
Abstract
Background:
Preoperative body mass index (BMI) is one of the correctable factors before surgery. Few studies have investigated the effect of BMI on the survivorship of lateral meniscal allograft transplantation (MAT).
Hypothesis:
Patients with a high BMI have inferior survivorship after lateral MAT when compared with those with a normal BMI.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
Overall, 306 consecutive patients who underwent lateral MAT were retrospectively reviewed. According to the classification criteria of the World Health Organization, patients were split into 2 groups: normal weight (BMI <25.0) and overweight (BMI ≥25.0). There were 104 patients (34.0%) allocated into the overweight group. Given the demographic heterogeneity between the groups, propensity score matching was performed. Before and after propensity score matching, the anatomic and clinical survival rates of the 2 groups were compared by Kaplan-Meier survival analysis. Anatomic failure was defined as a tear covering >50% of the allograft or unstable peripheral rim on follow-up magnetic resonance imaging and second-look arthroscopy. Clinical failure was defined as a Lysholm score <65 or need for additional surgery, such as revision MAT.
Results:
For all patients, the mean ± SD follow-up period was 6.9 ± 4.2 years. The mean BMI of the overweight and normal weight groups was 27.8 ± 2.6 and 22.0 ± 1.9, respectively. The mean Lysholm scores at the last follow-up were not significantly different between the groups. However, the anatomic survival rate in the overweight group (77.9%) was significantly lower than that in the normal weight group (90.1%) (P < .001). The clinical survival rate (82.7%) in the overweight group was significantly lower than that in the normal weight group (95.0%) (P < .001). After propensity score matching for patient characteristics, which left 87 patients per group, the anatomic and clinical survival rates were significantly lower in the overweight group.
Conclusion:
Preoperative high BMI was associated with inferior anatomic and clinical survival rates. The results of the current study suggest that weight loss before lateral MAT may be required in overweight patients for the improvement of anatomic and clinical survival rates.
Meniscal allograft transplantation (MAT) is an effective treatment choice in patients with postmeniscectomy syndrome.1,7,8,10,17 Several prognostic factors of graft survivorship after MAT have been reported in mid- to long-term follow-up studies, such as age-related factors, alignment, instability, osteoarthritis, and body mass index (BMI).5,11,23,24 Among them, BMI can be corrected with nonsurgical treatment before MAT. However, few studies have investigated the effect of BMI on survivorship after MAT.
To date, the relationship between BMI and the outcomes of MAT has been disputed. A previous study reported that patients who were obese (BMI ≥30) had higher clinical failure rates after MAT as compared with those who were not obese, 3 whereas other studies found no significant correlation between BMI and the outcomes of MAT.18,25 However, as the number of patients was <50 in the aforementioned studies, it is difficult to elucidate this relationship. In addition, all these studies were performed without separating the groups according to medial and lateral MAT. Considering the structural, functional, and surgical differences between the medial and lateral meniscus,4,19,22 evaluation of the effect of BMI may be necessary after dividing medial and lateral MAT. Furthermore, because the load on the knee joint is increased in patients with high BMI, 13 the actual status of the graft after MAT could be influenced by BMI. Yet, most previous studies have not investigated objective outcomes determined by allograft status on follow-up magnetic resonance imaging (MRI) or second-look arthroscopy.
This study aimed to investigate the effect of BMI on survivorship by objective and clinical evaluations, especially in patients undergoing lateral MAT. We hypothesized that patients with a high BMI have inferior survivorship after lateral MAT as compared with those with a normal BMI.
Methods
Patient Selection
This study was approved by our institutional review board. A total of 444 consecutive patients who underwent primary lateral MAT between November 1997 and April 2020 were retrospectively reviewed. Physically active patients with persistent localized knee pain in the lateral compartment after subtotal or total lateral meniscectomy were eligible to undergo lateral MAT. Patients having ≤5° of mechanical valgus alignment on hip-knee-ankle standing radiographs and >2-mm preserved joint spaces on the Rosenberg view were eligible. 14 Localized International Cartilage Regeneration & Joint Preservation Society (ICRS) grade 3 or 4 cartilage lesions covered by the meniscal transplant were acceptable for lateral MAT; however, diffuse grade 3 or 4 degenerative arthritis was a contraindication. The inclusion criteria were as follows: minimum 2-year follow-up and evaluation with not only clinical scores but also MRI scans for anatomic assessment of the allografts. Of the 444 patients, 136 with <2-year follow-up and 2 without postoperative MRI scans were excluded. Finally, 306 patients were enrolled in the study.
