
Abstract
Background:
The traditional index of return-to-sport (RTS) readiness after anterior cruciate ligament reconstruction (ACLR) is the achievement of physical competence criteria. Emerging research indicates that psychological response and self-perceptions of physical competence may be critical mechanisms for successful RTS among young athletes.
Hypothesis:
Young athletes with higher actual physical competence (APC) and perceived physical competence (PPC) will demonstrate a more positive psychological response at the time of RTS after ACLR.
Study Design:
Cross-sectional study; Level of evidence, 3.
Methods:
A total of 41 young athletes after primary ACLR completed testing within 8 weeks of medical clearance to RTS. APC was measured with isokinetic knee extension strength, single-limb crossover hop for distance, and the Knee injury and Osteoarthritis Outcome Score. PPC was measured with the Athletic Competence subscale of the Self-Perception Profile. Criteria for APC and PPC were based on established age- and activity-relevant cutoff scores. Different constructs of psychological response were assessed with the adapted Sport Motivation Scale, Brief Resilience Scale, and Anterior Cruciate Ligament Return to Sport after Injury (ACL-RSI) total and subscale scores (Emotions, Confidence, and Risk Appraisal). Multiple linear regression analyses were used to determine differences in measures of psychological response based on achievement of APC and PPC, while adjusting for age and sex.
Results:
Of the 41 participants, 10 (24.4%) met all criteria for APC and 22 (53.7%) met the PPC criteria. The regression models estimating the ACL-RSI score (P < .001; adjusted R2 = 0.331), ACL-RSI Emotions score (P < .001; adjusted R2 = 0.427), and ACL-RSI Risk Appraisal score (P = .013; adjusted R2 = 0.212) were statistically significant. Although APC was not associated with any measure of psychological response, meeting PPC criteria, younger age, and male sex were found to be associated with a more positive psychological readiness to RTS, but not with motivation or resilience.
Conclusion:
Meeting PPC criteria was associated with higher psychological readiness to RTS among young athletes after ACLR, while meeting APC criteria was not associated with any construct of psychological response.
Keywords
After anterior cruciate ligament reconstruction (ACLR), the achievement of objective measures of function or physical competence criteria has served as the traditional index of return-to-sport (RTS) readiness.1,18 However, emerging research indicates that nonphysical factors from the psychological domain may play a significant role in RTS readiness. 52 Psychological readiness has been identified as the most significant predictor of an athlete’s return to their preinjury performance level after ACLR, 53 while fear of reinjury is the most consistently cited reason for not returning.5,32 Among young athletes in particular, lower psychological readiness and higher fear have been associated with increased incidence of second ACL injury.29,34 Motivation,17,37 resilience, 24 and knee-related self-efficacy6,47 have also been identified as key elements for returning to preinjury level of sport after knee injury.
Together, these factors form one’s psychological response to ACLR, the emotional and behavioral manifestation of the perceived impact of the ACLR experience. This psychological response can affect both immediate and long-term participation in sports and physical activity. 11 However, little is known about the elements needed to catalyze a positive psychological response after ACLR, particularly among youth. Factors within all domains of the biopsychosocial model are theorized to contribute to this response.3,59 Yet, most of the available research has sought to identify only the physical factors that influence one’s psychological response, such as adequate muscle function.9,33,57 A better understanding of how one’s psychological response is formed and develops after ACLR is imperative for the optimization of health and activity outcomes.
Seminal research from the motor behavior field has indicated that a person’s perceived physical competence (PPC), in addition to actual physical competence (APC), may be a key determinant of motivation and subsequent movement behavior. 49 The notion that PPC plays an essential role in one’s behavior and participation is reinforced by the self-determination theory. 45 According to the self-determination theory, competence is 1 of 3 innate needs, along with autonomy and relatedness (sense of belonging), that is necessary for psychological well-being and motivation. Thus, the degree to which competence is satisfied or thwarted after ACLR may influence one’s psychological response, and subsequently one’s RTS readiness.
To our knowledge, this association between competence and psychological response to ACLR has not been studied among a population of young athletes. Therefore, the purpose of this study was to determine how APC and PPC are associated with psychological response among young athletes after ACLR. Our hypothesis was that athletes who meet APC and PPC criteria at the time of RTS after ACLR will demonstrate more positive scores on psychological measures compared with athletes who do not meet APC and PPC criteria.
Methods
Participants
The cohort for this cross-sectional study included 41 athletes from a longitudinal multicenter study of outcomes after ACLR among young, active individuals. Inclusion criteria for participation in the study were (1) 13 to 25 years of age; (2) underwent primary, unilateral ACLR; (3) assessed for joint stability and function and released to sports by care provider (surgeon/physical therapist) within the previous 8 weeks; and (4) planned to return to a pivot/cutting sport or activity (eg, soccer, basketball, and lacrosse). Study participants were excluded if they (1) required a concomitant surgical procedure (aside from meniscal debridement or repair), (2) sustained a concomitant ligament injury (aside from a grade 1 medial collateral ligament injury), (3) reported a history of lower extremity (beyond current ACL) or spine injury requiring surgery or continued medical care, or (4) underwent a physeal-sparing ACLR. The decision to allow RTS clearance, the criteria used in RTS decision-making, and the rehabilitation program were not controlled by the current study. This study was approved by the internal institutional review boards at Cincinnati Children’s Hospital and The Ohio State University. Written formal consent and/or parental permission were obtained before testing.
Data Collection
Actual Physical Competence
Data from all participants were collected at a laboratory-based testing session within 8 weeks of medical clearance to RTS. In alignment with current RTS recommendations,1,7,14,18 APC was operationally defined using RTS criteria measures of strength, functional performance, and self-reported function.
Strength: Isokinetic Knee Extensor Peak Torque
An isokinetic dynamometer (Biodex Medical Systems Inc.) was used to measure quadriceps muscle strength of the involved limb at 180 deg/s. The axis of the dynamometer was aligned with the knee joint line, and the distal shank was securely strapped to the resistance arm of the dynamometer, as previously reported. 51 Quadriceps peak torque was measured during the knee extension phase and was normalized to body weight for each participant (measured in newton-meters per kilogram).
