
Abstract
Background:
Various muscle contraction modalities have differing effects on the musculoskeletal system. To understand the magnitude of these effects, the authors investigated the effects of eccentric and concentric contractions on the bone-tendon interface after rotator cuff repair in mice.
Hypothesis:
Eccentric contraction promotes healing of the bone-tendon interface after rotator cuff repair in mice better than other muscle contraction patterns.
Study Design:
Controlled laboratory study.
Methods:
The authors performed acute supraspinatus tendon repair of the right shoulder in 104 C57BL/6 mice. Animals were randomized into 4 groups postoperatively: control group (Con group), horizontal running group (Horz group), +15° uphill running group (Up group), and −15° downhill running group (Down group), with 26 animals in each group. At 4 and 8 weeks postoperatively, the authors removed the eyeball, collected blood samples, and extracted the supraspinatus tendon–humerus complex for histological, immunological, bone morphological, and biomechanical tests.
Results:
At 4 and 8 weeks postoperatively, the Down group exhibited a better collagen cell arrangement and fibrocartilage layer than the other 3 groups. At 4 weeks postoperatively, anti-inflammatory macrophages (M2 macrophages) were observed at the repair site in all groups except for the Con group. At 8 weeks postoperatively, M2 macrophages were withdrawn from the tendon site in all groups. The transforming growth factor β1 concentration in the Down group was greater than that in the other 3 groups at 4 weeks postoperatively, and it was higher than that in the Con group at 8 weeks postoperatively. The bone volume fraction, number of trabeculae, and thickness of trabeculae at the repair site in the Down group, as well as the ultimate strength and failure load in the biomechanical tests, were greater than those in the other 3 groups at 8 weeks postoperatively.
Conclusion:
Eccentric contraction promotes healing of the bone-tendon interface after rotator cuff repair in mice better than other muscle contraction patterns.
Clinical Relevance:
After clinical rotator cuff repair, patients can be rehabilitated by eccentric training to speed up the functional recovery of the shoulder joint.
Rotator cuff injury is a common injury of the musculoskeletal system that is seen in the clinical setting and that primarily manifests as shoulder pain and dysfunction. Among rotator cuff injuries, supraspinatus tendon (SST) injuries are the most common, with the injury site often located 1 cm away from the end of the greater tuberosity of the humerus. 36 Because of inadequate blood supply to this region, the injured tendon is prone to atrophy, degeneration, and fatty infiltration, 32 which predisposes up to 95% of cases to poor bone-tendon interface (BTI) healing after rotator cuff repair.12,20
Exercise is the primary treatment for tendon disorders. Moderate mechanical stimulation not only maintains skeletal tissue homeostasis but also helps repair muscle, ligament, and tendon injuries.13,39 In addition, different forms of exercise can induce various biological adaptations. For example, concentric contraction–based uphill running and eccentric contraction–based downhill running have different biomechanical, neuromuscular, and physiological responses because of their unique muscle contraction characteristics, 8 which can have varying effects on the healing of an injury. Currently, eccentric training can be safely and effectively applied in chronic heart diseases, 10 tendon disease, 37 and following cruciate ligament repair.15,30 However, there is still controversy regarding how muscle contractions affect the healing of shoulder joint and upper limb injuries.
Kim et al 23 found that eccentric shoulder abduction training was superior to concentric training in maintaining fiber bundle length and promoting tendon healing. Garma et al 14 found no significant differences in the effects of concentric or eccentric training with the same mechanical stimulus on healing after a musculoskeletal injury. To date, the effect of different muscle contraction patterns on BTI healing after rotator cuff injury repair remains unclear.
The aim of this study was to investigate the effect of different muscle contraction patterns on tendon-bone healing after rotator cuff repair and to determine which muscle contraction modality promotes healing. We hypothesized that, after rotator cuff injury repair in mice, eccentric contractions would promote BTI healing better than concentric contractions. Histological, immunological, biomechanical, and bone morphological tests were performed to evaluate the quality of BTI healing.
Methods
Study Design
The study protocol was approved by the local laboratory animal committee (No. 2019020). A total of 104 male C57BL/6 mice (age, 8 weeks; weight, 20 ± 22 g) underwent acute SST repair of the right shoulder. The animals were randomized into 4 groups postoperatively: control group (Con group), horizontal running group (Horz group), +15° uphill running group (Up group), and −15° downhill running group (Down group), with 26 animals in each group. At 4 and 8 weeks postoperatively, the eyeball was removed so that blood could be collected for testing, and the SST–humerus (SSTH) complex was examined. Six samples were collected from each group at 4 weeks postoperatively for histological and immunological testing, and 6 bone morphological samples and 8 biomechanical samples were added to each group at 8 weeks postoperatively (Figure 1). Five animals were in each cage.
