
Abstract
Background:
There is ongoing debate about the best way to manage ramp lesions at the time of anterior cruciate ligament (ACL) reconstruction (ACLR). Type 3 lesions are not visible by the transnotch approach without superior debridement, making the management debate even more problematic.
Purpose/Hypothesis:
The purpose of this study was to evaluate the rate of secondary surgical interventions according to the management method of a type 3 ramp lesion concomitant with primary ACLR. The hypothesis was that the rate of secondary ACL or meniscal interventions would be higher in patients who underwent all-inside repair.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
A retrospective analysis of all patients who underwent primary ACLR with a type 3 ramp lesion between January 2012 and May 2020, regardless of the treatment method, was performed. The main criterion analyzed in this cohort was a secondary surgical intervention, defined as revision ACLR or a reintervention of the repaired meniscus. A survivorship analysis was performed to evaluate secondary surgical interventions in 3 groups: all-inside repair, suture hook repair, and left in situ. The following data were collected preoperatively and at the last follow-up: patient characteristics, time to surgery, side-to-side difference in laxity, pivot shift, Lysholm score, subjective International Knee Documentation Committee score, Knee injury and Osteoarthritis Outcome Score, Tegner score, and meniscal repair failure rate.
Results:
A total of 113 patients who underwent type 3 ramp lesion repair concomitant with ACLR were included: 52 (46.0%) in the all-inside repair group, 23 (20.4%) in the suture hook repair group, and 38 (33.6%) in the lesion left in situ group. There were 17 patients (15.0%) who underwent a secondary intervention because of ACL graft failure (n = 6) or meniscal repair failure (n = 15 [4 of whom underwent a concomitant ACL reintervention]). Overall, 62 patients (54.9%) underwent combined ACLR and anterolateral ligament reconstruction, while 51 patients (45.1%) underwent isolated ACLR. In the adjusted Cox model, the type of meniscal repair was not statistically significantly associated with secondary surgical interventions. The only risk factor for secondary surgical interventions in this cohort was isolated ACLR (hazard ratio, 8.077; P = .007).
Conclusion:
The rates of secondary surgical interventions after medial meniscal type 3 ramp lesion repair concomitant with ACLR were similar regardless of the management method of the meniscal lesion. Despite not being associated with meniscal treatment, this rate was 8 times higher for patients who underwent isolated ACLR in this cohort; this is probably because of the protection that lateral extra-articular procedures provide to the ACL graft.
Concomitant anterior cruciate ligament (ACL) and peripheral injuries severely affect knee stability. Among them are longitudinal meniscocapsular lesions of the posterior horn of the medial meniscus, or ramp lesions, present in up to 39.5% of ACL ruptures. 5 Arthroscopic diagnosis using the transnotch approach is the gold standard for ramp lesions and allows them to be classified into 5 types. 20
Inferior partial lesions, described as type 3, are visible anteriorly and palpable with a suture hook but are not visible with the transnotch approach without superior debridement. 8 They are lesions of the meniscotibial ligament and are associated with significant mobility of the medial meniscus, thus contributing to knee instability. 3
Even though an increasing number of studies have shown interest in suturing ramp lesions,7,22 there is still no consensus for the treatment of type 3 injuries.2,4,11,23 They cannot be identified through isolated anterior arthroscopic visualization of the posterior horn of the medial meniscus, which is why they were recently called “hidden” lesions. 15 The partial nature of these lesions leads some surgeons to leave them in situ, hoping for spontaneous healing.1,23 Others prefer a suture hook technique, which requires debridement to be performed in the lesion's upper part to visualize the passage of the suture hook.15,20
Finally, an all-inside technique is also possible, but it does not provide a proper visualization of the capsular plane and the meniscotibial ligament. 9 No study has specifically evaluated the surgical management of type 3 injuries concomitant with ACL ruptures.
The primary objective of this study was to compare the rate of secondary meniscectomy after type 3 ramp lesion repair concomitant with primary ACL reconstruction (ACLR). The techniques used were all-inside repair, suture hook repair via a posteromedial approach, or leaving the lesion in situ. Secondary objectives were to evaluate functional scores and return to sport, as well as the rate of ACL graft ruptures, according to the technique of medial meniscal repair. The hypothesis was that the rate of secondary meniscectomy would be higher in patients who underwent all-inside repair than in patients who underwent suture hook repair or in whom the lesion was left in situ.
Methods
Institutional review board approval (COS-RGDS-2023-05-001-THAUNAT-M) was granted for this retrospective cohort study. A retrospective analysis of prospectively collected data was performed. All patients with a type 3 ramp lesion who underwent primary ACLR between January 2012 and May 2020 by 2 senior surgeons (J.M.F, M.T.), regardless of the treatment method, and with a minimum follow-up of 2 years were eligible for this study. Patients who underwent major concomitant procedures, including multiligament reconstruction or osteotomy, were excluded from the analysis.
Some patients underwent combined ACLR and anterolateral ligament (ALL) reconstruction based on risk factors for an ACL graft rupture. Indications for combined reconstruction included young patients playing pivot sports, chronic instability, explosive rotatory protrusion, and significant anteroposterior laxity.