Functional Performance: Crossover Hop for Distance
Participants performed 2 measured trials of the crossover hop for distance on the involved leg, as previously demonstrated. 51 The mean distance (measured in centimeters) of the trials was calculated and divided by the participant’s height (in centimeters) for a normalized crossover hop for distance score. Among the standard single-limb hop tests, crossover hop for distance limb symmetry has been shown to be most closely related to loading symmetry between limbs. 38
Self-Reported Function: Knee injury and Osteoarthritis Outcome Score Sport and Recreation Function Subscale
The Knee injury and Osteoarthritis Outcome Score (KOOS) is a widely used measure of self-reported knee function shown to be reliable and valid for patients after ACLR.43,46 Although the 5 subscales of the KOOS have all demonstrated positive reliability (intraclass correlation coefficient [ICC], 0.75-0.93) and internal consistency (Cronbach α = .74-.96),43,46 items within the Sport and Recreation Function (Sport) subscale have been identified as being highly important to patients after ACLR. 20 These items assess function related to tasks of physical competence, such as jumping and twisting/pivoting, and are able to fulfill the criteria of a unidimensional measurement scale for patients after ACLR. 13
Perceived Physical Competence
PPC refers to an individual’s perception of his or her ability to do well at sports and demonstrate athletic prowess. 22 For this study, PPC was measured with the Athletic Competence subscale of either the Self-Perception Profile for Adolescents (ages 13-17 years) or the Self-Perception Profile for College Students (SPP) (ages 18-22+ years).21,31 Responses are scored from 1 (low competence) to 4 (high competence) and averaged for a total score. The SPP Athletic Competence subscale has demonstrated good reliability and validity, in addition to good internal consistency (Cronbach α = .86-.92).21,31
Psychological Response to ACLR
Motivation
Motivation was measured with an adapted version of the Sport Motivation Scale (ASMS), 40 developed to evaluate athlete motivations for returning to sport after injury.39,40 Items are formatted on a 7-point Likert scale from 1 (does not correspond) to 7 (corresponds exactly). Scores for the “intrinsic motivation stimulation” and “intrinsic motivation accomplishment” subscales were used in this study, which represent the athlete’s level of motivation to experience stimulation (eg, performing for enjoyment and satisfaction) after injury and the degree to which an athlete is intrinsically motivated toward accomplishing self-imposed expectations after injury, respectively. Internal consistency for the subscales was deemed adequate when tested in a population of athletes (Cronbach α = .70-.77). 40
Resilience
Resilience, the ability to bounce back after a significant sport-related trauma, was measured with the Brief Resilience Scale (BRS). 48 The BRS measures resilience as a unitary construct, with 6 total items scored on a Likert scoring scale from 1 (strongly disagree) to 5 (strongly agree). The BRS has been validated in multiple populations, demonstrating good internal consistency (Cronbach α = .80-.91) and reliability (ICC, 0.62-0.69). 48 The BRS demonstrates good convergent validity, positively associated with measures of optimism, purpose in life, social support, and positive affect, and negatively associated with measures of pessimism, negative interactions, behavioral disengagement, perceived stress, anxiety, and pain. 48
Psychological Readiness to RTS
Psychological readiness to RTS was measured with the Anterior Cruciate Ligament Return to Sport after Injury (ACL-RSI) scale. The ACL-RSI consists of 12 items within 3 subscales designed to measure the 3 types of psychological responses believed to be associated with RTS after ACLR: Emotions, Confidence, and Risk Appraisal. 56 Scores from all items are summed and averaged to calculate an overall ACL-RSI score and respective subscale scores, with higher scores representing a more positive psychological response. The ACL-RSI has shown acceptable reliability (Cronbach α = .92) 56 and good predictive value for successful RTS.4,26
Operationalization of Physical Competence Criteria
Cutoff scores for measures of APC were based on preliminary and published age- and activity-relevant data from healthy control participants in a longitudinal study of ACLR outcomes (Table 1) (Zwolski C, Paterno M, Thomas S, Schmitt L. Limb Symmetry and Sufficiency Among Adolescents After Anterior Cruciate Ligament Reconstruction. Abstract presented at APTA Combined Sections Meeting; January 24, 2019; Washington, DC). 23 Participants who achieved cutoff scores for all 3 APC measures were categorized as having met APC criteria. For PPC, participants who achieved a score ≥3.5 on the SPP Athletic Competence subscale were classified as having met PPC criteria. Previous work has reported mean scores of the SPP Athletic Competence subscale to range between 2.7 and 3.1 (SD, 0.6-0.9) for similar populations.21,31 All criteria for APC and PPC are listed in Table 1.
APC and PPC Criteria a
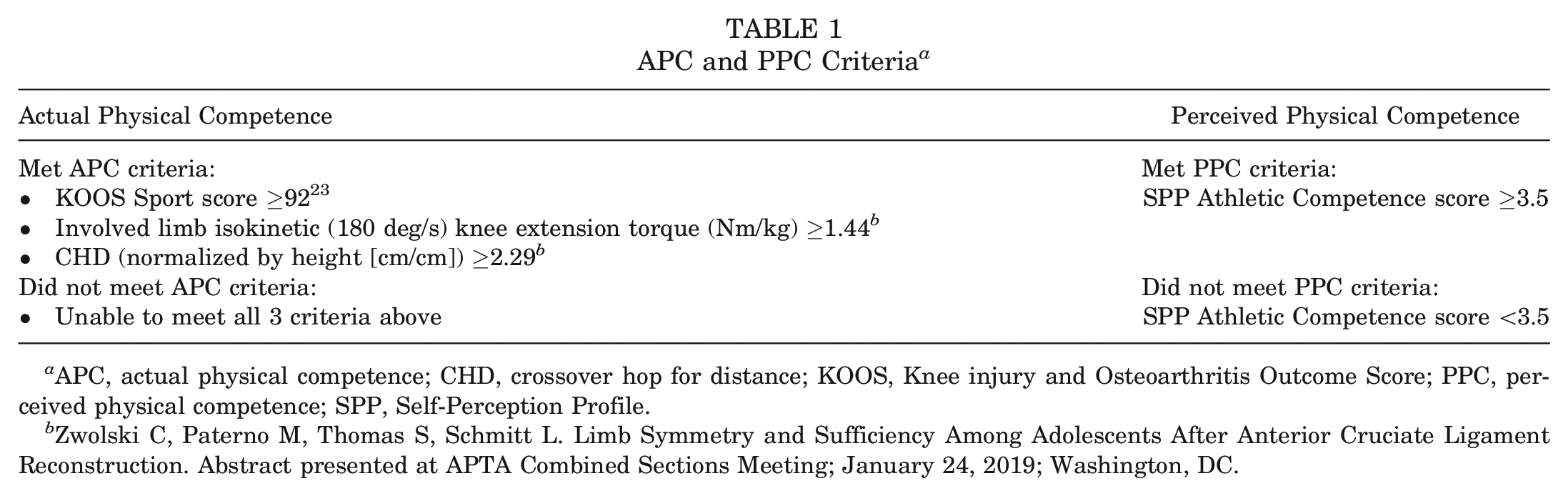
APC, actual physical competence; CHD, crossover hop for distance; KOOS, Knee injury and Osteoarthritis Outcome Score; PPC, perceived physical competence; SPP, Self-Perception Profile.
