
Abstract
Background:
The discoid medial meniscus is a rare congenital anomaly of the knee. The literature is limited to small case series.
Purpose/Hypothesis:
Our purpose is to report the clinical manifestations and operative treatments of discoid medial menisci in children from multiple centers in North America. We hypothesized that symptoms and signs, arthroscopic findings, surgical treatments, and outcomes are similar to those for symptomatic discoid lateral menisci.
Study Design:
Case series; Level of evidence, 4.
Methods:
A retrospective review identified patients with a diagnosed discoid medial meniscus confirmed at surgery across 8 children’s hospitals between January 2000 and June 2021. The literature on discoid lateral menisci was reviewed and summarized for comparison.
Results:
A total of 21 patients (9 female, 12 male) with 22 discoid medial menisci were identified. The mean ± SD age at the time of diagnosis was 12.8 ± 3.8 years. The most common symptoms and signs were locking and/or clunking, present in 12 of 22 knees (55%), similar to that reported in patients with discoid lateral menisci. Twelve discoid medial menisci were complete (55%); 8, incomplete (36%); and 2, indeterminate (9%). Tears were present in 13 knees, most commonly horizontal cleavage (54%). Five discoid medial menisci were unstable (23%): 3 for posterior tears and 2 for rim insufficiency. All 22 knees underwent arthroscopic saucerization, and of the 13 torn menisci, 7 (54%) were repaired. The median follow-up was 24 months (range, 2-82 months). Four knees underwent reoperation. All knees that required reoperation had undergone repair for a posteriorly located tear. There was a significant association between operative repair and need for reoperation (P = .0048). High rates of peripheral instability were also noted in case series of patients with discoid lateral menisci.
Conclusion:
Patient presentations and treatments for those with discoid medial menisci were similar to those reported for patients with discoid lateral menisci. Knees with discoid medial menisci also demonstrated instability attributed to peripheral insufficiency and posterior tears. Tears were present in over half of knees with discoid medial menisci, and reoperation was more common in knees that underwent repair of tears than those without repair.
The discoid meniscus is a rare aberration in the growth and development of the meniscus that results in hypertrophic meniscal tissue, decreased content of collagen fibers with a more disorganized course than seen in the normal meniscus, and an atypical shape.1,31 Rather than the crescent shape of a typical meniscus, the discoid meniscus is thicker and wider, at times covering an entire half of the tibial plateau. These differences predispose the discoid meniscus to tearing from shear stresses. Even in the absence of tears, the size and shape of the discoid meniscus alone may impair joint motion. When symptomatic, discoid menisci can be painful and limit the mobility of otherwise healthy, active children.
Much of our current knowledge of discoid menisci comes from studying the more common discoid lateral meniscus, which has a prevalence of approximately 0.4% to 20%, depending on the population and the mode of sampling.8,24,29,30,33,35 Individuals with a discoid lateral meniscus commonly present with knee pain, swelling, and mechanical symptoms, often in the absence of an acute injury. §§ Typical symptoms are a snapping or clunking knee, swelling, a block to motion, locking, and giving way. ‖‖ Treatment for the symptomatic discoid lateral meniscus often includes saucerization and repair of an unstable rim, when present, as well as repair of tears.
The discoid medial meniscus, however, is exceedingly rare, with an estimated prevalence between 0.06% and 0.3%, depending on the population studied.10,14,37 Literature on the clinical presentation, operative treatment, and outcomes for discoid medial meniscus is sparse.
Given the rarity of the discoid medial meniscus, few centers have adequate numbers to produce more than small case series of patients. Through pooling patients from multiple centers across North America, this study aims to identify and report patterns in presentation and treatment outcomes limited to rates of reinjury and re-repair for children with a symptomatic discoid medial meniscus.
We hypothesized that symptoms and signs at clinical presentation, arthroscopic findings, surgical treatments, and outcomes for discoid medial menisci are similar to those for symptomatic discoid lateral menisci.
