
Abstract
Background:
The adductor tubercle of the distal femur is utilized by surgeons as an anatomic landmark to identify graft anchor placement during medial patellofemoral ligament (MPFL) and medial quadriceps tendon femoral ligament (MQTFL) reconstruction for patellofemoral instability. In the skeletally immature population, its location relative to the physis has not been well defined.
Purpose:
To identify the location of the adductor tubercle relative to the distal femoral physis in skeletally immature individuals and gain insight regarding optimal graft anchor placement for pediatric patients undergoing MPFL and MQTFL reconstruction.
Study Design:
Descriptive laboratory study.
Methods:
Thin-cut computed tomography scans of 37 male cadaveric specimens (age, 4-16 years) were obtained from the New Mexico Decedent Image Database. A measurement protocol to identify the adductor tubercle was created with guidance from a fellowship-trained musculoskeletal radiologist. By utilizing axial, coronal, and sagittal views of knee computed tomography scans, the adductor magnus tendon was identified and followed distally to its insertion (adductor tubercle) on the distal femur. Distance from the midpoint of the adductor magnus tendon insertion relative to the physis in the proximal-distal orientation was measured. The anterior-posterior distance of the midpoint tendon insertion relative to the posterior femoral cortex line was also evaluated.
Results:
The midpoint of the adductor magnus tendon was at the physis in 30 specimens. One 8-year-old cadaveric specimen had an insertion 1.1 mm distal to the physis. In all specimens ≥15 years old (n = 6), the adductor magnus tendon insertion was distal to the physis with a mean distance of 2.73 mm. The location of the adductor tubercle was always posterior (mean, 5.1 mm) with respect to the posterior femoral cortex line.
Conclusion:
The location of the adductor tubercle in male pediatric patients is likely at or distal to the physis. Thus, the findings of this study directly conflict with previous studies that suggested a more proximal location.
Clinical Relevance:
Optimal graft anchor placement during MPFL and MQTFL reconstruction in the skeletally immature patient can be challenging because of the variability reported in previous studies of the medial patellofemoral complex origin relative to the physis. This study suggests that distal—rather than proximal—graft anchor placement might better help restore patellofemoral isometry.
Keywords
Patellofemoral instability is associated with significant pain, patellofemoral arthritis, and disability. 1 In the pediatric population, the average age range of presentation is between 10 and 16 years. 17 However, patients with neuromuscular and hyperlaxity disorders may present even earlier owing to muscle imbalance, laxity, weakness, and knee joint dyskinesia that potentially increase their risk of patellar dislocation and instability. 10 Thus, patellofemoral instability affects a wide range of pediatric patients, and recurrent dislocations often lead to the need for surgery.
Medial patellofemoral ligament (MPFL) reconstruction has been widely adopted and used to treat patellofemoral instability with favorable functional outcomes. 9 More recently, medial quadriceps tendon femoral ligament (MQTFL) reconstruction has become popular, as it avoids patellar drilling and may more closely restore native resistance to lateral translation.5,15 However, in the skeletally immature patient undergoing either procedure, careful attention must be paid during graft anchor placement to avoid iatrogenic injury to the distal femoral physis while optimizing patellofemoral isometry. Thus, anatomic knowledge of the adductor tubercle relative to the physis is instrumental when performing MPFL and MQTFL reconstruction in the skeletally immature patient with recurrent patellofemoral instability. 16 Poor patellofemoral isometry is associated with worse functional outcomes. 9
The MPFL and MQTFL are part of the MPFL complex (MPFC), which originates between the adductor tubercle and medial epicondyle of the distal femur, with the MQTFL fibers being more proximal (Figure 1). Studies investigating the location of the MPFL relative to the physis have reported variable results. In a cadaveric study by Farrow et al, 3 the origin of the MPFL was determined to be distal to the physis. In a follow-up cadaveric and radiographic study, Shea et al 12 determined the MPFL origin to be more proximal and anterior in specimens ≥7 years of age, whereas in specimens <7 years old, the origin was more distal and posterior to the physis. It is unclear why there has been such variability among studies investigating this topic.
