
Abstract
Background:
Primary repair of the anterior cruciate ligament (ACL) has some potential advantages over the reconstruction technique, which include but are not limited to better knee sensation due to preservation of the natural ACL tissue in patients compared with tendon graft. Proprioception is impaired after ACL injuries and the sense of the joint position is lost.
Purpose/Hypothesis:
The purpose of this study was to compare arthroscopic ACL primary repair and ACL reconstruction techniques clinically and functionally and analyze the differences in proprioception. It was hypothesized that primary repair would restore knee joint proprioception more successfully because the original tissue of the ACL is preserved.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
A total of 63 patients (34 underwent reconstruction and 29 underwent primary repair between 2017 and 2020) and 33 healthy controls, as well as the healthy knees of the operated groups, were evaluated between 24 and 48 months (mean, 29 months) postoperatively. Patients with proximal femoral avulsion tears and stump quality suitable for repair underwent primary repair, and those with tears outside these criteria underwent reconstruction using hamstring tendon autograft. Proprioception was evaluated using the active joint position sensation method during weightbearing, with a digital inclinometer used to measure differences between the target and achieved flexion angles of 15°, 30°, and 60°.
Results:
At 15° of knee flexion, the deviation angles for the healthy knee of the reconstruction and primary repair groups were significantly smaller than those of the control group (P < .001), but there was no statistically significant difference between the groups in terms of deviation angle at 30° and 60° of flexion. The deviation angle of the operated knees was statistically significantly larger in the reconstruction group than in the primary repair group at all angles. The deviation angles at 15°, 30°, and 60° were 2.83°, 2.66°, and 2.66° in the reconstruction group and 1.00°, 1.00°, and 1.33° in the primary repair group, respectively (P < .001). There was no statistically significant difference between the reconstruction and primary repair groups in terms of clinical scores.
Conclusion:
Primary ACL repair can preserve proprioception in a well-selected patient group. In short-term follow-up, primary repair of the ACL in patients with proximal femoral avulsion tears and stump quality suitable for repair appears to be proprioceptively protective. Future studies are needed to clarify the long-term consequences of primary repair on proprioception in a larger population.
While most anterior cruciate ligament (ACL) injuries cause instability in the short term, meniscal and cartilage damage can be observed in mid- and long-term follow-ups, with patients experiencing pain and limitation in range of motion. 17 Various treatment options exist that aim to return patients to their preinjury functional capabilities. Until the late 1980s, primary repair was widely accepted as the standard treatment for ACL injuries. Despite the good results in short-term follow-ups, the outcome was poor in mid- to long-term follow-ups; therefore, the primary repair technique was abandoned and reconstruction surgery using allografts or autologous tendon grafts became the new standard for the treatment of the ACL injuries.30,34 Over the years, the historical outcome of primary ACL repair has been influenced by many variables, including limitations in diagnosis, treatment, and technological standards. For example, primary repair was routinely performed in all patients arthrotomically (open), regardless of the stump quality, tear type, and other accompanying injuries, and postoperative care consisted of long-term immobilization and nonweightbearing. 34 With more advancements in arthroscopic techniques, in recent years ACL primary repair has come to the foreground again, and its use has increased for certain groups of patients in some centers. 39
ACL primary repair has some potential advantages over the reconstruction technique, including better knee sensation due to preservation of the natural ACL tissue in patients compared with tendon graft. 41 Moreover, in the event of failure of either treatment method, revision surgery after primary repair is expected to be similar to primary reconstruction because no tunnels or grafts have been used, whereas revision of reconstruction surgery may be complicated by tunnel malposition and preexisting implants that may adversely affect healing.4,37 One of the most important advantages of the primary repair method is that the physis is not damaged in pediatric patients with open growth plates, whereas reconstruction techniques performed in children may lead to growth disorders such as leg shortening due to physis injury.6,19 Recent studies have shown an increased success rate after primary repair of proximal ACL tears. 35 In the early 1990s, Sherman et al 28 divided patients who underwent open primary ACL repair into 4 categories based on the location of the tear and found that better results were obtained in the patient group with proximal tears than in the group with midsubstance tears. The reasons for this are the increased vascularity in the proximal part of the ACL 32 and the potential for better healing of this region, similar to the healing of extra-articular ligaments. 24 At the present time, primary repair methods such as suture anchors, 1 dynamic intraligamentary stabilization, 18 and internal bracing 16 have been described for use in arthroscopic surgery. In this context, it has been shown that primary repair of the ACL can be reconsidered as an effective treatment modality in a selected group of patients with tears only in the proximal region of the ACL and with good stump quality. 31
There are several types of neural mechanoreceptors inside the ACL (Ruffini, Pacini, and Golgi-like receptors) that have a proprioceptive function and form an afferent arc to provide information to the central nervous system about the position and movement of the knee upon postural changes. All the mechanoreceptors for proprioception provide input to the central nervous system regarding tissue deformation. Through this reflex, the cruciate ligament sensory system alters periarticular muscle tone to increase dynamic knee stability. 15 Stimulation of these receptors has been shown to initiate a reflex arc leading to the contractions of the stabilizing muscles; thus, these mechanoreceptors have a protective role. 33 Proprioception is impaired after ACL injuries and the sense of joint position is lost because it is directly related to the number of mechanoreceptors available. 26 Because of the decrease in proprioceptive feedback, patients are more at risk for reinjury. 21 Therefore, preservation of the ACL stump may help to maintain proprioception. 2 According to the available literature, whether proprioception improves after ACL reconstruction (ACLR) is still controversial, and there are no studies evaluating proprioception after primary ACL repair. This led us to evaluate proprioception in patients who have undergone primary ACL repair surgery.
The aim of this study was to compare arthroscopic ACL primary repair and ACLR techniques clinically and functionally and analyze the differences in postoperative proprioception. We hypothesized that primary repair restores knee joint proprioception more successfully because the original tissue of the ACL is preserved, and because of the healing potential of the proximal part of the ACL, the knee joint gains as much stability and function as seen in cases using the gold standard in treatment, the reconstruction technique.
