
Abstract
Background:
Bone marrow stimulation (BMS) techniques such as microfracture, nanofracture, and the crimson duvet procedure expose the bone marrow of the proximal humerus to the rotator cuff tendon footprint. The effect of performing BMS on tendon healing is a subject of interest.
Purpose:
To compare studies on arthroscopic rotator cuff repair with BMS versus without BMS for rotator cuff tears according to healing rates and clinical and radiological outcomes.
Study Design:
Systematic review and meta-analysis; Level of evidence, 2.
Methods:
The 2020 PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines were followed in conducting a search. Studies that compared arthroscopic rotator cuff repair with and without BMS were included if they provided postoperative patient-reported outcomes and healing rates. Dichotomous outcomes were expressed as mean differences (MDs), while continuous outcomes were expressed as odds ratio.
Results:
Included were 5 studies (N = 499 shoulders); 4 studies had level 1 evidence, and 1 study had level 2 evidence. The healing rate of rotator cuff repair was similar between the 2 groups (ie, with and without BMS) (odds ratio, 1.58 [95% CI, 0.63 to 4.00]; P = .33). Furthermore, there were no significant differences in the postoperative Constant score (MD, 1.41 [95% CI, –0.58 to 3.39]; P = .16), American Shoulder and Elbow Surgeons score (MD, 0.77 [95% CI, –1.43 to 2.96]; P = .49), or range of motion for forward flexion (MD, 2.45 [95% CI, –0.66 to 5.57]; P = .12) and external rotation (MD, 0.81 [95% CI, –2.35 to 3.97]; P = .62) at the final follow-up between the 2 groups.
Conclusion:
The healing rate of rotator cuff repair was similar, regardless of whether BMS was performed or not. Additionally, there was no significant difference in postoperative patient-reported outcome scores, range of motion, and complications.
Registration:
CRD42023388427 (PROSPERO).
Good functional outcomes have been achieved with arthroscopic rotator cuff repair,24,30 but this procedure has a significant retear rate of up to 20% to 94% for large to massive tears depending on the surgical technique, and functional outcomes gradually deteriorate over time.12,14,23 The risk factors for a retear after rotator cuff repair have been reported as age, body mass index, diabetes, initial tear size, tendon retraction, and fatty degeneration of the rotator cuff.17,33 The failure of tendon-to-bone healing frequently leads to retears after rotator cuff repair, 6 and novel approaches to improving healing rates are required. Additionally, a method known as “biological augmentation” has been created and is thought to be useful for enhancing the healing rate.7,13,15 The use of platelet-rich plasma injections, adipose-derived mesenchymal stem cells, and bone marrow aspirate concentrate is gaining popularity among surgeons. 19 A potential strategy to enhance healing is to stimulate bone marrow, which will increase growth factors and mesenchymal stem cells released at the repair site and is also cost-effective. Through the use of bone marrow stimulation (BMS) techniques such as microfracture,20,21 nanofracture, 25 and the crimson duvet procedure,26,29 the bone marrow of the proximal humerus is exposed to the rotator cuff tendon footprint. According to an animal study by Bilsel et al, 2 BMS at the footprint may reduce the rate of retears after rotator cuff repair.
Clinical studies on the effect of BMS in enhancing healing rates and outcomes after rotator cuff restoration have shown variable results.1,11,16,20,21,25,28,29 Several previous systematic reviews by Ajrawat et al, 1 Li and Zhang, 18 Yang et al, 31 and Zhang et al, 32 which included level 3 evidence studies, found that rotator cuff repair with BMS reduces the retear rate but shows no difference in postoperative patient-reported outcomes compared with repair without BMS. However, the systematic reviews included retrospective studies and might have selection biases. Multiple high-quality randomized controlled trials have produced evidence indicating that there is no discernible distinction between the 2 techniques.16,20,21,29 Therefore, performing BMS may not necessarily have an effect on tendon healing, as the process of attaching suture anchors onto the footprint involves bone drilling, which could potentially release bone marrow or growth factors that may already be present in the area, and there is a risk of anchor loosening and greater tuberosity fractures.16,25 According to previous studies of cartilage defect treatment (Cite), the holes in BMS may lead to subchondral collapse and may increase the likelihood of anchor loosening and fracture.4,8
The objective of this study was to identify and analyze currently available randomized controlled trials with level 1 or 2 evidence regarding the clinical and radiological outcomes of patients treated with BMS with arthroscopic rotator cuff repair. We hypothesized that BMS with rotator cuff repair leads to a similar healing rate and comparable outcomes with those after conventional repair.
Methods
Data Sources and Search Strategy
This systematic review was carried out in accordance with the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines. 22 This study was registered with the PROSPERO international prospective register of systematic reviews (No. CRD42023388427).
Overall, 2 authors (N.T., T.I.) searched PubMed, Scopus, and Embase to find relevant research articles that examined arthroscopic rotator cuff repair with and without BMS from the beginning of the database through January 31, 2023. The following Medical Subject Headings terms were inserted into an electronic search browser: (“rotator cuff repair” or “rotator cuff tear”) and (“bone marrow stimulation” or “microfracture or nanofracture” or “crimson duvet”). The authors manually scanned published reference lists to find more pertinent articles. The authors used EndNote (Version 20; Clarivate) to merge the reference lists from the databases and remove duplicate studies.
Study Selection
Eligibility criteria for the inclusion of studies were as follows: (1) randomized controlled trials with level 1 or 2 evidence; (2) studies making direct comparisons between arthroscopic rotator cuff repair with and without BMS; (3) studies reporting rotator cuff healing rates, patient-reported outcomes, or complications; (4) English-language articles; and (5) full-text availability. The exclusion criteria were (1) basic science or biomechanics articles, (2) retrospective studies with level 3 to 4 evidence, (3) review articles, and (4) overlap of patient populations when studies were conducted by the same author(s) or institution.
Data Extraction
Data were separately extracted by 2 authors (N.T., T.I.). The following information was retrieved from each study: (1) article information, (2) patient demographic data, (3) surgical techniques, (4) healing rates, (5) patient-reported outcome scores, (6) range of motion, and (7) complications.
