
Abstract
Background:
There are limited data comparing the beach-chair (BC) versus lateral decubitus (LD) position for arthroscopic anterior shoulder stabilization.
Purpose:
To identify predictors of instability recurrence and revision after anterior shoulder stabilization and evaluate surgical position and glenoid bone loss as independent predictors of recurrence and revision at short- and midterm follow-ups.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
A consecutive series of 641 arthroscopic anterior stabilization procedures were performed from 2005 to 2019. All shoulders were evaluated for glenohumeral bone loss on magnetic resonance imaging. The primary outcomes of interest were recurrence and revision. Multivariable logistic regression models were used to assess the relationships of outcomes with age, position, glenoid bone loss group, and track.
Results:
A total of 641 shoulders with a mean age of 22.3 years (SD, 4.45 years) underwent stabilization and were followed for a mean of 6 years. The overall 1-year recurrent instability rate was 3.3% (21/641) and the revision rate was 2.8% (18/641). At 1 year, recurrence was observed in 2.3% (11/487) and 6.5% (10/154) of BC and LD shoulders, respectively. The 5-year recurrence and revision rates were 15.7% (60/383) and 12.8% (49/383), respectively. At 5 years, recurrence was observed in 16.4% (48/293) and 13.3% (12/90) of BC and LD shoulders, respectively. Multivariable modeling demonstrated that surgical position was not associated with a risk of recurrence after 1 year (odds ratio [OR] for LD vs BC, 1.39; P = .56) and 5 years (OR for LD vs BC, 1.32; P = .43), although younger age at index surgery was associated with a higher risk of instability recurrence (OR, 1.73 per SD [4.1 years] decrease in age; P < .03). After 1 and 5 years, surgical position results were similar in a separate multivariable logistic regression model of revision surgery as the dependent variable, when adjusted for age, surgical position, bone loss group, and track. At 5 years, younger age was an independent risk factor for revision: OR 1.68 per SD (4.1 years) decrease in age (P < .05).
Conclusion:
Among fellowship-trained orthopaedic surgeons, there was no difference in rates of recurrence and revision surgery after performing arthroscopic anterior stabilization in either the BC or the LD position at 1- and 5-year follow-ups. In multivariable analysis, younger age, but not surgical position, was an independent risk factor for recurrence.
Glenohumeral instability presents a common issue among young and active individuals. Although various instability types exist, anterior instability remains the most common.18,30 Despite advancements in surgical technique and implants, recurrence presents a significant problem, with rates of 10% to 30% reported in the literature.11,13,17,23,27 Open stabilization procedures were traditionally considered the gold standard treatment for this condition, but in recent years arthroscopic stabilization has demonstrated equivocal results in select patient populations.9,11 The growing popularity and familiarity of arthroscopic techniques, along with advancements in surgical tools and implants, likely contribute to the results seen with arthroscopic stabilization. In addition, an improved understanding of the involved pathoanatomy has guided the surgeon's ability to appropriately address the injury.
A deeper understanding of the pathoanatomy seen in the setting of anterior glenohumeral instability is imperative for developing and executing an appropriate surgical plan. The most common injury seen after an anterior glenohumeral dislocation is a “Bankart lesion,” which has been shown to be present in 97% of first-time dislocators.1,19,26 This lesion involves detachment and associated laxity of the capsulolabral structures located on the glenoid labrum and scapular neck, most commonly at the anteroinferior aspect of the glenoid. Adequate tensioning and restoration of this native capsulolabral complex is necessary for a successful repair and optimal outcomes after surgery. Recent studies have additionally emphasized the importance of glenoid bone loss (GBL) and its relationship to glenohumeral stability and recurrence.2,3,7,15,21,22 Optimal stabilization should be focused on the ability to properly diagnose, access, and restore the involved pathoanatomy to appropriately restore glenohumeral stability.