Zwolski C, Paterno M, Thomas S, Schmitt L. Limb Symmetry and Sufficiency Among Adolescents After Anterior Cruciate Ligament Reconstruction. Abstract presented at APTA Combined Sections Meeting; January 24, 2019; Washington, DC.
Data Analysis
Frequencies and percentages were calculated for categorical descriptive data. The normality of residuals was confirmed with histograms and quantile-quantile plots of residuals. Means and standard deviations were calculated for all normally distributed continuous descriptive data and measures of psychological response. Medians and interquartile ranges were calculated for all nonnormally distributed continuous descriptive or psychological response data. Effect sizes were calculated for mean differences in descriptive variables and competence measures between participants who did and did not meet criteria for both APC and PPC.
Multiple linear regression analyses were used to determine differences in psychological response between participants who achieved APC and PPC criteria, respectively, and those who did not. Independent contributions of APC and PPC were determined for each measure of psychological response, while adjusting for age and sex. All statistical analyses were performed using SPSS software (Version 25; IBM Corp). A Benjamini-Hochberg procedure using a 10% false discovery rate was performed to adjust the level of significance because of multiple comparisons. 10
Our sample size calculations indicated a sample size of 35 to be sufficient to detect an effect size of 0.40 (f2) with 0.80 power and an alpha level of .05 for a multivariable regression model with 4 predictor variables (APC, PPC, age, and sex) (G*Power Version 3.1).
Results
A total of 41 young athletes were enrolled in this study after ACLR (Table 2). Scores for all measures of APC and PPC are reported in Table 3. Of the 41 participants, 10 (24.4%) met APC criteria, while 31 (75.6%) participants did not, and 22 (53.7%) met PPC criteria, while 19 (46.3%) did not (Table 4). Characteristics of the cohort categorized by achievement of APC and PPC criteria are shown in Tables 5 and 6, respectively. Median scores and ranges for all measures of psychological response are reported in Table 7.
Patient Characteristics a
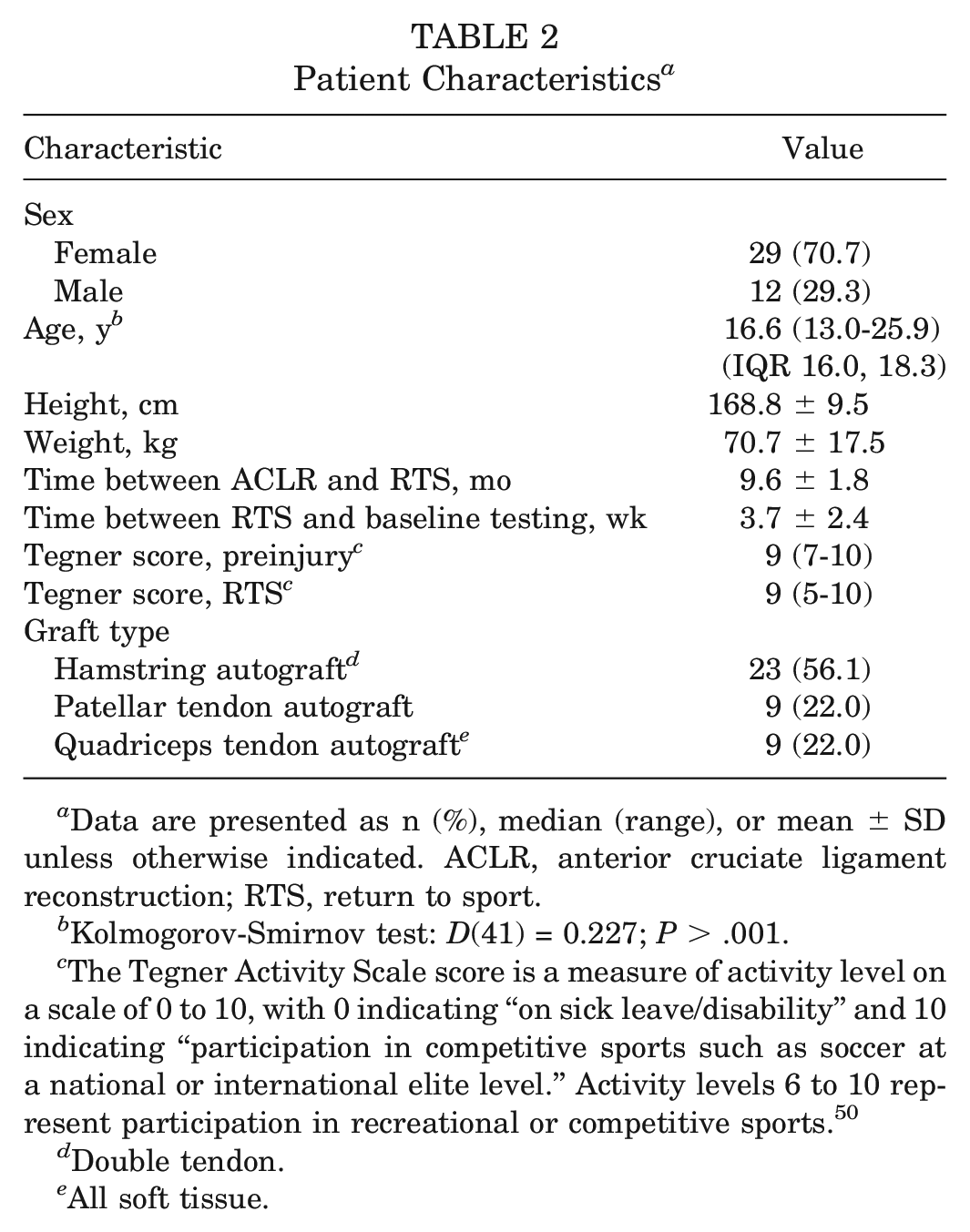
Data are presented as n (%), median (range), or mean ± SD unless otherwise indicated. ACLR, anterior cruciate ligament reconstruction; RTS, return to sport.
Kolmogorov-Smirnov test: D(41) = 0.227; P > .001.
The Tegner Activity Scale score is a measure of activity level on a scale of 0 to 10, with 0 indicating “on sick leave/disability” and 10 indicating “participation in competitive sports such as soccer at a national or international elite level.” Activity levels 6 to 10 represent participation in recreational or competitive sports. 50
Double tendon.
