
Abstract
Background:
Functional restoration of the bone-to-tendon interface (BTI) after rotator cuff repair is a challenge. Therefore, numerous biocompatible biomaterials for promoting BTI healing have been investigated.
Purpose:
To determine the efficacy of scaffolds with spatiotemporal delivery of growth factors (GFs) to accelerate BTI healing after rotator cuff repair.
Study Design:
Controlled laboratory study.
Methods:
An advanced 3-dimensional printing technique was used to fabricate bioactive scaffolds with spatiotemporal delivery of multiple GFs targeting the tendon, fibrocartilage, and bone regions. In total, 50 rabbits were used: 2 nonoperated controls and 48 rabbits with induced chronic rotator cuff tears (RCTs). The animals with RCTs were divided into 3 groups: (A) saline injection, (B) scaffold without GF, and (C) scaffold with GF. To induce chronic models, RCTs were left unrepaired for 6 weeks; then, surgical repairs with or without bioactive scaffolds were performed. For groups B and C, each scaffold was implanted between the bony footprint and the supraspinatus tendon. Four weeks after repair, quantitative real-time polymerase chain reaction and immunofluorescence analyses were performed to evaluate early signs of regenerative healing. Histological, biomechanical, and micro–computed tomography analyses were performed 12 weeks after repair.
Results:
Group C had the highest mRNA expression of collagen type I alpha 1, collagen type III alpha 1, and aggrecan. Immunofluorescence analysis showed the formation of an aggrecan+/collagen II+ fibrocartilaginous matrix at the BTI when repaired with scaffold with GFs. Histologic analysis revealed greater collagen fiber continuity, denser collagen fibers, and a more mature tendon-to-bone junction in GF-embedded scaffolds than those in the other groups. Group C demonstrated the highest load-to-failure ratio, and modulus mapping showed that the distribution of the micromechanical properties of the BTI repaired with GF-embedded scaffolds was comparable with that of the native BTI. Micro–computed tomography analysis identified the highest bone mineral density and bone volume/total volume ratio in group C.
Conclusion:
Bioactive scaffolds with spatially embedded GFs have significant potential to promote the BTI healing of chronic RCTs in a rabbit model.
Clinical Relevance:
The scaffolds with spatiotemporal delivery of GF may serve as an off-the-shelf biomaterial graft to promote the healing of RCTs.
Keywords
Rotator cuff tear (RCT) is a common shoulder disorder among the elderly. 59 Unfortunately, the retear rate continues to be high (up to 90%), despite continuous progress in surgical repair techniques.1,4,13 The native bone-to-tendon interface (BTI) is an exquisitely designed tissue junction comprising a cellular transition from the tendon to a nonmineralized fibrocartilage region to a mineralized fibrocartilage region and ultimately to the bone.35,58 It transfers the stress between mechanically dissimilar materials and sustains the heterotypic cellular communications required for interface function and homeostasis. 32 The BTI reveals a gradual decrease in collagen fiber contents transferring from tendon to bone. 15 This specific gradation allows for seamless distribution of mechanical stress, thus enhancing the strength of the bonding and decreasing the risk of injury or rupture. 2 However, BTI healing is always accompanied by fibrovascular scar tissue formation and loss of its original structure, which decreases mechanical properties and results in high retear rates.3,14,56 Therefore, the ideal outcome of rotator cuff repair mainly consists of the reduction of scar tissue formation and the maximum regeneration of each zone into the native structure.
Biological growth factors (GFs) have been studied extensively for regenerative potential via the promotion of cell recruitment, proliferation, differentiation, extracellular matrix synthesis, and remodeling at the repair site of the rotator cuff.39,42 Although repair with GF augmentations could achieve ideal biomechanical results, it could not reach levels of the native enthesis.18,36,53,55,60 Furthermore, owing to their unstable nature, short half-life, and fast blood clearance, several GFs are not widely applicable clinically, such as vascular endothelial GF 121, platelet-derived GF BB, bone morphogenetic protein 2 (BMP2), and insulin-like GF 1.33,34,38 Therefore, complexities are unresolved—specifically, (1) the GFs or GF combinations that are most suitable for BTI healing and (2) how to achieve the correct spatiotemporal delivery of GFs to each target region to regenerate the native hybrid complex tissue of the BTI while maintaining bioactivity.
Polymer biomaterials have become essential components of regenerative medicine and tissue engineering. In terms of rotator cuff repair, polymer scaffolds have been proposed as a potential approach to promote BTI healing.45,57 Furthermore, the scaffolds can be seeded with stem cells and GFs and delivered to accelerate BTI healing.8,60 Therefore, a specific scaffold that could promote the regeneration of each area in the BTI should be characterized. We recently developed a bioactive 3-dimensional (3D) printed scaffold with spatiotemporally delivered multiple GFs, connective tissue GF (CTGF), transforming GF beta 3 (TGF-β3), and BMP2, designed to promote BTI healing. We delivered CTGF, CTGF + TGF-β3, and BMP2 for tendon, fibrocartilage, and bone regions in the BTI, respectively, using our US-patented advanced 3D-printing technique. The bioactive scaffolds with spatiotemporal delivery of GFs resulted in the reconstruction of native-like BTI in a rodent model of acute RCT.47,50 Despite the promising outcomes, it was pivotal to validate the efficacy of our bioactive scaffolds in healing a clinically relevant chronic RCT model. The present study investigated the potential of 3D-printed bioactive scaffolds for the spatiotemporal delivery of GFs in a well-established chronic RCT rabbit model.10,11,21,26,37,40 We hypothesized that the bioactive scaffolds would have significant potential to promote BTI healing of chronic RCTs.
Methods
GF Selection
CTGF promotes tendon healing by inducing exogenous and endogenous stem cell tenogenic differentiation.22,25 A combination of CTGF and TGF-β3 is an inducer for fibrochondrogenic differentiation potentials of mesenchymal stem cells obtained from different sources. 24 Furthermore, BMP2 is a positive regulator of osteogenic differentiation of mesenchymal stem cells. 9 Therefore, we sought to construct a novel triple-layered scaffold with spatially delivered CTGF, CTGF + TGFβ3, and BMP2 for the tendon-fibrocartilage-bone layer order of BTI healing in a chronic RCT rabbit model.
Fabrication of a 3D-Printed Multilayer GF Scaffold
To guide the restoration of the BTI, we fabricated a 3D-printed triple-layered scaffold containing multiple GFs using a 3D Bioplotter (EnvisionTec) according to our established methods (Figure 1A).27,50 The double-emulsion technique was employed to encapsulate CTGF, TGF-β3, and BMP2 in polylactic-co-glycolic acid microspheres for sustained release according to our established protocols.23,27 The microspheres encapsulated with CTGF and BMP2 were printed as embedded in polycaprolactone microstrands at the top and bottom layers of the scaffold, respectively. The microspheres encapsulated with CTGF and TGF-β3 were embedded in polycaprolactone microstrands printed on the middle layer. The top layer facing the tendon region during surgery was designed to accelerate tendon restoration; the bottom layer facing the supraspinatus tendon (SST) footprint, for bone restoration; and the middle layer, for fibrocartilage restoration. The fabricated scaffolds were in the form of a thin membrane suitable for surgical implantation (Figure 1B). Throughout the printing process, the distance between adjacent electrodes ranged from 300 to 400 μm, and each strand diameter ranging from 200 to 400 μm was maintained. The same approach was used to fabricate scaffolds without GF. The printed scaffolds were surface treated with 6M NaOH for 4 hours to control the release of the GFs and scaffold degradation in vivo.5,50 The bioactivities of the scaffolds were confirmed via regionally induced multilineage differentiation of human mesenchymal stem/progenitor cells as reported in our previous study. 47 The release kinetics of the GFs were also reported in our previous study. 47
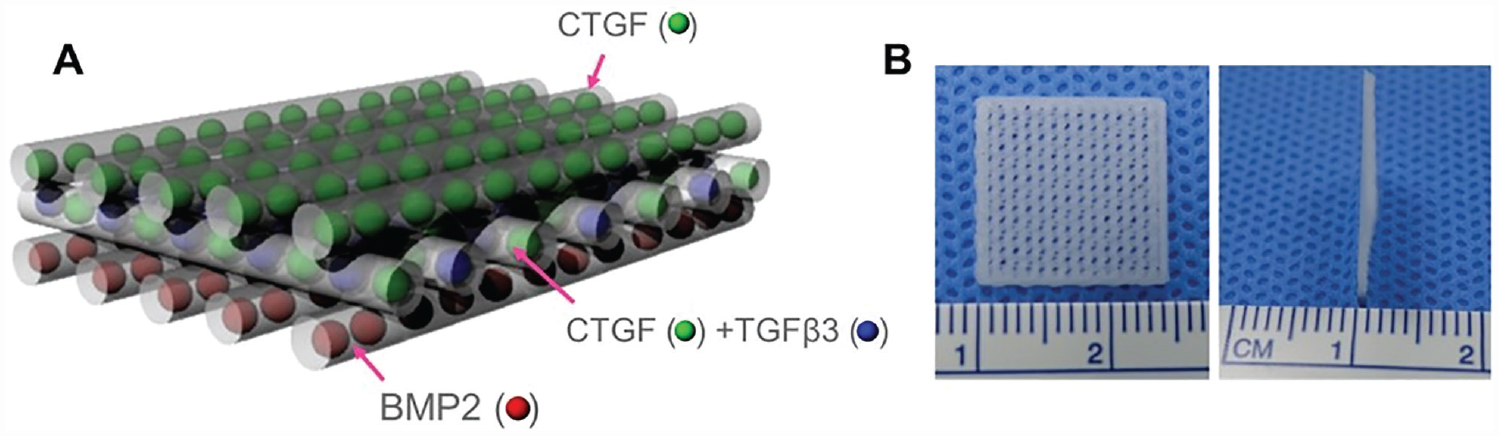
(A) Bioactive scaffolds were designed as triple layer. The top layer (facing the tendon region) was embedded with CTGF µS; the middle layer, with CTGF µS and TGF-β3 µS; and the bottom layer (facing the supraspinatus tendon footprint), with BMP2 µS. (B) The scaffold dimensions were set to 1.5 cm × 1.5 cm × 1.0 mm (length × width × thickness) to fit the rabbit supraspinatus footprint. BMP2, bone morphogenetic protein 2; CTGF, connective tissue growth factor; TGF-β3, transforming growth factors beta 3; µS, microsphere.
