
Abstract
Background:
Tarsal navicular bone stress injuries (BSIs) are considered “high risk” because of prolonged healing times and higher rates of nonunion in adult populations but, to our knowledge, have not been comprehensively examined in adolescent athletes.
Purpose:
To describe the characteristics of tarsal navicular BSIs in adolescents.
Study Design:
Case series; Level of evidence, 4.
Methods:
A retrospective analysis of patients aged 10 to 19 years with a radiographically diagnosed tarsal navicular BSI was performed at 8 academic centers over a 9-year study period. Age, sex, body mass index (BMI), primary sport, physical examination findings, imaging, treatment, surgical technique, return-to-sport time, and complications were analyzed.
Results:
Among 110 patients (mean age, 14.7 ± 2.7 years; 65% female), common primary sports were cross-country/track and field (29/92 [32%]) and gymnastics/dance (25/92 [27%]). Grade 4 BSIs were identified in 44% (48/110) of patients, with fracture lines present on radiography or magnetic resonance imaging. Nonoperative treatment (mean age, 14.4 ± 2.6 years), consisting of protected weightbearing and either a protective boot (69/88 [78%]) or a cast (19/88 [22%]), was trialed in all patients and was successful in 94 patients (85%). Operative treatment (mean age, 17.1 ± 1.4 years) was ultimately pursued for 16 patients (15%). Patients who required surgery had a higher BMI and a higher percentage of fracture lines present on imaging (nonoperative: 36/94 [38%]; operative: 14/16 [88%]). The median time to return to weightbearing, running, and full sport was significantly longer in duration for the operative group than the nonoperative group (P <.05). Complications associated with surgery included 1 case each of delayed union, nonunion, and painful implants, the latter of which required secondary surgery.
Conclusion:
Adolescent tarsal navicular BSIs were identified most commonly in female patients in leanness sports. Adolescents who required surgery were more likely to be older, have higher BMIs, and have grade 4 BSIs, and they returned to sport within a median of 5 months after single- or double-screw fixation with a low risk of postoperative complications. A better understanding of the presenting signs and symptoms and appropriate diagnostic imaging of navicular BSIs may lead to an earlier diagnosis and improved outcomes.
Bone stress injuries (BSIs) result from chronic, repetitive mechanical loading of bone over an extended period of time. Although the exact pathophysiology is incompletely understood, it is believed that impact loading forces impede adequate bone remodeling and result in structural fatigue, causing localized bone pain and tenderness. 13 In a healthy person, with appropriate recovery between sessions of impact loading and adequate nutrition, the bone can recover and adequately heal. 30 However, if not managed appropriately, the injury can progress to a BSI and delays in return to activity. 1 BSIs account for around 10% of all injuries seen in sports medicine clinics and affect athletes across a wide range of sports, with the highest rates occurring among cross-country, track, and gymnastics athletes. 3 Female patients have a higher risk of sustaining BSIs than male patients.6,13,31
The tarsal navicular bone is a wedge-shaped bone located in the midfoot that articulates with the talus, the calcaneus, 3 cuneiform bones, and the cuboid.9,25 Its anatomic location makes it critical for midfoot stability, and it plays a significant role in force transmission and push-off during gait. The unequal distribution of high-impact weightbearing forces from medial and lateral compression may allow for shear stress to concentrate at the central third of the tarsal navicular bone, making the bone prone to stress injuries. 30 Injuries to the tarsal navicular bone are considered high risk for fracture nonunion and avascular necrosis because of the complex anatomic forces and poor blood supply in its midportion. 26
Tarsal navicular BSIs are rare in the general population, with reports of fractures, including BSIs, to the midfoot accounting for around 5% of all foot injuries, and of those, 35.5% occur to the navicular bone.21,24 However, navicular BSIs are more common among athletes, most notably track and field athletes in whom sprinting, hurdling, and jumping are common.8,9 Tarsal navicular stress injuries in athletes were found to have as high as a 14% incidence rate in some series. 32
Given the insidious onset and unique pathophysiology of tarsal navicular BSIs, their diagnosis can be challenging and thus has not been well studied. 23 This is true particularly in the younger population, and recent research has shown an increasing rate of overuse injuries, likely related to more intense regimens of training and competition and the trend of youth sport specialization.5,13,17,18 The purpose of this study was to examine and describe the characteristics of tarsal navicular BSIs in adolescent athletes, with particular attention to clinical presentation, diagnostic approach, injury severity, and functional recovery. An additional aim of this study was to enhance the understanding of tarsal navicular BSIs in this younger cohort in comparison with older subpopulations gleaned from the historical literature.
Methods
This institutional review board–approved study was a multicenter retrospective chart review of adolescent patients at 8 academic centers with a radiographically diagnosed tarsal navicular BSI. Medical records between January 1, 2013, and May 1, 2021, of patients receiving care at an orthopaedic or sports medicine clinic at participating institutions were reviewed. Given the retrospective nature of this study, informed consent/assent was not obtained.