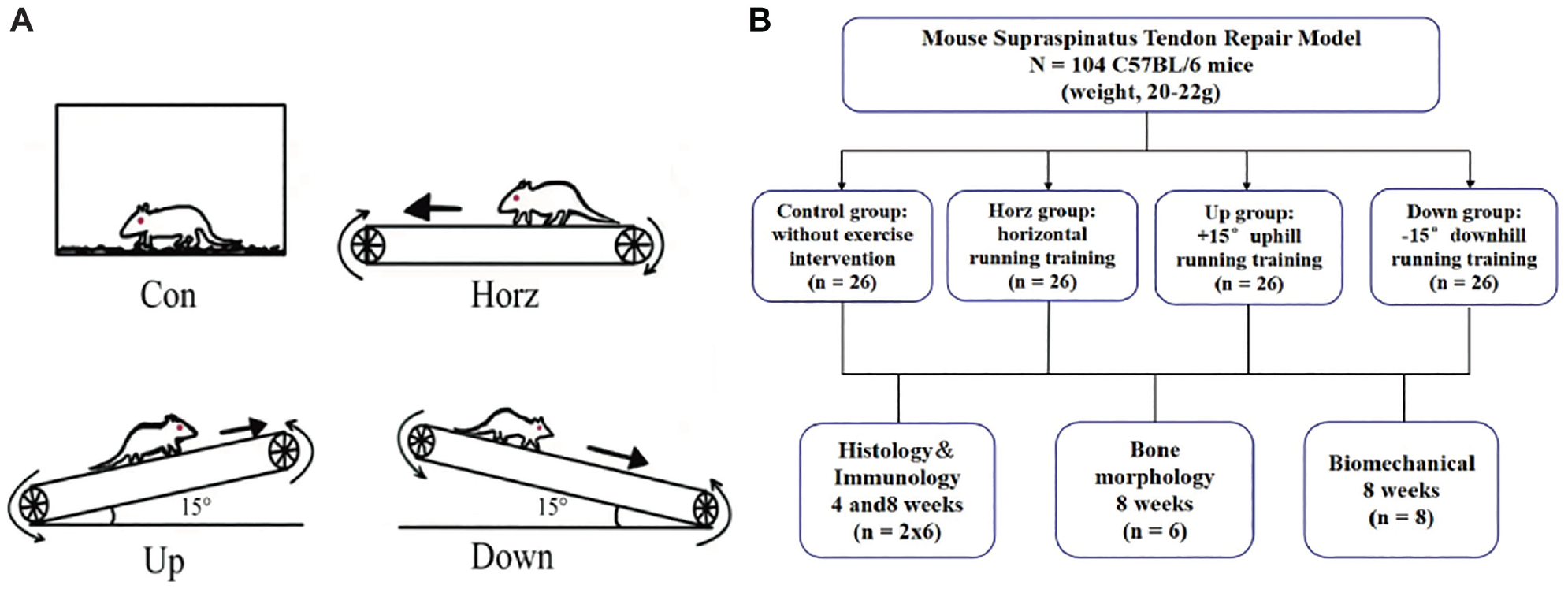
(A) Experimental groups. (B) Flowchart depicting the study design. Con, control group; Down, –15° downhill running group; Horz, horizontal running group; Up, +15° uphill running group.
Surgical Procedure
Modeling was performed using the injury model protocol established by Bell et al. 2 Mice were anesthetized intraperitoneally (0.3% sodium pentobarbital; 0.6 mL/20 g) and placed in the left lateral recumbent position. After aseptic preparation, an anterolateral incision was made on the right shoulder to expose the deltoid muscles. Using dissecting scissors, we peeled the deltoid muscle and the surrounding tissue along the distal posterior edge of the vessel. After exposure of the SST by pulling the acromion, the humerus was adducted and rotated outward to observe the coracoacromial arch. A 15-gauge blade was used to separate the SST from the humeral head after braiding with a 6-0 PDS suture (Ethicon). The blade was used to remove the cartilage layer from the foot impression to expose the spongy bone. Saline and gauze were used to clean the surgical sites. A 1-mm tunnel was drilled transversely from posterior to anterior at the insertion site of the SST. The tendon was fixed and the PDS suture was tightened and knotted, after which the deltoid muscle was reset. The skin was then closed using 5-0 nonabsorbable sutures. All mice were allowed to move freely in the cage postoperatively.
All animals received buprenorphine (0.05 mg/kg; intramuscular injection, once a day; TIPR Pharmaceutical Co) for 3 consecutive days after surgery.
Experimental Grouping and Training Programs
Before surgery, all mice underwent a 5-day acclimatization period and were trained on a treadmill set at 0° incline and a speed of 10 m/min for 30 minutes each day. 39 After the surgery, the animals were randomly divided into 4 groups (n = 26) and began group-specific exercise training on the seventh postoperative day. The Con group received regular feeding without any exercise intervention. The Horz group underwent horizontal treadmill training with an angle of 0°. The Up group underwent uphill running training with an incline of +15°.6,38 Finally, the Down group underwent downhill running training with an incline of −15°. The treadmill speed was 10 m/min, the duration of each session was 20 minutes per day, and the frequency was 5 days per week for 5 consecutive days with 2 days of rest.5,31 During treadmill running, a low-intensity electrical stimulation of 0.8 Hz was used to encourage running.
Histology Testing
Immediately after obtaining SSTH specimens, we fixed them in 10% neutral formalin buffer for 24 hours. After fixation, specimens were decalcified and dehydrated for transparent embedding. The specimens were serially sectioned in the coronal plane with a thickness of 5 µm using a microtome. Sections were routinely dewaxed and stained with hematoxylin-eosin and safranin O/fast green. Immunohistochemical analyses were performed according to the manufacturer's instructions. After pretreatment with 3% H2O2 to block endogenous peroxides, sections were incubated overnight at 4°C with primary antibody (1:200; CD163ab182422; Abcam). After incubation, sections were removed, equilibrated for 30 minutes at room temperature, washed 3 times with phosphate-buffered saline, developed with 3,3′-diaminobenzidine and 3-amino-9-ethylcarbazole, and washed 3 times with phosphate-buffered saline, and the nuclei were restained with hematoxylin.
