
Abstract
Background:
Patellofemoral instability commonly occurs during sports activities. The return to sports (RTS) rate for pediatric patients after bilateral medial patellofemoral ligament reconstruction (MPFLR) is unknown.
Purpose/Hypothesis:
The purpose of this study was to evaluate RTS outcomes for pediatric patients undergoing bilateral MPFLR. It was hypothesized that (1) fewer pediatric patients would RTS after bilateral MPFLR compared with unilateral MPFLR and that (2) for those in the bilateral cohort who were able to RTS, fewer patients would attain the same level of play as or higher level than the preinjury level.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
We prospectively collected RTS data on retrospectively identified matched cohorts of patients aged ≤18 years who underwent unilateral and bilateral MPFLR. We matched each participant with bilateral MPFLR at a 1 to 2 ratio with a participant with unilateral MPFLR by concomitant procedure, age, and sex. Postoperative complications and preoperative imaging measurements were collected from medical records. Patient-reported outcomes were obtained using a current Single Assessment Numeric Evaluation score collected at the time of primary outcome data.
Results:
We matched 16 participants (mean age, 14 years) who underwent bilateral MPFLR to 32 participants (mean age, 14.3 years) in a corresponding unilateral MPFLR cohort. We found a significant decrease in RTS rates for pediatric patients after bilateral MPFLR when compared with unilateral MPFLR (69% vs 94%; P = .03). Among those who returned to sports, there was no difference in the level of play achieved. For participants who did not RTS or returned at a lower level of play after bilateral MPFLR, 57% cited fear of reinjury as the primary reason. There were no differences in postoperative complications or current Single Assessment Numeric Evaluation scores between cohorts. The bilateral cohort had a significantly higher Caton-Deschamps index compared with the unilateral cohort, although the absolute difference was small (1.3 vs 1.2; P = .005).
Conclusion:
We found that pediatric patients have a lower RTS rate after bilateral MPFLR when compared with a matched unilateral MPFLR cohort. No differences in the level of play were achieved among those who returned to sports. Fear of reinjury was a commonly cited reason for not returning to sports.
Keywords
Patellofemoral instability is a common knee injury among adolescents, with an overall annual incidence of patellar dislocation of 23 to 77 per 100,000 persons and up to 147 per 100,000 in the age range of 14 to 18 years.6,18,19,25,28 After initial patellar dislocation, 5% to 9% of patients sustain contralateral patellar dislocations.4,24 Consequences of patellofemoral instability include cartilage injury, osteochondral fracture, persistent pain, patellofemoral arthritis, and decreased physical activity.25,26,28 Risk factors for recurrent patellofemoral instability include trochlear dysplasia, patella alta, tibial tuberosity–trochlear groove (TT-TG) distance of >20 mm, skeletal immaturity, and contralateral dislocation.4,10,13,24,25
Although unilateral medial patellofemoral ligament (MPFL) reconstruction (MPFLR) outcomes have been extensively studied, little is known about bilateral MPFLR outcomes. Return to sports (RTS) outcomes are particularly interesting, as initial patellar dislocation frequently occurs during sports activities at reported rates of 61% to 72%.1,6,28 RTS after unilateral MPFLR has been reported to be 84% to 100%, with or without combined procedures such as tibial tubercle osteotomy or trochleoplasty.15,16,21,26 However, with sequential bilateral MPFLR surgeries, the prolonged time away from sports and the potential for additive psychological barriers may have a negative effect on RTS, particularly in the young and highly active population.
The study objective was to evaluate RTS outcomes for pediatric patients undergoing bilateral MPFLR. Given the association of patellar dislocations with athletic activities, RTS outcomes are an important prognostic metric for this patient population and may aid orthopaedic surgeons in counseling patients regarding postoperative recovery expectations. Our hypotheses were as follows: (1) fewer pediatric patients would RTS after bilateral MPFLR compared with unilateral MPFLR, and (2) for those in the bilateral cohort who were able to RTS, fewer patients would attain the same level of play as or higher level than the preinjury level.
Methods
We retrospectively reviewed prospectively collected data on RTS in matched cohorts of patients who underwent unilateral and bilateral MPFLR. This study was approved by our institutional review board and categorized as no more than minimal risk to patients. Informed consent was obtained for each participant as specified by the institutional review board.