Data Acquisition
Data were collected by study co-investigators across 8 geographically varied academic institutions in the United States. Adolescent patients were defined as those aged between 10 and 19 years at the time of the diagnosis, according to the definition described by the World Health Organization. 35 Patient charts were initially identified using International Classification of Diseases–9 and −10 and Current Procedural Terminology codes that included a diagnosis of a stress fracture to the tarsal navicular bone (Figure 1). Charts were then reviewed to assess descriptions of discrete radiological findings consistent with a tarsal navicular BSI. Any records with equivocal radiological findings or indeterminate diagnoses were excluded. The team identified a total of 110 patients aged between 10 and 19 years with tarsal navicular BSIs. In all cases, the diagnosis was confirmed via plain radiography, magnetic resonance imaging (MRI), or computed tomography (CT) using radiological reports, documented physical examinations, or both. Any questionable diagnosis prompted a secondary review of actual imaging by study investigators (B.E.H., K.R., M.H., N.B., Z.S., A.G., E.K.).
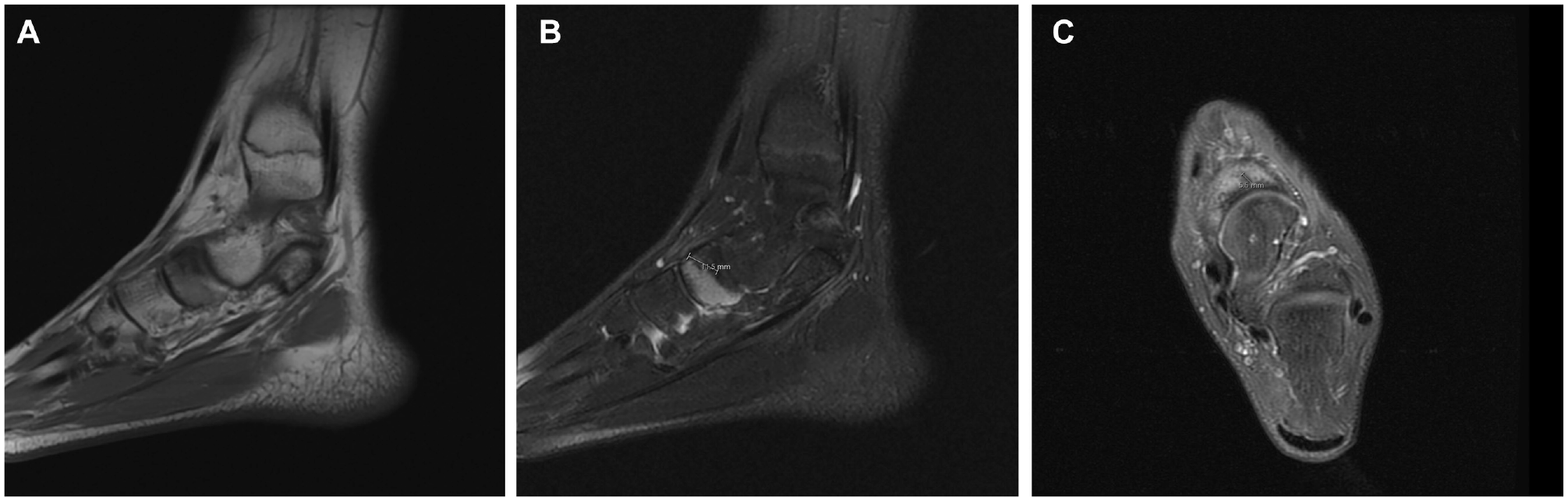
Magnetic resonance imaging of the foot demonstrating a navicular bone stress injury of the dorsal aspect: (A) sagittal T1-weighted image, (B) sagittal T2-weighted image with a fracture line measured at 11.5 mm, and (C) axial fat-suppressed proton density–weighted image with a fracture line measured at 5.5 mm. Images securely obtained from Stanford University.
Principal investigators and research coordinators (S.M., E.Z., B.E.H., K.R., M.H., N.B., Z.S., E.D.N., A.G., N.S., E.K.) also abstracted data from medical records on self-identified demographics, primary sport, relevant medical history, clinical presentation, diagnostic approach, nonoperative and operative treatment approaches, timing of protected weightbearing, return to running, and return to sport, defined as documented clearance for full sport participation. Timing was based on the date of the diagnosis for nonoperatively treated patients and the date of surgery for operatively treated patients. The date of surgery was used, given the more variable timing from the diagnosis to the surgical intervention. Data were entered using a standard Research Electronic Data Capture (REDCap) form. REDCap is a secure, web-based database hosted at the Stanford Center for Clinical Informatics.11,12 BSIs were classified based on anatomic location (dorsal, body, other); presence of a fracture line on plain radiographs, CT scans, and MRI scans (defined as grade 4 per the grading criteria of Fredericson et al 8 ); and presence of bone marrow edema on MRI scans. 15
Statistical Analysis
Descriptive statistics were used to summarize the collected variables. Percentages were reported for available data only, with missing data excluded from the denominator. Comparisons between male and female patients were performed using the chi-square test and Fisher exact test for categorical variables and the 2-sample t test and Mann-Whitney U test for continuous variables. Risk factors such as disordered eating, menstrual cycle, previous BSIs, and previous navicular injuries were compared between patients presenting with and without fracture lines and among different treatment options using the chi-square, Fisher exact, 2-sample t, and Mann-Whitney U tests. All analyses were conducted in RStudio (Posit Software. Boston, MA. Version 1.1.456) using a 2-sided level of significance of .05.
Results
Patients
The study sample consisted of 110 patients with a mean age of 14.7 ± 2.7 years (Table 1). Overall, 65% of patients were female, 88% (87/99) were White, and the mean body mass index (BMI) at the time of presentation was 21.4 ± 3.5. Additionally, 94% (92/98) of patients were self-reported athletes, with 16% (15/92) primarily participating in cross-country; 15% (14/92), in track and field; 14% (13/92), in gymnastics; and 13% (12/92), in dance.
