
Abstract
Background:
There are limited studies designed by matching related factors to compare clinical outcomes and return to sport (RTS) between patients undergoing revision anterior cruciate ligament reconstruction (R-ACLR) and primary ACLR (P-ACLR).
Purpose:
(1) To compare the outcomes between R-ACLR and P-ACLR in a matched-pair analysis with 3- to 5-year follow-up and (2) to evaluate patient-reported factors for not returning to preinjury-level sport.
Study Design:
Cohort study; Level of evidence, 4.
Methods:
Patients who underwent R-ACLR between September 2016 and November 2018 were propensity matched by age, sex, body mass index, passive anterior tibial subluxation, and generalized hypermobility in a 1:1 ratio to patients who underwent P-ACLR during the same period. By combining in person follow-up at 2 years postoperatively and telemedicine interview at the final follow-up (January 2022), knee stability and clinical scores were compared, including International Knee Documentation Committee (IKDC), Lysholm, and Tegner. Status of RTS was requested, specifically whether the patient returned to preinjury level of sport. Patient-reported reasons for not returning were analyzed.
Results:
There were 63 matched pairs in the present study. Knee stability was similar in terms of KT-2000 arthrometer, Lachman test, and pivot-shift test results between the groups at 2 years of follow-up. At the final follow-up, no significant difference was found between groups for postoperative clinical scores (IKDC, Tegner, and Lysholm) (P > .05). There was a significant difference in total RTS: 53 (84.1%) in the P-ACLR cohort and 41 (65.1%) in the R-ACLR cohort (P = .014). No significant difference was shown in terms of RTS at the same level: 35 (55.6%) in P-ACLR and 31 (49.2%) in R-ACLR (P = .476). Significantly more patients showed fear of reinjury: 26 of 32 (81.3%) in the R-ACLR group as compared with 15 of 28 (53.5%) in the P-ACLR group (P < .021).
Conclusion:
R-ACLR resulted in similar clinical scores (IKDC, Tegner, and Lysholm) but significantly lower RTS versus P-ACLR at 3 to 5 years of follow-up. Fear of reinjury was the most common factor that caused sport changes in patients with R-ACLR.
There has been a considerable increase in the number of anterior cruciate ligament (ACL) primary reconstruction (P-ACLR) procedures performed every year globally. 35 Thus, the revision burden has also gone up, and contemporary rates of revision ACLR (R-ACLR) range between 4.1% and 13.3% of all P-ACLRs.35,38,47
Worse clinical results and lower rates of return to sport (RTS) have been reported for R-ACLR as compared with P-ACLR.1,2,12,26,30,50 However, most of these studies lacked homogeneity by including different patient populations, amounts of tunnel widening, graft types (autograft and allograft), and many predictors that might be nonmodifiable by the patient or surgeon. § Patient-reported outcomes (PROs) and rerupture rates were noted to improve with higher activity level at 2- and 6-year follow-up when an autograft was chosen for R-ACLR versus an allograft. 29 It has also been reported that passive anterior tibial subluxation (PATS) was greater in knees with failed ACLR versus P-ACLR.32,53 Inferiorclinical scores and knee stability were found in patients with excessive PATS after anatomic ACLR. 42 There was additionally a greater risk of ACL graft failure and worse subjective outcomes in patients with increased Beighton score and generalized hypermobility.20,21,53 To study the cohort of patients with matched related factors would more accurately determine the outcomes after R-ACLR in comparison with P-ACLR.
There is paucity of literature about the patient-reported reasons for not returning to preinjury levels of sport after R-ACLR. The patient-reported factors that influenced RTS were noted mainly in P-ACLR and a small number of revision cases. 14 In addition to persistent knee symptoms, psychological and social factors might play a role in the RTS.
The purpose of this study was (1) to compare the outcomes between R-ACLR and P-ACLR in a matched-pair analysis with 3- to 5-year follow-up and (2) to evaluate patient-reported factors for not returning to preinjury levels of sport. The hypothesis was that clinical outcomes would not be different between R-ACLR and P-ACLR at 3- to 5-year follow-up and that the decisions to RTS would be affected by multiple psychological and social factors after R-ACLR.
Methods
Study Design and Participants
Institutional ethics committee approval was granted for this study. Patients who underwent R-ACLR by the senior surgeon (J.K.Y.) between September 2016 and November 2018 were considered for study eligibility. All patients who underwent R-ACLR had graft ruptures confirmed by magnetic resonance imaging (MRI). Patient characteristics and clinical outcomes were prospectively collected by the surgical team in our institute for patients who underwent ACLR. Exclusion criteria included open physes, age >45 years, concomitant multiligament reconstruction, R-ACLR with a double-bundle procedure, and any additional procedure for a cartilage lesion (microfracture or osteochondral autograft transplantation).