Study Methodology and Risk-of-Bias Assessment
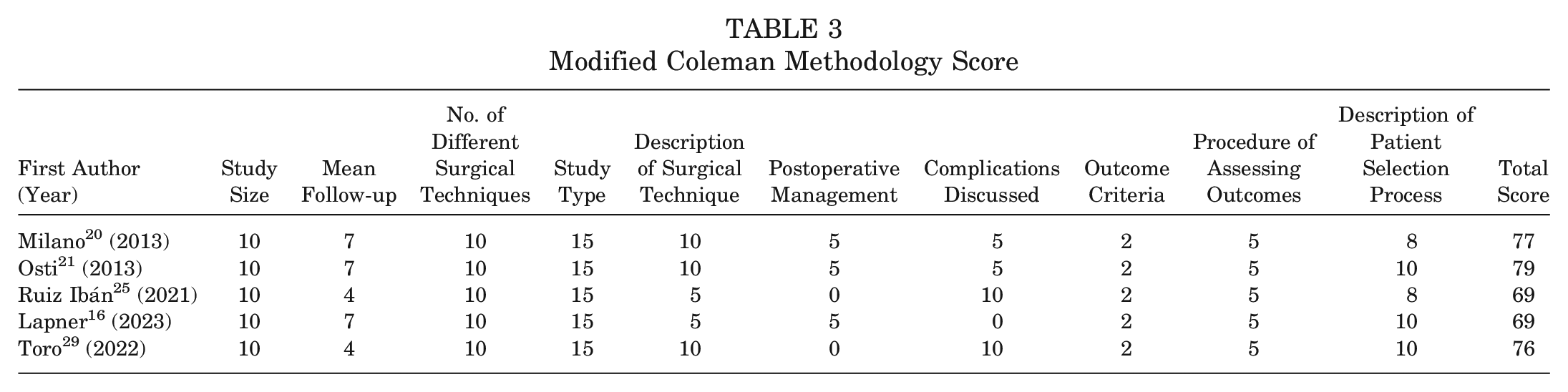
The same 2 authors independently evaluated the risk of bias in each study using the Cochrane risk-of-bias tool, 9 and each study’s methodological quality was examined using the modified Coleman Methodology Score (MCMS). 5 Any conflicts were resolved by another author (D.L.). The Cochrane risk-of-bias tool assessed the following 7 domains: (1) random sequence generation, (2) allocation concealment, (3) blinding of participants and personnel, (4) blinding of outcome assessment, (5) incomplete outcome data, (6) selective reporting, and (7) other bias. 7 The MCMS value ranges from 0 to 100. Part A of the MCMS mainly assesses baseline study characteristics, while part B of the MCMS mainly assesses outcome criteria and enrollment rates. Scores of 85-100 are excellent, 70-84 are good, 55-69 are fair, and <55 are poor. 5
Outcomes
The primary outcome of this study was the rotator cuff healing rate according to radiological imaging (magnetic resonance imaging [MRI] or ultrasound). Secondary outcomes included postoperative patient-reported outcome scores, range of motion, and complications.
Statistical Analysis
A meta-analysis was performed using RevMan (Version 5.4.1; Cochrane). Each study used odds ratios (ORs) with 95% CIs for continuous outcomes and mean differences (MDs) with 95% CIs for dichotomous outcomes. Significant heterogeneity was defined as an I2 value >50% and a significant Cochran Q test result (P < .1). If there was no statistical evidence of heterogeneity, a fixed-effects model was used. When statistical evidence of heterogeneity was present, a random-effects model was used. The results of the meta-analysis were demonstrated graphically using forest plots.
Results
Study Selection
