
Abstract
Background:
Matrix-induced autologous chondrocyte implantation (MACI) is an established cell-based therapy for the treatment of chondral defects of the knee. As long-term outcomes are now being reported in the literature, it is important to systematically review available evidence to better inform clinical practice.
Purpose:
To report (1) subjective patient-reported outcomes (PROs) and (2) the rate of graft failure, reoperation, and progression to total knee arthroplasty (TKA) after undergoing MACI of the knee at a minimum 10-year follow-up.
Study Design:
Systematic review; Level of evidence, 4.
Methods:
A comprehensive search of Ovid MEDLINE and Epub Ahead of Print, In-Process & Other Non-Indexed Citations and Daily; Ovid Embase; Ovid Cochrane Central Register of Controlled Trials; Ovid Cochrane Database of Systematic Reviews; and Scopus from 2008 to September 15, 2022, was conducted in the English language. Study eligibility criteria included (1) full-text articles in the English language, (2) patients undergoing a MACI within the knee, (3) clinical outcomes reported, and (4) a minimum 10-year follow-up.
Results:
In total, 168 patients (99 male, 69 female; mean age, 37 years [range, 15-63 years]; mean body mass index, 26.2 [range, 18.6-39.4]) representing 188 treated chondral defects at a minimum 10-year follow-up after MACI were included in this review. Significant and durable long-term improvements were observed across multiple PRO measures. Follow-up magnetic resonance imaging (MRI), when performed, also demonstrated satisfactory defect fill and an intact graft in the majority of patients. The all-cause reoperation rate was 9.0%, with an overall 7.4% rate of progression to TKA at 10 to 17 years of follow-up.
Conclusion:
At a minimum 10-year follow-up, patients undergoing MACI for knee chondral defects demonstrated significant and durable improvements in PROs, satisfactory defect fill on MRI-based assessment, and low rates of reoperation and TKA. These data support the use of MACI as a long-term treatment of focal cartilage defects of the knee.
Keywords
Articular cartilage injuries of the knee joint can be painful, causing significant disability and diminished quality of life.2,13 If these defects are left untreated, they can quickly deteriorate, causing degenerative changes as cartilage has no intrinsic capacity to repair because of its lack of blood supply, nerves, access to the lymphatic system, or stem/progenitor cells.5,16,37 This can lead to posttraumatic osteoarthritis and eventual joint replacement surgery. For these reasons, cartilage repair surgery has become the current clinical standard of care for treating chondral injuries. These procedures can be successful in alleviating symptoms, allowing patients to return to activity in a timely manner; provide mechanical stability; and possibly delay or prevent symptomatic, degenerative changes within the knee.
While there is currently no gold standard surgical procedure for knee cartilage lesions, orthopaedic surgeons have multiple treatment options spanning debridement, microfracture, mosaicplasty, and osteochondral allograft transplantation, depending on the size, depth, and location of chondral injury.38,40,46 One of the highly promising cell-based therapies is autologous chondrocyte implantation (ACI), which has shown overall successful long-term outcomes. 36 However, first- and second-generation ACI techniques relied on suture-fixated periosteum or collagen membranes to contain cell suspension injectate, resulting in technically challenging chondral defect treatment.4,18 More recently, third-generation matrix-assisted chondrocyte implantation (MACI) has become popular as it uses a collagen matrix onto which cells are seeded, thereby substantially streamlining cell implantation.
Short- and midterm prospective randomized trials using MACI have shown promise and satisfactory outcomes.11,41 With peer-reviewed, long-term data on MACI now emerging, it is important to systematically review the available literature to allow patients and surgeons to compare outcomes with other techniques 7 and to effectively counsel patients on outcomes. Therefore, the purpose of this systematic review was to report (1) subjective patient-reported outcomes (PROs) and (2) the rate of graft failure, reoperation, and progression to total knee arthroplasty (TKA) after undergoing MACI of the knee at a minimum 10-year follow-up.
Methods
The protocol for this systematic review was developed according to the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) 35 guidelines and registered in the PROSPERO international prospective register of systematic reviews 8 (registration ID CRD4202 3387909).
Search Criteria
A comprehensive search of several databases from 2008 to September 15, 2022, was conducted. The databases included Ovid MEDLINE and Epub Ahead of Print, In-Process & Other Non-Indexed Citations and Daily; Ovid Embase; Ovid Cochrane Central Register of Controlled Trials; Ovid Cochrane Database of Systematic Reviews; and Scopus. The search strategy was designed and conducted by an experienced librarian with input from the study’s principal investigator (M.H.). Controlled vocabulary supplemented with keywords was used to search for studies of MACI in patient knees. The actual strategy listing all search terms used and how they are combined is available in the Appendix (available in the online version of this article).
