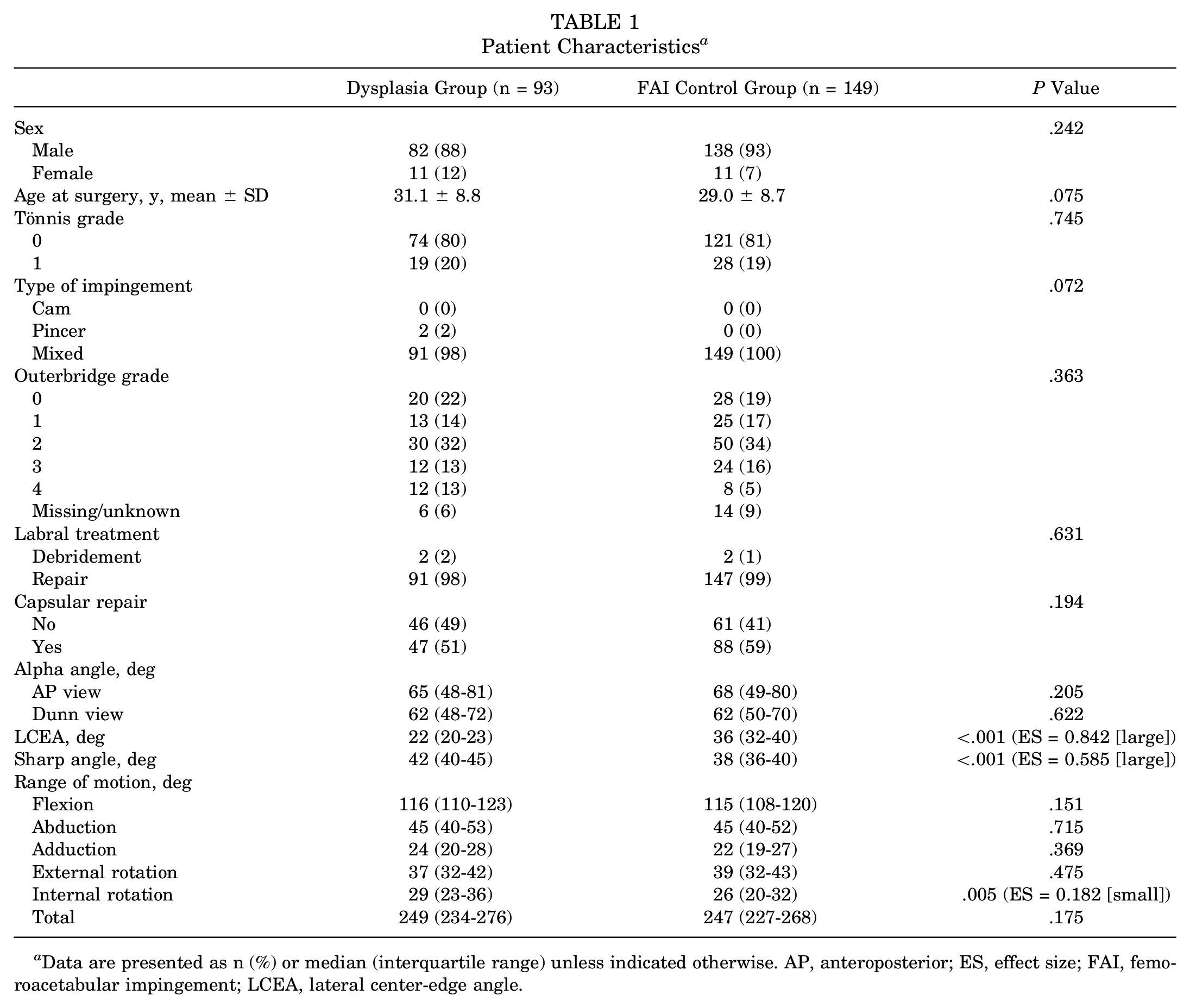
Data are presented as n (%) or median (interquartile range) unless indicated otherwise. AP, anteroposterior; ES, effect size; FAI, femoroacetabular impingement; LCEA, lateral center-edge angle.
