
Abstract
Background:
Preservation of articular cartilage in the setting of acute or chronic injury in the adolescent and young adult knee is paramount for long-term joint health. Achieving osseous union, minimizing implant-related injury, and eliminating the need for reoperation for traumatic chondral and osteochondral lesions (OCLs) and osteochondritis dissecans (OCD) remain a challenge for the orthopaedic surgeon.
Purpose:
To evaluate radiographic healing, patient-reported outcomes, and short-term complications after suture-bridge fixation of chondral fragments, osteochondral fractures, and OCD lesions in the knee.
Study Design:
Case series; Level of evidence, 4.
Methods:
The study included consecutive patients (38 patients, 40 knees) treated within a single academic sports medicine institution who underwent suture-bridge fixation of an OCL or an OCD lesion of the knee from initiation of the technique in October 2019 through March 2021. The suture-bridge technique entailed bioabsorbable knotless anchors placed on the outside margins of the lesion with multiple strands of hand-tensioned absorbable (No. 0 or No. 1 Vicryl) or nonabsorbable (1.3-mm braided polyester tape) bridging suture. Healing was assessed by radiography and magnetic resonance imaging (MRI), with MRI scans obtained on all OCD lesions and any chondral-only lesions. MRI scans were available for 33 of 40 (82.5%) knees within 1 year of surgery and were evaluated for lesion healing. Complications and rates and timing of return to sport were evaluated. Patient-reported outcomes in the OCD cohort were evaluated with the Knee injury and Osteoarthritis Outcome Score (KOOS) to determine early pain and functional improvement.
Results:
In total, 33 (82.5%) lesions demonstrated full union, and no lesions failed treatment. MRI assessment of healing (mean, 5.8 months; range, 3-12 months) demonstrated 9 (64.3%) OCD lesions with full union, 5 (35.7%) OCD lesions with stable union, and no OCD lesions with nonunion. Of the OCLs, 17 (89.5%) had full union, 2 (10.5%) had stable union, and none had nonunion. The 7 bony OCLs without an MRI scan demonstrated complete radiographic union. In 30 (75.0%) lesions, patients returned to sports at a mean of 6.5 months (range, 3.8-10.2 months). KOOS Activities of Daily Living, Pain, Quality of Life, and Symptoms scores demonstrated significant improvement from baseline at 6 months and at 1 year. There were 2 (5%) complications, consisting of reoperation for marginal chondroplasty on an otherwise stable lesion, and re-operation for intial un-treated patellar instability, with no reoperations for failure or revision of the suture-bridge construct.
Conclusion:
In this series of OCLs and OCD lesions of the knee, suture-bridge fixation demonstrated excellent rates of MRI and radiographic union and good early outcomes with minimal short-term complications. This technique may be used for lesion salvage as an alternative to metallic and nonmetallic screw/tack constructs in the treatment of these challenging lesions. Longer term follow-up and investigation are warranted.
Keywords
Preserving articular cartilage in the setting of acute or chronic injury in the adolescent and young adult knee is paramount for long-term joint health. Chondral and osteochondral lesions (OCLs) of the knee are significant sources of pain and joint dysfunction. 21 Acute patellofemoral instability and osteochondritis dissecans (OCD) of the knee are common conditions found in active adolescents treated at a pediatric sports medicine practice for symptomatic OCLs.
Osteochondral and chondral fractures of the patella, trochlea, and lateral femoral condyle are well-known concomitant injuries associated with acute patellofemoral instability events. OCD is a focal idiopathic alteration of subchondral bone or its epiphyseal cartilage precursors with risk for instability and disruption of adjacent articular cartilage that may result in premature osteoarthritis. 37 OCD of the knee is an increasingly recognized pathology in the adolescent and young adult knee and often presents as an unstable lesion requiring operative treatment.1,2,22,43,44 Treatment options for OCLs and unstable OCD lesions include fixation, debridement and marrow stimulation, osteochondral autologous graft transfer, osteochondral allografting, and matrix-associated autologous chondrocyte implantation. ‡ Lesion fixation may be preferable, when possible, in order to reduce donor-site morbidity from autologous grafts and potentially avoid a second operation when osteochondral allograft is used.
Traditional osteochondral fixation methods have reports of good healing rates with both bioabsorbable implants and metallic compression screws. However, bioabsorbable implants have demonstrated implant-related complications associated with breakage and variable rates of degradation and loss of compressive forces. Complications associated with metallic headless screws may include screw backout or guidewire breakage, and most authors advocate for a second surgery for screw removal.5,16,47 Limited data are available on the short-term complications and outcomes and the healing rates of OCLs and OCD lesions after suture-bridge fixation.4,9,23
Thus, the purpose of this study was to evaluate osseous and chondral integration after a suture-bridge construct using magnetic resonance imaging (MRI) scans and/or radiographs. A secondary purpose was to assess the outcomes and short-term complications of suture-bridge fixation of OCLs and OCD lesions in the knee. It was hypothesized that good results equivalent or superior to other techniques would be observed.
