
Abstract
Background:
Arthroscopic capsulolabral repair for posterior shoulder instability has been shown to improve patient-reported outcomes and return to sport at short-term and midterm follow-up, but long-term outcomes are unknown.
Purpose:
To determine the objective and subjective clinical outcomes of shoulder function after arthroscopic posterior shoulder stabilization at a minimum 10-year follow-up.
Study Design:
Case series; Level of evidence, 4.
Methods:
A total of 53 patients (55 shoulders) with unidirectional recurrent posterior shoulder instability who underwent arthroscopic capsulolabral repair were evaluated at a mean follow-up of 15.4 years. Outcomes such as the American Shoulder and Elbow Surgeons (ASES) shoulder score, Kerlan-Jobe Orthopaedic Clinic shoulder and elbow score, and subjective strength, stability, range of motion, and pain were evaluated preoperatively and postoperatively at a minimum 10-year follow-up. Outcomes from the same patient cohort were previously collected at 3.0-year follow-up and were evaluated for longitudinal analysis. Subgroup analyses for sport type (contact vs noncontact), position (thrower vs nonthrower), and revision versus nonrevision were performed. Risk factors for revision surgery based on magnetic resonance imaging findings, patient characteristics, and surgical findings were investigated.
Results:
Arthroscopic capsulolabral repair for posterior shoulder instability led to a statistically significant improvement on all outcome measures, with similar values at short-term (3.0-year) and long-term (15.4-year) follow-up. Across the total population, patients with 19 of 55 shoulders (35%) returned to sport at the same preinjury level, and patients with 33 of 55 shoulders (60%) returned to sport at some level. At long-term follow-up, patients with only 22% of shoulders were involved in the primary sport in which the injury was sustained, with patients with 28% of shoulders discontinuing sporting participation because of ongoing shoulder issues. Throwers trended toward lower Kerlan-Jobe Orthopaedic Clinic scores than nonthrowers both preoperatively (36.5 ± 22.8 vs 48.7 ± 22.9, respectively; P = .10) and postoperatively (57.4 ± 27.0 vs 73.5 ± 26.8, respectively; P = .09) but had similar improvements. Contact and noncontact athletes had similar preoperative and postoperative values, with equal improvements after surgery. With failure defined as revision surgery, an ASES score <60, or a stability value >5, 19 of 55 shoulders (35%) met failure criteria at final follow-up. Overall, 7 of 55 shoulders (13%) underwent revision surgery. At long-term follow-up, patients who underwent revision surgery had worse outcomes than those who did not undergo revision (ASES score: 53.1 ± 25.9 vs 81.8 ± 19.4, respectively; P < .001). An acute injury in the postoperative period (P < .001) and a smaller glenoid bone width on magnetic resonance imaging (P = .02) were the only identified risk factors for revision surgery.
Conclusion:
Arthroscopic capsulolabral repair for posterior shoulder instability was a durable treatment option that improved long-term shoulder pain and function and facilitated return to sport in the majority of patients at a mean follow-up of 15.4 years, although a notable proportion of patients met various criteria for failure.
Posterior shoulder instability continues to be shown to account for a significant percentage of shoulder instability cases and has been increasingly recognized as a cause of persistent shoulder pain and dysfunction, especially among athletic populations.2,14,22 Although anterior shoulder instability is more commonly associated with a traumatic dislocation/subluxation with subsequent subjective and objective shoulder instability, posterior shoulder instability often has a more insidious, atraumatic onset thought to be secondary to sport-associated microtrauma, resulting in a chief concern of pain. 6 Notably, both contact and overhead sports are commonly associated with posterior shoulder instability.15,20 Even though an initial trial of nonoperative management is the first-line treatment approach, a high percentage of patients with posterior shoulder instability will experience persistent pain and dysfunction for which elective surgery is often pursued.16,26
Arthroscopic capsulolabral repair for posterior shoulder instability has been shown to improve pain and stability, with >90% of patients capable of returning to sport at short-term to midterm follow-up.10,19 However, despite arthroscopic stabilization, in certain populations, only two-thirds of patients return to sport (RTS) at the same preinjury level, and up to one-third experience persistent pain and/or instability, necessitating revision surgery. 12 Furthermore, long-term outcomes (ie, >10 years) after arthroscopic capsulolabral repair for posterior shoulder instability have not yet been reported.
A previous report on the clinical outcomes of 183 patients (200 shoulders) who underwent arthroscopic capsulolabral repair for posterior shoulder instability at a mean follow-up of 3.0 years demonstrated improvements in pain and function, which were supported by similar studies from independent research groups.10,12,13 The purpose of the present study was to investigate the objective and subjective clinical outcomes after arthroscopic shoulder stabilization at a minimum 10-year follow-up. It was hypothesized that long-term postoperative shoulder function would remain statistically superior to preoperative shoulder function, with a reduced benefit for those who required revision surgery.
Methods
Patient Selection
Institutional review board approval and informed consent were obtained before the initiation of the study. A cohort of 183 patients (200 shoulders) who underwent arthroscopic capsulolabral repair for isolated posterior shoulder instability between January 1998 and December 2009, for whom clinical outcomes at a mean follow-up of 35.9 months were previously published, 10 were recruited for this study. Patient participation was solicited by mail and telephone. As before, inclusion criteria were athletes of any level and sport (including contact and throwing athletes), the presence of unidirectional posterior shoulder instability, and a minimum 10-year follow-up from primary surgery. Patients who displayed posterior-inferior instability or multidirectional instability or those with habitual or psychogenic voluntary shoulder subluxations were excluded from the study. All included patients had a failed initial course of preoperative physical therapy for motion and strengthening, which included treatment for scapular dyskinesis as well as avoidance of aggravating activities. The timing of surgery was determined by the senior author (J.P.B.), in discussions with the patient and in consideration of patient preference, sport, level of competition, and timing for return to competitive athletics.
Operative Technique and Postoperative Rehabilitation
Operative treatment was individualized to each patient and was dictated by preoperative evaluation, examination under anesthesia, and intraoperative findings, as previously described in detail. 10 Briefly, surgery was performed with the patient in the lateral decubitus position using modern capsulolabral reconstruction tools and techniques including suture anchor fixation. Depending on the abnormality identified on preoperative and intraoperative evaluations, 1 of 3 procedures was performed: (1) capsulolabral plication with suture anchors, (2) capsulolabral plication without suture anchors, and (3) capsulolabral plication with suture anchors and additional sutures. Concomitant rotator cuff tears with <50% thickness were debrided, and those with >50% thickness were repaired. The postoperative rehabilitation protocol was carried out as previously described, with full RTS at approximately 6 months. 10
Patient Characteristics and Clinical Outcomes
Included patients completed a secure online survey that, when combined with a review of electronic medical records, provided the following patient characteristics: age at surgery, sex, hand dominance, side of injury, sport, position, level of participation, time between primary and revision surgery (if applicable), and length of follow-up. Sports were dichotomized into contact and noncontact sports, with the former including football, ice hockey, wrestling, lacrosse, or other combat sports such as martial arts. Athletes were asked to self-identify as throwers if they exposed their shoulder to repetitive stress from the throwing motion. 23 The level of participation at the time of the injury was categorized as professional, college, high school, or recreational.
Clinical outcome measures included the American Shoulder and Elbow Surgeons (ASES) shoulder score and Kerlan-Jobe Orthopaedic Clinic (KJOC) shoulder and elbow score. The ASES score is categorized as excellent (>80), good (61-80), satisfactory (41-60), and poor (≤40). Subjective values of pain (0-10; 0 = no pain, 10 = severe pain), stability (0-10; 0 = stable, 10 = completely unstable), strength (0-3; 0 = none, 1 = markedly decreased, 2 = slightly decreased, 3 = normal), and range of motion (ROM; 0-3; 0 = poor, 1 = limited, 2 = satisfactory, 3 = full) were also collected. For the above clinical outcomes, patients self-assessed their postoperative and preoperative shoulder status. RTS at the same level or any level (ie, lower level) was evaluated, as was involvement in the same (preoperative) sport. The reason for not returning to sport at the same preoperative level was also recorded, if applicable. Finally, patients were asked if surgery was worthwhile. Excluding the addition of the KJOC score at long-term follow-up, all clinical outcomes were measured in the earlier study of this patient cohort, 10 with long-term postoperative outcomes statistically compared with preoperative and short-term follow-up (~36 months) outcomes.