Surgical Technique and Rehabilitation
All lateral MATs were performed with size-matched6,16 fresh-frozen allografts by a single senior surgeon (S.-I.B.) using the keyhole technique. The status of the cartilage, ligaments, and menisci was evaluated through arthroscopic examination, after which the remaining host meniscus was completely resected. After tunnel preparation for the bone bridge, the allograft was introduced through an anterior miniarthrotomy. After confirming the optimal allograft position, we performed traditional inside-out meniscal repair. Postoperatively, a range of flexion of 90° was gradually achieved within 4 weeks and 120° by 6 to 8 weeks. Toe-touch weightbearing was allowed during the first 2 weeks, and full weightbearing was allowed at 6 to 8 weeks. The patients were advised to participate only in low-impact sport activities and light labor to avoid deterioration of the meniscal allograft.
Study Design
According to the overweight standard (BMI, 25.0) in the World Health Organization classification, 15 the study population was divided into 2 groups: normal weight (<25.0) and overweight (≥25.0). The additional cutoff values of BMI were measured by receiver operating characteristic (ROC) curves, including the survival rates, to determine whether the BMI cutoff of 25 was appropriate. There were 104 patients (34.0%) allocated into the overweight group (≥25.0) and 202 (66.0%) into the normal weight group (<25.0). The patient characteristics for each group are presented in Table 1. For data analysis, the cartilage lesions were categorized into low grade (ICRS 0, 1, or 2) and high grade (ICRS 3 or 4). There were significant differences in patient characteristics, including sex, cartilage status, and the follow-up period between the groups. Therefore, to minimize the potential confounding and selection bias, propensity score matching was performed with the following covariates: age, sex, alignment, meniscal deficiency period, cartilage status, and the last follow-up period. Before and after propensity score matching, comparisons of cumulative survival rates after lateral MAT were performed between the groups.
Patient Characteristics and Clinical Outcomes in the 2 Study Groups a
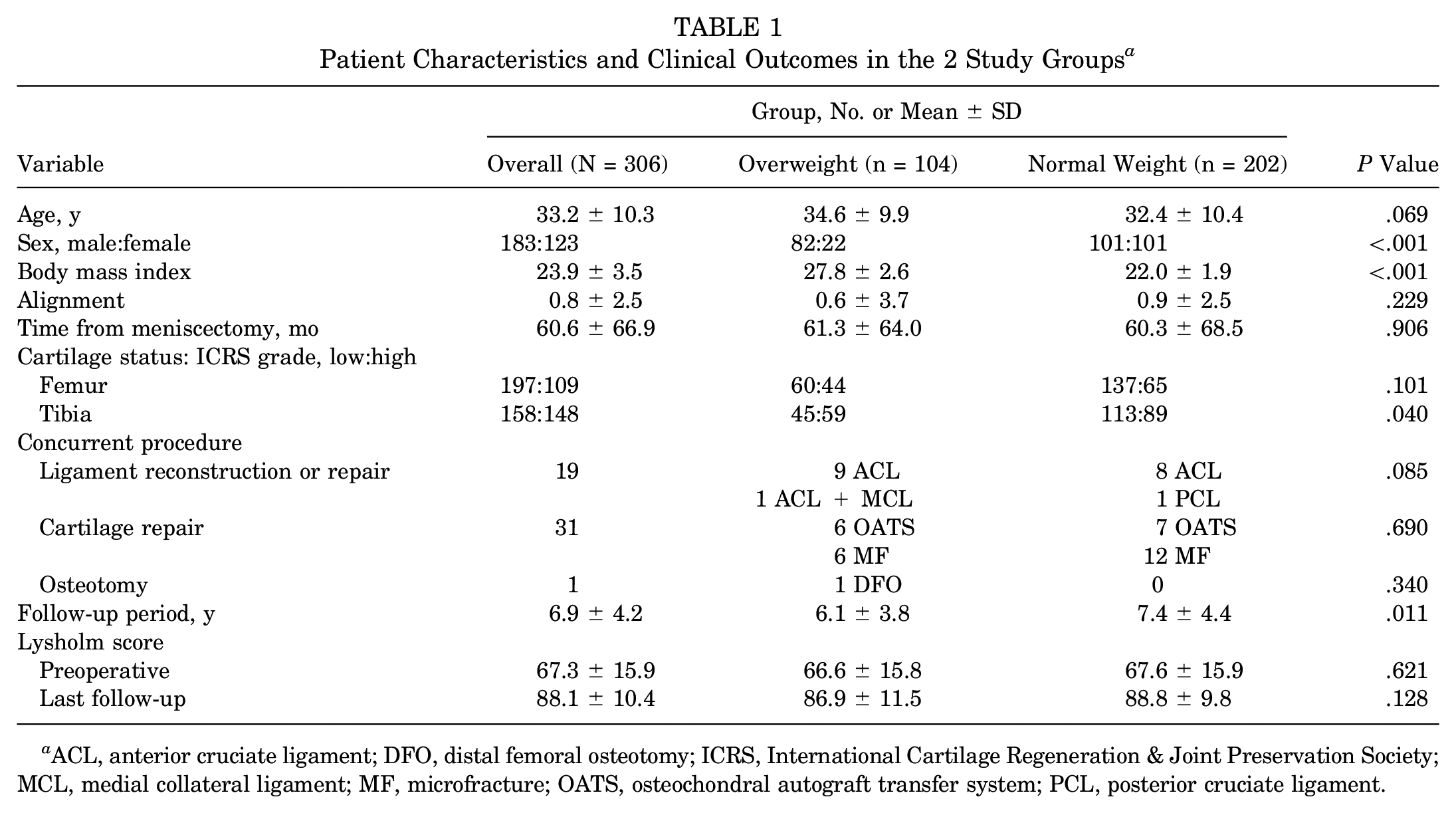
ACL, anterior cruciate ligament; DFO, distal femoral osteotomy; ICRS, International Cartilage Regeneration & Joint Preservation Society; MCL, medial collateral ligament; MF, microfracture; OATS, osteochondral autograft transfer system; PCL, posterior cruciate ligament.
Postoperative Objective and Clinical Evaluations and Definition of MAT Failure