A total of 232 articles were obtained through systematic searches of the databases. The retrieved articles were reduced by 91 duplicates. After screening the titles and abstracts of the remaining 141 articles, 125 additional studies that were not relevant to the objectives of this review were omitted. It was discovered after collecting and examining the full texts of the remaining 16 articles that 11 of them should not have been included because they reported results that did not correspond to this review’s main objectives. Finally, a total of 5 articles16,20,21,25,29 were included. The PRISMA flow diagram for study selection is shown in Figure 1.
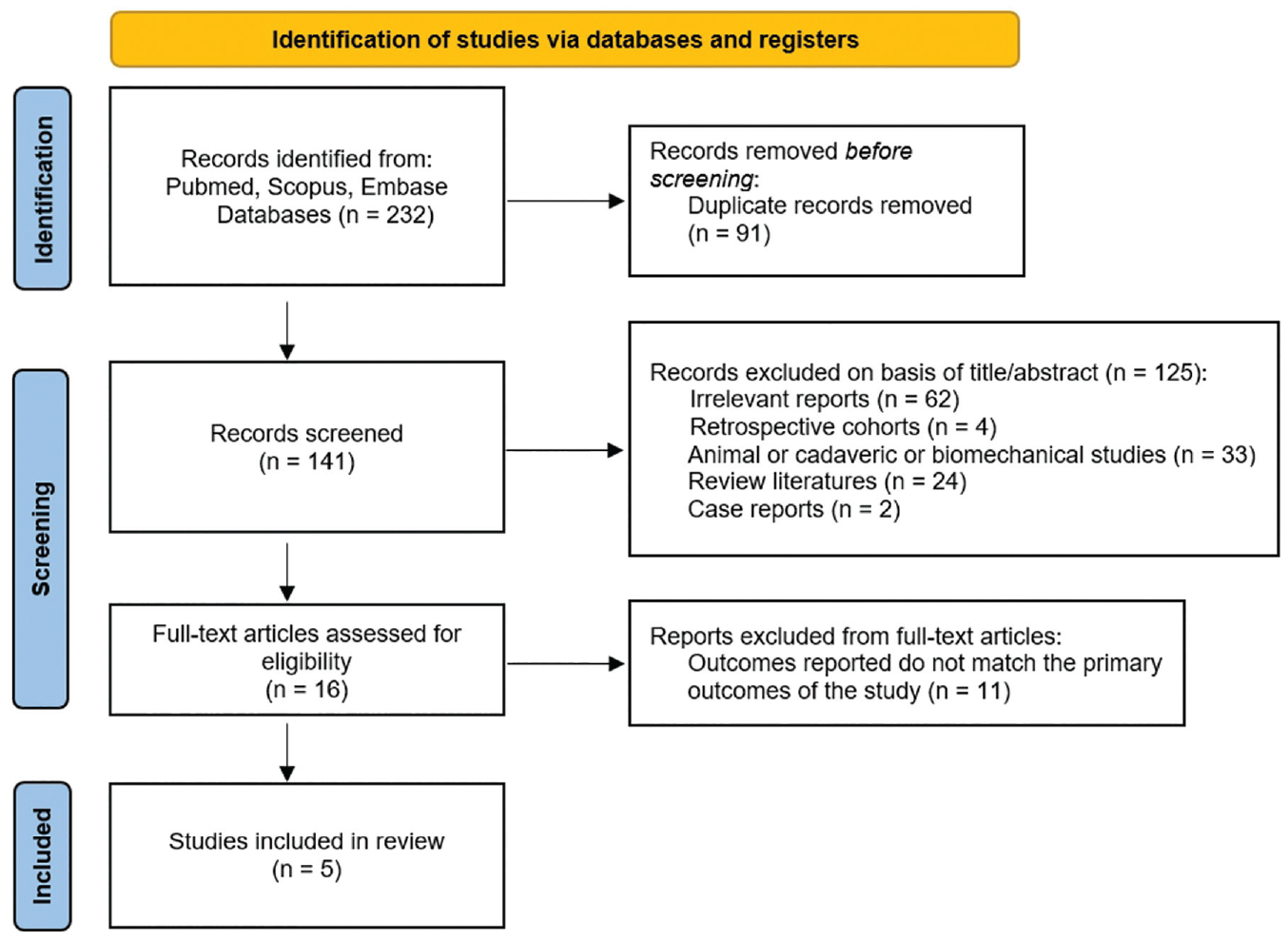
PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) flow diagram showing the literature search process.
Study Characteristics
All 5 studies16,20,21,25,29 with a total of 499 shoulders were included in this systematic review to identify the healing rates and clinical outcomes of arthroscopic rotator cuff repair with and without BMS. The studies had all been carried out utilizing a randomized controlled trial design. In all of the 5 included studies, there were no significant differences in patient characteristics between the groups. Most of the patients were >55 years, with a minimum 12-month follow-up. There were 4 studies16,20,21,25 that were classified as level 1 evidence, and the remaining study 29 was classified as level 2 evidence. Tables 1 and 2 contain detailed information about the included studies.
Study and Patient Characteristics a
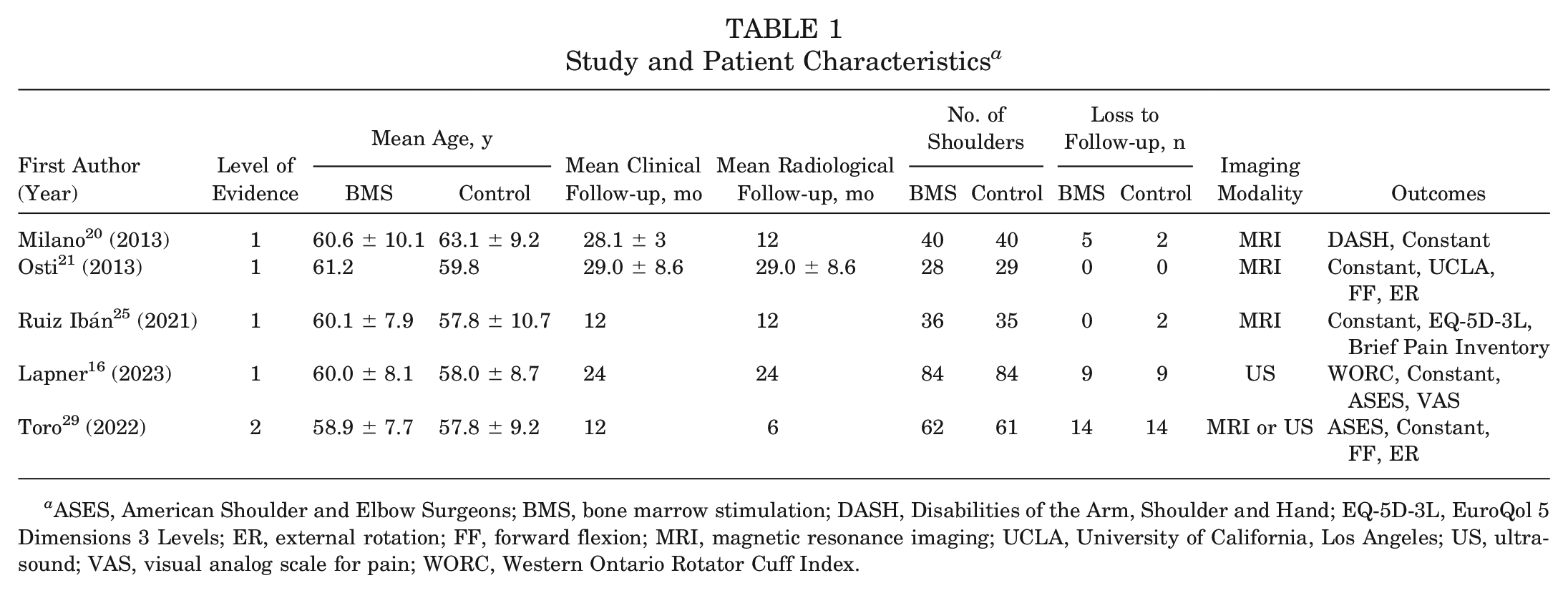
ASES, American Shoulder and Elbow Surgeons; BMS, bone marrow stimulation; DASH, Disabilities of the Arm, Shoulder and Hand; EQ-5D-3L, EuroQol 5 Dimensions 3 Levels; ER, external rotation; FF, forward flexion; MRI, magnetic resonance imaging; UCLA, University of California, Los Angeles; US, ultrasound; VAS, visual analog scale for pain; WORC, Western Ontario Rotator Cuff Index.