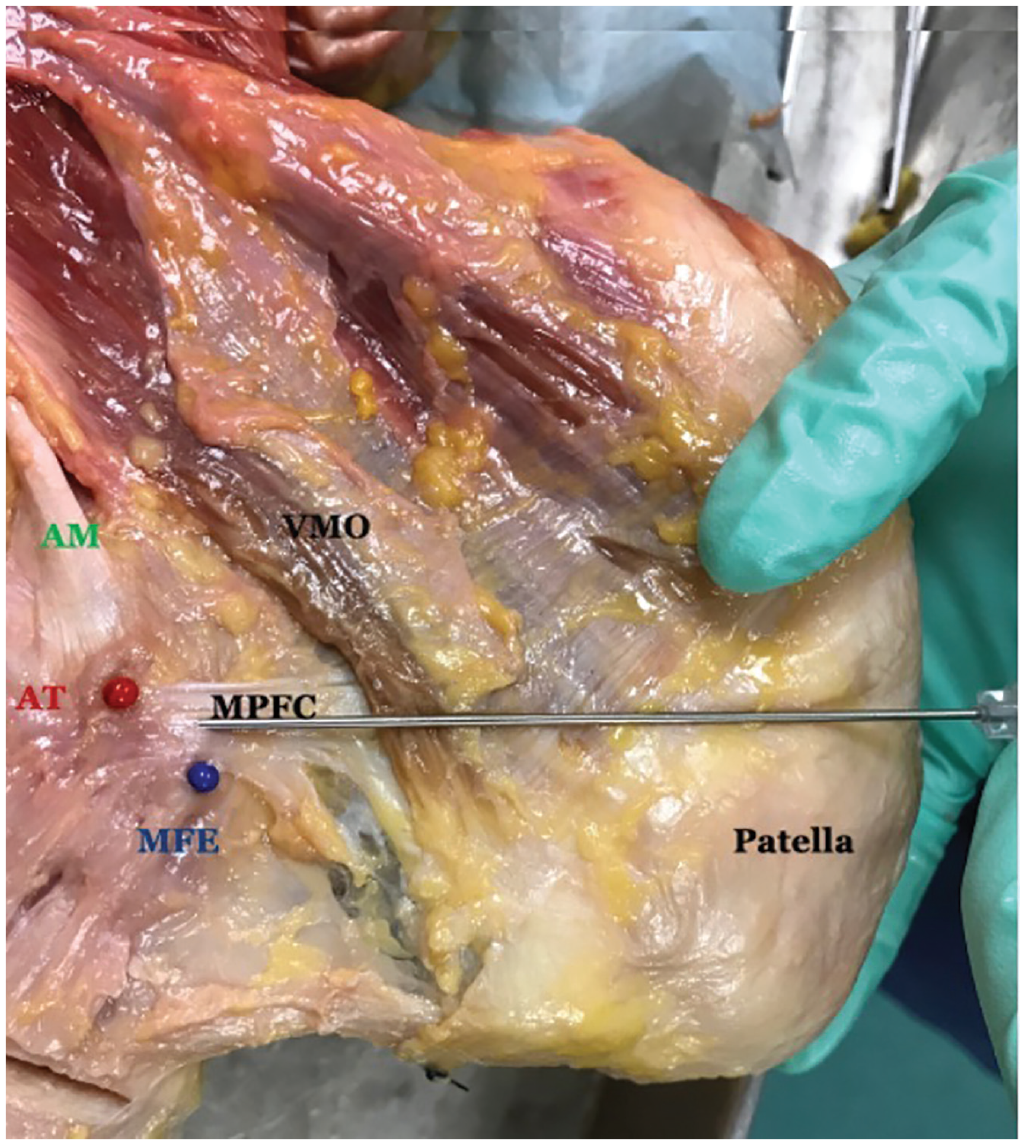
Adult cadaveric specimen demonstrating the adductor magnus tendon (AM), adductor tubercle (AT), medial femoral epicondyle (MFE), and the medial patellofemoral complex (MPFC) origin, made up of medial quadriceps tendon femoral ligament fibers proximally and medial patellofemoral ligament fibers distally. VMO, vastus medialis oblique. Courtesy of Dr John Fulkerson.
The adductor tubercle is an important anatomic landmark for identifying graft anchor placement during MPFL and MQTFL reconstruction. However, its exact location in relation to the physis has not been well defined. This anatomic study aims to identify the location of the adductor tubercle relative to the distal femoral physis as a function of age in the skeletally immature population to gain insight regarding optimal graft anchor placement in pediatric patients undergoing MPFL and MQTFL reconstruction.
Methods
Our study protocol was reviewed by the University of New Mexico research committee, and use of cadaveric computed tomography (CT) scans was approved. The University of New Mexico has determined that the data contained in the New Mexico Decedent Image Database are not subject to human participants review, and institutional review board approval was waived.
Male cadaveric specimens 4 to 16 years of age with available lower extremity CT scans from the New Mexico Decedent Image Database were included in this study. 2 Exclusion criteria included traumatic knee injury, knee deformity, previous knee surgery, and skeletal dysplasia. Exclusion criteria were applied by reviewing cadaveric cause-of-death reports as well as by evaluating CT scans for any bony abnormality.
In total, 37 male cadaveric specimens with CT scans of 1-mm slices and 0.5 mm of overlap were identified. Unfortunately, magnetic resonance imaging, which would provide more soft tissue detail, was not available for these cadavers. Nevertheless, CT scans, which are typically not used for soft tissue detail, are excellent for identifying tendons. 11 Given that the adductor magnus tendon is known to insert at the adductor tubercle on the distal femur, the adductor tubercle can be identified by following this tendon distally to its insertion.
OsiriX MD (Version 13.0) software was utilized for this study, as it is certified software for use in clinical medicine and offers advanced postprocessing techniques in 2 and 3 dimensions with the ability for volume rendering to evaluate soft tissue structures in addition to bony anatomy. A measurement protocol to identify the adductor tubercle was created under the guidance of a fellowship-trained musculoskeletal radiologist. All measurements were performed by orthopaedic surgeons (S.S.J. and D.C.) and later confirmed by the senior author (D.B.F.). The transepicondylar axis of the distal femur was identified on the axial view (Figure 2A). Next, by using the soft tissue window, we identified the adductor magnus muscle medial to the gracilis muscle, posterior to the adductor longus muscle, and anterior to the semimembranosus and semitendinosus muscles (Figure 2B). The adductor magnus muscle and tendon were identified and followed distally (Figure 2, C and D). The most distal aspect of the tendon at its midpoint was marked to identify the adductor tubercle (Figure 2E). This point was adjusted on coronal and sagittal views to accurately label the adductor tubercle in 3-dimensional space. Volume rendering of the CT scans with a focus on soft tissue as well as bony anatomy was then performed to obtain 3-dimensional imaging of the adductor magnus muscle, tendon, and adductor tubercle (Figure 3). The distance from the adductor tubercle to the most proximal aspect of the distal femoral physis was measured on the coronal view. A value of 0 was given if the point was at the physis proximally, centrally, or distally (Figure 4). A negative value was recorded if the insertion was clearly proximal to the physis, and a positive value was recorded if the insertion was clearly distal to the physis.