The histological images were semiquantitatively scored by 2 blinded observers (L.D. and Y.P.) using a modified tendon-bone maturing score adapted from a previous study, which includes cellularity, continuity, vascularity, fibrocartilage cells, and tidemark, on a scale of 1 to 4 (total 20 points), with higher scores indicating better BTI healing. 18 Anti-inflammatory macrophages (M2 macrophages) were examined according to CD163 expression. The cell numbers of M2 macrophages were calculated using ImageJ software (National Institutes of Health) at ×400 magnification: five 1000-μm2 squares were randomly selected in each section of the animal to calculate the mean number of positive cells.
Immunology Testing
Blood was collected at 4 and 8 weeks postoperatively, and serum was isolated. Serum levels of transforming growth factor β1 (TGF-β1) were measured by enzyme-linked immunosorbent assay. The assay was performed according to the manufacturer's instructions. After completion, the absorbance (optical density) was measured at 450 nm using a microplate reader (Thermo Fisher Scientific). Two replicate wells were set up for each specimen, and the results were repeated 3 times and averaged.
Bone Morphology Testing
The BTI specimens were fixed in 4% neutral buffered formalin for 24 hours at 8 weeks postoperatively, dehydrated in gradient alcohol, and scanned in a micro–computed tomography (CT) scanner (Scanco Medical). 5 The scan parameters were as follows: resolution of 11.4 μm, energy of 55 KVp, exposure duration of 0.4 seconds, rotation step of 0.36°, and rotation of 180°. On the axial image, the subchondral bone near the attachment of the internal tendon of the humeral head and the proximal end of the growth plate were the regions of interest. The region of interest was automatically acquired by 2 blinded observers (G.W. and C.Z.) using SkyScan CTAn software, and the bone volume/total volume fraction (BV/TV), trabecular bone number (Tb.N), trabecular bone thickness (Tb.Th), and trabecular bone space (Tb.Sp) were calculated.
Biomechanical Testing
A biomechanical testing system (MTS Insight; MTS Systems) was used to measure the ultimate strength (US) and failure load (FL) for assessing the mechanical properties of healing and regenerating tissues after BTI injury. Eight weeks postoperatively, the BTI specimens were trimmed and kept moist with 0.9% saline. The SST was fixed with sandpaper, the humerus was gripped with a clamp, and the specimen was placed in a biomechanical materials testing machine for uniaxial tensile testing at an abduction angle of 60°. Before testing, the SSTH was stretched with a force of 0.1 N for 1 minute, and the cross-sectional area (CSA) of the healing site was measured. The SSTH was pulled at a speed of 0.03 mm/s.5,47
Statistical Analysis
SPSS Version 25.0 software (IBM Corp) was used to analyze the experimental data. The experimental data were expressed as mean ± SD. The 4 groups were compared using 1-way analysis of variance with Bonferroni post hoc testing. P values <.05 were considered statistically significant, and P values <.01 were considered highly significant.
Based on the previous power analysis to determine the study sample size necessary to provide 80% statistical power at the .05% alpha level, 21 mice per group were required to detect the final expected difference. Therefore, a total of 104 mice (26 per group) were included in the study.
Results
Histology Analysis
At 4 weeks postoperatively, the Down group showed fibrocartilage tissue without tidal markings at the BTI, and the continuity and tropism of the collagen fibers were greater than those in the other 3 groups. The Con group exhibited a more disorganized collagen fiber arrangement (Figure 2A). At 8 weeks postoperatively, all groups showed better collagen fiber alignment order and area than those observed at 4 weeks. The Down group exhibited the formation of tidal lines in the fibrocartilage layer at the reconstructed site, and the proliferation of pale-blue hyaline cartilage and chondrocytes was more pronounced (Figure 2B). Thus, the Down group was superior to the other 3 groups in terms of collagen fiber alignment and fibrocartilage layer (Figure 2). The BTI maturing score of the samples in the Down group was highest, while that in the Con group was the lowest at 4 and 8 weeks postoperatively. The scores in the exercise groups were higher than those in the Con group (Figure 2C).