Characteristics of Total Cohort a
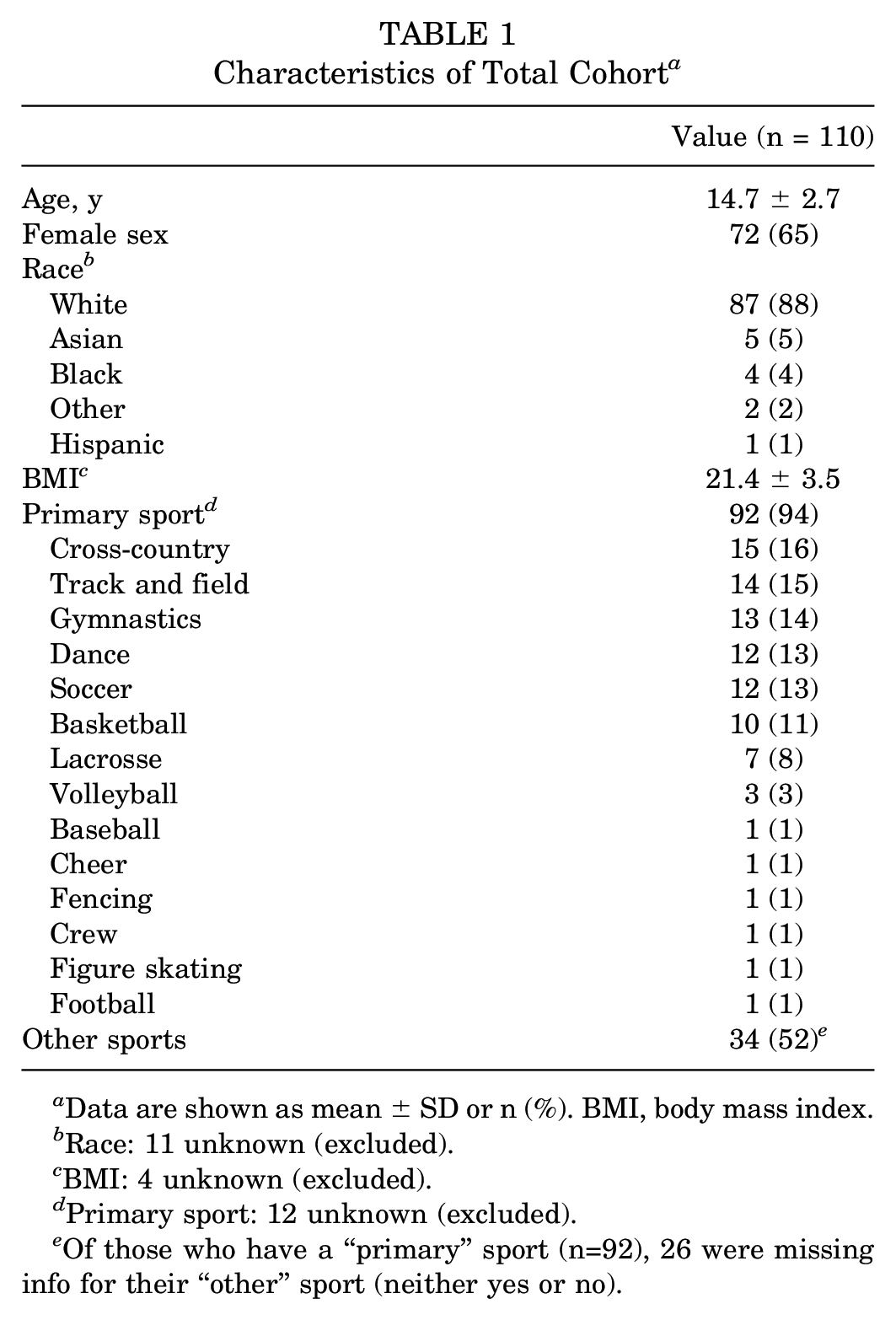
Data are shown as mean ± SD or n (%). BMI, body mass index.
Race: 11 unknown (excluded).
BMI: 4 unknown (excluded).
Primary sport: 12 unknown (excluded).
Of those who have a “primary” sport (n=92), 26 were missing info for their “other” sport (neither yes or no).
Physical Examination Findings
At the time of presentation, clinical findings demonstrated that 96% (105/109) of patients were noted to have tenderness to palpation over the navicular bone, 89% (78/88) reported pain when walking, and 55% (26/47) had pain with resisted inversion (Table 2). Also, 10% (9/91) of patients had limited range of motion of the foot. Of note, 35% (33/93) of patients had a previous diagnosis of a BSI, with 11% (11/101) of these patients having had a previous navicular stress injury. Questions regarding risk factors such as disordered eating, menstrual cycle, previous BSIs, and previous navicular BSIs were explored, but these data points were not consistently collected across study sites.