Comparisons of long-term postoperative, short-term postoperative, and preoperative results on the above clinical outcome measures were made across the total patient population (n = 55 shoulders), with subgroup analyses comparing findings between (1) nonthrowers and throwers, (2) noncontact and contact athletes, and (3) nonrevision and revision. For patients who underwent revision surgery, clinical outcomes were additionally assessed after failure but before revision surgery. Risk factors for revision surgery, including previously identified patient characteristics, injury mechanisms, surgical findings, and glenolabral morphologies on magnetic resonance imaging (MRI) scans (described below), were assessed in the included patient population. The rate of failure, previously defined as the need for revision surgery, an ASES score <60, or a stability value >5, was also determined. 10
Surgical Findings
Operative reports were reviewed and noted for the following findings: posterior labral tear, patulous posterior capsule, rotator cuff tear, biceps tear, general capsular laxity, capsular tear or reverse humeral avulsion of the glenohumeral ligament, cartilage injury, osteoarthritis, and reverse Hill-Sachs lesion. The surgical technique was noted for the use of sutures, suture anchors, or a combination of sutures and suture anchors. The number of sutures and/or suture anchors was recorded.
MRI Measurements
Measurements of radiographic parameters on preoperative MRI scans were performed as previously described and included bone, chondral, and labral version; bone and labral width; and labral version weight and labral width weight, representing the effect of the labrum in proportion to the version and width, respectively, of the overall bone-labral complex. 17 Namely, labral version weight = (labral version – bone version)/bone version and labral width weight = (labral width – bone width)/bone width. Any additional abnormality, such as biceps tendinopathy or rotator cuff injury, was also noted. Radiographic parameters on MRI scans were compared between the revision and nonrevision groups.
Statistical Analysis
Data are presented as mean ± SD unless otherwise noted. Comparisons of continuous variables over multiple time points, including the ASES score, KJOC score, pain, and stability, were performed using the Kruskal-Wallis test with the Dunn test of multiple comparisons. Between-group comparisons of continuous variables, such as sport type (noncontact vs contact) and position (nonthrower vs thrower), were performed using the Mann-Whitney U test. Ordinal data, including subjective ROM and strength, were compared using the Mann-Whitney U test. Categorical data, including patient characteristics, injury mechanisms, surgical findings, and RTS rates, were analyzed using the Fisher exact test. Statistical significance was set at P≤ .05. Statistical analyses were performed using Prism 8 statistical software (GraphPad Software).
Results
Patient Characteristics
Of the original cohort of 183 patients (200 shoulders), 10 53 patients (55 shoulders) were available for analysis at a mean follow-up of 15.4 years (range, 10.9-19.4 years). Reasons for exclusion are shown in Figure 1. All of the included patients had existing outcome scores from the previous study 10 at a mean follow-up of 35.9 months (range, 12.0-86.9 months). Of the 53 patients, 34 (64%) were male, and 19 (36%) were female, with a mean age at surgery of 22.7 years (range, 13.7-52.0 years). There were 39 shoulders (71%) in patients exposed to noncontact sports compared with 16 shoulders (29%) in patients in contact sports. There were 31 shoulders (56%) in nonthrowing athletes and 24 shoulders (44%) in throwing athletes. Additional patient characteristics, including sport type and level of participation, are shown in Table 1.
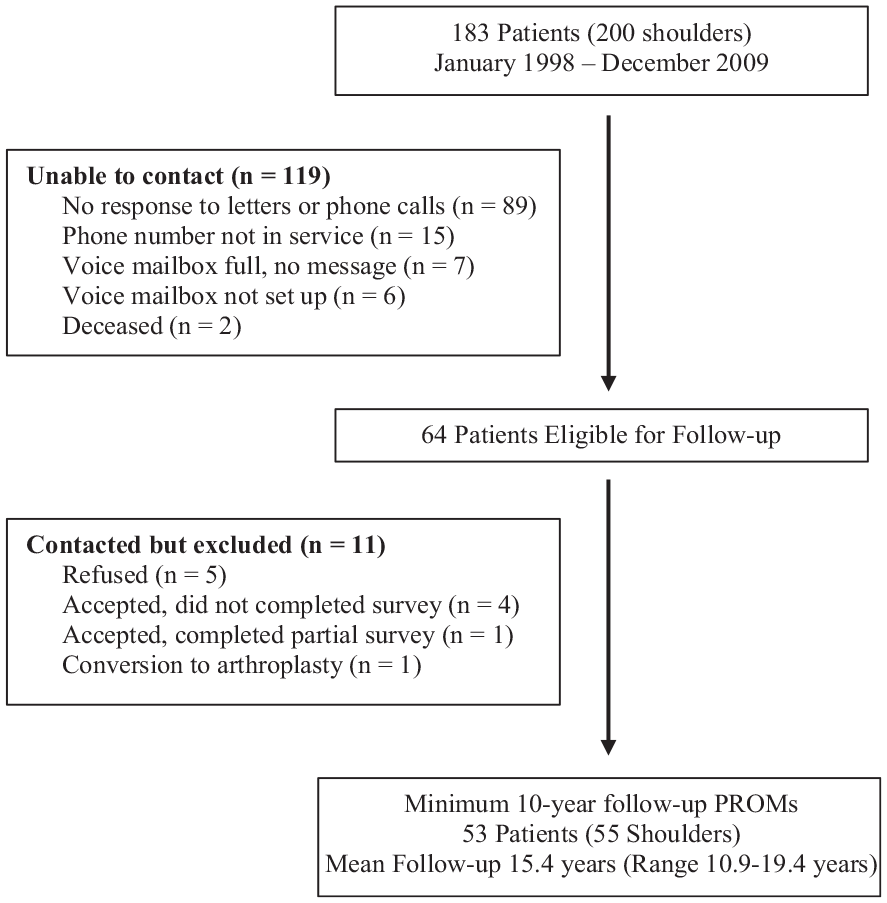
Flow diagram of study cohort. PROMS, patient-reported outcome measures.