Inclusion/Exclusion Criteria
We identified patients aged ≤18 years who underwent an MPFLR procedure by the senior author (E.A.C.) between 2017 and 2023. We only included patients who participated in sports preoperatively at any level of competition or organization. We included patients who underwent concomitant procedures with MPFLR—including tibial tubercle osteotomy, Roux-Goldthwait procedure, lateral retinacular release, open reduction with internal fixation of osteochondral fracture, loose body removal, osteochondritis dissecans drilling, microfracture, partial meniscectomy, meniscal repair, chondroplasty, and matrix-induced autologous chondrocyte implantation (MACI) procedures. However, we excluded those who underwent MPFL repair, vastus medialis oblique advancement, or medial quadriceps tendon-femoral ligament reconstruction. We also excluded patients with high-grade ligamentous injuries to the cruciate or collateral ligaments or those with knee (tibiofemoral) dislocations.
Matching
After applying the inclusion and exclusion criteria, we found 18 patients who underwent staged bilateral MPFLR and 78 patients who underwent unilateral MPFLR who also participated in sports preoperatively (Figure 1). The senior author does not perform simultaneous bilateral MPFLR during a single index procedure. We individually matched each procedure of the 18 patients in the bilateral MPFLR cohort at a 1 to 2 ratio to 36 patients who underwent unilateral MPFLR. Listed in order of priority, we matched cohorts based on concomitant procedures, age ±2 years, and sex. We grouped similar concomitant procedures on the extent of surgery and potential effects on postoperative recovery protocols by the following: (1) isolated MPFLR; (2) distal patellar tendon realignment procedure (tibial tubercle osteotomy, Roux-Goldthwait); (3) MACI procedure; (4) open reduction with internal fixation of osteochondral fracture and meniscal repair; (5) osteochondritis dissecans drilling and microfracture; and (6) loose body removal, chondroplasty, partial meniscectomy, and lateral retinacular release. All patients were matched to the concomitant procedures protocol, with 69% matched to all 3 confounders, 22% matched to the procedure and age, and just 9% matched to only the procedure. We could not contact 2 of the patients who had bilateral MPFLR to collect RTS data. We also were unable to contact 3 of the patients who had unilateral MPFLR who were initially matched, and an additional 2 families in this cohort declined participation in the study, which required us to rematch using the same protocol as above.
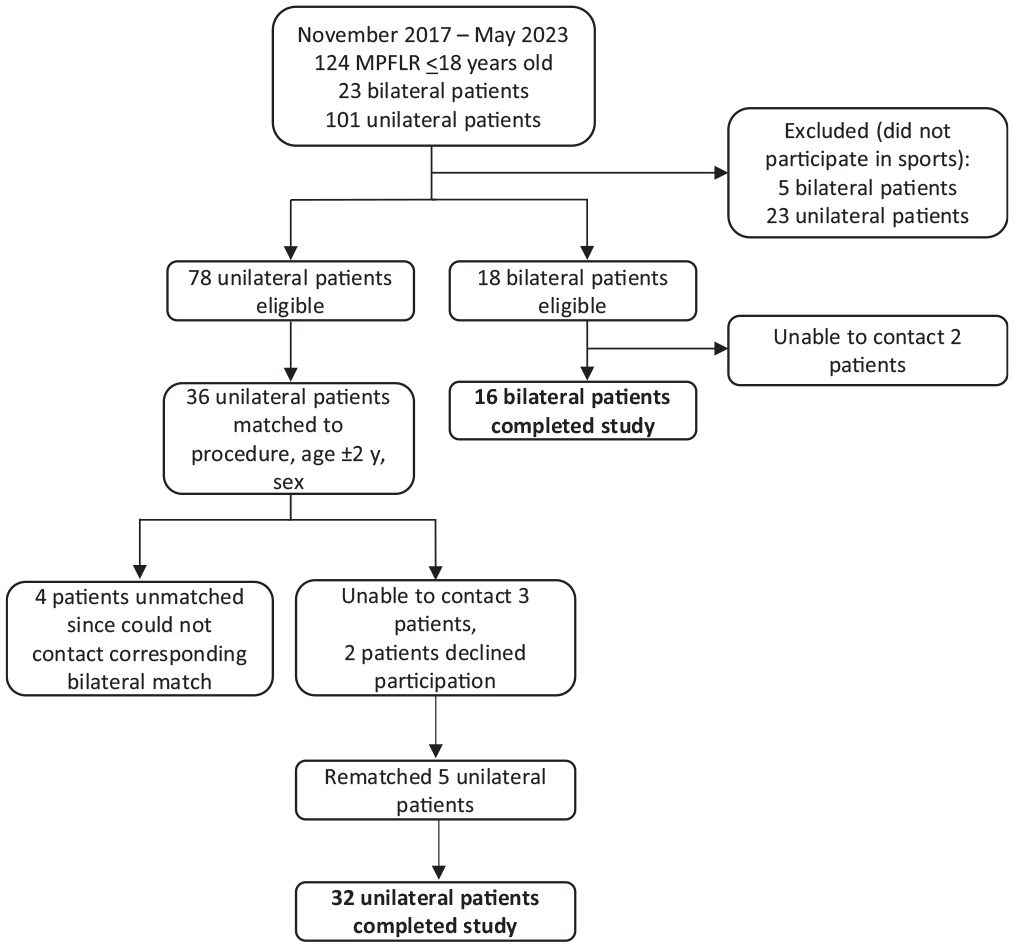
Cohort matching flowchart. MPFLR, medial patellofemoral ligament reconstruction.
Preoperative Radiographic Measurements
Patella alta was assessed using the Caton-Deschamps index (CDI), which is the ratio of the distance from the anterior tibial plateau to the inferior aspect of the patellar articular cartilage to the length of the patellar articular surface. 23 Values of ≥1.3 were considered to be patella alta. The TT-TG distance was measured on preoperative magnetic resonance imaging scans as computed tomography studies were not routinely obtained. Trochlear dysplasia was evaluated using lateral radiographs and magnetic resonance imaging scans. On lateral radiographs, we classified trochlear dysplasia according to the Dejour classification.5,23 Because the Dejour classification has poor interrater reliability,2,22 we also measured lateral trochlear inclination as the angle between the most proximal lateral trochlear cartilage and a line connecting the posterior femoral condyles as described by Carrillon et al 3 and Joseph et al. 11 Values <11° have been associated with trochlear dysplasia contributing to patellofemoral instability. 3