Eligibility Criteria
Study eligibility criteria included (1) full-text articles in the English language, (2) investigation of MACI of the knee, (3) clinical outcomes reported with scoring systems validated for minimal clinically important difference (MCID) or Patient Acceptable Symptom State estimates in cartilage restoration of the knee, and (4) a minimum 10-year follow-up. Studies were excluded if they (1) reported on revision cartilage procedures not including debridement/chondroplasty or (2) used first- or second-generation or biologically augmented MACI (Bone Marrow Aspirate Concentrate (BMAC), platelet-rich plasma (PRP), microfracture, etc). No restrictions on type of study design were included as long as patient outcomes were recorded.
Article Selection and Data Extraction
All studies were reviewed for eligibility by 2 independent reviewers (A.S.W. and C.V.N.). Any discrepancies were discussed to make a final decision. One reviewer (A.S.W.) manually extracted study characteristics, study patient characteristics, and primary and additional outcome data. This process was repeated by another reviewer (C.V.N.) who was blinded to the previous extraction. Discrepancies between the 2 extractions were resolved by discussions with the senior author (M.H.). Any additional data considered to be important to the study were requested from individual study authors via email.
Quality Assessment
The methodological quality of studies was assessed by 2 authors independently (A.S.W. and A.L.) using the methodologic index for non-randomized studies (MINORS) criteria. 45 Reviewers scored each article independently, and discrepancies were discussed extensively before consensus was reached.
Data Analysis
When possible, the Cochrane formula for combining groups 12 was applied sequentially for means and standard deviations between groups. Determination of the MCID was based on previous studies pertaining to (non-MACI) ACI, 34 including an International Knee Documentation Committee (IKDC) score of 16.4, Knee injury and Osteoarthritis Outcome Score (KOOS) Pain of 18.8, KOOS Activities of Daily Living of 17.3, KOOS Sport and Recreation of 16.9, and KOOS Quality of Life (QL) of 19.6.
Results
Study Identification
The initial search of several databases resulted in 251 articles. Titles and abstracts were reviewed for preliminary application of inclusion and exclusion criteria, resulting in 7 articles. Full-text reviews of the remaining articles were performed, with 5 articles meeting all inclusion criteria.1,15,17,25,32 One additional record was identified during methodological quality assessment. Two studies by the same author were further evaluated to determine overlapping patient populations. We reached out to the lead author who confirmed that the patient cohort used in the initial study was also included in full for their later study. Figure 1 summarizes the article selection process. Both reviewing authors had selected the same articles for inclusion, resulting in 100% agreement with a kappa of 1.00. All 5 studies were case series with level 4 evidence and MINORS scores of 11 ± 1.1 (range, 9-12).1,15,17,25,32
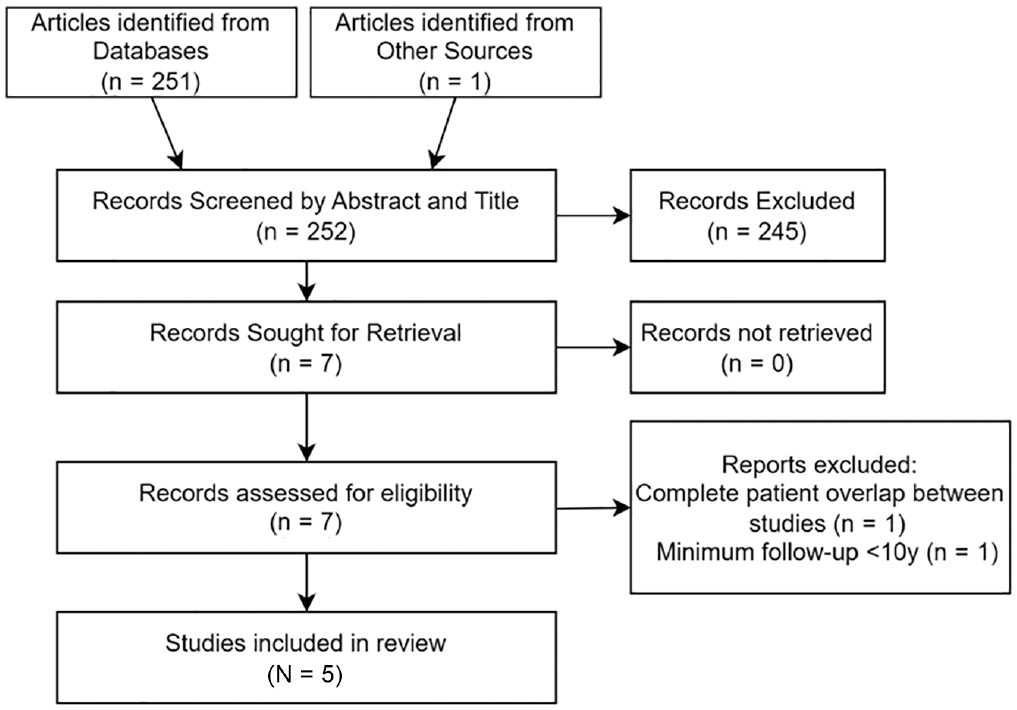
Study selection for systematic review.