All soft tissue.
Actual and Perceived Physical Competence Scores for All Participants (N = 41) a
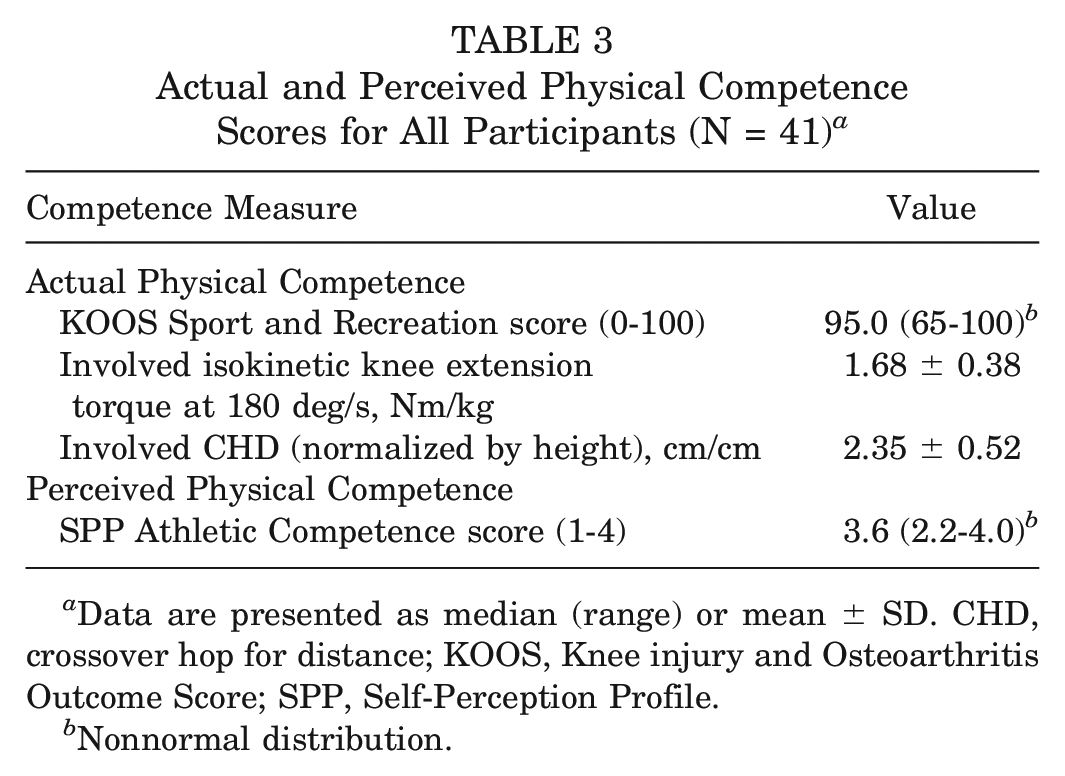
Data are presented as median (range) or mean ± SD. CHD, crossover hop for distance; KOOS, Knee injury and Osteoarthritis Outcome Score; SPP, Self-Perception Profile.
Nonnormal distribution.
Achievement of APC and PPC Criteria a
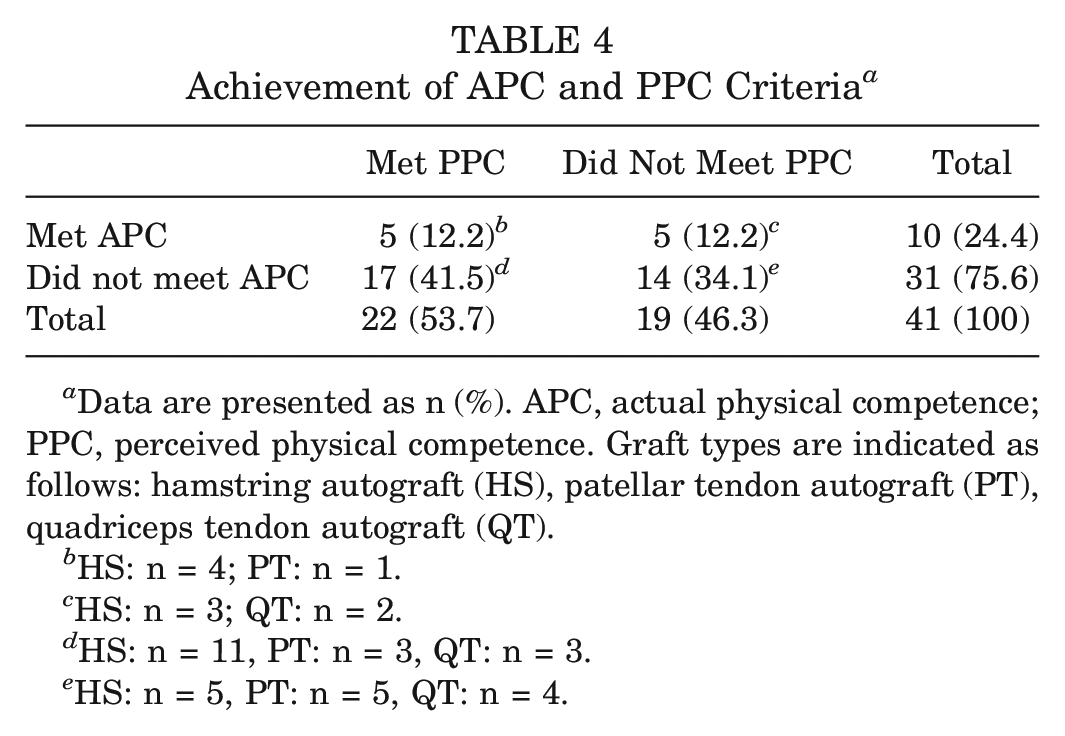
Data are presented as n (%). APC, actual physical competence; PPC, perceived physical competence. Graft types are indicated as follows: hamstring autograft (HS), patellar tendon autograft (PT), quadriceps tendon autograft (QT).
HS: n = 4; PT: n = 1.
HS: n = 3; QT: n = 2.
HS: n = 11, PT: n = 3, QT: n = 3.
HS: n = 5, PT: n = 5, QT: n = 4.