Surgical Technique
Patients were placed in the supine position with 90° of knee flexion, lateral support, distal support, and a tourniquet at the proximal half of the thigh. Arthroscopic exploration and eventual meniscal repair were performed before ACLR. The medial meniscus was palpated with an arthroscopic hook from the anterior portal to confirm instability or an inferior fissure. Then, posteromedial exploration by the transnotch approach was systematically performed, allowing the classification of longitudinal meniscocapsular lesions of the posterior horn of the medial meniscus. 20 For the transnotch approach, the arthroscope was passed through the space at the edge of the condyle while a valgus force was first applied in extension and then in flexion, 20 and no pie-crusting of the medial collateral ligament was ever necessary to gain access to the posteromedial compartment. Classification was performed retrospectively based on data in the operative report for patients who underwent surgery before 2016. The meniscal repair technique was determined according to the surgeons’ preferences, which have evolved during their practice. Before the posteromedial portal started to be used at the end of 2012, type 3 lesions were treated nonoperatively or with an all-inside implant. With the advent of exploration through the posteromedial portal, the technique has evolved with the addition of a suture hook.
All-inside Repair
First, the lesion was debrided with a shaver through the anteromedial approach and then repaired with 1 to 3 vertical sutures using an all-inside meniscal repair system (Ultra Fast-Fix; Smith & Nephew).
Suture Hook Repair
The arthroscope was introduced into the posteromedial compartment via the transnotch approach. Then, a posteromedial portal was created under arthroscopic control. 20 The shaver was introduced through the posteromedial portal for debridement of the lesion in the upper part of the meniscocapsular area. Repair was performed using a right suture hook (QuickPass Lasso; Arthrex) for the left knee and a left suture hook for the right knee, loaded with a monofilament absorbable suture (PDS 0; Ethicon). Overall, 1 to 3 sutures were used depending on the longitudinal extent of the lesion. Finally, the stability of the repaired meniscus was examined using a probe via the anterior approach.
Lesions Left In Situ
After the lesion had been diagnosed by anterior probing and verified as a type 3 lesion by the transnotch approach, it was simply debrided by anterior shaving of the inferior portion of the meniscus, without any associated repair.
ACLR Technique
ACLR was performed either with hamstring tendon grafts (isolated or combined with ALL reconstruction) 13 or bone–patellar tendon–bone grafts with a press-fit technique. 10
Rehabilitation Protocol
All patients followed the same postoperative rehabilitation protocol, regardless of the ACLR technique or management method of the medial meniscal lesion. The protocol included full weightbearing with the aid of crutches for 2 weeks, progressive recovery of joint mobility from 0° to 90° for the first 6 weeks, and early quadriceps activation exercises. The resumption of nonpivot sports was allowed at 3 months, noncontact pivot sports at 6 months, and contact pivot sports and competitions at 9 months.
Data Collection
All patients were followed up by the surgical team or a sports medicine physician at 3 and 6 weeks and at 3, 6, 12, and 24 months. All patient reports were reviewed to collect information on possible revision surgical procedures or residual pain. The study endpoint was determined to be May 1, 2022. All patients were contacted by email or telephone by one of the investigators at the last follow-up. The questionnaires included queries about any reoperations performed at another center, possible imaging or management of their knee performed at another center, and patient-reported outcome measure scores: Tegner activity scale, subjective International Knee Documentation Committee score, Knee injury and Osteoarthritis Outcome Score, and Anterior Cruciate Ligament–Return to Sport after Injury scale.
Statistical Analysis
Descriptive data analysis was conducted depending on the nature of the considered criteria. For qualitative data, this included the numbers of available and missing data as well as, for each technique, the frequency and percentage (referring to available data). Proportions were estimated with their exact 95% CIs when appropriate. For quantitative data, this included the numbers of available and missing data as well as the mean, standard deviation, range, median, and interquartile range. Comparisons of data between the 3 groups were made using the chi-square test or 1-way analysis of variance, depending on the nature of the variable. The risks of the occurrence of events were described in terms of the probability of the occurrence and 95% CI using the Kaplan-Meier method.
The date of origin was the date of surgery, and the time to the event was the duration between the date of failure or last follow-up date and the date of surgery. For the occurrence of meniscal repair failure, a survival analysis was performed using a Cox proportional hazards model, taking into account different adjustment factors: treatment group (all-inside/left in situ/suture hook), age at surgery (<20 years/≥20 years), side-to-side difference in laxity (≤7 mm/>7 mm), and ACLR technique (combined ACLR with hamstring tendon graft + ALL reconstruction/isolated ACLR). A check of the proportional hazards assumption for the factors selected was performed (assessment of the time to selected factor interaction and plots of the log of negative log of estimated survivor functions versus the log of time).
All calculations were made with SAS for Windows (Version 9.4; SAS Institute).
Results
Patient Characteristics
A total of 5132 patients underwent primary ACLR during the study eligibility period, and 1034 patients had a concomitant ramp lesion and an ACL injury. Of these, a type 3 ramp lesion was identified in 113 patients (Figure 1). Preoperative clinical characteristics were similar between the 3 groups. The meniscal lesion was neither symptomatic nor visible on magnetic resonance imaging in 25.4% of patients. One of the surgeons (M.T.) performed all-inside repair in 56.5% (39/69) of the cases, suture hook repair in 33.3% (23/69) of the cases, and simple debridement in 10.15% (7/69) of the cases, whereas the other surgeon (J.M.F.) performed all-inside repair in 29.54% (13/44) of the cases, simple debridement in 70.45% (31/44) of the cases, and suture hook repair in 0.0% of the cases (Table 1). At a mean follow-up of months, 9 patients (8.0%) were lost to follow-up. Intraoperative data are presented in Table 2.
