
Abstract
Background:
Approximately 100,000 anterior cruciate ligament (ACL) reconstructions (ACLRs) occur annually in the United States, and postoperative surgical-site infection is a relatively rare but devastating complication, often leading to graft failure or septic arthritis of the knee, necessitating repeat surgery. Wrapping allografts in vancomycin-soaked gauze has been adopted as a common sterilization technique in the operating room to reduce surgical-site infection; however, identifying effective alternatives to vancomycin has not been extensively pursued.
Hypothesis:
Tobramycin would be as effective as vancomycin in reducing the concentrations of Staphylococcus epidermidis bacteria on tendon allografts.
Study Design:
Controlled laboratory study.
Methods:
S. epidermidis strain ATCC 12228 was inoculated onto the human cadaveric gracilis tendon. The tendons were wrapped in sterile gauze saturated with tobramycin or vancomycin at various experimental concentrations. Bacteria remaining on the tendon were dislodged, serially diluted, and plated for colony counting. Statistical analysis was performed utilizing 2-way analysis of variance testing. Results were considered statistically significant when P < .05.
Results:
Vancomycin (P = .0001) and tobramycin (P < .0001) reduced bacterial concentration. Tobramycin was found to produce a statistically significant reduction in bacterial concentration at concentrations as low as 0.1 mg/mL (P < .0001 and P = .01 at 10 and 20 minutes), while vancomycin produced a statistically significant reduction at a concentration as low as 2.5 mg/mL (P < .0001 at both 10 and 20 minutes).
Conclusion:
This study demonstrates that tobramycin is as effective as vancomycin in bacterial concentration reduction but can achieve this reduction level at lower doses. Further studies clarifying the biomechanical and cytotoxic effects of tobramycin on tendon tissue are indicated to solidify its use as a clinical alternative to vancomycin in ACLR.
Clinical Relevance:
These results will begin establishing tobramycin as an alternative to vancomycin in ACL graft decontamination. Because of relatively frequent shortages of vancomycin, establishing tobramycin as an alternative agent is a useful option for the orthopaedic surgeon.
Anterior cruciate ligament reconstructions (ACLRs) are a common orthopaedic surgery, with approximately 100,000 reconstructions completed annually in the United States. 4 Infection is a rare but devastating complication requiring further treatment, and infection rates have been described to be between 0.14% and 2.20%, with the most common organisms of infection being skin commensal organisms, including Staphylococcus aureus and Staphylococcus epidermidis.3,14,20 Wrapping allografts in vancomycin-soaked gauze has been incorporated into surgical protocols and has been demonstrated as effective in significantly reducing postoperative infection rates. However, alternatives to vancomycin for this purpose have yet to be fully investigated. Thus, there is a need to validate an alternative agent in the event of vancomycin shortage.12,15,20
Vancomycin has experienced periodic global shortages, limiting its availability. 13 For these reasons, alternative agents are being explored. Gentamycin solution is one such possible alternative and has recently been reported to help decrease the incidence of septic arthritis after ACLR surgery.2,10 Both adult and pediatric formulations of gentamycin are frequently in shortage; however, some Canadian medical centers replaced gentamycin with tobramycin during the shortage period.13,19 Tobramycin is another possible alternative to vancomycin, and both are already used in orthopaedic applications.8,9 The European Committee on Antimicrobial Susceptibility Testing breakpoints indicate that vancomycin has a minimum inhibitory concentration (MIC) of 4 µg/mL for coagulase negative staphylococcus, while tobramycin and gentamycin both have MICs at 2 µg/mL, indicating higher potency than vancomycin. 6 Tobramycin produces a slightly smaller zone of inhibition than gentamycin at an equivalent dose, with 20 mm and 22 mm zones of inhibition respectively, indicating potentially slightly higher potency against coagulase-negative staphylococcus with gentamycin. 6 The relative availability advantage, coupled with the very similar potency against common pathogens in ACLR, would make tobramycin a valuable alternative to gentamycin and vancomycin. This study aimed to compare the efficacy of tobramycin compared with vancomycin in graft decontamination using the antibiotic-wrapping technique. Tobramycin would be a valuable alternative to vancomycin because of its more consistent availability than gentamycin or vancomycin. 13 We hypothesized that tobramycin would demonstrate equal or greater efficacy to vancomycin in decontaminating a graft inoculated with S. epidermidis.
