
Abstract
Background:
The glenoid track concept is used to determine preoperatively whether a Hill-Sachs defect is engaging or not. Currently, the glenoid track concept relies on measurements of bony structures as well as on the confines and elasticity of the rotator cuff as a reference point, which varies extensively among individuals and therefore limits the reliability and accuracy of this concept.
Purpose:
To evaluate the reliability of the global track concept, which determines the angular distance of the Hill-Sachs defect from the center of the articular surface of the humeral head as a new reference point with the help of an automated image analysis software and 3-dimensional analysis of the humeral head.
Study Design:
Controlled laboratory study.
Methods:
Computed tomography scans of 100 patients treated for anterior shoulder instability with different sizes of Hill-Sachs defects were evaluated manually by 2 orthopaedic surgeons independently using the software OsiriX as well as automatically by using a dedicated prototype software (ImFusion). Obtained manual and automated measurements included the Hill-Sachs length, Hill-Sachs width, and Hill-Sachs depth of the defect; the Hill-Sachs interval (HSI); and the glenoid width for the glenoid track concept, as well as the angular distance of the Hill-Sachs defect from the center of the articular surface of the humeral head (global track concept). The reliability of the different measurement techniques was compared by calculating intraclass correlation coefficients (ICCs).
Results:
There was a significant difference for all obtained parameters comparing manual and automatic measurements. For manually obtained parameters, measurements referring to bony boundaries (glenoid width, Hill-Sachs length, and Hill-Sachs width) showed good to excellent agreement (ICC, 0.86, 0.82, and 0.62, respectively), while measurements referring to soft tissue boundaries (HSI and glenoid track; ICC, 0.56 and 0.53, respectively) or not directly identifiable reference points (center of articular surface and global track) only showed fair reliability (ICC middle excursion, 0.42). When the same parameters were measured with the help of an automated software, good reliability for the glenoid track concept and excellent reliability for the global track concept in the middle excursion were achieved.
Conclusion:
The present study showed that the more complex global track measurements of humeral defects are more reliable than the current standard HSI and glenoid track measurements. However, this is only true when automated software is used to perform the measurements.
Clinical Relevance:
Future studies using the new proposed method in combination with an automated software need to be conducted to determine critical threshold values for defects prone to engagement.
Keywords
Humeral defects play a crucial role in recurrent anterior shoulder instability.3,7 Thus, the reliable identification of Hill-Sachs defects prone to engagement is important to plan adequate surgical treatment.7,9,12
Although many different measurement methods using a variety of different imaging modalities have been described in the literature, there is no current consensus on the accuracy of the available methods to make a precise imaging evaluation of the Hill-Sachs lesion or to predict its engagement before surgery.5,12 Di Giacomo et al 2 proposed the concept of glenoid track, classifying Hill-Sachs defects as “on-track” or “off-track,” whether the Hill-Sachs lesion is engaging or not. In this paradigm, calculations are completed using the measured size of the glenoid and Hill-Sachs interval (HSI) to calculate potential engagement. Although the clinical application of this concept showed that the glenoid track may be an accurate predictor of instability, 10 there are concerns that it is difficult to determine the location of the rotator cuff insertion using computed tomography (CT) and to delineate the medial margin of the Hill-Sachs lesion, which may lead to a high level of variability and poor interobserver reliability in the measurement of Hill-Sachs lesions, as shown previously. 8 Furthermore, a standardized CT image view for Hill-Sachs lesion measurement has not been confirmed compared with the widely accepted en face view of the glenoid. Additionally, the elasticity of the rotator cuff as a reference point, which varies extensively among individuals, may limit the reliability and accuracy of this concept. With the increasing complexity of the technique to measure humeral bone loss, manual performance of these measurements might also not be sufficiently reliable. A software that can be used to automatically segment and analyze humeral bony anatomy could potentially be more reliable in evaluating humeral bone loss compared with manual measurements, especially if applying a 3-dimensional (3D) measurement technique.
The aim of this study was therefore to establish a new method to measure Hill-Sachs lesions called the global track, which determines the angular distance of the Hill-Sachs defects from the center of the articular surface of the humeral head as a new reference point to eliminate the difficulty of localizing the rotator cuff insertion and constitutional differences in rotator cuff elasticity as a source of error. Furthermore, we hypothesized that the glenoid track concept has limited reliability regardless and that the global track concept would offer more reliable results when software is used in support to perform the measurements.
Methods
Patients
Our institutional radiology database was searched for patients with humeral bone loss due to recurrent anterior shoulder instability who received a thin-layer CT scan of the affected shoulder between January 2018 and December 2020. Inclusion criteria were a visible Hill-Sachs lesion and a slice thickness of 0.625 mm for 3D rendering. Patients who had a previous surgery on the affected shoulder or osteoarthritis grade ≥2 according to the Samilson and Prieto classification 4 on radiological imaging were excluded. A total of 100 CT scans were collected. All CT scans were obtained using a 64-slice CT scanner and uploaded as DICOM (Digital Imaging and Communications in Medicine) files to the analyzing software.
