
Abstract
Background:
Osteochondral allograft transplantation (OCAT) is an accepted knee joint–preserving treatment strategy for focal osteochondral lesions that is often conducted in combination with meniscal allograft transplantation (MAT). Despite its frequent and simultaneous utilization, there remains a lack in the literature reporting on outcomes and failure rates after concomitant procedures.
Purpose:
To determine (1) the midterm clinical success rate after OCAT+MAT in comparison with a matched-pair cohort undergoing isolated OCAT, (2) whether patient-specific and procedural variables influence the risk of failure, and (3) patient-reported outcome measures over time.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
A single-center matched-pair cohort study was conducted investigating outcomes in patients who underwent OCAT of the medial or lateral femoral condyle with and without MAT between 2004 and 2020. Patients were matched 1:1 by age (±5 years), sex (male or female), body mass index (±5), and grouped Kellgren and Lawrence grade (grades 0-1 or 2-4). The minimum follow-up time was 2 years. Radiographic variables (International Cartilage Regeneration & Joint Preservation Society [ICRS] grade and Kellgren and Lawrence grade) were assessed preoperatively and at follow-up. Subjective patient-reported outcome measures (Lysholm score, Knee injury and Osteoarthritis Outcome Score [KOOS] including subscores, International Knee Documentation Committee [IKDC] score, and visual analog scale score) were collected preoperatively and at follow-up. Clinical failure was defined as revision surgery for graft failure or conversion to total knee arthroplasty. Patient-reported, clinical, and radiographic outcomes were compared between groups.
Results:
In total, 66 patients (33 treated with isolated OCAT, 33 treated with OCAT+MAT; 57.6% male) with a mean age of 26.3 years (range, 18-62 years) were followed for a mean of 5.6 years (minimum, 2 years; range, 24-218 months). The 2 cohorts showed no difference in Kellgren and Lawrence grade postoperatively (P = .59). There was a significantly higher ICRS grade detected at follow-up in the OCAT+MAT group (2.81 ± 1.10) compared with the OCAT group (2.04 ± 0.96) (P < .05). There were no statistically significant differences between the groups regarding reoperation rate (OCAT: n = 6; OCAT+MAT: n = 13; P = .116), time to reoperation (OCAT: 46.67 ± 47.27 months vs OCAT+MAT: 28.08 ± 30.16 months; P = .061), and failure rate (OCAT: n = 4 [12.1%] vs OCAT+MAT: n = 5 [15.2%]; P = .66). In the OCAT+MAT group, an increase of tibial slope by 1° conferred a 1.65-fold increase in the hazard for failure over decreased slope (hazard ratio, 1.65; 95% CI, 1.10-2.50; P < .05). The overall survival rate was 86% at a mean follow-up of 5.6 years. Patient-reported outcome scores were significantly improved at the final follow-up compared with preoperative status. No significant differences were seen between groups with respect to subjective IKDC, Lysholm, Tegner, and KOOS results, except for the KOOS Symptoms subscale score, which was significantly higher in the OCAT+MAT group than in the OCAT group (mean difference, 14.6; P < .05) and did exceed the minimal clinically important difference threshold of 10.7.
Conclusion:
Midterm results after isolated OCAT and OCAT+MAT show high rates of healing and sustainable subjective improvement of knee function and quality of life. However, it should be noted that the difference in reoperation rate and time to reoperation between the groups is arguably clinically important and that lack of statistical significance may be because of low power. These results imply that isolated OCAT is an efficient joint-preserving treatment that can be combined with MAT in well-selected patients with meniscal insufficiency without negative influence on global clinical outcomes.
Keywords
Osteochondral allograft transplantation (OCAT) and meniscal allograft transplantation (MAT) are established standard-of-care procedures in joint-preserving surgery.10,12,30 These techniques have garnered strong support from studies showcasing their effectiveness in addressing osteochondral defects11,15,19,31 and meniscal deficiency, respectively.10,32,46,50 When conducted individually, both procedures exhibit favorable mid- to long-term outcomes, with success rates ranging from 64% to 93% at 5 to 10 years after transplantation.2,10,12,17,27,30,50 The use of freshly obtained allografts, typically implanted within 24 to 48 hours of donor expiration, has led to enduring graft survival rates of 66% to 69% even after 20 years. 12 Nevertheless, the co-occurrence of meniscal and chondral lesions within the same knee often necessitates a combined repair strategy for patients with multifaceted knee issues encompassing chondral lesions, meniscal deficiency, and occasionally ligamentous instability and malalignment. 18
Biomechanical research compellingly links meniscal deficiency to diminished chondroprotection, promoting chondrosis and osteochondrosis.34,41 Many young patients present with previous knee surgeries and a history of vigorous preinjury activity, leading to heightened postoperative expectations for joint preservation outcomes.37,49 This conjunction of elevated patient hopes and substantial knee damage underscores the significance of comprehensive pre- and postoperative patient education within this challenging cohort. Although OCAT and MAT are occasionally viewed as remedies to enhance function and alleviate pain in patients with compromised quality of life and daily activities, they also hold the potential, in specific instances, to enable a return to recreational, competitive sports or activities for those otherwise unable to participate.5,16,38
First described as early as 1908 by Eric Lexer, OCAT has become the gold standard for the treatment of cartilage defects >2 cm2, with well-established safety, efficacy, and durability.27,36,39 Research conducted over the past several decades has improved our understanding of the physiology of graft incorporation and the conditions that lead to improved graft survivorship. The technique allows for the simultaneous transplantation of cartilage and underlying bone, enabling clinicians to address pathology extending beyond the subchondral plate if needed. 25 OCAT was initially used to treat large osteochondral defects or unicompartmental arthritis 5 ; however, indications for OCAT have been refined, and more recently, use of OCAT for the treatment of high-grade cartilage defects has increased. 3
A meniscus-deficient knee can lead to accelerated cartilage wear and therefore a shortened survival time of implanted osteochondral allografts. 26 Consequently, loss of continuity of meniscal hoop stress by radial or root tear, or loss of a significant amount of meniscal tissue, creates a relative contraindication to cartilage-restoration procedures.7,47 Former studies have shown that inferior outcomes of OCAT have to be expected if carried out in the presence of meniscal deficiency, malalignment, and/or ligamentous instability. 45 Because of this challenging combination of pathologies and with recent advances in tissue preservation, transplantation techniques, and postoperative rehabilitation techniques, concurrent OCAT+MAT is considered a biologic joint restoration option in these common and complex cases.5,6,8,43,44
Taken together, OCAT+MAT can be considered symbiotic procedures given a complementary spectrum of indications and reciprocal contraindications. 14 However, few outcomes of concomitant OCAT+MAT have been reported in the literature, and the effects of concomitant MAT on outcomes of OCAT as a strategy for knee joint preservation have rarely been discussed. The purpose of this study was to determine (1) the midterm clinical success rate after OCAT+MAT in comparison with a matched-pair cohort undergoing isolated OCAT, (2) whether patient-specific and procedural variables influence the risk of failure, and (3) patient-reported outcome measures (PROMs) over time. We hypothesized that the clinical results of OCAT+MAT would be equally as good as outcomes after isolated OCAT.
Methods
Study Design and Participants
This analysis of prospectively collected data was performed at the Mayo Clinic between 2005 and 2020. Institutional review board approval was obtained before the beginning of the study. A search of the institutional medical records database was performed to identify all patients who had undergone surgery involving OCAT of the medial femoral condyle or lateral femoral condyle and MAT of the knee. Patients who underwent OCAT without concurrent MAT (n = 33) were matched in a 1:1 ratio to patients who underwent OCAT+MAT (n = 33) (Figure 1). Matching criteria were sex (male or female), age (±5 years), body mass index (BMI; ±5), and preoperative Kellgren and Lawrence grade (grades 0-1 or 2-4). The predetermined threshold of the absolute standardized differences for the variables matched was 0.25 and was not exceeded by any variable (Table 1). All MAT procedures were performed in the same compartment as the OCAT. Patients were included if they underwent OCAT for symptomatic, isolated, full-thickness chondral lesions >1 cm in diameter recalcitrant to nonoperative treatment. Indications for MAT included symptomatic meniscal deficiency, including previous failed meniscal surgeries. Exclusion criteria consisted of (1) previous osteochondral allograft, osteochondral autograft transfer, or a similar procedure in the ipsilateral knee; (2) previous MAT in the same compartment; (3) OCAT to the patella or the trochlea; and (4) patients <18 years of age. When indicated, patients underwent concurrent alignment-correcting osteotomy of the proximal tibia or distal femur. Indications included correction of a mechanical axis that preferentially loaded or overloaded the involved compartment. These cases were addressed with an axis correction aiming to generate a neutral axis through the center of the tibial plateau to offload the targeted compartment. In cases with axial varus malalignment ≥5° and/or instability of the knee joint, a corrective osteotomy or stabilization procedure was performed at the time of transplantation. All procedures were performed in a 1-stage setting to (1) avoid the surgical morbidity of 2 separate surgical procedures, both associated with extended rehabilitation periods, and (2) immediately generate an ideal biomechanical environment for the cartilage/meniscal grafts from the day of implantation (Figure 2).