Physical Examination Findings
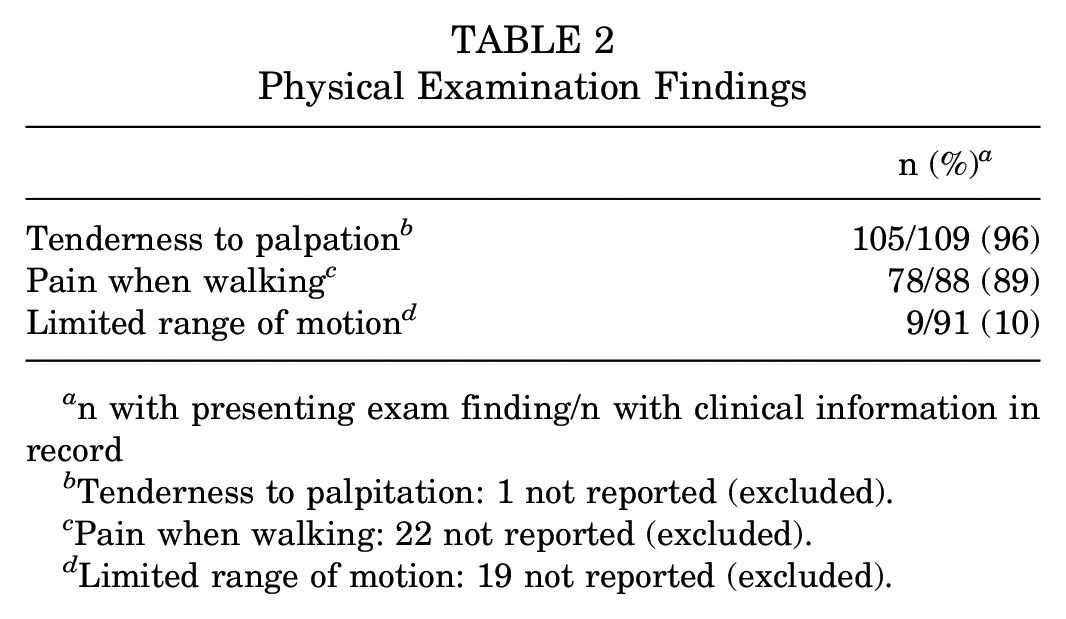
n with presenting exam finding/n with clinical information in record
Tenderness to palpitation: 1 not reported (excluded).
Pain when walking: 22 not reported (excluded).
Limited range of motion: 19 not reported (excluded).
Imaging Findings
In total, 91% (n = 100) of patients had documented plain radiographs, with 83% (n = 91) having a plain radiograph of the foot and 24% (n = 26) having a plain radiograph of the ankle out of the total patient population (n = 110). Some patients had both foot and ankle radiographs. Further, 91% (n = 100) of patients underwent MRI, and CT was performed for 30% (n = 33) of patients. All patients underwent either plain radiography or MRI, whereas both a plain radiograph and an MRI scan were obtained for 83% (n = 91) of patients.
A fracture line was identified on 9% (8/91) of plain radiographs, 44% (41/93) of MRI scans, and 75% (24/32) of CT scans. A fracture line was identified on plain radiographs or MRI scans in 44% (48/110) of patients. The most commonly identified location of the fracture line as seen on imaging was the dorsal aspect of the navicular bone (Table 3 and Figure 2).
Imaging Findings a
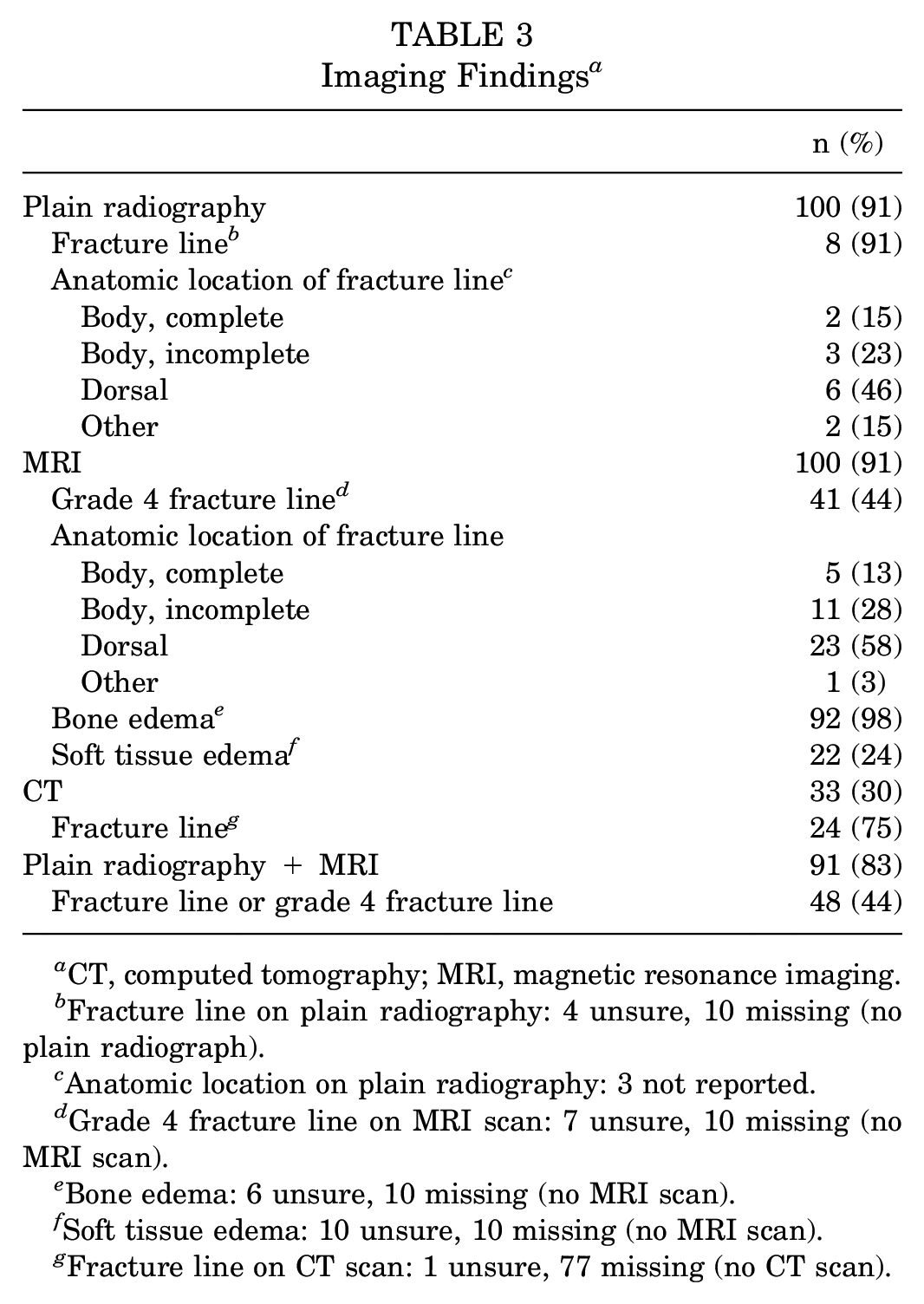
CT, computed tomography; MRI, magnetic resonance imaging.