Surgical Technique
All patients were indicated for MPFLR for recurrent patellofemoral instability. The decision to include concomitant procedures was made on an individual basis depending on associated pathology (eg, chondral or osteochondral injury) and other anatomic considerations (eg, elevated TT-TG distance). The physeal-sparing technique was used for patients who were skeletally immature with significant growth remaining. Each procedure began with an examination under anesthesia and a diagnostic arthroscopy. A semitendinosus allograft was prepared to a folded diameter of 6 to 7 mm and a folded length of 110 to 120 mm. The graft was secured to the medial patella using 2 anchors—1 placed at the midaxial position and 1 placed 10 mm proximal to the first anchor. The graft was shuttled between layers 2 and 3 of the knee to an incision made over the medial knee, centered at the medial epicondyle. The site for graft fixation on the medial femur was identified via palpation of anatomic landmarks and fluoroscopic identification of the Schöttle point. A 6 to 7 mm–diameter tunnel was created at this site, and the graft was inserted into the tunnel. With the knee in low flexion for the patella to engage with the trochlea, the graft was fixed with a soft tissue screw. The full range of motion was checked to ensure the graft was not overtensioned. The wounds were irrigated and closed in layers, followed by the placement of a hinged knee brace locked in full extension. Patients were restricted to minimal (“toe-touch”) weightbearing for the first week, then they were allowed to bear weight as tolerated and advance range of motion as tolerated after the first week. Physical therapy was initiated after the first week. The surgical technique was the same for sequential bilateral procedures as it was for unilateral procedures.
Outcomes
Our primary outcome was the percentage of patients who returned to sports and the level of play or ability that they returned to compared with preoperative or preinjury levels. RTS data were obtained ≥1 year after unilateral MPFLR and ≥1 year after the second knee MPFLR for the bilateral cohort. We assessed the highest level attained postoperatively to reduce the effect of recall error. If applicable, we inquired why patients did not return to the preinjury level of play. After MPFLR with and without combined procedures, the senior author typically releases patients to full activity by 5 to 6 months postoperatively, which would allow for at least an additional 6 months to gradually advance activity level before collection of primary outcome data. Our primary RTS data were collected prospectively via recruitment during routine postoperative follow-up visits with the senior author or by contacting the patient and/or his or her guardian by telephone.