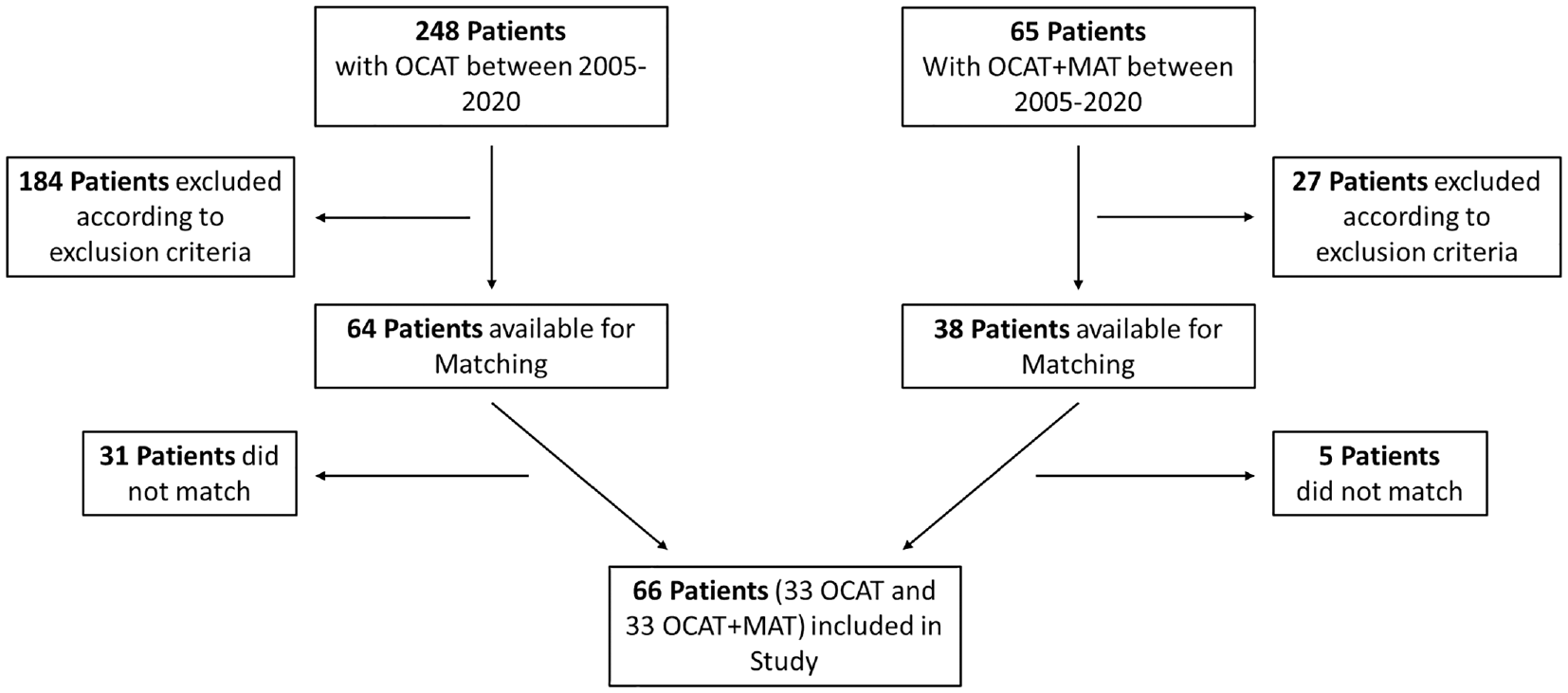
Flowchart showing patient selection. Patient screening and enrollment based on inclusion and exclusion criteria. MAT, meniscal allograft transplantation; OCAT, osteochondral allograft transplantation.
Absolute Standardized Differences for Each Variable Used in Matching a
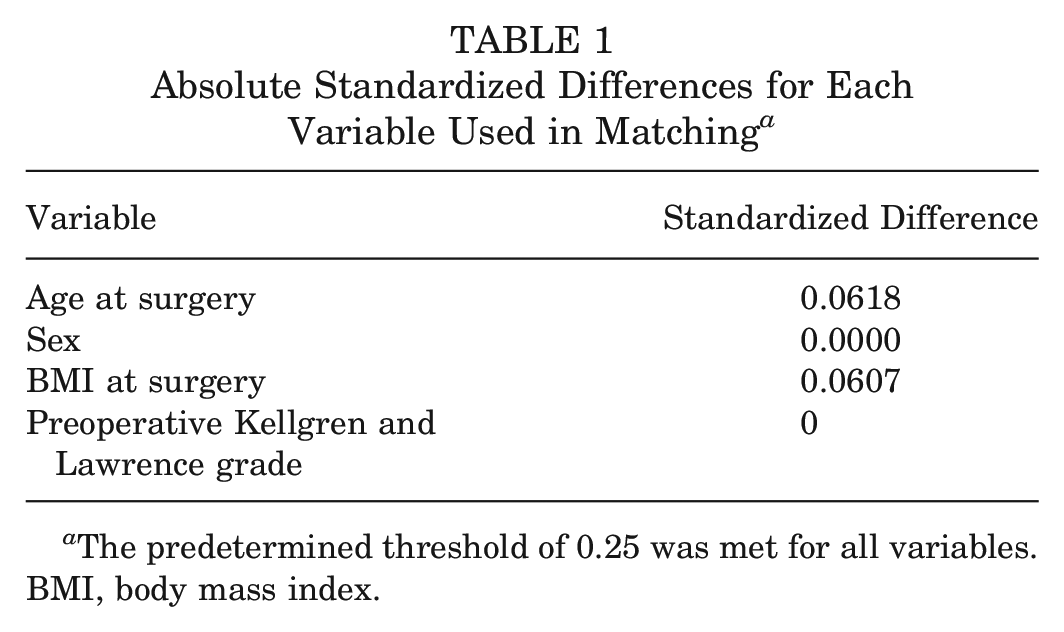
The predetermined threshold of 0.25 was met for all variables. BMI, body mass index.
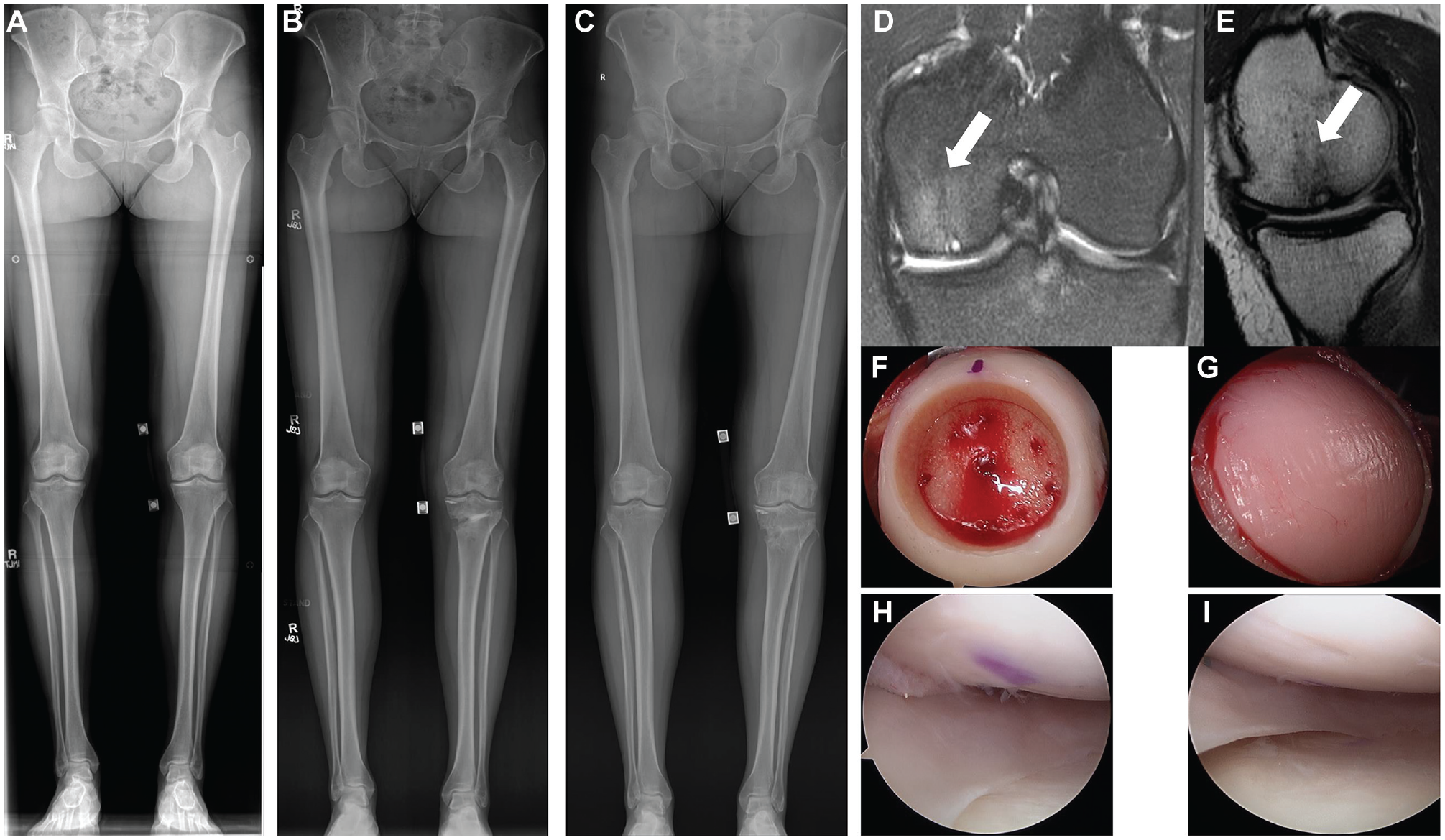
(A-C) Serial radiographs obtained in a 34-year-old patient undergoing concurrent medial, valgus-producing open-wedge osteotomy, medial femoral condylar allograft transplantation, and medial meniscal allograft transplantation. (A) Preoperative long-leg radiographs with a 5° varus malalignment of the left leg. (B) A neutral leg axis after valgus-producing osteotomy 6 months after index surgery. (C) Status at 6 years. (D, E) Preoperatively, an advanced grade 4 chondromalacia with focal subchondral cystic change in the weightbearing area (white arrows) of the medial femoral condyle was visible. (F, G) Intraoperatively, the full-thickness chondral lesion (16 × 18 mm) was addressed with a 20 mm–diameter fresh osteochondral allograft. (H, I) A medial meniscal allograft was fixed with anterior and posterior bone plugs. (B, C) Two suture anchors were placed in the medial tibial plateau margin to reattach the deep medial collateral ligament.