Although the association of both patient-specific and surgical factors has been examined in relation to the recurrence of instability, the relationship between surgical positioning and recurrent instability has not been well studied. Arthroscopic glenohumeral stabilization can be performed in either the beach-chair (BC) or lateral decubitus (LD) position. Both positions have demonstrated good results with low complication rates. Surgeon preference, training, and familiarity play a significant role in determining the position used. Among other factors, BC allows for easy conversion to an open procedure if needed, while LD provides easier access to the inferior glenoid, as well as posterior and superior visualization and portal placement. In the only systematic review evaluating the contribution of BC versus LD positioning to recurrent instability after arthroscopic anterior stabilization, it was observed that LD provides lower rates of recurrence, although both provide good results. 8 In this systematic review and meta-analysis, bone loss was not accounted for in the recurrence rate. There is a paucity of data directly examining the BC versus LD position while controlling for surgeon training, follow-up time periods, associated bone loss.
The purpose of this study was to compare the rates of recurrent instability and revision surgery after anterior shoulder stabilization performed in the BC versus LD position by fellowship-trained sports medicine surgeons with similar short- and midterm follow-ups in an active duty military population. Additionally, the present study seeks to evaluate patient and surgical risk factors as well as GBL as independent predictors of the outcomes of interest, recurrence and revision.
Methods
Guidelines/Data Source
This retrospective observational study followed the Strengthening the Reporting of Observational Studies in Epidemiology guidelines for reporting observational studies. 28 The military electronic medical record contains comprehensive records of all health care encounters occurring within the military health care system for active-duty servicemembers, dependents, retirees, and those with medical disabilities. The follow-up time was defined by date of eligibility in the military health care system.
Study Design
After institutional review board approval, patient demographic and procedure characteristics were abstracted from a consecutive series of 641 arthroscopic Bankart stabilizations. All arthroscopic Bankart procedures performed by sports medicine–certified and fellowship-trained orthopaedic surgeons between January 2005 and January 2019 with the patient in either the BC or LD position were reviewed. All procedures performed in the BC and LD positions were performed by surgeons who only use the BC (7 surgeons, including B.O. and M.P.) and LD (4 surgeons, including L.L. and J.R.) positions for arthroscopic stabilization procedures. The choice of procedure (arthroscopic vs open stabilization) in the patients evaluated with isolated anterior instability was at the discretion of the treating surgeon, and only patients who underwent an isolated primary arthroscopic anterior capsulolabral repair were included in the study. Patients were excluded if concomitant posterior labral repair and/or remplissage procedures were performed at the time of surgery, or if an open stabilization procedure was performed. Shoulders were additionally excluded if magnetic resonance imaging (MRI) was not available at the time of preoperative evaluation or if the patient was lost to follow-up, with a minimum follow-up of 1 year. Of the remaining stabilizations, analysis included 383 patients who had ≥5 years of follow-up for recurrence and revision. Short- and midterm follow-ups were defined as ≥1 and 5 years, respectively.
Variables
All shoulders were evaluated for glenohumeral bone loss using the perfect circle technique on sagittal en face MRI as well as for bipolar lesions according to the on-/off-track method of Di Giacomo et al. 5 GBL was grouped into 3 categories: <5%, 5% to 13.5%, and >13.5%. A cutoff of >13.5% was chosen, as this amount of GBL has been termed as “subcritical bone loss” and has been associated with increased rates of recurrent instability and worse patient-reported outcomes.6,24 Other covariates evaluated as potential confounders were age (years) at the time of stabilization, surgical position (BC vs LD), and humeral head Hill-Sachs lesion type (on-track vs off-track).
Outcomes of Interest
The primary outcomes of interest were recurrent instability and revision stabilization through 1- and 5-year follow-up periods. Recurrent instability was defined as the presence of a recurrent subluxation and/or dislocation event and/or the presence of a positive apprehension. Multivariable logistic regression models were used to estimate the associations of age, surgical position, GBL group, and track as independent variables with recurrent instability and revision as dependent variables.
Statistical Methods
Rates of recurrence and revision were calculated among the full cohort among patients with available 1- or 5-year follow-up. Patient and procedure characteristics were compared by BC or LD group using 2-sample t tests or chi-square tests. Separate multivariable logistic regression models were used to estimate odds ratios (ORs) and 95% CIs to examine the associations between age, surgical position, GBL group, and track as independent variables with recurrent instability and revision as dependent variables. Models were repeated to evaluate both 1- and 5-year follow-up periods. All reported P values are 2-sided, with the significance level set at P < .05. Statistical analysis was performed using R (Version 3.6.1; The R Foundation for Statistical Computing).