Methods
Study Design
After institutional review board/human participants approval and data use agreements for sharing of data were obtained, a retrospective cohort study was performed to examine patients with discoid medial meniscus treated across 8 pediatric hospitals in North America between January 2000 and June 2021. We included all patients with a diagnosed discoid medial meniscus confirmed through direct surgical observation via an arthroscopic or open procedure. Patients with a presumed diagnosis of a discoid medial meniscus by indirect means, such as magnetic resonance imaging (MRI) or arthrogram without confirmation at surgery, were not included. Patient records with the following diagnostic codes were reviewed: International Classification of Diseases, Ninth Revision, 717.3, 717.5, 717.8, and Tenth Revision, Q68.6, M23.006, M23.007, M23.009, M23.305, S83.20-24. The following data were collected from patient records and operative reports: patient characteristics, clinical manifestation, presence of unilateral or bilateral meniscal abnormalities, type of discoid meniscus, tear patterns, quality of cartilage, concomitant injury, operative procedures, and treatment outcomes limited to reinjuries and re-repairs. We compared these results with those of case series of discoid lateral menisci reported in the literature between 1976 and 2022, obtained via a PubMed search using the term discoid lateral meniscus, limited to the English language.
Statistical Analysis
Descriptive statistics were used to summarize clinical features, operative treatment, and outcomes for children with a discoid medial meniscus. Demographic characteristics are described as means and standard deviations for continuous variables and counts and percentages for categorical variables. Continuous data were reviewed for normality using the Shapiro-Wilk test. Nonparametric data are presented as median (range). The Fisher exact test was used to calculate P values for comparisons of categorical variables. A 2-sided P < .05 was considered significant.
Results