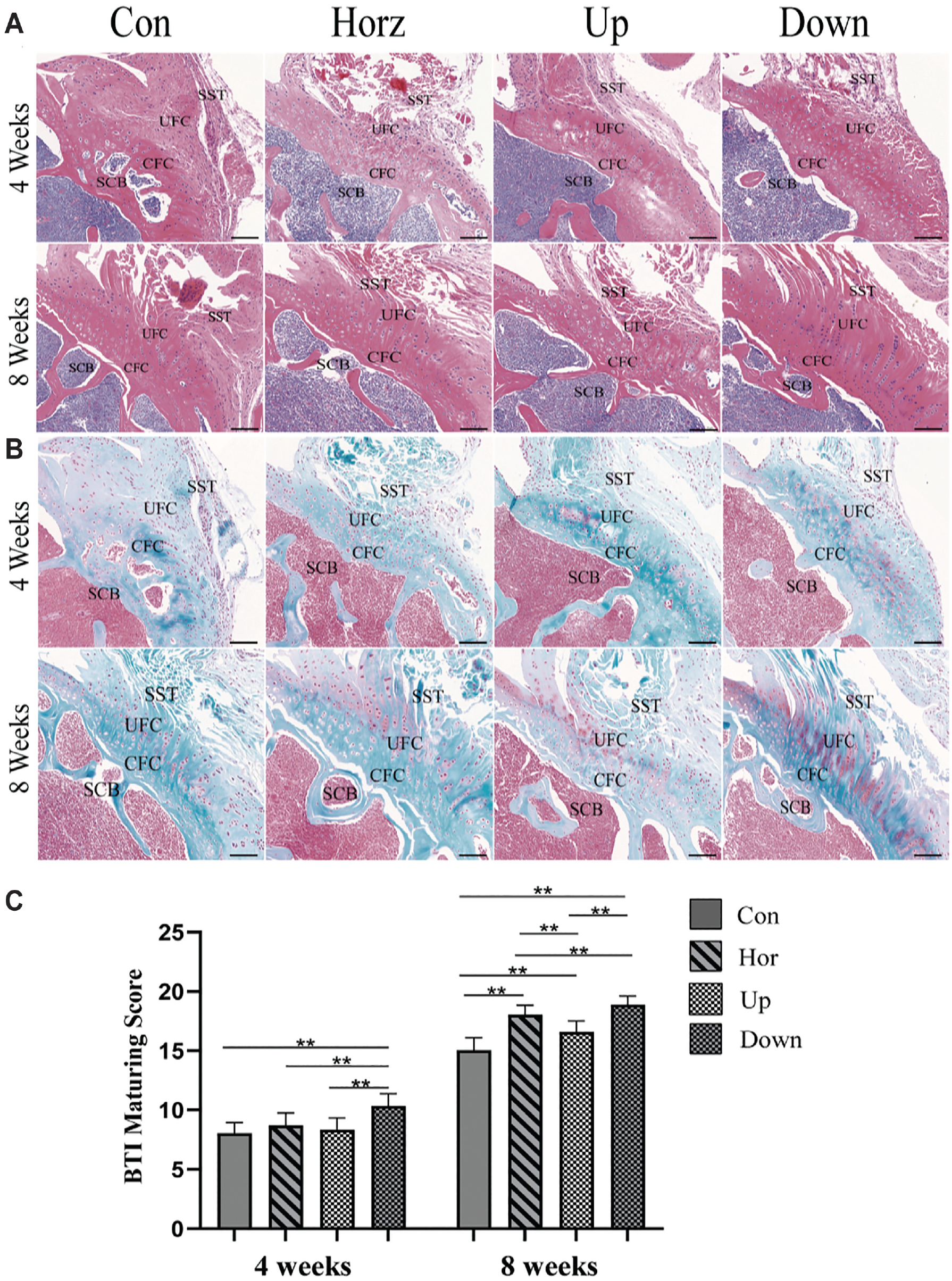
(A) Representative hematoxylin-eosin staining images at 4 and 8 weeks after surgery. (B) Representative safranin O/fast green staining images at 4 and 8 weeks after surgery. (C) Bone-tendon interface (BTI) maturing score of supraspinatus tendon (SST) insertion in each group at weeks 4 and 8 postoperatively. Scale bar = 50 μm. **P < .01. CFC, calcified fibrocartilage; Con, control group; Down, –15° downhill running group; Hor, horizontal running group; SCB, subchondral bone; UFC, uncalcified fibrocartilage; Up, +15° uphill running group.
To assess the proliferation of M2 macrophages during tendon osseointegration healing, we performed immunostaining for CD163 cells at 4 and 8 weeks postoperatively. These are distributed at the site of injury early in the healing process and subsequently attach to the surface of fibrocartilage tissue. At 4 weeks after surgery, M2 macrophages were observed at the repair insertion site in all groups except for the Con group, and the expression of CD163 was higher in the Down group than in the other 3 groups. However, at 8 weeks postoperatively, M2 macrophage expression was observed in all groups, including the Con group, and all were withdrawn from the tendon site. There were no differences between the groups (Figure 3). Statistical analysis showed that the density of CD163+ cells at 4 and 8 weeks in the exercise groups was higher than that in the Con group; among them, the density in the Down group was higher than that in the other exercise groups (Figure 3).