Chronic RCT in a Rabbit Model
All the animal experimental procedures were approved by the Institutional Animal Care and Use Committee of the Clinical Research Institute (Seoul National University Bundang Hospital, No. BA-2106-322-061-02). A total of 48 male New Zealand White rabbits (5 months old; weight, 2.8-3.0 kg) were randomly divided into 3 groups: saline injection (group A; n = 16), scaffold without GF (group B; n = 16), and scaffolds with GFs (group C; n = 16). Power calculations from our previous study 26 revealed that a minimum sample size of 6 per group is required for every time point of euthanasia to detect any significant difference in biomechanical values (mean difference, 15.2 N/kg; α error = .05; β error = 0.1). Furthermore, considering an assumed dropout rate of 25%, at least 8 rabbits per group were required at each euthanasia time point. Two normal rabbits that did not undergo any procedures were enrolled and served as healthy controls (Figure 2).
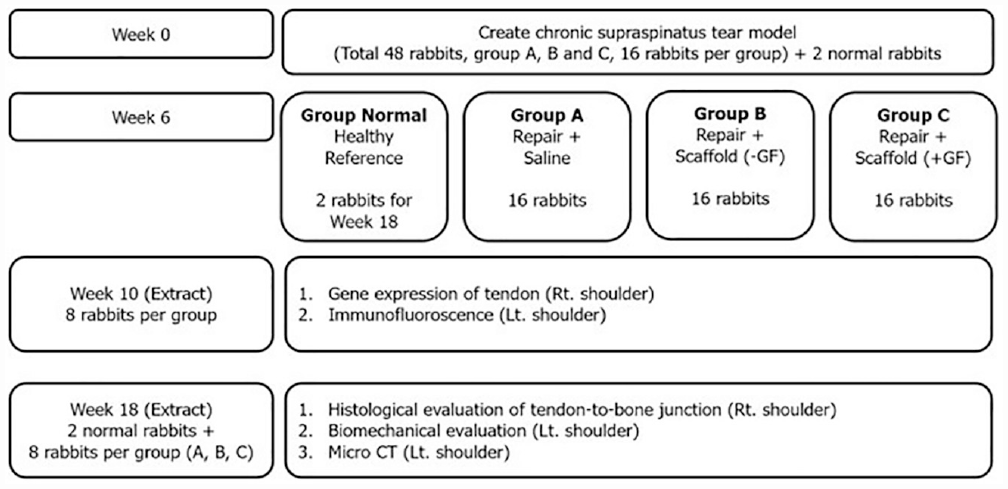
Schematic of the experimental workflow. CT, computed tomography; GF, growth factor; Lt., left; Rt., right.
A longitudinal skin and fascia incision of 5 cm was made bilaterally over the relatively large tuberosity. After retraction of the deltoid muscle, the insertion of the SST at the greater tuberosity was sharply transected using a scalpel. The entire tendon was wrapped with a 10 mm–long silicon Penrose drain (outer diameter, 8 mm; Yushin Corp). According to our established methods for creating chronic RCTs in rabbit models,10,11,21,26,37,40 the drain was removed 6 weeks after repair, and the status of chronic SST tear was determined (Figure 3A), followed by surgical repair. The soft tissue and fibrocartilage left on the greater tuberosity were debrided, and decortication was performed with a No. 11 blade scalpel. Four tunnels were made transversely through the proximal part of the humerus using a 1.0-mm drill (Multipro 395; Dremel). The sutures (2-0 Ticron; Tyco Healthcare) were then passed through the drill hole, and the tendon was reopposed to its anatomic site in a transosseous manner. Before the sutures were tightened, a scaffold with dimensions of 10 × 3 × 1 mm (length × width × thickness) was administered into the BTI in groups B and C. Subsequently, the sutures were compressively tied over the scaffold (Figure 3B).
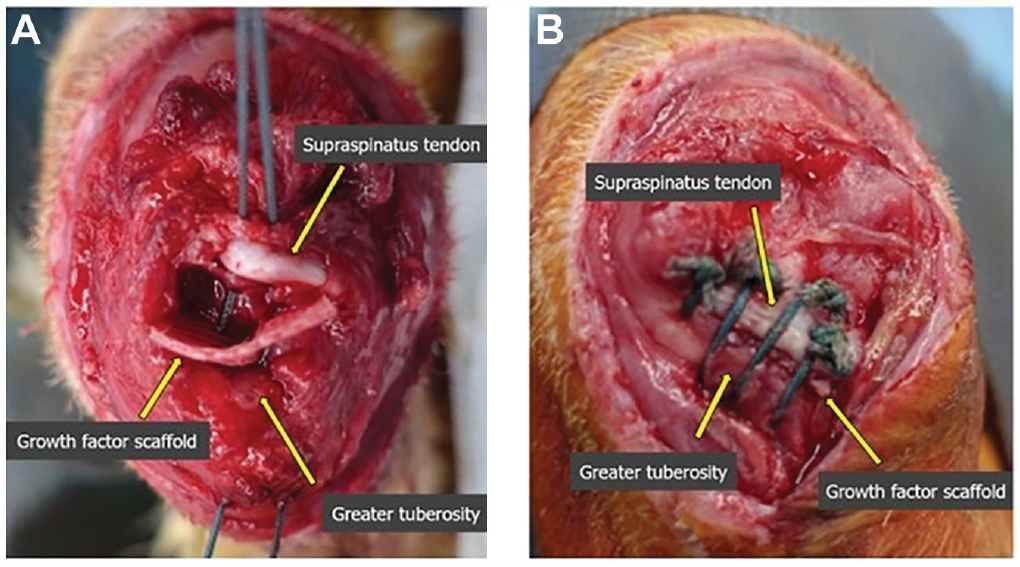
Repair procedures were performed in a transosseous manner with 4 simple stitches. (A) Two main suture ends for the medial row and lateral row were passed through the 4 bone tunnels. (B) Each suture end was then tied over the supraspinatus tendon, followed by 2 subsutures on either side of the main sutures to reattach enough tendon portion to the scaffold.
Polymerase Chain Reaction Analysis for mRNA Expression of Repaired Tissue in the BTI
For genetic evaluation, total RNA was extracted from SST tissue obtained from the right shoulder of each rabbit in the fourth week after repair, using TRIzol reagent (Invitrogen) according to the manufacturer’s protocol. For cDNA synthesis, 1 μg of total RNA and the AMV First-Strand cDNA Synthesis Kit (Invitrogen) were used. Quantitative real-time polymerase chain reaction (qRT-PCR) was performed using the SYBR Green PCR Master Mix (Applied Biosystems) and QuantStudio 6 Flex Real-Time PCR System. Polymerase chain reaction was performed under the following conditions: denaturing at 95°C for 10 minutes, followed by 40 cycles of denaturation at 95°C for 15 seconds and annealing at 60°C for 60 seconds without extension. These steps were repeated to calculate linear phase values. The relative gene expression levels were analyzed via the 2-ΔΔCT method using glyceraldehyde-3-phosphate dehydrogenase (GAPDH) as a housekeeping gene. 31 The sequences of the gene-specific primers (Bioneer Corporation) are listed in Table 1. The entire procedure was performed by an independent experimenter who was blinded to the group (H.J.J.).