Measurement of CT Images
Measurements were independently conducted by 2 orthopaedic surgeons (K.K. and D.A.) using the image software OsiriX and the shoulder segmentation software ImFusion. Every rater performed the measurements once.
Within the manual measurements, first, the Hill-Sachs length (HSL) and Hill-Sachs width (HSW) of the lesion were calculated at their largest distances in the longitudinal and vertical directions. For this, the 3D model of the humeral head was adjusted to obtain an en face view of the Hill-Sachs lesion, and measurements were performed accordingly (Figure 1). The HSI was defined as the distance from the estimated rotator cuff attachment to the medial rim of the Hill-Sachs lesion corresponding to the HSW plus the intact bone bridge between the rotator cuff and Hill-Sachs lesion. 14 For calculating the glenoid track, the diameter of the best-fit circle placed on the en face view of the glenoid was measured, as well as the diameter of the defect, which was defined as the largest width along the best-fit circle diameter perpendicular to the defect border.2,6,11 If the HSI was >83% of the diameter of the glenoid diameter minus the defect length, the lesion was defined as off-track according to Di Giacomo et al. 2 Furthermore, the area of the best-fit circle as well as the defect area were obtained (Figure 1).
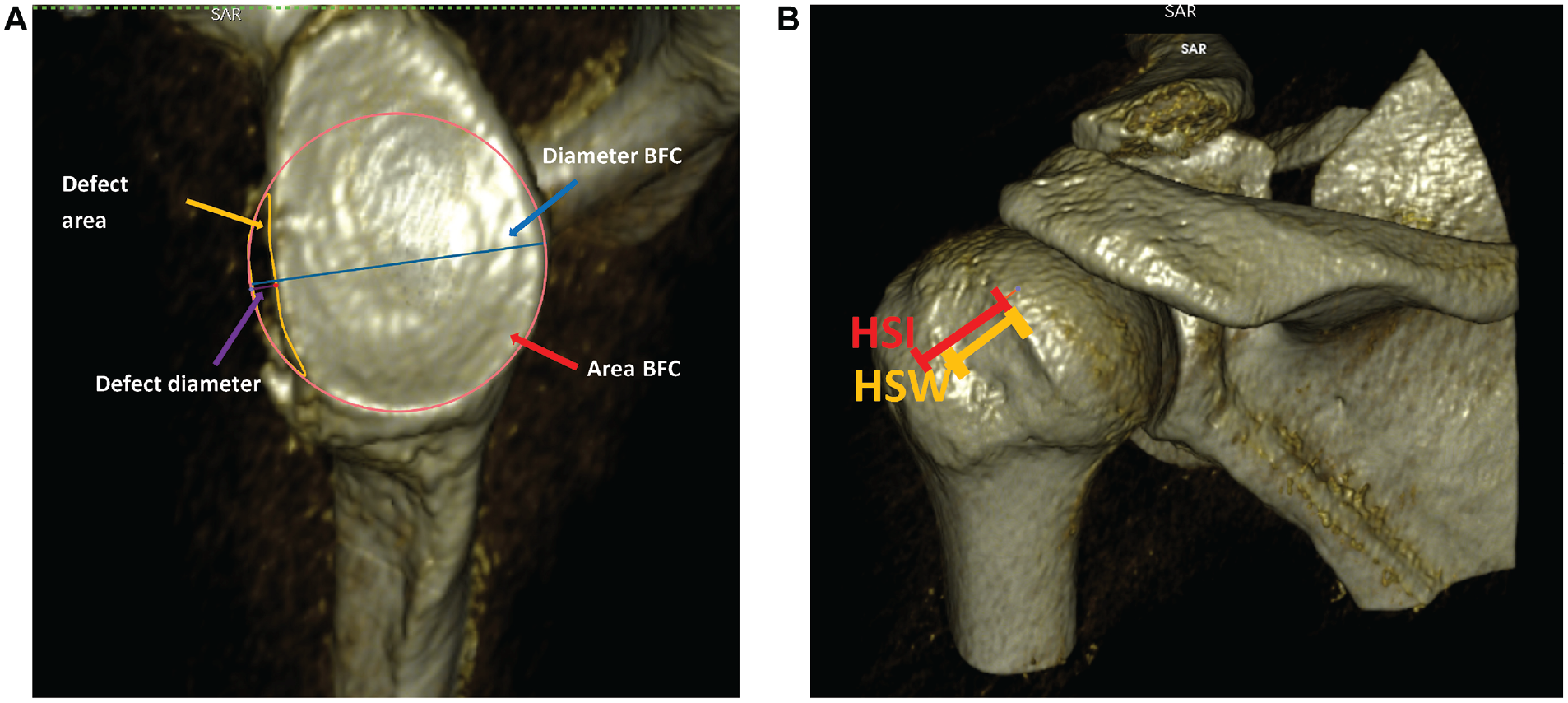
Manually obtained measurements using the image processing software OsiriX. (A) Measurements on the glenoid site including the area and diameter of the best-fit circle (BFC) placed on the en face view of the glenoid as well as the area and diameter of the bony defect. (B) Calculating the Hill-Sachs width (HSW) and Hill-Sachs interval (HSI) in a 3-dimensional model of the humeral head.