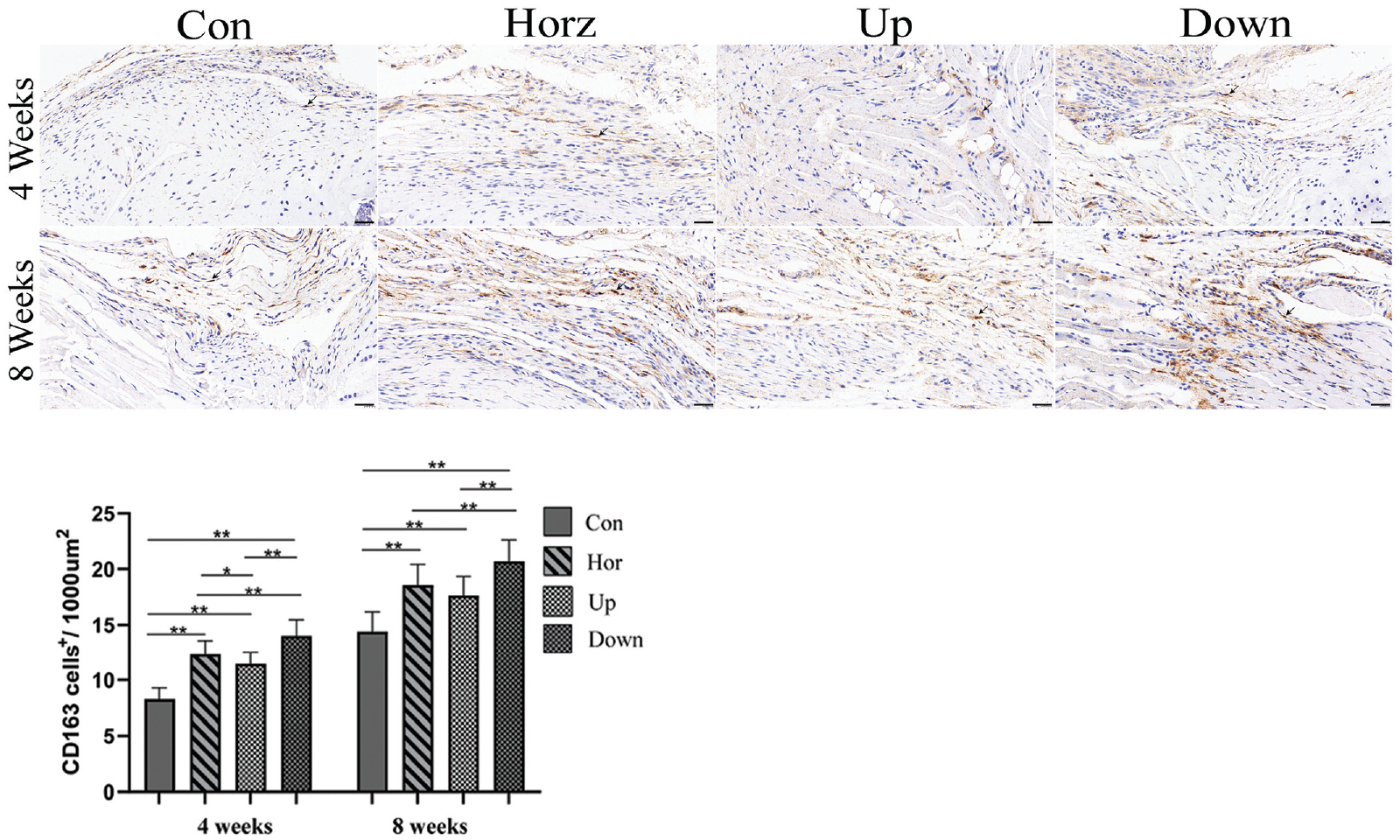
Statistical analysis showed that the density of CD163+ cells at 4 and 8 weeks in the exercise groups was higher than that in the Con group. Scale bar = 20 μm. *P < .05; **P < .01. Con, control group; Down, –15° downhill running group; Horz, horizontal running group; Up, +15° uphill running group.
Immunology Analysis
At 4 weeks postoperatively, the TGF-β1 concentration in the Con group (0.59 ± 0.12 ng/mL) was significantly lower than that in the Down group (1.19 ± 0.21 ng/mL) (P < .01), Horz group (0.90 ± 0.20 ng/mL) (P < .05), and Up group (0.88 ± 0.16 ng/mL) (P < .05). The concentration of TGF-β1 in the Down group was significantly higher than that in the Horz and Up groups (P < .05). There was no significant difference between the Horz and Up groups (P > .05).
At 8 weeks after surgery, TGF-β1 concentrations decreased in all groups compared with those at 4 weeks. The concentration of TGF-β1 in the Down group (0.73 ± 0.18 ng/mL) was significantly higher than that in the Con group (0.46 ± 0.12 ng/mL) (P < .05). There was no statistically significant difference between the Horz (0.65 ± 0.15 ng/mL) and Up (0.57 ± 0.13 ng/mL) groups and between the Down and Con groups (P > .05) (Figure 4).
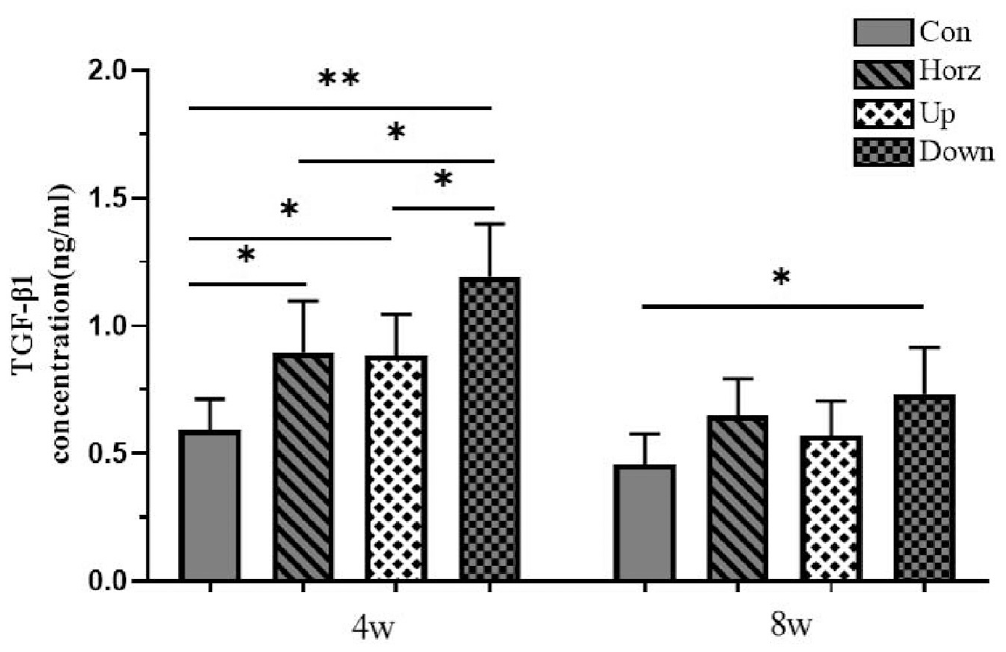
Enzyme-linked immunosorbent assay of transforming growth factor β1 factor concentration. Data are expressed as mean ± SD. *P < .05; **P < .01. Con, control group; Down, –15° downhill running group; Horz, horizontal running group; Up, +15° uphill running group.