Participants Categorized by Achievement of APC Criteria a
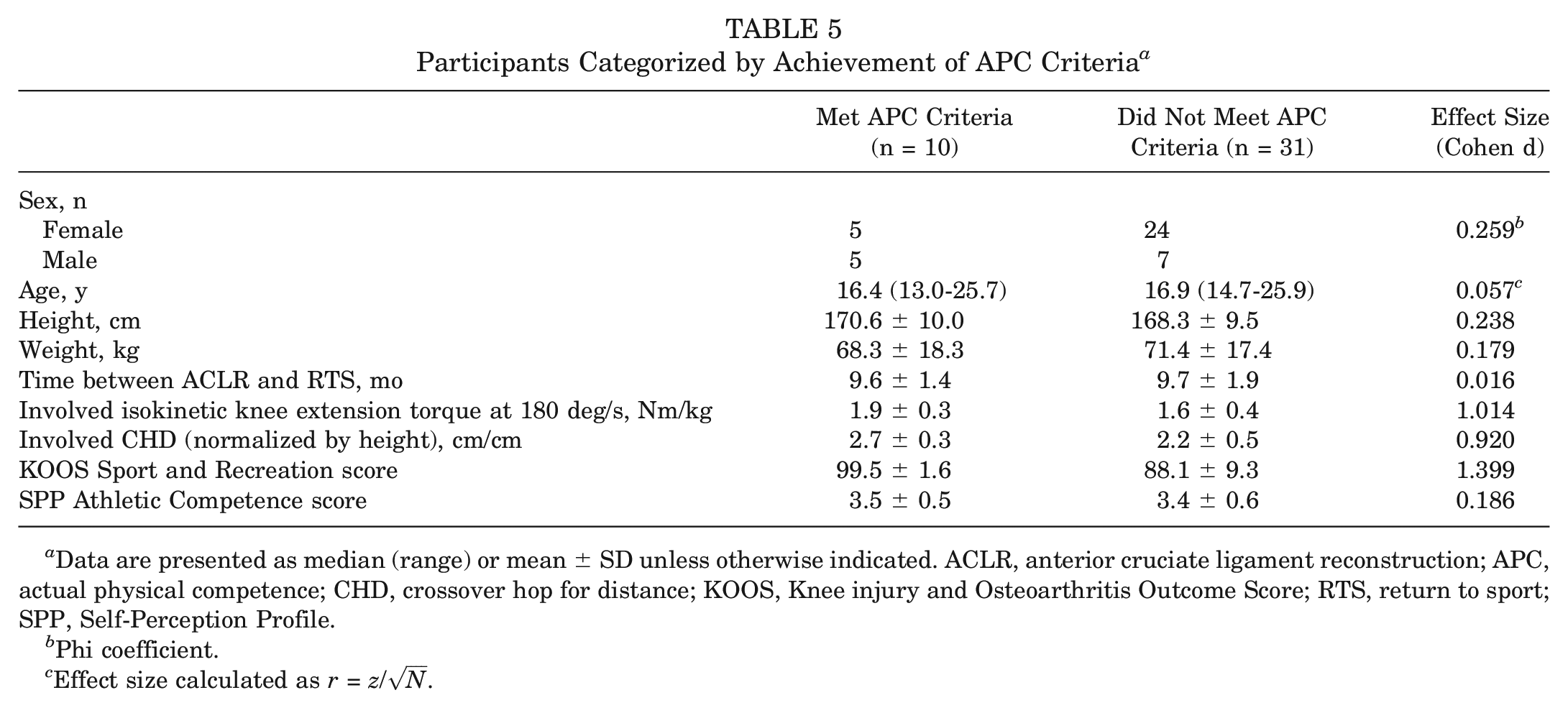
Data are presented as median (range) or mean ± SD unless otherwise indicated. ACLR, anterior cruciate ligament reconstruction; APC, actual physical competence; CHD, crossover hop for distance; KOOS, Knee injury and Osteoarthritis Outcome Score; RTS, return to sport; SPP, Self-Perception Profile.
Phi coefficient.
Effect size calculated as r = z/
Participants Categorized by Achievement of PPC Criteria a
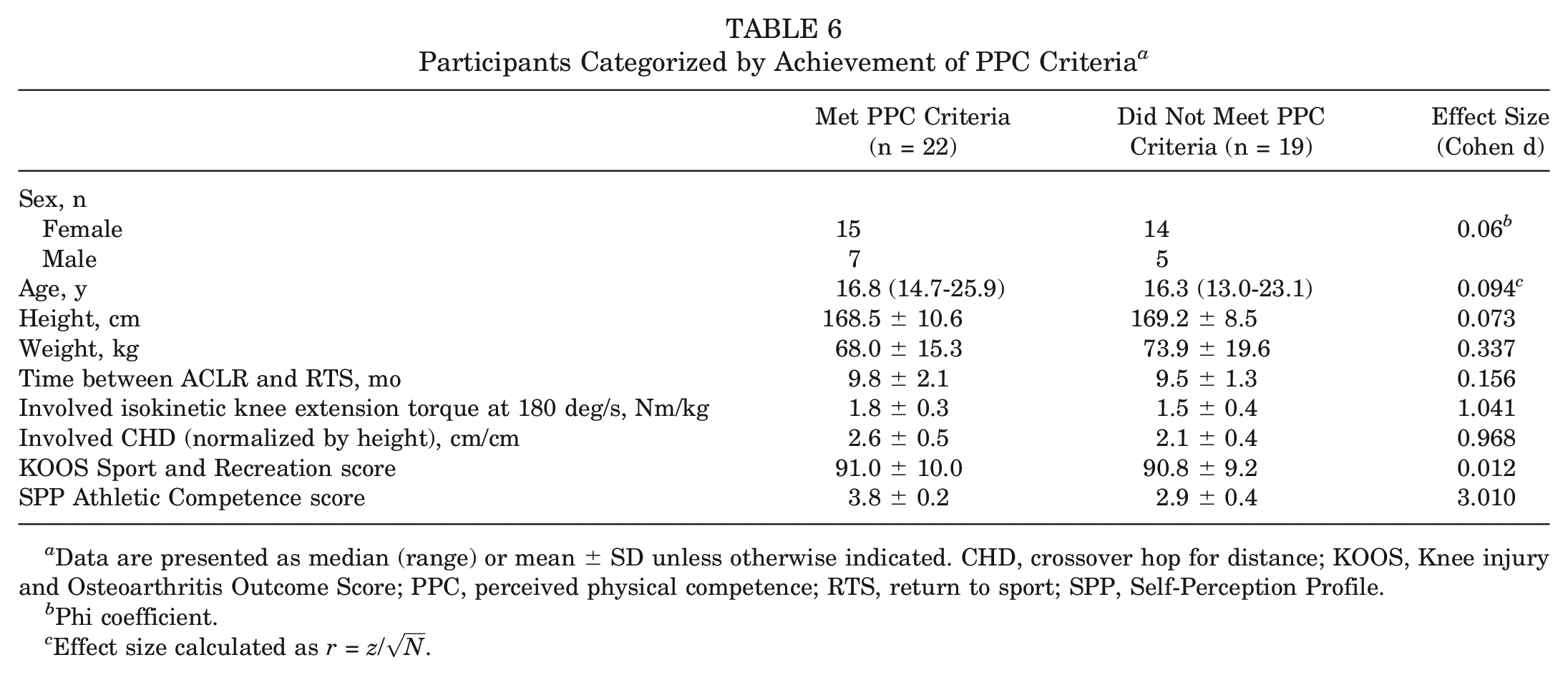
Data are presented as median (range) or mean ± SD unless otherwise indicated. CHD, crossover hop for distance; KOOS, Knee injury and Osteoarthritis Outcome Score; PPC, perceived physical competence; RTS, return to sport; SPP, Self-Perception Profile.