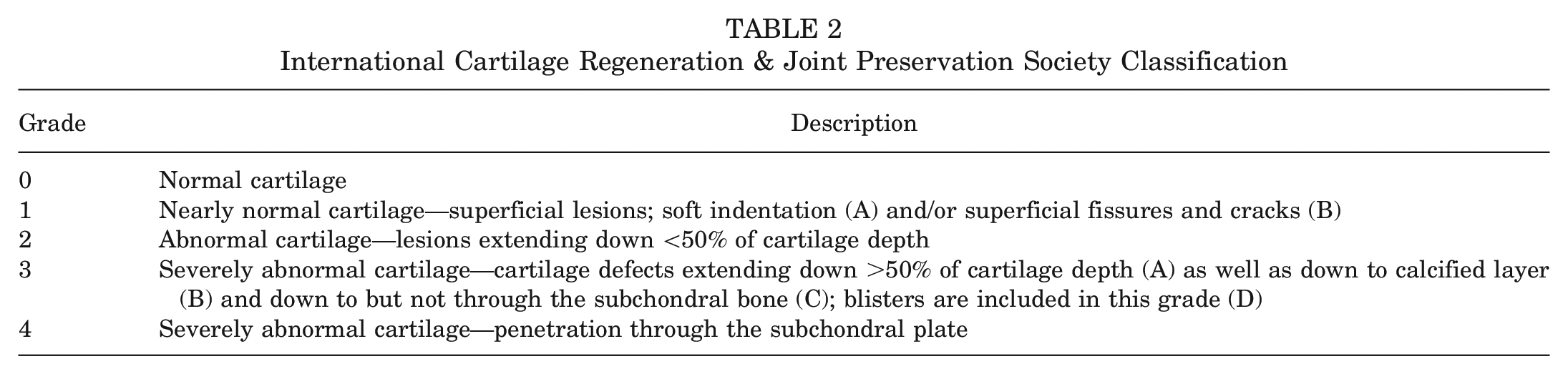
OCAT+MAT was indicated in patients with a combined osteochondral defect of the femoral condyle or tibial plateau and meniscal deficiency resulting in pain and loss of function. Stability was assessed using a combination of clinical, radiographic, and magnetic resonance imaging (MRI) findings and confirmed intraoperatively. The extent of the cartilage lesion was graded intraoperatively using the International Cartilage Regeneration & Joint Preservation Society (ICRS) classification (Table 2). Healing was assessed using postoperative MRI scans when available (46 of 66 patients); otherwise, the last postoperative radiograph was used. Failure was defined as any definitive reoperation for the same osteochondral graft, such as refixation, fragment excision, or (osteo-)chondral restoration procedures such as chondroplasty. Hardware removal was not considered a failure. For patients with healed lesions, pre- and postoperative International Knee Documentation Committee (IKDC) Subjective Knee Evaluation Form, Lysholm score, visual analog scale (VAS), Tegner activity scale, and Knee injury and Osteoarthritis Outcome Score (KOOS) results were recorded. 52
International Cartilage Regeneration & Joint Preservation Society Classification
Surgical Technique
Isolated OCAT
The surgical technique used for OCAT in this study has been described in detail by Cavendish et al. 3 In brief, all patients underwent examination under anesthesia and diagnostic arthroscopy before OCAT. If concomitant alignment-correcting osteotomy was performed, this procedure was always carried out last, after OCAT and, if applicable, MAT.
OCAT With MAT
The surgical technique used for MAT in this study has been described in detail by Woodmass et al. 51 In brief, all patients underwent meniscal allograft fixation using a bone plug. The MAT was completed first, followed by the OCAT procedure.
Rehabilitation Protocol
In brief, the postoperative rehabilitation protocol started with a restricted range of motion of 0° to 90° and protected weightbearing in full extension using crutches for 4 to 6 weeks for both patient groups. Isometric exercises, cryotherapy, and closed kinetic chain strengthening were performed. At 4 weeks postoperatively, weightbearing as tolerated was allowed, full range of motion and aerobic exercise were introduced, and the knee immobilizer was discontinued. At week 16, patients were allowed to return to activity as tolerated and a jogging program was initiated. Basic plyometric exercises were introduced with caution to avoid loaded high knee flexion. Attention was shifted to strength, endurance, and proprioception training. Noncontact sports were allowed after 6 months, with a return to high-demand sports after 8 months. There were no substantial differences in rehabilitation protocol between patients treated with isolated OCAT and patients undergoing OCAT+MAT.
Statistical Analysis
Statistical matching was performed by a formally trained statistician. Descriptive statistics including mean, standard deviation, and range were used to characterize results with continuous values, while percentages were used for proportions. Patient and surgery details were compared between groups using Wilcoxon rank-sum tests for continuous variables (age, BMI, and lesion size) and Fisher exact tests for categorical variables (sex, laterality, and condylar location). Kaplan-Meier survival curves were constructed for the OCAT and OCAT+MAT cohorts to compare failure rates and assess for survival. A univariate Cox proportional hazards model was used to analyze the risk of failure based on skeletal maturity. Within each group, other risk factors for failure were assessed using odds ratios and Fisher exact tests for dichotomous variables along with nominal logistic fit models for continuous or ordinal variables. Significant variables were used to construct a multivariate Cox proportional hazards model for the effect of these variables on failure rate. The PROMs (IKDC, Lysholm, VAS, and KOOS) were compared using Wilcoxon rank-sum tests; analyses were performed between pre- and postoperative scores for each measure within each group and for the baseline and final scores between groups. Statistical significance was set at P < .05. All statistical analyses were performed using SPSS Statistics for Windows (Version 28.0; IBM Corp). Graphics were designed with SPSS Statistics for Windows (Version 28.0) and Microsoft Excel (Version 2021).
Post Hoc Power Analysis
Post hoc power analyses were performed to examine the achieved power for detecting the minimal clinically important difference (MCID) in patient-reported outcome scores as well as failure and reoperation rates. The achieved power was >0.99 for detecting an MCID of 16.7 for KOOS Pain and an MCID of 25 for KOOS Sport and Recreation, and >0.99 for detecting an MCID of 9.8 for the IKDC at an alpha of .05. 40
Results
Study Group Characteristics
In total, 66 patients met the inclusion criteria for this study (Table 3). The mean age ± SD of both cohorts at the time of index surgery was 26.3 ± 8.7 years (range, 18-62 years), and the mean follow-up was 66.6 ± 39.6 months (range, 24.0-218.1 months). Of the patients, 57 (86.4%) underwent ≥1 surgical procedure on the ipsilateral knee before OCAT, with the entire cohort undergoing 1.5 ± 1.3 ipsilateral knee operations before index surgery. Table 3 demonstrates that matching was successful in achieving covariate balance between the groups, with all criteria having absolute standardized differences <0.25 (as per predetermined threshold). The characteristics of the study population, stratified by group, according to the criteria used for matching are reported in Table 3. The groups were similar with respect to mean preoperative Tegner score (4.27 ± 1.29 in the OCAT group; 4.12 ± 2.38 in the OCAT+MAT group), mean duration of follow-up (67.21 ± 44.84 months [range, 24-218 months] for the OCAT group; 65.97 ± 33.65 [range, 24-129 months] for the OCAT+MAT group; P = .84), and mean preoperative ICRS grade (P > .05). All these characteristics indicate that matching was successful in reducing bias and that the groups were similar enough to allow reliable comparisons.