Patient Characteristics a
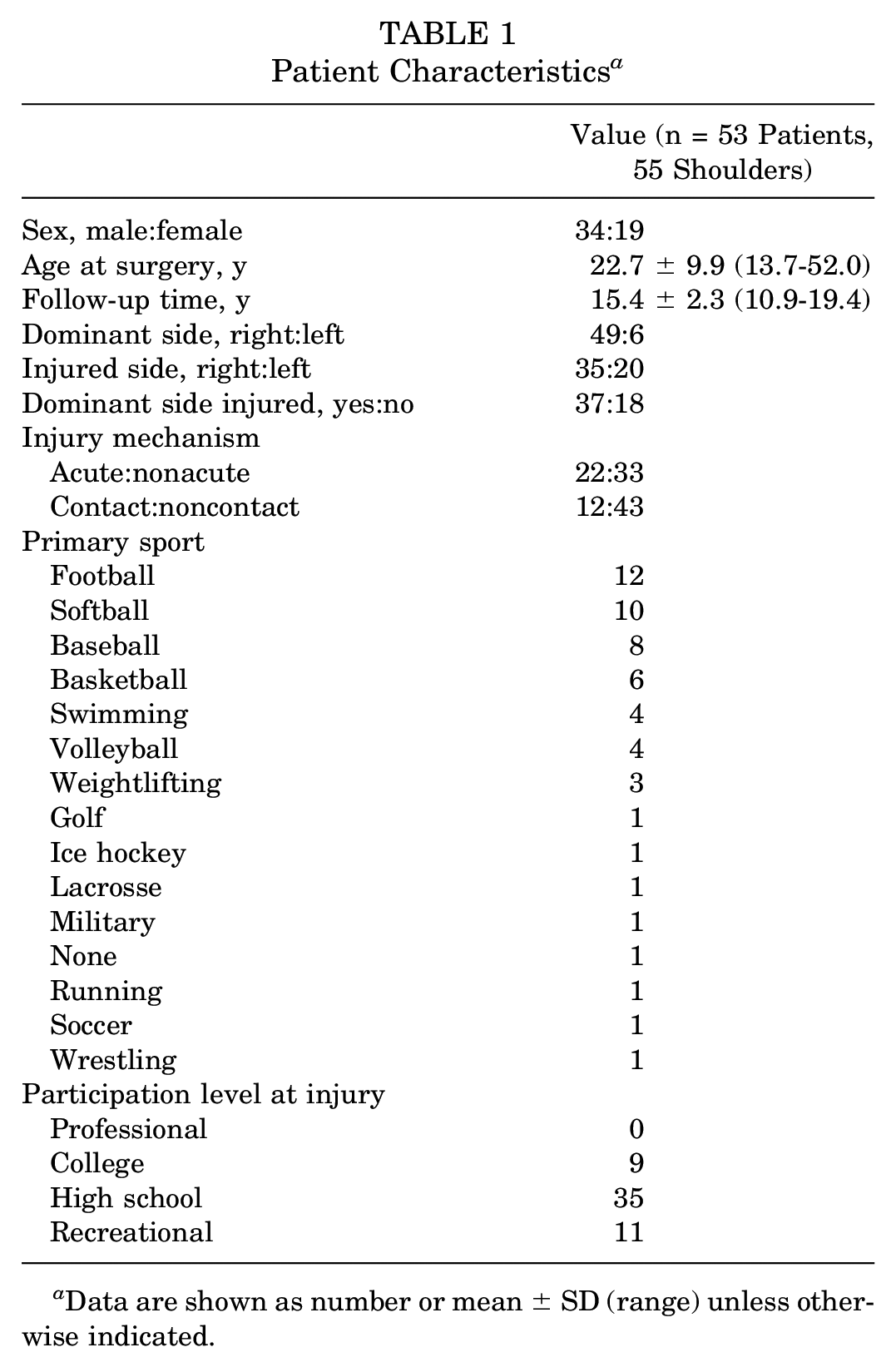
Data are shown as number or mean ± SD (range) unless otherwise indicated.
Total Population
Across all included shoulders (n = 55), the long-term postoperative results were significantly higher for all clinical outcome measures (ASES, KJOC, pain, stability, ROM, strength) compared with preoperatively (P≤ .001) (Table 2). According to the ASES score, 58% of shoulders were excellent; 19%, good; 15%, satisfactory; and 8%, poor. Thus, 77% of shoulders had excellent or good results on the ASES score at final follow-up. Only the subjective ROM was significantly worse at final follow-up than short-term follow-up (Table 2).
Outcomes for Total Population (n = 55) a
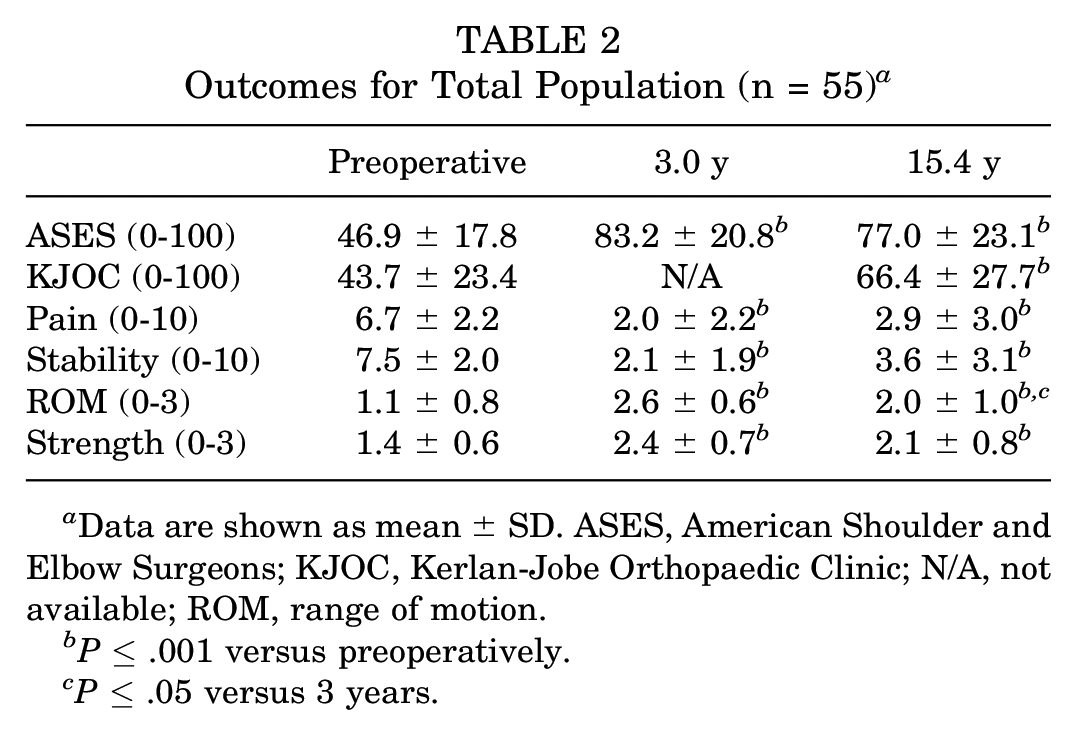
Data are shown as mean ± SD. ASES, American Shoulder and Elbow Surgeons; KJOC, Kerlan-Jobe Orthopaedic Clinic; N/A, not available; ROM, range of motion.
P≤ .001 versus preoperatively.
P≤ .05 versus 3 years.
Across the total population, patients with 19 of 55 shoulders (35%) returned to sport at the same preinjury level, whereas patients with 33 of 55 shoulders (60%) returned to sport at some level (Table 3). For patients unable to return to sport at the same level, 13 of 36 shoulders (36%) had persistent problems, and for patients unable to return to sport at any level, 11 of 22 shoulders (50%) had persistent problems. At long-term follow-up, patients with only 21% of shoulders were involved in the primary sport in which the injury was sustained, with patients with 28% of shoulders discontinuing sporting participation because of ongoing shoulder issues. Instead, school graduation (48%) and age (32%) constituted the 2 major reasons for discontinuing sport. Despite a considerable proportion of shoulders in patients who forwent continued sport participation, 89% were in patients who endorsed surgery as worthwhile at final follow-up. This was nearly equivalent to the 88% in patients who reported surgery was worthwhile at 3.0-year follow-up.
Return to Sport for Total Population (n = 55)
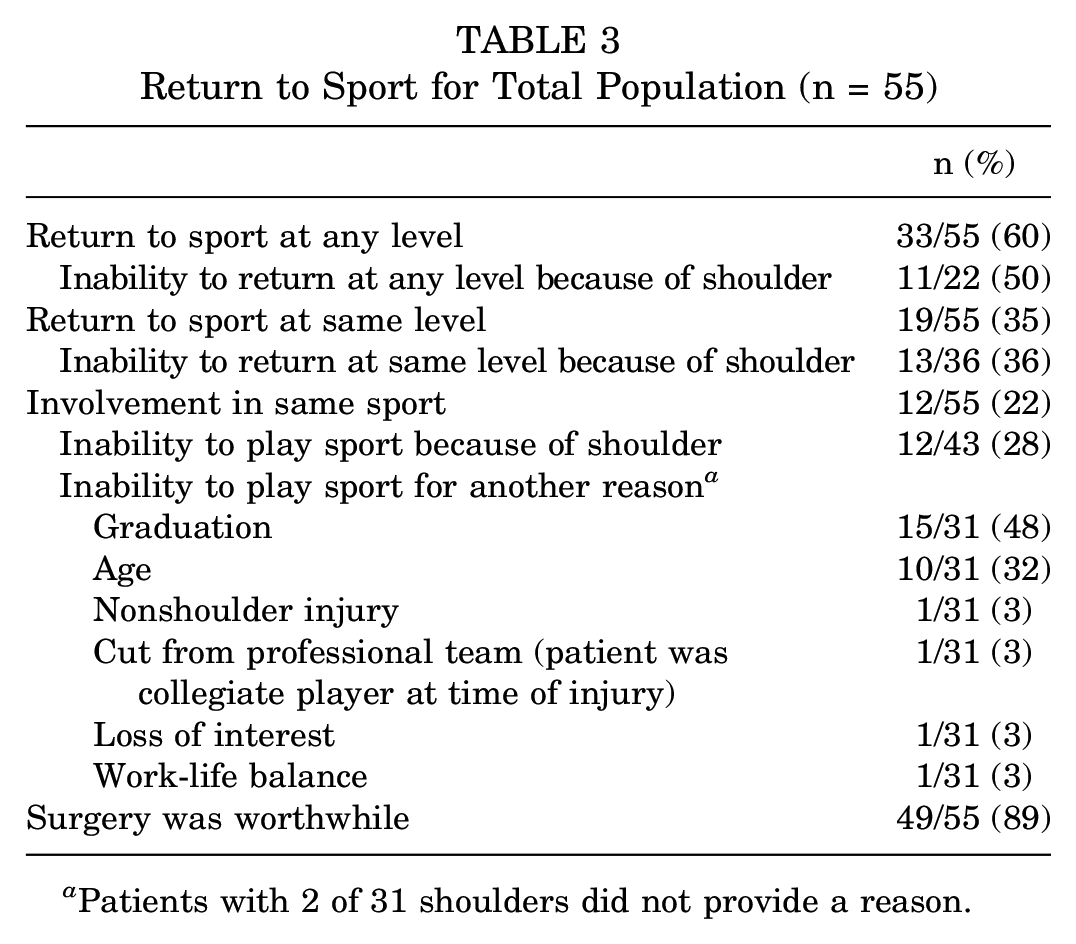
Patients with 2 of 31 shoulders did not provide a reason.