Phi coefficient.
Effect size calculated as r = z/
Psychological Response Scores for Entire Cohort (N = 41) a
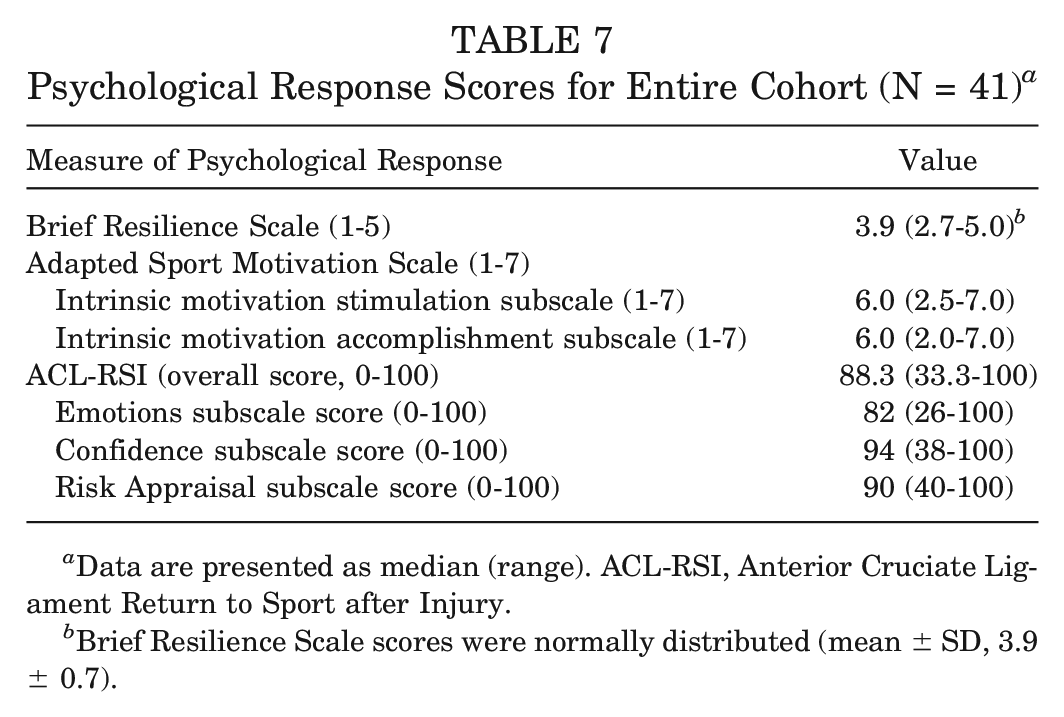
Data are presented as median (range). ACL-RSI, Anterior Cruciate Ligament Return to Sport after Injury.
Brief Resilience Scale scores were normally distributed (mean ± SD, 3.9 ± 0.7).
Based on adjustment for multiple comparisons using the Benjamini-Hochberg procedure, P values ≤.013 were statistically significant for the regression analyses (Table 8). 10 The regression model for resilience, as measured by the BRS, was not significant (F[4,36] = 1.906; P = .131; adjusted R2 = 0.083). Similarly, the regression models for intrinsic motivation stimulation (F[4,36] = 1.850; P = .141; adjusted R2 = 0.078) and intrinsic motivation accomplishment (F[4,36] = 0.746; P = .567; adjusted R2 = −0.026) as measured by the ASMS were not significant.
Regression Results for All Measures of Psychological Response a
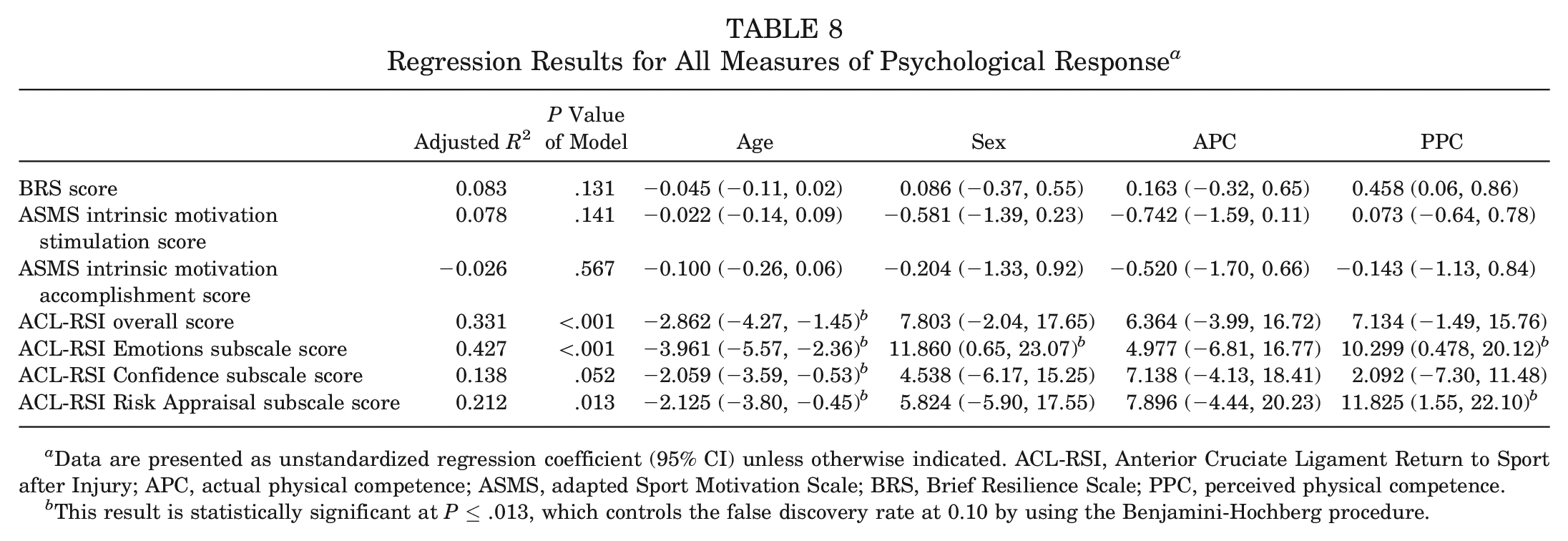
Data are presented as unstandardized regression coefficient (95% CI) unless otherwise indicated. ACL-RSI, Anterior Cruciate Ligament Return to Sport after Injury; APC, actual physical competence; ASMS, adapted Sport Motivation Scale; BRS, Brief Resilience Scale; PPC, perceived physical competence.