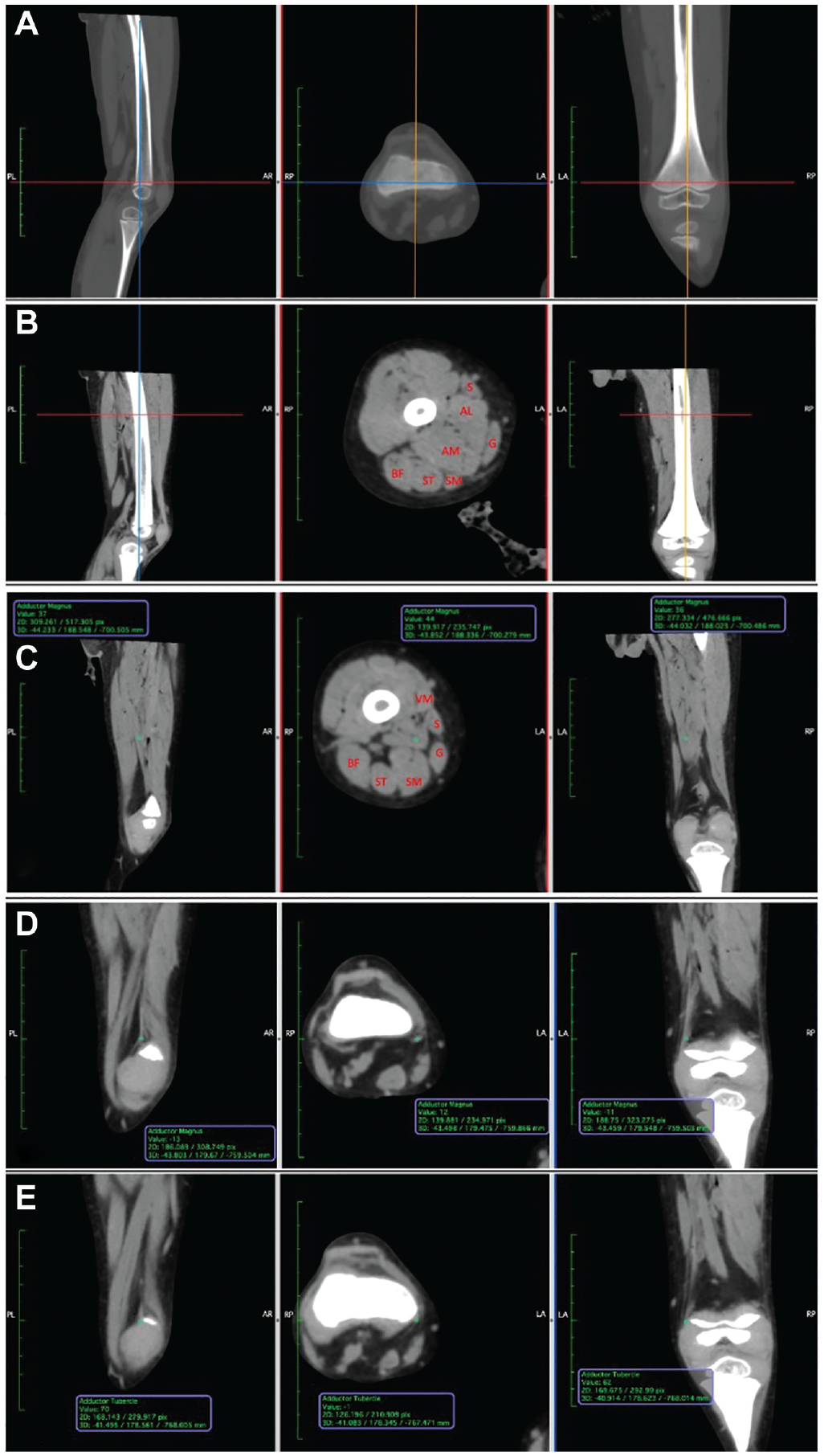
Computed tomography scans of the right knee of a 4-year-old cadaveric specimen including sagittal, axial, and coronal cuts: (A) the transepicondylar line in blue, (B) axial cross-sectional anatomy, (C, D) adductor magnus muscle identified in green and followed distally to its tendon, and (E) the region of the adductor tubercle relative to the physis. AL, adductor longus; AM, adductor magnus; BF, biceps femoris; G, gracilis; S, sartorius; SM, semimembranosus; ST, semitendinosus; VM, vastus medialis.