Preoperative and Postoperative Radiographic Findings a
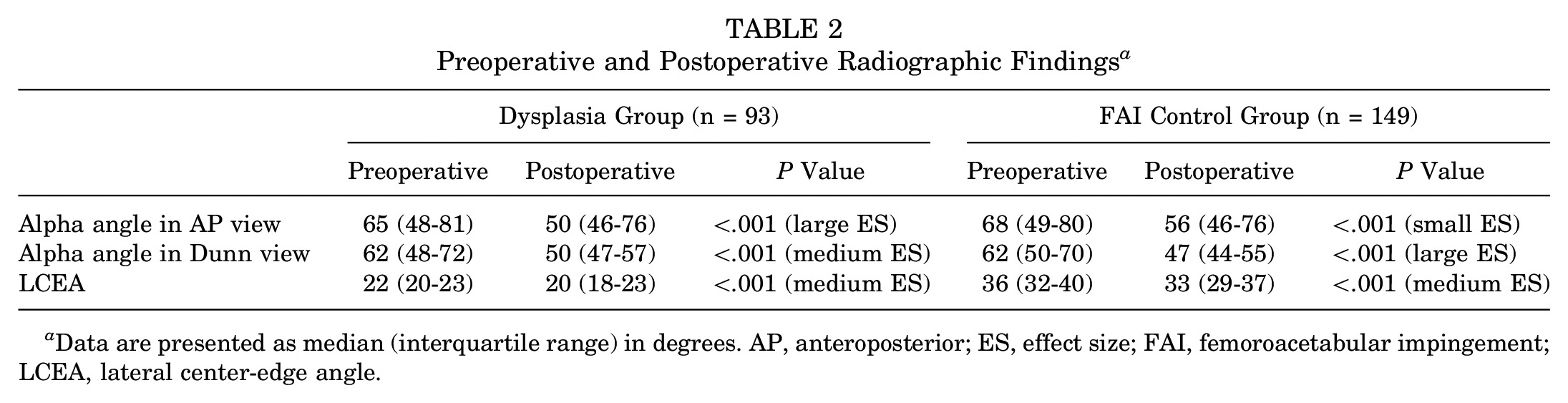
Data are presented as median (interquartile range) in degrees. AP, anteroposterior; ES, effect size; FAI, femoroacetabular impingement; LCEA, lateral center-edge angle.
Survivorship
The 5-year survival rate for the dysplasia group was 97% (Figure 2). Only 2 cases converted to THR (3%), which occurred at 2 and 7 months after arthroscopic surgery, both of which were female and rated as Outerbridge grade 4. There were 5 reoperations (7%) carried out at a mean of 16 ± 13 months. In comparison, in the FAI control group, there was no THR, with 16 reoperations (13%). The mean time to a reoperation in the FAI control group was 15 ± 13 months. There was no statistical difference in the proportion of reoperations between the groups (P = .076) or the time to reoperation (P > .05). The reasons for a reoperation in the dysplasia group were removal of adhesions (n = 3) and further labral repair (n = 1) and capsular repair (n = 1). In the FAI control group, there were 8 adhesion removals, 1 labral excision, 3 labral repairs, 1 capsular plication, and 3 cam and pincer resections. Capsular repair was not associated with survivorship in either group.