For the software-assisted measurements, the prototype of a shoulder segmentation software (ImFusion) was used. The same CT images that were used before (N = 100) were uploaded independently by the same 2 orthopaedic surgeons, and the software was used to automatically identify the humerus and scapula, which could be manually modified (Figure 2).
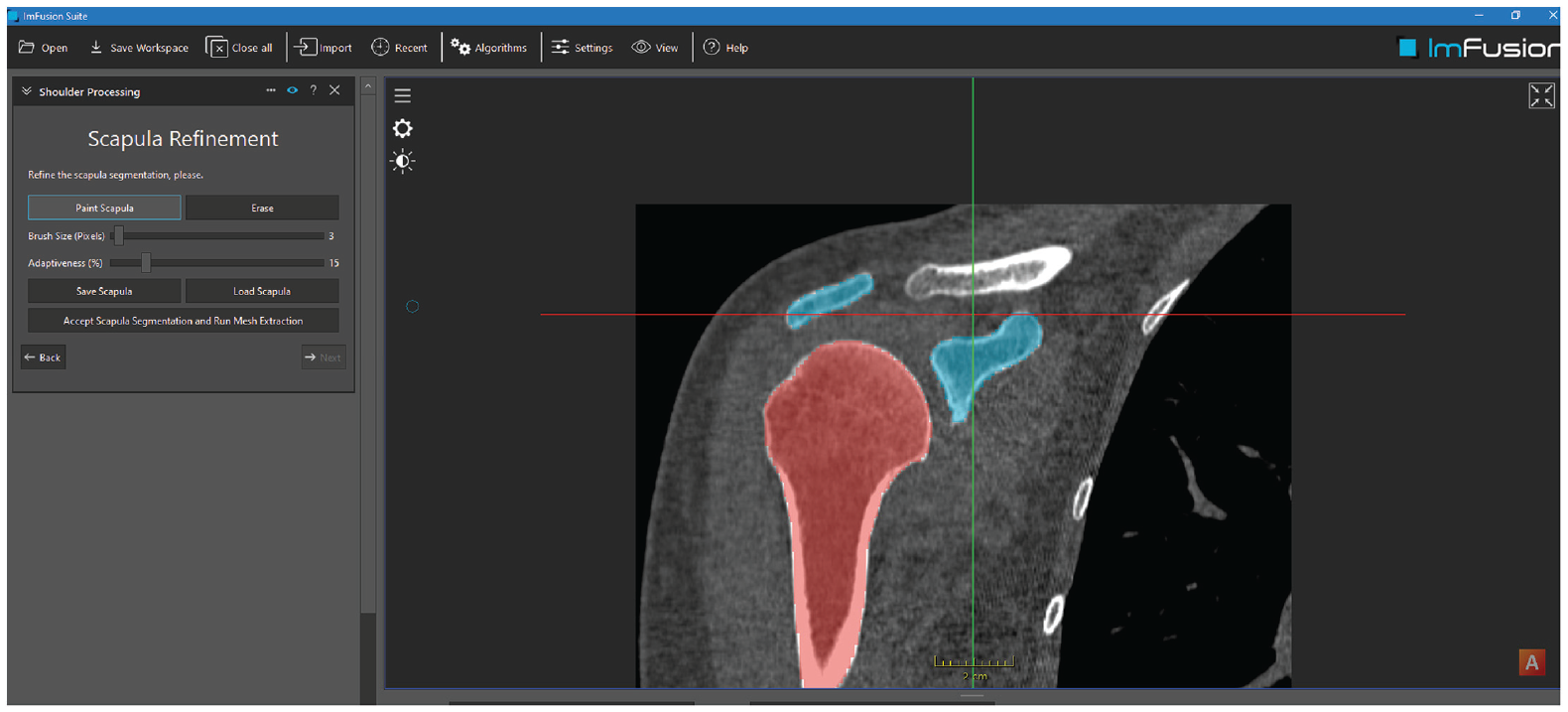
Computed tomography–based shoulder segmentation within coronary view. A segmentation of the humerus and scapula is conducted automatically using the software ImFusion.