Methods
The following experiments were exempt from institutional review board approval.
Strain Selection and Growth
S. epidermidis ATCC 12228 was selected for the study. This strain is an intracellular adhesin negative strain, which forms low levels of biofilm. 5 This strain was subsequently cultured in brain heart infusion media (BHI) (Beckton; Dickinson and Company) for 18 hours in a shaker at 37°C.
Inoculation Concentration and Exposure Duration
To determine experimental inoculation conditions, inoculum concentrations of 1×104, 1×105, and 1×106 colony-forming units (CFU)/mL were assessed. Assessments were completed utilizing an adapted procedure protocol developed by Schüttler et al. 16 The human cadaveric gracilis tendon graft was segmented into 2 cm sections and submerged in 5 mL of sterile BHI media for 20 minutes. They were then transferred to 5 mL of bacterial inoculum and incubated at room temperature with gentle rocking for 30 minutes. After incubation, the tendon segments were moved to 2 mL of sterile BHI and vortexed for 1 minute to dislodge any loosely adhered bacteria. Also, 10 µL of the vortexed media was pipette spotted onto BHI agar plates for colony counting. Only inoculum concentrations of 1 × 106 CFU consistently achieved recoverable infection using this technique. Thus, 1 × 106 CFU/mL was used for the remainder of the experiment.
Gracilis Graft Preparation
Human cadaveric gracilis graft tendons were surgically dissected from donor tissue under sterile conditions over several years. These tendons were packaged in vacuum-sealed plastic and stored at −20°C. Frozen tendons were removed from the freezer and allowed to thaw before use. In a sterile biosafety cabinet, tendons were removed from their packaging and placed in a sterile petri dish. Using sterilized instrumentation, the tendons were trimmed of any remaining muscular or fascial attachments and cut into 2-cm segments.
Inoculation Protocol
Gracilis tendon segments were rehydrated by submerging in 5 mL of sterile BHI in a 12-well plate (Sigma-Aldrich) for 20 minutes. Once this rehydration period elapsed, tendons were transferred for submersion in 5 mL of inoculum at 1 × 106 CFU/mL for 30 minutes at room temperature with shaking at 125 rpm.
Antibiotic Treatment
After bacterial inoculation was complete, the tendon allograft segments were transferred to sterile petri dishes. In each dish, a 3-in × 3-in × 12-ply sterile gauze pad was saturated with 5 mL of tobramycin or vancomycin at a concentration of 1, 2.5, 5, or 10 mg/mL. In addition, 5 mL of normal saline was used as a control sham treatment. Antibiotic administration via the gauze wrapping was performed for either 10 or 20 minutes. After this treatment, the tendons were unwrapped and placed in a 15 mL conical centrifuge tube with 2 mL of sterile BHI media.
CFU Determination
The conical tubes containing tendon segments were vortexed for 1 minute to dislodge any planktonic and loosely attached bacteria on the surface of the tendon. These specimens immediately underwent two 1 to 10 serial dilutions with phosphate-buffered saline. For bacterial counting, 10 µL drops were spotted on a BHI agar plate. These plates were incubated overnight at 37°C. Moreover, the remainder of the solution and tendon from the 20-minute BHI-soaked samples were transferred into 15-mL conical tubes and incubated for 1 week at 37°C with 220-rpm shaking to look for visible signs of bacterial contamination. The colony count assay has a detection limit of 33 CFU/mL, and the log10 of this limit is 1.52.
Disk Diffusion Assay
An undiluted bacterial culture was spread on a BHI agar plate. Sterile filter disks were transferred to sterile petri dishes, and 10 µL of undiluted bacterial recovery and the first 1 to 10 dilution were placed onto disks for each antibiotic treatment. These disks were then placed onto the BHI agar plate and incubated overnight at 37°C. Zones of inhibition were measured from the edge of the filter disk to the edge of bacterial growth. Zones of inhibition indicated residual antibiotics above the MIC present in the sample.