Primer Sequences of Genes Used for the Quantitative Real-Time Polymerase Chain Reaction Analysis at 4 Weeks After Surgery a
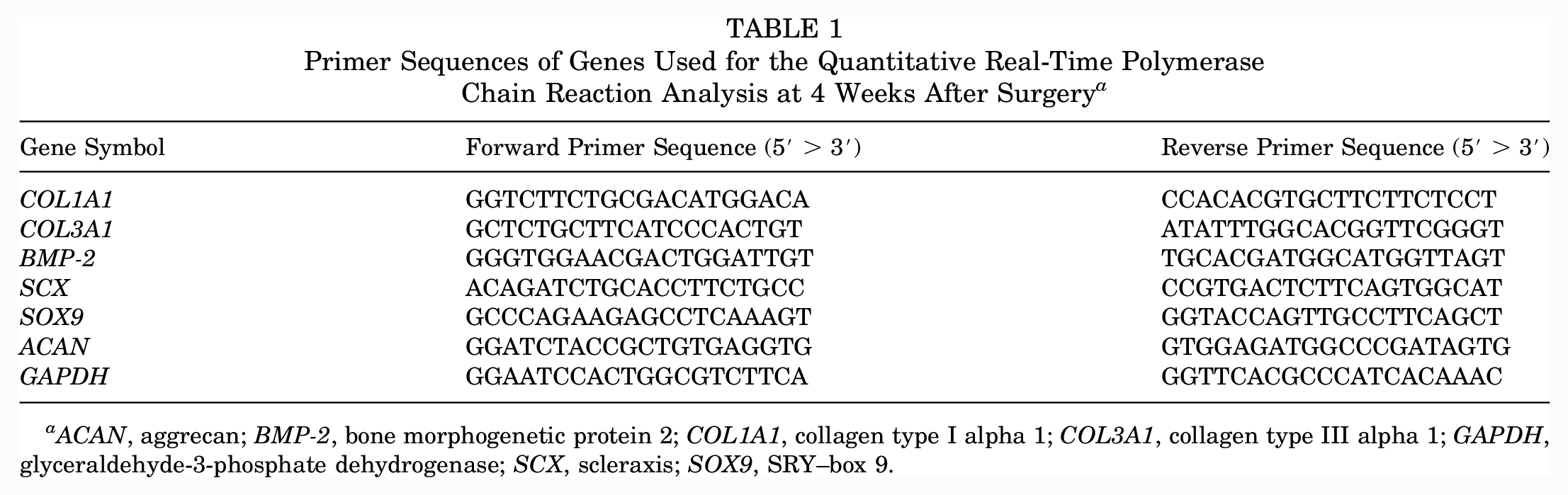
ACAN, aggrecan; BMP-2, bone morphogenetic protein 2; COL1A1, collagen type I alpha 1; COL3A1, collagen type III alpha 1; GAPDH, glyceraldehyde-3-phosphate dehydrogenase; SCX, scleraxis; SOX9, SRY–box 9.
Immunofluorescence Analysis for the Regenerative Component of BTI
To assess the formation of a fibrocartilaginous matrix at the BTI,20,41 we evaluated the expression of collagen type II and aggrecan by immunofluorescence using our well-established methods.22,24,47,48 The BTI specimens harvested from the left shoulder of each rabbit in the fourth week after repair were fixed in 10% formalin, and embedded in paraffin and then sectioned. After removal of the paraffin layer and rehydration, the sections were boiled for 15 minutes in a sodium citrate solution for antigen retrieval. The tissue sections were blocked with 5% normal goat serum (Vector Laboratories) in 0.3% Triton X-100 in phosphate-buffered saline for 1 hour at room temperature. After incubating overnight at 4°C with antibodies for collagen II (NB600-844; Novus Biological) and aggrecan (MA3-16888; Thermo Fisher Scientific), the samples were washed with phosphate-buffered saline/Triton.
Then the samples were incubated for 1 hour at room temperature with Alexa Fluor 488 and 568 isotope-matching secondary antibodies (Thermo Fisher Scientific) for aggrecan and collagen II, respectively. Nuclei were stained with DAPI for 15 minutes.
Histologic Analysis for the Healing Integrity of Each Area in the BTI
The specimens collected from the right shoulder of each rabbit in the 12th week after repair were fixed with 10% buffered neutral formalin overnight, decalcified in hydrochloric acid (Surgipath Decalcifier II; Leica Biosystems) for 8 to 12 hours, and then embedded in paraffin. Formalin-fixed paraffin-embedded sections were deparaffinized in xylene and rehydrated. The 5 µm–thick sections were stained with hematoxylin and eosin, alcian blue, and picrosirius red according to well-established protocols. 22 Picrosirius red–stained sections were also imaged using polarized microscopy to evaluate collagen organization and alignment. In addition, the vascularity, cellularity, continuity, and density of the collagen fiber and maturation of the BTI structure were quantitatively evaluated by 2 blinded examiners (S.C.H. and Y.K.K.) in accordance with the semiquantitative grading system (graded 0-3) as reported in a previous study. 10 Digital images from stained sections were obtained using a Coolpix 995 camera (Nikon) connected to an Eclipse E200 microscope (Nikon).
Collagen Fiber Orientation Analysis
To quantify the fibrous collagen fiber orientation in the BTI area, we performed digital image processing using FiberFit software. The fiber dispersion parameters of each group were calculated using picrosirius red–polarized images of the BTI area. For every group, 3 polarized images were obtained and subjected to 8-bit digitization using ImageJ software (National Institutes of Health) at a resolution of 1360 × 1024 pixels.
Nanoindentation-Based Micromodulus Mapping
Mechanical modulus mapping was conducted using a PIUMA nanoindenter (Optics11) with unfixed and unstained tissue slide samples and applied using a probe radius of 9 µm with a maximum force of 10 mN. To determine the effective indentation modulus (EEff) at the BTI area, we measured every 20 µm using an embedded high-resolution mobile X-V stage. The collected modulus data were processed via MATLAB (R2022b) to create x-, y-, and z-axis graph maps, according to a previous method. 49
Biomechanical Analysis for Healing Strength of the Repaired Rotator Cuff
Tensile tests were performed on the BTI tissues harvested from the left shoulder of each rabbit using a universal materials testing machine (AGS-X; Shimadzu) as previously reported.16,21 The specimens were kept hydrated in saline solution during preparation and were wrapped in gauze, wetted with saline solution, maintained in plastic film, and stored at −20°C. On the testing day, the specimens were thawed at room temperature and placed in 2 fixation units (Figure 4). Before the tensile test, the specimen was preloaded with a static preload of 5 N for 5 seconds, and 5 preconditioning cycles were conducted from an initial preload of 5 N to a peak load of 50 N at a loading rate of 15 N/s. It was then elongated at a rate of 1 mm/s until failure. Throughout the test, the tendons were kept moist by physiologic saline solution spray. The maximum tensile force and stiffness were derived from load displacement plots following previously established protocols.10,51 The absorbable extent and biodegradable capacity of the scaffold were confirmed after the test.
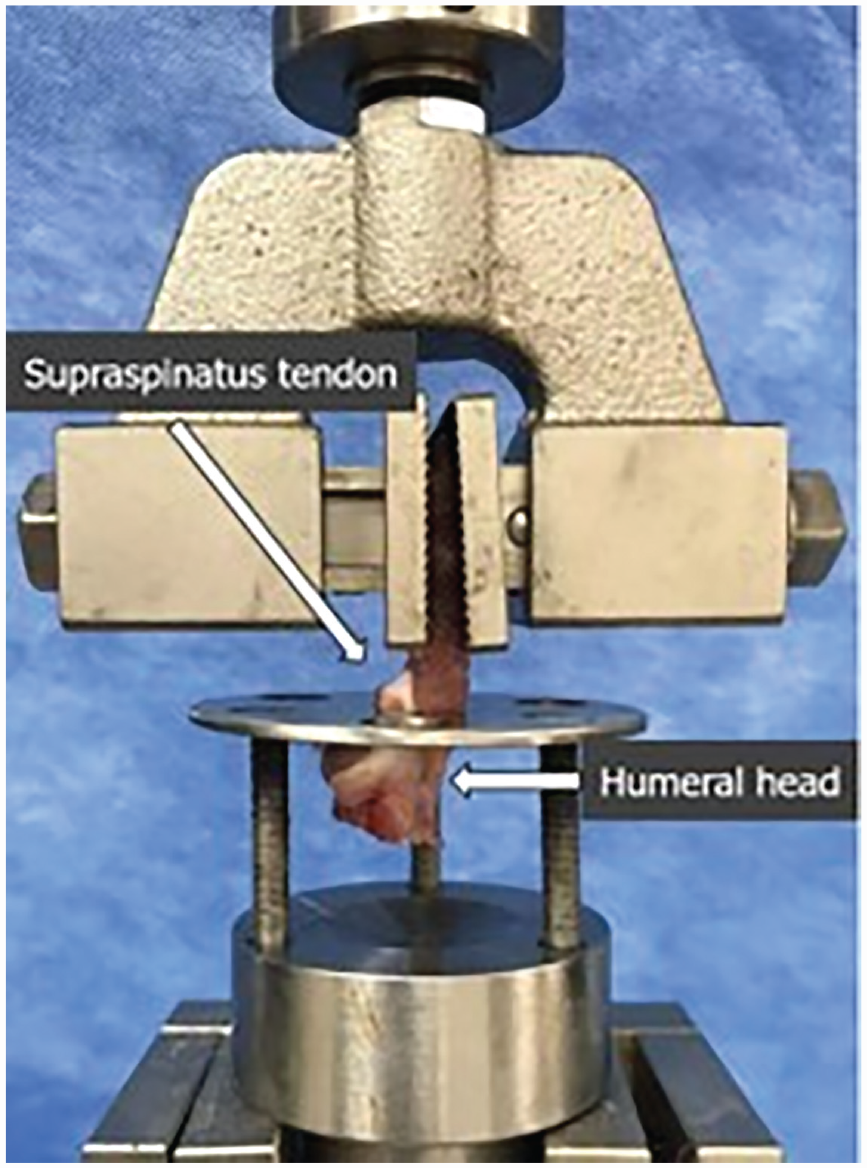
Each end of the harvested specimen was positioned at the upper and lower fixation unit in a universal materials testing system.