After the glenoid surface was identified, the best-fit circle was placed on the en face view of the glenoid that could be modified manually in 3 dimensions, and the defect area and diameter were determined in the same manner as described before to obtain the glenoid track (Figure 3).2,6
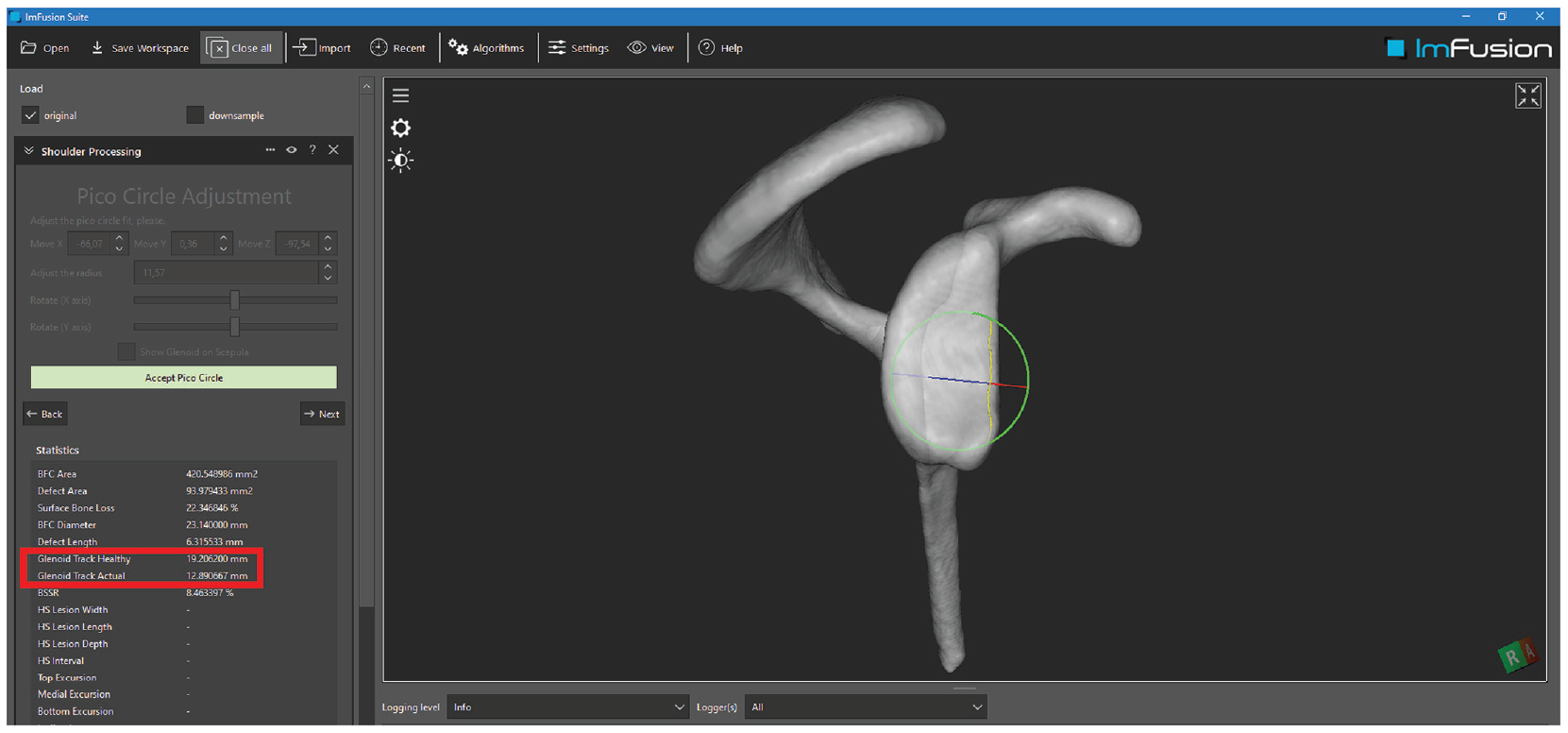
Automatic calculation of the glenoid defect length and area using the software ImFusion with automatic calculation of the glenoid track (glenoid track healthy = 83% of glenoid width; glenoid track actual = 83% of glenoid width minus defect length).
Then, the Hill-Sachs lesion was determined at the en face posterolateral view of the humeral head. The edges are easily visualized as the software displays different depths defined as distance to the center of the humeral head with different colors. The length, width, and depth of the lesion are calculated at their largest distances (Figure 4).