Statistical Analysis
Data were analyzed using standard software on Microsoft Excel (Microsoft). Bacterial concentrations for each experimental condition were back-calculated by averaging the number of colonies counted and multiplying by the cumulative dilution factor. Further analysis was performed on geometric means, and differences were reported as the difference of log10 values. To assess the effect of antibiotic exposure, 2-way analysis of variance (ANOVA) was conducted comparing each antibiotic experimental condition to the saline condition at the same time point. Differences were considered significant at P < .05.
Results
Disk Diffusion Assays
In undiluted samples, tobramycin demonstrated a zone of inhibition at all concentrations. Following a 1 to 10 serial dilution, only media that had been exposed to tendons treated with 10 mg/mL of tobramycin demonstrated zones of inhibition, demonstrating a MIC for tobramycin over 1 mg/mL. Figure 1 shows disk diffusion assays for 10 mg/mL of both tobramycin and vancomycin and their 1 to 10 and 1 to 100 dilutions when taken from both 10- and 20-minute treatment media samples.
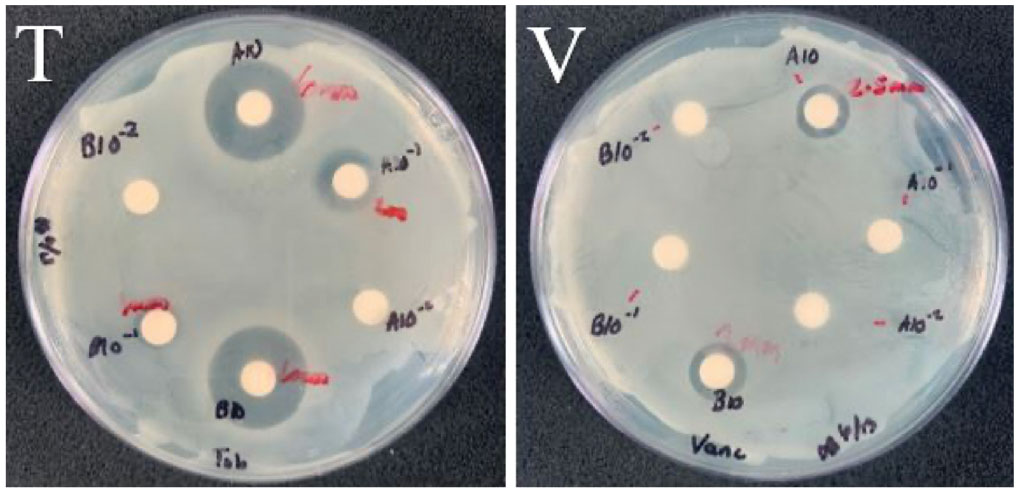
Disk diffusion assays of 10-µL recovery media taken from 10 mg/mL treatment conditions with tobramycin (T) and vancomycin (V). Disks are coded with an A or a B, representing 10- and 20-minute treatment time respectively, as well as no exponent, −1, or −2, representing undiluted and the first and second serial dilutions, respectively.
Interpretation of Experimental Colony Counts
Tobramycin concentrations as low as 0.1 mg/mL were significantly effective (P < .0001) at reducing bacterial concentration on the tendon, producing a 5.435-log reduction, and concentrations above 1 mg/mL reduced bacteria to below detectable levels (Figure 2).