Micro–Computed Tomography Analysis for Regeneration of the BTI Bone Layer
After biomechanical testing, micro–computed tomography (micro-CT) analysis was performed on the remaining proximal humeral bone harvested from the left shoulder. The adherent soft tissue was cleaned off, and humeral specimens were fixed in a 1:1 solution of ethanol and sterile water at room temperature for 24 hours. The bone mineral density and bone volume fraction (bone volume/total volume) of the humeral head at the SST footprint were assessed using a desktop micro-CT system (model 1076; SkyScan). The micro-CT was performed at 40 kV and 170 mA; the integration time was 300 milliseconds; and the resolution was 18.22 μm according to the established protocol. 29 SkyScan software was used for imaging and analysis of data. After the 3D-reconstructed image was obtained, a customized 10 × 10–mm cylindrical region of interest was centered at the surface of the SST repair site. The associated parameters were calculated using ImageJ software (National Institutes of Health) by an orthopaedic surgeon not involved in the study.
Statistical Analysis
One-way analysis of variance with post hoc Tukey honestly significant difference tests was performed for all quantitative data. The Kruskal-Wallis test was used to evaluate the data, followed by the post hoc Mann-Whitney U test. All statistical analyses were conducted in a blind manner by an independent statistician (J.Y.C.) using SPSS (Version 23.0; IBM), and P values <.05 were considered statistically significant.
Results
No animals showed signs of sepsis or wound infection throughout the experimental period. The scaffolds harvested at 4 weeks after repair demonstrated remarkable integration with newly formed tissues, with some retaining the scaffold structure (Figure 5A). After 12 weeks, the scaffolds were fully degraded and replaced with the newly formed tissue (Figure 5B). Macroscopic observations revealed no notable difference between the scaffolds with and without GFs.
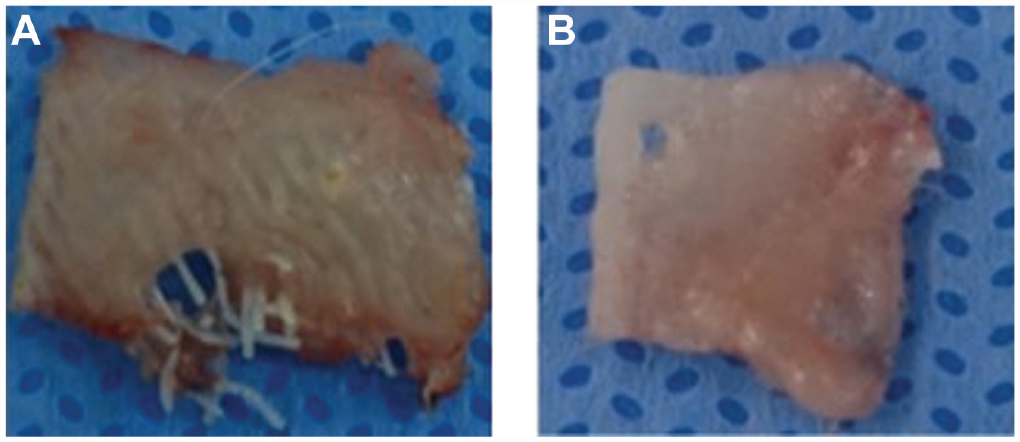
(A) Scaffold extracted from the tendon-bone interface of the right shoulder 4 weeks after the repair consistently failed to be absorbed within short periods. (B) Scaffold peeled off from the tendon after the biomechanical test 12 weeks after the repair appears almost totally absorbed.
QRT-PCR Analysis for mRNA Expression of Repaired Tissue in the BTI
qRT-PCR analysis showed that the mRNA expression levels of COL1A1, COL3A1, and ACAN were higher (P < .001, P = .005, and P = .006, respectively) in group C at 4 weeks after repair than in the other 2 groups (Table 2). The mRNA expression levels of BMP-2, SCX, and SOX9 demonstrated similar patterns among the 3 groups but without statistical significance.
Quantitative Real-Time Polymerase Chain Reaction Analysis Results at 4 Weeks a
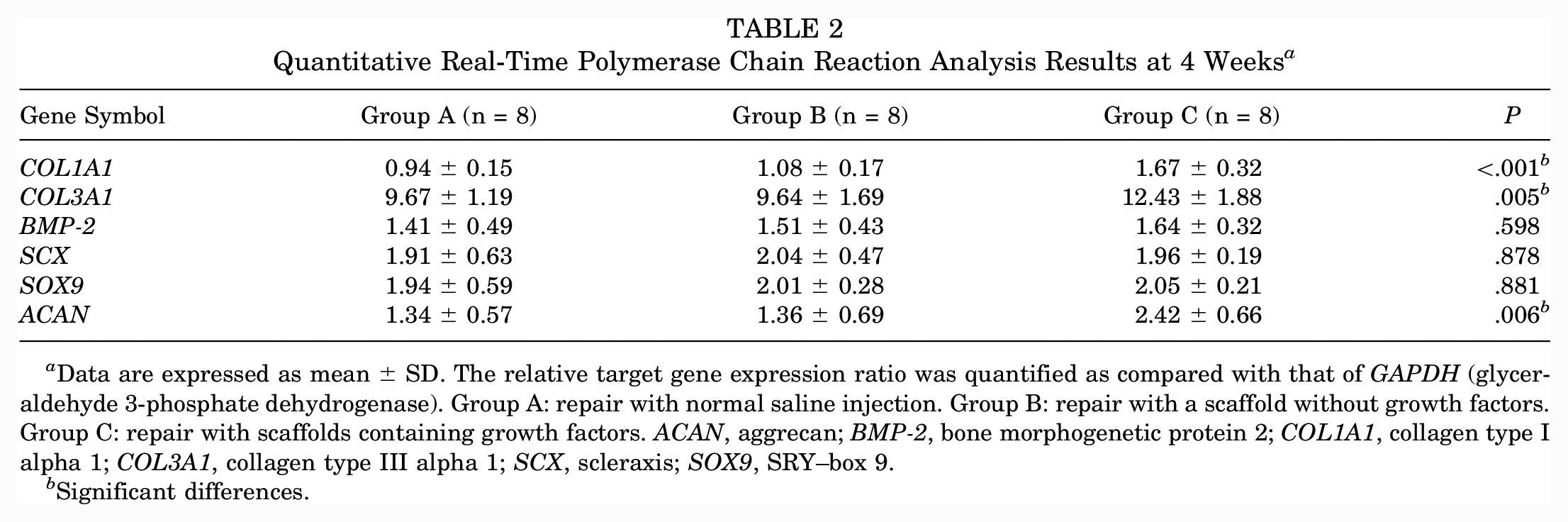
Data are expressed as mean ± SD. The relative target gene expression ratio was quantified as compared with that of GAPDH (glyceraldehyde 3-phosphate dehydrogenase). Group A: repair with normal saline injection. Group B: repair with a scaffold without growth factors. Group C: repair with scaffolds containing growth factors. ACAN, aggrecan; BMP-2, bone morphogenetic protein 2; COL1A1, collagen type I alpha 1; COL3A1, collagen type III alpha 1; SCX, scleraxis; SOX9, SRY–box 9.
Significant differences.
Immunofluorescence Analysis for the Regenerative Component of the BTI
Native BTI tissues showed a fibrocartilaginous matrix with abundant aggrecan and collagen II expression (Figure 6, A and E). Similarly, there was more preliminary formation of a fibrocartilaginous tissue matrix positive for aggrecan and collagen II in group C (Figure 6, D and H). In contrast, groups A and B demonstrated fibrous tissue healing with a lack of aggrecan and collagen II expression (Figure 6, B, C, F, G).