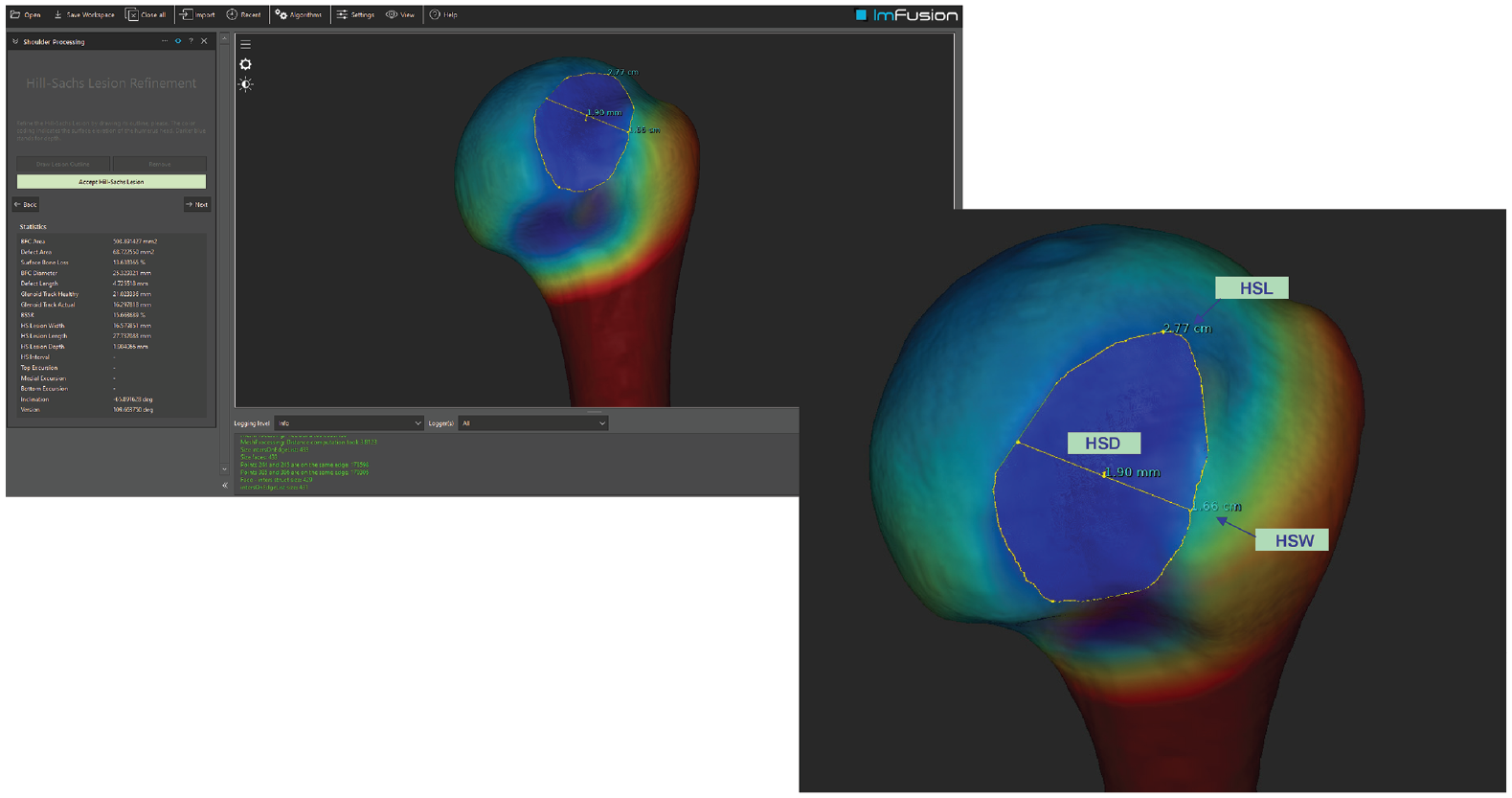
Automatic determination of the Hill-Sachs lesion using the software ImFusion. At the en face posterolateral view of the humeral head, the Hill-Sachs length (HSL), Hill-Sachs width (HSW), and Hill-Sachs depth (HSD) of the Hill-Sachs lesion are calculated at their largest distances.
Furthermore, using the manual determination of the rotator cuff insertion, the HSI can be calculated, and therefore whether the lesion is on- or off-track can be determined according to the glenoid track concept. 2
For determining the global track, the investigators marked the anatomic neck of the humeral head and used the software to calculate the top of the dome-shaped anatomic head of the humerus. Automated calculations of the angular distance between the top of the dome and the superior, middle, and inferior edges of the Hill-Sachs lesion were performed. All 3 distances were displayed in degrees (Figure 5). Manual measurements of the global track method involved multiplanar adjustment of the CT planes; best-fit circle placement on the humeral articular surface; and determination of the angle between the top of the articular surface, the center of the best-fit circle, and the superior, middle, and inferior edges of the Hill-Sachs lesion.