Methods
Approval was obtained from the Gazi University Clinical Research Ethics Committee (research No. 2022-98). In this study, we retrospectively evaluated the clinical outcomes of patients with a diagnosis of total ACL rupture who underwent ACLR or ACL primary repair between the dates of 2017 and 2020 at the Gazi University Department of Orthopaedics and Traumatology. Patients who regularly attended postoperative follow-up visits for ≥2 years were included in the study. Patients were excluded for the following reasons: previous surgery for partial or chronic ACL ruptures; concomitant multiple ligament injuries; previous surgery for the same or contralateral knee; lower extremity malalignment; inflammatory or infectious arthritis; endocrinologic, rheumatologic, and oncologic diseases; tibial avulsion–type ACL tears; and no preoperative magnetic resonance imaging (MRI), radiographs, or surgical records.
Of the 232 patients with a full-thickness ACL tear, patients who had been operated on within the first 90 days after injury (acute, <3 weeks; subacute, 3 weeks to 3 months) were included in the study because primary ACL repair could not be performed in chronic cases with poor stump quality. Thus, 146 of the 232 patients operated on were excluded from the study. Of the 86 patients who underwent surgery within the first 90 days after the injury, 8 had multiple-ligament knee injuries and 5 had distal tibial avulsion tears and were therefore excluded from the study. Of the remaining 73 patients, 8 patients had a history of previous operations and 2 patients did not attend follow-ups. The remaining 63 patients were included in the study: 29 patients with proximal femoral avulsion tear who underwent primary repair and 34 patients who underwent ACLR because of the absence of an indication for primary repair (Figure 1).
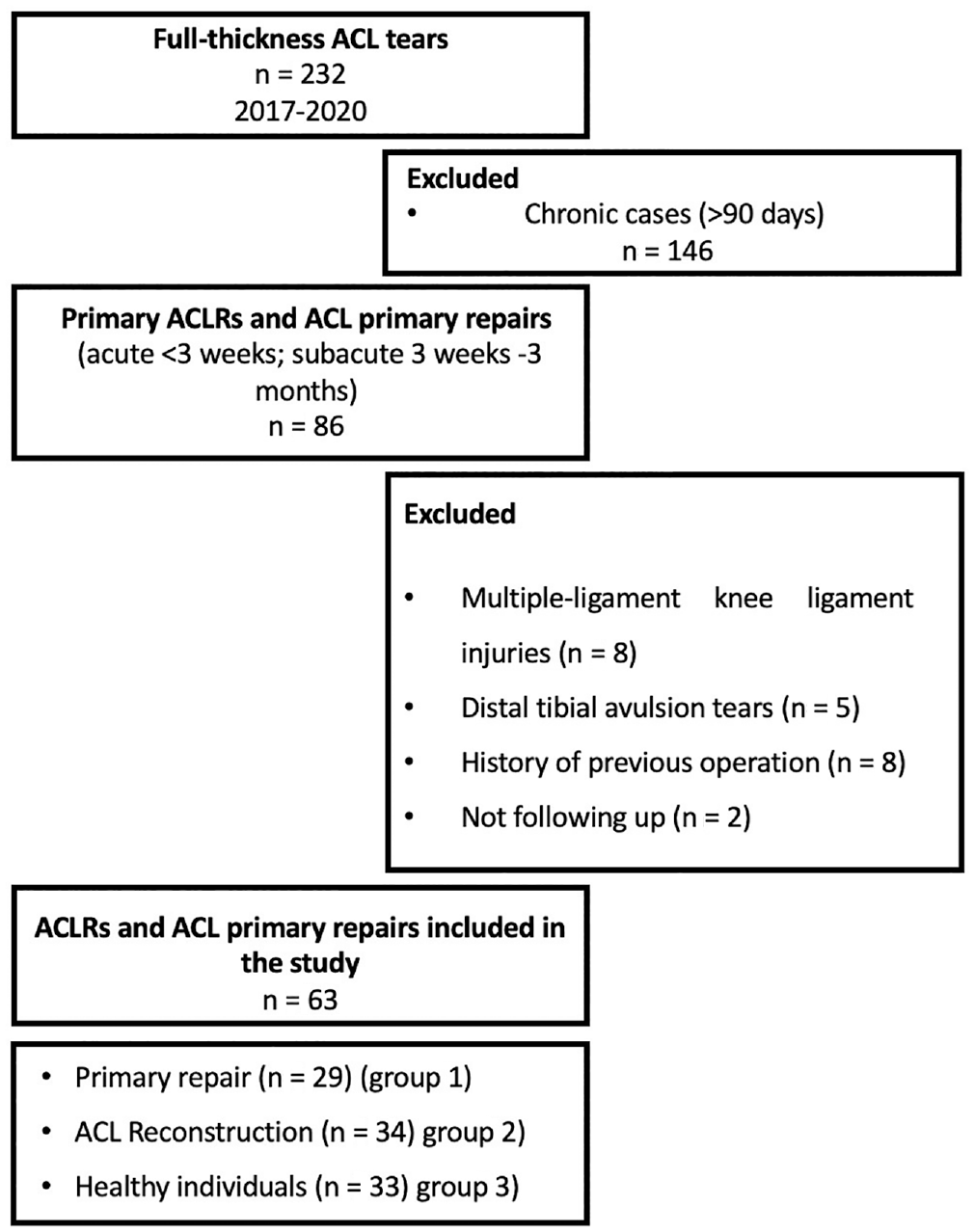
Flowchart of patient selection procedure. ACL, anterior cruciate ligament; ACLR, anterior cruciate ligament reconstruction.
The control group consisted of 33 healthy participants who had knee MRI scans taken for any reason and had no meniscal, chondral, or ligamentous damage detected. It included people aged 18 to 40 years who participated in sports ≥3 times a week, had no history of musculoskeletal injury in the lower extremity before the evaluation, and had no chronic disease. Between all groups (reconstruction, primary repair, and healthy control), there was no statistically significant difference according to age, sex, body mass index (BMI), dominant side, and operated side. Also, there was no statistically significant difference regarding the time between injury and surgery in the reconstruction group and primary repair group (P = .109) (Table 1). The follow-up periods after surgery in the reconstruction and primary repair groups were 27 months (range, 24-46 months) and 29 months (range, 24-48 months), respectively, and there was no significant difference regarding follow-up periods between the 2 groups (P = .356). In the reconstruction group, 4 patients (11.76%) had lateral meniscal tears and 9 patients (26.5%) had medial meniscal tears. In the primary repair group, 4 patients (13.8%) had concomitant lateral meniscal tears and 7 patients (24.1%) had concomitant medial meniscal tears. In the reconstruction group, repair was performed in 11 patients and partial meniscectomy in 2 patients. In the primary repair group, meniscal repair was performed in 9 patients and partial meniscectomy in 2 patients. There was no statistically significant difference between the groups.