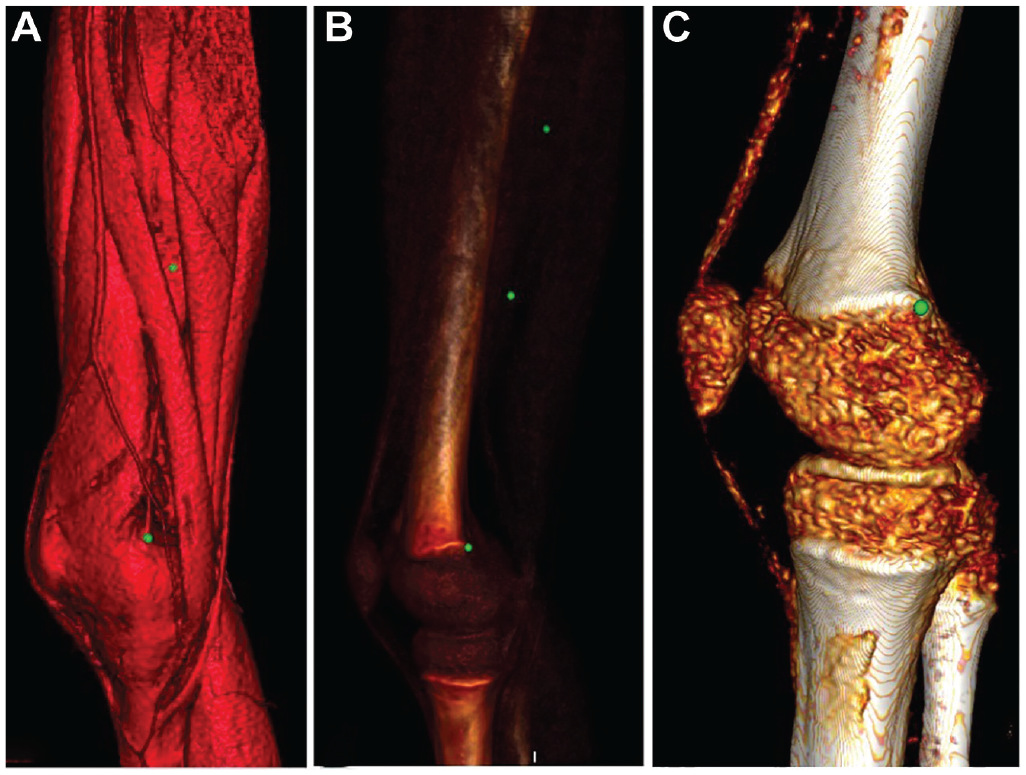
Three-dimensional computed tomography imaging of the right knee of a 4-year-old cadaveric specimen after volume rendering for soft tissue. The green marker identifies (A, B) the adductor magnus muscle, which is followed distally to its tendon, and (C) the region of the adductor tubercle.
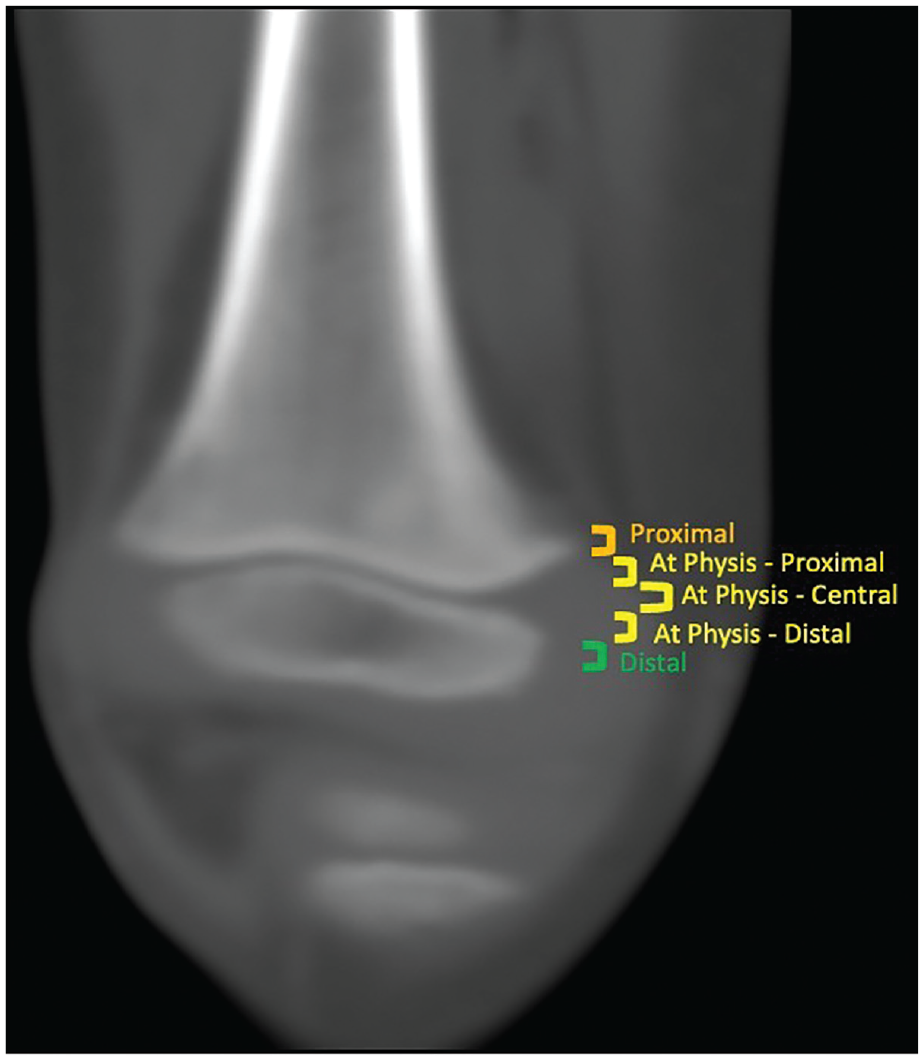
Classification of adductor magnus tendon insertion at the region of the adductor tubercle as proximal to the physis, at the physis (proximal, central, or distal), or distal to the physis.