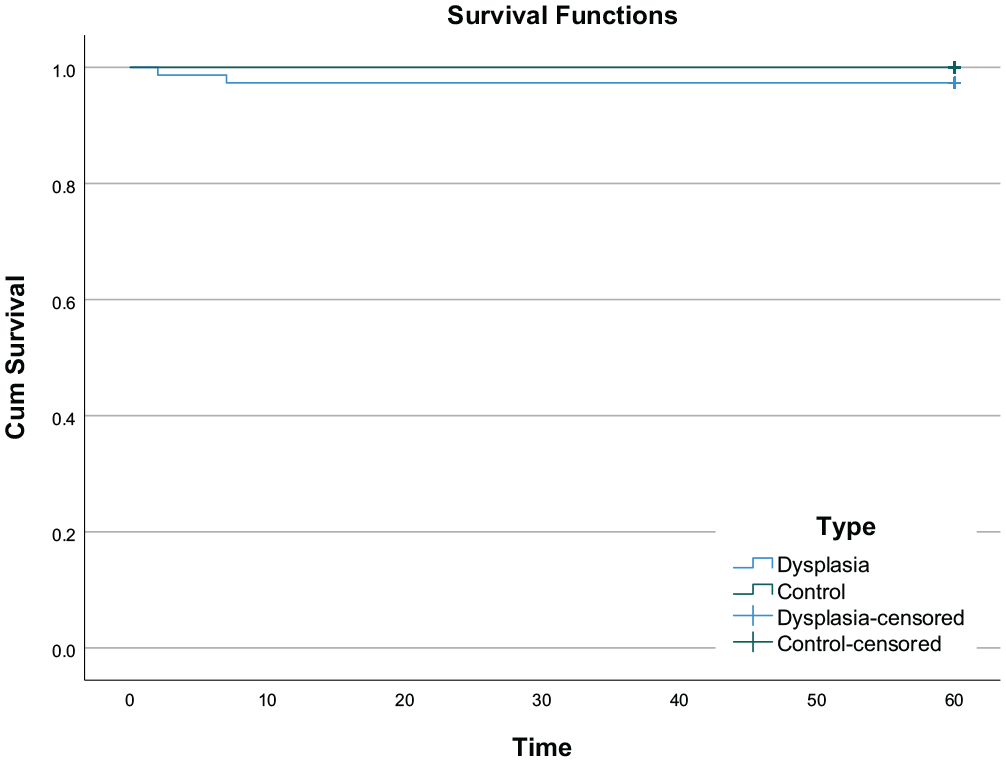
A Kaplan-Meier curve showing survival rates in the dysplasia (n = 75) and FAI control (n = 120) groups.
Patient-Reported Outcomes
Similar statistically significant improvements were noted in both the dysplasia and the FAI control groups for all PROMs (Table 3), with medium (>0.3) to large (>0.5) effect sizes for both groups on each measure. No significant difference in scores between the groups either preoperatively or at 5-year follow-up (P > .05 for all) was noted. There was no influence of capsular repair status on PROM scores.
Preoperative and Postoperative PROM Scores a
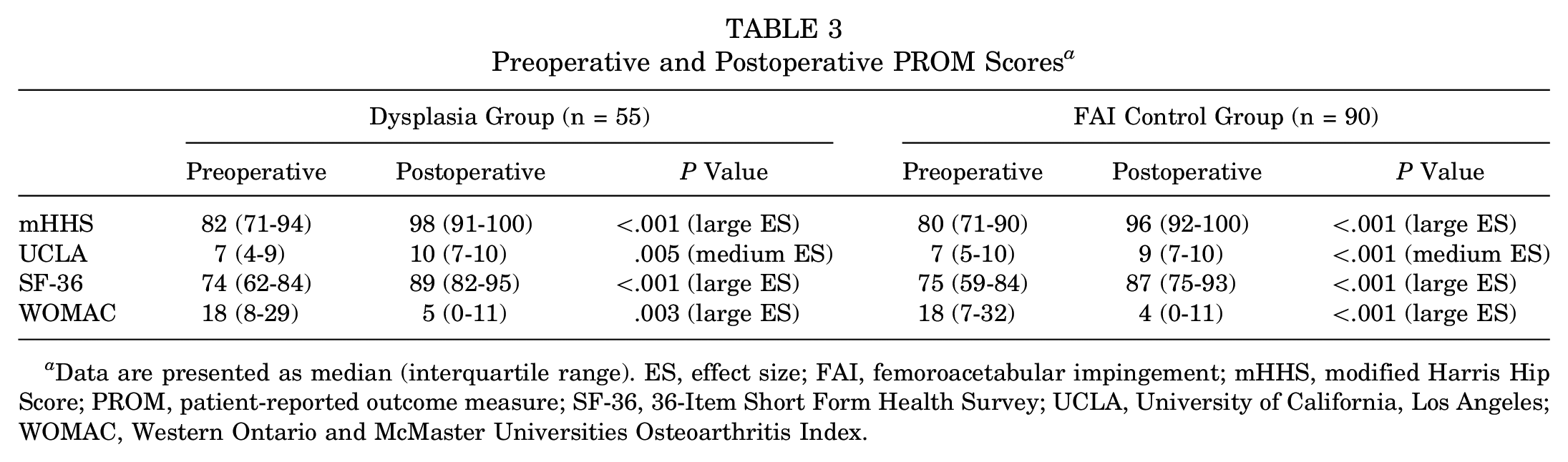
Data are presented as median (interquartile range). ES, effect size; FAI, femoroacetabular impingement; mHHS, modified Harris Hip Score; PROM, patient-reported outcome measure; SF-36, 36-Item Short Form Health Survey; UCLA, University of California, Los Angeles; WOMAC, Western Ontario and McMaster Universities Osteoarthritis Index.