Review of medical records identified 21 patients, 9 female and 12 male, with 22 discoid medial menisci who met the study inclusion criteria. Patients had a mean ± SD age of 12.8 ± 3.8 years at diagnosis. One patient had bilateral discoid medial menisci, and 1 patient had medial and lateral discoid menisci in the same knee. Twelve (55%) discoid menisci were in the right knee. All patients were treated via arthroscopic surgery between July 1, 2003, and June 2, 2021. The time from initial diagnosis to operative treatment was a mean 13 months (range, 0-121 months), although for 2 patients there was >3 years between diagnosis and treatment. Excluding these outliers, the mean time from diagnosis to treatment was 4 months (range, 0-18 months). There was a nonnormal distribution for the time from initial diagnosis to operative treatment and the time from operative treatment to the last postoperative follow-up.
Clinical Manifestations
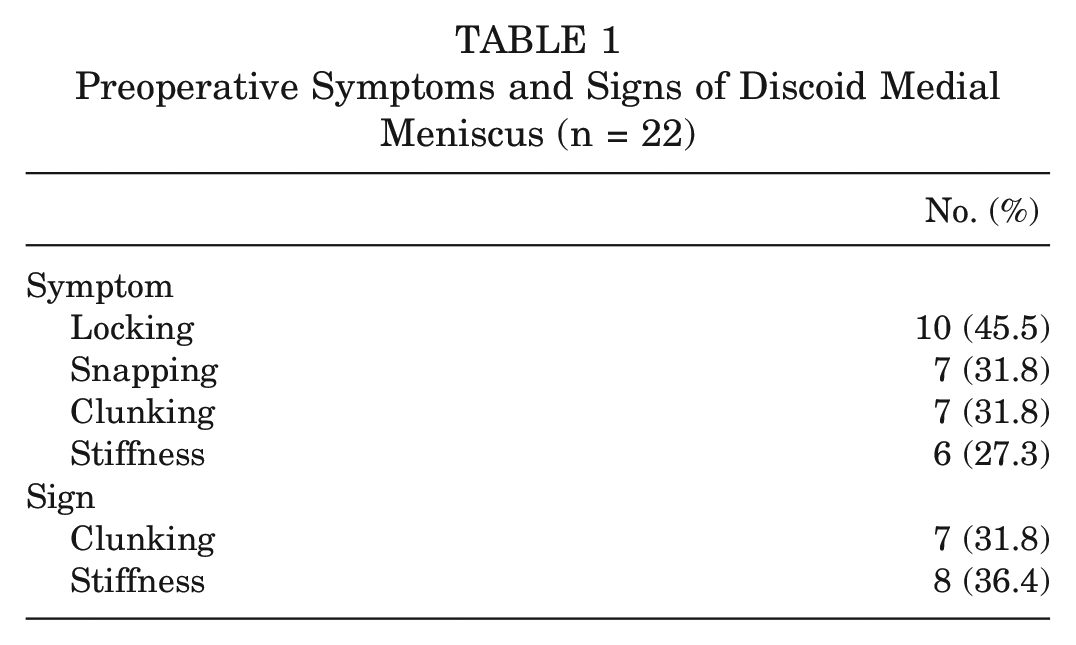
The most common symptom of patients with discoid medial meniscus was locking, and the most common sign was clunking (Table 1), with locking and/or clunking present in 12 of 22 knees (55%). Eighteen knees (81.8%) were initially diagnosed with a discoid medial meniscus through MRI before confirmation at surgery. Eight patients (38%) had a concurrent diagnosis of the affected knee: 2 with parameniscal cysts, 1 anterior cruciate ligament (ACL) sprain, 1 ACL tear, 1 chondral defect of the anterior medial tibial plateau, 1 obligate patellar dislocation, 1 with postseptic arthritis, and 1 with lateral patellar congenital dislocation and ACL deficiency.
Preoperative Symptoms and Signs of Discoid Medial Meniscus (n = 22)
Operative Evaluation
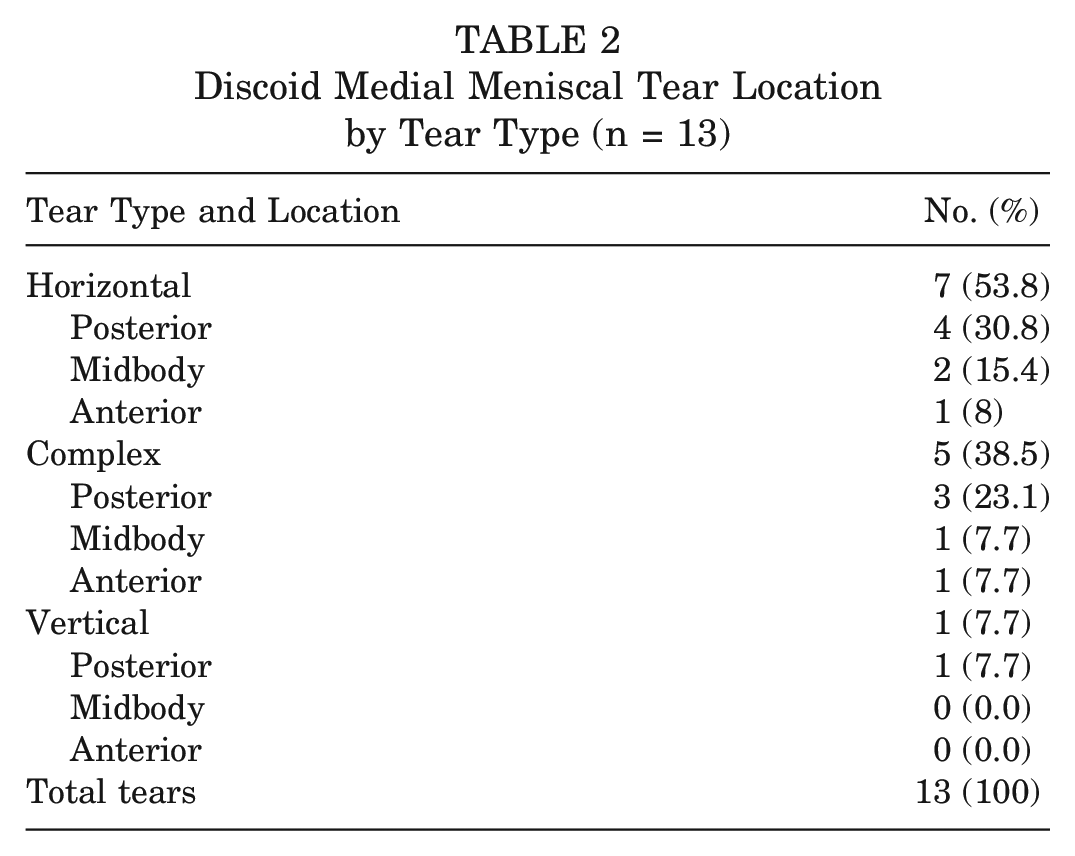
Of the 22 discoid medial menisci, 12 (55%) were complete, 8 (36%) were incomplete, and 2 (9%) were indeterminate. A majority of discoid medial menisci (17/22; 77%) were stable. Five discoid medial menisci were unstable (23%): 3 for posterior tears and 2 for rim insufficiency. Tears were present in 13 (59%) cases. Of these, 8 (62%) were posterior tears, 3 (23%) were midbody tears, and 2 (15%) were anterior tears. Horizontal cleavage tears were most common, followed by complex and vertical tears (Table 2).