Study Population
In total, 168 patients representing 188 treated chondral defects were included in the present systematic review. Study periods covered 1998 to 2018, with a mean follow-up of 12.9 years (range, 10-17 years). Across all studies, 138 of 310 (44.5%) patients were lost to follow-up, with individual studies reporting rates ranging from 14.7% to 73.4%. The mean age of the patients was 37 years (range, 15-63 years). The mean body mass index was 26.2 (range, 18.6-39.4). Chondral defects were most commonly seen at the femoral condyles (129 defects; 68.6%), with a mean chondral lesion size of 3.5 cm2 (range, 1.0-10.0 cm2). Type 1/3 collagen matrices were the most frequently used scaffold types, which were used in 151 (80.3%) of treated chondral defects. Overall, 101 (60.1%) patients had surgery to their knee before undergoing MACI. Study characteristics, patient characteristics, and defect characteristics are shown in Tables 1 and 2.
Study and Patient Characteristics a
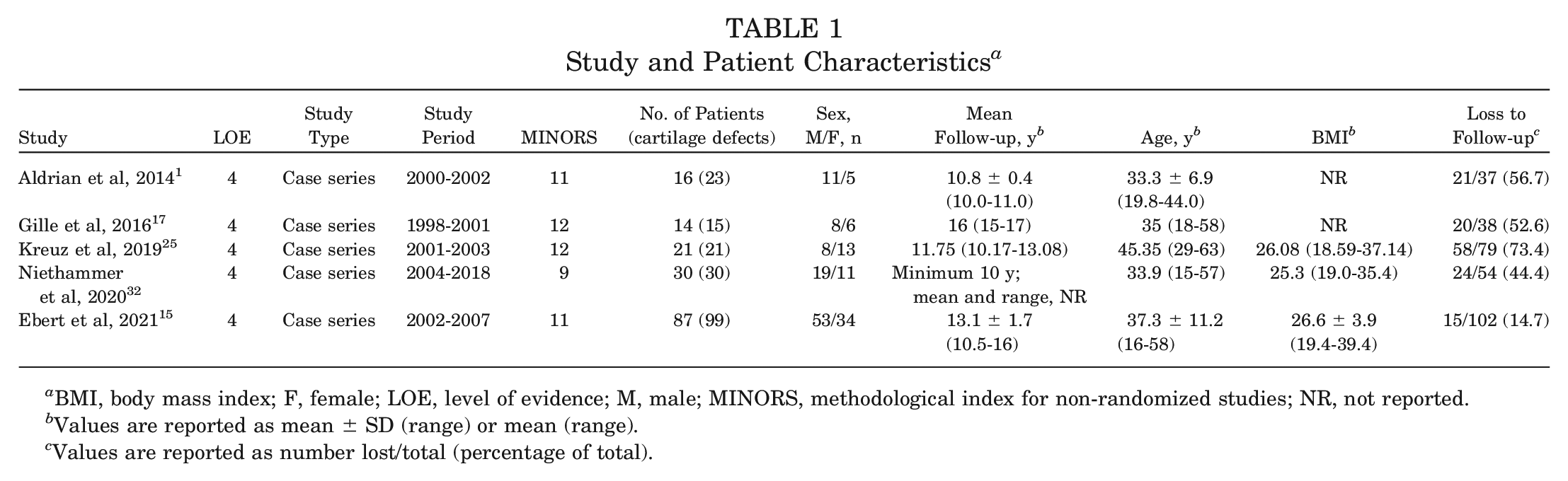
BMI, body mass index; F, female; LOE, level of evidence; M, male; MINORS, methodological index for non-randomized studies; NR, not reported.
Values are reported as mean ± SD (range) or mean (range).
Values are reported as number lost/total (percentage of total).