Methods
Institutional review board approval (protocol No. 062017-100) was obtained, with a waiver of informed consent, before data collection. We reviewed consecutive patients (38 patients, 40 knees) who underwent suture-bridge fixation of an OCL or an OCD lesion of the knee from initiation of the technique in October 2019 through March 2021. All such lesions treated using this technique were included. OCD lesions treated with isolated drilling or other fixation techniques were excluded. Radiographic and MRI measurements were recorded, and prospectively collected patient-reported outcome measures (PROMs) were analyzed. We documented patient demographic characteristics and preoperative MRI lesion characteristics, including lesion type (OCL vs OCD), presence of bone within the fragment, lesion size, and lesion location. Arthroscopic versus open surgical fixation method and absorbable versus permanent suture type were recorded. OCLs with a visible bone component were evaluated for healing using multiplanar radiographs. For inclusion in this study, purely chondral lesions and all OCD lesions were required to have an MRI within 12 months of the procedure for assessment of lesion healing. We analyzed complications, rates and timing of return to sports, and the Knee injury and Osteoarthritis Outcome Score (KOOS).
Patient Characteristics
Patient characteristics and mechanism of injury were collected retrospectively using chart review of the electronic medical record (EPIC). Standardized questionnaires regarding injury mechanism and athletic participation were collected prospectively and used for data in this study. Pre- and postoperative physical examination data were recorded. Surgery data were recorded to include the size, type, and number of implants used as well as the number of suture strands used. Concomitant procedures were recorded from operative reports and intraoperative and arthroscopic photographs.
Radiologic Data
Pre- and postoperative radiographic and MRI data were reviewed for all patients. The preoperative MRI scan was reviewed for classification of lesion type, size, and location as well as concomitant injury. Lesion size was defined and recorded as length of the lesion multiplied by the width: length (mm) × width (mm) = size (mm2). Lesion major length was defined and recorded as the larger dimension of the lesion's length or width measured in millimeters. MRI scans were available for 33 of 40 (82.5%) knees within 1 year of surgery and were evaluated for lesion healing. MRI was available in all OCD lesions. The postoperative MRI scan was reviewed for classification of chondral and osseous integration as well as the number of anchors used in the suture-bridge construct and the type of suture used (absorbable vs permanent). Lesions were classified as full union (100% cancellous or cancellous–chondral lesion continuity), stable union (>50% continuity with some fibrous tissue present), or nonunion (<50% continuity and extensive fibrous signal or fluid signal below the lesion).
Surgical Technique
A standard knee arthroscopy was performed by 1 of 2 fellowship-trained, pediatric orthopaedic sports surgeons (P.L.W. or H.B.E). In the OCL cohort, the fracture fragment was mobilized and removed via an enlarged arthroscopic portal and taken to the back table for inspection and debridement of the synovialized and nonviable elements on the undersurface of the fracture fragment in preparation for fixation. In subacute lesions, chondral hypertrophy was commonly noted and the fragment was trimmed to appropriate size for reduction and fixation. A limited arthrotomy was performed with an infrapatellar approach for condylar lesions and a limited parapatellar approach allowing 90° of eversion of the patella for patellar lesion treatment. Uncommonly, for large trochlear or far posterior condylar lesions, a full medial parapatellar arthrotomy was used. The fracture bed was debrided and prepared with irrigated drilling with a 0.045-inch Kirshner wire (K-wire) followed by use of a single, midlesion K-wire through the reduced fragment for manipulation and provisional fixation. A suture-bridge construct was then performed beginning with placement of either a sliding bioabsorbable poly-L-lactide (PLLA) suture anchor or a slotted, knotless bioabsorbable PLLA suture anchor (Arthrex) that was loaded with a single or double strand of size 0 or No. 1 Vicryl suture (Ethicon) at the visually determined periphery of the lesion, with care taken to place the anchor at the level of the subchondral bone below the chondral surface. When a suture anchor was used, a size 0 or No. 1 Vicryl suture was spliced through the permanent suture and shuttled through the anchor, replacing the permanent suture with an absorbable suture. A slotted, knotless, bioabsorbable suture anchor was then loaded with each of the used free ends of the absorbable suture from the initial anchor and was positioned across the chondral surface of the fracture and tensioned under visual inspection in sequential fashion at the periphery of the lesion, with care taken not to overtension the suture to avoid cutting into the chondral surface. In most OCLs, the lesion was treated concurrent with patellar instability treatment using an allograft medial patellofemoral ligament (MPFL) reconstruction.
In the OCD cohort, the lesion was carefully examined and characterized using the Research in Osteochondritis of the Knee (ROCK) arthroscopic classification scheme. 7 A mini-arthrotomy was used to either remove the lesion (for displaced lesions or at the surgeon's discretion for improved lesion preparation) or hinge open the lesion for debridement and repair. In 2 cases (1 medial femoral condylar locked door lesion and 1 lateral trochlear locked door lesion), the OCD lesion underwent transarticular drilling and in situ arthroscopic fixation. Standard OCD lesion preparation included fibrous tissue debridement and curettage of the parent bed to viable cancellous bone. Next, irrigated fine-wire drilling with a 0.045-inch K-wire was used within the parent bed for additional marrow stimulation followed by local (proximal tibial or distal femoral) autologous cancellous bone grafting in most cases. Compacted morselized bone graft was used to fill any resultant cavitary defect between the parent and progeny fragments and was adjusted to achieve appropriate chondral reduction with the surrounding native surface. Provisional fixation of the OCD progeny with a 0.045-inch K-wire was performed followed by placement of an absorbable suture-anchor, suture-bridge construct as described above for OCL fixation. In contrast to the OCL suture-bridge fixation technique, 1.3-mm permanent polyester braided suture tape (Arthrex) was used in some OCD lesions to provide longer compression and stability in the setting of chronic avascularity and interpositional bone grafting inherent to these repairs.