Discoid Medial Meniscal Tear Location by Tear Type (n = 13)
Eighteen knees (82%) had normal quality of the medial articular cartilage and lateral cartilage. Two knees (9%) had Outerbridge grade I (softening and swelling) medial articular cartilage; 1 knee (5%) had grade IV (exposed subchondral bone) medial articular cartilage; and 1 knee (5%) had grade IV medial and lateral cartilage changes in the patient with a history of septic arthritis.
Operative Procedures
All discoid medial menisci underwent arthroscopic saucerization. Of the 13 torn menisci, 7 (54%) were repaired. The 2 knees with posterior rim instability without a meniscal tear were not repaired. Repair techniques were as follows: 3 all-inside, 1 outside-in, 1 inside-out, 1 all-inside and inside-out, and 1 unknown.
Postoperative Course
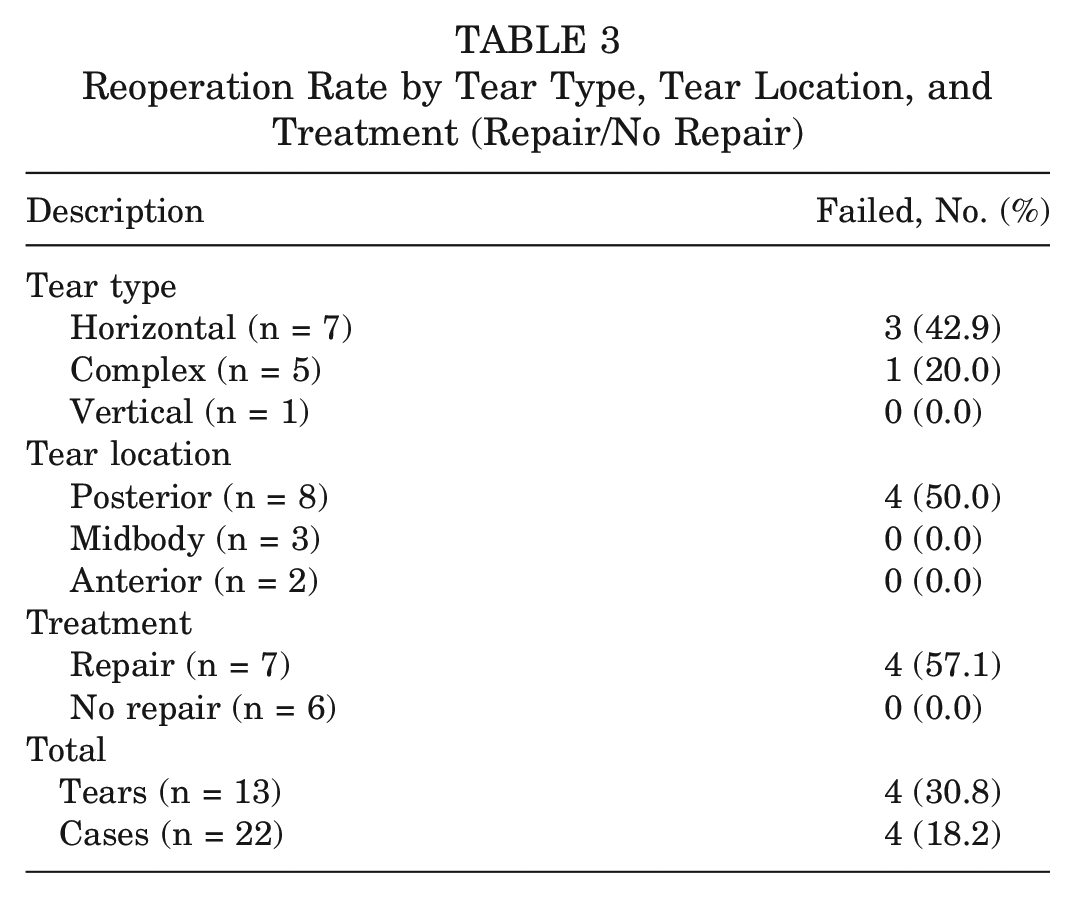
Patients were followed postoperatively for a median 20 months (range, 2-82 months). Four knees (18%) required retreatment. One patient with reinjury to the knee did not undergo reoperation. All knees that required retreatment had a tear that was repaired during the initial procedure. There was a significant association between operative repair of a medial discoid meniscal tear and need for retreatment (P = .0048). Reoperation was most common in a horizontal tear type and a posterior tear location (Table 3).
Reoperation Rate by Tear Type, Tear Location, and Treatment (Repair/No Repair)
Literature Review: Discoid Lateral Menisci