Results
Patient Population
A total of 1571 shoulders underwent a stabilization procedure during the observed time period. After criteria were applied, the final cohort consisted of 641 shoulder stabilizations with a minimum follow-up of 1 year (Figure 1). The baseline characteristics of all participants are reported in Table 1. The mean age of the cohort was 22.28 years (SD, 4.5 years); 17% were women. The overall 1-year recurrent instability and revision rates for the BC and LD positions were 3.3% (21/641) and 2.8% (18/641), respectively. At 1 year, recurrent instability was observed in 2.3% (11/487) and 6.5% (10/154) of BC and LD shoulders, respectively. The 5-year recurrent instability and revision rates were 15.7% (60/383) and 12.8% (49/383), respectively. At 5 years, recurrent instability was observed in 16.4% (48/293) and 13.3% (12/90) of BC and LD shoulders.
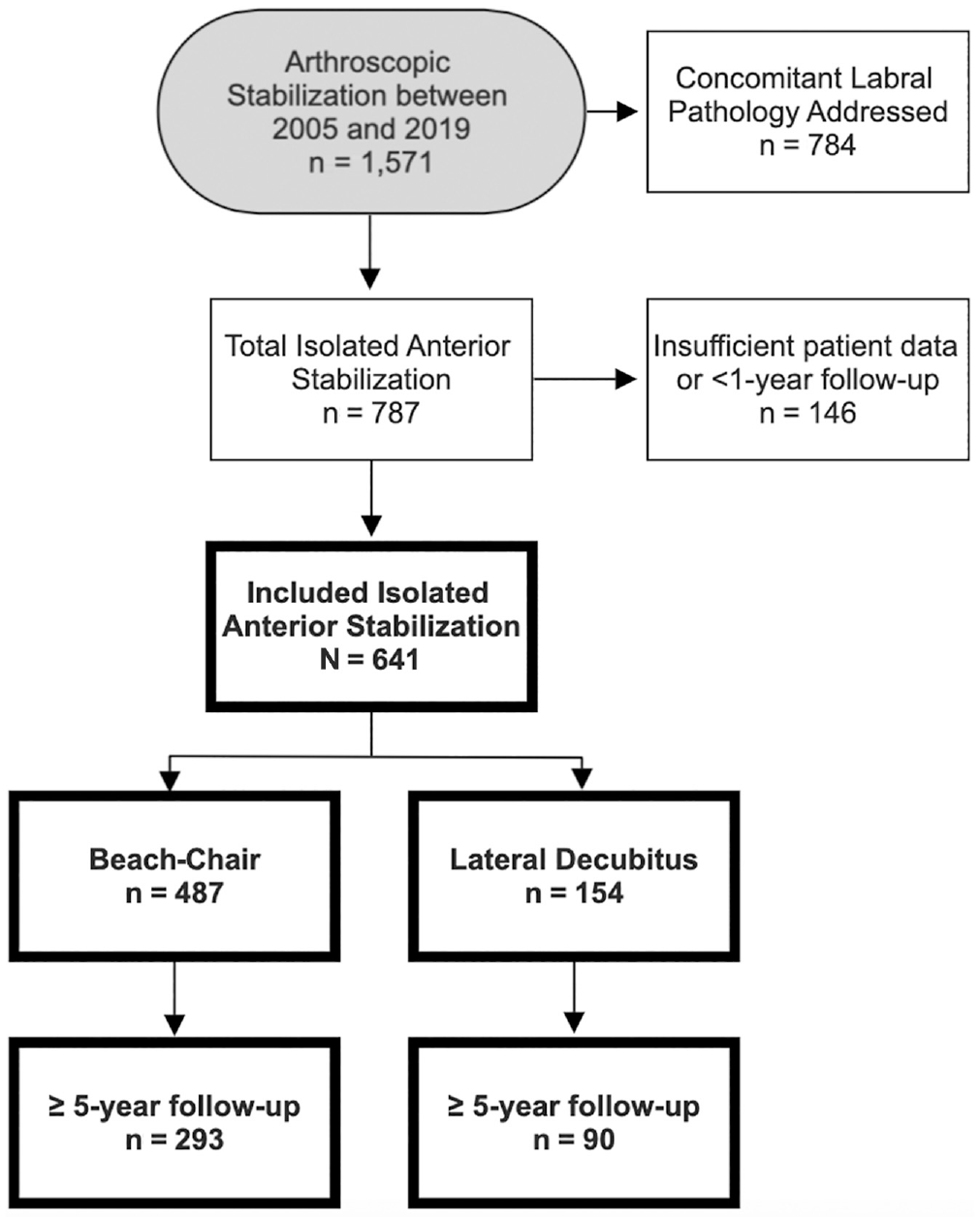
Flowchart demonstrating included patients (in bold).