Postoperatively, patients were instructed to be flat-foot touch weightbearing with immediate early active assisted and passive range of motion to full range of motion. A locked range of motion brace was used to assist mobility until full range of motion and quadriceps control were achieved. At 6 weeks, patients were transitioned to full weightbearing; an unloader brace was occasionally used at the surgeon's discretion for condylar lesions during early weightbearing. Concentric, nonimpact strengthening was initiated at approximately 8 weeks with subsequent impact activity after confirmation of union by imaging.
Outcome Measures
For assessment of early pain and functional improvement in the setting of isolated osteochondral treatment (without confounding concurrent patellar instability or other treatment in conjunction with OCL treatment), we analyzed prospectively collected KOOS outcome scores. 41 These scores were collected prospectively as part of a standardized, electronically delivered PROM platform (OBERD) that has demonstrated reliability in the pediatric and adolescent setting. 42 Baseline and 6- and 12-month KOOS outcome scores were analyzed. Clinical and operative data from the electronic medical record were reviewed for complications and the rates and timing of return to sport.
Statistical Analysis
Descriptive statistics were reported as mean and standard deviation. All continuous variables were compared using nonparametric tests, such as the Kruskal-Wallis and Mann-Whitney U test, as appropriate. For categorical variables, a Fisher exact test was used. Statistical significance was set at P < .05. Missing data were excluded from analysis, and the number of patients available for each variable was noted. Statistical analysis was performed using SAS Version 9.4 (SAS Institute).
Results
Patient Characteristics
After application of our inclusion criteria, 26 OCLs (12 condylar and 14 patellar) and 14 OCD lesions (8 condylar, 3 trochlear, 3 patellar), for a total of 40 knees in 38 patients, were available for study. The total sample had a mean age of 14.9 years (range, 10.1-21.6 years) and a mean body mass index of 25.1 (range, 18.6-40.7), and 45% of patients were White; 23 (57.5%) were male. Two patients had bilateral knee lesions, 1 patient in each cohort. There were no statistically significant differences in demographic characteristics between the 2 groups. We found that 24 of 26 (92.3%) OCLs were associated with an acute patellofemoral instability event and underwent concurrent MPFL reconstruction. One patient had an isolated lateral femoral condylar chondral shear type fracture when landing after heading a ball during a club soccer match, and 1 patient had a medial femoral condylar osteochondral fracture in the setting of an acute anterior cruciate ligament tear and LaPrade type 2 posterior lateral meniscus root tear. OCLs were treated at a mean of 26 days (range, 3-164 days) from injury overall, with purely chondral lesions treated at a mean of 19 days (range, 11-37 days).
Lesion Characteristics
For all patients and knees, a preoperative MRI scan was reviewed for classification of lesion type, size, and location as well as concomitant injury. The OCL mean size was 235.6 mm2 (range, 96-460 mm2) and mean major length was 17.7 mm (range, 11-27 mm). In total, 21 of 26 (80.8%) OCLs were osteochondral lesions, with 5 purely chondral lesions treated. Fourteen (53.8%) OCLs were patellar lesions, with a mean size of 215.2 mm2 (range, 140-368 mm2) and a mean major length of 17 mm (range, 14-23 mm). Twelve OCLs were lateral femoral condylar lesions, with a mean size of 314.3 mm2 (range, 216-459 mm2) and a mean major length of 21 mm (18-27 mm). The OCD lesions were significantly larger than the OCL lesions, with an OCD lesion mean size of 362 mm2 (range, 130-780 mm2), mean major length of 20.4 mm (range, 13-30 mm), and mean depth of 9.5 mm (range, 5.3-14 mm). Eight of 14 (57.1%) OCD lesions were condylar, with 3 each in patellar and trochlear locations. Ten (71.4%) OCD lesions had bone in the progeny at the time of treatment (Table 1).