Inclusion/Exclusion Criteria and Surgical Techniques a
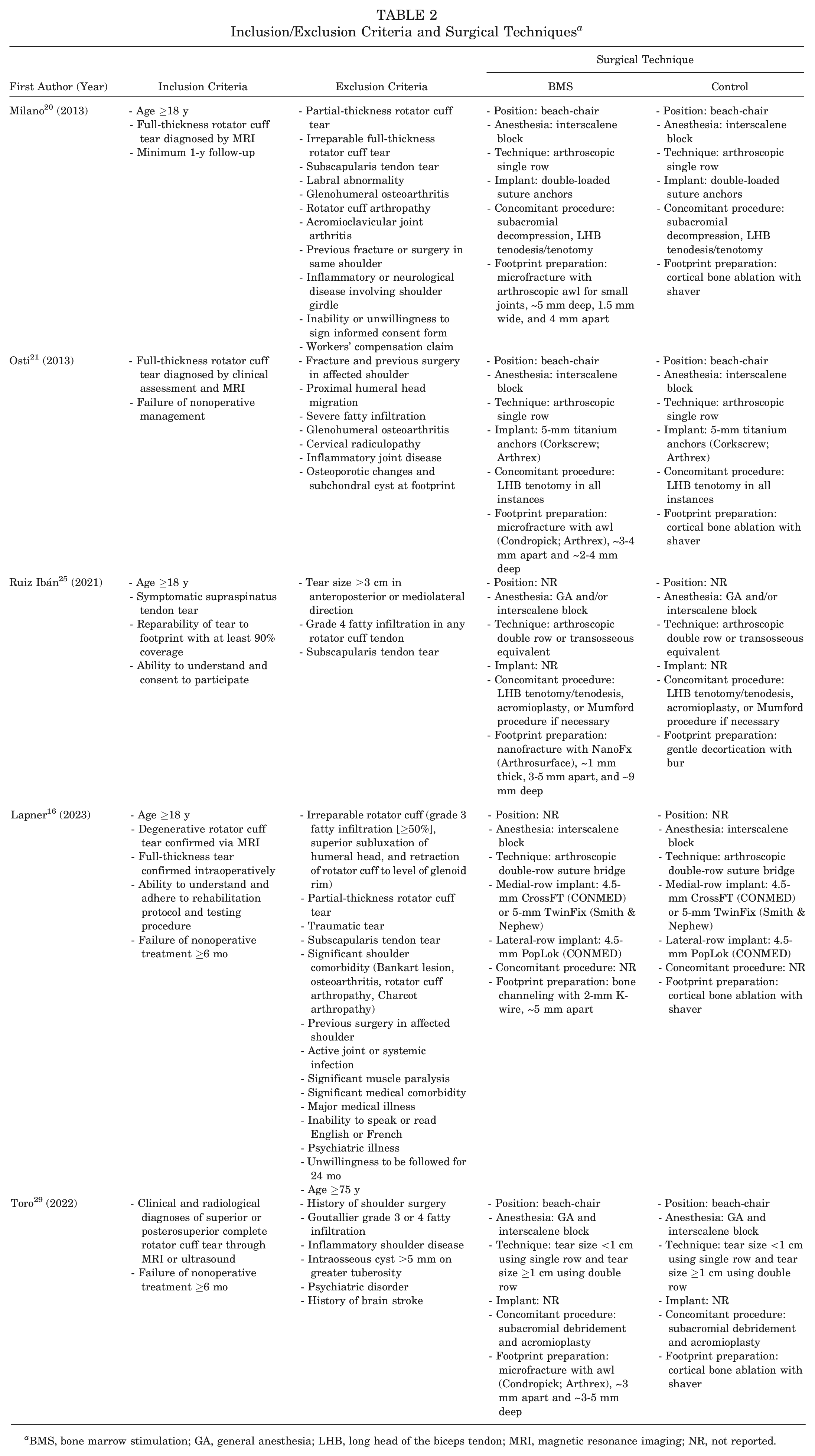
BMS, bone marrow stimulation; GA, general anesthesia; LHB, long head of the biceps tendon; MRI, magnetic resonance imaging; NR, not reported.
Risk of Bias
The Cochrane risk-of-bias tool was used to conduct a risk-of-bias assessment of the 5 included studies.16,20,21,25,29 There were 2 studies16,21 that were classified as having some bias concerns. The risk of bias was found to be high for 3 studies.20,25,29 Figure 2 shows the summarized proportions and details on the rating for each domain of the Cochrane risk-of-bias tool for all included studies.