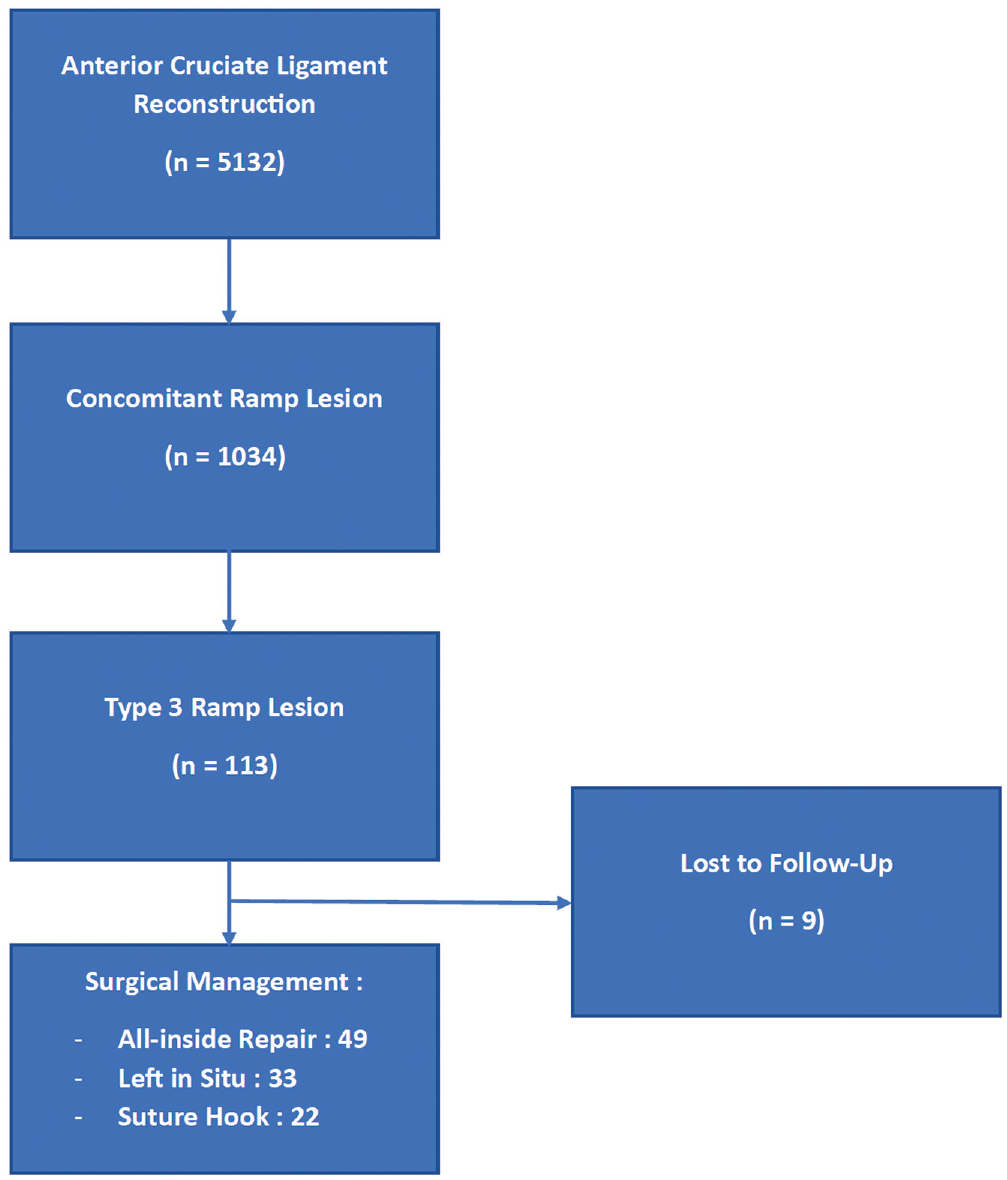
Study flowchart.
Preoperative Characteristics of Patients a
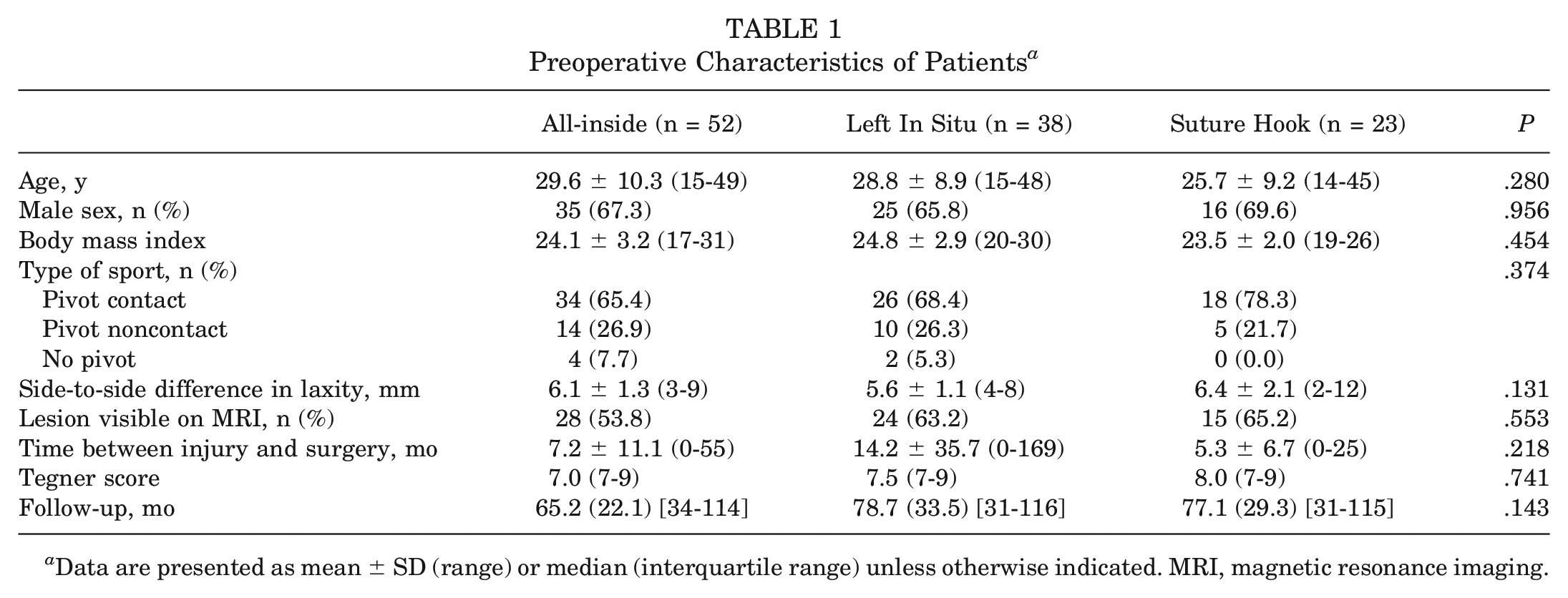
Data are presented as mean ± SD (range) or median (interquartile range) unless otherwise indicated. MRI, magnetic resonance imaging.