Patient and Lesion Characteristics a
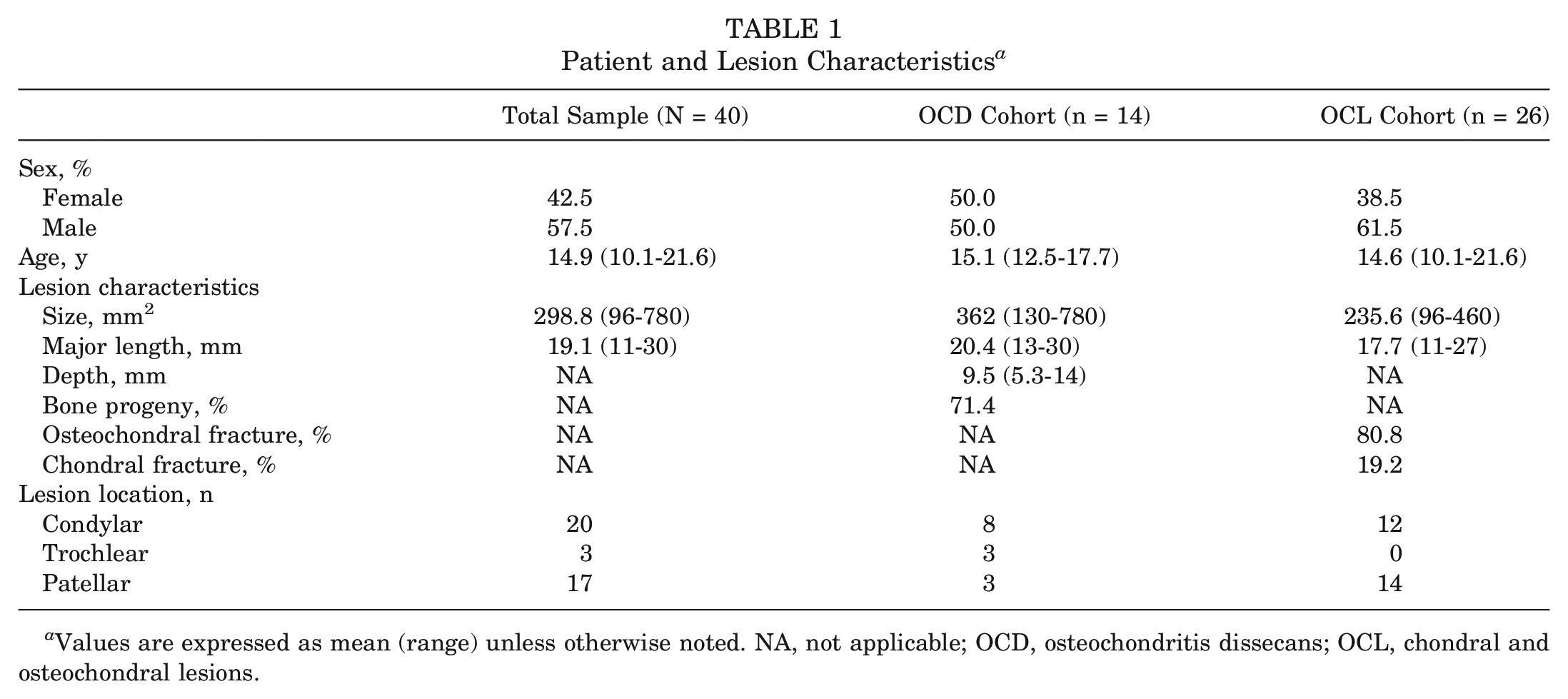
Values are expressed as mean (range) unless otherwise noted. NA, not applicable; OCD, osteochondritis dissecans; OCL, chondral and osteochondral lesions.
OCD lesions were further classified at the time of arthroscopy using the ROCK classification system. All 14 were noted to have surface characteristics of instability; 12 (85.7%) were found to have gross instability (9 trapdoor and 3 crater lesions) and subsequently underwent mini-arthrotomy. The 2 locked door lesions were treated arthroscopically in situ after transarticular drilling. In all cases involving a trapdoor, the lesion was elevated or hinged open and the avascular fibrous tissue was debrided, as was also performed in the 3 crater lesions. Autologous local cancellous bone grafting was performed in 10 of 12 (83.3%) OCD lesions requiring an arthrotomy. Absorbable suture was used in the suture-bridge construct in 10 (71.4%) OCD lesions. Permanent polyester braided suture tape was used in the suture-bridge construct in 4 OCD lesions at the surgeon's preference, seeking longer term compression of the lesion than what can be expected from an absorbable suture construct. All cases of nonabsorbable fixation were recommended for arthroscopic suture removal between 3 and 6 months.
Radiologic Outcomes and Complications
Of the total sample of knees, 33 (82.5%) lesions demonstrated full union, and no lesions exhibited early treatment failure at a mean of 16.3 months (range, 4-46.2 months). MRI assessment of healing (5.8 months; range, 3-12 months) demonstrated 9 of 14 (64.3%) OCD lesions with full union, 5 of 14 (35.7%) OCD lesions with stable union, and none with nonunion (Figure 1). Of the 26 OCLs, 24 (92.3%) had full union, 2 (7.75%) had stable union, and none demonstrated nonunion (Figure 2). All 7 bony OCLs without an MRI scan demonstrated radiographic union. All 5 purely chondral lesions were among the completely healed lesions. We found no association with the number of anchors used in the suture-bridge construct or the type of suture used and union classification.