Fracture line on plain radiography: 4 unsure, 10 missing (no plain radiograph).
Anatomic location on plain radiography: 3 not reported.
Grade 4 fracture line on MRI scan: 7 unsure, 10 missing (no MRI scan).
Bone edema: 6 unsure, 10 missing (no MRI scan).
Soft tissue edema: 10 unsure, 10 missing (no MRI scan).
Fracture line on CT scan: 1 unsure, 77 missing (no CT scan).
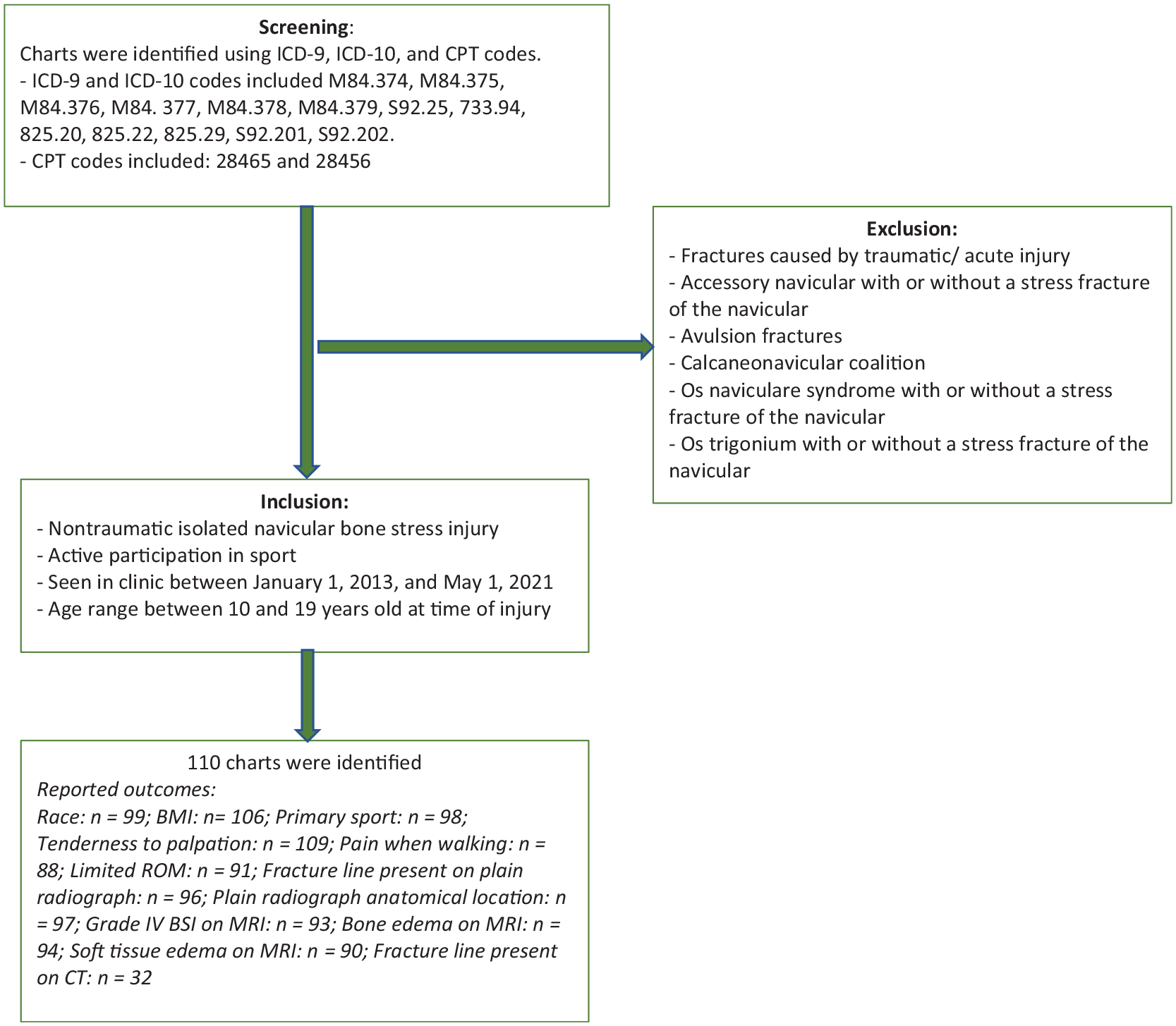
Chart review methods. BMI, body mass index; BSI, bone stress injury; CPT, Current Procedural Terminology; CT, computed tomography; ICD, International Classification of Diseases; MRI, magnetic resonance imaging; ROM, range of motion.