Secondary outcomes involved the time to RTS, patient-reported outcomes (PROs), and retrospective chart review data to evaluate common postoperative complications. The time to RTS was described as a secondary outcome, as it was heavily influenced by standardized rehabilitation protocols. PROs were obtained using a current Single Assessment Numeric Evaluation (SANE) score collected at the time of primary outcome data.20,27,30,31 We asked patients to rate their current knee function on a scale of 0 to 100, with 100 being normal. This was selected to provide insight into the current knee function while minimizing the time burden to participants and reducing the risk of recall error. Time to RTS and SANE scores were collected prospectively. A retrospective chart review was performed ≥1 year after surgery for secondary postoperative complications, including recurrent patellofemoral instability, fractures, surgical-site infections, knee pain >3 months after surgery, knee stiffness, and revision procedures. Recurrent patellofemoral instability was defined as either postoperative patellar subluxation or dislocation.
Exploratory outcomes were also obtained using preoperative imaging studies to evaluate underlying anatomic risk factors for recurrent patellofemoral instability4,13,24,25 Secondary postoperative complication outcomes and exploratory anatomic imaging measurements were collected to provide potential insight into any differences found between unilateral and bilateral MPFLR primary outcomes.
Statistical Analysis
Unadjusted statistical analysis was used to compare outcomes between the matched cohorts. Chi-square test was used to compare categorical outcomes, and t test was used for continuous data. Statistical significance was set at an alpha level of .05. Prestudy power calculations were performed to determine that this study was adequately powered to detect a significant difference in primary outcomes. Because there were no known data for RTS outcomes after bilateral MPFLR at the time of our study development, we derived estimations from a study on anterior cruciate ligament reconstruction (ACLR) that reported a >80% RTS after unilateral ACLR but only a 40% RTS after subsequent contralateral ACLR. 29 Even though this is not ideal because of the differences between anterior cruciate ligament injuries and patellar instability, outcomes after ACLR provide the most studied data on knee ligamentous reconstruction and rehabilitation. Given that our bilateral MPFLR patient pool was limited in overall size, we increased the matching ratio to 1 to 2 to increase the power of our study, noting that there were diminishing returns for higher ratios. This also allowed us to match a patient who underwent unilateral MPFLR with each knee in the bilateral cohort. Power was calculated to be 0.81 for a 1 to 2 ratio (16 with bilateral MPFLR, 32 with unilateral MPFLR). As all potential participants were patients of the senior author, we expected a high participation rate in the study. Analyses were performed using SAS Version 9.4 (SAS Institute Inc).
Results
We identified 18 patients and recruited 16 participants who underwent bilateral MPFLR; the patients’ age ranged from 9 to 17 years, with a mean age of 14 years (SD, 1.8 years), and 62.5% of them were male (Table 1). There was a mean of 1.2 years (SD, 0.8 years) between MPFLR procedures in the bilateral cohort, with 50% occurring within 1 year. Only 1 participant in the bilateral cohort had >2 years between procedures. The mean age of the bilateral cohort at the time of the second MPFLR procedure was 14.5 years (SD, 1.9 years [range, 9-17 years]). For participants with bilateral MPFLR who did not RTS, the mean age at the second procedure was 13.8 years (SD, 1.3 years [range, 12-15 years]), and the mean time between procedures was 0.7 years. Each knee of a participant in the bilateral cohort was matched via our protocol to the knee of a participant who underwent unilateral MPFLR. The unilateral cohort comprised 32 patients, with a mean age of 14.3 years (SD, 1.4 years [range, 12-17 years]), and 50% of them were male. The mean age of participants in the unilateral cohort who did not RTS was 15 years (SD, 1 year [range, 14-16 years]). Patient characteristics are presented in Table 1.