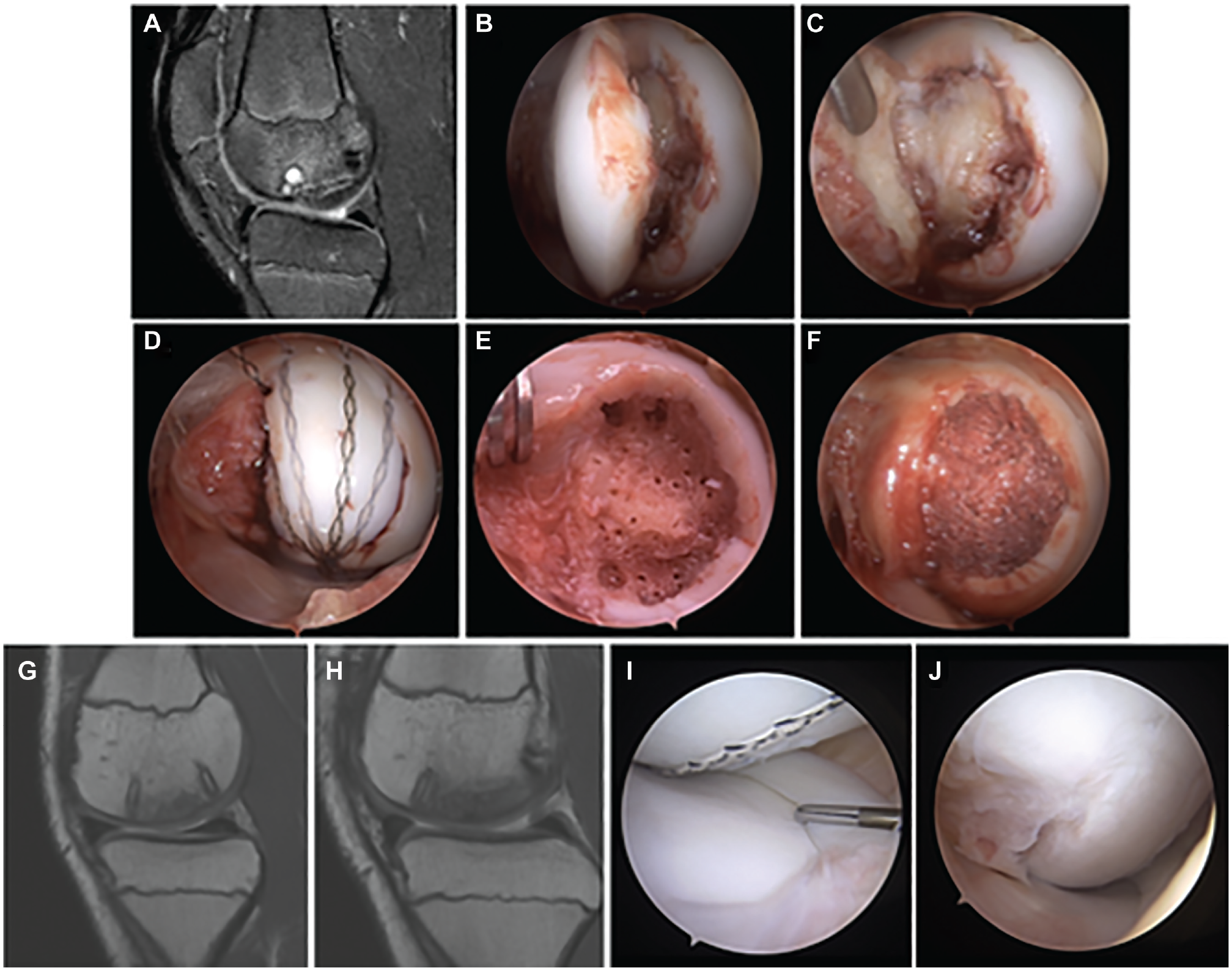
Osteochondritis dissecans (OCD) lesion treated with suture-bridge fixation. (A) Sagittal proton density magnetic resonance imaging (MRI) scan of unstable OCD lesion with minimal ossification within the progeny fragment. (B and C) Unstable progeny fragment and fibrous interposed tissue at arthrotomy after arthroscopic examination. (D) Parent bed of the OCD lesion after fibrous and cystic tissue debridement and fine wire drilling. (E) Cancellous autograft bone within the parent bed. (F) Suture-bridge fixation of the progeny articular fragment using bioabsorbable knotless anchors and braided polyester tape suture. (G and H) Sagittal proton density MRI scan of healed lesion 6 months postoperatively. (I and J) Arthroscopic images of healed lesion at suture removal 6.5 months postoperatively.
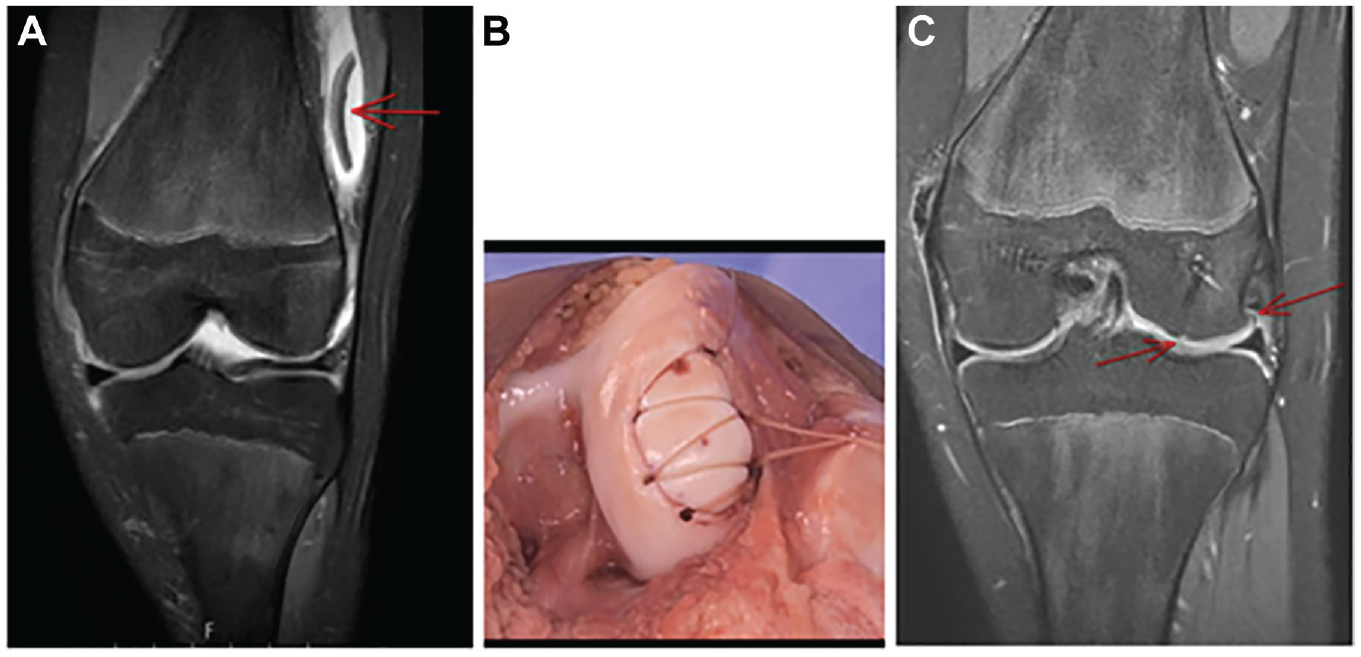
Typical adolescent osteochondral lesion (OCL) treated with suture-bridge fixation. (A) Preoperative magnetic resonance imaging (MRI) scan of OCL occurring in the setting of patellar instability. OCL in lateral gutter with minimal subchondral bone present (arrow). (B) Intraoperative image of OCL fixed concurrent to medial patellofemoral ligament reconstruction (MPFLR). Suture-bridge construct using bioabsorbable knotless anchors and No. 0 Vicryl absorbable suture. (C) Postoperative MRI scan (6 months postoperatively, with femoral-sided MPFLR visualized medially) demonstrating full union of the lesion with no fluid or fibrous signal and with full incorporation and appropriate cartilage signal (arrows).
There were 2 (5%) complications (1 in each cohort of OCL and OCD lesions) that required reoperation for marginal chondroplasty (1 of which had also been indicated for primary patellar stabilization) on otherwise stable lesions. The complication in the OCL cohort entailed a repeat arthroscopy for chondroplasty and marrow stimulation of the distal 20% margin of a patellar OCL that was associated with a patellar instability event. The remaining cartilage displayed no additional fissuring on the