Nonoperative and Operative Treatment
Overall, 85% (n = 94) of patients were reported to demonstrate healing with nonoperative treatment alone. Of these, the foot of 78% (69/88) was initially immobilized in a walking boot, and the foot of 22% (19/88) was placed in a short leg cast. Physical therapy was prescribed for 70 patients (64%), with 6 patients (38%) undergoing physical therapy before surgery. Evidence of a fracture line on imaging did not result in any significant differences in the immobilization technique (36% walking boot, 39% cast; P > .999). The median time from initial presentation to full weightbearing for all nonoperatively treated patients was 7 weeks (interquartile range [IQR], 5-11 weeks; range, 0-20 weeks), the median time to running clearance was 12 weeks (IQR, 8-16 weeks; range, 3-40 weeks), and the median time to full sport clearance was 14 weeks (IQR, 9-18 weeks; range, 4-40 weeks). There was no significant difference in any of these metrics between patients treated initially with a cast (n = 19) versus a boot (n = 69) (P > .05). There were 16 patients (15%) who underwent operative treatment for their navicular BSI. After an initial period of nonoperative management (range, 2-14 weeks), 15 patients (14%) underwent operative therapy, apart from 1 patient who was not offered nonoperative treatment and underwent surgery directly. Of these patients, 8 underwent operative management after ≥3 months of nonoperative treatment after the initial diagnosis. Notably, the mean age of the 8 patients who underwent ≥3 months of nonoperative treatment was 17.3 ± 1.5 years, and the mean age of those who returned to sport with nonoperative treatment alone was 14.4 ± 2.6 years (n = 94) (P < .001). The 16 patients ultimately treated operatively were, on average, almost 3 years older than those who were successfully treated nonoperatively (17.1 vs 14.4 years, respectively; P < .001). The mean BMI of operatively treated patients was also significantly higher (23.7 ± 3.6 vs 21.0 ± 3.4, respectively; P = .011). There was no significant difference in the sex or primary sport distribution between the operative and nonoperative groups.
A fracture line was evident on diagnostic imaging in 88% of the operative group compared with 38% of the nonoperative group (P < .001). Even though the median time from presentation to surgery was 3 weeks, the majority of patients had undergone nonoperative treatment at outside institutions before presentation at the study institution. Additionally, 69% (11/16) of operatively treated patients underwent open reduction internal fixation, and 25% (4/16) underwent percutaneous screw fixation. Among operatively treated patients, 8 patients underwent 1-screw fixation, and 8 patients underwent 2-screw fixation. The median time from surgery to return to weightbearing was 10 weeks (IQR, 8-14 weeks), the median time to running clearance was 18 weeks (IQR, 15-24 weeks), and the median time to full sport clearance was 20 weeks (IQR, 17-32 weeks). Each of these intervals was significantly longer in duration than that of patients treated nonoperatively using the date of the diagnosis as the starting point (Table 4).
Characteristics of Patients by Treatment a
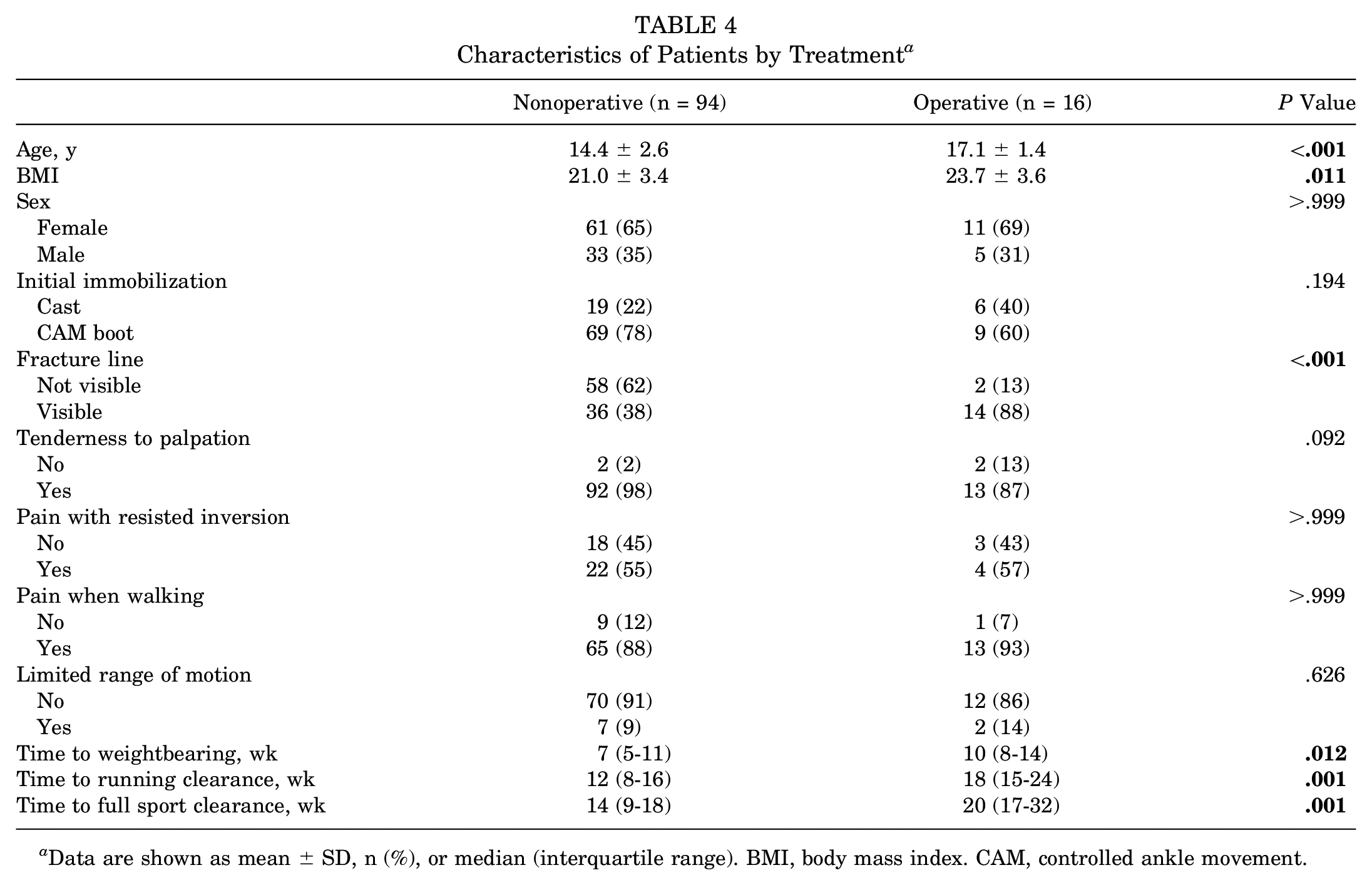
Data are shown as mean ± SD, n (%), or median (interquartile range). BMI, body mass index. CAM, controlled ankle movement.
Complications
No intraoperative or early postoperative complications were reported. A total of 3 complications were reported for the patients who underwent surgical treatment. There was 1 patient diagnosed with delayed union postoperatively, 1 patient was diagnosed with postoperative nonunion, and 1 patient was reported as having painful implants after percutaneous screw fixation. The patient with painful implants underwent a second surgical procedure for implant removal. There were no reports of additional surgery for the patients with delayed union and nonunion.
Discussion