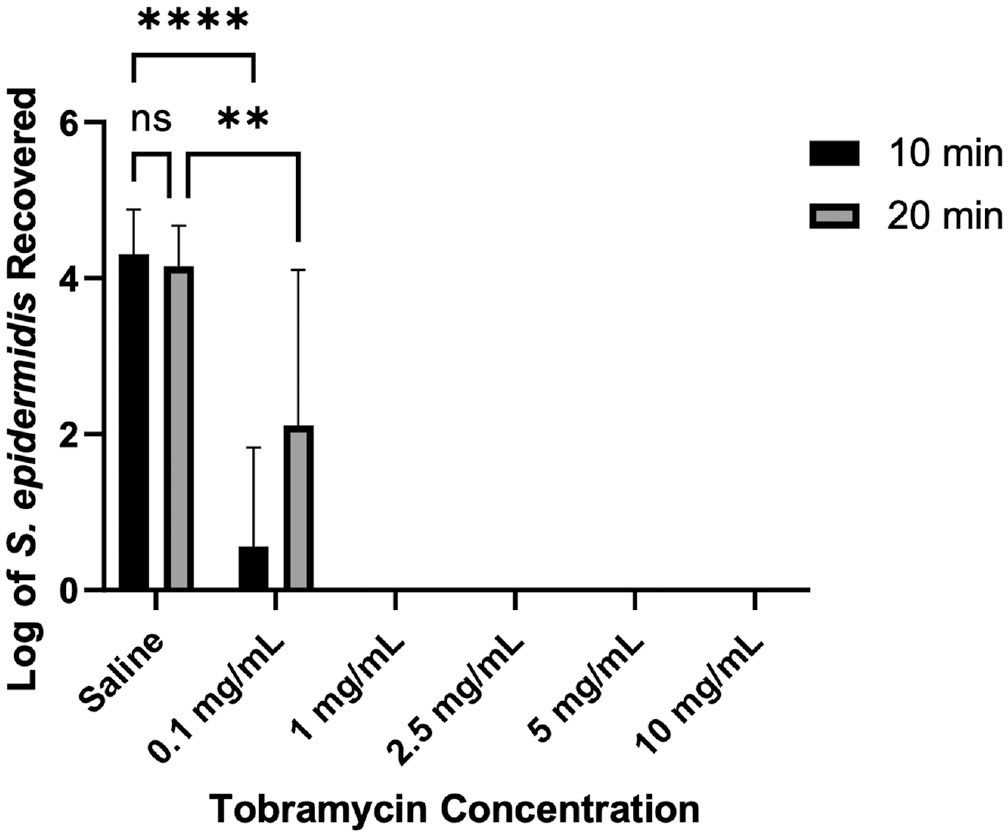
Recovered Staphylococcus epidermidis after treatment with tobramycin. **P≤ .01. ****P≤ .0001. ns, nonsignificant.
Vancomycin demonstrated a 5.108-log significant reduction (P < .0001) in bacterial concentration at 2.5 mg/mL doses, with a bacterial reduction below detectable concentrations at 10 mg/mL, equivalent to a 6-log reduction. While there were no significant differences at any 1 treatment concentration, 2-way ANOVA (Table 1) showed that treatment time was significant across vancomycin treatment concentrations (Figures 1 and 3).
ANOVA Analysis of the Effect of Treatment Time and Antibiotic Concentration on Reduction of Bacterial Concentration a

Bold P values represent significance. ANOVA, analysis of variance.
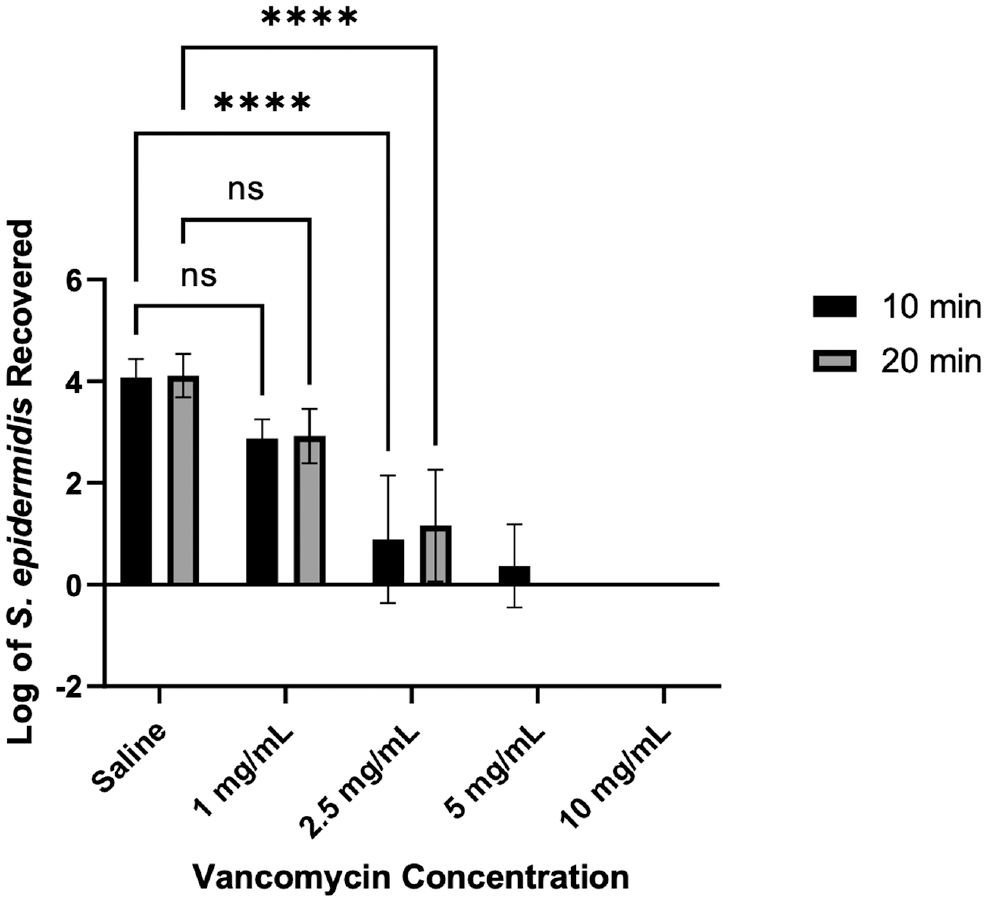
Recovered Staphylococcus epidermidis after treatment with vancomycin. ****P≤ .0001. ns, nonsignificant.