On the sagittal view, the proximity of the adductor tubercle to the line of the posterior femoral cortex (PFC; a fluoroscopic landmark often used intraoperatively) was also measured to determine the anterior-posterior orientation (Figure 5). A negative value was recorded for measurements posterior to the PFC and a positive value recorded for measurements anterior to the PFC.
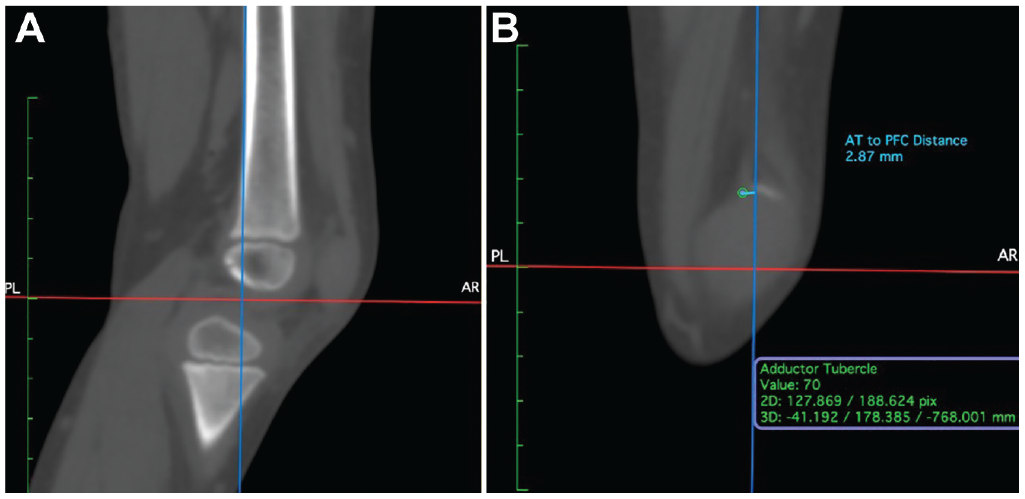
Computed tomography scans of the right knee of a 4-year-old cadaveric specimen with sagittal views identifying (A) the posterior femoral cortex (PFC) line in blue and (B) the distance from the adductor tubercle (AT) to the PFC.
Statistical Analysis
Descriptive analysis of the midpoint of the adductor magnus tendon was recorded. The distance (in mm) from the physis (proximal, distal, or at the physis) was reported for each cadaveric specimen, and the mean and standard deviation were described. Similarly, the proximity from the PFC (in mm) was described using mean and standard deviation.
Even though the primary objective of this study was to describe the anatomic location of the adductor tubercle relative to the physis, a secondary post hoc analysis was performed to relate distance to age. After the data had been compiled, a noticeable difference in distance from the physis was observed after the age of 15 years. Thus, a post hoc analysis was performed to compare the mean distance from the physis between those <15 and ≥15 years old. A Welch t test was used, as the standard deviation between the samples was not assumed to be equal. Alpha was set at .05 and beta set at 0.20. P < .05 was considered significant.
The distance to the PFC was secondarily analyzed. Given the similarity in standard deviations between those aged <15 and ≥15 years, the Student t test was utilized to compare means. Alpha was set at .05 and beta set at 0.20. P < .05 was considered significant.
Because these analyses were performed post hoc and were not the primary focus of the study, a priori power analyses were not performed before data collection. However, post hoc power analyses were reported to provide insight into any nonsignificant results. Statistical Package for the Social Sciences (SPSS; Version 28; Armonk, NY) software was used for statistical analysis.
Results
The midpoint of the adductor magnus tendon was found at the physis in 81% of cadaveric specimens (n = 30), 14 of which had the midpoint at the proximal aspect of the physis. Twelve specimens had insertions centrally, and 4 had an insertion point noted at the distal aspect of the physis (Table 1). The mean distance from the physis was 0.47 mm distally (SD, 1.35 mm). One 8-year-old specimen had an insertion 1.1 mm distal to the physis. In all specimens ≥15 years old (n = 6), the insertion of the adductor magnus tendon was distal to the physis with a mean distance of 2.73 mm (SD, 2.37 mm) (Figure 6). Those aged <15 years (n = 31) had a mean distance to the physis of 0.04 mm (SD, 0.20 mm). On Welch t test, the mean difference between these groups was significant (P = .038) (Table 2). No specimens had an adductor magnus tendon insertion that was clearly proximal to the physis.