Patient and Procedural Characteristics a
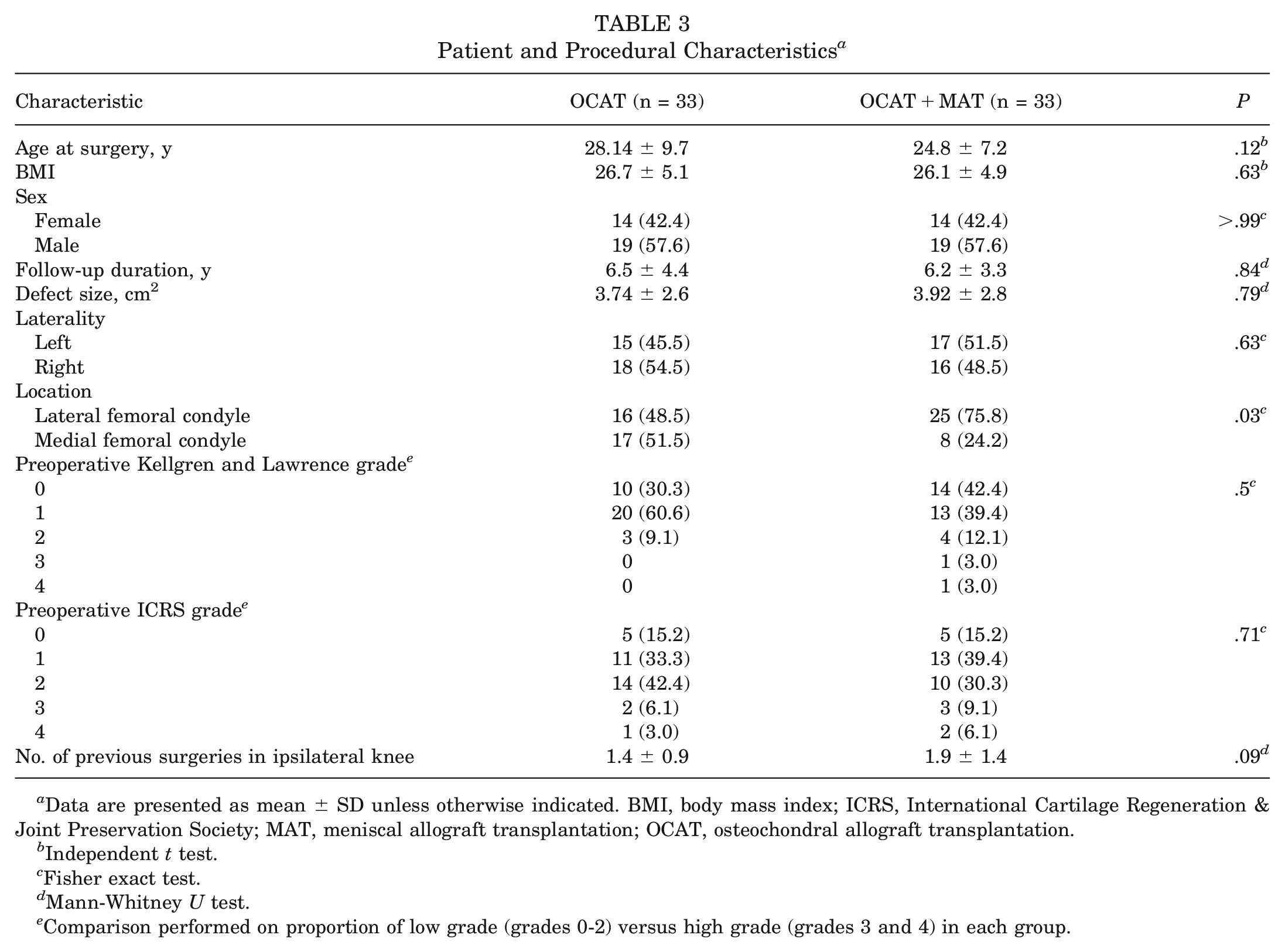
Data are presented as mean ± SD unless otherwise indicated. BMI, body mass index; ICRS, International Cartilage Regeneration & Joint Preservation Society; MAT, meniscal allograft transplantation; OCAT, osteochondral allograft transplantation.
Independent t test.
Fisher exact test.
Mann-Whitney U test.
Comparison performed on proportion of low grade (grades 0-2) versus high grade (grades 3 and 4) in each group.
None of the patients in either group underwent concomitant ligament repair or reconstruction surgery. Six patients undergoing isolated OCAT had concomitant realignment osteotomies, while 4 patients treated with OCAT+MAT had concomitant realignment osteotomies (P = .55) (Table 4).
Concurrent Procedure Performed at the Time of OCAT in the Same Compartment a
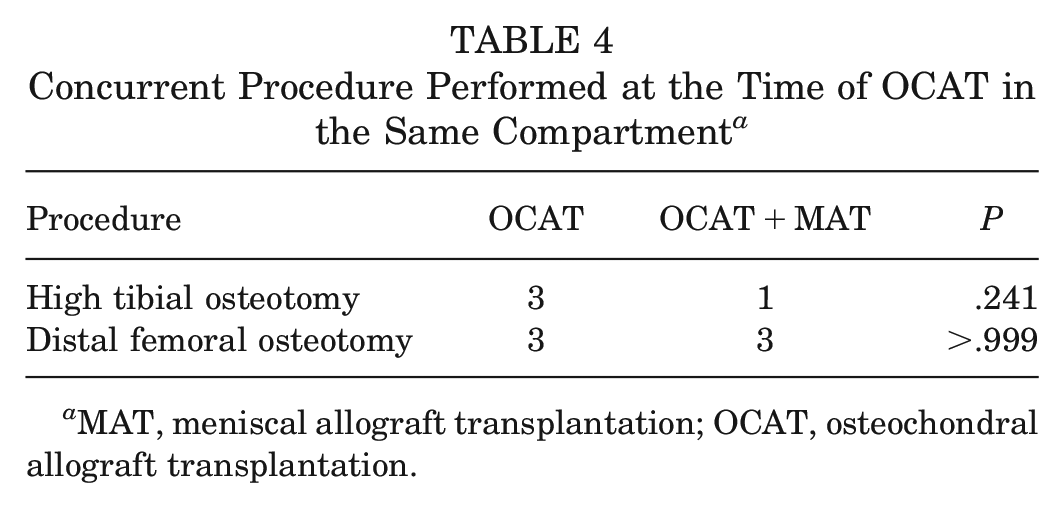
MAT, meniscal allograft transplantation; OCAT, osteochondral allograft transplantation.
Reoperations
Of the 66 patients, 19 underwent reoperation at 33.9 ± 37.5 months after index surgery (Table 5). There were no significant differences in the number of patients in either group undergoing reoperation (OCAT: 6 vs OCAT+MAT: 13; P = .116) or in the mean time until reoperation (OCAT: 46.7 ± 47.3 months vs OCAT+MAT: 28.1 ± 30.2 months; P = .06). Of the 19 patients who underwent reoperation, 13 (68.4%) received reoperation within 2 years of the index surgery, with patients undergoing OCAT+MAT demonstrating a similar rate of reoperation within this time frame (OCAT: 50% vs OCAT+MAT: 76.9%; P = .55). Arthroscopic debridement was performed in 17 of these 19 (89.5%) initial reoperations, with 14 knees (73.7%) showing arthroscopic evidence of an intact osteochondral graft. Arthroscopic debridement was performed to smooth any incongruent but nondegenerative chondral surfaces in and around the graft, resect partial tears of the MAT, and remove loose bodies. Of the 17 patients receiving debridement, 1 underwent a partial bone block resection of the MAT bone block. The osteochondral allograft was pristine at the time of reoperation. Of the 19 knees that underwent reoperation, 7 knees ultimately progressed to failure at 57.7 ± 42.5 months after index surgery.
Subsequent Surgeries Performed After Index Surgery a
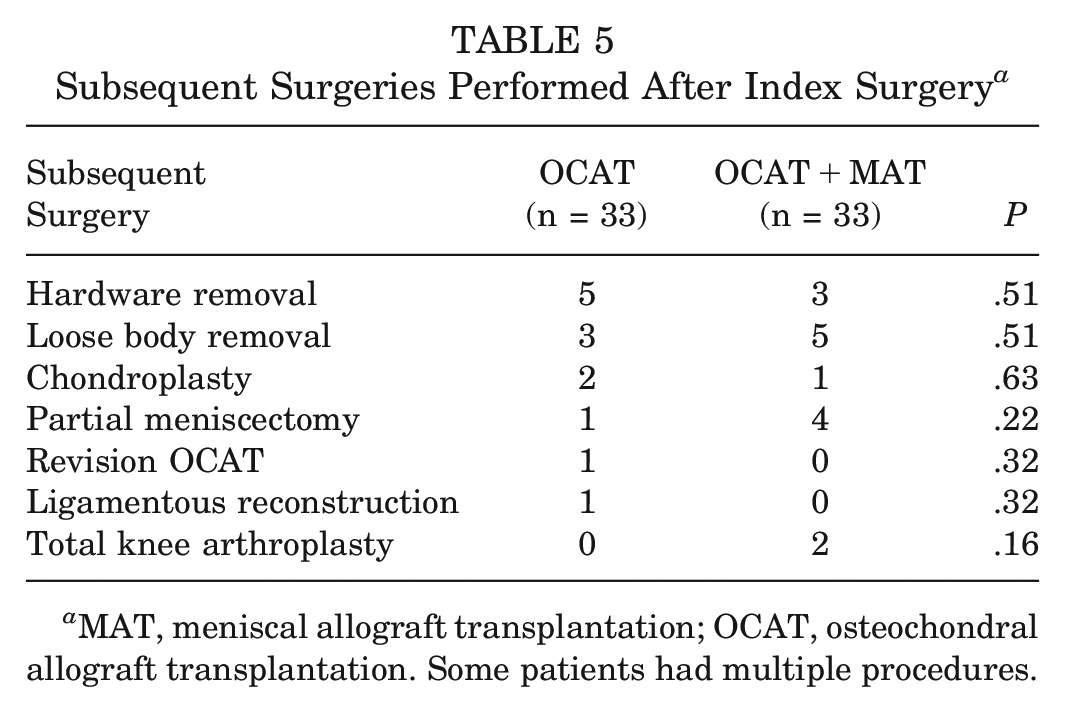
MAT, meniscal allograft transplantation; OCAT, osteochondral allograft transplantation. Some patients had multiple procedures.
Clinical Outcomes and Failures
Failures were recorded in 9 of 66 (13.6%) patients based on the need for further surgical management, including graft fragment excision, total knee arthroplasty, and cartilage procedures such as chondroplasty (Table 6). Failure occurred at a mean of 65.1 months (range, 21-114) after surgery. Of these 9 patients, 2 (22.2%) underwent subsequent knee arthroplasty, 2 (22.2%) received revision OCAT, and 5 (55.6%) had a fragmentation of the poorly incorporated graft at second-look arthroscopy and were treated with chondroplasty. There were no significant differences between the groups with respect to failure rates (OCAT: n = 4 [12.1%] vs OCAT+MAT: n = 5 [15.2%]; P = .66).