Patient Characteristics a
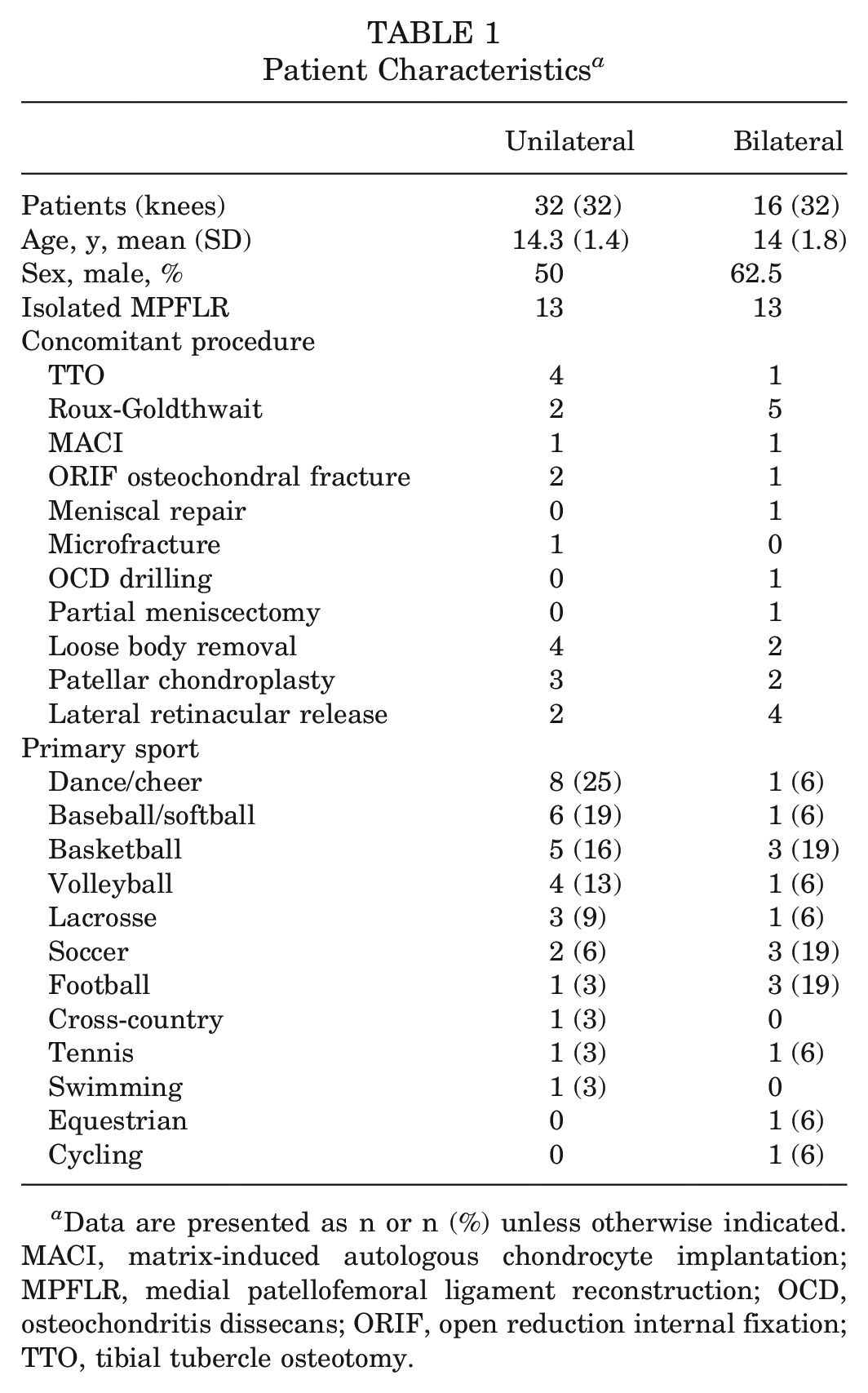
Data are presented as n or n (%) unless otherwise indicated. MACI, matrix-induced autologous chondrocyte implantation; MPFLR, medial patellofemoral ligament reconstruction; OCD, osteochondritis dissecans; ORIF, open reduction internal fixation; TTO, tibial tubercle osteotomy.
A total of 41% (13/32) of procedures in both cohorts were isolated MPFLR. Six procedures in each cohort included a distal patellar tendon realignment procedure because of a high TT-TG distance, and 1 procedure in each group included the MACI procedure. The remainder of the concomitant procedures as well as the participants’ primary sport are included in Table 1.