Adductor Magnus Tendon Insertion Relative to the Distal Femoral Physis and Proximal Femoral Cortex Line
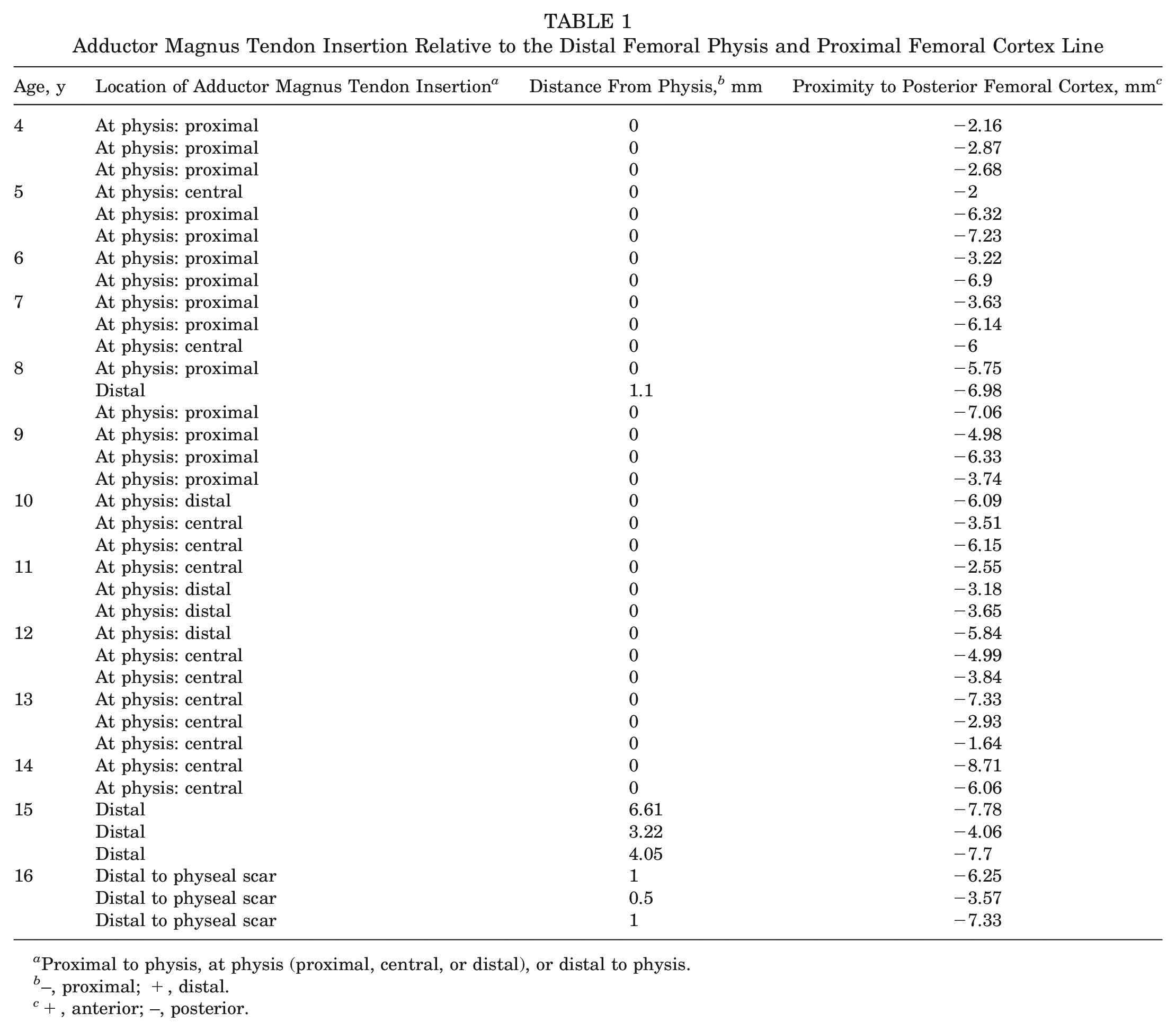
Proximal to physis, at physis (proximal, central, or distal), or distal to physis.
–, proximal; +, distal.
+, anterior; –, posterior.
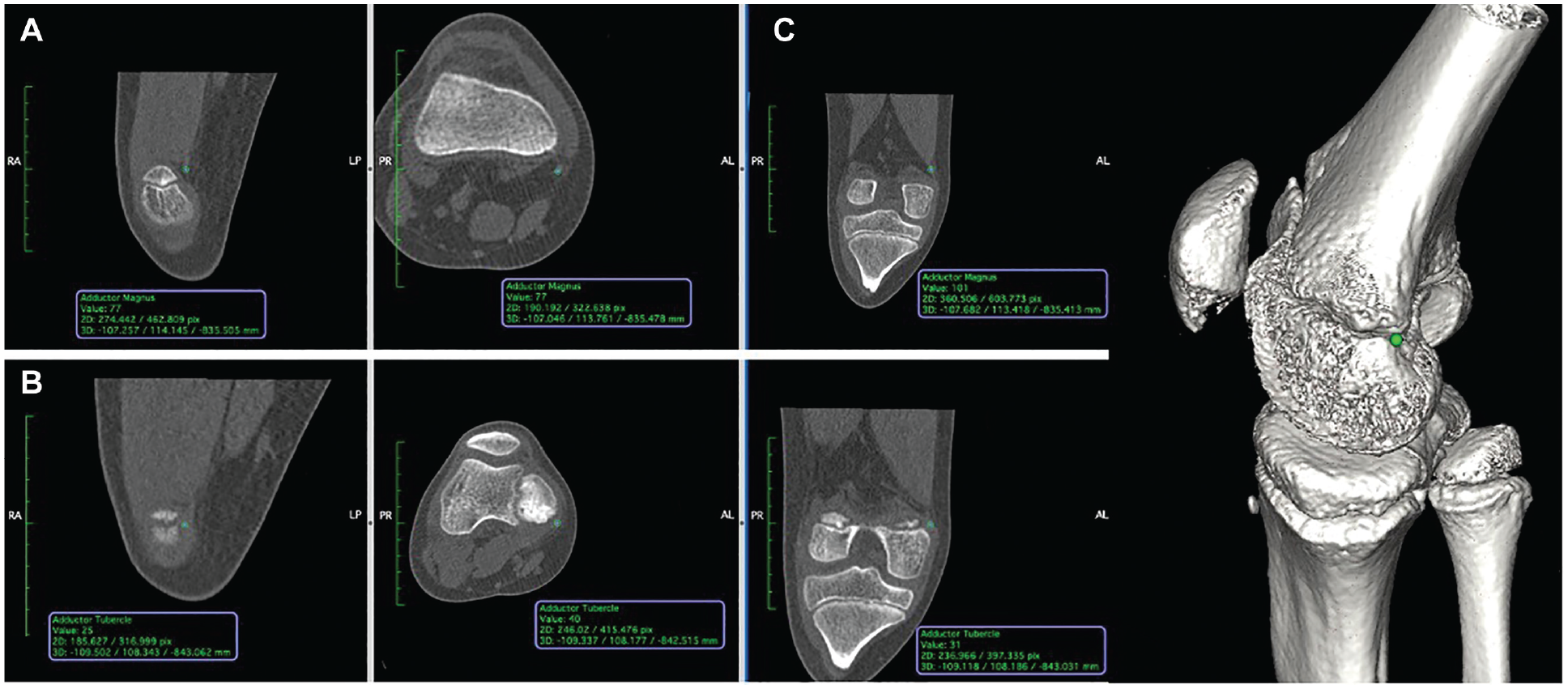
Computed tomography scans of the right knee of an 11-year-old cadaveric specimen including sagittal, axial, and coronal cuts identifies (A) the adductor magnus tendon with (B) the adductor tubercle localizing at the distal aspect of the physis. (C) Three-dimensional imaging illustrates the region of the adductor magnus tendon insertion at the adductor tubercle relative to the physis.