Patients undergoing R-ACLR were matched to patients undergoing P-ACLR during the same period in a 1:1 allocation using propensity score matching by age, sex, body mass index, PATS in the lateral compartment, and generalized hypermobility. Measurements of generalized hypermobility were based on a modification of the criteria established by Beighton and Horan 4 and Carter and Wilkinson. 7 The measurements of ligamentous laxity included fifth metacarpophalangeal joint hyperextension angle, thumb-radius apposition, elbow recurvatum, and knee recurvatum.
MRI Measurement of PATS
A standard institutional MRI examination with a 1.5-T superconducting magnet (Optima MR360; GE) was performed. Electronic measurements were performed by observers to determine anterior subluxation in the lateral tibial compartment relative to a posterior femoral condylar reference line on sagittal MRI scans, as first described and validated by Iwaki et al 18 and later utilized by Tanaka et al. 44 This technique was also used by Song et al 42 and Lin et al. 25 The amount of PATS was measured on the MRI scans within 2 months preoperatively.
Three-Dimensional Computed Tomography Evaluation
All patients underwent 3-dimensional computed tomography (3D-CT) within 2 months before revision surgery in our hospital. The tunnel positions were evaluated using a digital radiography system (Siemens) with a built-in digital rule. CT images provided greater precision and reliability than plain radiographs in terms of position and geometry of the tibial and femoral tunnels, which was crucial for preoperative planning.10,49,52 The femoral and tibial tunnel positions were evaluated in terms of the quadrant method on the 3D-CT reconstruction image described in previous studies.6,9,22,46 Measurements of width were obtained at the widest point of each tunnel by drawing a line perpendicular to its longitudinal axis.
Surgical Technique
For P-ACLR in the control group, hamstring tendon (HT) autografts were used in all patients in the present study. For R-ACLR in the study group, all patients initially had ACLR with HT autografts. The decision to use a particular graft type for R-ACLR (HT or bone–patellar tendon–bone [BPTB] autograft) was based on patient factors and choice, and all R-ACLRs were performed in a single-stage procedure in the present study.
The position of previous tibial and femoral tunnels was evaluated by 3D-CT. (1) If the tunnels were anatomically placed and could be reused and once potential tunnel interference was addressed and the tunnel was adequately debrided, the tunnel could be serially re-reamed to healthy metaphyseal bone with punctate bleeding. (2) If the tunnels were completely nonanatomic, new tunnels could be drilled without any risk of convergence. (3) If drilling new anatomically placed tunnels would result in convergence with previous semianatomic tunnels, such convergence was managed by drilling the new tunnels from a different angle to achieve a completely different tunnel trajectory, thereby allowing stable graft fixation. Using a completely different tunnel trajectory also obviated most issues with tunnel widening. Previous hardware was removed only if required to complete the revision procedure or if it was symptomatic.
R-ACLR Using BPTB Graft
The BPTB graft was 9 to 11 mm in diameter based on individualized evaluation and was harvested with a patellar bone plug (20 mm in length) and tibial bone plug (25-mm plug). The femoral tunnels were drilled by using the inside-out technique through the accessory anteromedial portal. On the tibial side, a tibial guide (Smith & Nephew) was used to drill the bone tunnel. Emphasis was placed on secure tibial fixation, which was achieved by a combination of interference screw fixation and secondary fixation by passing the traction sutures from the bone block to the tibial harvest site and tying them over a bony bridge.
P-ACLR and R-ACLR Using HT Graft
The semitendinosus and gracilis tendons were prepared in 3 or 4 strands, with a total diameter of 8 to 12 mm. Anatomic reconstruction was performed for P-ACLR. For R-ACLR, similar techniques were used to drill the femoral and tibial tunnels by following the methods mentioned earlier, for, HT autografts were harvested from the opposite leg. Each graft was fixed with an EndoButton (Smith & Nephew) on the femoral site and with 1 bioabsorbable interference screw on the tibial site. A staple was used as secondary fixation by tying the sutures of HT grafts in addition to interference screw fixation.
Postoperative Rehabilitation Protocol
The postoperative regimen did not vary by revision technique and was similar to the regimen after primary reconstruction. A standardized rehabilitation procedure was used for all patients. Quadriceps sets, straight-leg raises, and prone hangs were started on postoperative day 1 for HT ACLR and straight raises on week 2 for BPTB ACLR. Patients were permitted to walk with crutches and braces but without bearing weight. Range of motion exercises were begun on postoperative day 3. Closed kinetic chain exercises and full weightbearing were started in the sixth week. Patients progressed to running without a brace at 4 to 6 months. Sports activities were allowed approximately 6 months after surgery. Patients were allowed to return to preinjury levels of sport at 9 to 12 months after surgery.
Follow-up and Data Collection
In person postoperative follow-up was undertaken by the surgical team at 3 and 6 weeks and 3, 6, 12, and 24 months. Because of the geographically mobile nature of young populations (particularly for mid- to long-term follow-up) and the effects of the COVID-19 pandemic, the final follow-up was performed using a standardized telemedicine interview (January 2022). Lysholm, Tegner, and International Knee Documentation Committee (IKDC) scores were collected from all patients. Patients were queried about reinjury and reoperation and their responses were recorded.