Patient Characteristics a
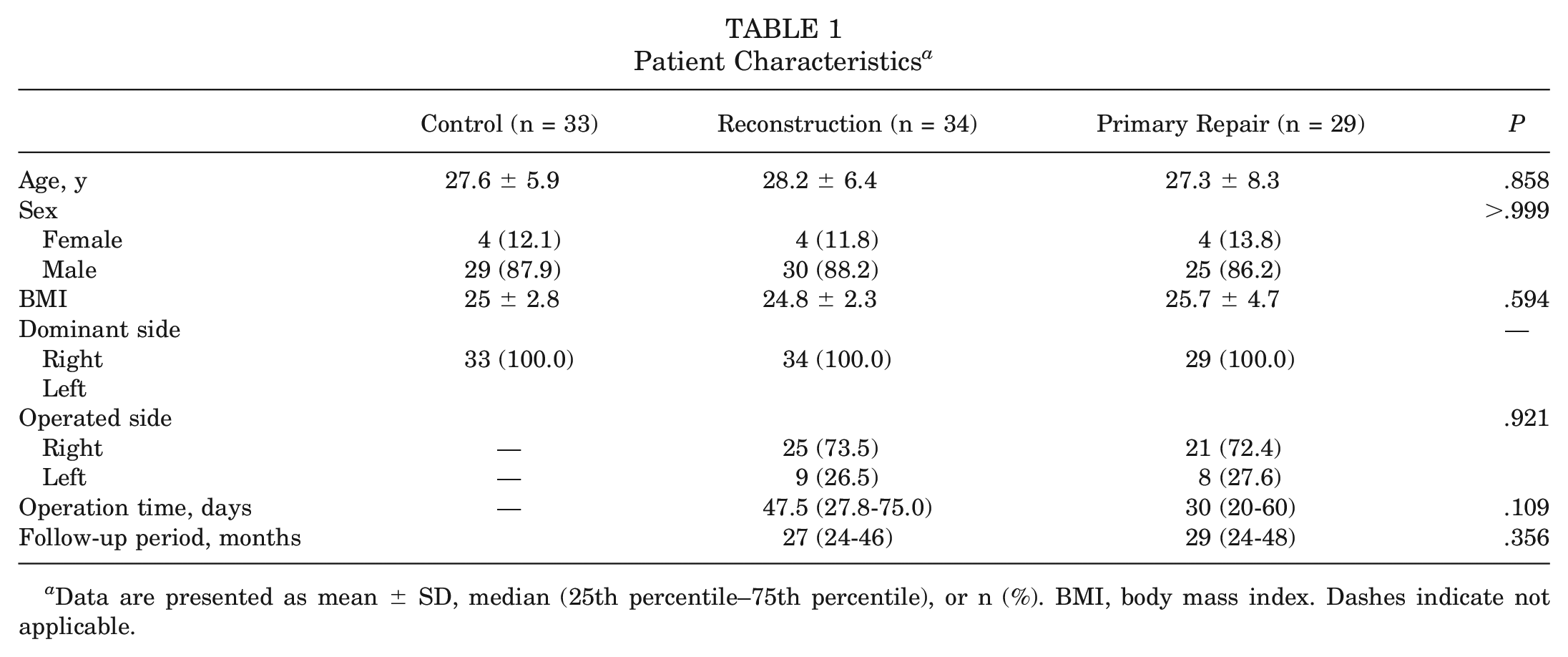
Data are presented as mean ± SD, median (25th percentile–75th percentile), or n (%). BMI, body mass index. Dashes indicate not applicable.
Surgical Technique
Reconstruction and primary repair operations were performed by a single senior surgeon (U.K.) through the same approach. The patient was placed supine and a pneumatic thigh tourniquet was used. A 30° scope was inserted through standard anteromedial and anterolateral portals, diagnostic arthroscopy was performed, and the ACL was examined. After the procedures related to the concomitant pathologies were performed, those patients who met the criteria (proximal femoral avulsion tear and stump quality suitable for repair) underwent primary repair; otherwise, reconstruction using hamstring tendon autograft was performed for tears that did not meet these conditions.
Primary Repair
After the treatment of concomitant pathologies and the identification of the proximal avulsion injury of the ACL, the remaining stump quality was evaluated arthroscopically and it was decided to perform primary repair. After identification of the lesion, the femoral attachment site of the ACL was debrided and the femoral footprint was prepared for the suture anchor. Microfractures were made around the footprint to increase biological adhesion without disrupting the anchor's adhesion. Subsequently, a far anteromedial portal was opened for easier access to the femoral adhesion site and to make the anchor placement easier. A double-stranded biodegradable anchor (Smith & Nephew) was placed in the femoral footprint. After the first suture was passed through the proximal ACL once, with the help of a suture passer, the suture was stretched to the femoral footprint and the first knot was tied. Thus, the ACL was suspended to the femoral attachment site. The ligament was repaired by passing the second suture from proximal to distal and then from distal to proximal ≥4 times, and then the knot was tied and fixed. After intraoperative examination of the repaired ACL with the help of a probe and confirmation that the ACL was attached to the femoral adhesion point, ensuring its stability, the operation was concluded (Figure 2).