A review of 503 abstracts from the PubMed query revealed 27 reports on discoid lateral menisci that included clear descriptions of numbers of patients with various symptoms, signs, and/or rim instability (Table 4). A summation of numbers of patients and affected knees with classic symptoms, signs, and rim instability revealed 44% with a history of mechanical symptoms, 31% with mechanical signs, and 35% with rim instability, similar to the frequencies seen in our patients with discoid medial meniscus.
Reports Including Characteristics of Primarily Discoid Lateral Menisci: 1976-2022 a
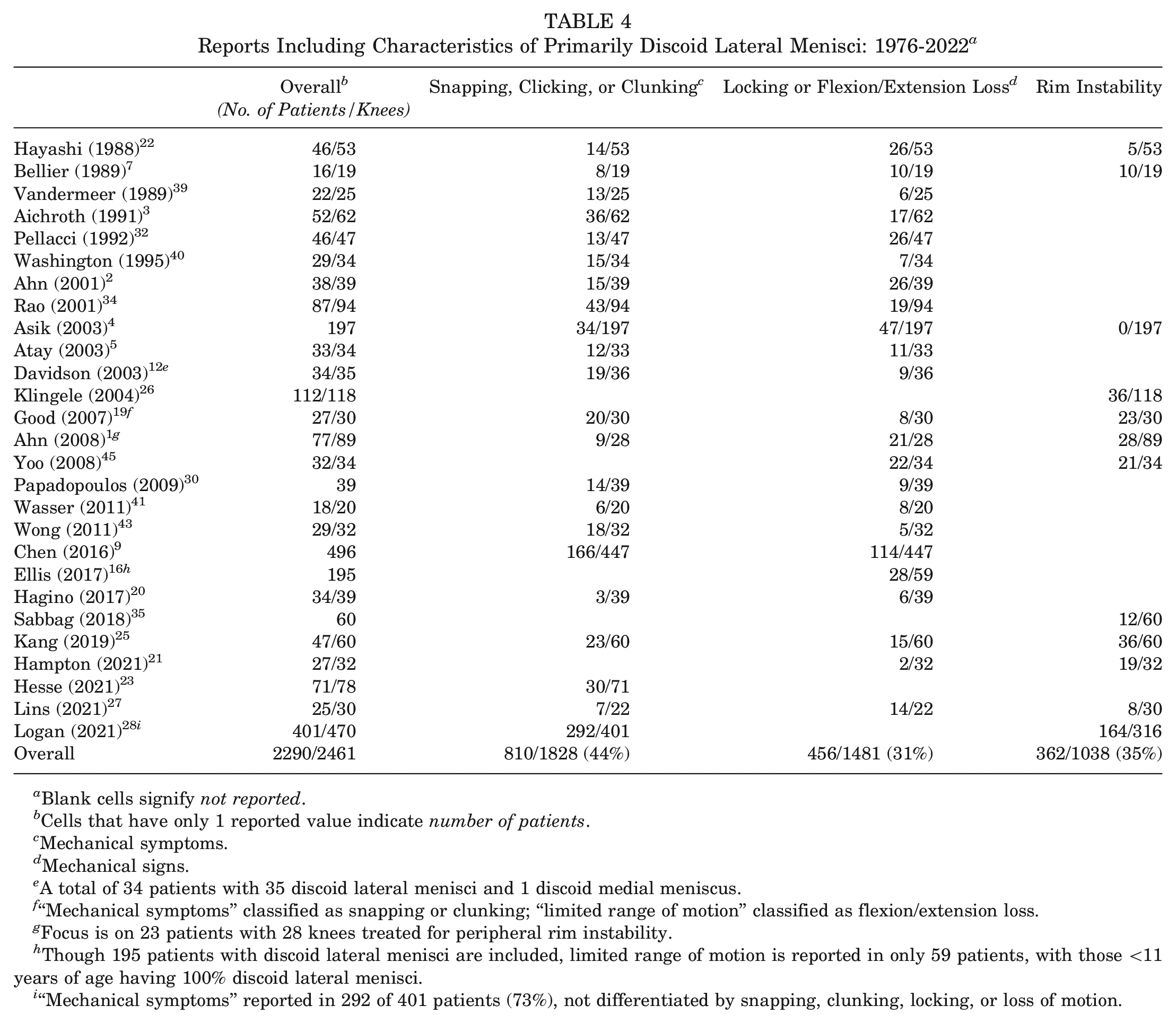
Blank cells signify not reported.
Cells that have only 1 reported value indicate number of patients.
Mechanical symptoms.
Mechanical signs.
A total of 34 patients with 35 discoid lateral menisci and 1 discoid medial meniscus.
“Mechanical symptoms” classified as snapping or clunking; “limited range of motion” classified as flexion/extension loss.
Focus is on 23 patients with 28 knees treated for peripheral rim instability.
Though 195 patients with discoid lateral menisci are included, limited range of motion is reported in only 59 patients, with those <11 years of age having 100% discoid lateral menisci.
“Mechanical symptoms” reported in 292 of 401 patients (73%), not differentiated by snapping, clunking, locking, or loss of motion.
Discussion
This multicenter review of operative treatment of 21 patients with 22 discoid medial menisci revealed presenting symptoms and signs similar to those of patients with discoid lateral menisci, with patients presenting most commonly with mechanical symptoms and signs (locking and clunking).1,3,8,29,30 Our findings are consistent with previous literature, although limited, on discoid medial menisci. Small case series report knee pain without mechanical symptoms6,42 or knee pain and mechanical symptoms after trauma or of spontaneous onset. ¶¶