Nonthrowers Versus Throwers
Subgroup analyses comparing nonthrowing and throwing athletes revealed statistically significant improvements (P≤ .05) for both groups when comparing 15.4- and 3.0-year follow-up to preoperatively on all clinical outcome measures (Table 4). Throwers trended toward inferior preoperative ASES and KJOC scores compared with nonthrowers, but these differences did not reach statistical significance (both, P = .10). Similarly, throwers trended toward lower postoperative KJOC scores (P = .09). Nonthrowers had superior subjective strength at 3.0-year follow-up compared with throwers (P = .01), an effect not seen at long-term follow-up. Only nonthrowers experienced a reduction in subjective stability and worsening ROM at 15.4- versus 3.0-year follow-up (P≤ .05).
Outcomes for Nonthrowers (n = 31) Versus Throwers (n = 24) a
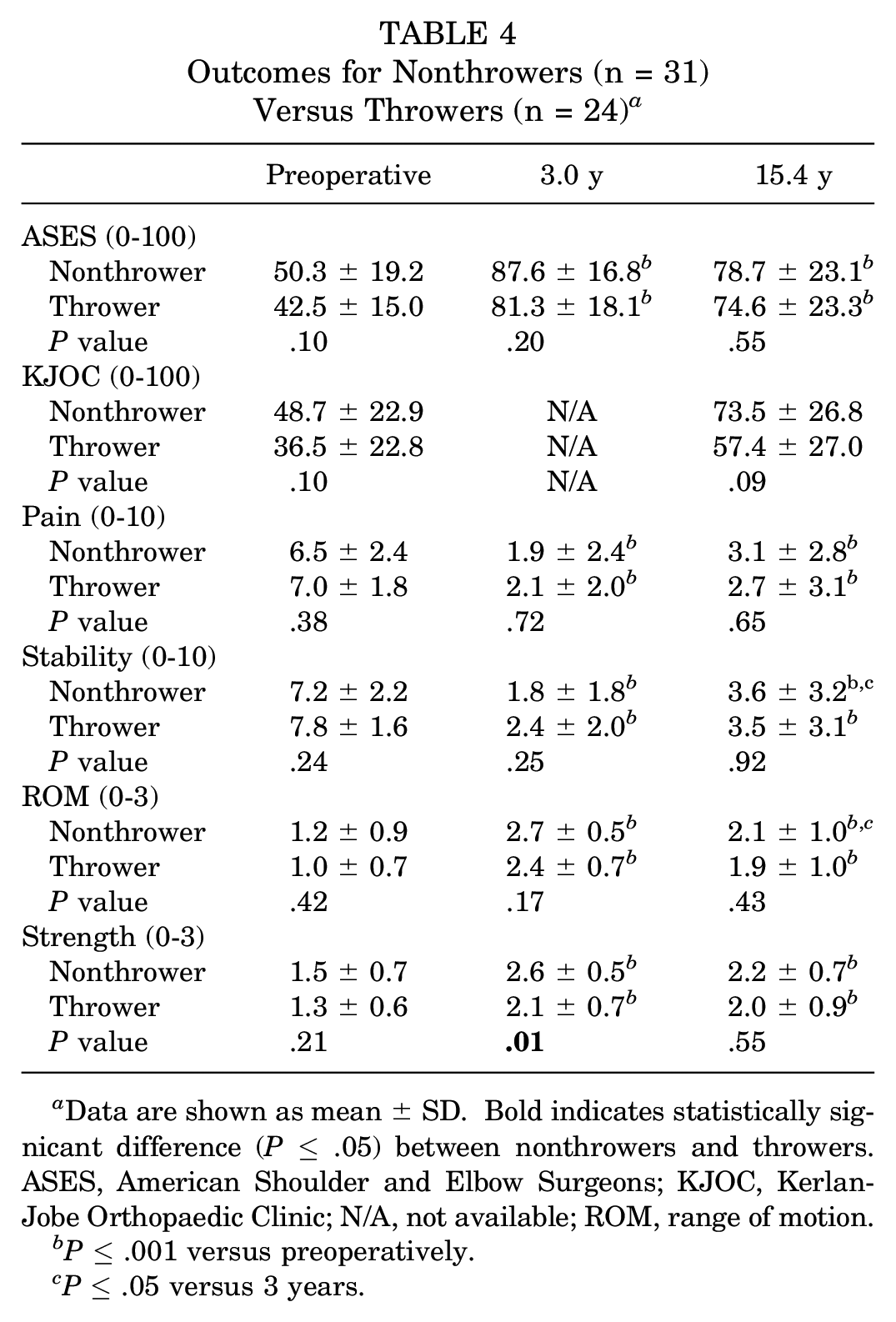
Data are shown as mean ± SD. Bold indicates statistically signicant difference (P≤ .05) between nonthrowers and throwers. ASES, American Shoulder and Elbow Surgeons; KJOC, Kerlan-Jobe Orthopaedic Clinic; N/A, not available; ROM, range of motion.
P≤ .001 versus preoperatively.
P≤ .05 versus 3 years.
Despite not achieving statistical significance, throwers returned to the same preoperative level of sport (5/24 shoulders [21%]) at less than half the rate of nonthrowers (14/31 shoulders [45%]), for whom persistent shoulder problems were the principal cause in 50% (9/18) versus 25% (4/16) of cases, respectively. Likewise, involvement in the preoperative sport occurred at a rate of only 4% (1/24 shoulders) for throwers compared with 32% (10/31 shoulders) for nonthrowers (P = .01), with throwers endorsing shoulder problems at 3 times the rate of nonthrowers (45% vs 16%, respectively). Similar but less dramatic trends were seen in the ability to RTS at any level. Despite the reduced capacity of throwers to RTS in general, nonthrowers (90% of shoulders) and throwers (88% of shoulders) found surgery equally worthwhile.
Noncontact Versus Contact Athletes
Subgroup analyses comparing noncontact and contact athletes revealed statistically significant improvements (P≤ .05) for both groups when comparing 15.4- and 3.0-year follow-up to preoperatively on all clinical outcome measures (Table 5). Contact athletes demonstrated statistically superior ASES scores (P = .007), subjective pain values (P = .03), and subjective strength values (P < .001) compared with noncontact athletes at 3.0-year follow-up, an effect lost at long-term follow-up. Contact athletes experienced statistically significant reductions in stability and strength values at long-term follow-up compared with 3.0-year follow-up, whereas noncontact athletes experienced worsening ROM over time. There were no other significant changes in outcomes within each group when comparing 15.4- versus 3.0-year follow-up. Likewise, noncontact and contact athletes returned to sport at similar rates. Surgery was similarly thought to be worthwhile for both noncontact (87% of shoulders) and contact (94% of shoulders) athletes.