This result is statistically significant at P≤ .013, which controls the false discovery rate at 0.10 by using the Benjamini-Hochberg procedure.
The regression model estimating the overall score for ACL-RSI was statistically significant (F[4,36] = 5.942; P < .001; adjusted R2 = 0.331) (Table 8). Age was the only variable independently associated with the ACL-RSI overall score, explaining 28.4% of the total variance. For every 1-year increase in age, the estimated mean change in ACL-RSI overall score decreased by 2.9 points, adjusting for sex, APC, and PPC.
The regression model estimating the ACL-RSI Emotions subscale score was also statistically significant (F[4,36] = 8.440; P < .001; adjusted R2 = 0.427) (Table 8). Age, sex, and PPC were independently associated with the ACL-RSI Emotions score, explaining 35.9%, 6.6%, and 6.5% of the total variance, respectively. For every 1-year increase in age, the estimated mean change in ACL-RSI Emotions score decreased by 4.0 points. Male patients had a mean estimated ACL-RSI Emotions score that was 11.9 points higher than that of female patients, adjusting for age, APC, and PPC. Participants who met PPC criteria had a mean estimated ACL-RSI Emotions score that was 10.3 points higher than that of participants who did not meet PPC criteria, adjusting for age, sex, and APC.
Last, the regression model estimating the ACL-RSI Risk Appraisal score was statistically significant (F[4,36] = 3.694; P = .013; adjusted R2 = 0.212) (Table 8). Age and PPC were independently associated with the ACL-RSI Risk Appraisal score, explaining 13.0% and 10.8% of the total variance, respectively. For every 1-year increase in age, the estimated mean change in ACL-RSI Risk Appraisal score decreased by 2.1 points, adjusting for sex, APC, and PPC. Participants who met PPC criteria had a mean estimated ACL-RSI Risk Appraisal score that was 11.8 points higher than that of participants who did not meet PPC criteria, adjusting for age, sex, and APC.
Discussion
The purpose of this study was to determine how APC and PPC are associated with psychological response among young athletes at the time of RTS after ACLR. In partial accordance with our hypothesis, meeting PPC criteria was significantly associated with higher psychological readiness to RTS. Younger age and male sex were also positively associated with psychological readiness to RTS. Although the influence of APC on psychological response after ACLR has been studied previously,33,57 this study serves as a unique investigation of the association between PPC and psychological response in a young athlete population.
Effect of Competence on Psychological Response
The regression model estimating the association between psychological readiness to RTS, as measured by ACL-RSI, and APC, PPC, age, and sex was statistically significant. Further assessment of each ACL-RSI subscale allowed for a deeper investigation of psychological readiness domains, revealing that PPC, but not APC, was associated with participants’ reinjury anxiety (ACL-RSI Emotions subscale) and their perception of risk involved in returning to sport (ACL-RSI Risk Appraisal subscale).
Biopsychosocial models of RTS after injury suggest that one’s perception of one’s physical outcomes (eg, strength and rate of recovery) can influence affect and behavior during rehabilitation.41,59 This effect, in turn, has the potential to influence rehabilitation outcomes, such as treatment satisfaction and readiness to RTS. 41 Empirical work also indicates that a negative emotional response to injury may include fear of not meeting performance expectations, or athletic competency. 40 In the present study, young athletes who did not meet PPC criteria demonstrated more negative ACL-RSI Emotions subscale scores, representing higher reinjury anxiety. 56 Interventions aimed at improving self-perceptions of competence, such as successive approximation and systematic desensitization, have been shown to be useful for reducing fear and anxiety among professional athletes. 41 The findings from our study suggest that further work is needed for the development of interventions that facilitate high perceptions of competence among young athletes, in addition to the traditional focus on promotion of APC.
PPC was also independently associated with the Risk Appraisal construct, as participants who met PPC criteria demonstrated higher ACL-RSI Risk Appraisal subscale scores. In accordance with Mahood et al, 28 many athletes described employing “situational risk awareness” during sport participation after ACLR. This awareness was informed by the athletes’ perceptions of their movement, particularly when attempting to repeat movements that matched their ACL injury mechanism. Others emphasized the need to reach a high level of PPC at the start of every athletic exposure (eg, by engaging in a tough tackle) to build the confidence for a more positive Risk Appraisal response. 28 Furthermore, research has shown that athletes who undergo on-field rehabilitation in their sport environment also demonstrate higher ACL-RSI scores at the time of RTS. 44 Exposure to sport-specific movements and the competitive environment may serve as a means of enhancing competence before full clearance to sport participation. Together, these findings indicate that one’s perception of his or her physical abilities may inform the risk appraisal process during sport participation.
It is important to note that the regression model estimating ACL-RSI Confidence subscale scores was not statistically significant. Somewhat contrary to our findings, previous research in active young adults has shown that between-limb differences in strength 16 and jumping performance 2 may be associated with knee confidence after ACLR. However, little is known about the relationships between PPC and confidence among young athletes after ACLR. The findings of the current study would indicate that PPC may be more closely associated with the Emotions and Risk Appraisal constructs of RTS readiness.
The variance in both resilience and motivation was also not explained by factors within the regression model. Unfortunately, both constructs are not well understood as they relate to RTS after ACLR. Johnson et al 24 reported that the psychological factors perceived to enhance resilience during rehabilitation include relatedness, self-efficacy, and the ability to set goals. Physical competence has not been previously associated with resiliency after sport-related injury, nor did the results of this study indicate that competence levels are associated with self-reports of resilience. Similarly, this study found no relationship between competence and motivation to RTS after injury. Evidence has shown that young athletes who achieve ≥90% limb symmetry on muscle function tests after ACLR demonstrate higher motivation to achieve post-ACLR goals. 9 Accordingly, the self-determination theory posits that a rehabilitation experience conducive to the attainment of competence should result in higher intrinsic motivation. 45 A positively skewed distribution of scores may indicate that the ASMS subscales were not sensitive enough for the measurement of intrinsic motivation among this young population. Collectively, these findings indicate the need for further research to better understand the relationship between competence and additional domains of the psychological response after ACLR.