Status of RTS was also requested, specifically whether the patient returned to his or her preinjury level of sport or, if not, whether the knee was the main cause of sport modification. An open-ended question was asked about the factors that stopped patients from RTS or influenced the level of sport. The factors were categorized as knee, choice, and life event related.14,19 A relative weightage was not assigned, but the first reason cited by the patient was considered the most important factor.
As a result of follow-up management, physical examination findings (range of motion and knee stability) are reported at 2 years of follow-up. The physical examinations were performed by an author (H.W.) with >15 years of sports medicine practice who was blinded to group assignment. Complications and PROs are reported for the final follow-up.
Statistical Analysis
Statistical analysis was conducted using SPSS 24.0 (IBM). For numerical data, the Student t test for paired data was used when the normality of the distribution was confirmed using the Shapiro-Wilk test, and the Wilcoxon rank-sum test was used elsewhere. For categorical data (2 levels), the McNemar test was used when the sum of discordances between pairs was >10, and the binomial test was used elsewhere. For categorical data (>2 levels), the larger class was compared with the sum of the others using the McNemar test or the binomial test as previously specified. P < .05 was regarded as statistically significant.
Results
Patients and Clinical Characteristics
There were 81 R-ACLRs identified during the study period between September 2016 and November 2018; 4 patents were lost to follow-up. By applying the exclusion criteria, 63 patients were recruited as the study group. These were propensity matched to 63 patients who underwent P-ACLR (control group). No patients were lost to follow-up in the control group. As a result, the final population consisted of 126 matched pairs (126 patients) (Figure 1).
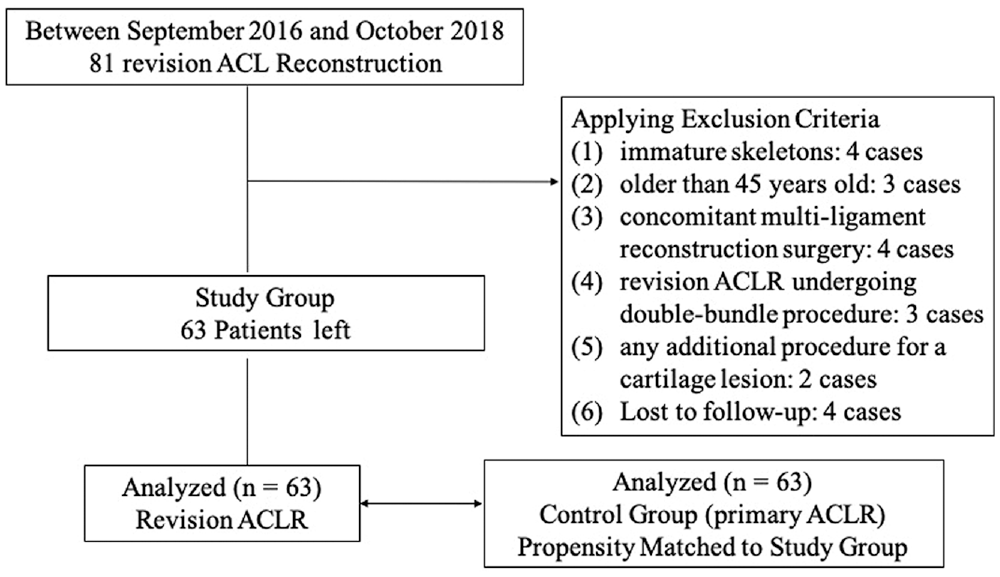
Flowchart. ACL, anterior cruciate ligament; ACLR, ACL reconstruction.
Table 1 lists baseline descriptive statistics related to surgery of the study population at the time of R-ACLR. Table 2 summarizes patient and clinical characteristics in the study and control groups. There was no difference in age, sex, body mass index, PATS, Beighton score, and follow-up duration between the groups. There were significantly more severe injuries in terms of medial meniscal and patellar cartilage in the R-ACLR group at P = .003 and .040, respectively.