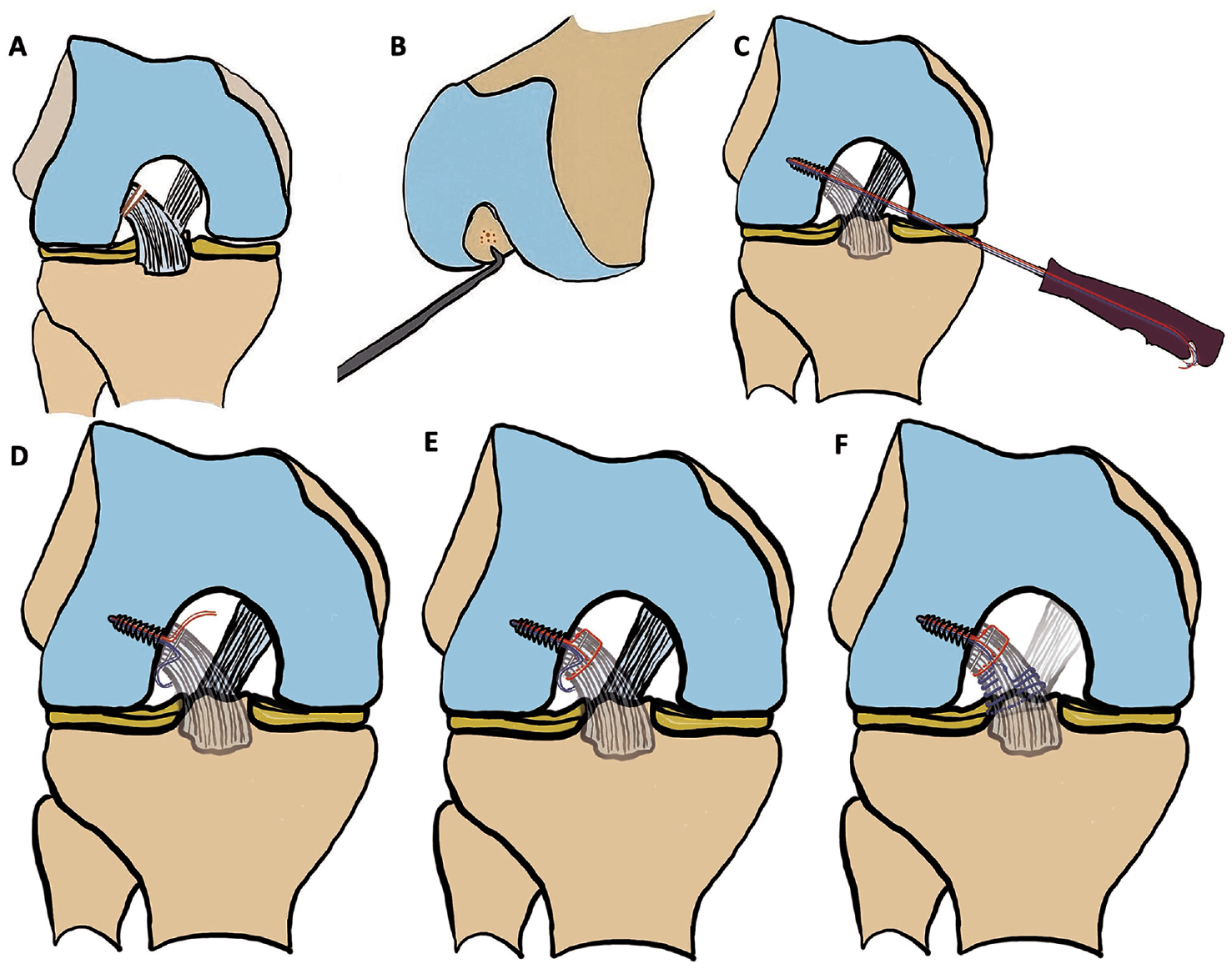
Illustration of the primary repair technique. (A) Proximal injury of the anterior cruciate ligament (ACL). (B) The femoral attachment site of ACL is debrided and microfractures are made surrounding the footprint. (C, D) A biodegradable anchor is placed in the femoral footprint. (E) The suture is used to pull the remaining ACL to the femoral footprint, and the first knot is tied. (F) A second suture is passed from proximal to distal and then from distal to proximal ≥4 times, and the knot is then tied and fixed.
Reconstruction
Reconstruction was performed in cases in which the tear type was not suitable for primary repair (nonproximal tears and poor stump quality). Hamstring autograft was used in all reconstruction operations. After preparation of the tunnels, the graft was fixed at the appropriate tension to the femur with the Ultrabutton system (Smith & Nephew) and to the tibia with biodegradable screws (Smith & Nephew), with the knee at 15° to 30° of flexion. After fixation, arthroscopic examination was performed to evaluate graft tension and graft compression during extension and the operation was concluded (Figure 3).
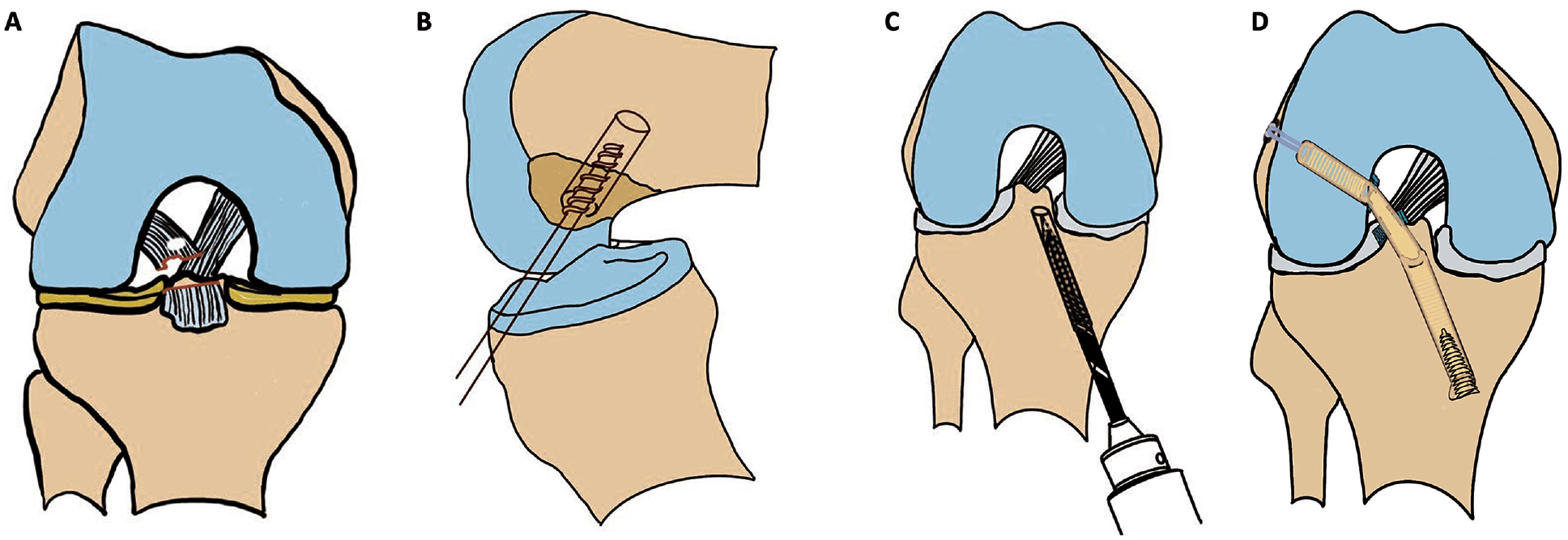
Illustration of the reconstruction technique. (A) Injury of the anterior cruciate ligament. (B) Preparation of the femoral tunnel. (C) Preparation of the tibial tunnel. (D) Graft fixation to the femur with the Ultrabutton system and to the tibia using a biodegradable screw.