Outcomes for Noncontact (n = 39) Versus Contact (n = 16) Athletes a
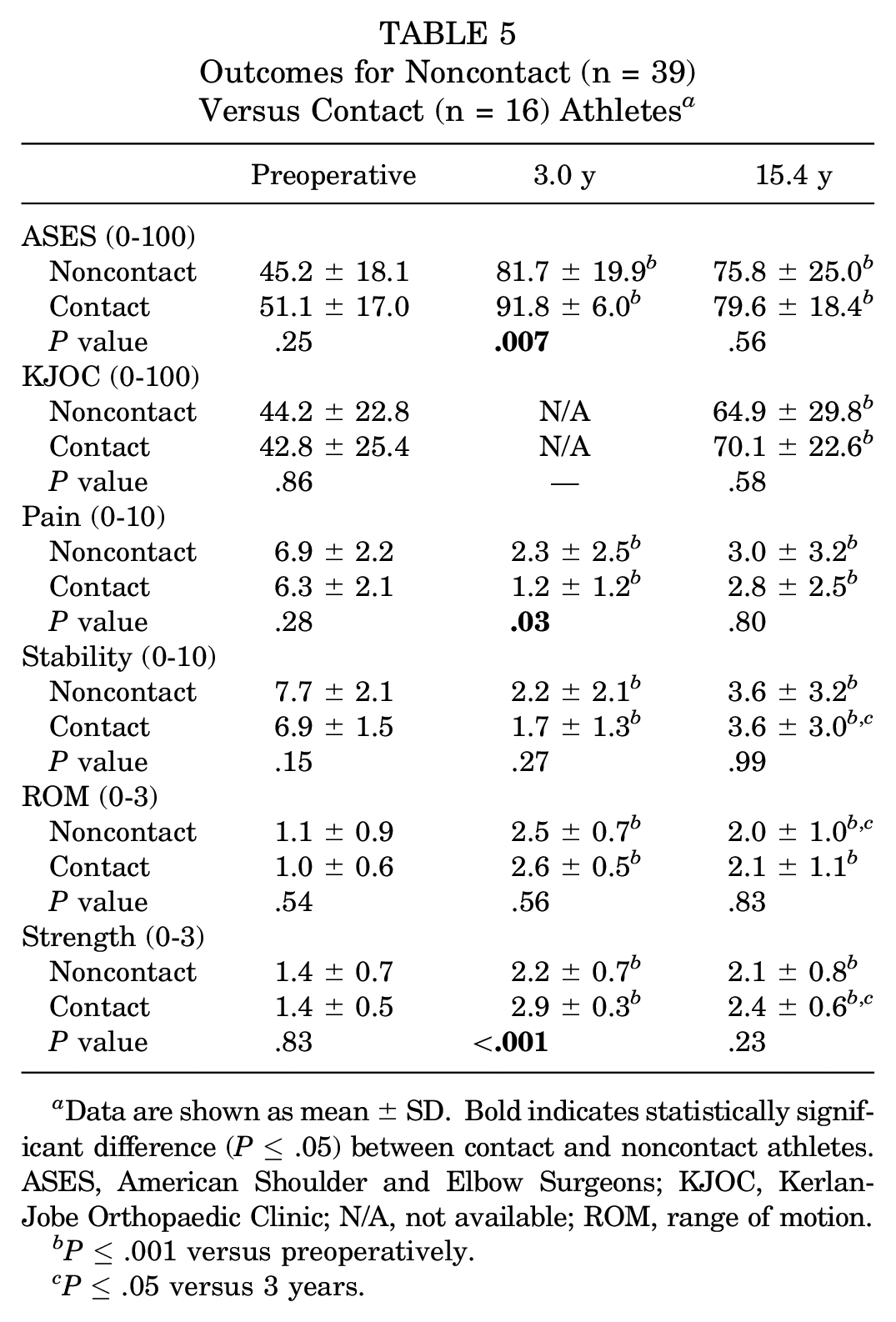
Data are shown as mean ± SD. Bold indicates statistically significant difference (P≤ .05) between contact and noncontact athletes. ASES, American Shoulder and Elbow Surgeons; KJOC, Kerlan-Jobe Orthopaedic Clinic; N/A, not available; ROM, range of motion.
P≤ .001 versus preoperatively.
P≤ .05 versus 3 years.
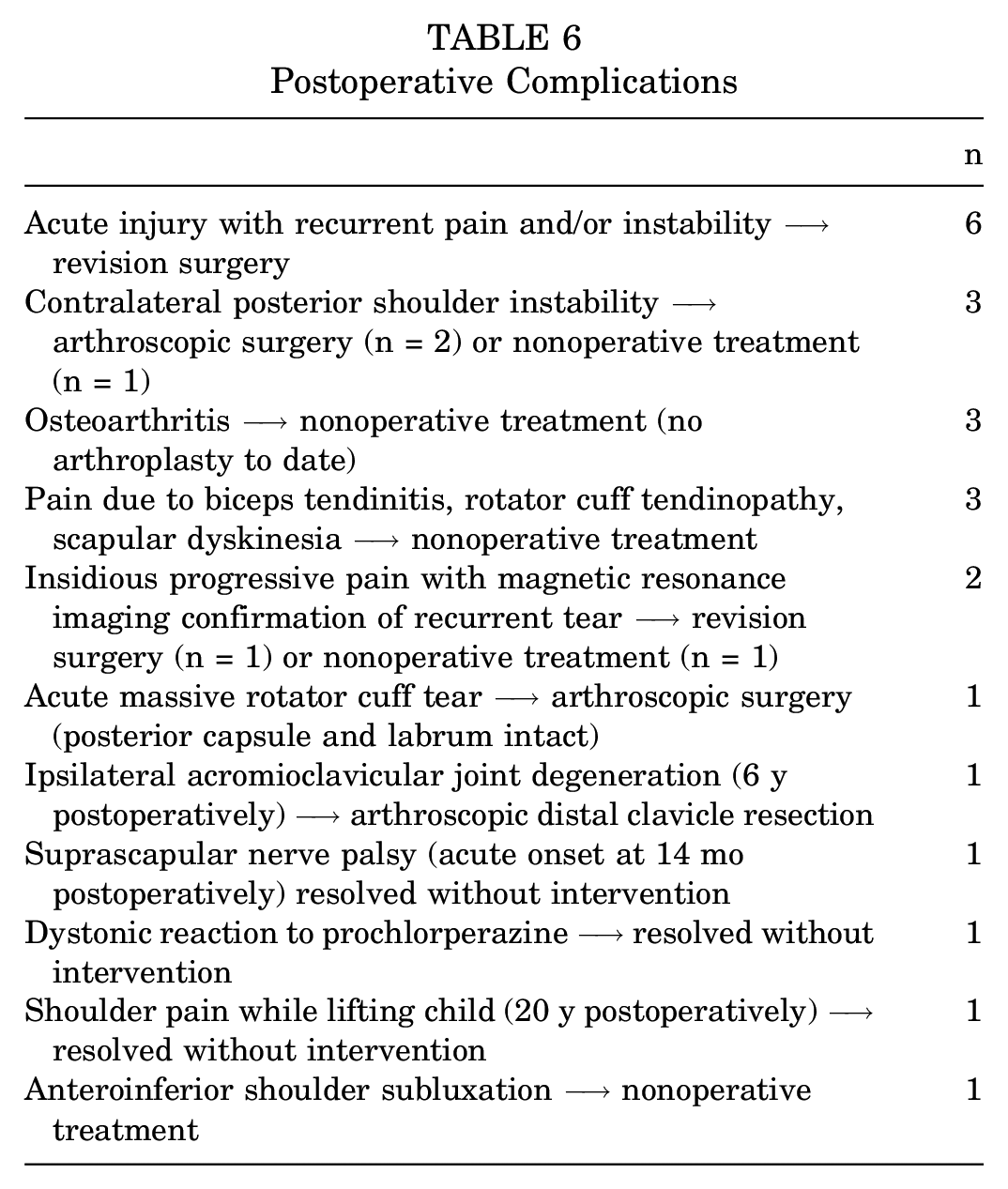
Complications
There were 23 total complications, as listed in Table 6. Notably, 6 shoulders had an acute injury in the postoperative period, for which revision surgery was performed in all 6 cases. Additionally, 2 shoulders had a progressive onset of right shoulder pain, for which repeat MRI demonstrated recurrent posterior capsulolabral tearing, with 1 shoulder undergoing revision surgery and the other shoulder undergoing nonoperative treatment. Overall, 7 of 55 shoulders (13%) underwent revision surgery. Furthermore, 3 shoulders developed posterior instability of the contralateral shoulder, with 2 treated with arthroscopic stabilization and 1 treated nonoperatively.