Comparison of Characteristics of Patients With Anterior Shoulder Instability in Beach-Chair Versus Lateral Decubitus Positions a
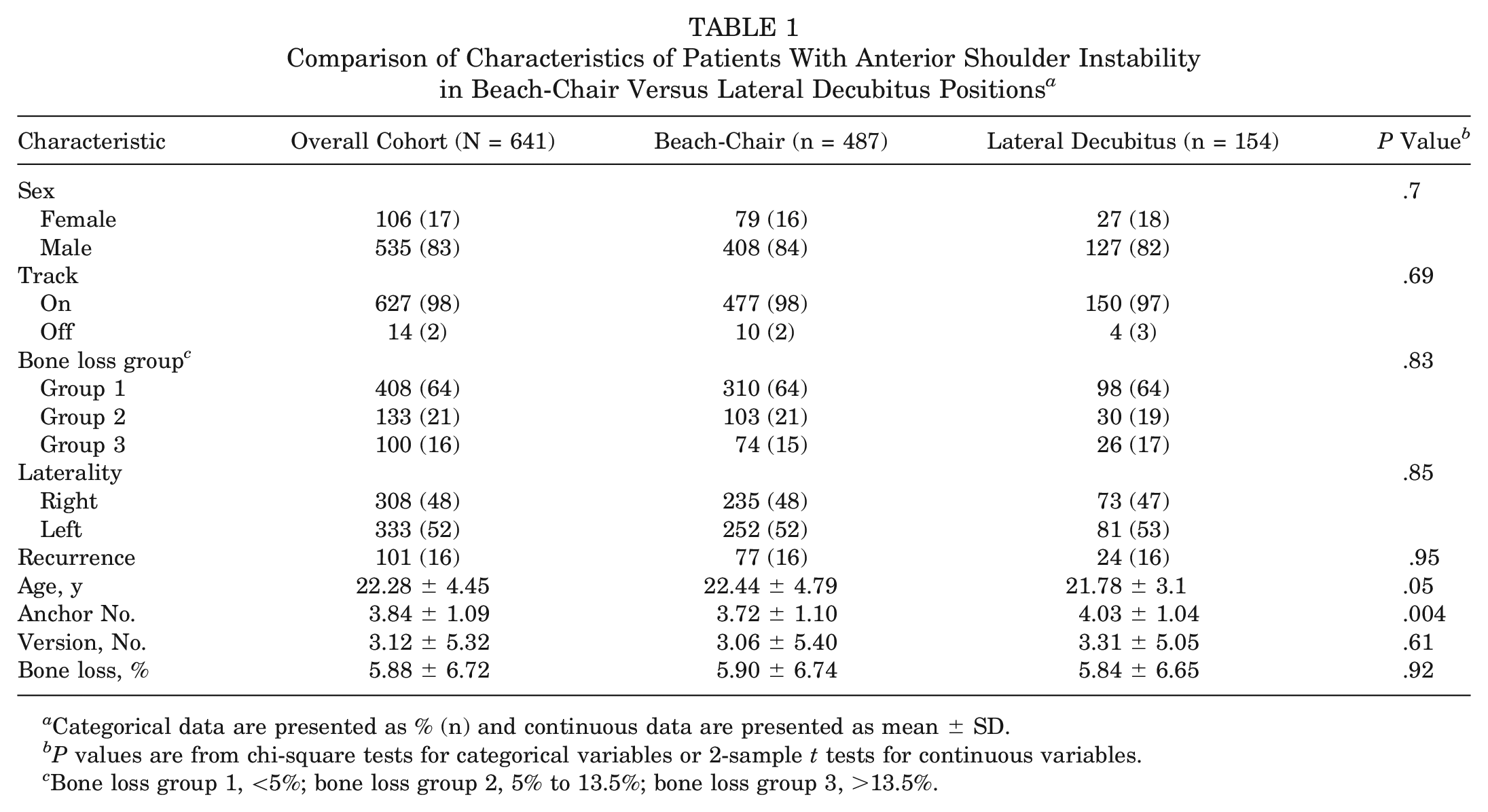
Categorical data are presented as % (n) and continuous data are presented as mean ± SD.