Postoperative Rehabilitation
Primary Repair
Postoperatively, the main goals were to control swelling and early range of motion. All patients were fitted with an adjustable angle knee brace locked at 0° for 4 weeks, and mobilization was allowed with double crutches without weightbearing. Straight-leg raises, isometric terminal knee extension, 0° to 30° of knee flexion, hip exercises, and passive range of motion exercises were started on the first day after the surgery. Partial weightbearing was started with crutches after 3 weeks postoperatively. After the sixth week, full weightbearing was allowed and gait training, open and closed kinetic chain exercises, balance, and proprioception exercises were initiated. Concentric and eccentric knee strengthening exercises were started at the 4-8 weeks. All exercises progressed gradually and continued until the sixth month. Unrestricted activities of daily living and return to sports were allowed after 6 months postoperatively when the patient reached full range of motion and strength.
Reconstruction
Postoperatively, the main goals were to control swelling and early range of motion. If there was no concomitant meniscal injury, the patient was allowed to bear weight as tolerated with crutches immediately after the surgery. Knee braces were not fitted to the patients. Crutches were discontinued 3 to 4 weeks after surgery. Controlled range of motion exercises, straight-leg raises, isometric terminal knee extension, and hip exercises were started on the first postoperative day. After 3 to 4 weeks, full weightbearing was allowed and gait training, open and closed kinetic chain exercises, balance, and proprioception exercises were initiated. Concentric and eccentric knee strengthening exercises were started at 4-8 weeks. All exercises progressed gradually and continued until the sixth month. Unrestricted activities of daily living and return to sports were allowed after 6 months postoperatively when the patient reached full range of motion and strength.
Clinical and Functional Evaluation
Patient data such as name, sex, age, dominant side, and operated side were recorded. The height and weight of the patients were measured by standardized methods using an adult scale (Seca 799 Adult Scale with Height Measurement; Seca), and BMI was calculated. The International Knee Documentation Committee (IKDC) subjective knee evaluation form, Lysholm knee scoring scale, and visual analog scale for pain were used to evaluate outcomes. Stability tests such as the anterior drawer, Lachman, and pivot-shift tests and anterior translation measurements with the KT-1000 arthrometer were performed.
In addition, proprioception was evaluated using the active joint position sensation method with a digital inclinometer (Dualer IQ; J Tech Medikal) to load weight on the affected limb between 24 and 48 months (mean, 29 months) postoperatively. In the assessment of proprioception as a dynamic position, weightbearing while standing on the affected extremity was selected. In the current study, a device and method previously validated for knee proprioception measurements were used. 29 Participants were positioned upright with 1 knee in extension and the other knee in 15° to 20° of flexion and their hands on their hips. Participants were instructed to pause for 10 seconds at the target angles of 15°, 30°, and 60° of knee flexion. The patients were then asked to flex the knee and stop at the aforementioned target angles. The difference between the target angle shown to the participants and the angle at which they brought their knees was calculated as the deviation angle. The deviations of the knee joint from the target angles of 15°, 30°, and 60° were recorded. Three repeated measurements were performed for each knee at each angle, and the mean deviation angles were calculated (Figure 4).

Proprioception assessment.
Statistical Analysis
Data distributions were summarized as number and percentage for categorical variables and mean ± SD or median (25th percentile–75th percentile) for continuous variables. The Pearson chi-square or Fisher exact test was used to analyze categorical data depending on the distribution of the data. The normality assumption of continuous variables was examined by the Shapiro-Wilk test and histogram graphs. For normally distributed continuous variables, comparisons between groups were made with 1-way analysis of variance or by using an independent-group t test. If the data were not normally distributed, the Kruskal-Wallis or Mann-Whitney U test was applied. The measurements of the intact knee and the operated knee were compared by a dependent-group t test or Wilcoxon signed-rank test. SPSS Version 25.0 (IBM Corp) was used for data analysis, and statistical tests were performed at the significance level of P < .05.
Results
In total, there were 63 patients, 34 of whom underwent reconstruction and 29, primary repairs. There were 33 healthy controls included (Figure 1).
Two patients were considered to have failed results (1 in the reconstruction group and 1 in the primary repair group. In the reconstruction group, 1 patient had a 3+ for the pivot-shift examination and 2+ for the Lachman and anterior drawer tests; the anterior translation difference relative to the intact side was measured as 5.33 mm with the KT-1000 arthrometer. Similarly, in the primary repair group, the pivot-shift, Lachman, and anterior drawer test results of 1 patient were also 2+ and the anterior translation difference relative to the intact side was measured as 6.42 mm. Thus, the failure rate was 3.45% in the primary repair group and 2.94% in the reconstruction group. The pivot-shift, Lachman, and anterior drawer tests were negative for the remaining patients in the reconstruction and primary repair groups, and the anterior translation difference in relation to the intact knee was <3 mm.