Intraoperative Characteristics of Patients a
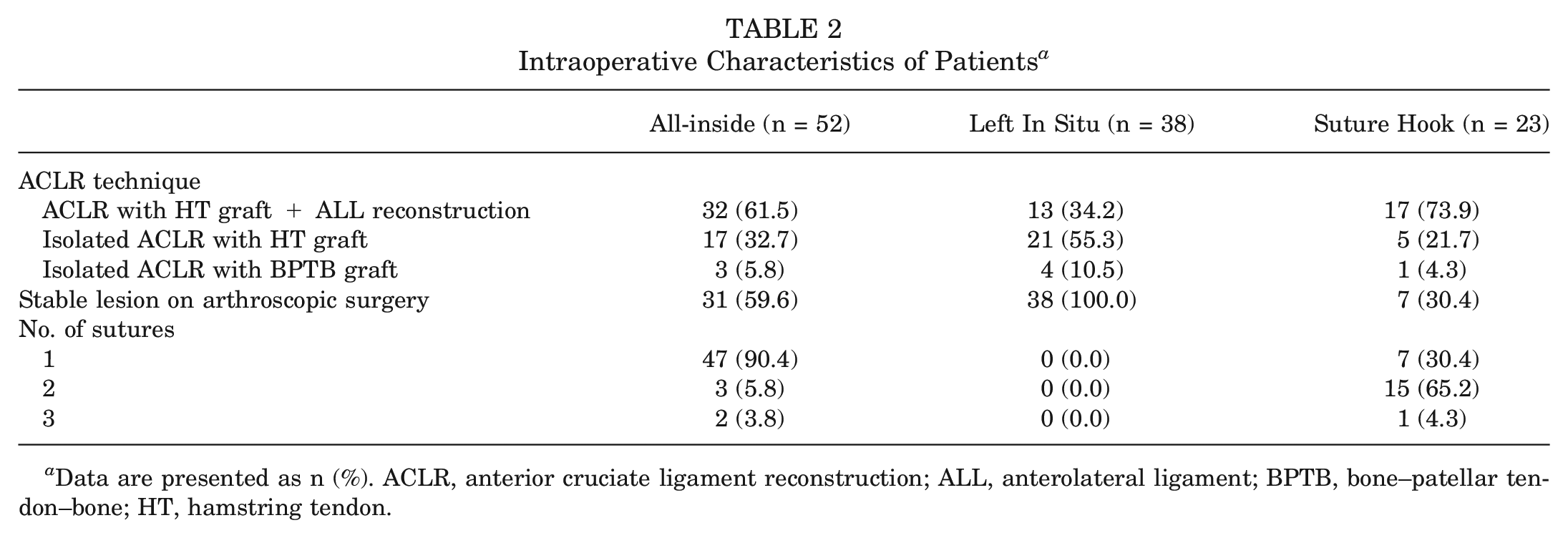
Data are presented as n (%). ACLR, anterior cruciate ligament reconstruction; ALL, anterolateral ligament; BPTB, bone–patellar tendon–bone; HT, hamstring tendon.
Secondary Meniscectomy
During the follow-up period, a medial meniscal lesion was found in 19 patients (18.26%). Table 3 shows the secondary meniscectomy rates stratified by type of treatment. The rate of secondary meniscectomy was higher in patients with a preoperative side-to-side difference in laxity >7 mm, (41.7% vs 14.9%, P = 0.044). The rate of secondary meniscectomy associated with ACL graft failure was 3.8% (4/104), which refers to 33.3% of the cases of secondary meniscectomy in the left in situ group (1/3), 50% in the suture hook group (3/6), and 0 in the all-inside group (0/10).