Postoperative allograft status was evaluated through follow-up MRI scans (Achieva 3T; Philips Healthcare) during the first year and every 2 years with the patient’s agreement. Second-look arthroscopic surgery was considered if there was persistent postoperative knee pain and positive MRI findings for allograft tears or indications, such as debridement, adhesiolysis, and revision ligament reconstruction. Clinical outcomes were estimated using modified Lysholm knee scores immediately after surgery and every 1 or 2 years at follow-up visits.
MAT failure was defined from 2 points of view: objective and clinical evaluations. The poor results of objective and clinical outcomes were defined as anatomic and clinical failure, respectively. Anatomic failure was determined objectively by graft status on follow-up MRI and second-look arthroscopy. Anatomic failure was defined as an allograft tear involving >50% of the graft or unstable peripheral rim as confirmed through second-look arthroscopy. Clinical failure was defined as a poor Lysholm score <65 or any requirement for additional surgery, such as revision MAT, realignment osteotomy, arthroplasty, and meniscectomy for >50% of the allograft. 20 Two orthopaedic surgeons who did not perform the surgeries independently evaluated anatomic failure in a blind manner. Any disagreements in the evaluation were resolved through discussion.
Statistical Analysis
SPSS statistics (Version 27.0; IBM) was used for the statistical analyses with a P value <.05 considered statistically significant. The Student t test was applied to verify the differences in the clinical outcomes. The chi-square test was applied for categorical variables. The cumulative anatomic and clinical survival rates for each group were evaluated using a Kaplan-Meier survival analysis, including patients with early anatomic or clinical failure within 2 years after lateral MAT. A log-rank test was used to compare the survival rates between the groups. Propensity score matching was performed with a logistic regression model. The matched ratio is 1:1 for the 2 groups, and nearest neighbor matching was performed with the caliper 0.1.
Results
For all patients, the mean Lysholm score significantly improved from 67.3 ± 15.9 preoperatively to 88.1 ± 10.4 at the last follow-up (P < .001; mean ± SD, 6.9 ± 4.2 years) (Table 1). The mean Lysholm scores at the last follow-up were not significantly different between the groups (86.9 ± 11.5, overweight; 88.8 ± 9.8, normal weight).
The calculated ROC curves based on the anatomic and clinical survival rates indicated BMI cutoff values of 24.3 and 24.9, respectively. The areas under the curve were 0.635 for the anatomic survival rate (P = .006) and 0.657 for the clinical survival rate (P = .005).