When proprioception was evaluated in the operated knee compared with the intact knee in the reconstruction group, the deviation angle was significantly larger in the operated knee at all target angles (P < .001). In the primary repair group, only the deviation angle at 15° was significantly larger in the operated knee than in the intact knee (P < .001), while no significant differences were found between the operated knee and the intact knee at 30° and 60° (P = .474 and P = .569) (Table 2).
Comparison of Absolute Angle Error in Healthy and Operated Knees as a Measure of Proprioceptive Sense in the Reconstruction and Primary Repair Groups a
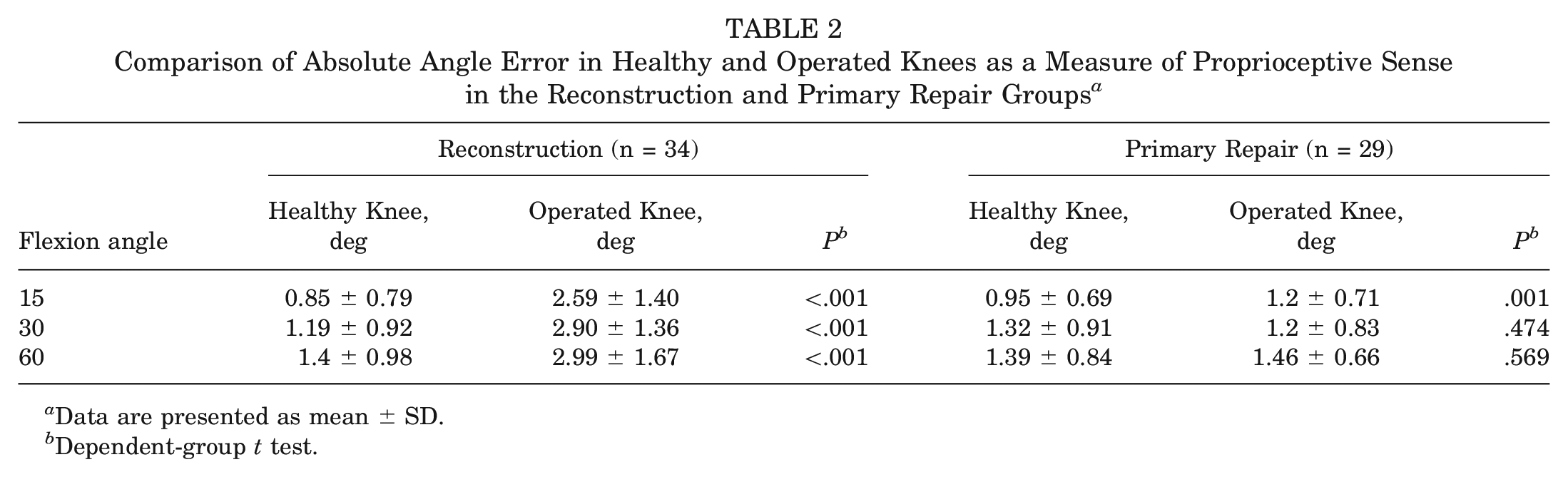
Data are presented as mean ± SD.
Dependent-group t test.
At 15° of flexion, the deviation angle for the healthy knee of the reconstruction and primary repair groups was significantly lower than that in the control group (P < .001), but there was no statistically significant difference between the groups in terms of deviation angle at 30° and 60°. The deviation angles of the operated knees were statistically significantly larger in the reconstruction group than in the primary repair group at all angles (P < .001) (Table 3).
Comparison of Sense of Proprioception Between the Groups a
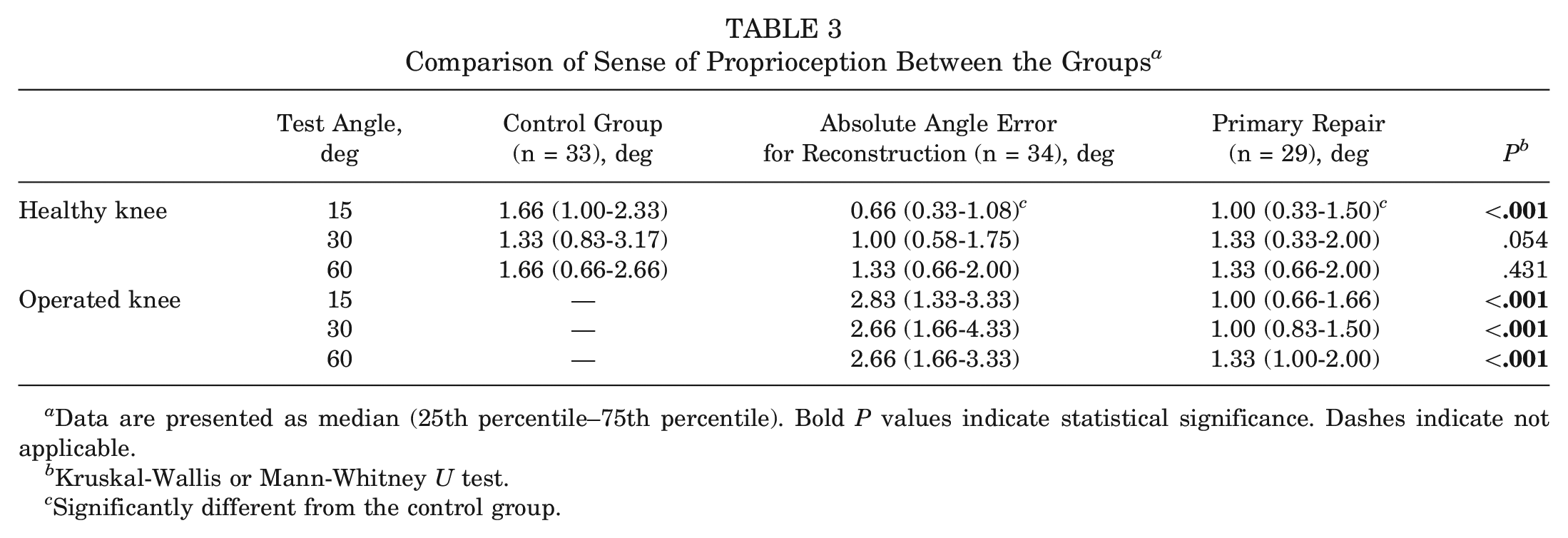
Data are presented as median (25th percentile–75th percentile). Bold P values indicate statistical significance. Dashes indicate not applicable.