Defect Characteristics and Previous Surgeries a
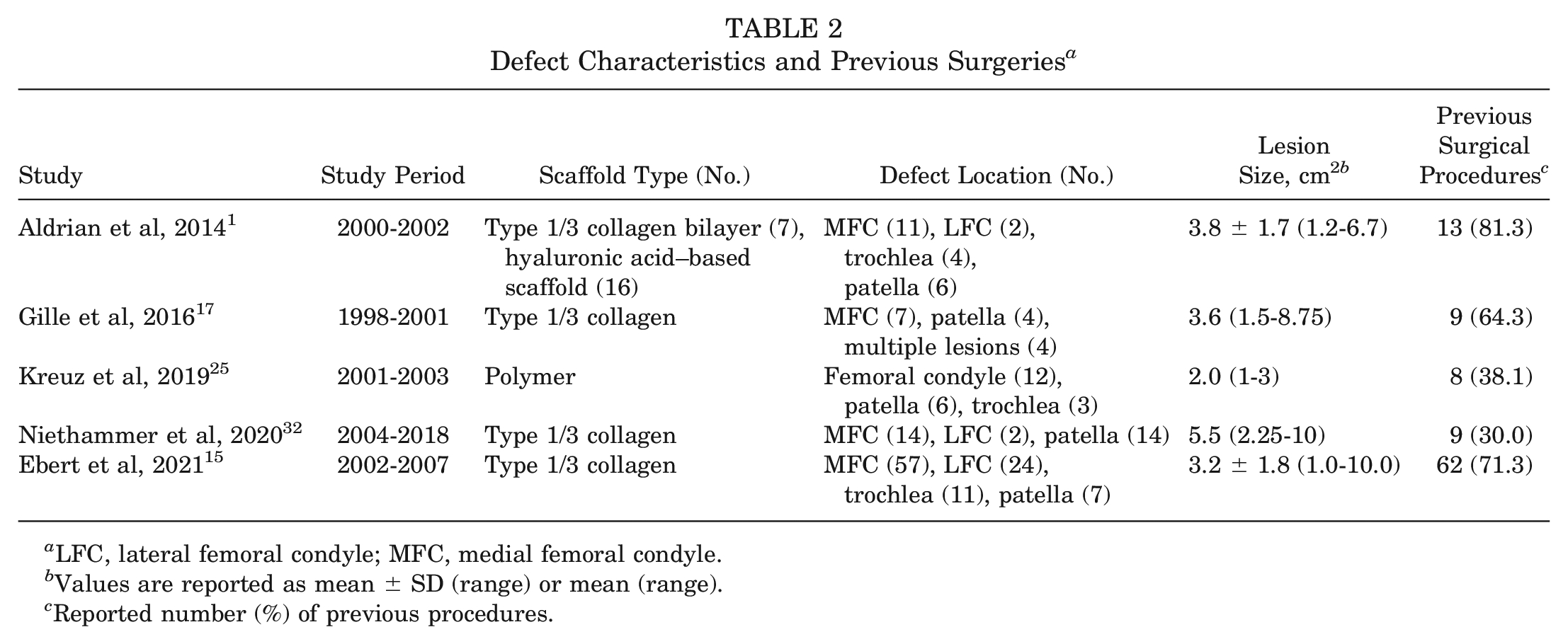
LFC, lateral femoral condyle; MFC, medial femoral condyle.
Values are reported as mean ± SD (range) or mean (range).
Reported number (%) of previous procedures.
Surgical Technique
All studies proceeded with the typical 2-stage surgical technique employed for MACI (harvest, implantation). An initial arthroscopic procedure was performed to harvest cartilage from a nonweightbearing articular surface of the knee. Chondrocytes were subsequently isolated from the sample via enzymatic digestion, expanded in vitro, and seeded onto a scaffold. Expansion took place over a 3- to 4-week period in 4 studies1,17,25,32 and a 6- to 8-week period in 1. 15 At the time of the second stage surgery, an open arthrotomy was performed, the cartilage defect was debrided down to a stable base to the level of the calcified cartilage layer, and the graft was inserted. Fixation of the graft was reported in 4 studies, with 2 using fibrin glue,1,15 1 using transosseous sutures, 25 and 1 using either sutures on surrounding articular cartilage or resorbable polylactide pins. 32
Postoperative Rehabilitation
There was excellent agreement among studies in postoperative rehabilitation protocols. In general, patients with tibiofemoral joint defects were kept partial weightbearing until 8 to 10 weeks postoperatively. Patients with patellofemoral defects were managed with varying, generally accelerated weightbearing protocols. Return to impact sports was not recommended before 12 months postoperatively. Kreuz et al 25 used a uniform rehabilitation protocol regardless of defect location, with gradual return to full weightbearing beginning at 13 weeks postoperatively.
Outcome Measures
All 5 studies reported PROs, and a summary of these scores is included in Table 3. The IKDC score 23 was the most commonly used PRO and was reported in 4 studies.1,17,25,32 The mean preoperative and postoperative IKDC scores ranged from 31.3 to 50.6 and 59.0 to 71.15, respectively (Table 3). Three of these studies17,25,32 demonstrated pre- and postoperative differences that exceeded the MCID, although a statistically significant improvement in IKDC was observed in all studies. When combining study results, there was a mean pre- to postoperative improvement in IKDC of 23.9 (41.2 ± 21.6 to 65.1 ± 20.6), exceeding MCID.