Baseline Descriptive Statistics Related to Surgery at the Time of the Revision ACLR (n = 63) a
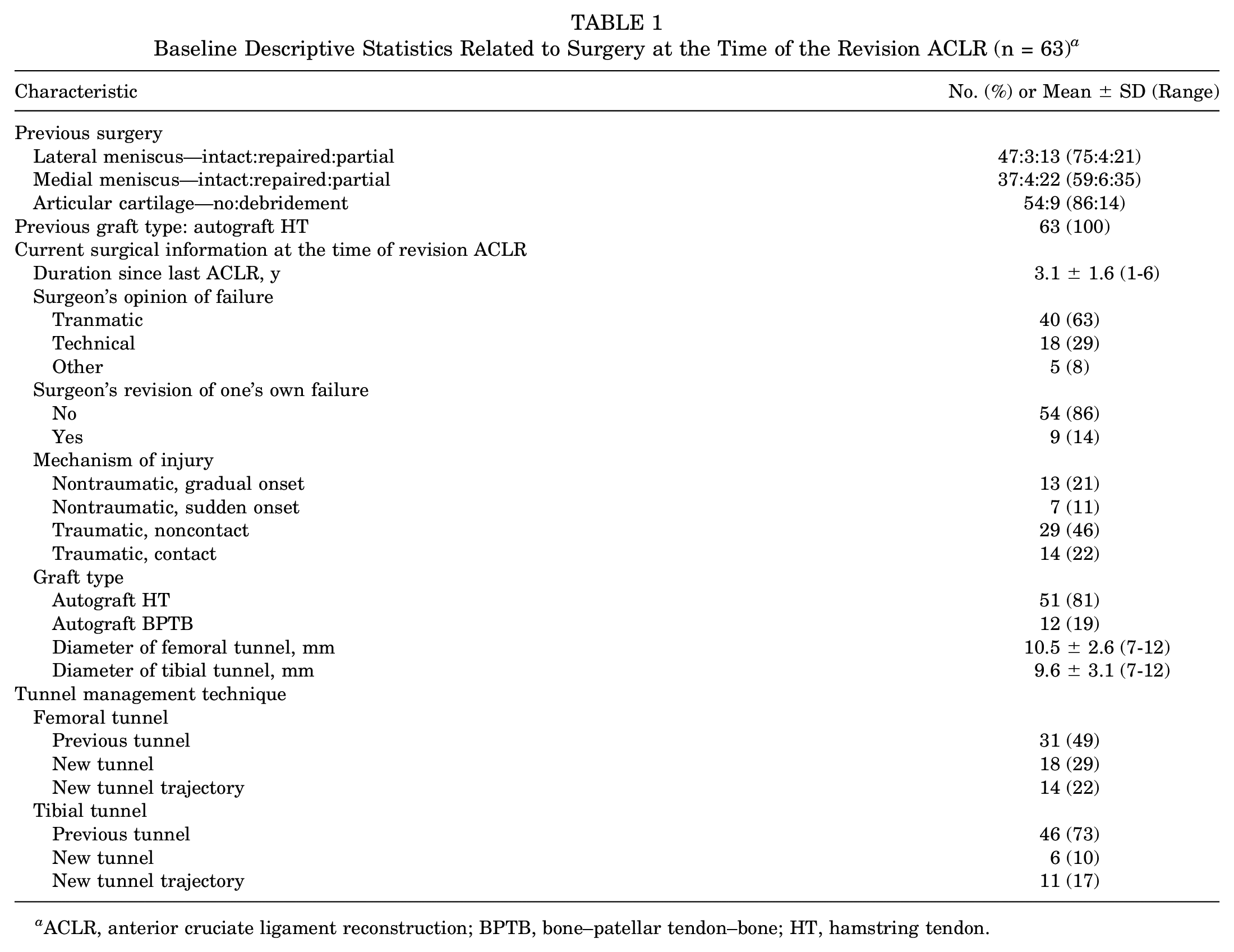
ACLR, anterior cruciate ligament reconstruction; BPTB, bone–patellar tendon–bone; HT, hamstring tendon.
Patient and Clinical Characteristics and Intraoperation Comparisons Between the Groups a
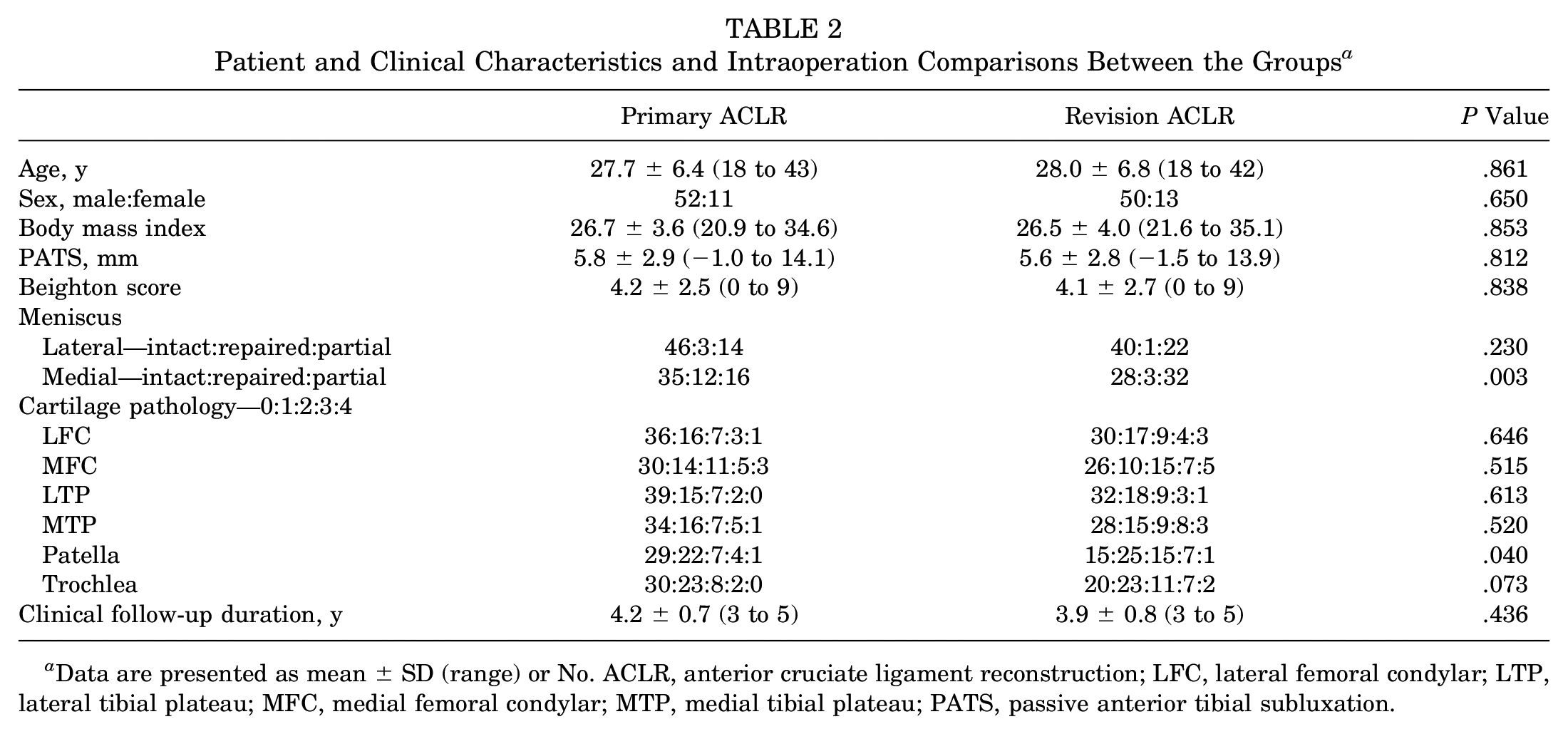
Data are presented as mean ± SD (range) or No. ACLR, anterior cruciate ligament reconstruction; LFC, lateral femoral condylar; LTP, lateral tibial plateau; MFC, medial femoral condylar; MTP, medial tibial plateau; PATS, passive anterior tibial subluxation.
PROs and Clinical Outcomes
The differences in preoperative knee stability (Lachman test, pivot-shift test, and KT-2000) and clinical scores (IKDC, Tegner activity, and Lysholm) (Table 3) were not significant