Bone Morphology Analysis
At 8 weeks postoperatively, micro-CT scans showed recovery of the tendon-bone union injury in all groups, but the Down group recovered more quickly from bone cortex damage and humeral tuberosity tears (Figure 5A).
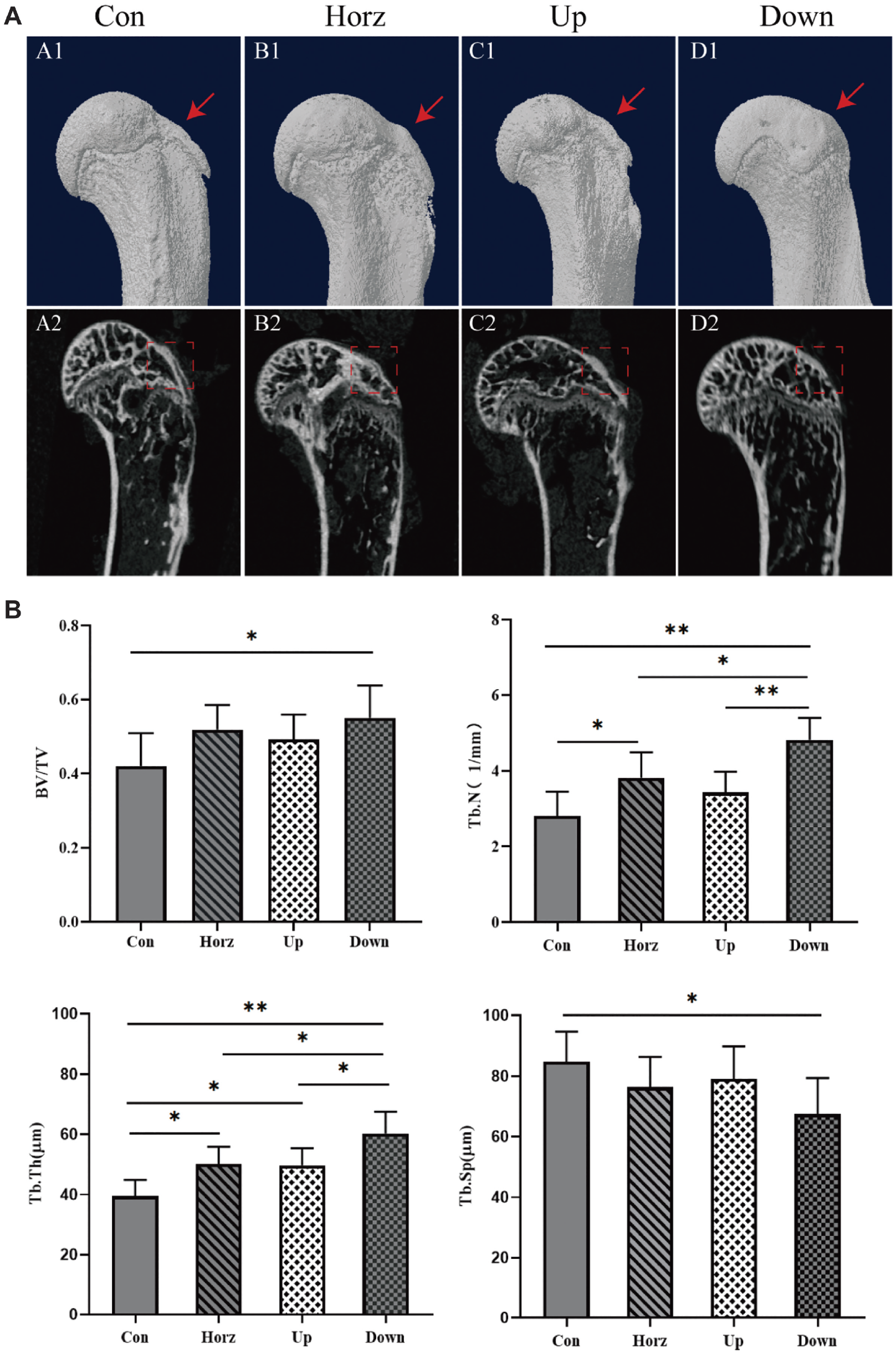
(A) Micro–computed tomography reconstruction of the supraspinatus tendon–humerus complex at 8 weeks postoperatively. Images A1 to D1 are 3-dimensional reconstructions, and images A2 to D2 are their sagittal sections. Regions of interest (ROIs) are indicated by dashed boxes. (B) Quantitative analysis of ROIs. Data are expressed as mean ± SD. *P < .05; **P < .01. BV/TV, bone volume/total volume fraction; Con, control group; Down, –15° downhill running group; Horz, horizontal running group; Tb.N, trabecular number; Tb.Sp, trabecular bone spacegap; Tb.Th, trabecular thickness; Up, +15° uphill running group.
The morphological results of subchondral bone in SSTH specimens showed significantly higher BV/TV (%) in the Down group (0.55 ± 0.09) than in the Con group (0.42 ± 0.09) (P < .05). There was no statistically significant difference between the Horz group (0.52 ± 0.07) and the Up group (0.49 ± 0.07) (P > .05). Tb.N in the Down group (4.82 ± 0.58 mm−1) was significantly higher than that in the Con group (2.81 ± 0.65 mm−1), Up group (3.43 ± 0.55 mm−1) (P < .01), and Horz group (3.82 ± 0.67 mm−1) (P < .05). Tb.N in the Horz group was significantly higher than that of the Con group (P < .05). Tb.Th in the Down group (60.20 ± 7.26 μm) was significantly higher than that in the Con group (39.41 ± 5.44 μm) (P < .01), Up group (49.66 ± 5.75 μm), and Horz group (50.03 ± 5.83 μm) (P < .05). Tb.Th in both the Horz group and the Up group was significantly higher than that in the Con group (P < .05). There was no statistically significant difference between the Horz and Up groups (P > .05). Tb.Sp of the Con group (84.70 ± 9.95 μm) was significantly higher than that of the Down group (67.43 ± 11.89 μm) (P < .05), with no statistically significant difference between the other groups (P > .05) (Figure 5B).