Psychometric Analysis
The thresholds for achieving the MCID for the mHHS, UCLA, SF-36, and WOMAC were 8, 1, 8, and 9, respectively. The proportions of cases achieving the MCID are reported in Table 4. Apart from the SF-36 in which a greater proportion of the FAI control group achieved the MCID, there were no other differences in the proportions of cases achieving the MCID for the PROMs. Capsular repair was not associated with achieving the MCID.
Achievement of the MCID a
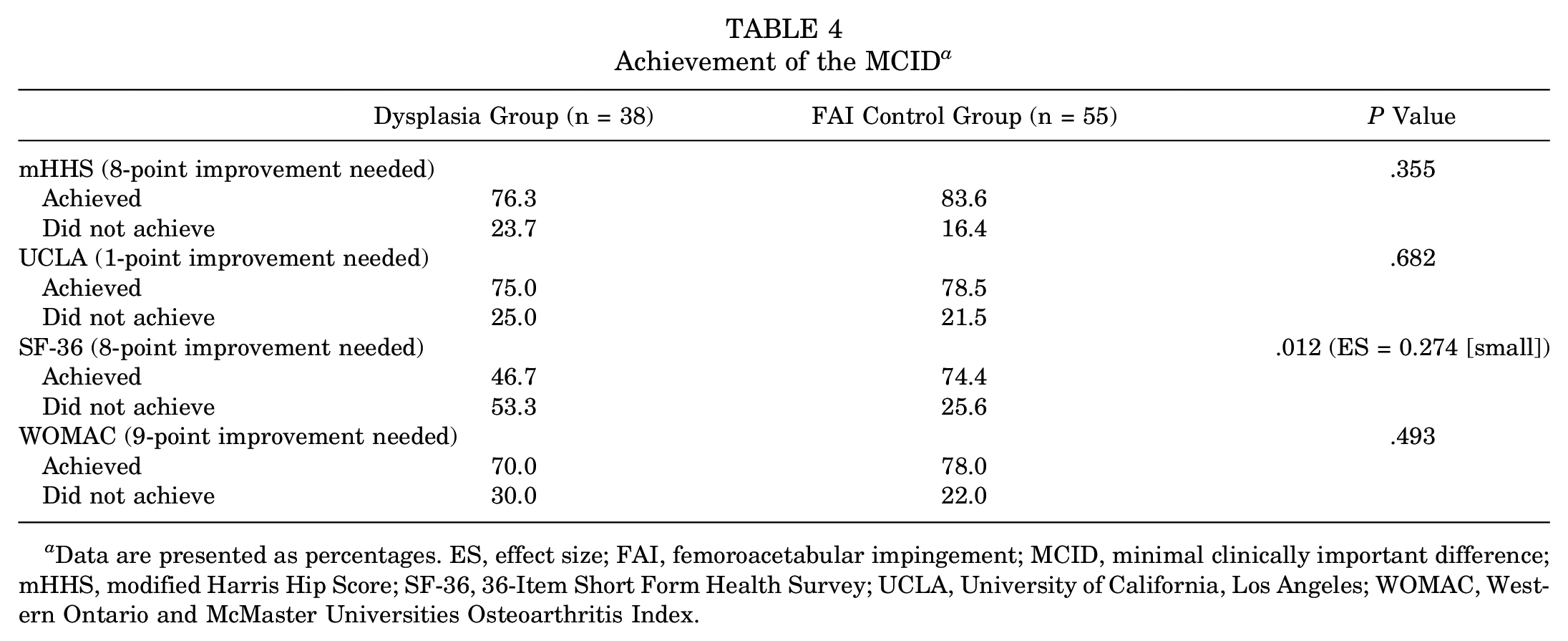
Data are presented as percentages. ES, effect size; FAI, femoroacetabular impingement; MCID, minimal clinically important difference; mHHS, modified Harris Hip Score; SF-36, 36-Item Short Form Health Survey; UCLA, University of California, Los Angeles; WOMAC, Western Ontario and McMaster Universities Osteoarthritis Index.