between the groups. At 2-year follow-up, knee stability significantly improved in terms of KT-2000 arthrometer, Lachman test, and pivot-shift test results as compared with baseline in both groups, and no significant difference was found between the groups postoperatively (Tables 3 and 4). At final follow-up, no significant difference was noted between groups for clinical scores (IKDC, Tegner, and Lysholm) (P > .05) (Table 5). The IKDC, Tegner, and Lysholm scores all significantly improved at the final time point versus baseline in both groups.
Preoperative Stability Evaluations and Scores for the Primary and Revision ACLR Groups a
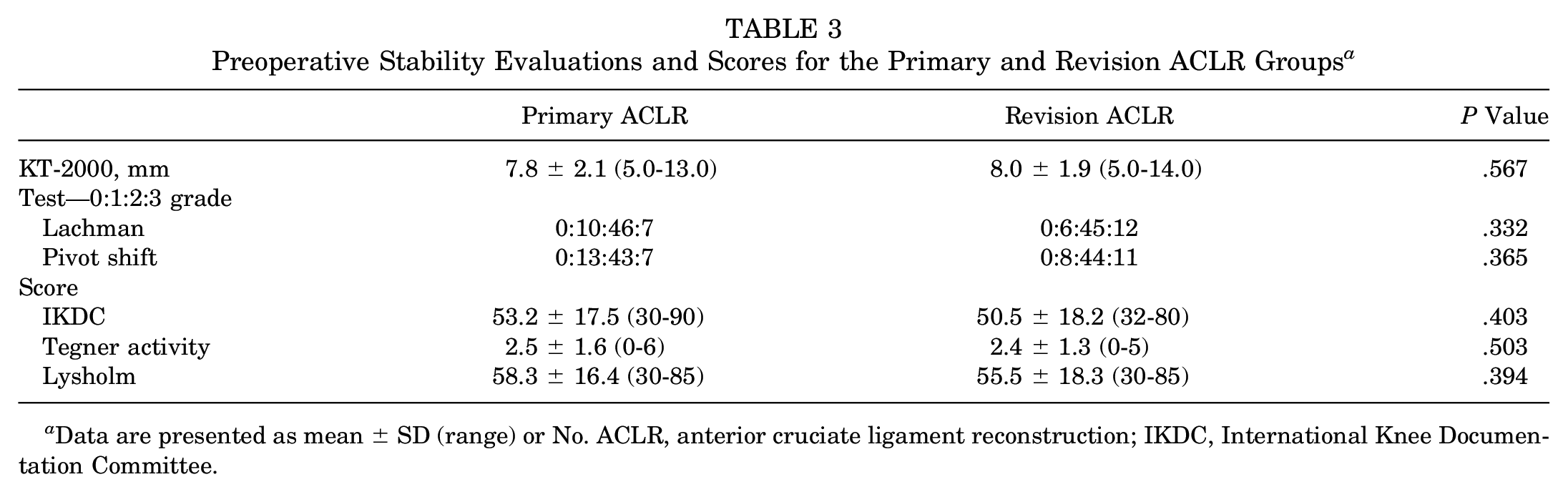
Data are presented as mean ± SD (range) or No. ACLR, anterior cruciate ligament reconstruction; IKDC, International Knee Documentation Committee.