Complications and Failures a
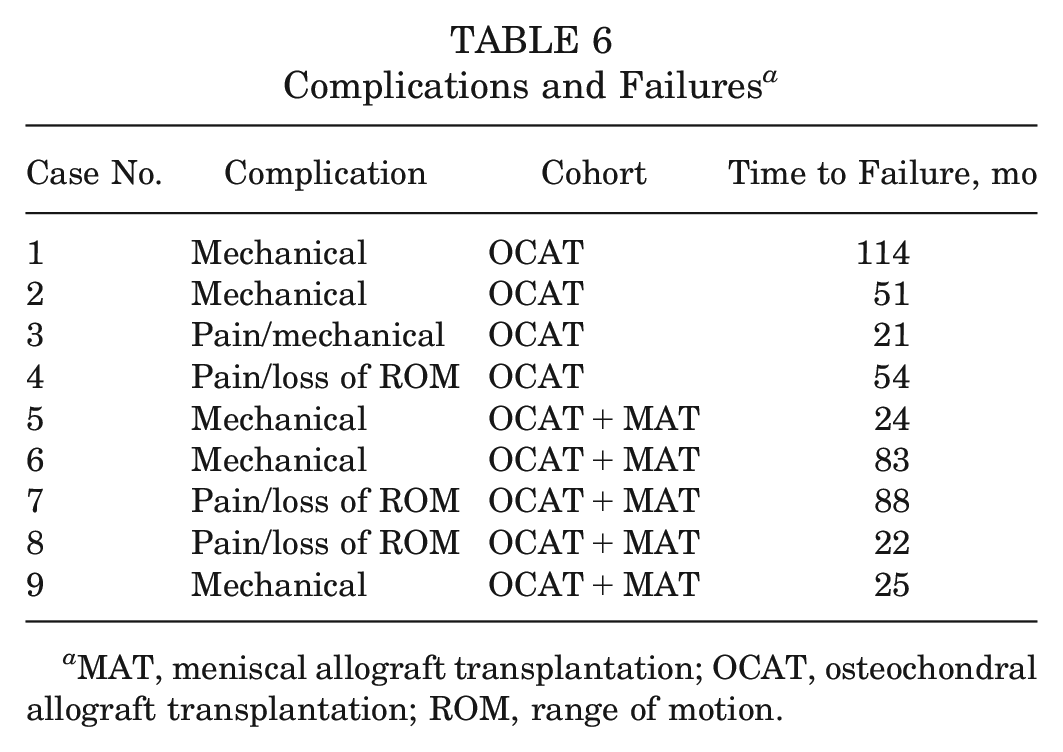
MAT, meniscal allograft transplantation; OCAT, osteochondral allograft transplantation; ROM, range of motion.
Survival Based on Procedure
Kaplan-Meier survival curves were used to compare the time-dependent survival of patients who underwent isolated OCAT versus OCAT+MAT (Figure 3). Failure occurred in 4 of 33 (12.1%) patients in the OCAT group and 5 of 33 (15.2%) patients in the OCAT+MAT group. For patients who received OCAT alone, survival free from revision was 100% at 1 year after surgery, 97% at 2 years, 91% at 5 years, and 88% at 10 years. Patients who underwent OCAT+MAT had survival rates of 100%, 94%, 91%, and 85% at 1, 2, 5, and 10 years (P = .66). The combined survival rates were 100%, 97%, 92%, and 86% at 1, 2, 5 and 10 years. In the univariate Cox proportional hazards model for treatment type alone, there was no significant difference in the risk of failure between the groups (hazard ratio [HR], 1.34; 95% CI, 0.35-5.10; P = .67).
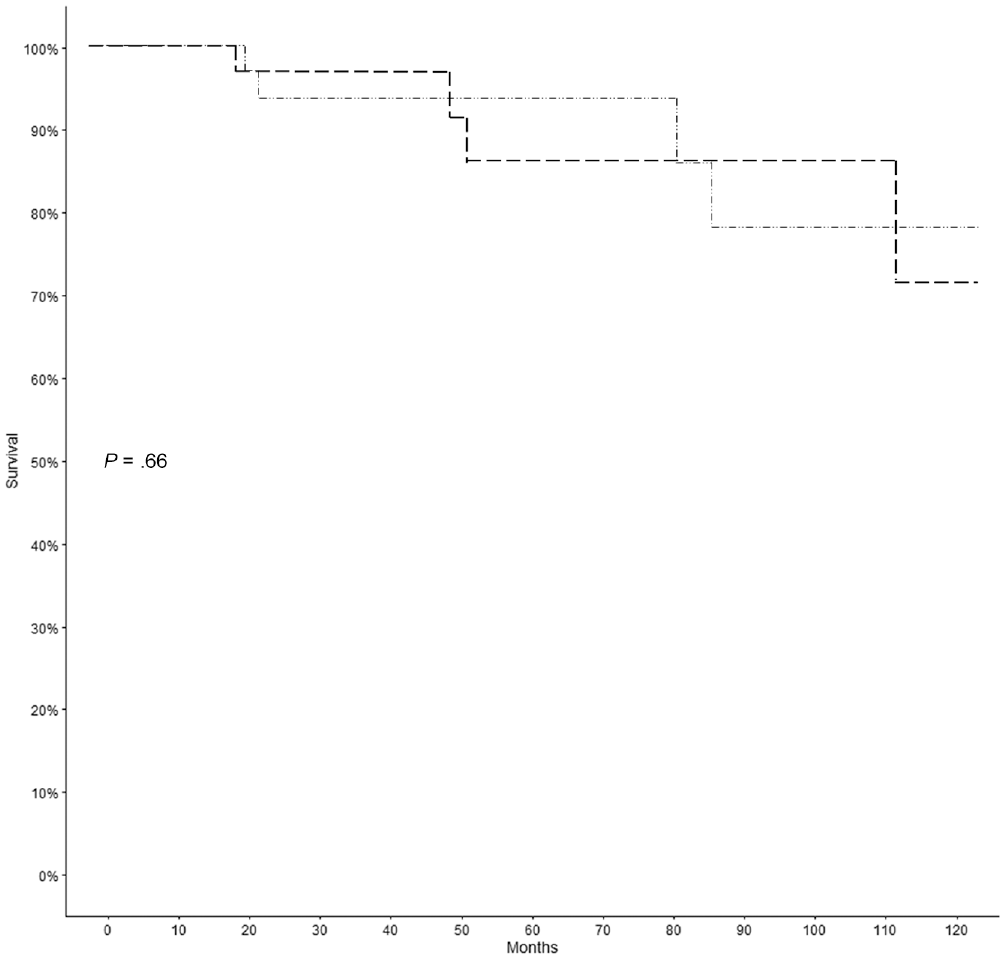
Kaplan-Meier survival analysis curves showing failure and survival after OCAT and OCAT+MAT (P = .66). Bold line, OCAT; thin line, OCAT+MAT. MAT, meniscal allograft transplantation; OCAT, osteochondral allograft transplantation.
Intergroup Analysis
Because of the preoperative differences in surgery type (OCAT vs OCAT+MAT), Kaplan-Meier analysis was conducted to assess survival by these characteristics in the overall group. In the group overall, there was no difference in survival by type of surgery (OCAT 87.9% vs OCAT+MAT 84.8%; P = .66) (Figure 3) or lesion location (percentage of medial vs lateral; P = .56) (Figure 4). Results were similar in the OCAT+MAT group, where preoperative ICRS grade (low 85.7% vs high 80%; P = .76) and preoperative Kellgren and Lawrence grade (low 85.2% vs high 83.3%; P = .7) were not significant for survival within the group. In the OCAT group, lesion location (medial 84.2% vs lateral 92.9%; P = .57), preoperative ICRS grade (low 86.7% vs high 100%; P = .94), and preoperative Kellgren and Lawrence grade (low 90% vs high 66.7%; P = .52) were also not significant for survival within the group.
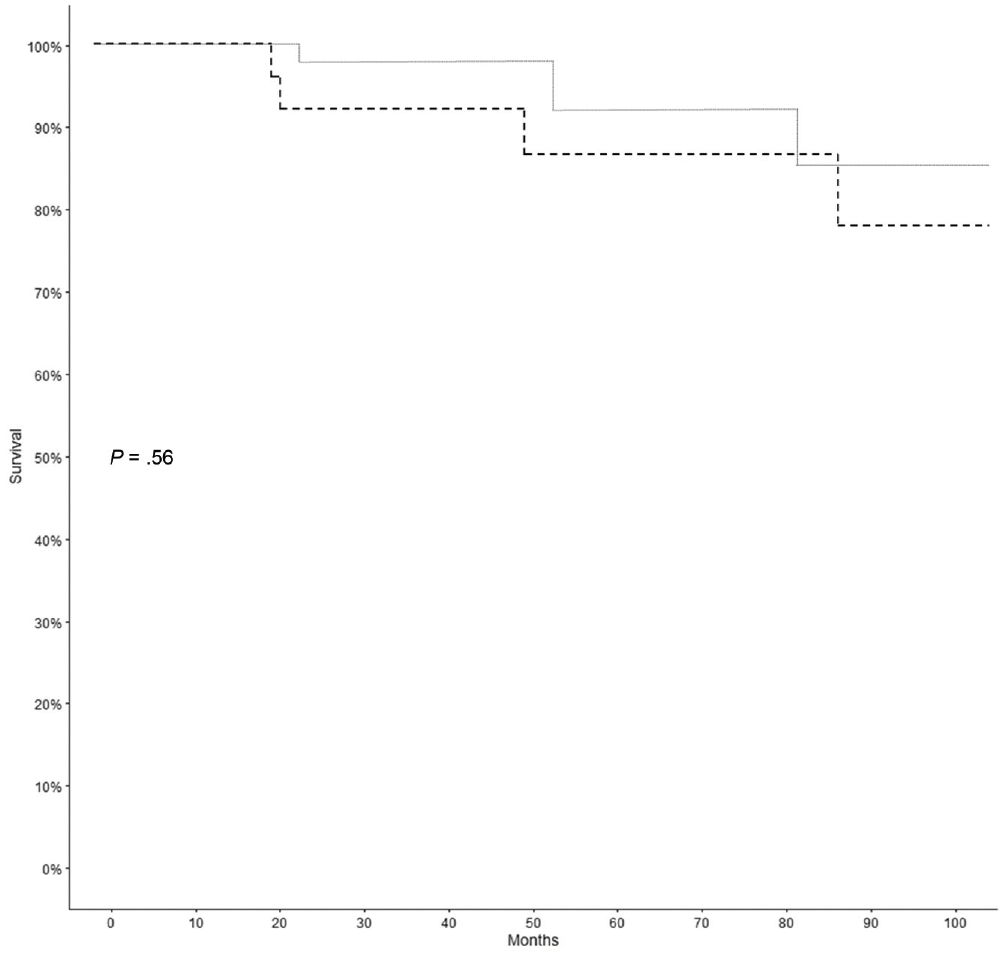
Kaplan-Meier survival analysis curves showing failure and survival after OCAT and OCAT+MAT in reference to lesion location (P = .56). Thin dotted line, medial compartment; bold line, lateral compartment. MAT, meniscal allograft transplantation; OCAT, osteochondral allograft transplantation.