Survivorship Analysis
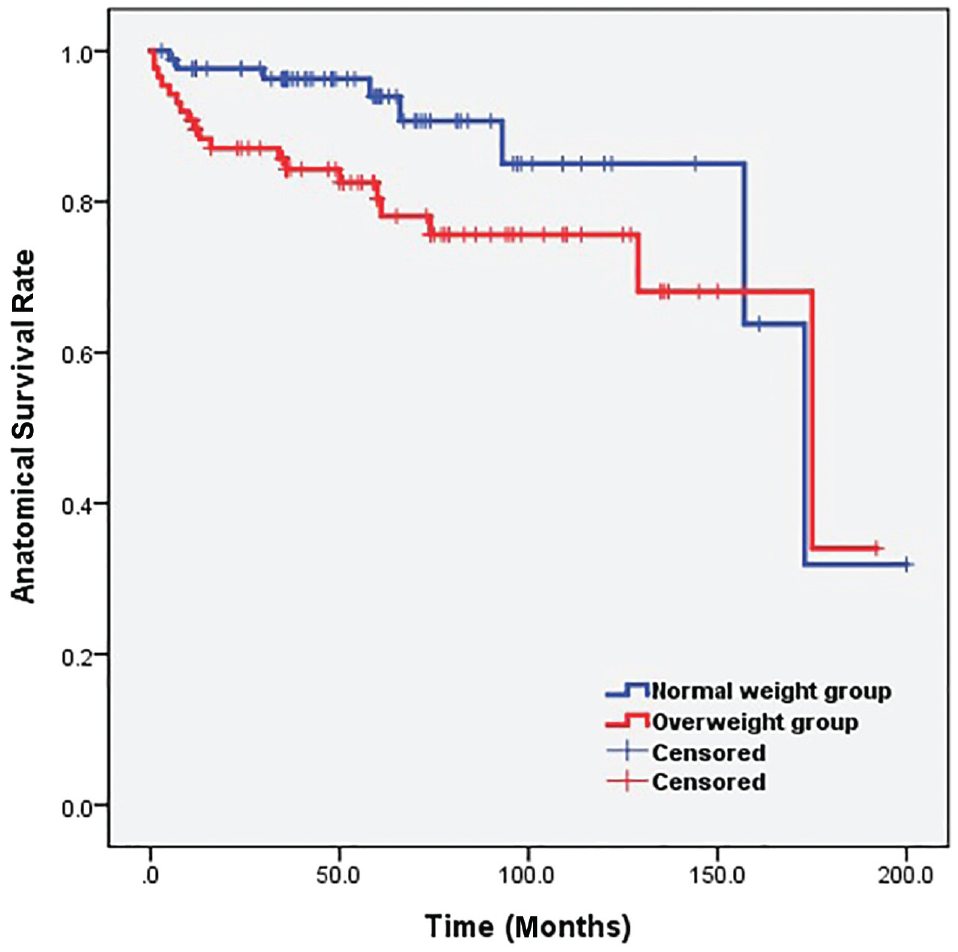
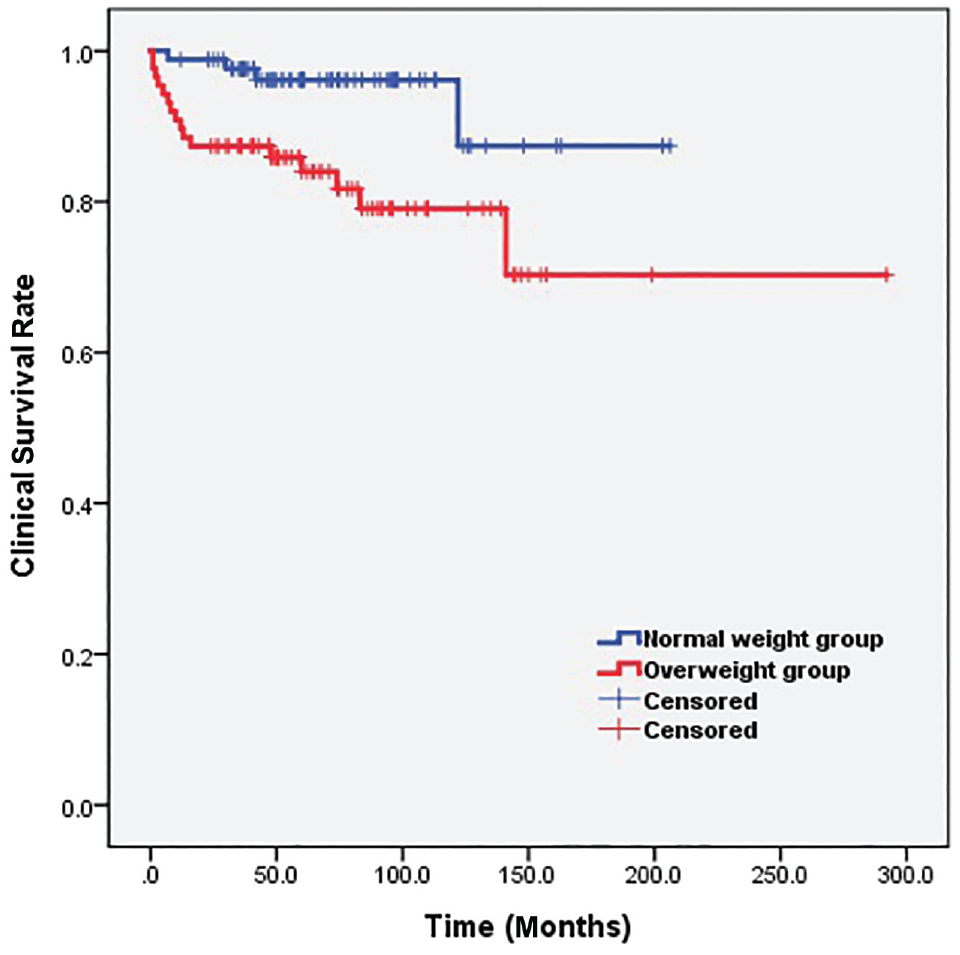
In the overweight group, 23 patients (22.1%) underwent anatomic failure and 18 (17.3%) underwent clinical failure. In the normal weight group, 20 patients (9.9%) underwent anatomic failure and 10 (5.0%) underwent clinical failure. The cumulative anatomic survival rate in the overweight