Kruskal-Wallis or Mann-Whitney U test.
Significantly different from the control group.
There was no statistically significant difference between the reconstruction and primary repair groups in terms of clinical scores (Table 4).
Comparison of Clinical Scores Between Reconstruction and Primary Repair Groups a
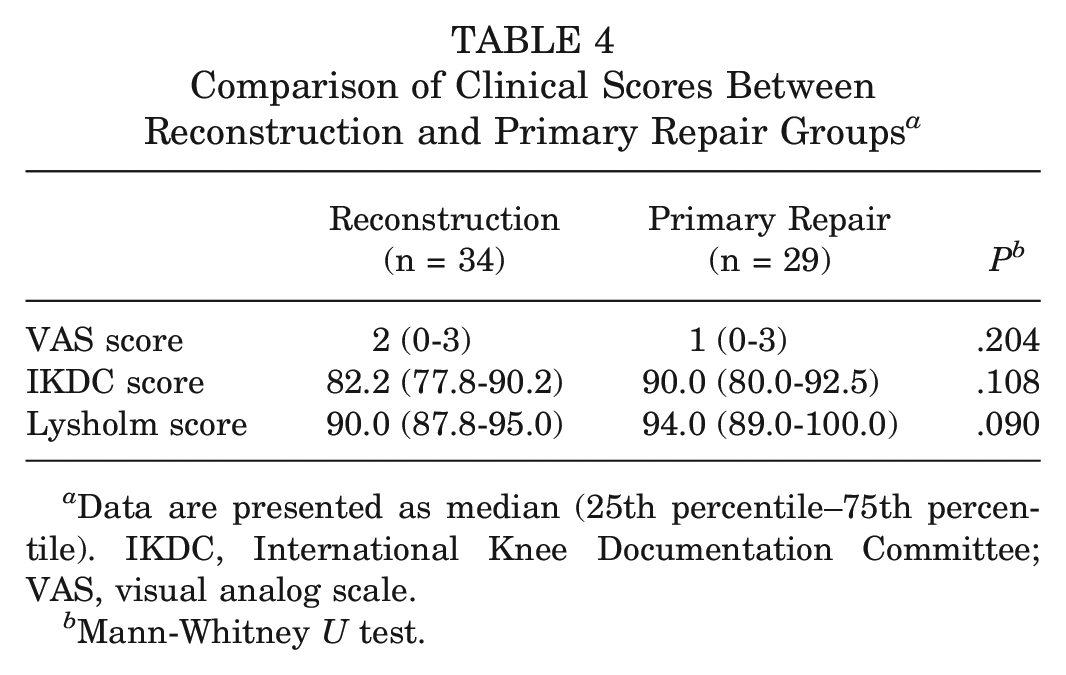
Data are presented as median (25th percentile–75th percentile). IKDC, International Knee Documentation Committee; VAS, visual analog scale.
Mann-Whitney U test.
There was no significant difference in KT-1000 arthrometer measurements between the reconstruction and primary repair groups (P = .208) (Table 5).
Comparison of KT-1000 Arthrometer Measurements Between the Reconstruction and Primary Repair Groups a
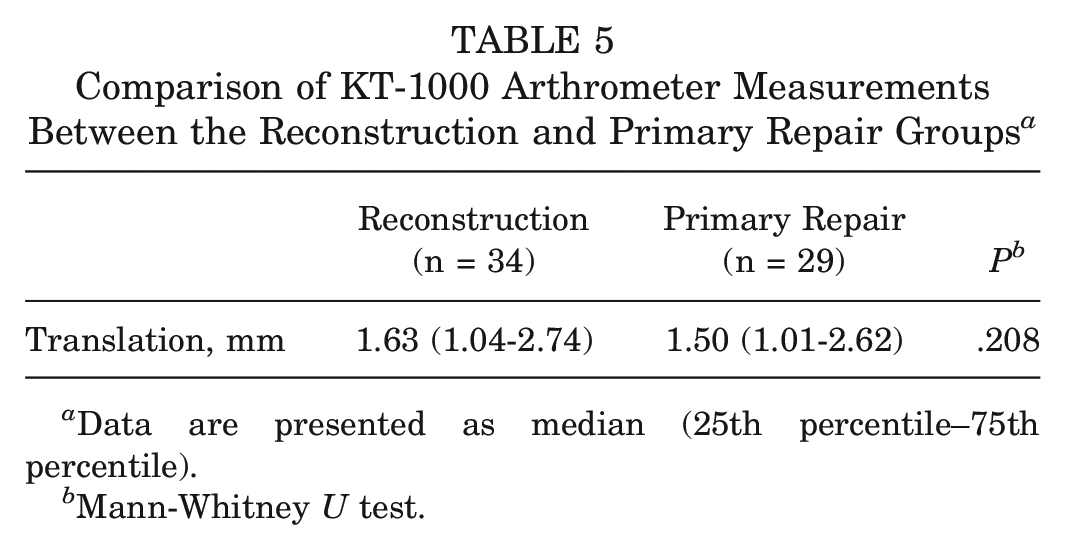
Data are presented as median (25th percentile–75th percentile).
Mann-Whitney U test.
Discussion
The most important result of the present study is the demonstration of normalization of proprioception in patients undergoing primary ACL repair. To our knowledge, this is the first study to evaluate the sense of proprioception in patients undergoing primary ACL repair. Additionally, at a median follow-up of 27 months, 28 of 29 patients (97%) who underwent primary repair achieved knee joint stability. Excellent subjective results were recorded with a median IKDC score of 90 (80-92.5) and Lysholm score of 94 (89-100). At the end of the study, proprioception sensation was found to be significantly better in patients who underwent primary repair than in patients who underwent reconstruction.