fragment or the opposing surface. This was notably the largest patellar OCL in the series, at 368 mm2 in size and 23 mm in major length, and was determined to be 80% healed at the time of repeat arthroscopy. The arthroscopic and intraoperative images as well as the operative report from the index procedure were reviewed, which demonstrated comminution and a small residual osteochondral defect of the distal margin of the OCL donor site. The complication in the OCD cohort involved an unplanned second surgery for an arthroscopically assisted MPFL reconstruction after suture-bridge fixation of a trochlear OCD crater lesion in the setting of trochlear dysplasia without patellar stabilization performed at the primary procedure. Further review of the patient's medical history and preoperative MRI scan revealed no evidence of a history of patellar instability or microinstability and no evidence of MPFL incompetence to suggest the need for patellar stabilization at the index procedure. The cartilage on the repaired fragment displayed no additional fissuring on the fragment or the opposing surface. No reoperations for early failure or revision of a suture-bridge construct were required in our series.
PROMs and Return to Sport
In total, 30 (75.0%) knees in 30 patients returned to sports at a mean of 6.5 months (range, 3.8-10.2 months). Of knees that eventually returned to sports, 24 (80.0%) returned to their preoperative level of activity. In the OCD cohort, KOOS Activities of Daily Living, Pain, Quality of Life, and Symptoms scores demonstrated improvement from baseline at 6 months and at 1 year. Notably, the KOOS Quality of Life measure increased >100% from baseline to final follow-up (baseline, 37.5 ± 14.7; 12 months, 76.6 ± 23.8; P < .01), and all measures demonstrated progressive and significant improvement (Table 2).
Patient-Reported Outcomes in the OCD Cohort a
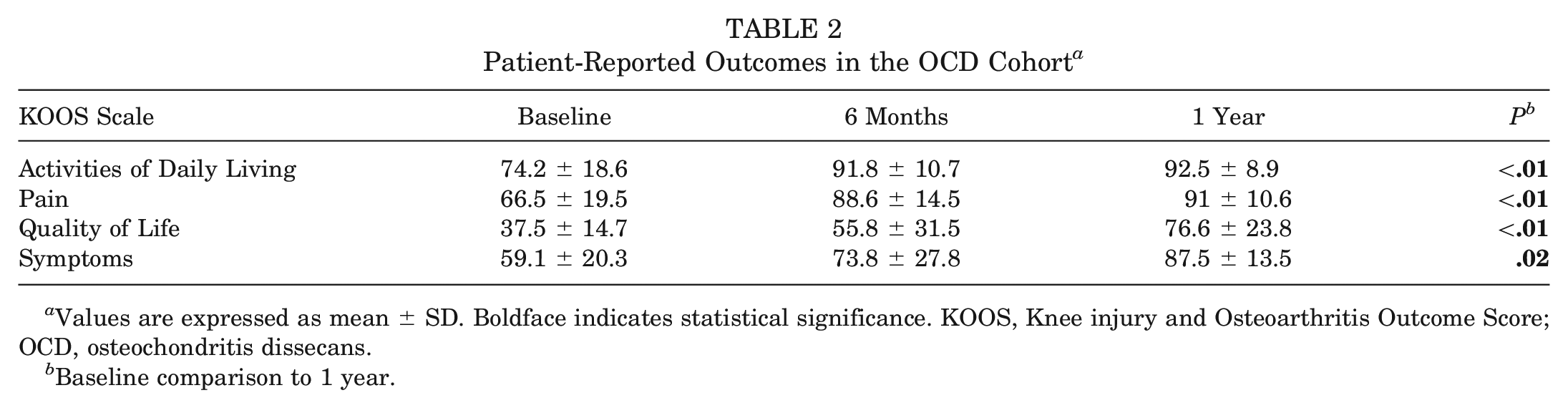
Values are expressed as mean ± SD. Boldface indicates statistical significance. KOOS, Knee injury and Osteoarthritis Outcome Score; OCD, osteochondritis dissecans.