group (77.9%) was significantly lower than that in the normal weight group (90.1%) (P < .001) (Figure 1). The cumulative clinical survival rate in the overweight group (82.7%) was significantly lower than that in the normal weight group (95.0%) (P < .001) (Figure 2).
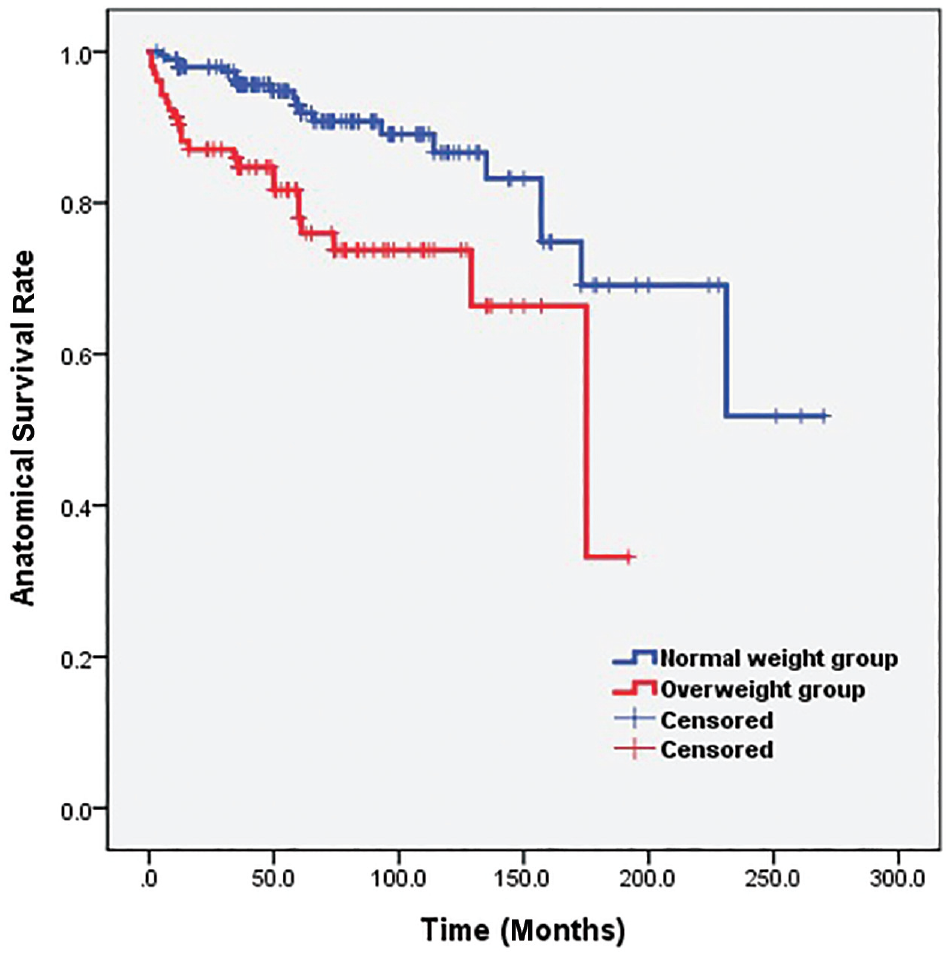
Anatomic survival rates in the 2 groups before propensity score matching.