Special Considerations for Young Athletes After ACLR
Effect of Age and Sex
Younger age was associated with higher ACL-RSI scores. According to work from the field of developmental psychology, adolescents and young adults differ in their self-perceptions, emotional responses, and motivations related to sports. 58 The age of participants in this study ranged from 13 to 25 years, which includes developmental stages of early/middle adolescence (12-15 years), late adolescence (16-18 years), and young adulthood (19-25 years). 58 Consistent with previous research, the findings of this study indicate that athletes of a younger age demonstrate a higher psychological readiness to RTS. 9 The results also indicate that the level of psychological readiness to RTS may be associated with athletes’ psychological responses in the Emotions and Risk Appraisal domains.
Greater psychological readiness 57 and higher RTS rates 55 have been reported among the young athletes after ACLR. Unfortunately, this population also experiences higher rates of second ACL injury.35,54 The attainment of high psychological readiness to RTS may be emphasized, but it does not ensure the athlete is safe to return to unrestricted sport participation. Traditional measures of RTS readiness, 12 such as time and physical function, are considered key elements within the RTS decision-making process for young athletes after ACLR.8,30 Caution should be taken to ensure that psychological readiness is not the sole determinant of RTS readiness.
Among the larger population of patients after ACLR, male sex has also been associated with a higher ACL-RSI overall score, indicating the occurrence of sex-related differences in psychological response to ACLR. 57 Furthermore, in a qualitative study of gender differences in psychological responses after ACLR, both male and female patients reported fear related to movement and activity. However, while male patients emphasized fear of movement during sport-specific activities, female participants spoke of fear with activities of daily living and general physical activity. 27 Similarly in our study, sex-related differences were found within the ACL-RSI Emotions scores, as young male athletes demonstrated higher scores reflective of a more positive emotional response.
Actual Physical Competence
Interestingly, within these analyses, APC was not significantly associated with any measure of psychological response. One explanation may be that only 24.4% of the cohort met APC criteria. These criteria were chosen as measures most representative of clinical assessments performed for RTS decision-making. Furthermore, the APC cutoff scores were based on recent evidence of age- and activity-relevant targets for this population. 23 The low proportion of young athletes who met these criteria at the time of RTS is consistent with previous work.23,51 According to Toole et al, 51 <14% of young athletes met all recommended RTS criteria on a similar battery of tests for strength and hop performance limb symmetry, and patient-reported function. The limb sufficiency targets used in the current study, which are based on healthy control data, are known to be more difficult to achieve than limb symmetry targets among young athletes after ACLR. Despite differences in criteria, the low proportion of athletes who met APC criteria in this cohort adds further evidence to the emerging belief that young athletes are returning to sport before physical RTS readiness. The findings of this study also indicate that performance on measures of APC may not be indicative of psychological readiness to RTS.
Perceived Physical Competence
In total, 41.5% of the cohort participants met PPC criteria but did not meet APC criteria, resulting in a large proportion of “overestimators.” Even though this phenomenon has been seen previously in adolescents, 15 the present study represents the first investigation of PPC among young athletes after ACLR. As a measure of PPC, the SPP Athletic Competence subscale items asked participants to rate their physical competence skills and athletic prowess against those of their peers. 21 As a cohort consisting of young, competitive athletes, it is likely that many perceived themselves to be more athletic than their peers. Additionally, all participants had been recently discharged from rehabilitation, an accomplishment often accompanied by an increase in confidence and self-efficacy.25,44,52 Furthermore, task-specific self-efficacy (eg, ability to participate in outdoor games) is known to be derived from perceptions of one’s past performance. 19 Therefore, it may be possible that participants’ perceptions of their physical abilities were informed by perceived preinjury capabilities. These findings provide novel insight into the significance of an athlete’s self-perceptions within the development of the psychological response after ACLR.
Strengths and Limitations
The sample of participants recruited for this study were all young, active individuals attempting to return to their preinjury level of sport participation. As such, the findings from this study may not be generalizable to populations of older athletes or those not intending to RTS. However, this cohort represents the population that experiences the highest rates of both primary 42 and second ACL injury36,54,60; thus, the investigation is highly warranted. Purposefully, the study team did not control for surgical procedure across both study sites to represent the larger population of young athletes who undergo ACLR. Further research is needed to better understand the effect of graft type on both APC and PPC at the time of RTS, as >50% of the participants in this study underwent ACLR with hamstring autograft.
This study also represents the first investigation of the relationship between competence and psychological response to RTS after ACLR. As such, the definitions and criteria for both APC and PPC were operationalized for this study, which may not accurately represent one’s physical competence. Further work is warranted for the refinement of the meaning and assessment of APC within this population. Similarly, future work should aim to assess the validity of the SPP Athletic Competence subscale as a measure of PPC among young athletes after ACLR.
To our knowledge, this is the first time the BRS and ASMS have been used among a sample of young athletes after ACLR. Participants’ responses to these questionnaires were positively skewed, indicating a large proportion of positive psychological responses within these constructs. It remains to be known whether these measures are the most appropriate assessments of the psychological constructs of resilience and motivation, respectively, among this population. Other psychological factors associated with RTS outcomes, such as self-efficacy and depression, 32 were not analyzed in this study and may be important to include in future investigations.
Conclusion
In this investigation of the association between competence and psychological response to ACLR, 10 of 41 (24.4%) young athletes met APC criteria, and 22 of 41 (53.7%) met PPC criteria. In partial accordance with our hypothesis, achievement of PPC criteria, younger age, and male sex were independently significantly associated with higher scores on measures of psychological readiness to RTS. Within our analyses, APC was not associated with psychological response to ACLR. Furthermore, neither APC nor PPC was associated with resilience or motivation to RTS after ACLR.
Footnotes
Acknowledgements
The study team thanks the AOSSM for funding this work through the 2019 Return to Play Clinical Research Award.
Submitted January 25, 2023; accepted June 5, 2023.
One or more of the authors has declared the following potential conflict of interest or source of funding: This work was funded by the AOSSM through the 2019 Return to Play Clinical Research Award. R.A.M. has received support for education from CDC Medical and a grant from DJO. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.