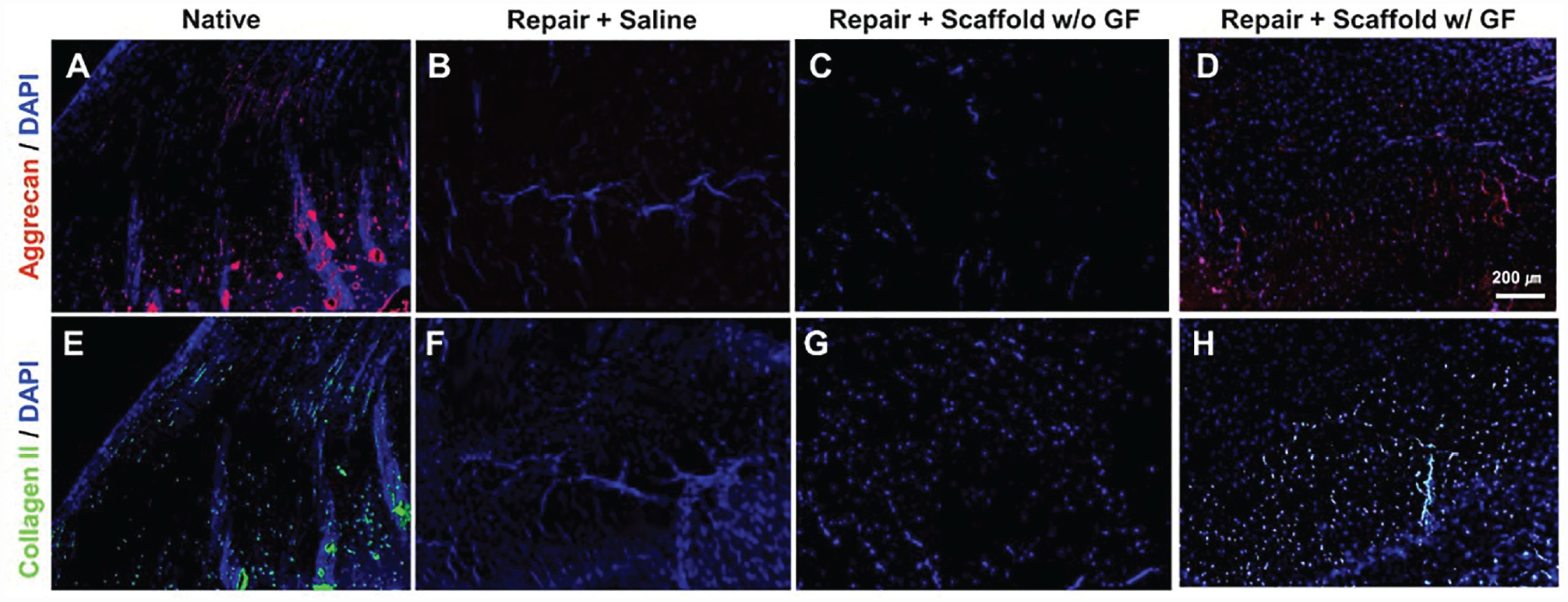
Representative immunofluorescence images of tendon-bone interface sections at 4 weeks after repair. (A) Aggrecan expression was notable at the BTI region of native tissue. However, (B) RCR with saline and (C) scaffold without GF showed no aggrecan expression. (D) RCR with GF-embedded scaffolds demonstrated aggrecan expression at the BTI region. Similarly, the native BTI region had (E) collagen II expression but not with (F) RCR with saline and (G) scaffold without GF. (H) RCR with GF-embedded scaffold showed collagen II expression at the BTI region. BTI, bone-to-tendon interface; GF, growth factor; RCR, rotator cuff repair; w/, with; w/o, without.
Histologic Analysis for Healing Integrity of Each Area in the BTI
Hematoxylin and eosin–stained sections revealed notable collagen organization and reconstruction of the native BTI-like multitissue interface in group C (Figure 7). Groups A and B exhibited disrupted fibrovascular healing. Alcian blue staining confirmed the reconstruction of the fibrocartilaginous BTI in group C, similar to the native tissue, whereas groups A and B had a lack of a fibrocartilaginous matrix. Picrosirius red staining with polarized microscopy revealed densely aligned collagen fibers in the tendon region in group C, similar to native tissues. Groups A and B showed disrupted collagen fiber orientation.
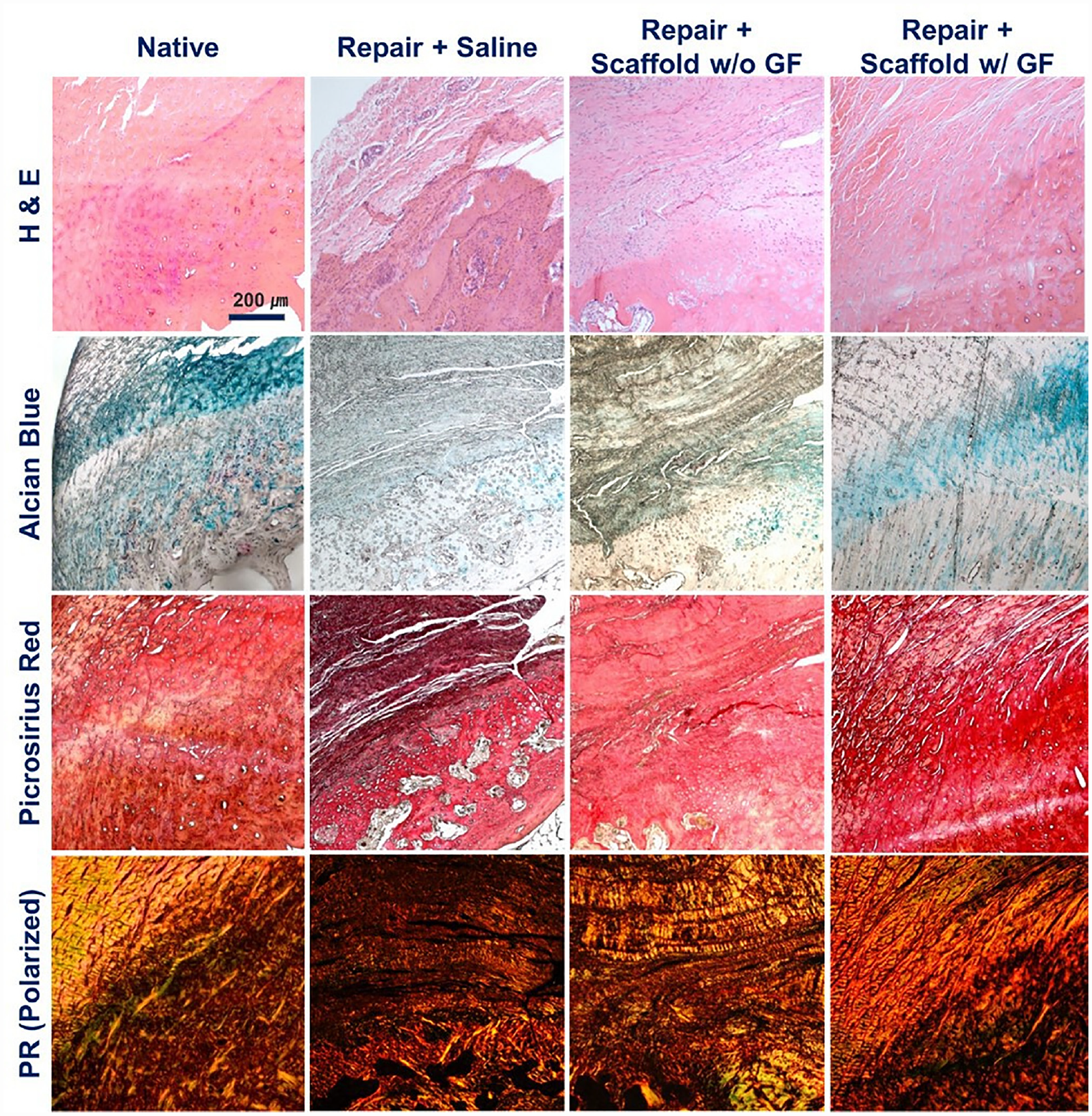
Representative histology of BTI sections stained with hematoxylin and eosin (H&E), alcian blue, picrosirius red (PR), and PR with polarized microscopy at 12 weeks after repair. Notable reorganization of collagen fibers was observed in native tissue and the repaired tissue with GF-embedded scaffolds. In contrast, the groups with saline repair and scaffolds without GF had disoriented fibrous healing. In addition, alcian blue staining showed the fibrocartilaginous BTI interface in the native tissues and repaired tissues with GF-embedded scaffolds. However, saline repair and scaffolds without GF resulted in fibrous scar–like healing without alcian blue–positive fibrocartilaginous matrix. BTI, tendon-bone interface; GF, growth factor; w/, with; w/o, without.
The semiquantitative histology scores (Table 3) showed no statistically significant differences in the extent of vascularization and cellularization among the groups (P = .237 and P = .202, respectively). Collagen fiber continuity in group C was similar to that in the native tissue and was significantly higher than that in the other 2 groups 12 weeks after repair (P = .004). Similarly, the density and maturation of collagen fibers were significantly higher in group C than in groups A and B (P = .002 and P = .004, respectively).