P values are from chi-square tests for categorical variables or 2-sample t tests for continuous variables.
Bone loss group 1, <5%; bone loss group 2, 5% to 13.5%; bone loss group 3, >13.5%.
Risk Factors for Recurrence
When adjusted for age, surgical position, bone loss group, and track, multivariable logistic regression modeling demonstrated that surgical position was not associated with a risk of recurrent instability after 1-year (OR for LD vs BC, 1.39; P = .56) and 5-year (OR for LD vs BC, 1.32; P = .43) follow-up time periods. However, after the 5-year follow-up, younger age at index surgery was independently associated with a higher risk of recurrent instability: OR of 1.73 per SD (4.1 years) decrease in age (P < .03; 95% CI, 1.39-15.49) (Tables 2 and 3).
1-Year Multivariable Models for Instability Recurrence and Revision a
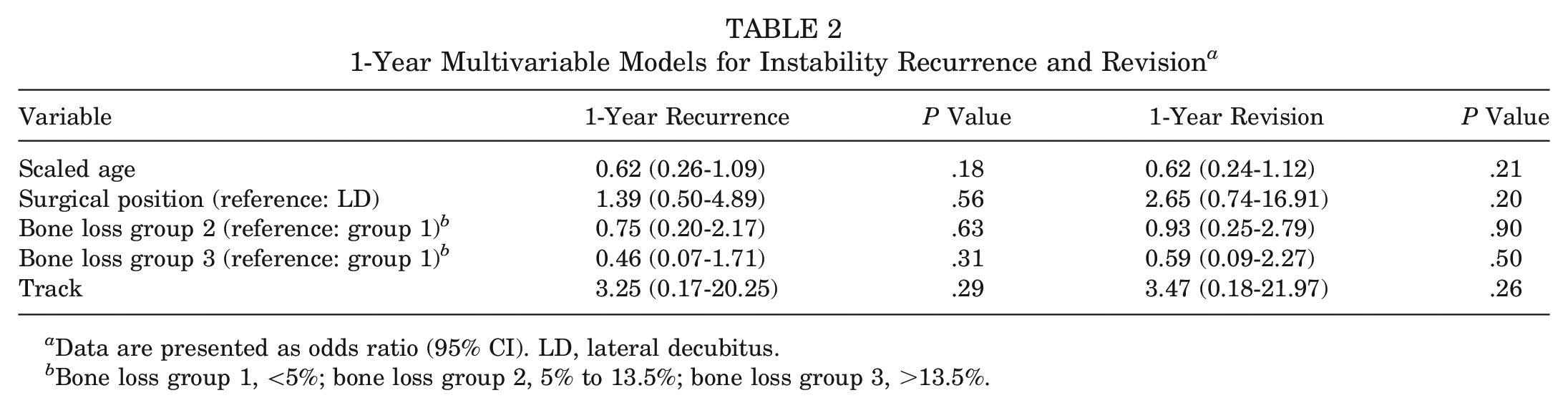
Data are presented as odds ratio (95% CI). LD, lateral decubitus.
Bone loss group 1, <5%; bone loss group 2, 5% to 13.5%; bone loss group 3, >13.5%.