Bilateral discoid medial menisci were previously reported in 1 of 4 patients, 18 1 patient, 36 3 of 4 patients, 38 2 of 2 patients, 44 and 4 of 8 patients. 17 Our rate of bilateral discoid medial menisci was substantially lower at 1 of 21 patients. We did have 1 patient with discoid medial and lateral menisci, as did Jeannopoulos, 24 and 1 of 13 patients also had a discoid lateral meniscus as well as a discoid medial meniscus in the same knee in the study by Chen et al. 10 Specifically, Chen et al 10 reported on 13 operatively treated patients with discoid medial menisci over a 43-year period at 1 hospital. Most of the 13 patients had knee pain and mechanical symptoms and signs. All 13 patients had tears of the discoid medial meniscus: 10 were treated with complete medial meniscectomy, 1 with partial meniscectomy, and 2 by saucerization.
A 2021 retrospective case series at 1 institution reported 8 patients with discoid medial menisci in 12 knees, with tears in 75% of knees, a majority of which were horizontal cleavage tears. 17 Furthermore, 2 patients (16.7%) required reoperation after saucerization and meniscal tear repair. This is consistent with the 17.4% of cases that required reoperation in our study. A review of 407 knees in patients with a symptomatic discoid lateral meniscus found tears in 63% of knees, with horizontal cleavage tears being the most common tear type. 28 The reoperation rate of 17% in patients with a discoid lateral meniscus treated with arthroscopic saucerization was similar to our reoperation rate for discoid medial menisci.