Comparisons of Mean Distance From the Adductor Magnus Tendon Insertion to the Distal Femoral Physis and PFC Line a
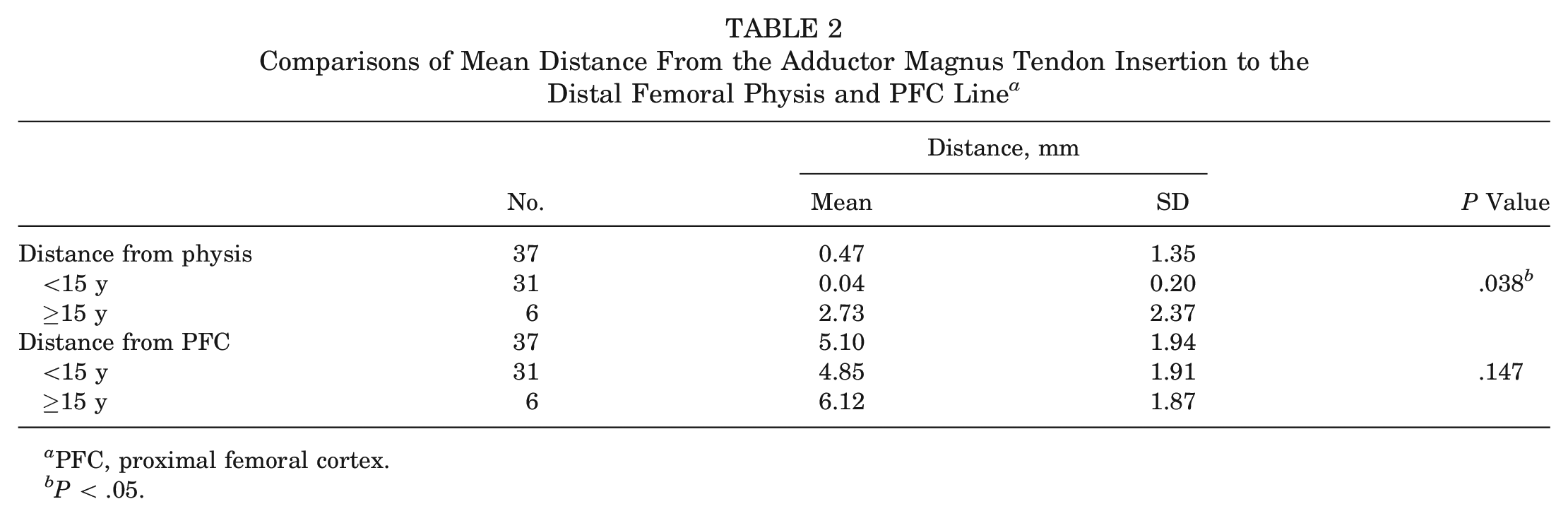
PFC, proximal femoral cortex.
P < .05.
Regarding the relationship of the midpoint of the adductor magnus tendon insertion with the PFC line, the location was always posterior and averaged 5.1 mm (SD, 1.94 mm) (Table 2). In specimens ≥15 years old, the mean distance from the PFC line was 6.12 mm (SD, 1.87 mm), and in those <15 years old, the mean was 4.85 mm (SD, 1.91 mm). These 2 means were not significantly different on Student t test (P = .147). On post hoc power analysis, the a priori power was low (0.193); thus, this study was underpowered to detect a difference in distance to the PFC line based on age.