Knee Stability in Terms of KT-2000, Lachman Test, and Pivot-Shift Test at 2-Year Follow-up Between the ACLR Groups a
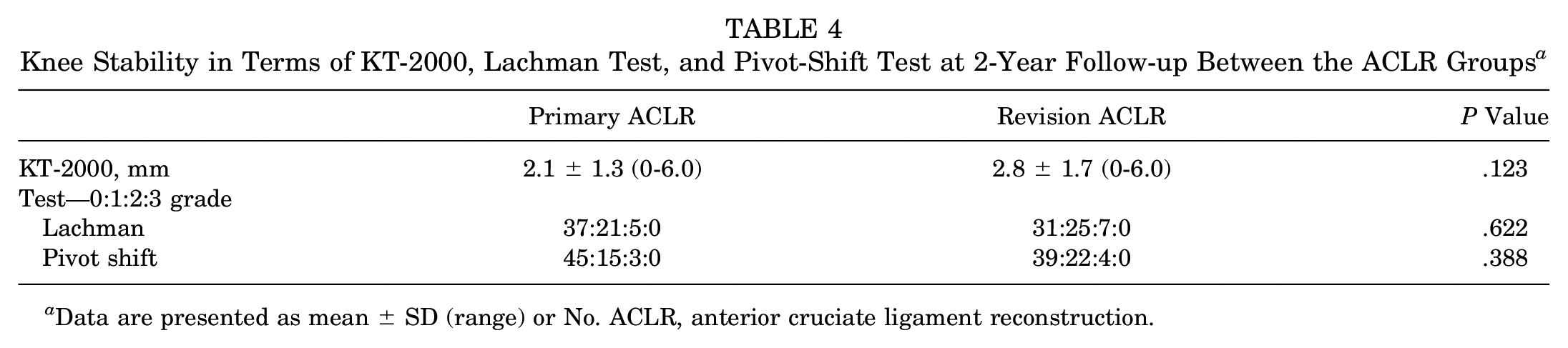
Data are presented as mean ± SD (range) or No. ACLR, anterior cruciate ligament reconstruction.
Postoperative Clinical Scores for the Primary and Revision ACLR Groups a
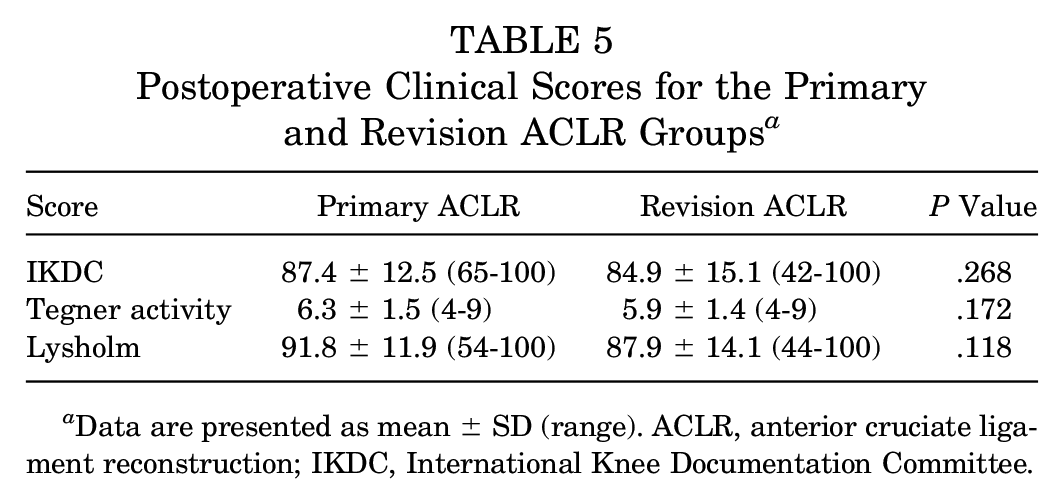
Data are presented as mean ± SD (range). ACLR, anterior cruciate ligament reconstruction; IKDC, International Knee Documentation Committee.