Histologic Scoring for the Tendon-to-Bone Interface in All Groups at 12 Weeks After Repair a
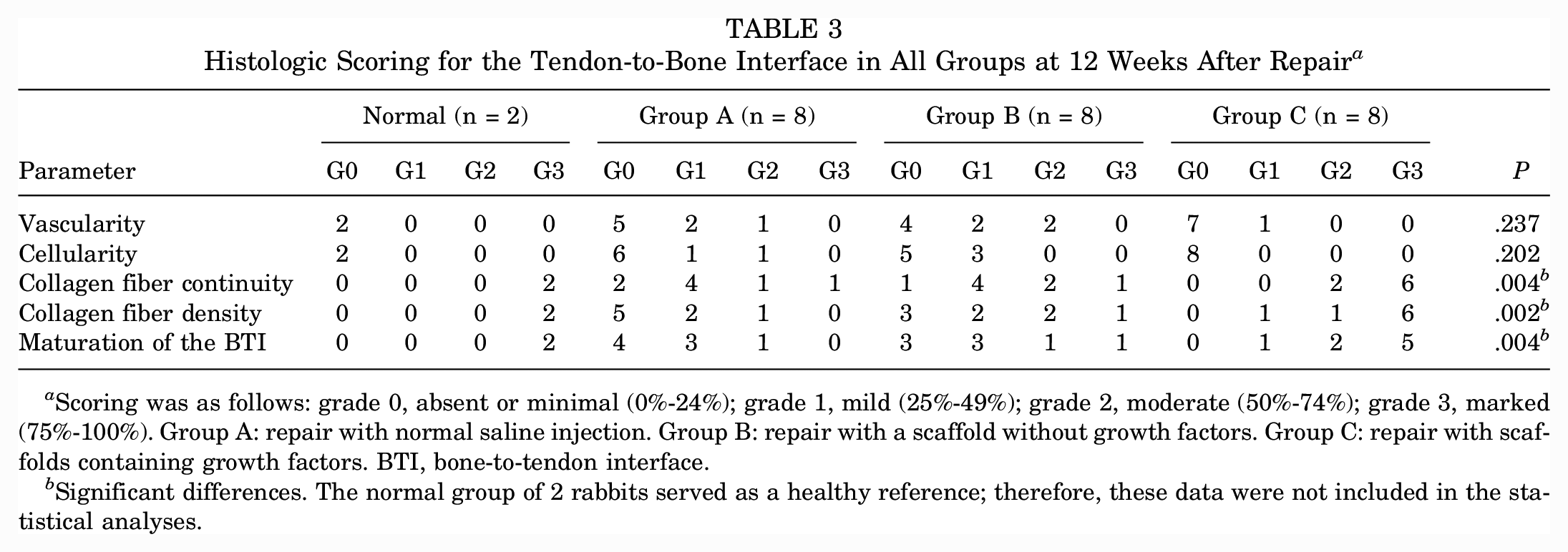
Scoring was as follows: grade 0, absent or minimal (0%-24%); grade 1, mild (25%-49%); grade 2, moderate (50%-74%); grade 3, marked (75%-100%). Group A: repair with normal saline injection. Group B: repair with a scaffold without growth factors. Group C: repair with scaffolds containing growth factors. BTI, bone-to-tendon interface.
Significant differences. The normal group of 2 rabbits served as a healthy reference; therefore, these data were not included in the statistical analyses.
Quantitative Analysis of Collagen Fiber Orientation
From the polarized images of picrosirius red–stained sections, we quantitatively analyzed collagen fiber orientation using the FiberFit software (Figure 8). Native and repaired BTI with bioactive scaffolds embedded with GFs showed narrowed histograms of the fiber angles (Figure 8, A and D), indicating densely aligned collagen fibers. In contrast, tissue repair with saline and scaffolds without GF resulted in a spread histogram, indicative of disoriented collagen fibers (Figure 8, B and C). Quantitatively, the fiber dispersion parameter (K), an indicator of collagen fiber orientation, was significantly higher in the native group and group C than in groups A and B (P < .0001) (Figure 8E).
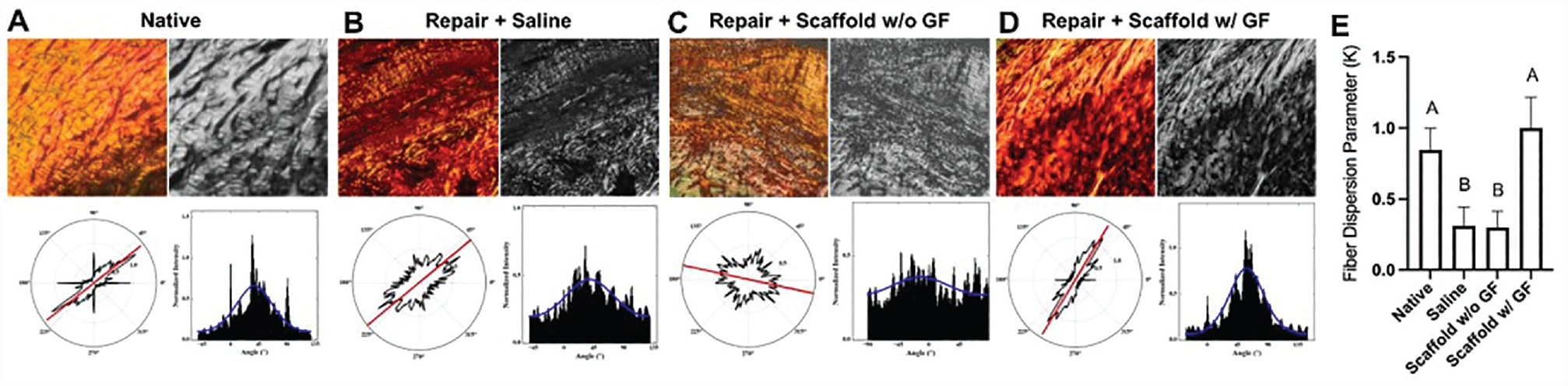
Quantitative analysis of collagen fiber orientation using FiberFit Software with polarized picrosirius red images. (A) Native and (D) repaired tissues with scaffold embedded with GFs showed narrowed histograms of fiber angles, suggesting densely aligned collagen fibers as compared with dispersed fiber orientation observed in the groups of (B) saline repair and (C) scaffold without GF. (E) Fiber dispersion parameter, K, was significantly higher in native tissue and scaffold with GF than saline repair and scaffold without GF (n = 5 per group; Different letters indicate statistically significant differences [P < .0001]). Data are presented as mean ± SD. GF, growth factor; w/, with; w/o, without.
Biomechanical Analysis for Healing Strength of the Repaired Rotator Cuff
There were no differences in body weight among the 3 experimental groups (P = .153) (Table 4). For the tensile test, the ultimate values of load to failure were as follows (mean ± SD): normal group, 59.2 ± 0.3 N/kg; group A, 36.2 ± 8.5 N/kg; group B, 38.1 ± 8.8 N/kg; and group C, 51.9 ± 7.1 N/kg. Group C had the highest load-to-failure value (P = .003). Although the results failed to reach normal levels, according to the Bonferroni post hoc test, there were differences between groups A and C (P = .005) and groups B and C (P = .012). Yet, there was no difference between groups A and B (P = .9). Stiffness was significantly lower in the experimental groups than the normal group and showed no differences among the 3 groups (P = .981). According to the failure mode analysis in a previous study, midsubstance tearing suggested strong BTI healing. 54 Owing to well-healed repaired tendons in all experimental groups, the study revealed high proportions of midsubstance tendon tears that included 3 insertional tears and 5 midsubstance tears (62.5%) in group A, 3 insertional tears and 5 midsubstance tears (62.5%) in group B, and 2 insertional tears and 6 midsubstance tears (75.0%) in group C. However, there was no statistical difference (P = .604).