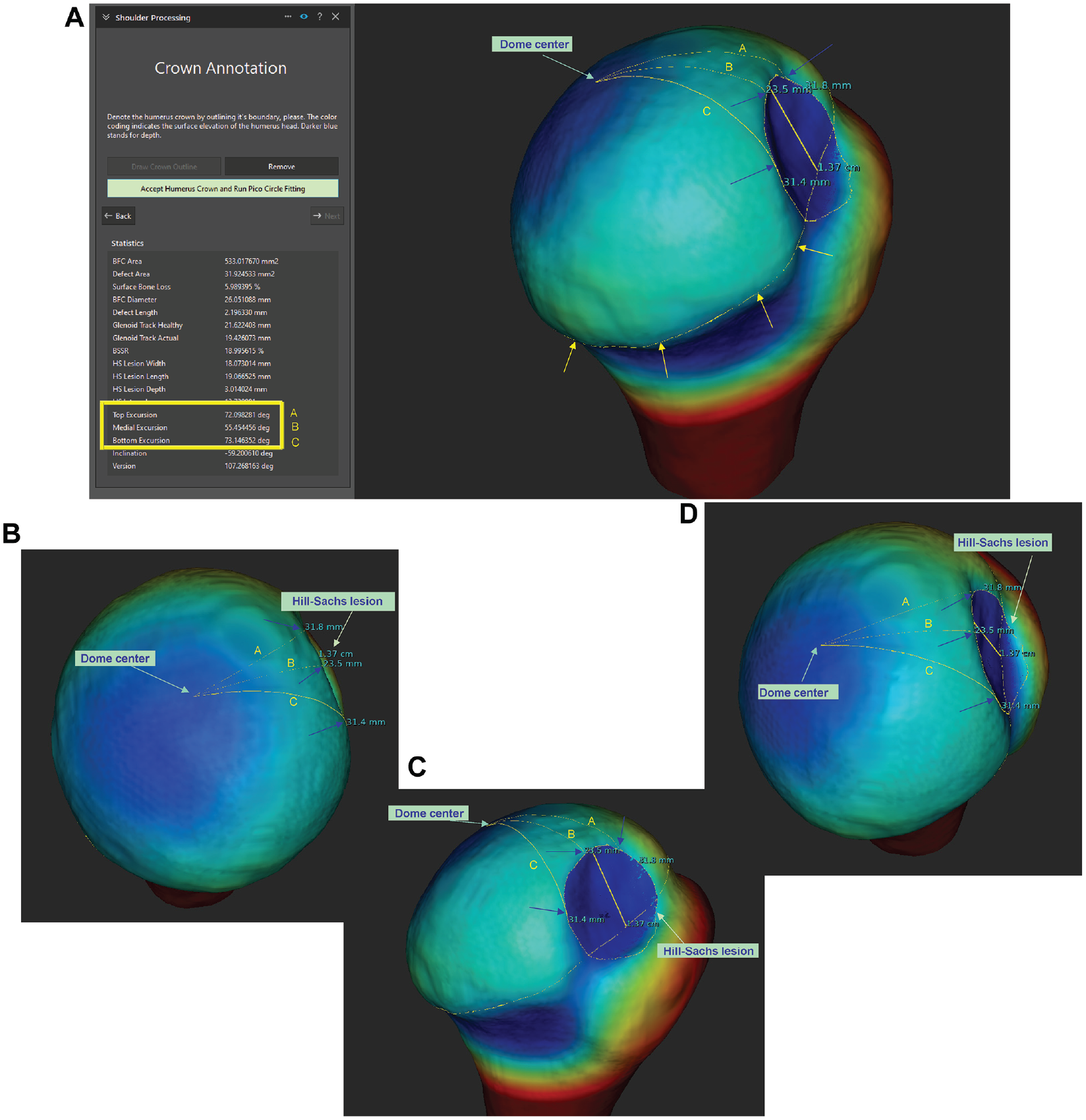
Analysis of the distances from the medial border of the Hill-Sachs lesion (blue arrows) to the dome center of the surface of the humeral head using the software ImFusion. (A) After the Hill-Sachs lesion and the outline of the anatomic neck (yellow arrows) of the humeral head were drawn by the investigator, the software was used to calculate the center of the dome-shaped anatomic head of the humerus (dome center) and the distances from the superior (A), middle (B), and inferior (C) medial edges of the Hill-Sachs lesion. (B) En face view from the apex of the humeral head (dome center). (C) View from medial. (D) View from posterior.
Statistical Analysis
Patient characteristics are presented using descriptive statistics. Variations within the collected parameters are shown as intraclass correlation coefficient (ICC) with 95% CI, interpreted according to Cicchetti. 1 An ICC of <0.40 specifies poor agreement, 0.40 to 0.59 indicates fair agreement, 0.60 to 0.74 indicates good agreement, and values ≥0.75 are considered to be excellent agreement. To calculate the ICC for the evaluation of whether a lesion is on- or off-track, we used the Cohen kappa test. The means of every parameter were calculated, including standard deviation and range. The parameters were tested for normal distribution using the Kolmogorov-Smirnoff test. A paired t test for normally distributed parameters and the Wilcoxon signed rank test for nonnormally distributed parameters were used to compare manually and automatically measured parameters. A P value <.05 was considered to be statistically significant. All statistical analyses were performed using the IBM SPSS Statistics software (Version 27.0).