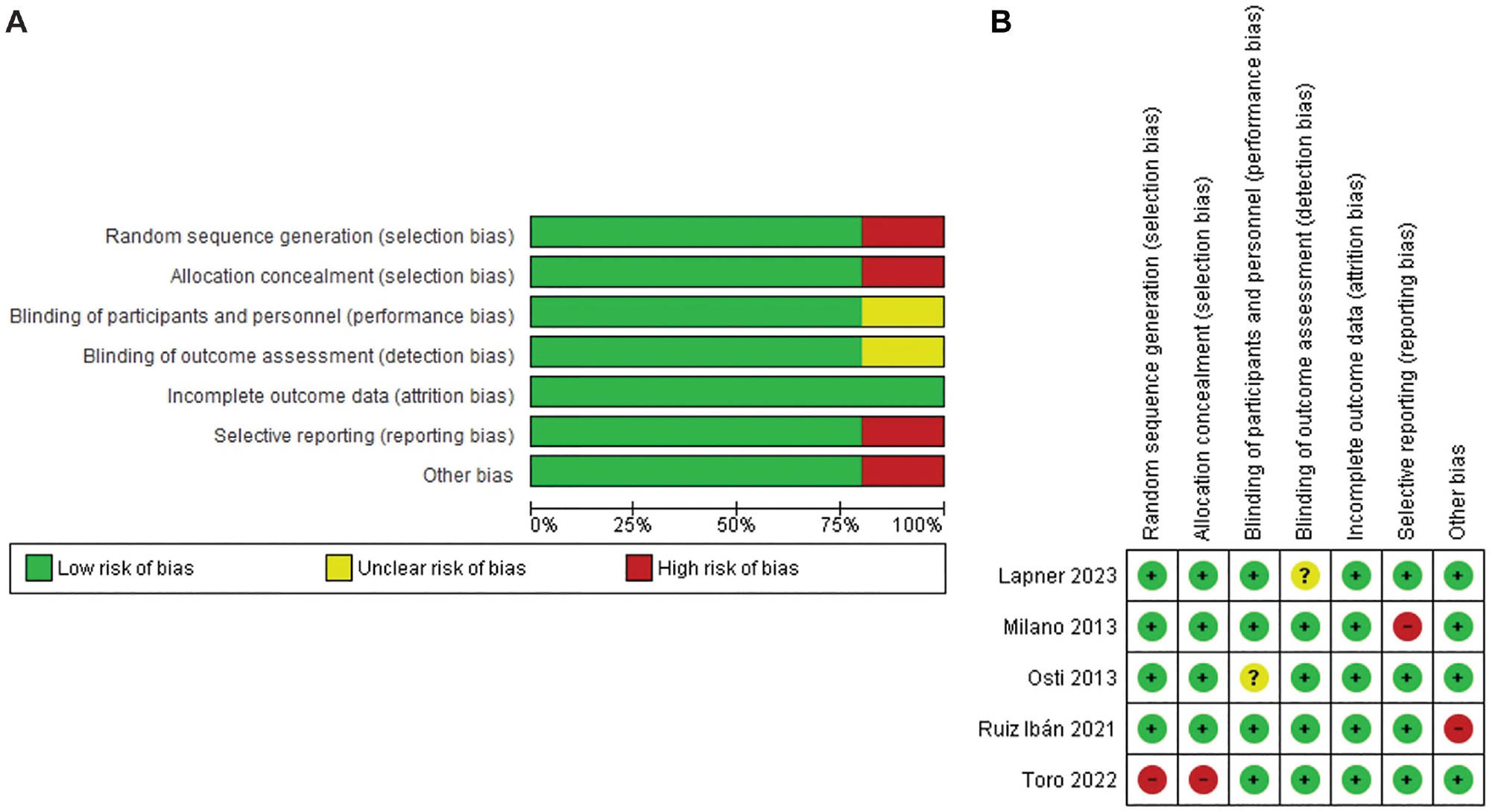
(A) Risk-of-bias graph: reviewers’ judgments about each risk-of-bias item presented as percentages across all included studies. (B) Risk-of-bias summary: reviewers’ judgments about each risk-of-bias item for each included study.
Modified Coleman Methodology Score
The MCMS values for the 5 included studies16,20,21,25,29 are shown in Table 3. Overall, 2 studies16,25 had fair scores, while 3 studies20,21,29 had good scores.
Modified Coleman Methodology Score
Healing Rate
The mean radiological follow-up among the 5 studies16,20,21,25,29 that reported on the healing rate was 6 to 29 months. In all, 3 studies20,21,25 used MRI, 1 study 16 used ultrasound, and 1 study 29 used either MRI or ultrasound. In studies employing MRI, the evaluation of tendon healing was conducted utilizing the Sugaya classification. 27 In studies utilizing ultrasound, a fellowship-trained musculoskeletal radiologist assessed healing of the tendon by determining whether it was in continuity and devoid of any signs of full-thickness tearing. If these criteria were met, the repair site was considered healed. There were 4 studies16,20,21,29 that found no significant differences between the groups regarding the healing rate, but 1 study 25 found that performing BMS at the footprint during rotator cuff repair increased the healing rate by half. The overall healing rate of rotator cuff repair with and without BMS was 83.3% and 79.0%, respectively. No statistically significant difference was found between the 2 groups (OR, 1.58 [95% CI, 0.63-4.00]; P = .33) (Figure 3).
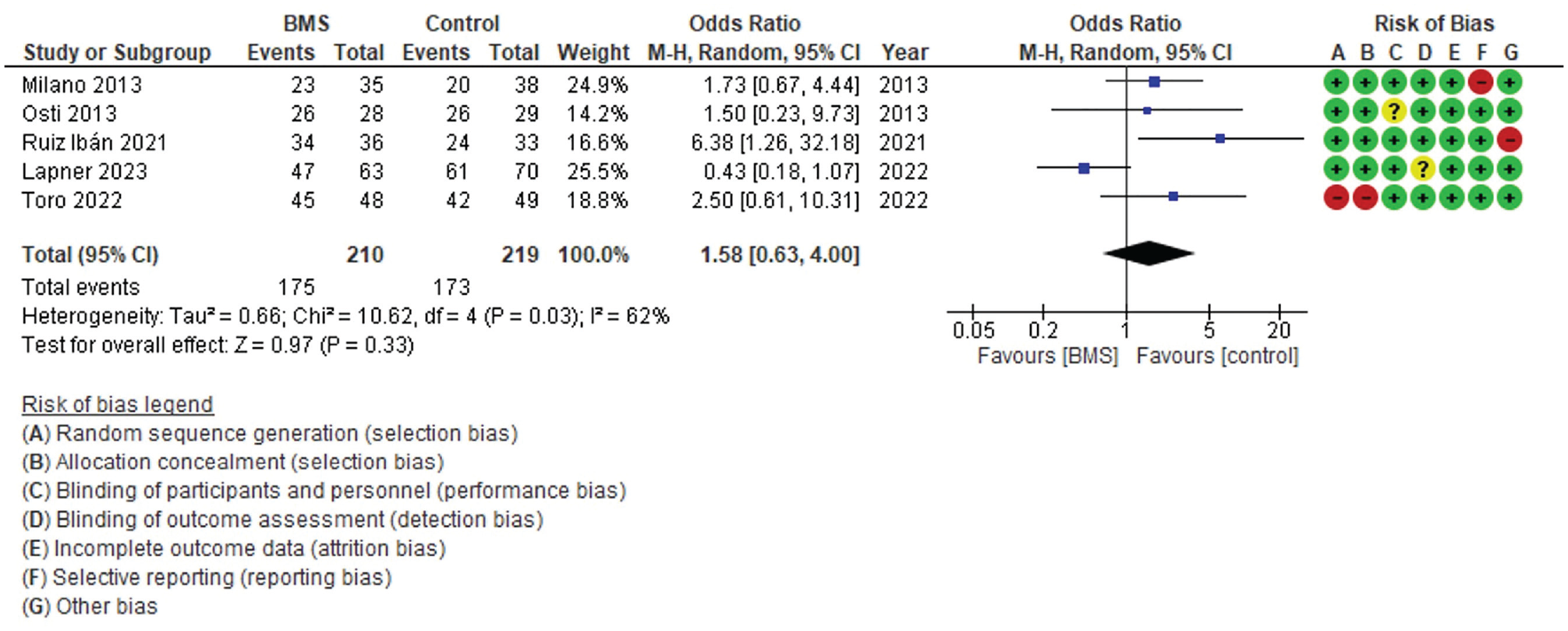
Forest plot comparing the healing rate between rotator cuff repair with and without bone marrow stimulation (BMS). M-H, Mantel-Haenszel.