Discussion
Identification of the adductor tubercle location is critical for anatomic reconstruction of the MPFC in pediatric patients undergoing patellofemoral reconstruction. Previous studies have demonstrated variable results when it comes to the MPFC origin with respect to the distal femoral physis. The location has been reported to be proximal, at, or distal to the physis.7,8
Our study utilized thin-cut high-quality CT scans of cadaveric specimens to directly follow the adductor magnus tendon to its insertion on the adductor tubercle. We found that the adductor tubercle was always at or distal to the physis. Thus, given that the MPFC is known to be distal to the adductor tubercle, it is reasonable to conclude that it is also likely at or distal to the physis and unlikely proximal.
In a cadaveric study by Shea et al, 13 5 of 6 pediatric cadaveric specimens had the central aspect of the MPFL footprint insert distal to the physis, and 1 specimen had an insertion at the physis. Kepler et al 6 found the anatomic insertion of the MPFL origin on magnetic resonance imaging scans to be distal to the physis in 93% of their study population, which included children and adolescents with acute patellar dislocation. In a cadaveric study by Farrow et al 3 as well as a systematic review, 14 the origin of the MPFL was determined to be distal to the physis in all specimens. Thus, these findings are congruent with our findings.
However, other studies reported variable findings. In a follow-up study by Shea et al, 12 13 of 36 pediatric cadaveric specimens had MPFL origins proximal to the distal femoral physis. The authors also suggested the origin changes as a function of age with a more proximal and anterior location in specimens ≥7 years of age versus more distal and posterior in those <7 years old. Our study did not note any significant difference of the adductor tubercle location as a function of age around 7 years. Yet, we did find that specimens ≥15 years old were more likely to have the adductor tubercle located distal to the physis. The adductor tubercle was also found to be posterior with respect to the PFC in all specimens, regardless of age, but based on the post hoc power analysis and a priori power of 0.193, the study was determined to be underpowered to detect a difference in distance to the PFC line based on age. Overall, our findings suggest that as patients reach skeletal maturity, the adductor tubercle eventually migrates from the level of the physis to a location that is more distal and it likely maintains a more posterior location with respect to the PFC line.
In the skeletally immature patient undergoing patellofemoral reconstruction surgery, it may be difficult to achieve optimal patellar isometry while minimizing iatrogenic physeal injury. The Schöttle point, a radiographic landmark of the isometric point of the MPFL, is commonly used for graft anchor placement in adults undergoing MPFL reconstruction. However, graft anchoring in this location may not be appropriate in the skeletally immature patient. 4 Avoiding physeal injury in the pediatric population has been described by identifying the Schöttle point and then aiming distal to the physis and anterior.3,8 Some surgeons have alternatively opted to anchor the graft proximal to the physis. Yet, there have been reports of proximal graft migration and even subsequent graft failure when anchoring in the metaphysis. 7 In addition, anchoring in the metaphysis may be associated with less-than-ideal patellofemoral isometry, as our study found the anatomic origin of the MPFC to be at or more likely distal to the physis. Thus, we suggest that pediatric patients undergoing MPFL or MQTFL reconstruction, regardless of age, have the patellofemoral graft anchored distal to the physis to maximize patellar isometry, minimize physeal injury, and avoid risk of graft migration and failure.
Our study included a spectrum of male cadaveric specimens aged 4 to 16 years and had a larger sample size than that in previous studies investigating this topic. Additional strengths include our measurement protocol, which was developed under the guidance of a fellowship-trained musculoskeletal radiologist, and our use of volume-rendering software to evaluate bony and soft tissue anatomy.
One of the limitations of this study is that we used CT instead of magnetic resonance imaging, which would potentially have finer soft tissue detail. It is likely that the adductor tubercle is slightly more distal than identified in our study, as we were able to label only the most distal aspect of the adductor magnus tendon that was visible on CT scans. Nevertheless, the CT images were of high quality with thin cuts and enabled us to identify the adductor magnus tendon and general region of insertion, which was clearly at or distal to the physis. We had just 1 orthopaedist record measurements, so no interrater data are available. However, measurements were confirmed by the senior author at a later time as a quality control measure. There is also a possibility of intrarater error, although localization to the appropriate anatomic landmarks was confirmed in 3 planes (axial, sagittal, and coronal) on CT scans and evaluated with volume-rendering software to ensure accuracy. In addition, only male specimens were included in this study, and it is unclear if these results are generalizable to female patients. Further study with female cadaveric specimens and a larger sample size may be needed to corroborate our findings.
Conclusion
This study suggests that the location of the adductor tubercle in male pediatric patients is at or distal to the physis. Thus, our findings directly conflict with those of previous studies that suggested a more proximal location. When MPFL and MQTFL reconstruction is performed in the skeletally immature patient, distal—rather than proximal—graft anchor placement with respect to the physis might better help restore patellofemoral isometry and avoid the issues of graft migration seen with proximal anchors.
Footnotes
Acknowledgements
We appreciate the assistance of Dr. Andrew Haims (musculoskeletal radiologist) with development of our measurement protocol.
Submitted October 23, 2022; accepted February 13, 2023.
One or more of the authors has declared the following potential conflict of interest or source of funding: J.F. has received consulting fees from Linvatec and a grant from Encore Medical. D.B.F. has received hospitality payments from Medtronic USA and consulting fees from Orthofix, Orthopediatrics, and Ultragenyx. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.