Risk Factor Analysis
Risk factors for failure were first analyzed independently within the OCAT and OCAT+MAT groups (Table 7). In the OCAT+MAT group, an increase of tibial slope by 1° conferred a 1.65-fold increase in the hazards for failure (HR, 1.65; 95% CI, 1.10-2.50; P < .05). A univariate Cox proportional hazards model was used to evaluate the interaction between procedure type and risk factor. Tibial slope did not significantly affect the failure rate in the OCAT group (HR, 0.97; 95% CI, 0.73-1.30; P = .83) (Table 7). Otherwise, there was no significant change in the risk ratio of failure in either group based on sex, laterality, number of previous surgeries, time from first surgery to index surgery, medial or lateral compartment, or defect size (Figure 5). The continuous and ordinal variables were analyzed separately using nominal logistic fit models. There were no significant differences in failure rate based on BMI (OCAT, P = .44; OCAT+MAT, P = .63), lesion size (OCAT, P = .89; OCAT+MAT, P = .77), ICRS grade (OCAT, P = .52; OCAT+MAT, P = .92), or Kellgren and Lawrence grade (OCAT, P = .92; OCAT+MAT, P = .41).
Univariate Analysis of the Hazards for Clinical Failure Based on Patient-Specific Variables a
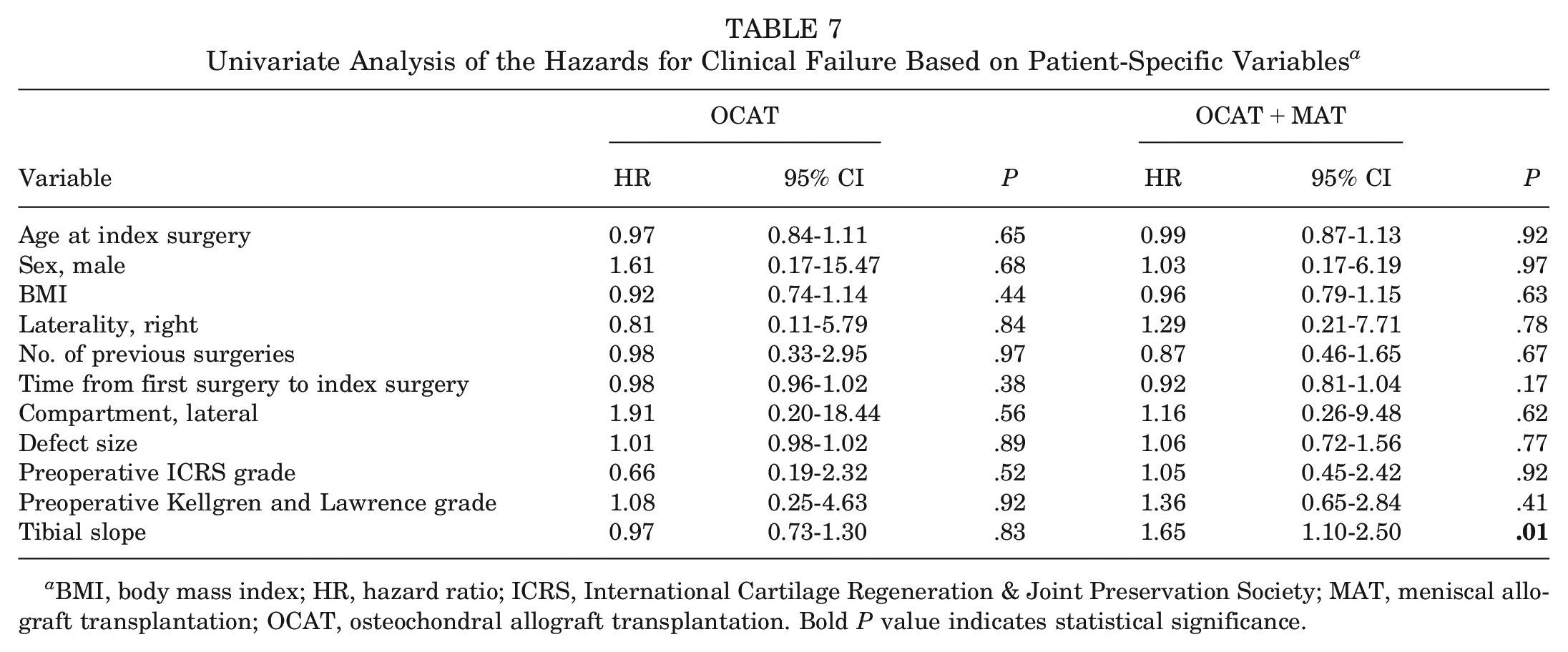
BMI, body mass index; HR, hazard ratio; ICRS, International Cartilage Regeneration & Joint Preservation Society; MAT, meniscal allograft transplantation; OCAT, osteochondral allograft transplantation. Bold P value indicates statistical significance.
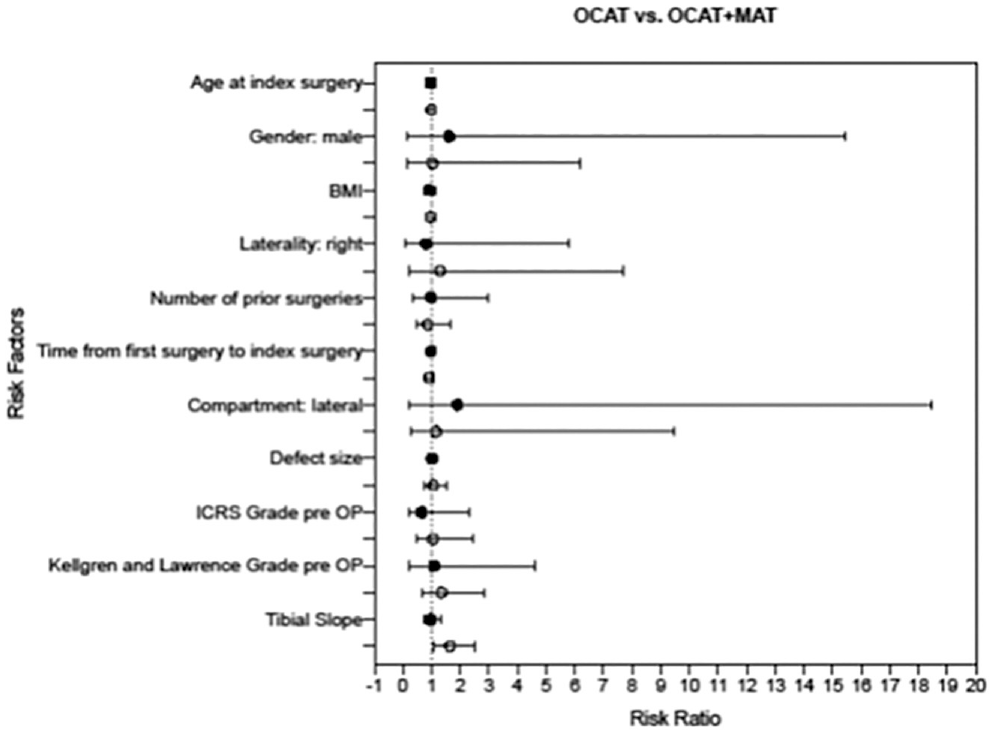
Forest plot of risk factors for failure and conferred risk ratio. Squares, OCAT; circles, OCAT+MAT. BMI, body mass index; ICRS, International Cartilage Regeneration & Joint Preservation Society; MAT, meniscal allograft transplantation; OCAT, osteochondral allograft transplantation; pre OP, preoperatively.
Radiographic Outcomes
The cohorts were similar in Kellgren and Lawrence grade (P = .50) and ICRS grade (P = .71) at the beginning of the study. The mean Kellgren and Lawrence grade of the OCAT cohort was 0.79 ± 0.59 preoperatively and 1.39 ± 0.79 at the final follow-up (P < .05). In the OCAT+MAT cohort, the preoperative mean Kellgren and Lawrence grade was 0.85 ± 0.96 and that at the final follow-up was 1.52 ± 1.16 (P < .05). The 2 cohorts showed no difference in Kellgren and Lawrence grade postoperatively (P = .59).