Outcome Measures a
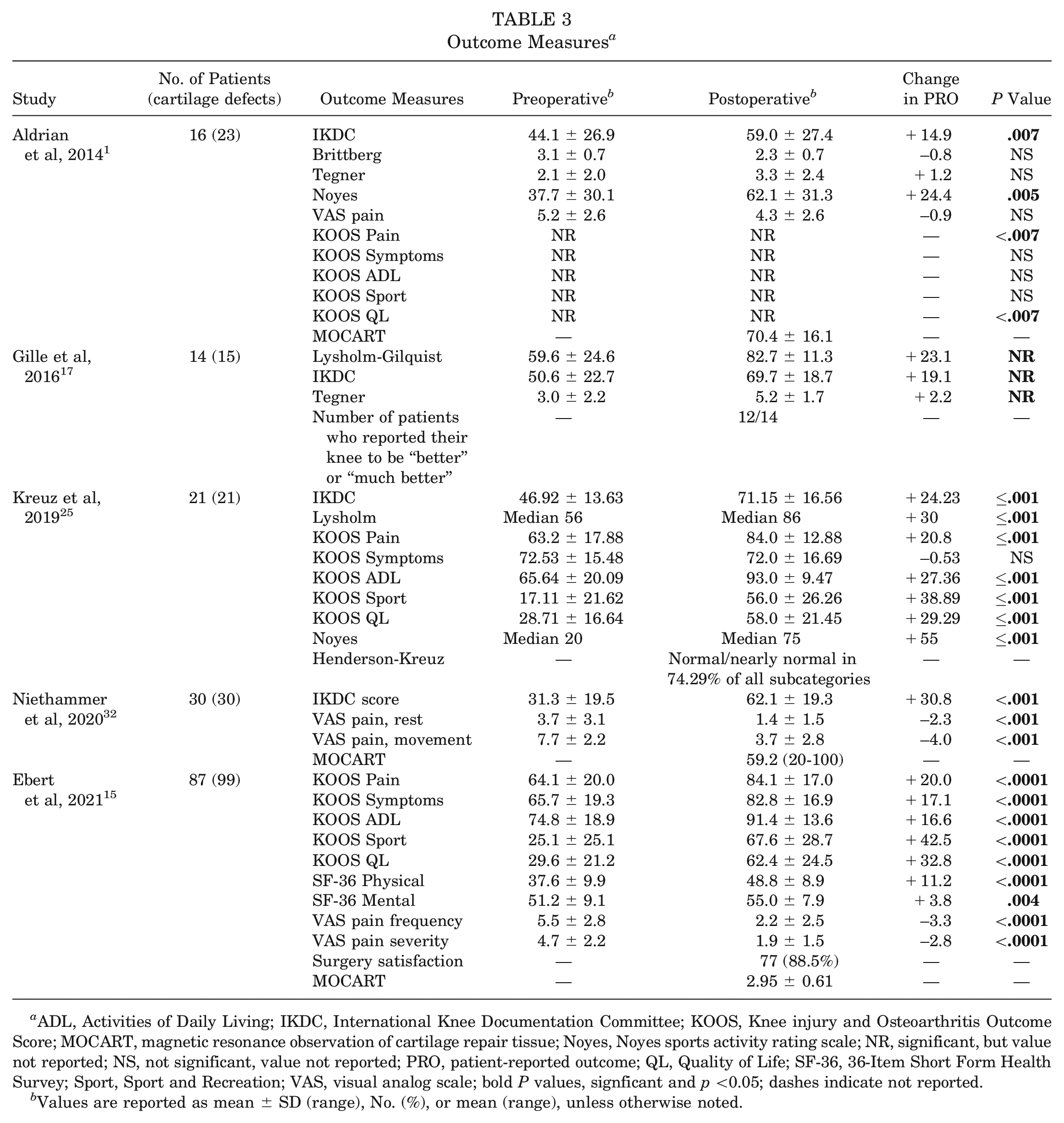
ADL, Activities of Daily Living; IKDC, International Knee Documentation Committee; KOOS, Knee injury and Osteoarthritis Outcome Score; MOCART, magnetic resonance observation of cartilage repair tissue; Noyes, Noyes sports activity rating scale; NR, significant, but value not reported; NS, not significant, value not reported; PRO, patient-reported outcome; QL, Quality of Life; SF-36, 36-Item Short Form Health Survey; Sport, Sport and Recreation; VAS, visual analog scale; bold P values, signficant and p <0.05; dashes indicate not reported.
Values are reported as mean ± SD (range), No. (%), or mean (range), unless otherwise noted.
The KOOS 6 was used in 3 studies.1,15,25 Significant improvements were reported in KOOS Pain and KOOS QL subscores across all studies. Two studies15,25 reported specific pre- and postoperative values for KOOS subscales, with both exceeding the MCID for KOOS Pain, Sport and Recreation, and QL subscores.
The visual analog scale (VAS) for pain was used in 3 studies, but was reported as general VAS pain, 1 VAS pain frequency and severity, 15 or VAS pain at rest and with movement. 32 Other reported PROs included Tegner scores, Noyes sports activity rating scale, 33 36-Item Short Form Health Survey, Brittberg score, 10 and Likert scales for surgery satisfaction or subjective improvement. All studies demonstrated statistically significant improvements across multiple PROs at a minimum 10-year follow-up (Table 3). Gille et al 17 reported that 85.7% of patients felt “better” or “much better” after MACI, and Ebert et al 15 reported that 88.5% of patients were satisfied with surgery.