Baseline comparison to 1 year.
Discussion
In this series of suture-bridge fixation for traumatic chondral and osteochondral lesions and OCD lesions of the knee, excellent rates of complete MRI and radiographic union (82.5%) were demonstrated. All lesions in each group exhibited >50% bone incorporation, and there were no early failures. Purely chondral lesions and just over 90% of OCLs exhibited full union with the use of an absorbable Vicryl construct. The OCD lesions represented a challenging cohort of large, unstable lesions. Most required extensive debridement and autologous bone grafting before suture-bridge fixation. Nine of the 14 OCD lesions (64.3%) had full osseous union on MRI, 5 (35.7%) had stable union, and none demonstrated nonunion.
The majority of patients (in 30 of 40 treated lesions; 75.0%) were able to return to sports at a relatively early time point of 6.5 months on average (r = 3.8-10.2). Patient-reported outcomes were assessed in the OCD cohort to allow assessment of the suture-bridge intervention without the confounding associated patellar stabilization performed in the majority of acute lesions. PROMs demonstrated that the suture-bridge technique provided significant relief of symptoms and improvement of function related to OCD of the knee. KOOS subscale scores (Activities of Daily Living, Pain, Quality of Life, and Symptoms) demonstrated significant improvement from baseline at 6 months and 1 year. Complication rates were low after this technique, with no cases of stiffness, infection, wound complications, or reoperation for early lesion repair failure. There were 2 reoperations: 1 procedure for 20% marginal lesion chondroplasty and 1 case in which primary patellar stabilization was required in an unplanned second surgery after suture-bridge fixation of a trochlear OCD crater lesion in the setting of trochlear dysplasia without patellar stabilization performed at the primary procedure.
Salvage of OCLs and OCD lesions has significant support within the literature, but challenges exist and it is not clear which care techniques are best.43,44 In a recent retrospective series, fixation of large osteochondral fractures associated with first-time patellofemoral instability yielded significantly better mid- to long-term clinical outcome scores (International Knee Documentation Committee, P < .001; KOOS, P = .006; Lysholm, P = .001) than debridement. 18 Other studies have shown good outcomes with fixation of osteochondral fractures, § whereas a very limited number of studies and case reports of chondral fracture fixation have also shown good healing rates and outcomes.8,14,24,31 Several osteochondral and chondral fracture fixation methods have been developed and described, including bone plugs, bioabsorbable pins, meniscal arrows, fibrin glue, metallic and bioabsorbable headless compression screws, and, more recently, suture-bridge constructs.13,20,29,31,46 The optimal osteochondral and chondral fracture fixation method to minimize implant-related complications or reoperation remains unclear and continues to present challenges to the treating surgeon.
Operative intervention with lesion drilling and stabilization/fixation for unstable, salvageable OCD lesions is generally agreed upon and has shown superior outcomes compared with debridement and marrow stimulation.22,26,43 However, optimal fixation methods and choice of implants remain unclear, and there are only limited, evidence level 4 studies evaluating bioabsorbable implants and/or metal screws. A paucity of evidence exists, particularly in the pediatric literature, comparing bioabsorbable implants versus metallic screws. In a study of 20 skeletally immature knees with OCD, Webb et al 47 reported that bioabsorbable implants had high rates of failure and complications, whereas metallic headless compression screws showed excellent healing and no complications. These findings support an earlier study in the adult literature by Millington et al, 36 who found that 18% of adult patients treated with bioabsorbable nails required reoperation. In a study of 30 knees in skeletally immature patients with OCD treated with bioabsorbable headless compression screws, Camathias et al 5 found that 23% of screws had broken at the time of MRI assessment and 17% of patients required revision surgery for mechanical symptoms. Drawing on MRI evidence, the investigators hypothesized that early degradation was the possible cause of implant failure. Similar to observations in skeletally immature patients, high healing rates, good outcomes, and low complication rates have been observed in OCD lesions in adults treated with metal headless compression screw fixation. 3 Although the current literature seems to favor the use of metallic headless compression screws for unstable OCD lesions, many surgeons recommend a second surgery for implant removal, and metal artifact from these implants can limit MRI evaluation of the knee, which has further encouraged the development of suture-bridge construct techniques.