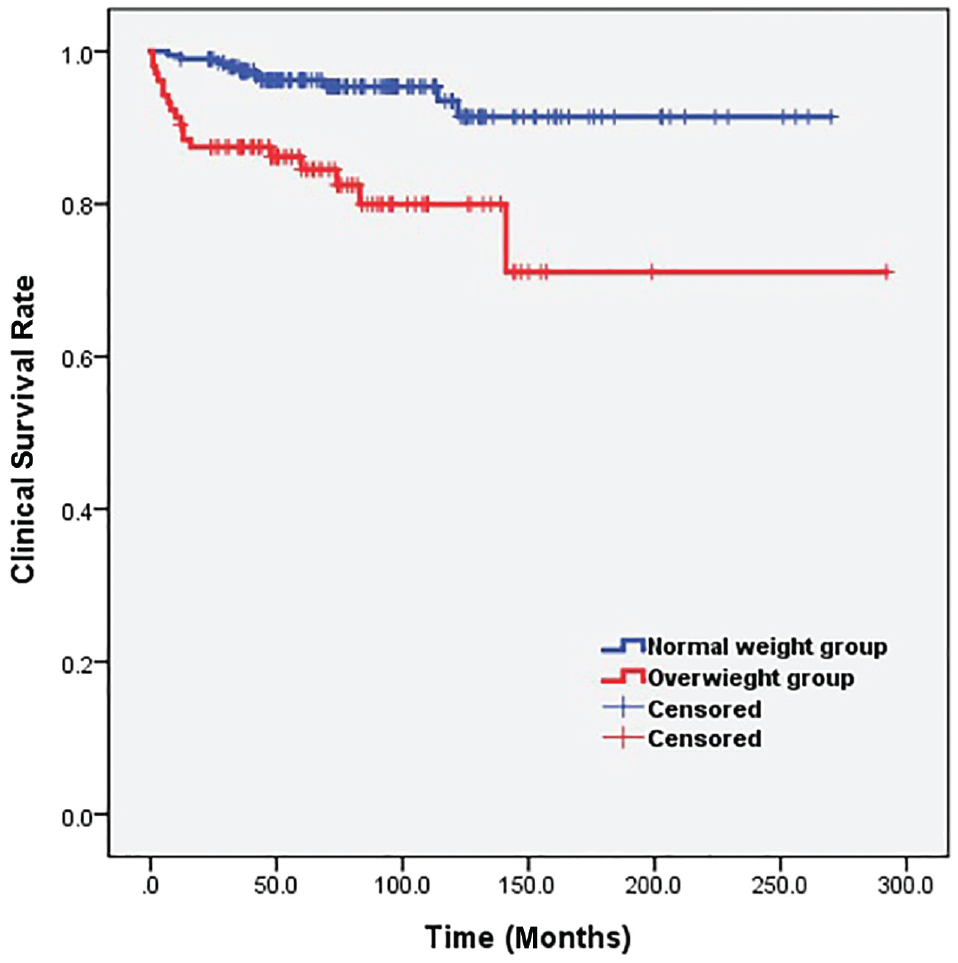
Clinical survival rates in the 2 groups before propensity score matching.
After propensity score matching for patient characteristics, 87 patients remained in each group (Table 2). There were no significant differences with respect to sex, cartilage status, and follow-up period, which showed a significant difference before propensity score matching. The cumulative anatomic survival rate in the overweight group (78.2%) was significantly lower than that in the normal weight group (90.8%) (P = .045) (Figure 3). Also, the cumulative clinical survival rate in the overweight group (81.6%) was significantly lower than that in the normal weight group (95.4%) (P = .007) (Figure 4).