Dysplasia Subgroup Analysis
No baseline characteristic was predictive of failure in the dysplasia group (P > .05 for all variables) on regression analysis. Tönnis grade, surgical approach to the labrum, type of impingement, and capsular repair were not associated with failure. In contrast, as the THR cases were both female cases (Figure 3) and both were Outerbridge grade 4, the survival rate for female cases was statistically significantly lower than that of male cases (78% vs 100%, respectively; P < .001), and an Outerbridge grade 4 had a lower survival rate compared with all other grades (80% vs 100%, respectively; P = .018).
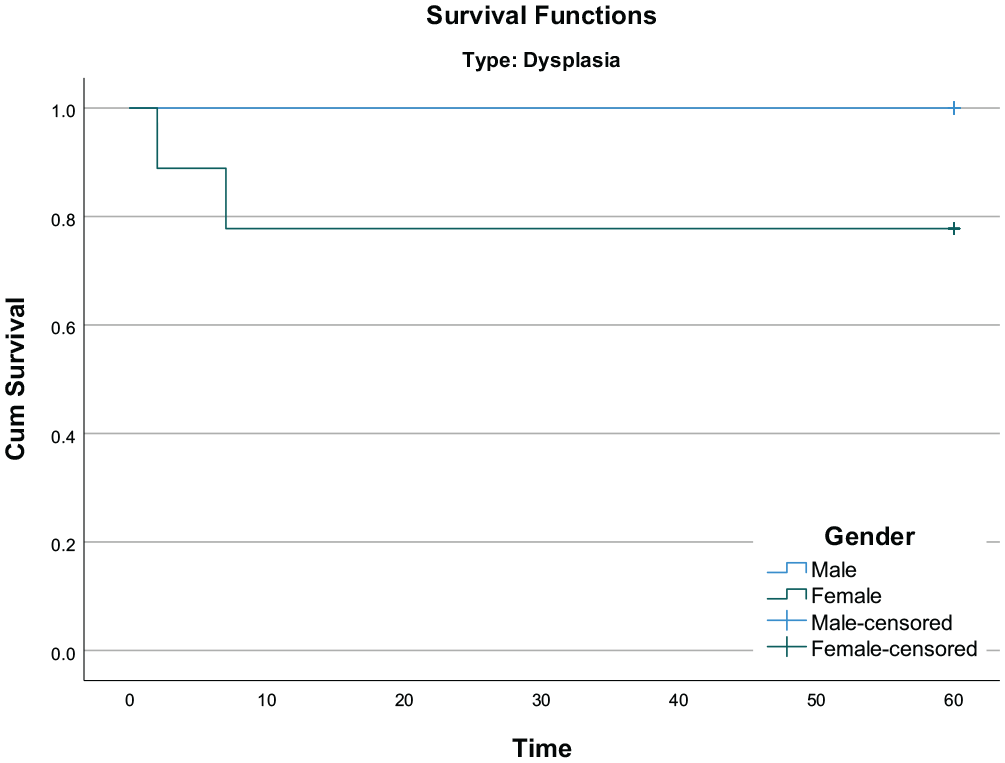
A Kaplan-Meier curve showing survival rates in male (n = 66) and female (n = 9) dysplasia cases.
Male dysplasia cases had significantly higher preoperative mHHS (83 vs 73, respectively; P = .034; effect size = 0.221 [small]), UCLA (7 vs 4, respectively; P = .027; effect size = 0.230 [small]), and WOMAC (16 vs 34, respectively; P = .004; effect size = 0.301 [medium]) scores than female dysplasia cases. At 5-year follow-up, the only difference between sexes was for the UCLA scale (10 vs 6, respectively; P = .003; effect size = 0.378 [medium]). There were no differences in PROM scores between Tönnis grades, types of impingement, Outerbridge grades, and whether the capsule was repaired (yes/no) (P > .05 for all). Age at the time of surgery was not correlated with 5-year scores for the mHHS, SF-36, or WOMAC; however, a statistically significant negative correlation was identified between age at surgery and 5-year UCLA scores (P = .004; r = −0.382). There were no significant correlations between preoperative radiological parameters and 5-year PROM scores.