Return to Sport
There was a significant difference in total RTS, with 53 of 63 (84.1%) in the P-ACLR group and 41 of 63 (65.1%) in the R-ACLR group (P = .014), and no significant difference was calculated in terms of RTS at the same level, with 35 (55.6%) after P-ACLR and 31 (49.2%) after R-ACLR (P = .476). Patient-reported factors that influenced RTS and level of RTS are shown in Table 6. Fear of reinjury was the most common factor cited by sports-changed patients in the P-ACLR and R-ACLR groups, at 15 of 28 (53.5%) and 26 of 32 (81.3%), respectively, with significantly more patients in the R-ACLR group (P = .021). There were 9 (32.1%) patients in the P-ACLR group and 13 (43.8%) in the R-ACLR group who also had persistent knee pain. Significantly more patients in the R-ACLR group cited a non–knee related reason at 27 of 32 (84.3%) versus 15 of 28 (53.6%) in the P-ACLR group (P = .009). All patients with sport changes had multifactorial causes, and each component was counted individually.
Patient-Reported Factors for Sport Change in the Primary and Revision ACLR Groups a
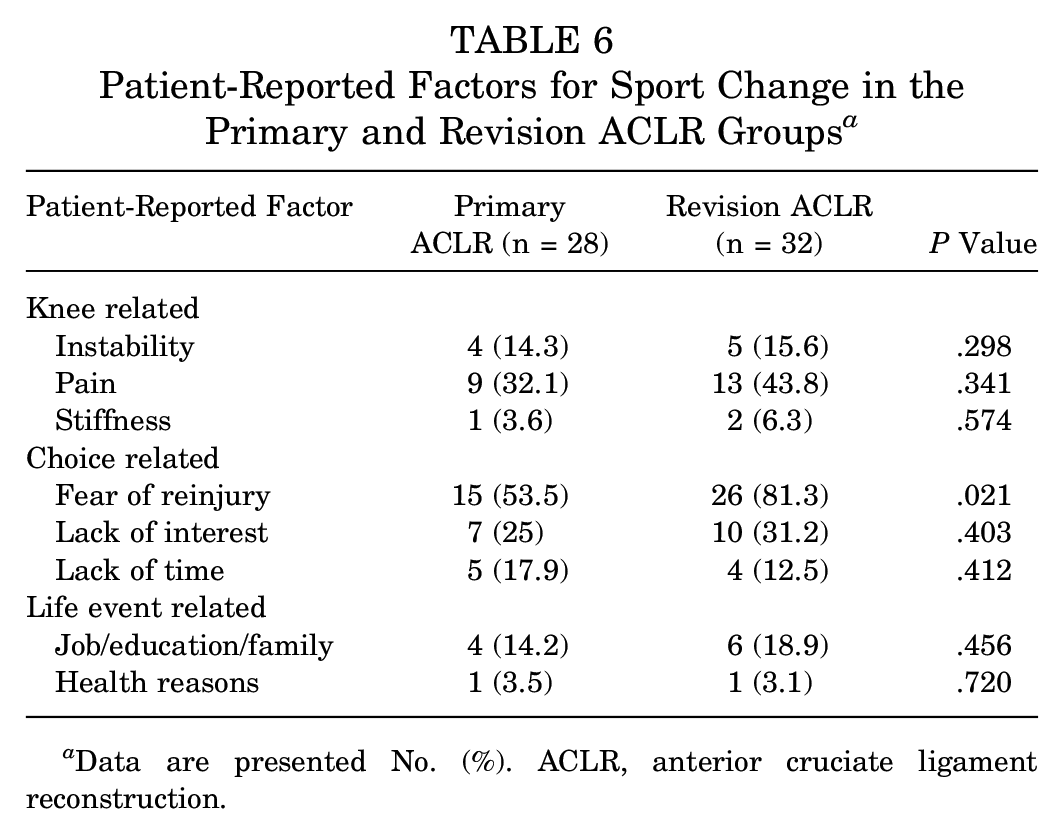
Data are presented No. (%). ACLR, anterior cruciate ligament reconstruction.
Complications
No infection was recorded. No graft rupture or reoperation occurred in the R-ACLR and P-ACLR groups. There was also no contralateral ACL rupture in either group.
Discussion
The most important findings of this matched-pair study were that the PRO scores (IKDC, Tegner, and Lysholm) were not significantly different, but there was a significant difference in RTS between the R-ACLR and P-ACLR groups at 3- to 5-year follow-up. Multiple factors resulted in a significantly lower RTS rate in the R-ACLR group; psychological factors (ie, fear of reinjury) especially had a significant influence, though knee symptoms notably did not.