Results
The study included 100 patients (84 male, 16 female) with a mean age of 28.6 ± 7.3 years (range, 13-48 years) at the time of surgery. In total, 46 left and 54 right shoulders were evaluated. Every CT scan (N = 100) was evaluated by both raters (K.K. and D.A.).
There was a significant difference between all manually and automatically obtained parameters. The measurement results are shown in Table 1.
Manual and Automated Measurement Parameters a

Data are presented as mean ± SD (range) for manual (using the software OsiriX and Visage Imaging) (N = 100) or automated (using the software ImFusion) (N = 100) measurements unless otherwise indicated. Significance was set at P < .05. HSI, Hill-Sachs interval; HSL, Hill-Sachs length; HSW, Hill-Sachs width.
Equal to 83% of glenoid width according to the glenoid track concept.
The measurements for manually obtained parameters showed fair agreement for the HSI and glenoid track concept, good agreement for the HSW, and excellent agreement for the HSL and glenoid width. With regard to the global track, the ICC was good for the top and bottom excursions and fair for the middle excursion.
Within the automatically obtained parameters, the agreement between raters was good for calculating the HSI, the glenoid track concept, and the top and bottom excursions of the global track. Agreement was excellent for the glenoid width, HSW, HSL, and middle excursion of the global track. The exact values can be seen in Table 2.
ICCs Between Raters 1 and 2 for All Manually and Automatically Measured Parameters a
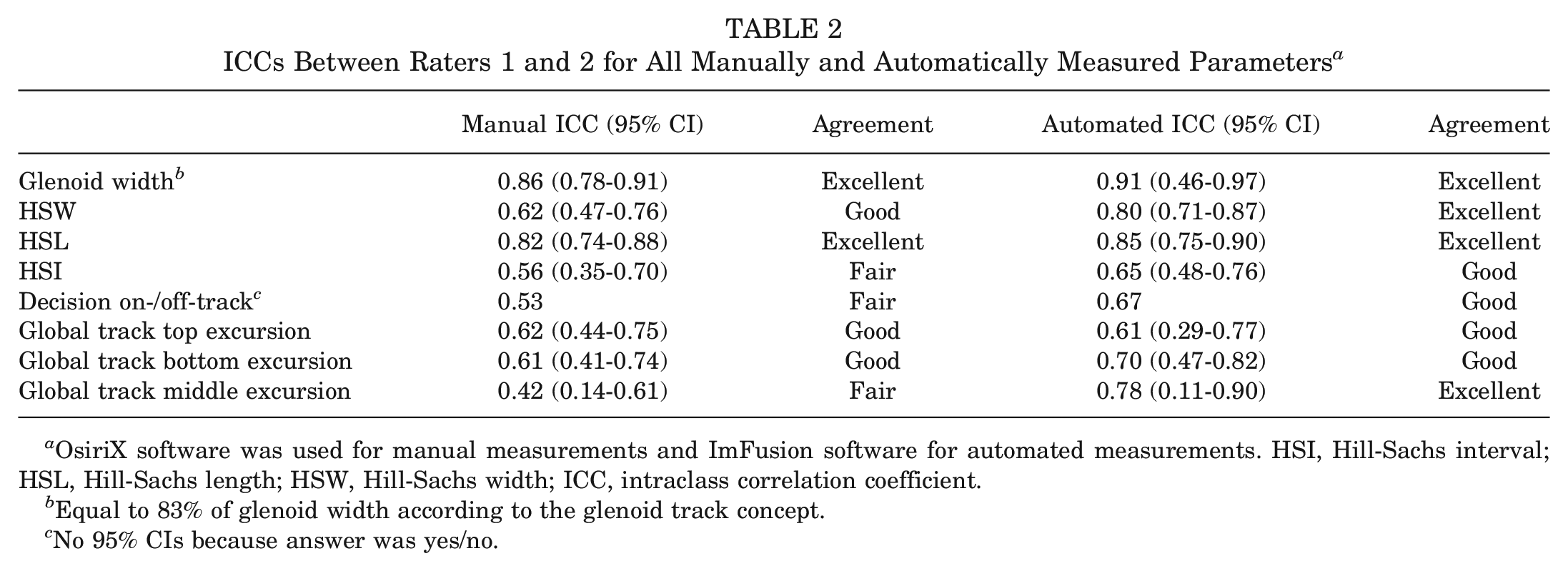
OsiriX software was used for manual measurements and ImFusion software for automated measurements. HSI, Hill-Sachs interval; HSL, Hill-Sachs length; HSW, Hill-Sachs width; ICC, intraclass correlation coefficient.