For 25 of 33 (75.8%) patients who underwent OCAT, a postoperative MRI scan was available. The mean preoperative ICRS grade was 1.48 ± 0.93, and the postoperative grade was 2.04 ± 0.96 (P < .05). In the OCAT+MAT group, 23 of 33 (69.7%) patients had undergone postoperative MRI. Preoperatively, the ICRS grade was 1.51 ± 1.04 and progressed to 2.81 ± 1.10 at the final follow-up (P < .05). There was a significantly higher ICRS grade detected in the OCAT+MAT group than in the OCAT group (P < .05).
Patient-Reported Outcome Measures
Outcomes were assessed using IKDC, Lysholm, VAS, and KOOS results and the Tegner activity scale (Table 8). At the mean final follow-up of 75.82 ± 46.69 months (range, 18-218 months), no significant differences were seen between groups with respect to subjective IKDC, Lysholm, Tegner, and KOOS results, except for the KOOS Symptoms subscale score, which was significantly higher (better) in the OCAT+MAT group than in the OCAT group (mean difference, 14.6; P < .05) and did exceed the MCID threshold of 10.7 (Table 8). 40 Outcome scores were compared between the OCAT and OCAT+MAT groups before surgery (P > .05) and at a minimum of 2 years after surgery (P > .05). The mean scores were significantly increased on final assessment when compared with preoperative scores (P < .01). Overall, the mean final IKDC score was 73.3 ± 18.2, the mean Lysholm score was 78.3 ± 17.4, and the mean final KOOS scores were 84.4 ± 16.2 for Pain, 69.1 ± 21.0 for Symptoms, 90.6 ± 13.5 for Activities of Daily Living, 64.6 ± 26.0 for Sport and Recreation, and 61.9 ± 22.8 for Quality of Life (Figure 6).
Pre- and Postoperative Clinical Outcomes a
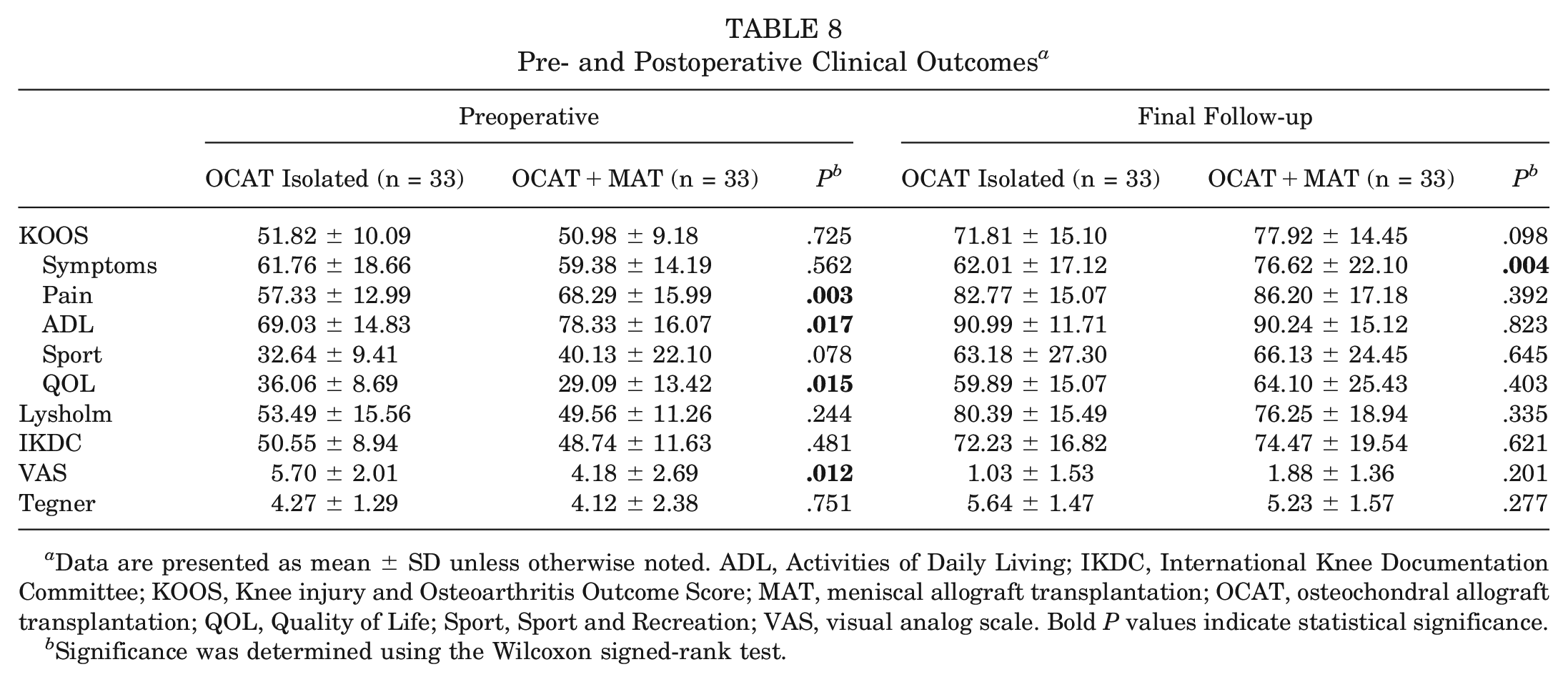
Data are presented as mean ± SD unless otherwise noted. ADL, Activities of Daily Living; IKDC, International Knee Documentation Committee; KOOS, Knee injury and Osteoarthritis Outcome Score; MAT, meniscal allograft transplantation; OCAT, osteochondral allograft transplantation; QOL, Quality of Life; Sport, Sport and Recreation; VAS, visual analog scale. Bold P values indicate statistical significance.
Significance was determined using the Wilcoxon signed-rank test.
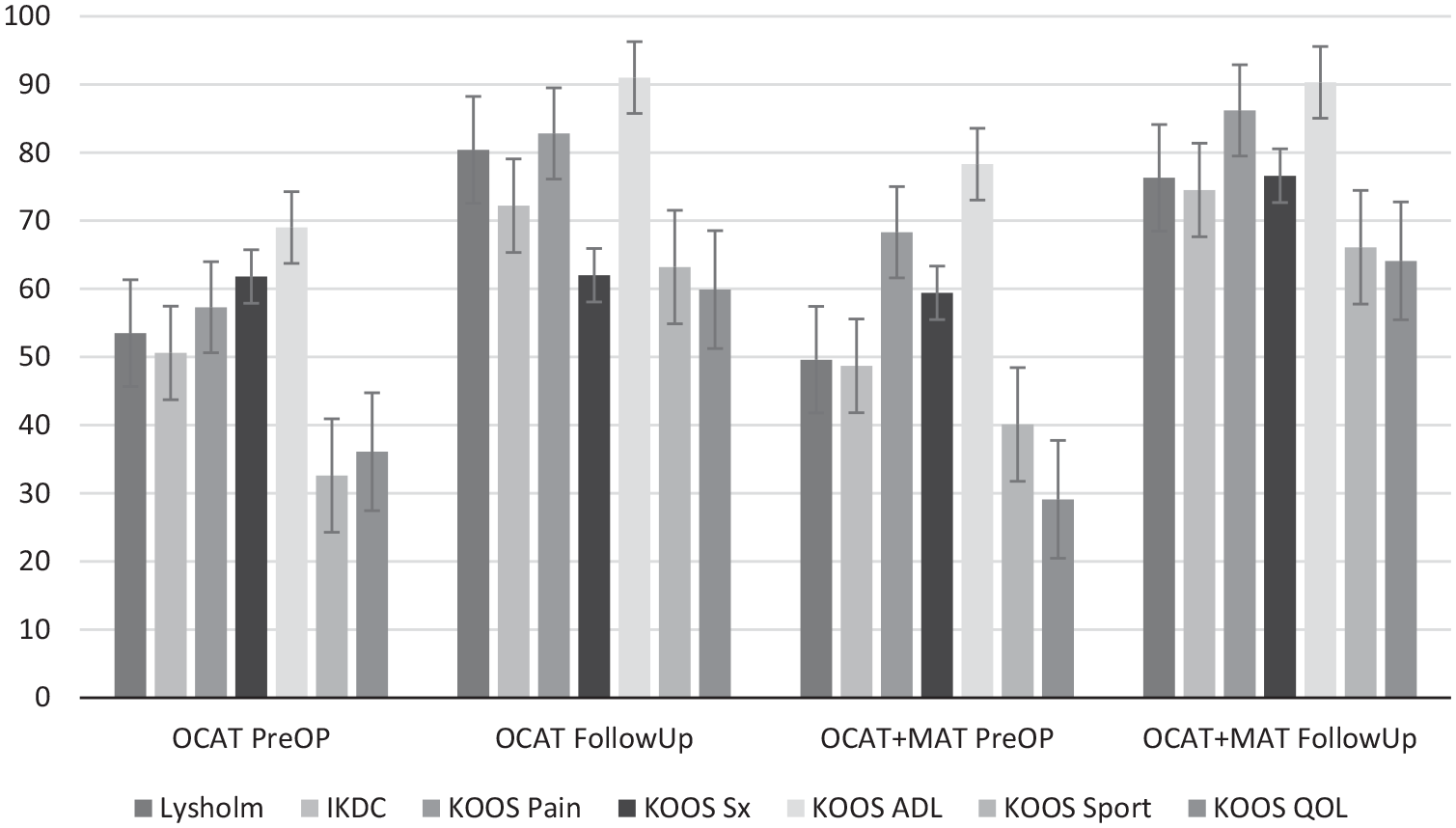
Comparison of Lysholm score, International Knee Documentation Committee (IKDC) Subjective Knee Evaluation Form, and Knee injury and Osteoarthritis Outcome Score (KOOS) results. Error bars indicate SE. ADL, Activities of Daily Living; MAT, meniscal allograft transplantation; OCAT, osteochondral allograft transplantation; PreOP, preoperatively; QOL, Quality of life; Sport, Sport and Recreation; Sx, Symptoms.