Magnetic resonance imaging (MRI)–based scoring (magnetic resonance observation of cartilage repair tissue [MOCART]1,15,32 and Henderson-Kreuz 25 ) was used in 4 studies. The MOCART scoring system by Marlovits et al 28 provides subjective evaluations of 9 separate parameters for graft outcomes: degree of defect fill, integration to the border zone, surface and structure of the repair tissue, signal intensity on 2 different sequences, integrity of the subchondral lamina and bone, and presence of adhesions and/or effusion. However, different point-allocating methods have been described.39,43 Aldrian et al 1 and Niethammer et al 32 reported mean scores on a scale of 0 to 100 (70.4 ± 16.1 and 59.2 [range, 20-100], respectively). Ebert et al 15 used a scoring system with a weighting factor, resulting in a score on a scale of 1 to 4 (2.95 ± 0.61 [range, 1.20-3.95]). Kreuz et al 25 used the Henderson-Kreuz score, which combines the Henderson scoring system 21 and Kreuz score 26 for graft hypertrophy. The authors reported that normal or nearly normal values were present in a mean of 74.29% of all subcategories. Gille et al 17 did not perform MRI-based scoring but reported that 6 patients had follow-up radiographs showing signs of progressive osteoarthritis, such as the development of osteophytes or subchondral sclerosis.
Complications, Reoperations, and Arthroplasty Rates
Complications and reoperations were explicitly reported in 3 of the 5 studies (Table 4).1,15,32 The most commonly reported postoperative complication was arthrofibrosis/adhesions, affecting 5 patients. The incidence of graft failure was only explicitly defined by Ebert et al, 15 who noted an overall failure rate per MRI of 9.1%. However, all other studies that used MRI scoring did identify filling of the chondral defect, reporting incomplete filling in 23.1% to 42.9% of cases. Gille et al 17 used radiographs and Kellgren-Lawrence scores to note that 6 of 14 (42.9%) showed signs of progressive osteoarthritis. Of note, Aldrian et al 1 noted 1 patient with an oblique meniscal tear of the posterior horn of the medial meniscus, but it is unknown when postoperatively that this occurred.
Complications, Reoperations, Arthroplasties a
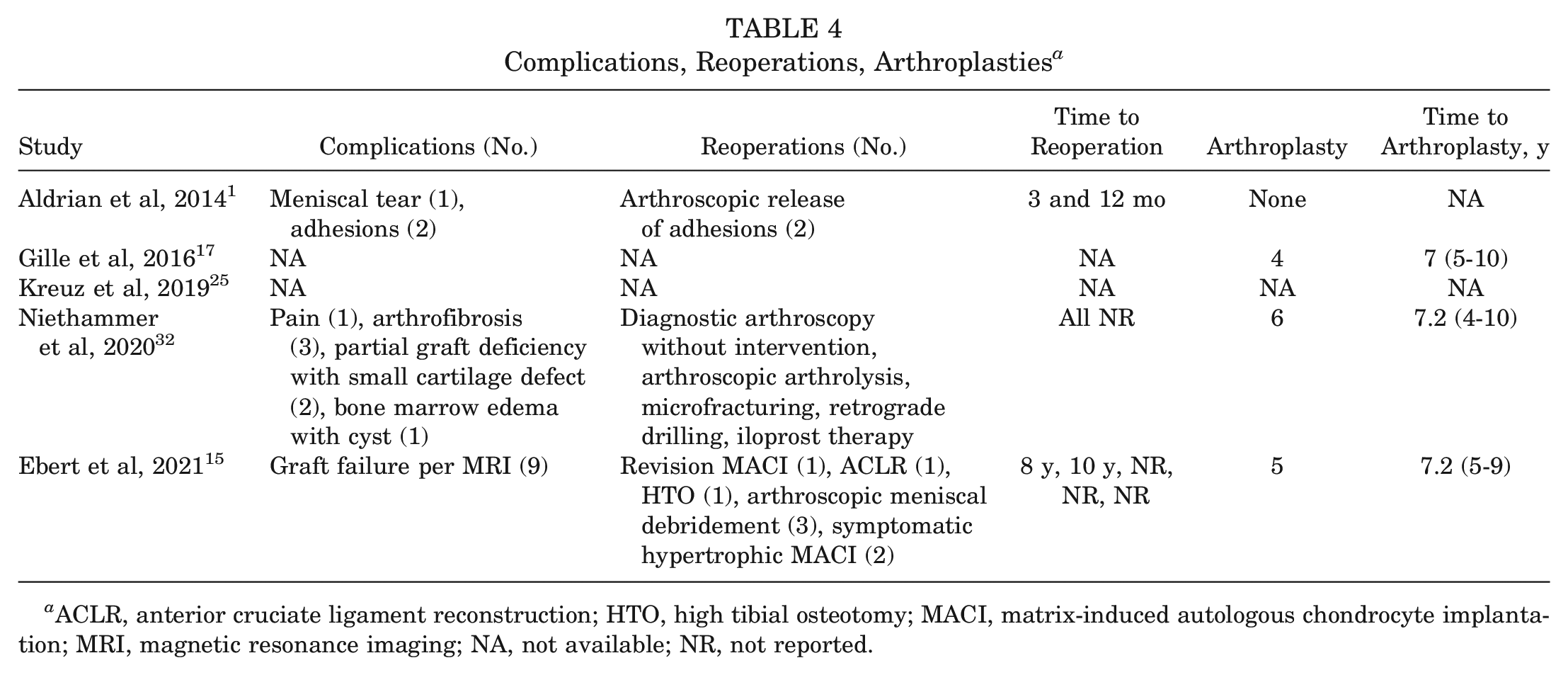
ACLR, anterior cruciate ligament reconstruction; HTO, high tibial osteotomy; MACI, matrix-induced autologous chondrocyte implantation; MRI, magnetic resonance imaging; NA, not available; NR, not reported.