The current study was designed to characterize tarsal navicular BSIs in adolescent athletes. Despite this subpopulation’s demonstrating an increasing risk of overuse injuries in multiple recent studies,2,14,28 navicular BSIs have not been the subject of investigations specific to this young age group to date. Using descriptive and comparative statistics for a large, diverse cohort of adolescent athletes from 8 different academic centers across the United States, the current study sought to comprehensively describe the onset, imaging modalities, treatment approaches, and clinical outcomes of these patients managed with both nonoperative and operative options.
Previous studies investigating tarsal navicular fractures have not necessarily differentiated between traumatic fractures and nontraumatic BSIs.4,7,19,21,26,30 Notably, traumatic navicular fractures are caused by acute, discrete mechanisms, such as high-energy shear injuries to the navicular tuberosity or body. 21 In contrast, tarsal navicular BSIs occur because of chronic, repetitive overloading of the forefoot. 21
In the initial literature examining tarsal navicular BSIs, male patients were found to have a higher prevalence of tarsal navicular BSIs 33 ; however, more recent research has found a growing prevalence in female athletes. 31 In the adult population, running and jumping athletes, such as sprinters and basketball players, were found to have a high incidence of tarsal navicular BSIs. 30 Additionally, a recent study by Patel et al 24 found favorable outcomes in adults with nonoperative treatment for early and nondisplaced fractures and success with surgical treatment for high-level athletes and more severe BSIs. The mean return-to-sport time for predominantly young, adult male patients with nonsurgical treatment was 4.9 months, which is longer than the 14 weeks (IQR, 9-18 weeks) for the nonoperative group in the present study.20,24,34
Ultimately, 2 distinct patient characteristic trends emerged from the current study, warranting attention. First, whereas an early study of adults with navicular BSIs demonstrated male patients to be at a higher risk than female patients, 24 the current study revealed a larger number of navicular BSIs in female patients. Second, adolescents engaging in specific sports were found to constitute the majority of the current cohort. Specifically, cross-country and track and field runners represented 16% and 15%, respectively, of the overall study population, suggesting a clear pattern of repetitive microtrauma with these injuries in adolescents. Gymnasts, dancers, soccer players, and basketball athletes represented additional subpopulations in this cohort, with higher impact mechanisms related to cutting, pivoting, jumping, and landing. BSIs in running and gymnastics have also been attributed to low-energy availability, resulting in a condition called the female athlete triad or relative energy deficiency in sport.1,13 Previous adult studies have been less clear about high-risk athletic subpopulations. For example, a study by Rizzone et al 27 in 2017, looking at National Collegiate Athletic Association athletes, found the highest rates of reported stress fractures in gymnastics, cross-country, and track. They also found a higher incidence of stress fractures in female athletes across all sex-comparable sports such as basketball, cross-country, soccer, indoor track, and outdoor track. 27
Because navicular BSIs have historically been associated with delays in the diagnosis, the physical examination findings reported in the current study can inform medical professionals when developing a differential diagnosis for the insidious onset of midfoot pain in an adolescent. The most prominent clinical findings were tenderness to palpation, specifically in the navicular area, pain when walking, and pain with resisted inversion. According to Patel et al, 24 initial clinical presentation includes medial midfoot pain over the “N-spot” (navicular tenderness) and medial midfoot tenderness. Range of motion was found to be relatively normal, with the possibility of pain with tarsal abduction/adduction or forefoot inversion/eversion. Previous studies have also found a relationship between foot posture, specifically pes cavus deformities, and the risk of navicular BSIs because of the tendency toward greater rigidity and decreased shock absorption.22,30 Unfortunately, foot posture was not reported consistently enough to include in our final analysis.