5-Year Multivariable Models for Instability Recurrence and Revision a
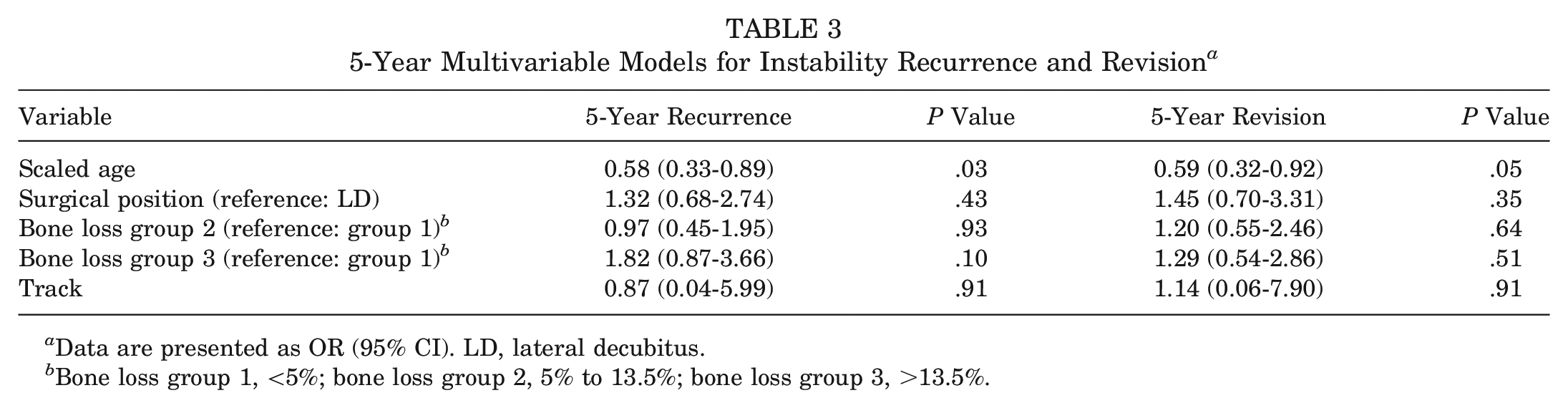
Data are presented as OR (95% CI). LD, lateral decubitus.
Bone loss group 1, <5%; bone loss group 2, 5% to 13.5%; bone loss group 3, >13.5%.
Risk Factors for Revision
After 1- and 5-year follow-up time periods, surgical position results were similar in a separate multivariable logistic regression model of revision surgery as the dependent variable, when adjusted for age, surgical position, bone loss group, and track. After the 5-year follow-up, only younger age at the time of index surgery remained an independent risk factor for revision: OR of 1.68 per SD (4.1 years) decrease in age (P < .05; 95% CI, 1.38-2.52) (Tables 2 and 3).
Discussion
Both BC and LD positions have demonstrated good short- and midterm results when used during anterior arthroscopic stabilization surgery. The purpose of the present study was to evaluate the rates of recurrent instability as well as revision surgery after index anterior stabilization performed in the BC versus LD position by fellowship-trained orthopaedic surgeons. The principal finding of this study was that there was no statistically significant difference in rates of recurrent instability and revision surgery noted in the BC versus LD position in patients undergoing arthroscopic anterior shoulder stabilization at short- and midterm follow-ups. GBL is a well-established risk factor for recurrent instability treated both operatively and nonoperatively, with subcritical bone loss being significantly associated with higher failure rates after surgical stabilization.6,24 In conducting this study, we sought to determine if surgical positioning affected patient outcomes, while also stratifying patients by the amount of measured GBL. Additionally, we sought to control for surgeon training experience as well as have standardized follow-up periods among the 2 groups. A secondary finding in this study was the rates of recurrent instability and revision surgery, 15.7% and 12.8% for BC and LD positioning, respectively, after arthroscopic anterior stabilization at the midterm follow-up.