Rates of Secondary Meniscectomy a
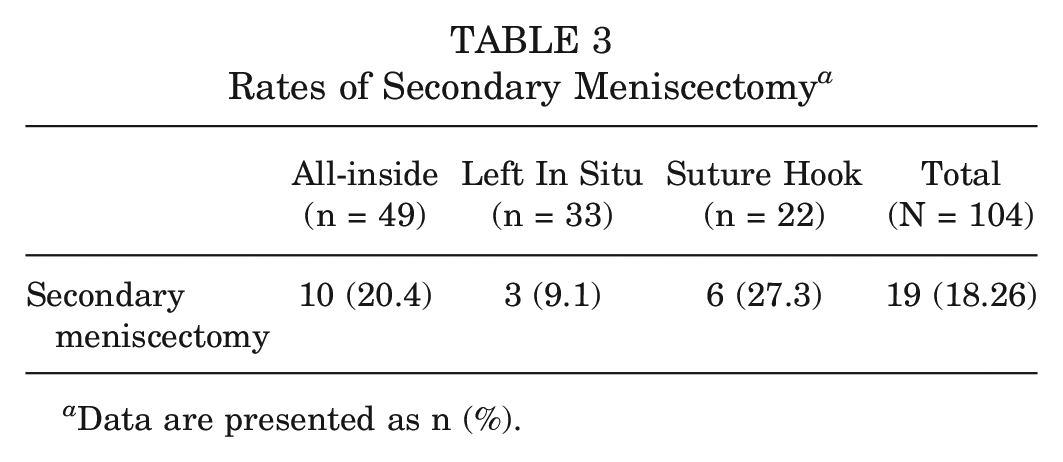
Data are presented as n (%).
Secondary Intervention
There were 17 patients (16.3%) who underwent a secondary intervention because of ACL graft failure (n = 6) or meniscal repair failure (n = 15 [4 of whom underwent a concomitant ACL reintervention]). The type of medial meniscal treatment was not statistically significantly associated with the occurrence of a secondary intervention in the adjusted Cox model. However, the risk of a secondary intervention was 7.850 (95% CI, 1.720-35.827) times higher in patients who underwent isolated ACLR (P = .008) compared with ACLR + ALL reconstruction (Table 4).
Cox Proportional Hazards Model for Risk of Secondary ACL or Meniscal Surgery a
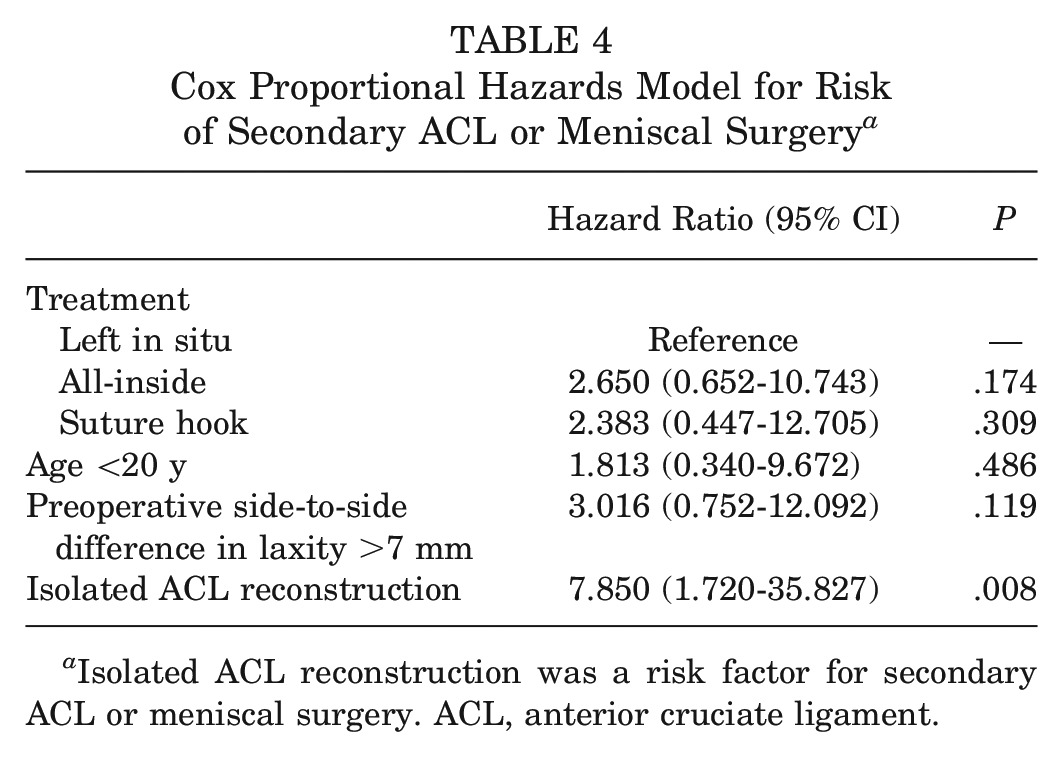
Isolated ACL reconstruction was a risk factor for secondary ACL or meniscal surgery. ACL, anterior cruciate ligament.
The log-rank test showed no statistically significant difference between the Kaplan-Meier survivorship curves (P = .6835) (Figure 2). In addition, a logistic regression analysis was carried out to assess the association between type 3 ramp lesions left in situ and ACL graft failure, finding no association between these variables (P = .931; odds ratio, 1.08 [95% CI, 0.188-6.218]; SE, 0.96).