Patient Characteristics and Clinical Outcomes After Propensity Score Matching a
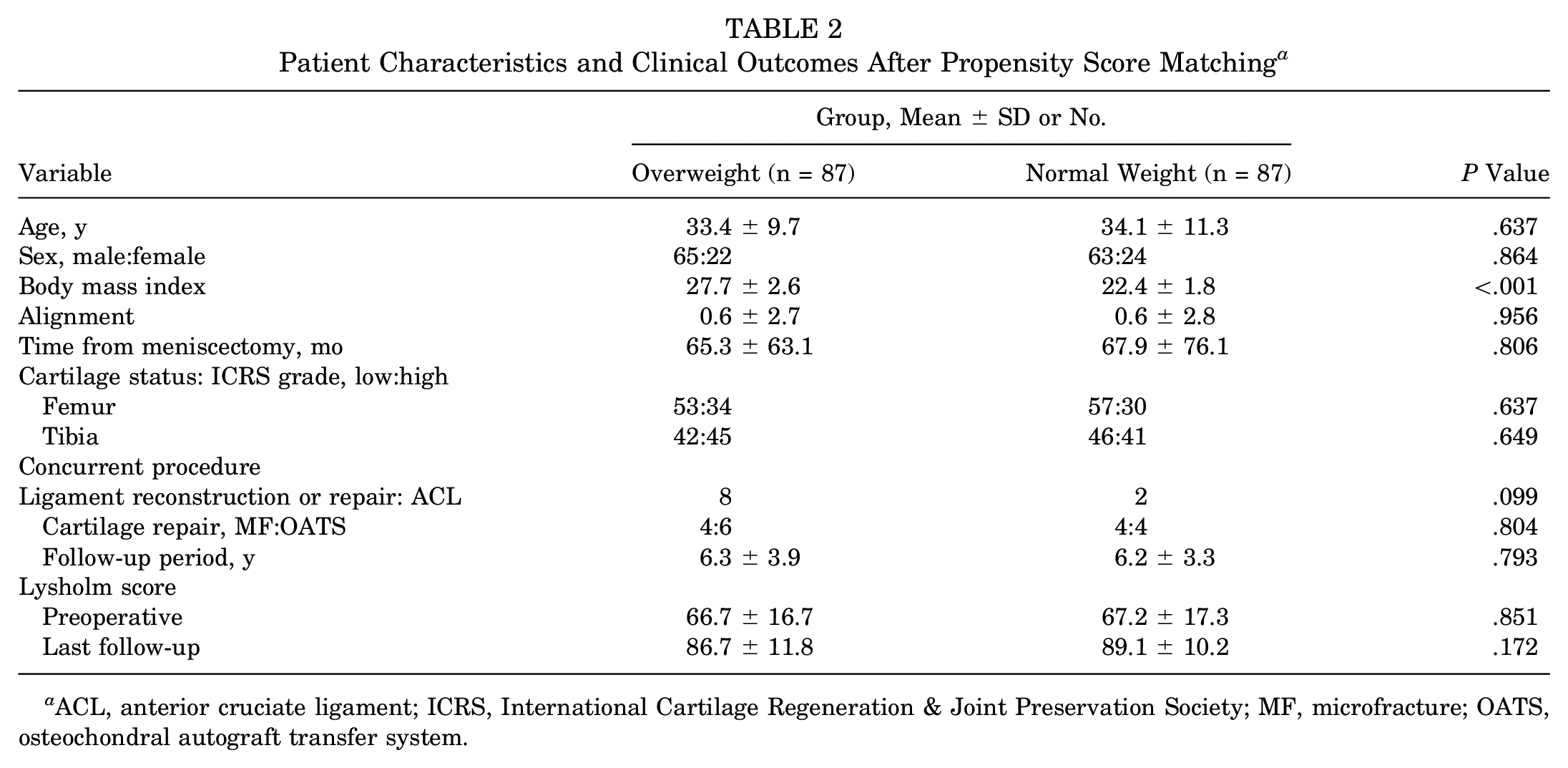
ACL, anterior cruciate ligament; ICRS, International Cartilage Regeneration & Joint Preservation Society; MF, microfracture; OATS, osteochondral autograft transfer system.
Anatomic survival rates in the 2 groups after propensity score matching.