When stratified by severity, 85% (n = 64) of the dysplasia group had an LCEA between 20° and 25°, and 15% (n = 11) had an LCEA <20°. There were no significant differences in survival rates (98.4% in borderline and 92.3% in severe), PROM scores (either before or at 5 years), or achievement of the MCID for each PROM (P > .05 for all).
Discussion
The results of this study indicate that patients with lateral rim dysplasia, irrespective of severity, can expect similar improvements in outcomes to the control (nondysplasia) group at 5 years after surgery. Similar survival rates and similar MCID achievement rates were noted, apart from the SF-36 for which a higher proportion of the FAI control group achieved the MCID.
The results of the current study support research that has been previously published, albeit with a shorter term follow-up. Jayasekera et al 19 reported improved mHHS scores at 1 year in a group of patients with severe dysplasia (LCEA <20°). The improvements were similar to those in their FAI control group, and there were no differences in mHHS scores between the dysplasia group and control group at 1 year. The current study included both borderline and severe cases of dysplasia. Overall, dysplasia cases improved to the same extent as the control group, and no difference in outcomes between borderline and severe dysplasia cases was observed. Nawabi et al 32 compared a group with dysplasia (LCEA of 18°-25°) with a nondysplastic FAI control group at 6 months, 1 year, and 2 years after arthroscopic surgery for FAI. At no time point were any differences in outcomes noted between the groups. 32 Similar results were also reported by Beck and colleagues, 2 who observed no difference in clinical outcomes between groups. Larson et al, 23 however, reported poorer outcomes and higher failure rates in the dysplasia group in comparison with the FAI control group. It must be noted that there were a number of other procedures apart from labral repair and bony resection conducted in that study, which included microfracture (16%), partial psoas tenotomy of the central compartment (11%), subspine decompression (24%), and partial ligamentum teres debridement (30%). In contrast, these additional procedures were not reported for their FAI control group. In the current study, a similar surgical approach was employed for both groups, with no additional procedures undertaken.
The surgical management of the capsule in patients with dysplasia is an important consideration; disruption of the capsule or excessive rim recession has the potential to exacerbate joint instability. 41 There was a similar distribution across the groups between those who did and those who did not undergo capsular repair in the current study, making comparisons between the groups more accurate. Domb and colleagues9,10 reported on the 2- and 5-year outcomes of patients in a purely borderline dysplasia group, all of whom were treated with capsular plication after bony resection and labral repair. The studies indicated significant improvements in PROM scores at both time points, with no THR reported. At 2 years, there was a 9% revision rate, which increased to 19% by 5-year follow-up. The current study reports a 7% revision rate at 5 years. In both studies by Domb et al,9,10 no control group was included; thus, it was not possible to compare survival rates with those of an FAI control group or patients with dysplasia who did not undergo plication. In the current study, capsular repair only became routine in our clinic in 2013, therefore permitting a subgroup analysis. The absence of capsular repair did not negatively affect outcomes; there were no differences in outcomes or survivorship between those who underwent capsular repair and those who did not.
In a recent study examining 10-year outcomes in patients with borderline dysplasia, with survivorship defined as the avoidance of THR, Beals et al 1 reported a 5-year survival rate of 87% and 10-year survival rate of 79%. In the current study, a survival rate of 97% was observed at 5 years. Beals et al highlighted older age, increased Tönnis grade, microfracture, and Tönnis angle >15° as predictive of conversion to THR. In our more homogeneous cohort, no one indicator was revealed as predictive of failure. However, both THR cases in the current study were Outerbridge grade 4, leading to statistically lower survival rates. Cartilage defects are common in FAI cases, both with and without concomitant dysplasia, and increase the risk of THR.3,14 It is likely that the low failure rate in the current study did not allow for a regression model that was sufficiently powered to identify Outerbridge grades as predictive of THR.