The literature is significantly limited on comparing outcomes of arthroscopic anterior stabilization based on surgical position. In the only systematic review 8 assessing rates of recurrent instability after isolated anterior arthroscopic stabilization, 64 articles were reviewed (38 articles for BC, 26 articles for LD) to compare rates of recurrence among shoulders that had undergone arthroscopic anterior stabilization in each surgical position with ≥2 years of follow-up. It was suggested that LD positioning may be associated with lower rates of recurrence, with no difference in patient-reported and functional outcomes when compared with those for the BC position. The analysis concluded that 14.7% of patients whose procedures performed in the BC position (mean age, 26.7 years) and 8.5% of those performed in the LD position (mean age, 26 years) went on to experience recurrent instability, with an overall recurrence rate of 12%. Even though the aforementioned study provides important insight into the outcomes of procedures performed in either of the 2 surgical positions, none of the studies within the systematic review were designed to directly evaluate outcomes of stabilizations performed in the BC versus LD position. Inherent to the systematic review design, controlling for variables such as bone loss and surgeon training could not be performed. The slightly longer follow-up in the BC group (mean, 49.9 months) than in the LD group (mean, 38.7 months) may contribute to the greater recurrence in the BC cohort. Additionally, with 64 studies analyzed, the variability among studies creates potential for significant bias. The heterogeneity of the patient population with regard to age and activity level, as well as varying definitions of recurrence among the studies, makes a direct comparison more difficult. Also, none of the included studies factor in the role of GBL, an established risk factor for recurrent instability. Last, this systematic review includes studies ranging a 23-year span (1990-2013), which may make results difficult to interpret given the advances in surgical technique that have been made in recent years and the positive effect they have had on outcomes.
The current investigation evaluated 641 shoulders that underwent an index arthroscopic stabilization for isolated anterior shoulder instability. In contrast to the previously mentioned systematic review comparing BC and LD positioning, the present study includes procedures performed only by fellowship-trained surgeons and with the same follow-up periods among the 2 groups. Additionally, all procedures in the current study occurred within the same time period, from 2005 to 2019. This allowed for all procedures to be performed in both groups within the same generation of available implants, tools, surgical techniques, and other technological advances, which allowed for a more direct comparison between the BC and LD groups.
The present study found recurrence rates of 2.3% (11/487) and 6.5% (10/154) in those who received procedures in the BC and LD positions, respectively, at the 1-year follow-up, with overall recurrence and revision rates of 3.3% (21/641) and 2.8% (18/641), respectively. At the 5-year follow-up, recurrence rates of 16.4% (48/293) and 13.3% (12/90) were seen in those who received procedures in the BC and LD positions, respectively, with overall recurrence and revision rates of 15.7% (60/383) and 12.8% (49/383), respectively. Several studies have demonstrated rates of recurrent instability after primary arthroscopic repair ranging from 4% to 35%.12,17,27 Additionally, risk factors for recurrent instability have been described in the literature to include male sex, younger patient age, and high activity level.4,16,29,31 The current study demonstrated rates of recurrent instability consistent with, but on the lower end of, those previously reported in the literature, regardless of the surgical position used. Furthermore, the patients in the current study exhibited characteristics that placed them at particularly high risk for recurrent instability, with a mean age of 22.3 years and active-duty military status.
The amount of measured GBL among the entire cohort was 5.88% (5.90% in the BC position vs 5.84% in the LD position). There was no statistically significant difference in recurrence and revision rates among GBL groups, which was demonstrated at both 1- and 5-year follow-up periods. Overall, age was an independent risk factor for recurrence at the 5-year follow-up, with younger age at time of index surgery being independently associated with a higher risk of recurrence (OR, 1.73 per SD [4.1 years] decrease in age; P < .03; 95% CI, 1.39-15.49), which is consistent with previous literature.4,29 Additionally, younger age remained an independent risk factor for revision surgery at the 5-year follow-up (OR, 1.68 per SD [4.1 years] decrease in age; P < .05; 95% CI, 1.38-2.52). Multivariable logistic regression results revealed no association between surgical position and recurrent instability, which was demonstrated at both 1-year (P = .56) and 5-year (P = .43) follow-ups.
The present study demonstrates low rates of recurrent instability after arthroscopic stabilization of a young and active military population at midterm follow-up. With an overall recurrence rate of 15.7% at the 5-year follow-up, these results are similar to rates previously reported in the literature.12,17,27 The authors believe that may be attributable to multiple factors. The study included only sports medicine fellowship–trained orthopaedic surgeons, who may have more experience dealing with these types of injuries than their non–fellowship-trained counterparts. Also, active-duty military personnel experience significantly higher rates of anterior shoulder instability than other populations. As such, shoulder instability comprises a significant portion of a military sports medicine surgeon's practice, which may provide the surgeon with more experience and refinement of surgical technique that could lead to improved outcomes.