Biomechanical Testing
The failure position among samples was the BTI between the supraspinatus and the humerus. In the biomechanical tests conducted 8 weeks after surgery, it was found that the Down group had higher FL and US than the other groups (Figure 6).
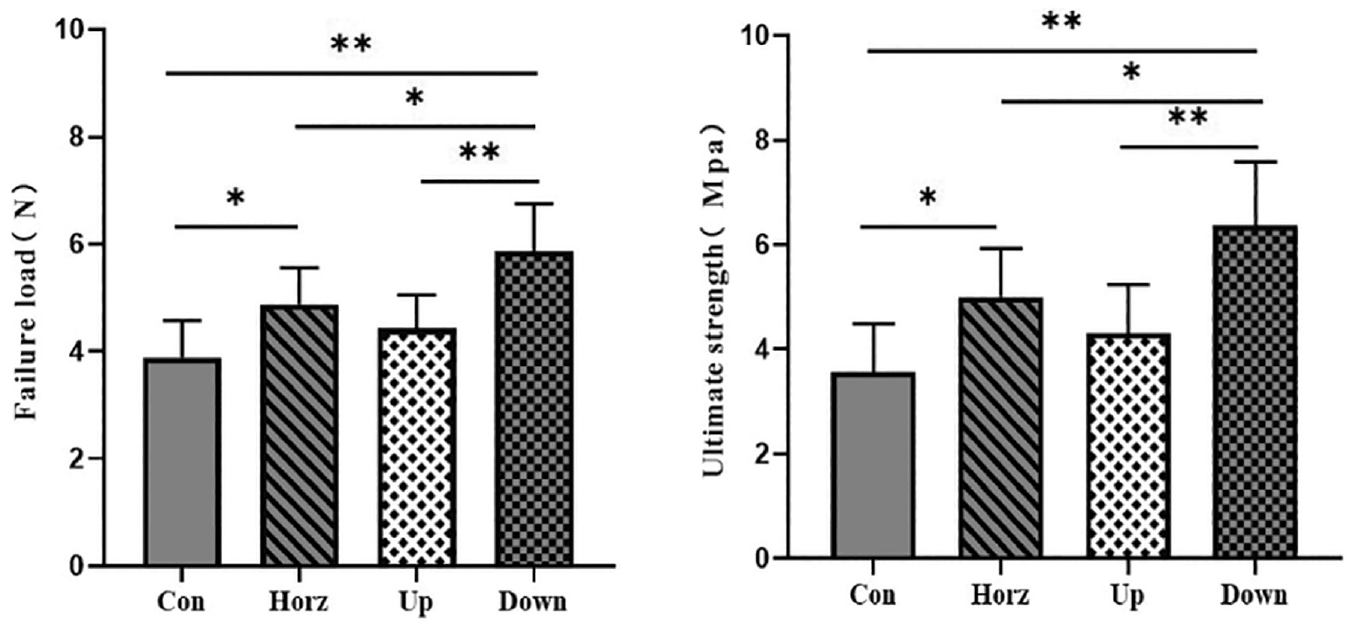
Biomechanical testing at 8 weeks postoperatively. Data are expressed as mean ± SD. *P < .05; **P < .01. Con, control group; Down, –15° downhill running group; Horz, horizontal running group; Up, +15° uphill running group.
At 8 weeks postoperatively, the differences in CSA between the Con group (1.11 ± 0.11 mm2), the Horz group (0.99 ± 0.17 mm2), the Up group (1.04 ± 0.10 mm2), and the Down group (0.95 ± 0.18 mm2) were not statistically significant (P > .05).
At 8 weeks postoperatively, the FL of the Down group (5.87 ± 0.88 N) was significantly better than that of the Con group (3.89 ± 0.70 N), Up group (4.42 ± 0.63 N) (P < .01), and Horz group (4.88 ± 0.68 N) (P < .05). The pullout load of the Horz group was better than that of the Con group (P < .05), while the difference between the Horz group and the Up group was not statistically significant.
The US values of the SSTH specimens were calculated using the following formula: US(Mpa) = FL(N)/CSA (mm2). At 8 weeks postoperatively, the US of the Down group (6.37 ± 1.21 Mpa) was significantly higher than that of the Con group (3.56 ± 0.92 Mpa), Up group (4.31 ± 0.92 Mpa) (P < .01), and Horz group (5.00 ± 0.99 Mpa) (P < .05). Additionally, the US of the Horz group was superior to that of the Con group (P < .05).