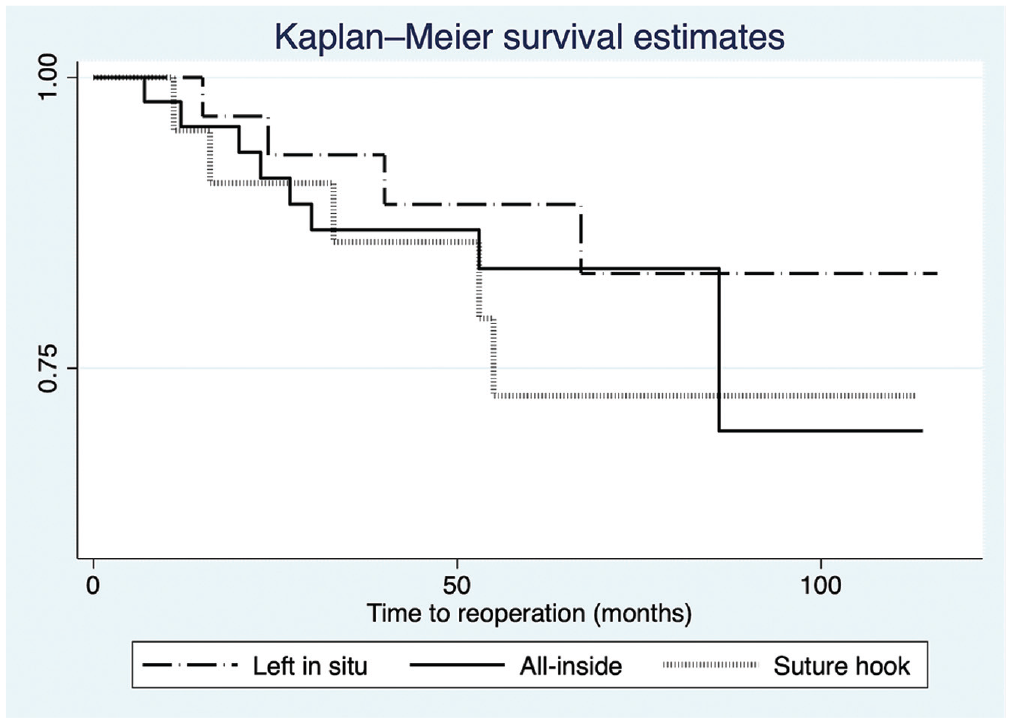
Kaplan-Meier survivorship curves stratified by type of management of type 3 ramp lesions.
Complications
At a mean follow-up of 72 months, 28 patients (28/104 [26.9%]) had ≥1 complication. An ACL graft rupture occurred in 1 patient (1/49 [2.0%]) in the all-inside repair group, 2 patients (2/33 [6.1%]) in the left in situ group, and 3 patients (3/22 [13.6%]) in the suture hook repair group, with no significant difference (P = .095) (Table 5).
Complications by Type of Meniscal Treament a
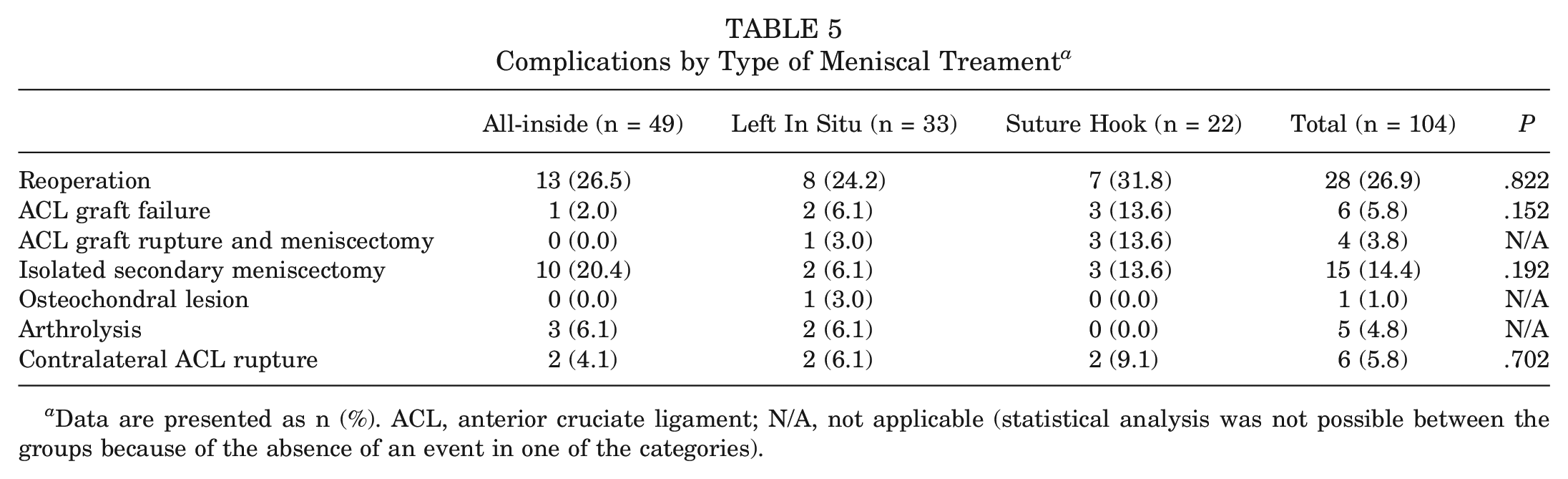
Data are presented as n (%). ACL, anterior cruciate ligament; N/A, not applicable (statistical analysis was not possible between the groups because of the absence of an event in one of the categories).
Functional Outcomes
A total of 73 patients (73/104 [70.2%]) reported having pain in the medial compartment at some level. The return-to-sport rate, the level of return to sport, and the functional scores (subjective International Knee Documentation Committee, Tegner, Knee injury and Osteoarthritis Outcome Score, Lysholm, ACL-Return to Sport after Injury scale) were comparable among groups (Table 6).