Additionally, the current study demonstrated similar rates of recurrent instability (15.7%) and revision surgery (12.8%). Given the unique high demands that are placed on this population of young active-duty military personnel, the authors believe that similar recurrence and revision rates that were observed may be attributable to a lower threshold to revise a previously failed repair, as those with continued symptoms of recurrent instability (copers) may otherwise not be able to return to duty with nonoperative treatment.
BC and LD positions provide the surgeon the ability to perform arthroscopic anterior stabilization. However, both positions present unique advantages and disadvantages. Advocates for the BC position cite ease of setup, lower risk of neurapraxia injuries, and easy conversion to an open approach, if needed, as advantages. An upright vantage point and visualization of a more anatomic orientation of the involved structures that may assist in certain procedures as well as in instructing trainees may also provide benefit.14,20,25 Supporters of the LD position state easier orientation with the glenoid fossa parallel to the floor, ease of portal placement, and access to posterior structures as advantages of the LD position. Additionally, the arm position and weighted traction in the LD position provide an increased working space within the glenohumeral joint.10,20 Although the positions differ, they both allow the surgeon the ability to perform adequate stabilization. The current study does not advocate for one surgical position over another. Rather, it demonstrates that equivalent and reproducible results can be achieved when performing arthroscopic anterior shoulder stabilization in either the BC or the LD position among fellowship-trained surgeons. A surgeon's preference and outcomes with a particular surgical position may be a result of the surgeon's familiarity with a particular position, training background, and case volume, all of which may contribute to a successful stabilization procedure, regardless of the surgical position.
This study is not without limitations. There were far more patients in the BC position group than in the LD position group (487 vs 154, respectively). Statistically significant conclusions were able to be drawn, but the results may be weakened by the dissimilar number of patients in each group. Additionally, even though the study does take into account surgical position, age, and instability type, it does not account for many other factors that contribute to outcomes after surgical stabilization. Anchor number, anchor type, and number of preoperative instability events may all play a role in recurrence rates but were not included in this study. Although data regarding anchor number were available in some cases, they were not available in an adequate number of instances to make significant conclusions possible. Additionally, the importance of GBL is increasingly recognized as a significant concern when treating patients with glenohumeral instability and may play a considerable role in the type of surgical technique (arthroscopic vs open) that is used for adequate stabilization. In the present study, the surgical stabilization performed (arthroscopic vs open) was at the discretion of the treating surgeon, presenting an inherent limitation because of the variability among surgeons when incorporating GBL into the surgical decision-making. The present study included only patients who were indicated by the treating surgeon for an isolated anterior arthroscopic stabilization and excluded those who the surgeon deemed appropriate for either an open or bony procedure. The outcomes of interest in this study were both recurrent instability and revision surgery. Clinical parameters such as range of motion, patient-reported outcome measures, and postoperative activity level were not assessed.
Conclusion
Among fellowship-trained orthopaedic surgeons, there was no difference in rates of recurrent instability and revision surgery after performing arthroscopic stabilization for isolated anterior shoulder instability in either the BC or the LD position at short- and midterm follow-ups. In multivariable analysis, younger age, but not surgical position, was an independent risk factor for recurrence.
Footnotes
Submitted May 3, 2023; accepted July 31, 2023.
One or more of the authors has declared the following potential conflict of interest or source of funding: B.G.Y. has received support for education from Southtech and Supreme Orthopedic Systems. A.B.A. has received support for education from Supreme Orthopedic Systems. D.J.T. has received support for education from Gemini Mountain Medical and Arthrex. L.E.L. has received support for education from Alpha Orthopedic Systems, Arthrex, and Supreme Orthopedic Systems and a grant from DJO. J.P.R. has received support for education from Supreme Orthopedic Systems and Stryker. B.D.O. has received consulting fees from Linvatec, DePuy Synthes, Vericel, Musculoskeletal Transplant Foundation, and Medical Device Business Services; royalties from Linvatec; and honoraria from Vericel; he is an associate editor for AJSM. M.D. has received support for education from Arthrex, SeaPearl, and Supreme Orthopedic Systems. J.F.D. has received support for education from Supreme Orthopedic Systems and compensation for services other than consulting from Arthrex. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Presented at the annual meeting of the AOSSM, Nashville, Tennessee, July 2021.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.