R-ACLR is generally considered to be a more technically demanding procedure, especially for cases that require extreme widening of the bone tunnels and/or semianatomic tunnels after P-ACLR.48,49 The decision to use a particular graft type for R-ACLR (HT or BPTB autograft) was based on patient factors and choice. If either the femoral or the tibial tunnel was >9 mm, a BPTB autograft was recommended. If both tunnels were not >9 mm, the contralateral HT tendon could be harvested for ACL graft. For some patients who did not wish to have tendons harvested from the healthy contralateral knee, the BPTB was harvested from the affected knee. Excessive tunnel widening is also an indication for a 2-stage procedure, and staged revision should be strongly considered in cases with tunnel widening >15 mm or >150%, although there is no absolute cutoff for tunnel enlargement.13,28,49 Studies have demonstrated no difference in outcomes between 1- and 2-stage R-ACLR.11,34,35 In the present study, all R-ACLRs were performed in single-stage procedure, and all tunnels were managed according to the methods mentioned earlier.
Although considerable advances have been achieved in P-ACLR and R-ACLR, a lot of patients do not recover from R-ACLR, and clinical results remain poor as compared with P-ACLR.2,50 A large number of factors have been identified to influence the results of ACLR, such as age, sex, technical mistakes, graft options, unaddressed concomitant meniscal and cartilage injuries, PATS, and generalized mobility, among others.26,33,36,39,40,50 Cristiani et al 12 compared the same cohort of patients who underwent P-ACLR and R-ACLR, and worse knee outcomes were found after R-ACLRs. The amount of PATS was not reported in their study because greater PATS occurred in patients with R-ACLR and inferior results were noted in patients with greater PATS.24,41 In present study, we analyzed the outcomes of R-ACLR and P-ACLR using propensity score matching by age, sex, body mass index, PATS, and generalized hypermobility at 3- to 5-year follow-up. Similar knee stability results (KT-2000, Lachman test, and pivot-shift test) were revealed at 2-year follow-up, and PRO scores (IKDC, Tegner, and Lysholm) were similar at final follow-up in both groups in the present study.
There was a lower RTS rate after R-ACLR versus P-ACLR. 2 Glogovac et al 15 performed a systematic review of 13 studies with 1130 patients and found an RTS rate of 56% to 100%, with an RTS rate at preinjury level of 13% to 69% at 6.4- to 12-month follow-up. Andriolo et al 2 evaluated 1185 patients from 29 studies and noted improved Tegner scores at a mean follow-up of 5 years, but 57% of patients did not return to the same level of sport activity, significantly inferior to results after a primary procedure. The rate of RTS to a preinjury level ranged widely from 14% to 56% after R-ACLR.2,8 Although R-ACLR yielded good stability restoration, similar to primary operation, it did not correlate directly with increased participation in sport. 3 This is in line with the present study, although some related factors were matched, such as PATS and Beighton score. In the present study, total RTS was significantly worse in the R-ACLR group as compared with the P-ACLR group.
Research is limited on the factors that prevent patients from RTS or influence the level of sport, especially after R-ACLR. 5 One possible reason that R-ACLR results in lower RTS rates is the presence or more damage in the knee compared with P-ACLR.42,43 A reinjured knee may have more severe chondral and meniscal injuries. 2 As expected, RTS at the preinjury level was lower than RTS at any level in our cohort and suggested that knee-related symptoms influence outcomes. However, there was no significant difference between the groups in terms of knee-related symptoms. Kinesiophobia or fear of reinjury has been suggested to influence RTS after P-ACLR even though the knee stability has been restored.14,19 Fear of reinjury was described as the most common factor influencing RTS in both groups in the present study, and significantly more patients in the R-ACLR group were afraid of reinjury. Other factors influenced RTS, such as changes in lifestyle attributed to age, job, or family commitments.17,19,23,27,45 This suggested that the decision by patients to RTS after R-ACLR was multifactorial and not restricted to persistent physical symptoms, accounting for the lower RTS rate after R-ACLR as compared with P-ACLR. Notwithstanding the technical aspects of surgery, it is important to understand the patient-reported psychological and social factors that influence the decision to RTS, which is considered a measure of a successful outcome after R-ACLR.
Our study has some limitations. First is the lack of on-site follow-up to obtain structural measures and radiographic assessment of osteoarthritis at the final follow-up. Telephone follow-up for all patients was obtained mainly due to COVID-19. We believe that the combination of patient recall and collection of corresponding operative and clinic notes for confirmation was feasible and reasonable. Furthermore, all patients were seen and evaluated at 2 years postoperatively, with pivot-shift test results and side-to-side differences reported. Second is the retrospective nature and nonrandomized design. Treatment selection bias for any comparative retrospective clinical study is unavoidable. The effect of this was alleviated through successful propensity matching. Last is a potential bias to data analysis; namely, that different autografts (BPTB and HT) were used for R-ACLR. Because the patients with BPTB autografts constituted 12 cases in our study, the clinical outcomes between grafts were not compared. Previous studies showed no differences between autografts regarding graft failure and clinical outcomes.16,29
Conclusion
R-ACLR resulted in similar clinical scores (IKDC, Tegner, and Lysholm) but a significantly lower RTS when compared with P-ACLR at 3 to 5 years of follow-up. Fear of reinjury was the most common factor that caused sport changes in patients with R-ACLR.
Footnotes
Submitted July 10, 2022; accepted November 18, 2022.
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.