Biomechanical Analysis Results in All Groups at 12 Weeks After Repair a
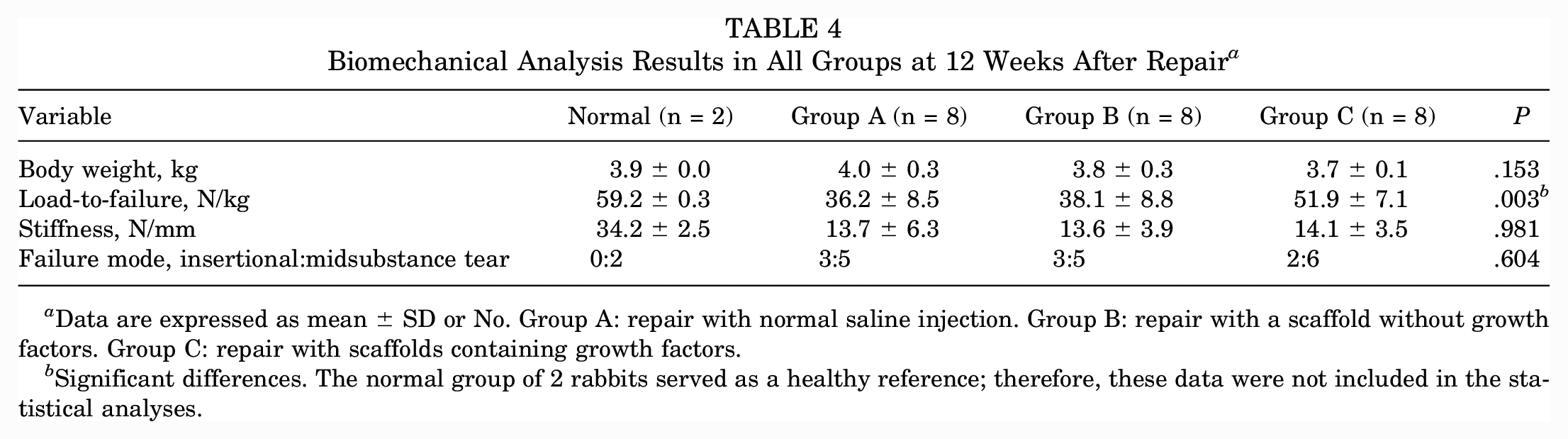
Data are expressed as mean ± SD or No. Group A: repair with normal saline injection. Group B: repair with a scaffold without growth factors. Group C: repair with scaffolds containing growth factors.
Significant differences. The normal group of 2 rabbits served as a healthy reference; therefore, these data were not included in the statistical analyses.
Modulus Mapping by Nanoindentation
Nanoindentation-based mapping of effective modulus (EEff) showed a gradient transition from soft to hard tissue in the native BTI region (Figure 9). Similar patterns were observed in EEff distribution and magnitude in tissues repaired with scaffolds embedded with GFs. In contrast, tissue repair with saline (group A) and scaffolds without GF (group B) had an acute increase in EEff in the repaired BTI region, likely associated with a disrupted collagen matrix.
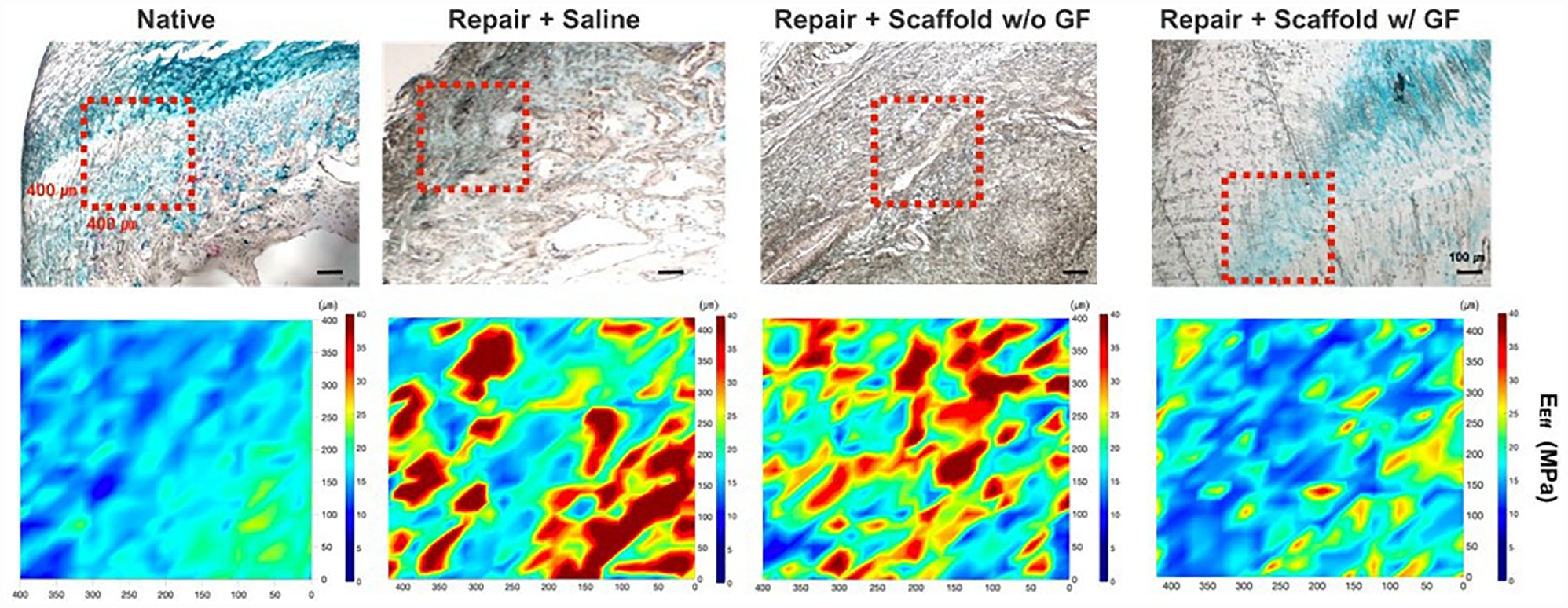
Modulus mapping by nanoindentation. Native BTI shows a gradient transition from soft to hard region. Repaired tissue with scaffolds delivered with GFs demonstrated a similar pattern of EEff magnitude at the BTI region. However, the saline-repaired group and repaired tissue with scaffolds without GF had large areas with acute increases in EEff, likely indicative of pathologic healing. BTI, bone-to-tendon interface; EEff, effective modulus; GF, growth factor; w/, with; w/o, without.
Micro-CT Analysis for Regeneration of the BTI Bone Layer
Despite failing to reach normal levels, the healing interface of group C was more optimally shaped than that in the other 2 groups (Figure 10). The results indicated that the bone mineral density and bone volume fraction of group C were higher than those of the other 2 groups (P = .001 and P < .001, respectively) (Table 5) at 12 weeks postoperatively.
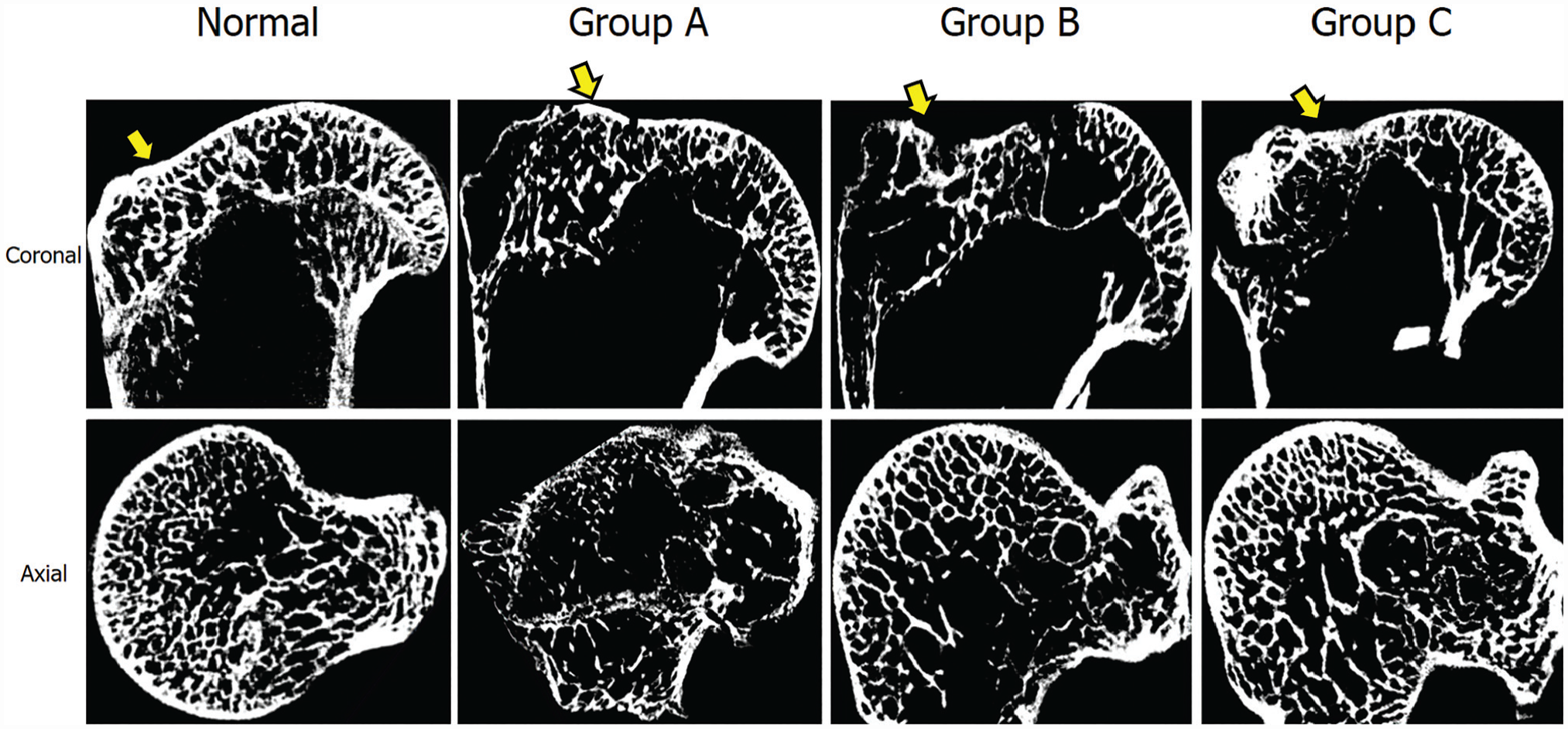
Micro–computed tomography images (coronal and axial views) show the structure of the proximal humerus at 12 weeks after repair. Group A: repair with normal saline injection. Group B: repair + scaffold without growth factors. Group C: repair + scaffold with growth factors. Yellow arrows indicate the tendon attachment sites.