In recent years, investigators have described suture-bridge fixation techniques for knee OCD; however, to date, no studies have described outcomes or complications. Barth et al 4 first described an all-arthroscopic retrograde suture fixation technique for nondisplaced patellar OCD lesions, proposing the following advantages: avoiding the morbidity of an arthrotomy, providing direct perpendicular compression similar to that of antegrade headless screw implantation, providing compression superior to that of retrograde bioabsorbable pins, avoiding potential inflammatory effects or breakage of bioabsorbable implants, and preventing the need for additional surgery for implant removal. The technique entails retrograde drilling through the center of the lesion and passage of multiple, bioabsorble No. 1 polydioxanone sutures in a clockwise fashion around the lesion, which are then tensioned with suture knots tied over the anterior surface of the patella under direct arthroscopic visualization. Barth et al did not report outcomes in their description of the technique, citing the rarity of patellar OCD lesions.
Chernchujit and Artha 9 later described an arthroscopic suture anchor fixation technique for unstable medial femoral condyle OCD lesions, also proposing the advantages of an arthroscopic all-suture technique, wide distribution of compressive force across the lesion, and absence of the need for hardware removal. Their technique entails elevation of the lesion, leaving a lateral hinge attached to the posterior cruciate ligament fibers; preparation of the bony bed with curettage of fibrous tissue and marrow stimulation with K-wire drilling; provisional K-wire reduction and fixation; and placement of a double-arm suture anchor with free limbs shuttled through and secured with knots to the posterior cruciate ligament after provisional K-wire removal. Patients are then immobilized in a long-leg cast in full extension to compress the lesion for 2 weeks.
Most recently, Ishibashi et al 23 described a suture-bridge internal fixation technique for knee OCD using slotted knotless suture anchors. In contrast to previous suture-bridge fixation techniques for knee OCD, Ishibashi et al advocated for use of their technique with both unstable and detached lesions, and the technique may be performed either arthroscopically or via arthrotomy. Similarly, the authors recommend hinged elevation of the lesion, bony bed preparation with curettage and marrow stimulation, and provisional fixation. A free No. 2-0 permanent polyester braided suture is then threaded through the first of 3 knotless suture anchors and malleted into place flush with the subchondral bone, leaving 2 suture limbs implanted. Then 1 limb of each suture is threaded through an additional knotless anchor and is tensioned and anchored into place in sequential fashion in a triangular pattern, and the remaining suture is cut flush at the level of the articular surface.
In the current series, absorbable suture anchors and slotted knotless anchors were used for fixation of the majority of traumatic osteochondral defects and OCD lesions. However, in 4 OCD lesions, a nonabsorbable polyester suture was selected given the chronicity and interposed bone graft required to treat a large lesion. The timing of suture removal in such cases and the possible effect on the opposing cartilage surface are unclear and require significant future study. Additional questions regarding tension required, mechanical and chemical effects to the chondral surface, and longevity of the chondral surface on the salvaged fragment will need to be answered. However, with this technique, a high percentage of lesions were stabilized and treated to union with no early implant-related complications or reoperations. The high osseous union rates achieved and the ability to minimize complications and reoperations make this technique attractive for further study. The large OCD lesions with significant fibrous interposition and instability requiring extensive debridement responded well to this fixation method. These lesions, similar to purely chondral acute lesions, often have very little bone available for screw fixation. The variability of compression across these often nonuniform lesions and the prolonged healing time required are additional factors that make the suture-bridge technique particularly appealing.
The limitations of this study are those primarily inherent to a retrospective series. No concurrent comparison group was available for study. The method of including all consecutive cases using this technique limits bias; however, this technique was not used exclusively for osteochondral lesions during the study time frame, and therefore some selection bias may remain. Intraoperative variables such as implant location, implant and suture density, quality of debridement, quantity of bone graft, and absorbable versus permanent suture were not controlled for within the series. With only 4 cases that involved nonabsorbable suture, no meaningful analysis of that variable was possible during the study. Additionally, the method of early imaging outcome does not allow for adequate follow-up of intermediate and late lesion survival. Regarding chondral lesions, the fragments were not histologically examined and chondral fragments were judged to be purely chondral when devoid of bone discernible by gross visualization; therefore, it is possible that some microscopic bone elements may have been present. Finally, the mixture of acute traumatic and chronic osteochondritis lesions makes comparison across the entire group difficult. However, the report of consecutive cases in a high-volume center with surgeons experienced in multiple techniques for lesion preservation and repair is a relative strength of the study.
Conclusion
The suture-bridge technique for OCL and OCD fixation may be a useful alternative to metallic and nonmetallic screw/tack constructs. In this study, 92% of OCLs and 64% of unstable OCD lesions demonstrated full osseous union, and no lesions in 40 knees required reoperation for failure of repair. Rates of complications and reoperation were low, and significant improvements were seen in patient-reported outcomes, with 75% of patients returning to sports. In the setting of these large, challenging OCD lesions and large traumatic osteochondral defects, salvage techniques may not always achieve good results, and the early promising results in this series warrant further study.
Footnotes
Submitted February 17, 2023; accepted June 14, 2023.
One or more of the authors has declared the following potential conflict of interest or source of funding: P.L.W. has received support for education from Pylant Medical. H.B.E. has received support for education from Pylant Medical and hospitality payments from Stryker Corporation. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.