Functional Outcomes by Type of Meniscal Treatment a
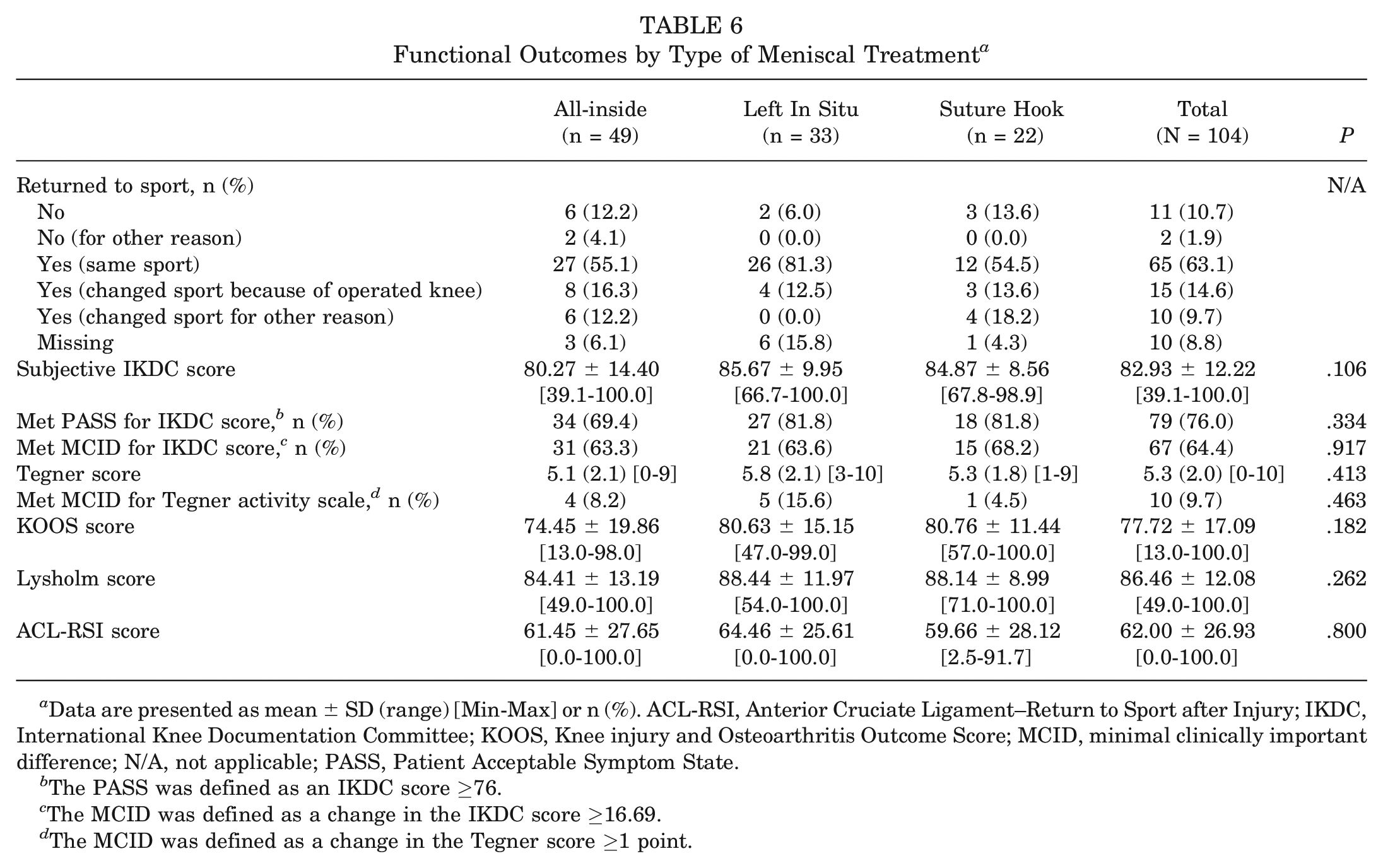
Data are presented as mean ± SD (range) [Min-Max] or n (%). ACL-RSI, Anterior Cruciate Ligament–Return to Sport after Injury; IKDC, International Knee Documentation Committee; KOOS, Knee injury and Osteoarthritis Outcome Score; MCID, minimal clinically important difference; N/A, not applicable; PASS, Patient Acceptable Symptom State.
The PASS was defined as an IKDC score ≥76.
The MCID was defined as a change in the IKDC score ≥16.69.
The MCID was defined as a change in the Tegner score ≥1 point.