Postoperative Complications
Failure
With failure defined as revision surgery, an ASES score <60, or a stability value >5, 19 of 55 shoulders (35%) met failure criteria at final follow-up. Overall, 7 shoulders (13%) underwent revision surgery, 15 shoulders (27%) had a stability value >5, and 10 shoulders (18%) had an ASES score <60. Additionally, 12 shoulders (22%) met 1 criterion for failure, and 6 shoulders (11%) and 3 shoulders (5%) met 2 and 3 criteria, respectively.
Of the 7 shoulders that ultimately underwent revision surgery, 6 experienced an acute injury after index surgery, most commonly while patients were engaged in sporting activities. The lone patient who underwent revision without a recurrent acute injury reported progressively worsening pain and bilateral multidirectional instability in the likely setting of an occult connective tissue disorder not appreciated on initial presentation after an acute sporting injury. In contrast, only 4 of the remaining 12 shoulders that met failure criteria by the ASES score and/or subjective stability value reported any postoperative complication, of which only 1 patient had an acute injury in which a massive rotator cuff tear was sustained, with subsequent arthroscopic rotator cuff repair demonstrating an intact posterior capsulolabral repair site. Therefore, for all shoulders (n = 55; P < .001) and specifically those meeting failure criteria (n = 19; P = .002), an acute injury in the postoperative period was significantly associated with undergoing revision surgery.
Revision surgery was performed, on average, 3.3 years (range, 0.8-6.0 years) after primary repair. As only 4 of 7 shoulders had undergone revision surgery at the time of the earlier publication, 10 analyses comparing revision and nonrevision at 3.0-year follow-up were not included. Although shoulders that did not undergo revision surgery (n = 48) demonstrated significantly improved results on all clinical outcome measures when the long-term postoperative status was compared to the preoperative status (Table 7), revised shoulders did not exhibit long-term postoperative outcomes superior to preoperative values. However, the long-term postoperative outcomes for the ASES score, KJOC score, pain, and stability in revised shoulders were significantly improved compared with the respective outcomes after failure (before revision surgery), supporting the benefit of revision surgery (Table 7). The preoperative findings of the nonrevision and revision groups did not differ on any clinical outcome measure, whereas nonrevised shoulders were superior to revised shoulders on the ASES score, pain, stability, ROM, and strength at long-term follow-up. Despite these differences, there were no significant differences in RTS rates between the nonrevision and revision groups, which may be caused by limited statistical power afforded with a small number of patients undergoing revision surgery.
Outcomes for Nonrevision (n = 48) Versus Revision (n = 7) a
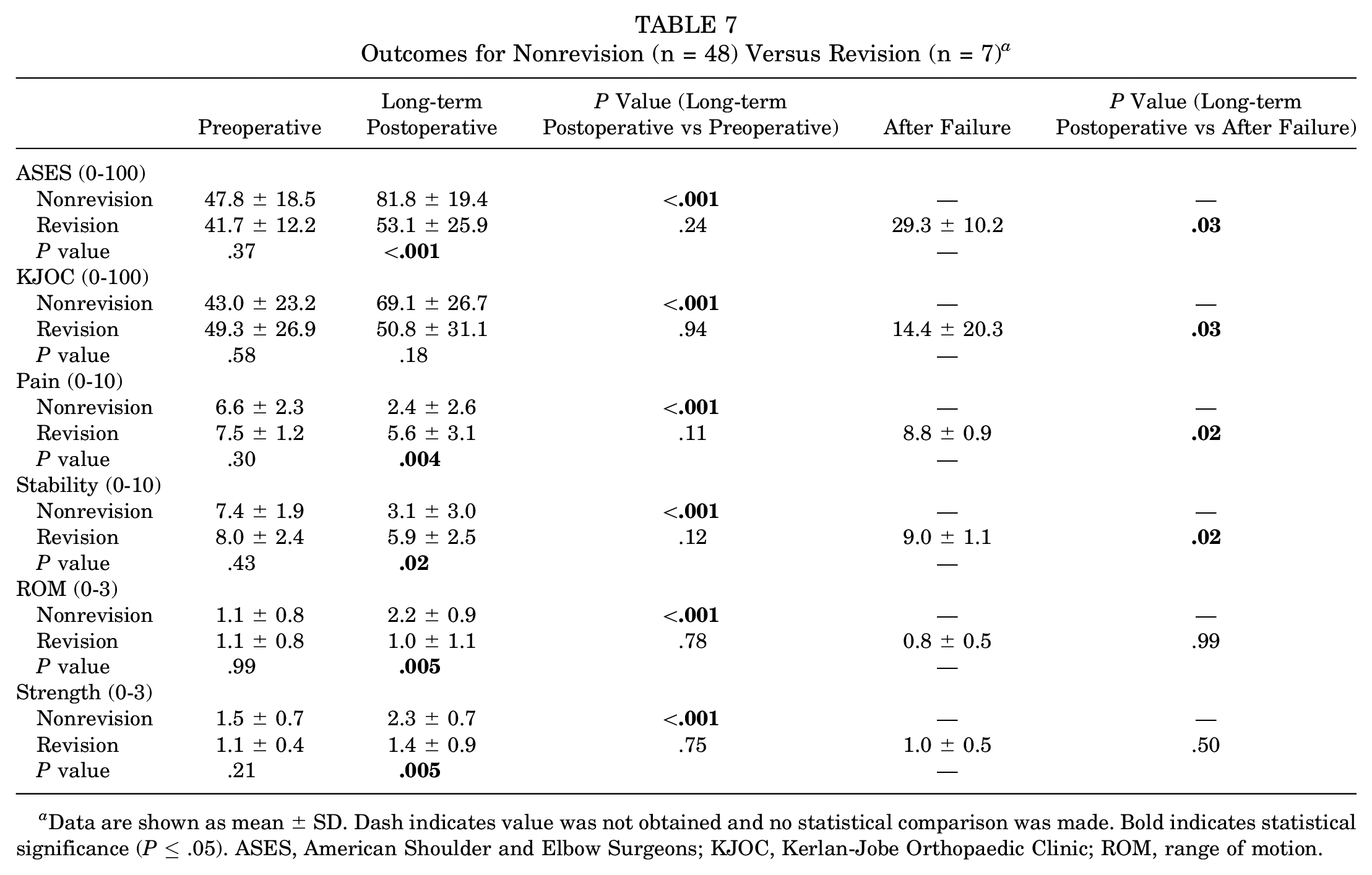
Data are shown as mean ± SD. Dash indicates value was not obtained and no statistical comparison was made. Bold indicates statistical significance (P≤ .05). ASES, American Shoulder and Elbow Surgeons; KJOC, Kerlan-Jobe Orthopaedic Clinic; ROM, range of motion.
In examining differences in glenolabral morphologies on MRI scans (Table 8), we found revised shoulders had a smaller glenoid bone width (23.7 ± 1.9 mm) compared with nonrevised shoulders (27.4 ± 3.2 mm) (P = .02), without significant differences in other measured parameters. In contrast to previously published risk factors for revision surgery, this study did not find statistically significant differences between nonrevised and revised shoulders in age, sex, follow-up time, acuity of the injury, contact sport participation, or position (ie, thrower). As noted above, an acute injury in the postoperative period was a predictor of revision surgery, although an acute injury as the initial injury mechanism (before primary surgery) was not a predictor of revision surgery.