In the literature, many studies examining proprioception after ACLR have been carried out. Some studies have reported that knee proprioception sensation returns to normal after reconstruction.3,12,25,27 On the contrary, other studies support that proprioception sensation after reconstruction can never be the same as before the injury.7,8,20,22 A histologic study showed a lower concentration of neurofilament protein in the ACL grafts of patients who have undergone ACLR compared with the native ACL tissue, and this deficiency was present regardless of whether an allograft or an autograft was used. This finding explains the proprioceptive deficits that persist clinically after ACLR. 42 Because the restoration of proprioception after ACL injuries depends on the innervation of the ACL, stump preservation during ACL surgery may potentially benefit the patient. 11
The most important aspect of the current study was the comparison of primary repair and ACLR techniques in terms of proprioception, and it was shown that primary repair of the ACL is superior to ACLR in preserving knee proprioception sensation. Although there are studies showing that knee proprioception improved after ACLR, these studies have not made any comparison between reconstruction and healthy control groups. The most important difference of the current study from other available studies is the comparison of primary repair, reconstruction, and healthy control groups. The underlying factor for the success of primary repair is the synergistic effect of preservation of the native ACL tissue and the beginning of proprioceptive strengthening exercises in the postoperative period. Through this interplay, proprioception of the patients who underwent primary repair was similar to the results of the healthy control group. Because the natural ligamentous structure is preserved with primary repair, proprioception may also be preserved. In the primary repair group, at 15° of knee flexion the deviation angle in the operated knee was significantly higher than that in the healthy knee (P < .001). If both groups are examined carefully, it can be seen that the deviation angles also increased with increasing flexion angles. This may be because a flexion angle of 15° is the most commonly used position during standing and walking. Measured proprioceptive deficits exhibited by injured athletes may predispose the athlete to knee injury. In 1 study, it was observed that injuries were more common in female athletes, especially with deviation angles >2°. 43 In the same study, for each degree increase in angle error, a 2.9-fold increase in the odds ratio of knee injury was observed and a 3.3-fold increase in odds ratio of ligamentous/meniscal injury was observed. 43 In the current study, the deviation angles at 15°, 30°, and 60° were 2.83°, 2.66°, and 2.66° in the reconstruction group and 1.00°, 1.00°, and 1.33° in the primary repair group, respectively (the deviation angles between the primary repair group and the control group were almost similar). In light of this information, it can be inferred that primary repair, in line with the literature, can minimize the risk of reinjury.
There are augmented and nonaugmented methods available for primary ACL repair. In the nonaugmented method, the avulsed ACL is arthroscopically fixed to the femoral footprint at the femoral attachment site with suture anchors.1,6,9,10,14 In augmented methods, internal bracing 13 and dynamic intraligamentary stabilization can be used. 5 Augmentation mainly provides additional stability to the repaired ligament and preserves its healing during early mobilization, thus avoiding the need for immobilization in the postoperative period. In this study, because primary repair was performed without augmentation, the knee was immobilized in an angle-adjustable knee brace for 4 weeks to eliminate the risk of retear in the early period. Jonkergouw et al 16 compared primary ACL repairs performed with and without augmentation in patients with proximal ACL tears. There was no difference in short-term follow-up results and complication rates, reoperation rate, or patient-reported outcomes, and it was shown that the use of an additional internal brace with primary ACL repair did not provide any advantage. van der List et al 38 compared primary repair with a suture anchor without augmentation, primary repair with static augmentation, and primary repair with dynamic augmentation. They reported that there was no statistical difference in the failure rate for any of the groups, but the need for revision surgery for implant irritation was more frequent in the primary repair with dynamic augmentation group than in the primary repair with static augmentation group. Similar to this study, Achtnich et al 1 compared patients who underwent primary repair with a single-suture anchor with those who underwent reconstruction for a proximal ACL tear. They reported that no instability occurred in any patient in the reconstruction group, whereas 3 patients in the primary repair group had recurrent instability, but they stated that this failure was because of noncompliance with the rehabilitation protocol. In another study, DiFelice et al 10 reported the early results of ACL primary repair with suture anchor without augmentation. Good clinical results were obtained in 10 of 11 patients with ≥2 years of follow-up. Only 1 patient had a 6-mm difference in the KT-1000 translation measurement, and this failure was not related to a technical error but rather to a new knee injury that occurred 3 months after surgery.
In the primary repair technique with suture anchors, 2 suture anchors10,16 or 1 suture anchor1,14 can be used. In the current study, primary ACL repair was performed using 1 biodegradable suture anchor without augmentation. In studies using 2 suture anchors, a single suture on each anchor was used and tied, but in the primary repair method of our study, both sutures on the double-strand suture anchor were used. In addition, better stability was achieved by descending to the distal part of the ACL first and then ascending to the proximal part to tie the second knot in a braided manner. In this study, adequate stability and good clinical results were obtained with the use of a nonaugmented primary repair method. Furthermore, the nonreinforced technique is less invasive than reinforced techniques and does not require drilling new tunnels into the bones.
Another important factor determining the repairability of an ACL tear is the amount of time that has passed between the tear and surgery. In an animal study, it was reported that when the interval between the tear and repair exceeded 2 weeks, retraction and scar formation in the ACL prevented repair with appropriate tension and it was biomechanically more unstable. 23 van der List et al 36 concluded that if the interval between ACL tear and repair is <4 weeks, the repairability of the ACL is significantly higher. Vermeijden et al 40 compared primary repairs performed in acute and chronic cases; they reported similar clinical results in short- and midterm follow-ups between the acute and chronic cases. Our current study has also put forth that ACL injuries operated on with the primary repair method in the first 12 weeks can have very good functional and clinical results.
The limitations of this study include its retrospective design, although the data were collected prospectively; the relatively limited number of patients because this method can only be applied to a certain patient population; and the lack of preoperative functional scores and measurements. In addition, the reliability of the proprioception measurements was not tested, and the results were short term. In the current study, only static proprioception was tested, and the level and durability of return to sports were not documented. Another limitation of this study was the division of the patients operated on for ACL tears into 2 groups, but the tear types in these 2 groups were not the same (proximal tears - midsubstance tears). However, there are no data in the literature in which different tear types have had an effect on clinical outcomes.
Conclusion
Primary repair of the ACL has successful results in a well-selected patient group. In the short term, primary repair of the ACL in patients with proximal femoral avulsion tears and a stump quality suitable for repair produces successful results because it is clinically, functionally, and proprioceptively protective.
Footnotes
Submitted June 27, 2023; accepted December 14, 2023.
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.