Micro-CT Analysis Result in All Groups at 12 Weeks After Repair a
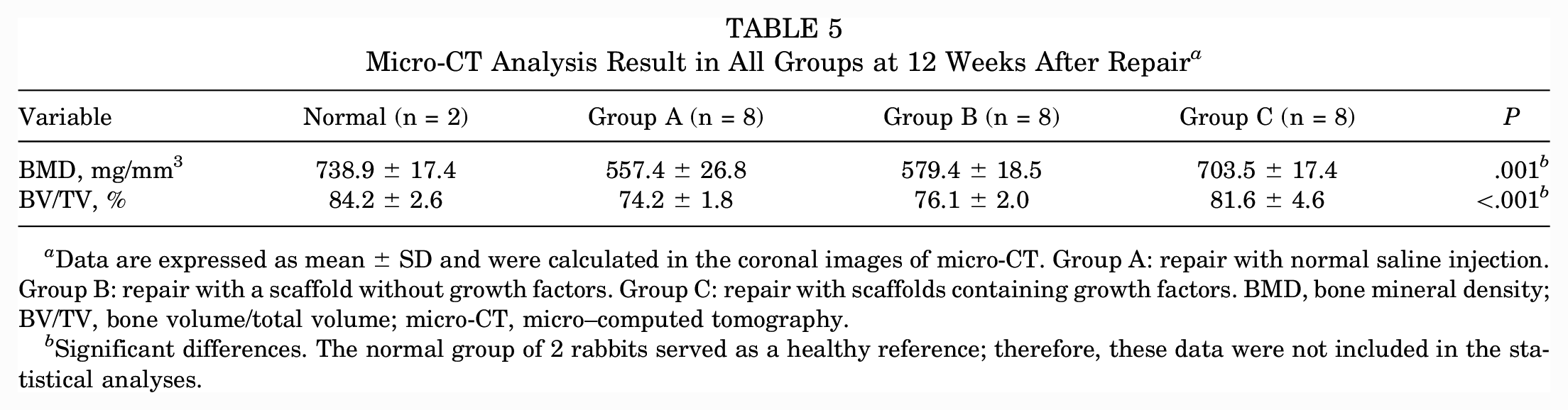
Data are expressed as mean ± SD and were calculated in the coronal images of micro-CT. Group A: repair with normal saline injection. Group B: repair with a scaffold without growth factors. Group C: repair with scaffolds containing growth factors. BMD, bone mineral density; BV/TV, bone volume/total volume; micro-CT, micro–computed tomography.
Significant differences. The normal group of 2 rabbits served as a healthy reference; therefore, these data were not included in the statistical analyses.
Discussion
Our findings suggested that the novel 3D-printed bioactive scaffold with spatiotemporal delivery of GFs significantly improved the outcomes of chronic rotator cuff repair. Histologic findings, qRT-PCR results, immunofluorescence, digital imaging processing of collagen alignment, micro-CT, and multiscale mechanical analyses collectively supported the potential of our 3D-printed bioactive scaffold in the reconstruction of the functional BTI after the repair of chronic RCT.
Various GFs play important roles in tendon enthesis healing by modulating multiple signaling pathways in various types of endogenous cells in a spatial and temporal manner.12,18,36,53,55,60 Given the complexity, direct injection of GFs has resulted in controversial outcomes in vivo. 19 Moreover, the rapid diffusion of injected GFs frequently attenuates biological effects on target tissues. 19 To address challenges, various controlled delivery systems have been developed that may provide localized and sustained bioactivity, leading to tissue healing.12,17,19,45 Our bioactive scaffolds embedded with a spatiotemporal delivery system were designed to guide the reconstruction of the microscale multitissue gradient at the BTI. Sustained and localized release of the 3 GFs successfully induced healing of native-like multitissue BTI. Our US-patented (US20230021383) advanced 3D-printing technique enables microprecise control of the delivery of multiple GFs, which can be applied to heal other complex tissues.
Previous studies demonstrated that CTGF is a potent cue for tendon regeneration because it can induce the recruitment of endogenous stem/progenitor cells and their tenogenic differentiation via FAK/ERK1/2 signaling.22,25,30 CTGF also shows specificity to CD146+ perivascular-originated tendon stem/progenitor cells.22,48 Rui et al 43 reported that CTGF restored the regenerative capacity of aged tendon-derived stem/progenitor cells. Importantly, CTGF-stimulated tendon stem/progenitor cells could regulate inflammation by secreting interleukin–10 via STAT3 signaling. 48 These properties make CTGF a unique fibrogenic cue that promotes the healing of acute and chronic tendon injuries. Our data consistently indicate that the tenogenic function of CTGF was not diminished by inflammatory and degenerative environments. Future studies should investigate the mechanisms underlying CTGF-mediated inflammatory modulation.
To form a mechanically functional enthesis, the tendon collagen fibers must be anchored into the bone via formation of a mineralized fibrocartilage, likely accompanied by positive remodeling of the underlying epiphyseal bone. 39 Although micro-CT data showed higher bone mineral density and bone volume fraction in group C, suggesting increased bone healing at the tendon attachment site, there was no difference among the early time point mRNA expression levels of BMP2. This is likely due to technical errors associated with sample preparation for qRT-PCR analysis, where tissue samples were peeled off from the bony footprint with a blade, frequently excluding the mineralized portion. Nonetheless, comprehensive outcome measurements at the 12-week samples consistently suggested bone regeneration at the SST footprint by the bioactive scaffolds.
For application of biodegradable scaffolds in large preclinical animal models and human patients, in vivo biodegradation has to be adjusted to balance with a tissue-healing rate. 46 The scaffolds’ in vivo degradation rate was preoptimized by controlling the surface porosity, as demonstrated in previous studies,47,50 resulting in full degradation in the rabbit model by 12 weeks. However, the in vivo degradation rate of polyester scaffolds can be affected by local biological, chemical, and physical environments,28,50 necessitating further adjustments for large animal models or human clinical trials. We recently developed an imaging-based technology to track in vivo degradation of 3D-printed polycaprolactone scaffolds. 44 Quantum dot labeling enabled quantitative visualization of the remaining portion of the scaffold in vivo without sacrificing animals. We plan to apply this in vivo tracking method to determine the optimal degradation rate of our bioactive scaffold in the next step of translational studies.
Several biological and synthetic grafts are available to augment the repair of severe RCTs. 19 There are typically 3 types of commercially available devices: synthetic grafts, allografts, and xenografts. Bovine, porcine, and human extracellular matrices are the major sources of allografts and xenografts. 19 Existing allografts and xenografts show relatively few patient-reported improvements in clinical outcomes and relatively high retear rates. Studies are limited on the clinical efficacy of commercially available synthetic grafts such as Regeneten (Smith & Nephew) and BioBrace (Biorez), which are rapidly becoming popular.6,19,52 Despite the ongoing development of several products designed to mechanically augment rotator cuff repair with some added bioinductivities to support tendon healing, 7 synthetic grafts to regenerate the BTI have not been designed. The 3D-printed bioactive scaffold proposed in this study exhibits translational potential as an off-the-shelf graft in the form of a microthin membrane that can be easily applied with surgical rotator cuff repairs. The overall configuration is identical to that of the currently available synthetic rotator cuff grafts, and the flexible and elastic scaffold can be easily inserted into the joint cavity arthroscopically and placed between the tendon and bone. The scaffolds are designed to immediately provide mechanical augmentation of the suture-repaired rotator cuff, and spatiotemporally released bioactive cues recruit the body’s own stem cells and guide the formation of the stratified multiphase BTI, as balanced with biodegradation of the scaffolds. These unique features and functions reinforce the potential clinical effect of bioactive scaffolds.
Conclusion
Bioactive scaffolds with spatially embedded GFs have significant potential to promote BTI healing of chronic RCTs in a rabbit model.
Footnotes
Submitted March 3, 2023; accepted April 11, 2023.
One or more of the authors has declared the following potential conflict of interest or source of funding: This research was supported by a grant from the Seoul National University Bundang Hospital research fund (No. 14-2021-0002) to J.H.O. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.