In total, there were 17 all-cause reoperations across the 5 studies analyzed. When applicable, all studies had excluded patients who progressed to TKA before the final follow-up. However, all studies also reported the number of patients excluded as a result of progressing to TKAs, as well as the number of years after MACI at which patients progressed to TKA. Overall, there were 15 TKAs that occurred at a mean of 7.1 years (range, 4-10 years) after MACI. Including these patients in the present study cohort and thus representing a total patient population of 203 treated chondral defects would represent an overall 7.4% rate of progression to TKA.
Discussion
The purpose of the present study was to systematically review available literature to report patient outcomes with MACI for the treatment of knee cartilage injuries at a minimum 10-year follow-up. Our main findings were that (1) patients demonstrated significant and durable improvements across multiple PROs at a minimum 10-year follow-up, 2) MRI-based scoring modalities demonstrated regeneration of articular cartilage or hyaline-like cartilage with overall low rates of graft failure, and 3) satisfactory, low rates of reoperations and progression to TKA were observed. This study represents the first comprehensive systematic review of the literature that reports on long-term, minimum 10-year outcomes of MACI in the knee.
Since first being described by Brittberg et al, 10 [M]ACI has become a widely used cell-based surgical procedure for the repair of articular cartilage defects. A systematic review of first- and second-generation ACI by Pareek et al 36 demonstrated significant improvements of multiple PROs over an 11.4-year mean follow-up. DiBartola et al 14 demonstrated similar improvements in their systematic review of the use of ACI in adolescent patients with a mean follow-up of 4.4 years. The evolution of third-generation MACI has further improved on the technical challenges and limitations of the first and second generations of ACI through the use of seeded biomaterial scaffolding/matrices. 20 These improvements have made MACI a popular treatment option with growing use in general orthopaedic practice. 44
The presented review observed results consistent with those of previously published, shorter-term series on patient outcomes after MACI. A systematic review by Grossman et al 19 on the 1-, 2-, and 5-year outcomes after MACI found significant improvements with medium to large effect sizes in all KOOS subscales. Another systematic review by Iordache et al 22 reported on typical MACI graft findings on MRI, noting that there was a tendency for MOCART scores to improve until 2 years postoperatively, with a subsequent modest decline after the 5-year follow-up, although MRI scores remained significantly improved overall. Brittberg 9 also performed a systematic review in 2010 and reported improvements in both Lysholm-Gilquist and IKDC scores at short- and midterm follow-up for patients undergoing MACI. In the present systematic review, we similarly observed durable, efficacious improvements in a variety of PROs at minimum 10-year follow-up after MACI. In addition, MRI also demonstrated normal findings or full-graft infill in the majority of patients. Importantly, it is of note that there was substantial heterogeneity in not only use of MRI-based scoring, but also how these scores were presented. Of studies reporting MRI scoring, 1 used the Henderson-Kreuz score, 25 whereas 3 used MOCART scores.1,15,32 Of the studies using MOCART scores, none reported specific values for the 9 parameters that make up the MOCART score, 1 did not report a standard deviation of their mean score, 32 and 1 used a modified score with a weighting factor. 15 There is a need for increased homogeneity in both selection of PROs and mode of presentation, as this would allow for more robust, granular analysis of existing literature. Previous studies of first- and second-generation ACI found rates of reoperation as high as 68%, further highlighting the low rates of reoperation in the present study.30,36 A database study by Anigwe et al 3 also found a decreasing risk of reoperation since 2017 and the introduction of MACI. Our study expands on previously published midterm evidence by demonstrating significant improvement in PROs with low rates of secondary complication at a minimum 10-year follow-up.