Patient-Reported Outcome Scores
We found that all 5 studies16,20,21,25,29 evaluated the Constant score, 2 studies16,29 evaluated the American Shoulder and Elbow Surgeons (ASES) score, 1 study 20 evaluated the Disabilities of the Arm, Shoulder and Hand questionnaire, 1 study 21 evaluated the University of California, Los Angeles, shoulder scale, and 1 study 16 evaluated the Western Ontario Rotator Cuff Index at the latest follow-up. The latest follow-up showed no significant differences between the groups in regard to the Constant score (MD, 1.41 [95% CI, –0.58 to 3.39]; P = .16) and ASES score (MD, 0.77 [95% CI, –1.43 to 2.96]; P = .49) across all studies (Figure 4).
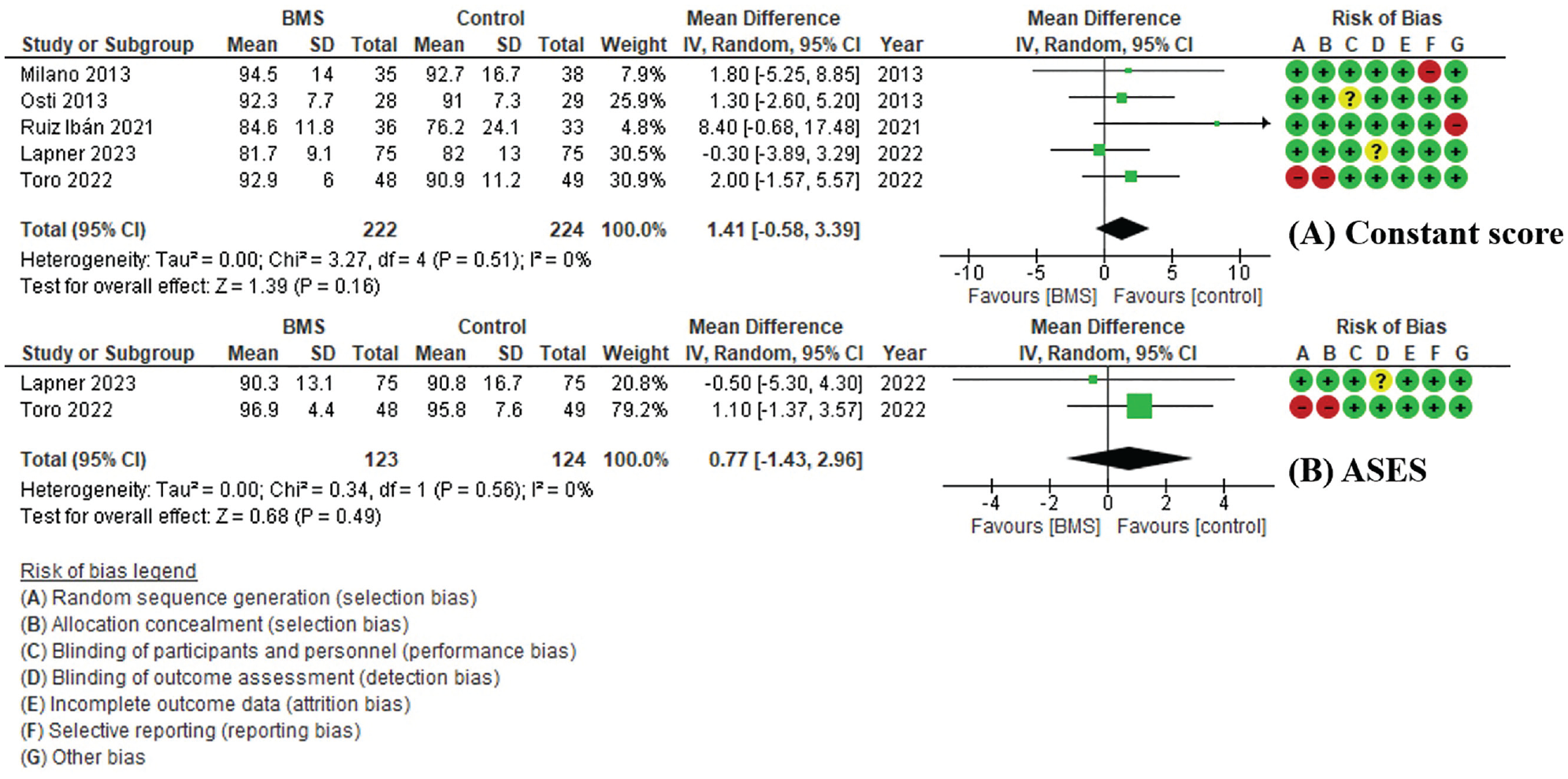
Forest plot comparing patient-reported outcome scores between rotator cuff repair with and without bone marrow stimulation (BMS): (A) Constant score and (B) American Shoulder and Elbow Surgeons (ASES) score. IV, inverse variance.
Range of Motion
The 2 studies21,29 that reported on shoulder range of motion at the latest follow-up found no significant differences between the groups regarding forward flexion (MD, 2.45° [95% CI, –0.66 to 5.57]; P = .12) and external rotation (MD, 0.81° [95% CI, –2.35 to 3.97]; P = .62) at the latest follow-up (Figure 5).