Discussion
Since the introduction of vancomycin wrapping in 2012, there has been very little research into alternative agents despite the occurrence of vancomycin shortages. To our knowledge, this is the first paper investigating tobramycin for this purpose, and the literature 10 investigating gentamicin is as new as 2021. Thus, much of the literature on alternative agents is limited to extrapolation from similar orthopaedic applications already described.
Our results demonstrate that when compared with vancomycin, which is the standard treatment recommended by the current literature, tobramycin is equally effective at reducing S. epidermidis load on allograft tendon samples.12,20 In addition, this equivalent effect was found to be achievable at much lower doses of tobramycin than vancomycin. Use of vancomycin at 5 mg/mL still showed some residual bacterial growth despite 5 mg/mL being both the surgically effective concentration and that approaching a cytotoxic level for human primary tenocytes (Figure 3).11,12,20 Use of tobramycin at a 1-mg/mL concentration was equally effective as vancomycin at 5 mg/mL. Tobramycin has been found to damage osteoblasts and lead to chondrocyte toxicity at concentrations above 2 mg/mL. 1 Tobramycin is considered a more cytotoxic antimicrobial than vancomycin; however, the risks of cellular damage may be avoidable by achieving allograft decontamination at a lower dose than its cytotoxic concentration.
While tobramycin is bactericidal, some of its effects on the tendons and surrounding tissue remain uncharacterized. The ability of tendons to behave as reservoirs for antibiotic elution has been described, and vancomycin elution from tendons, in particular, has been characterized by high-performance liquid chromatography. 7 Similarly, the effect of vancomycin concentration on the biomechanical properties of tendons has been quantified in a porcine model. 16 Quantitative characterization of the elution of tobramycin from tendons will guide further cytotoxicity and biomechanical studies based on the concentration of tobramycin being eluted into the surrounding tissue. Further studies should assess cytotoxic or mechanically destabilizing effects of tobramycin on the cartilage and bone of the knee joint.
While S. epidermidis is one of the most common knee pathogens, other pathogens beyond the scope of this study may have different antibiotic resistance profiles. Further, S. epidermidis ATC 12228 does not form a biofilm, although many hospital-acquired strains do, and biofilm formation has been shown to increase antibiotic resistance 17 and weaken tendon tensile strength. 18 This study, therefore, represents a window into the most likely pathogenic conditions within a knee after ACLR and requires further investigation into tobramycin action against biofilm.
Footnotes
Submitted June 13, 2023; accepted November 8, 2023.
One or more of the authors has declared the following potential conflict of interest or source of funding: This work was supported in part by The Ohio State University College of Medicine Roessler Research Scholarship (B.N.B.) and R01 GM124436 (P.S.). C.C.K. has received consulting fees and compensation for other services from Arthrex, Bioventus, and CDC Medical. D.C.F. has received consulting fees from Smith & Nephew, Vericel, Linvatec, Medical Device Business Services, and DePuy Synthes; and compensation for other than consulting from Smith & Nephew and KARL STORZ Endoscopy. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.