Our rate of peripheral instability in knees with discoid medial menisci was lower than that for knees with discoid lateral menisci. This finding may be a result of the basic structural differences of the medial and lateral menisci, as the typical lateral meniscus with a popliteus hiatus may predispose the lateral side to rim instability, or it may merely be the result of our small sample size.
Limitations
This study has several limitations. The small sample size did not allow for robust statistical comparison and was largely descriptive in nature. In addition, short follow-up for many patients may have led us to underestimate the reoperation rate. However, the literature on the rare discoid medial meniscus is sparsely described in the pediatric population, and to our knowledge, this case series remains the largest in the literature to date. Although our findings suggest that the discoid medial meniscus shares many similarities to the discoid lateral meniscus, a direct analysis comparing characteristics of discoid medial and lateral menisci was not performed. Furthermore, the retrospective study design presents substantial limitations. We were unable to include any patient-reported outcomes in our analysis, given their spotty inclusion in records from the various centers, and we relied on chart and operative notes. Similarly, imaging and its availability were variable and very heterogeneous across institutions and practices over this 20-year period and thus not feasible to collect or compare and contrast.
As our series included only patients who had a discoid medial meniscus confirmed at surgery, we have skewed our review to those who were likely more symptomatic. The review of the literature of discoid lateral menisci, although broad, was not a formal systematic review and may therefore be biased. As the majority of the reports on discoid lateral menisci were surgical, they also likely consisted of patients who were more symptomatic and more likely to have mechanical symptoms and signs, meniscal tears, and rim instability contributing to their indications for surgery.
Given the rarity of the discoid medial meniscus and the findings presented here, a future dedicated prospective study, although ideal, would be challenging to perform. However, a more general multicenter prospective pediatric meniscal study would provide the next step in our understanding of congenital anomalies of the pediatric meniscus. Such a study could include preoperative MRI scans, a standardized protocol with pre- and postoperative alignment radiographs and follow-up examinations, as well as validated pediatric patient-reported outcomes.
Conclusion
In this multicenter study of patients treated for a discoid medial meniscus, the symptoms and signs at presentation, findings at arthroscopy, and outcomes were similar to those commonly seen in knees with a discoid lateral meniscus. Tears and peripheral instability were frequent, and reoperation was significantly associated with meniscal tear repair at initial operation. Our understanding of the presentation and outcomes of arthroscopic saucerization and repair in discoid lateral menisci may be cautiously extrapolated to the medial counterpart. Future studies should seek to determine the long-term functional and patient-reported outcomes after treatment of a symptomatic discoid medial meniscus.
Footnotes
Acknowledgements
The authors thank additional members of the Pediatric Research in Sports Medicine Meniscus Research Interest Group: Jennifer Beck, Jennifer Brey, Matthew Brown, Benton Heyworth, Elaine Joughin, Matthew Milewski, Jeffrey Nepple, Emily Niu, Lee Pace, John Schlecter, Tyler Stavinoha, Marc Tompkins, and Philip Wilson. They also thank Hannah Prock Gibbs, Nathalie Jourdain, Patrick Sachsalber, Mei Chen, and Viviana Bompadre for their assistance.
Submitted September 22, 2022; accepted January 18, 2023.
One or more of the authors has declared the following potential conflict of interest or source of funding: S.C. has received support for education from Stryker and Smith & Nephew. Z.S. has received consulting fees and support for education from Arthrex and hospitality payments from Stryker Corp. I.K. has received support for education from MedInc of Texas. C.J.F. has received support for education from Medwest Associates. R.J.L. has received research support and support for education from Vericel and Arthrex and support for education from Supreme Orthopedic Systems. B.M.H. has received support for education from Sequoia Surgical Inc and Arthrex. G.A.S. has received research support from Arthrex and support for education from Summit Surgical Corp. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.