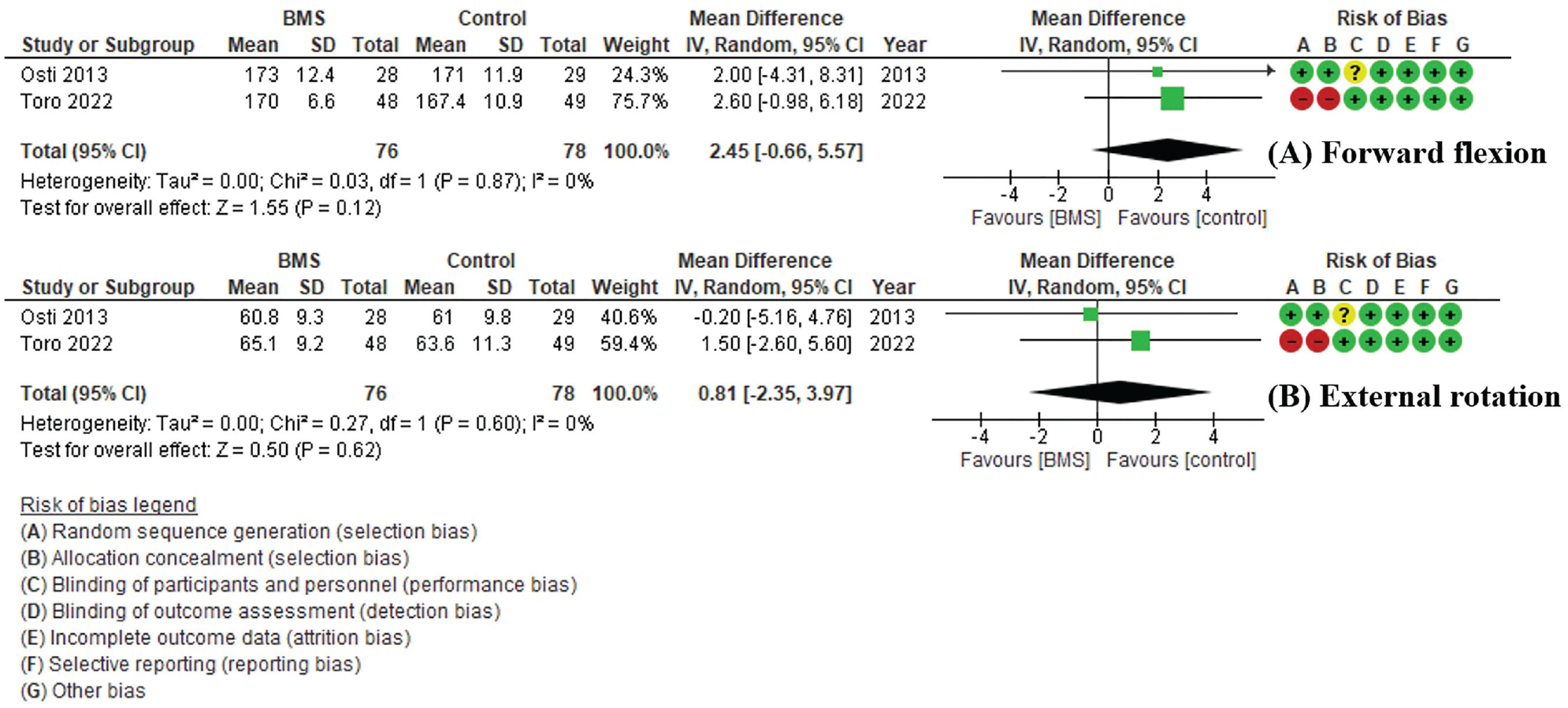
Forest plot comparing range of motion between rotator cuff repair with and without bone marrow stimulation (BMS): (A) forward flexion and (B) external rotation. IV, inverse variance.
Complications
According to Ruiz Ibán et al, 25 3 complications were observed in the BMS (nanofracture) group. One patient experienced a fracture during anchor placement, which necessitated the relocation of the anchor. However, this did not prevent successful repair, and the patient maintained a Constant score of 86, despite eventually developing a retear at the musculotendinous junction. In the other 2 cases, there were concerns about an infection, but the final Constant score was still good, with scores of 87 and 95.
In the study conducted by Lapner et al, 16 complications were observed in 10 patients who underwent BMS (using 2-mm K-wire to create a bone channel) and 6 patients in the control group. In the BMS group, 1 patient experienced a painful retear that was treated with a steroid injection and did not require further surgery. However, 4 patients required revision surgery for conditions such as biceps tendinitis, adhesive capsulitis, and infection. A total of 3 patients received steroid injections for adhesive capsulitis and shoulder pain, and 2 needed special physical therapy for impingement and radiculopathy. In the control group, 3 patients underwent revision rotator cuff repair, 1 underwent surgery for a traumatic dislocation and glenoid fracture, 1 received a steroid injection for adhesive capsulitis, and 1 received antibiotics for a superficial infection.
Discussion
The most important finding of this review was that the healing rate of rotator cuff repair with and without BMS was similar in both groups (OR, 1.58 [95% CI, 0.63 to 4.00]; P = .33). Also, there was no significant difference between the 2 groups in the postoperative Constant score (MD, 1.41 [95% CI, –0.58 to 3.39]; P = .16), ASES score (MD, 0.77 [95% CI, –1.43 to 2.96]; P = .49), or range of motion for forward flexion (MD, 2.45 [95% CI, –0.66 to 5.57]; P = .12) and external rotation (MD, 0.81 [95% CI, –2.35 to 3.97]; P = .62) at the last follow-up.
Jeong et al 10 found that functional outcomes deteriorated over time in patients with rotator cuff retears and worse functional outcomes were not detected at the 2-year follow-up, with the 5-year follow-up showing significantly worse outcomes for the retear group compared with the intact group. The BMS technique, which was first described by Snyder and Burns, 26 involves using bone marrow punctures to release mesenchymal stem cells, growth factors, and platelets that have the potential to enhance tendon healing. There is not a defined protocol for using BMS in patients with rotator cuff injuries who need arthroscopic repair. There is an advantage of possibly improving healing, but there are risks of anchor loosening and greater tuberosity fractures.16,25
Taniguchi et al 28 conducted a retrospective study to evaluate the effect of BMS on the integrity of rotator cuff repair. They found that BMS at the footprint results in superior rotator cuff healing, particularly for large to massive tears, highlighting the significance of biological treatment for rotator cuff healing after arthroscopic rotator cuff repair. Additionally, Jo et al 11 performed a retrospective cohort study that discovered that multiple channeling significantly decreased the retear rate after arthroscopic rotator cuff repair; however, there was no significant difference between the multiple channeling and conventional groups in terms of clinical outcomes.