Fukui et al 13 examined survival and changes in PROM scores among patients with dysplasia, without the use of a control group, with a mean follow-up of 42 months. The authors reported a 25% failure rate, with 18% converting to THR and 7% needing periacetabular osteotomy. In contrast to the current study in which both THR cases were female cases, Fukui et al highlighted male sex as a risk factor for subsequent surgery. It should be noted that 29% of that patient group underwent labral reconstruction with an iliotibial band autograft. In the current study, only minimal labral debridement and labral repair were performed. Fukui et al did not report on the differences in PROM scores between the sexes, and thus, it is unclear whether male patients in that study also scored lower compared with female patients on these measures. The current study observed lower PROM scores at baseline in the female cases that were not evident at 5 years, apart from lower activity levels. With a shorter follow-up time, Cvetanovich et al 7 reported greater improvements in female patients with dysplasia compared with male patients on the Hip Outcome Score–Activities of Daily Living and mHHS but no difference between the sexes on the Hip Outcome Score–Sports at 2 years. The longer follow-up period in the current study may account for this. Previous research has reported similar UCLA scores between the sexes at 2 years after surgery in patients without dysplasia, but at 10 years after surgery, UCLA scores were significantly lower in female patients compared with male patients.5,29 Lower participation in sports and physical activity by female patients over time may not, therefore, be caused by any adverse outcomes from arthroscopic surgery in the presence of dysplasia.
The ability to measure aspects of recovery that are clinically relevant to patients is important. 20 In this study, rates of achieving the MCID between the dysplasia and FAI control groups were compared for each PROM. We did not observe any difference in achievement for 3 of the 4 PROMs used. There was, however, a higher percentage of FAI control cases that achieved the MCID for the SF-36, although this difference was small. Neither Beck et al 2 nor Cvetanovich et al 7 observed differences in achieving the MCID between the dysplasia and FAI control groups at 2-year follow-up. Longer term data for the MCID in dysplasia cohorts are lacking. While Beals and colleagues 1 reported MCID rates in patients with dysplasia, they did not include a control group, and thus, it was not possible to determine whether MCID achievement rates differ between dysplasia and FAI control groups with a longer follow-up. There was no difference observed in MCID achievement rates between borderline and severe dysplasia cases in this study, indicating similar clinically relevant improvements after corrective FAI surgery.
Strengths and Limitations
The strengths of the study include the use of an age- and sex-matched control group for comparison, which provides a context for the improvements observed. The large difference in the LCEA between the groups reduced the likelihood of unintentional crossover. However, there are limitations to this research that must be considered. The use of the LCEA as the sole measure of dysplasia is a limitation. The LCEA examines only 1 aspect of a dysplastic hip, and other features such as anterior dysplasia, laxity, and acetabular and femoral version, among others, have not been assessed. As such, we have used the term “lateral rim dysplasia” to accurately reflect this. The LCEA is, however, a well-recognized and documented indicator of dysplasia in the literature and allows for comparison with previous research. This is a retrospective analysis, which may introduce selection bias, although the data were prospectively collected, reducing the risk of recall bias. All patients were operated on by 1 high-volume surgeon, which adds consistency to the surgical procedures across all patients, although it may reduce the external validity of the results. The 2-dimensional nature of the radiological assessment in this study is a limitation. Computed tomography would provide more detailed information regarding the presence and severity of dysplasia but is not widely used, owing to its increased time, cost, and radiation exposure. There was also no radiological follow-up for patients at 5 years, which would allow more objective analysis of the natural history of dysplasia after arthroscopic surgery for FAI. There was a much lower incidence of severe dysplasia compared with borderline dysplasia, and therefore, the risk of type II errors is increased. This also applies to the rate of conversion to THR. Although a low failure rate was a positive outcome of the intervention, the study power to determine factors associated with conversion to THR was reduced.
Conclusion
An arthroscopic intervention was a successful treatment option for FAI in the presence of lateral rim dysplasia at midterm follow-up. Irrespective of the severity of dysplasia, patients can expect similar improvements to those in patients with normal femoral head coverage.
Supplemental Material
sj-pdf-1-ajs-10.1177_03635465221145018 – Supplemental material for High Survivorship and Comparable Patient-Reported Outcomes at a Minimum 5 Years After Hip Arthroscopic Surgery in Patients With Femoroacetabular Impingement, With and Without Lateral Rim Dysplasia
Supplemental material, sj-pdf-1-ajs-10.1177_03635465221145018 for High Survivorship and Comparable Patient-Reported Outcomes at a Minimum 5 Years After Hip Arthroscopic Surgery in Patients With Femoroacetabular Impingement, With and Without Lateral Rim Dysplasia by Karen Mullins, David Filan and Patrick Carton in The American Journal of Sports Medicine
Footnotes
Submitted May 11, 2022; accepted November 10, 2022.
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.