MRI Characteristics for Nonrevision (n = 29) Versus Revision (n = 6) a
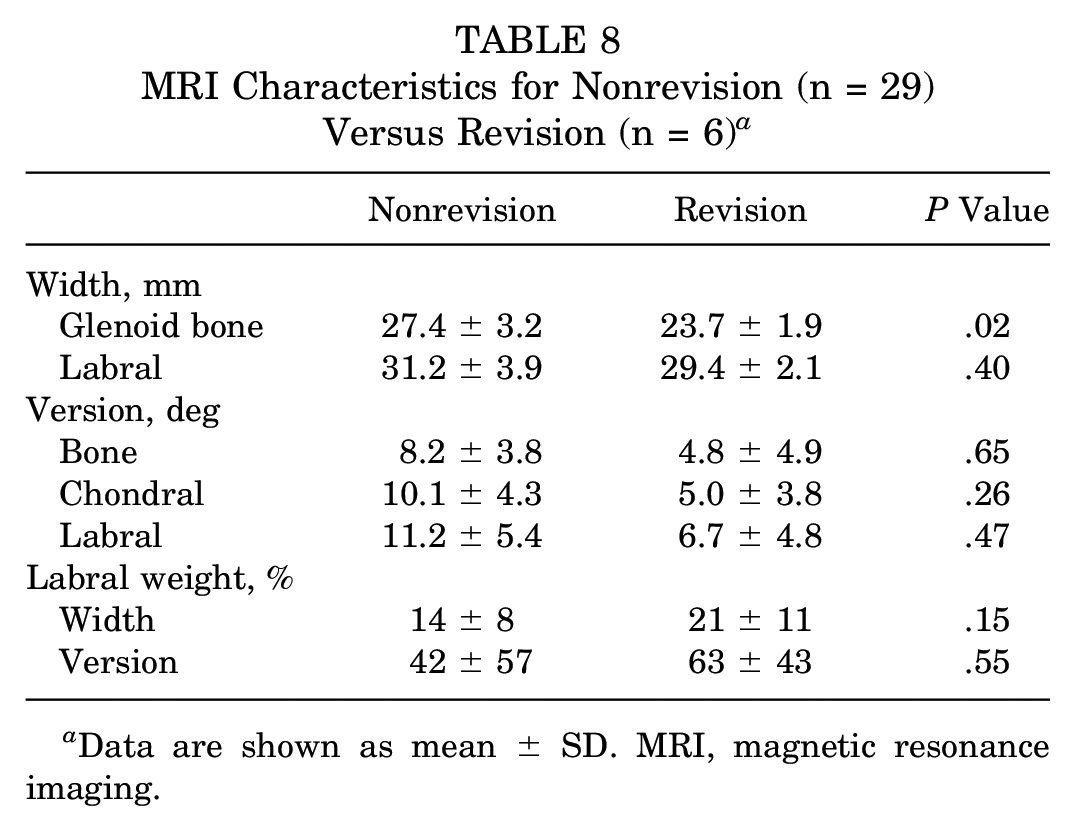
Data are shown as mean ± SD. MRI, magnetic resonance imaging.
There were no differences in the incidence of surgical findings (posterior labral tear, patulous posterior capsule, rotator cuff tear, biceps tear, general capsular laxity, capsular tear or reverse humeral avulsion of the glenohumeral ligament, cartilage injury, osteoarthritis, and reverse Hill-Sachs lesion) when comparing revised to nonrevised shoulders. Sutures, suture anchors, and the combination of sutures and suture anchors were equally employed in revised and nonrevised shoulders. When utilized, a mean of 3.8 suture anchors (range, 1-6) was used in nonrevisions compared with a mean of 3.5 suture anchors (range, 3-4) in revisions. A mean of 3.5 sutures (range, 1-7) was used in nonrevisions compared with a mean of 3.0 sutures (range, 1-5) in revisions. These differences were not statistically significant.
Discussion
This study found persistent long-term improvements in shoulder pain, stability, and function after arthroscopic capsulolabral repair for posterior shoulder instability at a mean follow-up of 15.4 years in most patients, although a notable proportion of patients met various criteria for failed repair. Athletes participating in noncontact and contact sports demonstrated similar long-term benefits from surgery on clinical outcome measures and RTS rates. Throwing athletes tended to have worse preoperative and postoperative sport-specific shoulder function, as evaluated using the KJOC score, and reduced rates of RTS compared with nonthrowing athletes, but few differences reached statistical significance. Nonthrowers had significantly superior subjective strength at 3.0-year follow-up compared with throwers, a difference not seen at final follow-up. Nonthrowers also experienced a greater loss of subjective stability and ROM between 3.0 years and final follow-up. Otherwise, outcomes at long-term (15.4-year) follow-up were generally similar to those at short-term (3.0-year) follow-up. Shoulders that underwent revision surgery were inferior to nonrevised shoulders on several clinical outcome measures at long-term follow-up but significantly improved compared with after failure but before revision. The above findings, coupled with patients deeming surgery worthwhile for approximately 90% of shoulders, which was stable from 3.0- to 15.4-year follow-up, support the use of arthroscopic capsulolabral repair for posterior shoulder instability as a durable treatment option to improve long-term shoulder pain and function and facilitate RTS in most patients.
To our knowledge, this is the first study to investigate long-term outcomes for arthroscopic repair of isolated posterior shoulder instability. Several studies have found a durable benefit to arthroscopic capsulolabral repair for anterior shoulder instability,1,25,27 but a recent meta-analysis found worse postoperative ASES scores and RTS rates in patients undergoing arthroscopic stabilization for posterior shoulder instability versus anterior shoulder instability. 24 In a related case series, Berthold et al 7 reported on the clinical outcomes of 21 patients who underwent arthroscopic repair of 270° labral tears (ie, anterior, inferior, and posterior) with a mean follow-up time of 11.9 years. Using several clinical outcome measures, including the ASES score, they found arthroscopic labral repair provided a significant improvement in the long-term postoperative shoulder status (mean ASES score, 91.8) compared with preoperatively (mean ASES score, 72.9). Additionally, the long-term postoperative score was notably similar to that in an overlapping cohort, for whom results were reported at 2-year follow-up, with a mean ASES score of 90.4. 18 RTS rates were not reported in the long-term study. 7
By comparison, this study of 55 shoulders (53 patients) found a larger gain in the ASES score (46.9 preoperatively to 77.0 long-term postoperatively; difference of 30.1) compared with Berthold et al 7 (72.9 preoperatively to 91.8 long-term postoperatively; difference of 18.9), with lower absolute scores at both time points. This parallels the findings of a systematic review and meta-analysis of studies comparing clinical outcomes after surgical repair for posterior shoulder instability in which the mean ASES score increased from 53.3 preoperatively to 89.6 postoperatively, as pooled from 7 studies. 12 The 53 patients included in the current study were recruited from the same cohort of 183 patients, for whom clinical outcomes at a mean follow-up of 3 years were previously published. 10 From that original cohort, 134 patients with a minimum follow-up of 2 years demonstrated an increase in the ASES score from 47.0 ± 18.5 preoperatively to 85.4 ± 15.8 postoperatively. These values closely parallel those of the population included in the present long-term follow-up study in which the ASES score increased from 46.9 ± 17.8 preoperatively to 83.2 ± 20.8 at a mean 3.0-year follow-up. Like Berthold et al, 7 this study largely found stable improvements in clinical outcomes comparing 15.4- and 3.0-year follow-up.