This systematic review along with previous evidence supports MACI as an efficacious and durable treatment for cartilage lesions of the knee. However, a discussion of MACI would not be complete without noting the practical limitations of the procedure. First, MACI is a 2-stage procedure requiring an initial harvest procedure, 3 to 8 weeks of in vitro chondrocyte proliferation, and then final implantation. Besides donor-site morbidity, additional risks are associated with 2 separate anesthesia events in addition to the logistical and rehabilitation considerations of 2-stage intervention. Furthermore, there is the need for MACI biopsy specimen shipment to a separate facility meeting Food and Drug Administration Good Manufacturing Practice standards. While this does not often directly affect surgeons, the availability of MACI as a therapeutic remains limited in some countries outside the United States given the lack of an available licensed manufacturing laboratory. Finally, the cost of MACI itself is worth mentioning given the estimate of approximately $40,000 29 for the graft itself and a total cost of care estimated at >$80,000 in the US-based population. 27 However, with these considerations taken into account, studies have demonstrated the overall cost-effectiveness of MACI as compared with nonoperative management27,47 and microfracture. 31 Further long-term investigations of MACI outcomes as well as comparisons with developing 1-stage surgical alternatives24,42 remain necessary.
Our review is not without important limitations. First, there were only 5 level 4 studies available for review, of which all achieved MINORS criteria scores <75% of the global ideal score for noncomparative studies. Existing prospective randomized clinical trials have only been presented with short- or midterm results,11,41 and further extension studies are necessary for a high level of evidence supporting the use of MACI. Second, published long-term follow-up data are likely limited by nonresponse bias, which is challenging to evaluate in a granular manner at the time of systematic review. Importantly, we identified an overall 42% loss to follow-up across all studies. Third, the information collected in the present study spans nearly 20 years of treatment, during which changes in surgical technique or chondrocyte-culturing modalities may contribute to treatment heterogeneity and thus limit the generalizability of results. Of note, this was mitigated, as is possible, with the inclusion of only third-generation MACI while excluding its first- and second-generation ACI precursors. Finally, the absence of standardization in data reporting in terms of timing and nature of outcomes collected limits direct comparison of available published study data.
Conclusion
At a minimum 10-year follow-up, patients undergoing MACI for knee chondral defects demonstrated significant and durable improvements in PROs, satisfactory defect fill on MRI-based assessment, and low rates of reoperation and TKA. These data support the use of MACI as a long-term treatment of focal cartilage defects of the knee.
Supplemental Material
sj-pdf-1-ajs-10.1177_03635465231205309 – Supplemental material for Minimum 10-Year Outcomes of Matrix-Induced Autologous Chondrocyte Implantation in the Knee: A Systematic Review
Supplemental material, sj-pdf-1-ajs-10.1177_03635465231205309 for Minimum 10-Year Outcomes of Matrix-Induced Autologous Chondrocyte Implantation in the Knee: A Systematic Review by Allen S. Wang, Christopher V. Nagelli, Abhinav Lamba, Daniël B.F. Saris, Aaron J. Krych and Mario Hevesi in The American Journal of Sports Medicine
Footnotes
Submitted May 17, 2023; accepted August 4, 2023.
One or more of the authors has declared the following potential conflict of interest or source of funding: Support was received from the Foderaro-Quattrone Musculoskeletal-Orthopaedic Surgery Research Innovation Fund. This study was partially funded by the following: National Institute of Arthritis and Musculoskeletal and Skin Diseases for the Musculoskeletal Research Training Program (T32AR56950). D.B.F.S. has received compensation for services other than consulting from Arthrex, research support from the Joint Restoration Foundation, and consulting fees from NewClip and Smith & Nephew. A.J.K. has received consulting fees from Arthrex, the Joint Restoration Foundation, and Responsive Arthroscopy LLC; royalty or license from Arthrex and Responsive Arthroscopy; a grant from DJO LLC; and honoraria from the Joint Restoration Foundation and Musculoskeletal Transplant Foundation; and he served on the board for the Musculoskeletal Transplant Foundation (through 2018). M.H. has received hospitality payments from Medical Device Business Services and Stryker Corp; education payments from Medwest Associates, Smith & Nephew, and Foundation Medical; honoraria from Encore Medical; and consulting fees from Vericel Corp. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
An online CME course associated with this article is available for 1 AMA PRA Category 1 Credit™ at https://education.sportsmed.org/Public/Catalog/Home.aspx?CourseSearch=1&Criteria=9&Option=25. In accordance with the standards of the Accreditation Council for Continuing Medical Education (ACCME), it is the policy of The American Orthopaedic Society for Sports Medicine that authors, editors, and planners disclose to the learners all financial relationships during the past 12 months with any commercial interest (A ‘commercial interest’ is any entity producing, marketing, re-selling, or distributing health care goods or services consumed by, or used on, patients). Any and all disclosures are provided in the online journal CME area which is provided to all participants before they actually take the CME activity. In accordance with AOSSM policy, authors, editors, and planners’ participation in this educational activity will be predicated upon timely submission and review of AOSSM disclosure. Noncompliance will result in an author/editor or planner to be stricken from participating in this CME activity.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.