Equal to 83% of glenoid width according to the glenoid track concept.
No 95% CIs because answer was yes/no.
Discussion
The present study showed that the more complex global track measurements on the humeral side are more reliable compared with the current standard HSI and glenoid track measurements. However, this is only true when automated software is used to perform the measurements.
Di Giacomo et al 2 established a method based on radiological imaging to describe if a lesion is, in relation to the glenoid surface, on- or off-track and therefore engaging.2,13 This glenoid track was defined as the contact area of the humeral head with the glenoid from inferomedial to superolateral when the arm is raised. 13 To predict possible engaging lesions, it is important to determine how the Hill-Sachs lesion relates to this track. 2 Based on cadaveric models, the so-called glenoid track was defined as 83% of the healthy glenoid diameter minus the defect length. 2 Although the glenoid track itself can be determined reliably, the HSI remains a concern, as the definition of the HSI is the distance from the rotator cuff attachments to the medial rim of the Hill-Sachs lesion but the rotator cuff insertion on the posterolateral humeral head varies and is difficult to determine. 7 Additionally, the dependence on the cuff insertion as a reference makes the glenoid track concept at the same time dependent on soft tissue laxity. As the glenoid is able to push itself into the cuff and thus is able to expand its natural track beyond the confinements of the cuff, only 83% of the glenoid width is used for the formula to calculate on- and off-track lesions. However, depending on laxity, this 17% overlap might be much lower or higher. With the global track method, it is possible to calculate the distance from the center of the anatomic humeral head to the medial rim of the Hill-Sachs lesion. This track is a defined distance that is independent of the rotator cuff insertion or laxity of the patient, which might vary extensively among individuals and therefore limit the reliability and predictive value of the glenoid track concept. Implementing automated determination of the center of the humeral articular surface and measurement of the angular distance to the Hill-Sachs defect may allow us to predict to what extent a patient can move his or her arm until the glenoid reaches the Hill-Sachs lesion. To determine threshold values for critical Hill-Sachs defects, we need to collect clinical data and include the concept of bipolar defects in the future.
For the global track approach, our study showed substantial ICCs between raters and suggests a good to excellent reliability of the automated software. Specifically, the ICC for the middle excursion improved significantly from manual to automated measurements, which might be due to the fact that the middle of the Hill-Sachs lesion is more difficult to estimate on a normal CT scan than a software that displays distances more precisely. The ICC obtained using the software was slightly worse for the top and bottom excursions compared with the middle excursion, which might be explained by the fact that it is sometimes hard to evaluate the exact beginning and end within the length of the HSL, which still needs to be drawn manually within the software. This might also explain the difference between the manually and automatically obtained results for the top excursion of the global track. An even better agreement potentially could be achieved if the software was able to recognize the HSL automatically.
The study also has its limitations. First, with regard to the software, it would be desirable to test a larger number of CT scans. This would improve the software's skills of automatically recognizing the Hill-Sachs lesion as well as the dome of the humeral head. Currently, this needs to be drawn manually by the rater, which takes time and might therefore be difficult to implement in the surgeon's daily practice. Besides, a standardized CT image view for Hill-Sachs lesion measurement is still lacking when compared with the widely accepted en face view of the glenoid. Furthermore, the prototype of the software can be used to calculate only the bottom, top, and middle distances from the dome apex to the HSL rim, while the shortest distance would be the most meaningful in clinical practice.
Besides, within this calculation, an intact glenoid is assumed to see to which degree the arm can be raised until the Hill-Sachs lesion is reached. Further investigation is needed to implement bipolar lesions, which occur in most cases. With regard to the method, another limitation is the lack of a definition of critical threshold. Only small differences between manually and automatically obtained results were obtained within this study, which might not always be decisive, especially when taking the patient with individual demands into account. Nevertheless, ICCs improved, showing that measurements can be more precise and reliable using a dedicated software. So far, no therapy recommendation can be given based on the global track distances displayed; this will be part of upcoming investigations and improvements of the software to hopefully simplify measurements and decision-making in clinical daily life once established.
Conclusion
The global track concept allows the localization of the Hill-Sachs defect to the center of the humeral articular surface based on a 3D measurement method instead of the rotator cuff insertion and therefore makes it independent from individual soft tissue differences in terms of insertion site and laxity. Based on our results, the more complex global track assessment can be more reliably measured than the current standard of HSI and glenoid track measurements when an automated software is used to perform the measurements. Even though future studies need to be conducted to assess critical threshold values for defects prone to engagement, the global track might be the evolution of the glenoid track concept in identifying critical Hill-Sachs defects. Further studies might aim to evaluate the therapy success based on clinical decisions using the software results.
Footnotes
Submitted May 20, 2023; accepted December 14, 2023.
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.