Across the included total cohort, patients with 35% of shoulders returned to sport at the preinjury level, and patients with 60% of shoulders returned to sport at some level. These rates are lower than those reported in a recent meta-analysis in which 68% of patients returned to sport at the preinjury level and 88% returned to sport at some level. 13 RTS rates reported herein were also lower than those found in overlapping studies from our group in which similar patient cohorts were investigated at shorter follow-up.9,12,23 Lower RTS rates at long-term follow-up may be expected, as patients have naturally transitioned away from sporting activities 15 years after surgery. Furthermore, the patient cohort of this study had a relatively high proportion of shoulders (44%) in throwing athletes, who have been previously found to RTS, especially at preinjury levels, at a lower rate than their nonthrowing counterparts. 12 Notably, in a related study by our group examining clinical outcomes exclusively in throwing athletes after posterior shoulder stabilization, 37% of athletes were found to RTS at preinjury levels, similar to RTS rates reported herein. 23 In this study, the majority of patients who did not RTS identified reasons other than shoulder problems as the principal deterrent. Specifically, for those unable to RTS at the same level, patients with 13 of 36 shoulders (36%) had persistent shoulder problems, and patients with 11 of 22 shoulders (50%) were unable to RTS at any level because of persistent shoulder problems. School graduation (52%) and age (34%) constituted the 2 major reasons for discontinuing sport. Despite a considerable proportion of shoulders in patients who forwent continued sport participation, 89% of shoulders were in patients who endorsed surgery as worthwhile at final follow-up, suggesting patient satisfaction with the surgical intervention.
Of the 55 total shoulders included in this study, 7 (13%) underwent revision, which is higher than the mean revision rate of 7.6% (range, 0%-33%) derived from 19 studies included in a meta-analysis of surgical stabilization for posterior shoulder instability. 12 The present revision rate is also higher than the reported rate (13/200 [7%]) in a previous larger patient cohort 10 from which our included patients were recruited and in an overlapping cohort of 297 shoulders (19 revisions [6.4%]) evaluated at a mean of 8.9 years after arthroscopic posterior capsulolabral repair. 9 With a mean time from primary to revision surgery of 3.3 years (range, 0.8-6.0 years) in the 7 revised shoulders found herein, it is likely that the higher revision rate of this cohort was caused by late revisions not captured in studies with an earlier follow-up. Notably, only 4 of 7 shoulders in this study had undergone revision surgery at the time of short-term follow-up in our earlier study. 10 Beyond capturing new revisions at longer time points, it is also a reasonable conjecture that patients with poorer outcomes, including complications and revisions, were more successfully recruited for follow-up, given a longer standing relationship with the senior author, contributing to the higher revision rate. That is, patients with highly successful outcomes without postoperative complications may be less inclined to participate in long-term follow-up. This study included throwing athletes, who were previously reported to undergo revision surgery at higher rates compared with other patient populations. 23 Nevertheless, neither sport type (ie, noncontact vs contact) nor position (ie, nonthrower vs thrower) was a significant risk factor for revision surgery. Similarly, previously identified risk factors for revision surgery, including female sex and dominant shoulder, 9 were not found to be risk factors in this study. On the other hand, an acute injury in the postoperative period was a predictor of revision surgery, although an acute injury as the initial injury mechanism (before primary surgery) was not a significant predictor of revision surgery.
Analysis of glenolabral morphologies on MRI scans found a smaller glenoid bone width to be a significant risk factor for revision surgery, as previously reported.9,12,17 A recent study identified even small amounts of glenoid bone loss as a risk factor for surgical failure. 4 No included patient demonstrated appreciable bone loss on preoperative MRI scans or the intraoperative evaluation, but the improved resolution of contemporary MRI and a heightened appreciation for even subtle bone loss may have identified occult bone loss if imaging were repeated today. Although other authors have found increased glenoid retroversion to be a risk factor for primary and recurrent posterior shoulder instability, bone, chondral, and labral version were not risk factors in this study or in similar studies from our research group.9,17,23 We and others have also found concomitant shoulder abnormalities (eg, rotator cuff injury), the use of ≤3 suture anchors, and the use of plication sutures alone to be risk factors for revision surgery and poorer outcomes.5,9,12,20,21 A review of operative reports found few cases of concurrent abnormalities, and the majority of repairs being performed were with suture anchors. Nevertheless, there were no predictors of revision surgery from the investigated surgical findings in this study.
Clinical failure, defined as revision surgery, an ASES score <60, or a stability value >5, was seen in 19 of 55 shoulders (35%). As noted, 7 shoulders (13%) underwent revision surgery, 15 shoulders (27%) had a stability value >5, and 10 shoulders (18%) had an ASES score <60 in the current study. These rates are higher than those in the larger cohort study with a 36-month follow-up in which 7% of shoulders underwent revision surgery, 7% had a stability value >5, and 6% had an ASES score <60. 10 The discrepancy in clinical failure rates between the past and present studies is likely attributable to similar reasons offered above regarding the increased revision rate seen in the current study. Furthermore, the senior author has transitioned from traditional knotted fixation for labral repair to knotless suture anchor fixation, as the latter was found to require less revision surgery and had higher RTS rates, ASES scores, and KJOC scores. 11 A high percentage of patients included in this study underwent labral repair with traditional knotted fixation, potentially contributing to the noted failure rate.
This study was not without several limitations. A considerable proportion of the original patient cohort was lost to follow-up, with only 53 patients (55 shoulders) of the original 183-patient (200-shoulder) cohort participating. Telephone and/or mail were the only permissible means of initial recruitment, with 119 of 183 patients (65%) unable to be reached by either form of communication. As the majority of the patient population was young (ie, high school or college students) and otherwise healthy at the time of surgery, it could be expected that patient recruitment would be difficult, as past contact information was often obsolete. With a small sample size, further divided by subgroup analyses, statistical tests may have been underpowered at times, especially in the context of rare frequency events (eg, revision surgery). Power analyses were not performed, as the intention was to retrospectively recruit as many patients as possible from the initial cohort of 183 patients (200 shoulders) in whom short-term outcomes were previously reported. 10 Therefore, the absence of statistically significant differences between groups suggests similarities in outcomes but should not be considered proof of statistical equivalence or noninferiority. Despite these limitations, to our knowledge, this constitutes the largest and longest follow-up of clinical outcomes after arthroscopic capsulolabral repair for isolated posterior shoulder instability. Furthermore, a direct comparison of clinical outcomes at long-term (15.4-year) follow-up with short-term (3.0-year) follow-up demonstrated largely stable improvements in the shoulder status compared with preoperatively.3,8-10 Nevertheless, the included outcome measures were largely subjective (ie, self-reported), with only a few objective measures. This permitted a comparison of long-term (15.4-year) outcomes with short-term (3.0-year) outcomes but entails limitations inherent in subjective outcome measures, such as recall bias.
As noted by Delong et al 12 in a systematic review and meta-analysis of studies on surgical stabilization for posterior shoulder instability, numerous clinical outcome measures have been previously used, as there is no consensus on the optimal outcome measure(s) to employ. The ASES score has been most used across related studies. Therefore, its use in the current study does permit comparisons across author groups. Furthermore, it has been recognized that commonly used clinical outcome measures for shoulder instability fail to adequately discern gradations of function in the throwing shoulder,12,13 for which we have begun using the KJOC score. Unfortunately, KJOC scores were not previously collected at 3.0-year follow-up, limiting direct comparisons between long-term postoperative and earlier findings. Future studies from our research group will seek to address the above limitations, and a greater consensus among researchers of posterior shoulder instability on what constitutes the best constellation of outcome measures is additionally needed to facilitate a comparison of outcomes across publications.
Conclusion
Arthroscopic capsulolabral repair for posterior shoulder instability was a durable treatment option that improved long-term shoulder pain and function and facilitated RTS in the majority of patients, although a notable proportion of patients met various criteria for failure. Athletes participating in noncontact and contact sports can expect similar long-term benefits from surgery, with equivalent scores on clinical outcome measures and RTS rates. Conversely, throwing athletes may expect worse preoperative and postoperative sport-specific shoulder function and reduced rates of RTS compared with nonthrowing athletes. Measuring RTS success remains challenging, especially at long-term follow-up, as many athletes change sporting activities for reasons other than persistent shoulder problems, such as graduation or life transitions with increasing age.
Footnotes
Submitted October 3, 2022; accepted February 2, 2023.
Presented at the interim meeting of the AOSSM, Chicago, Illinois, March 2022.
One or more of the authors has declared the following potential conflict of interest or source of funding: B.B.R. has received support for education from Mid-Atlantic Surgical Systems. J.W.A. has received grants from Arthrex and DJO and hospitality payments from Mid-Atlantic Surgical Systems and Smith+Nephew. J.P.B. has received consulting fees from DJO, support for education from Fones Marketing Management, and compensation for services other than consulting from Arthrex. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.