Discussion
The healing of the tendon-bone junction includes an initial inflammation period, maturation of fibrocartilage, and bone remodeling.32,33 Early treadmill exercise can help maintain the anatomic continuity of the healing interface, provide appropriate mechanical stimulation, and promote timely tissue healing.21,28 However, different parameters of mechanical stimulation have different effects on tendon injury repair.5,31,35
Andarawis-Puri et al 1 concluded that deficiencies in tendon healing are characterized by improper collagen fiber diameter formation, collagen fiber distribution, and overall protofibrillar misalignment. In the present study, histological results showed a significant difference between the Down group and the other groups in collagen fiber alignment and the fibrocartilage layer. Although the physiological metabolism differs between mice and humans, several studies have indirectly supported our results. Langberg et al 26 demonstrated that concentric training increased the collagen fiber content, reducing the tendency of tendon degeneration in the early stages of tendon injury. Kjaer et al 24 and Philippou et al 40 demonstrated that eccentric loading resulted in tendons with more angiogenesis and collagen accumulation than those produced by concentric loading, which provided evidence in support of its superior benefits for the healing of injured tendons. 4
CD163 is considered to be a specific marker of M2 macrophages with an anti-inflammatory phenotype, which exerts anti-inflammatory effects by binding to their ligands to transduce signals and release anti-inflammatory mediators. 9 At 4 weeks after surgery, each group except for the Con group had M2 macrophages at the repair site, indicating that exercise promotes macrophage recruitment during the early stages of tissue repair. Similarly, Lavin et al 27 found that exercise training exerts an anti-inflammatory effect on skeletal muscle. Ferreira et al 9 found that the induction of CD163 in macrophages directly affects fibroblasts and promotes gap closure. These findings suggest that eccentric contraction of the muscle promotes fibroblast proliferation and deposition of the cytoplasmic matrix to a greater extent than concentric contraction during the healing process of the tendon-bone junction. Mechanical stimulation modulates the polarization of M2 macrophages, which produce anti-inflammatory factors and growth factors. 29 TGF-β1 can stimulate monocytes to produce bioactive mediators that enhance fibroblast growth and inhibit the transcription and signaling of proinflammatory factors.22,43 This results in a well-circulated microenvironment at the site of injury, which aids in tissue repair after mechanical stimulation.16,45 At 4 weeks postoperatively, TGF-β1 concentrations were higher in the Down group than in the other 3 groups, and higher in the Horz and Up groups than in the Con group. This is consistent with the results of Kjaer et al, 24 which indicated that both concentric and eccentric training stimulate TGF-β1 expression and confirmed that the Down group had a higher immune anti-inflammatory repair response. Histology testing showed that the fibrocartilage in the Down group was significantly better than that in the Up group, confirming the findings of Yoon et al 46 and Kovacevic et al 25 that TGF-β1 effectively enhances the strength of tendon-bone healing and improves the collagen ratio at the BTI after rotator cuff repair. Studies have shown that in the early stages of rotator cuff repair, increased TGF-β1 concentration accelerates type 1 collagen and proteoglycan synthesis, promotes angiogenesis and osteoblast precursor proliferation, accelerates cartilage repair, and promotes bone resorption and bone formation.42,44
Compressive and tensile strains induced by muscle contraction during weightbearing exercise can induce osteogenesis and bone remodeling through mechanical conduction. 7 In this study, the Down group showed better improvement in bone morphology. This indicates that mechanical stimulation promotes healing of the tendon-bone junction, eccentric contraction of the muscle has a higher bone formation ability than concentric contraction, and the combination of eccentric and concentric contraction has a higher bone formation ability than concentric contraction alone. This may be related to the fact that during downhill running, each step is subjected to greater ground stress on bone tissue during descent than that during uphill running.3,38 Moreover, eccentric training has a greater effect on neovascularization than concentric training, and increased blood flow in the bone promotes the activation of osteoblasts and accelerates subchondral bone formation.7,40 Compared with the Up and Horz groups, the FL and US were significantly greater in the Down group at 8 weeks postoperatively, and this increase may be related to the fact that eccentric training intensifies the longitudinal growth of the muscle to extend the contraction. 17 Overall, the results showed that eccentric training improves the mechanical properties of the tendon-bone junction in the early stages of rotator cuff injury repair more than concentric training.
In tendinopathies, the tendon requires a low metabolic rate to maintain tension for a long period and carry the load. Eccentric training is more suitable for the rehabilitation of tendinopathies because it has lower oxygen consumption than does concentric training.11,19 Concurrently, numerous studies have shown that eccentric training is effective in preventing muscle sprains, recovering from muscle atrophy, and treating tendon pain.34,41 Our study demonstrated that exercise stimulation with different muscle contraction patterns can initially regulate macrophages according to the magnitude of the inflammatory response at the injury site, resulting in different states of fibroblast proliferation, cytoplasmic matrix deposition, and growth factor concentration, and demonstrating the benefits of eccentric muscle contraction.
This study has some limitations that need to be considered. First, the walking pattern of mouse extremities increases the pressure on the repair site of the supraspinatus muscle, unlike in humans. Second, the acute rotator cuff model was used, whereas most tears seen in the clinical setting are chronic, which may affect tendon viability and muscle atrophy. Future studies should investigate the effects of different eccentric angles on BTI healing after rotator cuff injury and determine the ideal eccentric angle that promotes healing, thereby providing more precise recommendations and theoretical support for the selection of clinical rehabilitation training.
Conclusion
Eccentric contraction promotes healing of the BTI after rotator cuff repair in mice better than other muscle contraction patterns.
Footnotes
Submitted March 24, 2023; accepted August 10, 2023.
One or more of the authors has declared the following potential conflict of interest or source of funding: This work was supported by the Hubei Provincial Natural Science Foundation of China (No. 2019CFB397), Research Fund for Young Teachers of Wuhan Sports University and Donghu Scholar Program of Wuhan Sports University (2019), and Young and Middle-Aged Scientific Research Team Project of Wuhan Sports University (No. 21KT14). AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.