Clinical survival rates in the 2 groups after propensity score matching.
Discussion
In the present study, the mean Lysholm scores at the final follow-up were not significantly different between the overweight and normal weight groups. However, patients who were overweight had inferior anatomic and clinical survival rates after lateral MAT when compared with patients of normal weight. To overcome potential confounding and selection bias attributed to the observational nonrandomized study design, we performed propensity score matching to achieve a more balanced study cohort. After propensity score matching, the anatomic and clinical survival rates were still significantly lower in the overweight group. The results of the present study show that high BMI values adversely affected not only the clinical outcomes but also the actual allograft status after lateral MAT.
There were several differences between previous studies and ours, which suggested that BMI and the outcome of MAT had a significant correlation. Lee et al 9 reported that BMI was a preoperative risk factor for joint space width narrowing after lateral MAT. However, their study did not investigate the relationship between BMI and survivorship after MAT. Jiménez-Garrido et al 3 analyzed the effect of obesity on the outcomes of MAT and found that patients with a BMI ≥30 showed higher clinical failure rates when compared with patients who were nonobese. The previous study found no significant difference in the radiological features of postoperative MRI, although our results showed that the overweight cohort performed poorly with respect to objective outcome on postoperative MRI or second-look arthroscopy. The difference in results between the studies might be justified by the fact that the previous study included a relatively small number of patients (N = 35) and combined medial and lateral MAT. Yet, we enrolled a relatively larger number of patients and focused on lateral MAT. Therefore, it may be more reasonable to assume that a high BMI adversely affected the actual status after lateral MAT. Furthermore, we set the BMI cutoff to 25 as opposed to 30 in the previous study. We measured the additional cutoff BMI by the ROC curves with the survival rates to determine whether the arbitrarily set value of 25 was appropriate. We found that these calculated BMI cutoff values (24.3 and 24.9) were similar to 25 rather than 30. Therefore, the cutoff BMI of 25 might be more reliable when determining the effect of BMI on the survival rates.
Although some studies suggested that there was no significant relationship between BMI and the outcomes of MAT, there were some limitations in arriving at conclusions. Vundelinckx et al 25 reported no evidence of a relationship between BMI and the outcomes. However, the previous study included a small number of patients, and patients who were obese (BMI ≥30) did not undergo transplantation because of their strict indications for MAT. Saltzman et al 18 compared long-term outcomes between patients with a BMI <25 and ≥25. They found that BMI was not a significant factor in predicting favorable long-term outcomes after MAT. The total number of included patients was 22, and only 8 had a normal BMI (ie, less than that of the overweight group). Therefore, the statistical power might be low for demonstrating the correlation because of the small sample size. Yet, in the present study, there was no absolute contraindication of lateral MAT according to BMI, and relatively large numbers of patients (normal weight and overweight) were included.
Our results showed that a high BMI (≥25.0) affected the actual status of the graft after lateral MAT because significant allograft tears or unstable peripheral rim tears occurred more frequently in the overweight cohort. These results were similar in the native meniscus, considering previous studies reporting that a BMI >25 is a significant risk factor for native meniscal tears.2,21 It may be that patients with a high BMI have an increased load on the knee joint, and it could affect the outcome of MAT in terms of meniscal tears or stability. 13 As it has been shown that the compressive force of the knee joint significantly decreased after weight reduction in patients with knee osteoarthritis who were overweight or obese, weight reduction may also help improve the survival rate after lateral MAT.12,13
This study had several limitations. First, its retrospective nature may have led to a selection bias. Therefore, we performed a propensity score matching analysis to reduce bias. Second, because we focused on patients undergoing lateral MAT, our results cannot be applied to patients with medial MAT owing to the differences in the surgical methodology and the functions of the medial and lateral menisci. Third, because we did not have postoperative BMI data, there was a limitation in determining the effect of postoperative BMI. Finally, we used only the Lysholm score for the clinical outcome analysis. However, this is the most commonly used outcome measure for evaluation and has a high level of compliance, making it easy to obtain data over a long period. 20
Conclusion
Although the mean postoperative Lysholm scores were not significantly different between the overweight and normal weight groups, preoperative high BMI was associated with inferior anatomic and clinical survival rates. The results of the current study suggest that weight reduction before surgery for patients who are overweight might improve anatomic and clinical survivorship after lateral MAT.
Footnotes
Submitted November 2, 2022; accepted March 3, 2023.
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.