The use of various diagnostic imaging modalities in the current study, and the relevant findings in this cohort, may help medical professionals regarding the utilization of advanced imaging and treatment approaches. MRI, plain radiography, and CT were all used as diagnostic imaging modalities. MRI detected a grade 4 BSI in 44% of the patients, with 58% of these injuries seen in the dorsal aspect of the tarsal navicular bone. CT was used inconsistently in our cohort (30%), which is likely because of its higher radiation exposure, and MRI was often necessary for a diagnosis, especially for BSIs without a fracture line visible on plain radiographs. In agreement with the findings of the current study, the use of MRI as a diagnostic approach for BSIs has been found to be a significant indicator for the severity of BSIs. Hoenig et al 13 found MRI-based grading to be significantly correlated with a longer time to return to sport. Although Saxena et al 29 used CT for the classification of navicular BSIs, this was not ideal for the current study for several reasons: (1) only 30% of study patients underwent CT, and (2) over half of the patients did not have a fracture line present, which is necessary for the grading criteria of Saxena et al. 29
Importantly, when comparing all navicular BSI cases, patients in the operative group had a significantly longer time to return to weightbearing, running, and sport compared with those in the nonoperative group, which is likely because of the higher prevalence of fracture lines and more severe navicular BSIs that required surgery. The mean age of operatively treated patients was also significantly higher, which could be from greater intensity of sport participation or other underlying metabolic bone health factors that were difficult to assess in a retrospective analysis.10,23 Thus, despite appropriate treatment, it was shown that tarsal navicular BSIs can lead to significant time lost from sport, and counseling patients on expectations for tarsal navicular BSIs is extremely important. Physicians need a high index of suspicion when treating both older athletes and athletes involved in high-risk sports. 16 An early diagnosis of these BSIs can be important to prevent the development of more severe fractures that require surgery.
To our knowledge, this is the first study that has investigated tarsal navicular BSIs in an adolescent population. There is a dearth of data pertaining to the diagnosis and management of isolated navicular injuries, especially those not stemming from a clear traumatic event. In the current era of increasing youth sport participation, greater sport specialization and intensity of training, and the associated rise of adolescent overuse injuries, these data are critical for caregivers devoted to keeping young athletes safe through thoughtful nonoperative and, when needed, operative management. 13 This case series highlights the importance of advanced imaging, such as MRI, in the diagnostic workup for navicular BSIs and how most of these athletes successfully returned to sport with nonoperative management.
Limitations
There are several limitations inherent in the current study. Because of its retrospective design, critical clinical information, such as the presence of laxity and hypermobility in these adolescent athletes, menstrual cycle, or nutritional intake history, was frequently absent in the reviewed medical records. Additional treatment methods such as referral to a sports dietitian, supplementation with vitamin D, or the use of bone stimulators were not consistently documented and thus were excluded from the final analysis. It is also not known if some of the nonsurgical and surgical interventions resulted in a long-term resolution of symptoms. Further, the fracture classification used has not been validated and was modified from MRI grading criteria utilized for other BSI anatomic locations 8 and/or navicular fractures resulting from acute trauma. Additionally, there were no standard criteria for deciding to proceed to surgery, and therefore, this study is limited in its ability to determine the appropriate indications and timing of surgery. Another limitation was that time to return to sport may be affected by the seasonality of different sports, especially in this young cohort.
Conclusion
In this retrospective study investigating a large cohort of 110 adolescent athletes from 8 geographically varied academic institutions over a 9-year period, tarsal navicular BSIs were found to occur more commonly in female patients and in athletes participating in repetitive impact sports, such as cross-country, track and field, gymnastics, dance, soccer, and basketball. Also, 85% of patients who were treated nonoperatively were able to return to running within a median time of 3 months and to return to sport within a median time of 4 months. Adolescents who required surgery were more likely to be older, have higher BMIs, and have grade 4 BSIs, and they returned to sport within a median time of 5 months after single- or double-screw fixation, with a low risk of delayed union or nonunion in this young subpopulation. This case series provides insight on how institutions throughout the country are managing this injury and can both guide clinicians and drive additional methodologically rigorous research on the topic. Future research is needed to explore the risk factors, imaging criteria, and treatment methods associated with tarsal navicular BSIs in adolescent athletes.
Footnotes
Submitted June 15, 2022; accepted March 3, 2023.
Presented at the annual meeting of the AOSSM, Colorado Springs, Colorado, July 2022.
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.