Milano et al 20 reported the results of a randomized controlled trial, evaluating the efficacy of BMS with microfracture of the greater tuberosity during arthroscopic rotator cuff repair. Their results showed that there was no significant difference in the overall tendon healing rate and postoperative patient-reported outcomes between the 2 groups. 20 Osti et al’s 21 randomized controlled trial found that microfracture at the footprint is effective in reducing pain in the short term, but at a minimum follow-up of 2 years, there were no significant differences in outcomes and healing rates compared with conventional rotator cuff repair. Lapner et al 16 conducted a randomized controlled trial that compared the effectiveness of arthroscopic rotator cuff repair with and without bone channeling for degenerative rotator cuff tears. Their study found no significant differences in healing rates, patient-reported function, or quality-of-life outcomes between the group that underwent bone channeling and the group that underwent conventional repair. 16 Toro et al 29 also discovered no significant difference in healing rates or functional outcomes between the control and crimson duvet groups in their randomized controlled trial. Ruiz Ibán et al 25 reported the results of a randomized controlled trial that used nanofracture to augment arthroscopic rotator cuff repair. For nanofracture, a technique used in BMS, they employed the NanoFx instrument (Arthrosurface) to create 1 mm–diameter holes in the bone. 25 These holes were smaller than those made by standard microfracture techniques and were deeper (9 mm) to access targeted bone marrow cells with minimal damage to the subchondral plate. The authors found better tendon healing rates to the footprint in the nanofracture group in their study of 69 participants followed up for 12 months. 25 It is possible that nanofracture is better than microfracture or the crimson duvet procedure because it penetrates deeper into the bone and provides more bone marrow to the footprint area. However, there are no studies comparing nanofracture with microfracture or the crimson duvet procedure. More studies are needed to confirm this. In that study, the surgeon was not blind to the assignment because he had to perform the nanofracture procedures, but the patients and investigators were. 25 However, there are some concerns that the study’s funding from Arthrosurface could lead to a potential bias. 25 Retrospective studies suggested that adding BMS to rotator cuff repair improved healing, but randomized controlled trials did not find any difference.
Previous systematic reviews1,18,31,32 have found that although the clinical outcomes were similar, arthroscopic rotator cuff repair with BMS had a significantly higher healing rate than conventional rotator cuff repair. However, these systematic reviews included retrospective cohort studies, which have a low level of evidence and can have some biases and limitations. Ajrawat et al 1 performed a systematic review comprising 4 studies, which consisted of 2 randomized controlled trials and 2 retrospective cohort studies. Li and Zhang 18 included 4 randomized controlled trials and 4 retrospective cohort studies in their review. Yang et al 31 conducted a review that involved 5 randomized controlled trials and 4 cohort studies. Zhang et al 32 included 4 randomized controlled trials and 4 retrospective cohort studies in their review. We conducted a systematic review and meta-analysis that included only randomized controlled trials and found that the results were different from previous reviews. The present study found no difference in healing rates and patient-reported outcome scores, as well as range of motion, between the BMS and control groups.
Overall, BMS did not promote rotator cuff healing or provide better clinical outcomes than conventional rotator cuff repair. The utilization of BMS in conjunction with arthroscopic rotator cuff repair can result in longer operative times, more susceptibility to greater tuberosity fractures, and an increased risk of anchor pullout in patients with osteoporosis.3,23 We do not endorse the use of BMS for the purpose of augmenting rotator cuff repair and suggest that performing decortication of the rotator cuff footprint using an arthroscopic shaver or high-speed bur is sufficient.
This study has strengths, including a comprehensive and systematic review conducted by 2 independent reviewers. Notably, this is the first systematic review, to our knowledge, that exclusively includes only randomized controlled trials comparing the outcomes of arthroscopic rotator cuff repair with and without BMS. However, this study has several limitations. First, the included studies demonstrate some heterogeneity, including single-row and double-row repair, a variety of tear sizes, diverse BMS adoption schemes, and different postoperative rehabilitation protocols. Second, because of our rigorous inclusion criterion for studies with level 1 or 2 evidence, we could only include 5 studies with a total of 499 shoulders in this systematic review. The study’s third limitation pertains to the variable follow-up times, which spanned from 12 to 29 months. This variability could potentially affect the accuracy and reliability of the findings. Furthermore, the relatively short duration of follow-up in the included studies calls for additional research into the long-term clinical outcomes of arthroscopic rotator cuff repair with and without BMS. Such research could provide more comprehensive insights into the effectiveness and durability of this intervention and inform clinical decision-making.
Conclusion
The healing rate of rotator cuff repair was similar, regardless of whether BMS was performed or not. Additionally, there was no significant difference in postoperative patient-reported outcome scores, range of motion, and complications.
Footnotes
Submitted March 29, 2023; accepted May 15, 2023.
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
An online CME course associated with this article is available for 1 AMA PRA Category 1 Credit™ at https://education.sportsmed.org/Public/Catalog/Home.aspx?CourseSearch=1&Criteria=9&Option=25. In accordance with the standards of the Accreditation Council for Continuing Medical Education (ACCME), it is the policy of The American Orthopaedic Society for Sports Medicine that authors, editors, and planners disclose to the learners all financial relationships during the past 12 months with any commercial interest (A ‘commercial interest’ is any entity producing, marketing, re-selling, or distributing health care goods or services consumed by, or used on, patients). Any and all disclosures are provided in the online journal CME area which is provided to all participants before they actually take the CME activity. In accordance with AOSSM policy, authors, editors, and planners’ participation in this educational activity will be predicated upon timely submission and review of AOSSM disclosure. Noncompliance will result in an author/editor or planner to be stricken from participating in this CME activity.