Discussion
The main finding of this study was that at midterm follow-up (mean, 67 months), patients who had undergone combined OCAT+MAT experienced comparable graft survivorship (15.2% vs 12.1%; P = .66), similar rates of patient-reported outcomes indicating a high satisfaction rate, and similar radiographic outcomes to those who had undergone isolated OCAT. In both groups, graft survivorship was high, and patient-reported outcomes were significantly improved when compared with preoperative status. No significant differences were found in pre- and postoperative Tegner activity levels between groups; however, the potential effect of activity levels on graft survival rates was accounted for in bivariate analysis. This analysis demonstrated that patients undergoing combined OCAT+MAT were at no greater risk of clinical failure (odds ratio, 1.343; 95% CI, 0.354-5.097; P = .665), regardless of preinjury activity level. These results allow for the hypothesis to be accepted in that, despite an elevated number of previous surgeries, additional surgical time, and higher complexity of cases, patients undergoing OCAT in conjunction with MAT can expect favorable outcomes and a high graft survival rate (84.8%) at 6 years. The treatment modality is a viable option for patients with meniscal deficiency and focal osteochondral lesions, and the current study can be used by orthopaedic surgeons in counseling patients and setting expectations. However, the potential lack of statistical power prompts a nuanced interpretation of our results, encouraging reflection on the long-term effectiveness and durability of the OCAT+MAT approach. Notably, the absence of statistical significance does not negate potential clinical importance, and the observed trends merit careful consideration.
This combined procedure is relatively uncommon, and therefore little is currently known about the indications, efficacy, survivorship, and associated complication rates. However, the outcomes after OCAT+MAT based on the data from the present study are within the realm of results reported by a few previous studies, which indicated a treatment failure rate of 14% to 23%.6,13,14 Although there remains a need for further investigation of the efficacy of treatment for focal cartilage defects in the presence of meniscal deficiency, increasing numbers of clinical studies have been published evaluating the short- and long-term clinical outcomes of OCAT versus alternative joint-preserving treatments. ‖ Recently, improved clinical, radiographic, and arthroscopic outcomes were reported in an experimental canine model treated for medial compartment gonarthrosis with bipolar osteochondral and meniscal allograft transplantation. 48
A former study by Frank et al 13 investigated outcomes after concurrent femoral condylar OCAT and same-compartment MAT procedures in 50 patients and reported favorable outcomes with a 5-year survivorship rate of 86%. Similar to the present study, all their patients (100%) had undergone ≥1 ipsilateral knee surgery before OCAT and often more than that (mean, 2.7 ± 1.7). This highlights that the combined procedure of OCAT+MAT is often carried out after unsuccessful treatment approaches. Similar to the Frank et al study, the current investigation was undertaken at a tertiary care center. Despite similarities in several parameters between the studies, differences in study design, concomitant surgeries, surgical technique, and rehabilitation approach make it difficult to compare the outcomes. For example, patients in their study were not matched for preoperative osteoarthritis grade and were not adjusted for by Tegner activity score. However, they reported a high survivorship (86%), similar to the survivorship found in our cohort (86%).
In 2015, Getgood and colleagues 14 reported on 48 cases of combined MAT and tibial OCAT at a mean 5-year follow-up. They noted a cumulative graft survivorship of 76%. However, their study cohort was significantly different from the one presented in the current study. In 30 of 48 patients, the indication for the combined procedure was primary osteoarthritis or cartilage damage after a tibial plateau fracture, while in our study only 2 patients demonstrated a preoperative Kellgren and Lawrence grade >2. Additionally, the surgical technique used for MAT differed significantly. Getgood et al used a compound tibial plateau osteochondral allograft with the native meniscus attached in 36 cases, while in the present study no compound grafts were used, making the clinical and surgical results difficult to compare. However, they reported a reoperation rate of 54% and a failure rate of 23%. For OCAT alone, they indicated a survivorship rate of 73% at 5 years, which is lower than the survivorship rate of 86% in the current study. These differences might be attributable to differences in initial patient cohort and surgical technique. However, the publication does not specify the pre- and postoperative Kellgren and Lawrence and ICRS grades, and therefore a direct comparison of results is difficult to achieve.
Even though radiographic parameters such as the Kellgren and Lawrence and ICRS grades did not show significant differences in preoperative status, they differed significantly at the final follow-up (P < .05). Both groups progressed in terms of cartilage status and osteoarthritis, but the OCAT+MAT group demonstrated a comparatively faster progression. The literature on radiographic outcomes of OCAT+MAT is fairly limited, but with no such parameters presented in the studies of Getgood et al 14 and Frank et al, 13 it can be hypothesized that the radiographic-detectable joint change may precede clinical symptoms in the long term. It has been shown that structural changes of the knee joint can often preface clinical symptoms.22-24,28 Supporting the current findings, Lee et al 33 compared clinical outcomes and graft survivorship of MAT between patients based on the degree and location of articular cartilage degeneration (ICRS grade ≤2 on both femoral and tibial sides vs ICRS grade 3 or 4 on either the femoral or the tibial side vs ICRS grade 3 and 4 on both sides). It was noted that while clinical survivorship was not significantly different between groups, on objective evaluation, the estimated 5-year graft survival rate was significantly lower in the high-grade bipolar cartilage lesion group. 33 However, the patient-reported outcome parameters were not significantly different between the groups. Parkinson and colleagues 42 reported that survivorship of MAT depended on preoperative cartilage status of the treated compartment, and a higher ICRS grade is associated with an elevated failure rate.
We found no clinically important differences between groups with respect to Lysholm, Tegner, IKDC, and KOOS results. Patients reported significantly improved clinical scores in both groups when compared with baseline scores. These results align well with recent findings by Cook et al, 6 who investigated outcomes after unicompartmental tibiofemoral bipolar osteochondral and meniscal allograft transplantation and found significant improvement in VAS, Patient-Reported Outcomes Measurement Information System, and IKDC scores.
The present study is unique in that it presents radiographic midterm data. Although former studies have focused on clinical and patient-reported outcomes, the current investigation enables the clinician to relate these important parameters to radiographic findings. Because of the matching methodology and the adjustment for the Tegner activity scale, concomitant MAT can be assessed as an independent variable in the treatment of patients with OCAT. The results suggest that OCAT+MAT can result in successful midterm outcomes and satisfaction in the majority of patients. OCAT+MAT for treatment of femoral condylar cartilage damage with concurrent meniscal deficiency was associated with statistically significant and clinically meaningful improvements in patient-reported outcome measures of pain and function and was on par with the thoroughly investigated treatment of isolated OCAT. Increased tibial slope was an independent risk factor for failure of the procedure.
Limitations
There are several limitations in our study design. First, the final follow-up time points ranged from 2 to 18 years. Although most failures occur within the first 2 years after OCAT, longer-term follow-up data are not yet available for this patient cohort such that conclusions must be limited to midterm outcomes. Second, the retrospective nature and nonrandomized design of the study were limitations. Although the constraints of retrospective study design are well recognized, it is important to highlight some specific limitations. Not all patients had postoperative MRI scans available. Therefore, a bias might be present as patients with symptoms are more likely to undergo further diagnostic measures than asymptomatic patients. This can result in an artificially increased postoperative ICRS grade in both cohorts. Third, a major limitation of any comparative, retrospective clinical study is treatment selection bias. However, the effects of this were mitigated through successful matching. Fourth, lateral and medial compartment locations were not evenly distributed among the groups, potentially affecting results and limiting comparability. Furthermore, it should be noted that the difference in reoperation rate and time to reoperation between the groups is arguably clinically important and that lack of statistical significance may be because of low statistical power.
Conclusion
Midterm results after isolated OCAT and OCAT+MAT show high rates of healing and sustainable subjective improvement of knee function and quality of life. A survival rate of 87% was noted at a mean follow-up of 5.6 years. The cohorts did not significantly differ in terms of failure rate and patient-reported outcomes. However, it should be noted that the difference in reoperation rate and time to reoperation between the groups is arguably clinically important and that lack of statistical significance may be because of low power. These results imply that isolated OCAT is an efficient joint-preserving treatment that can be combined with MAT in well-selected patients with meniscal insufficiency without negatively influencing global clinical outcomes.
Footnotes
Submitted March 7, 2023; accepted December 20, 2023.
One or more of the authors has declared the following potential conflict of interest or source of funding: This study was supported by Foderaro-Quattrone Musculoskeletal-Orthopaedic Surgery Research Innovation Fund. M.H. acknowledges research support by the Deutsche Forschungsgemeinschaft (grant No. 466023693). B.A.L. has received royalties and consulting fees from Arthrex; consulting fees from Smith & Nephew; and speaking fees from Linvatec. D.B.F.S. has received consulting fees from Smith & Nephew. M.J.S. has received royalties and consulting fees from Arthrex and research support from Stryker. A.J.K. has received research support from Aesculap/B.Braun, Arthrex, Arthritis Foundation, Ceterix, and Histogenics; consulting fees from Arthrex, JRF Ortho, Vericel, and Responsive Arthroscopy; royalties from Arthrex and Responsive Arthroscopy; honoraria from Joint Restoration Foundation, Vericel, and Musculoskeletal Transplant Foundation; a grant from DJO; and hospitality payments from Ceterix Orthopaedic, Gemini Mountain Medical, and Smith & Nephew. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.