Discussion
The main finding of this study is that the rate of secondary surgical interventions after type 3 ramp lesion repair concomitant with primary ACLR was not significantly different after suture hook repair, all-inside repair, or lesions left in situ. Although there was a lower percentage of combined ACLR + ALL reconstruction cases in the left in situ group, this was adjusted in the Cox model, and the only risk factor for reinterventions was isolated ACLR, without lateral extra-articular procedures, which was mainly associated with ACL graft failure, as has been demonstrated numerous times in the literature.13,17,18
The secondary meniscectomy rate was 18.26%, and despite the fact that we had more stable lesions in the left in situ group, there was no significant difference according to the technique used. The rate of secondary meniscectomy after meniscal repair was 13.3% in a recent meta-analysis. 14 Our rates of secondary meniscectomy in the subgroups are slightly different from the literature, more specifically, regarding a study comparing ramp lesion repair of all types found a failure rate of 21.1% with an all-inside suture and 4.3% with a suture hook using the posteromedial approach. 21
To the best of our knowledge, this is the first study to specifically examine type 3 ramp lesions: that is, partial inferior capsulomeniscal injuries. A cadaveric study showed the existence of the meniscotibial ligament, inserted from the posteroinferior aspect of the medial meniscus to the tibia, 3 which would be involved in type 3 injuries. However, in the present study, the suture hook technique used to suture this ligament did not reduce the failure rate compared with the all-inside technique or lesions left in situ at a minimum 2-year follow-up. This could be explained by the partial nature of these lesions, allowing stability and spontaneous healing. The stability of the ramp lesion seems to be an important element, as a prospective randomized study showed the same rate of meniscal healing at 2-year follow-up in 40 patients who had undergone meniscal repair and 33 patients who had lesions left in situ that were considered stable. 11 In a recent matched study on the failure rate of ramp lesions of all types, it was found that the all-inside group had twice as many failures as the suture hook group (31.2% vs 15.6%, respectively; P = .0003). 7
Moreover, suturing could be problematic because of the development of secondary radial lesions associated with the Tachibana effect, 19 described as the formation of new lesions anterior to the previous lesion due to the meniscal cleft created as a result of suture passage in a poorlylow vascularized zone of the meniscus. This may occur more often when an all-inside implant is used than a suture hook because of the size of the implant, the area of the penetration point of the needle/suture hook in meniscal tissue (Cooper zone 1 or 2), and the potential role of the nonabsorbable suture in the recurrence of the tear. All-inside devices might causebe exposed to a suture cut-through or cheese-wiring effect, 12 whereas this effect might be less present when performing suture hook repair with a resorbable suture, as suggested by Gousopoulos et al. 7 This difference between suturing with PDS absorbable sutures and all-inside repair with implants was also reported by El Helou et al, 6 who showed that the failure rate of patients who underwent bucket-handle medial meniscal tear repair with concomitant ACLR was 4 times higher with all-inside repair than with suture hook + outside-in repair. In our series, we had a greater rate of secondary meniscectomy in the suture hook group, compared to the all-side group, however, this can be explained by the fact that this represents the overall failure rate in patients who had a secondary meniscectomy at the same time as a failure of their graft (which represents half of the cases in the suture hook group). Our hypothesis is that these may actually be new lesions secondary to the new trauma (ACL graft failure) rather than a failure of the suture itself.
The treatment of stable ramp lesions is still a debated topic. Balazs et al 2 reported that nontreatment of stable ramp lesions, or lesions left in situ, does not degrade clinical outcomes in the setting of primary ACLR at a median follow-up of 2 years. Intraoperative assessments of ramp lesions relied on anterior inspection only, which represents bias, as 35% to 40% of ramp lesions can only be discovered by probing through a posteromedial portal, sometimes requiring minimal debridement with a motorized shaver.4,15
This study shows that leaving these lesions in situ did not expose patients to more reinterventions than if they had been repaired. This might be explained by the spontaneous healing potential of these types of lesions, which are partial-thickness tears. However, Tuphé et al 23 showed that the medial meniscal survival rate was 93% at 5 years and 71% at 20 years when a stable ramp lesion was left in situ. This highlights the need to observe these patients over the long term, as the fact that these lesions are not symptomatic at short-term follow-up does not warrant the conclusion that they will not recur or be the starting point of a bucket-handle tear in the long term.
The rate of secondary meniscectomy was higher in patients with a preoperative side-to-side difference in laxity >7 mm. This finding may be explained by the fact that the meniscus is less likely to heal in cases of persistent abnormal anteroposterior laxity. This risk factor has already been highlighted by Sonnery-Cottet et al. 16
The main limitations of this study include its retrospective nature and the inherent weaknesses of this design, including the potential for treatment selection bias and lack of a power analysis. Also, the mean follow-up time of 72 months is short, whereas a study that followed patients with stable partial ramp lesions over a period of 20 years showed that the majority of meniscal repair failures occurred between 96 and 120 months after ACLR. 23 The selection bias of stable lesions in the left in situ group is real but mitigated by the fact that there was no difference between the techniques in the multivariate analysis. Furthermore, indications and techniques for ACLR as well as different meniscal repair techniques have evolved over time and according to the preferences of the 2 surgeons. Lesions left in situ can be associated with the stability of these ramp lesions during arthroscopic surgery. This method was adopted mainly by 1 of the 2 surgeons; although this is subjective as an indication, it can be a source of selection bias. In addition, this is a retrospective study, with 8.0% (9/113) of patients lost to follow-up. Finally, our study lacks power because of the small sample size, which is correlated with the low frequency of this particular type of meniscal injury.
Conclusion
The rates of secondary surgical interventions after medial meniscal type 3 ramp lesion repair concomitant with ACLR were similar, regardless of the management method of the meniscal lesion. Despite not being associated with meniscal treatment, this rate was 8 times higher for patients who underwent isolated ACLR in this cohort; this is probably because of the protection that lateral extra-articular procedures provide to the ACL graft. Nontreatment of these hidden lesions may be a reliable management strategy, as it prevents failure because of exposure to the Tachibana and cheese-wiring effects. Further studies with long-term follow-up are needed to confirm these findings.
Footnotes
Submitted May 15, 2023; accepted December 14, 2023.
One or more of the authors has declared the following potential conflict of interest or source of funding: J.-M.F. is a consultant for Arthrex and Newclip Technics. M.T. is a consultant for Arthrex. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.