A significantly lower percentage of participants who underwent bilateral MPFLR successfully returned to sports by ≥12 months after the second procedure when compared with those who underwent unilateral MPFLR (69% vs 94%: P = .03) (Table 2). Among those who returned to sports, there were no significant differences in the level of play obtained postoperatively, with 81% of the bilateral cohort achieving the same or higher levels of play compared with 67% of the unilateral cohort (P = .64). Also, the time to RTS was similar between the cohorts—the bilateral cohort returned 8.4 months (SD, 5.8 months) after the second procedure, and the unilateral cohort returned to sports at 7.3 months (SD, 3.4 months) after surgery (P = .47). Of participants in the bilateral MPFLR cohort who did not RTS or returned at a lower level, 57% cited fear of reinjury as the reason, 29% attributed it to the long recovery, and just 1 patient (14%) reported that there was loss of interest (Table 3). However, 25% of patients in the unilateral MPFLR cohort noted fear of reinjury as the reason for either not returning to sports or returning at a lower level, with 33% attributing it to a long recovery period and 42% reporting knee pain as the reason. Qualitative analysis was not performed on these data. There was also no difference in current SANE scores, with both cohorts rating their current knee function as >90% (P = .33) (Table 4).
Comparison of RTS Outcomes After Bilateral Versus Unilateral MPFLR a
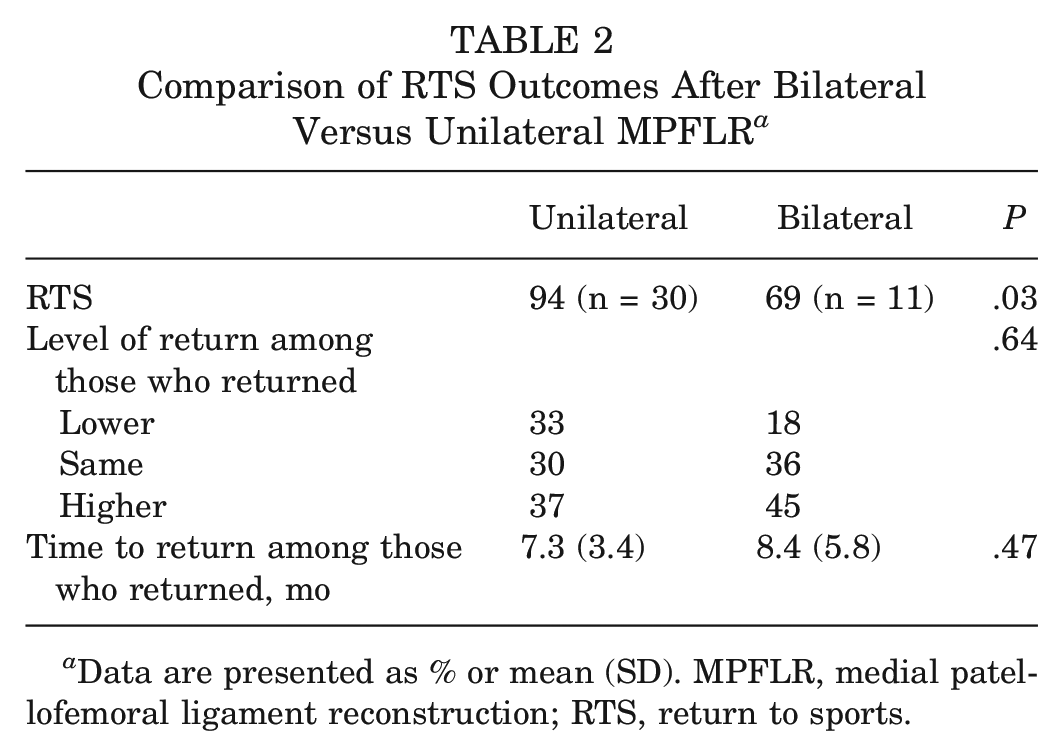
Data are presented as % or mean (SD). MPFLR, medial patellofemoral ligament reconstruction; RTS, return to sports.
Reason for Not Returning to Sports or Returning at a Lower Level of Play After MPFLR a
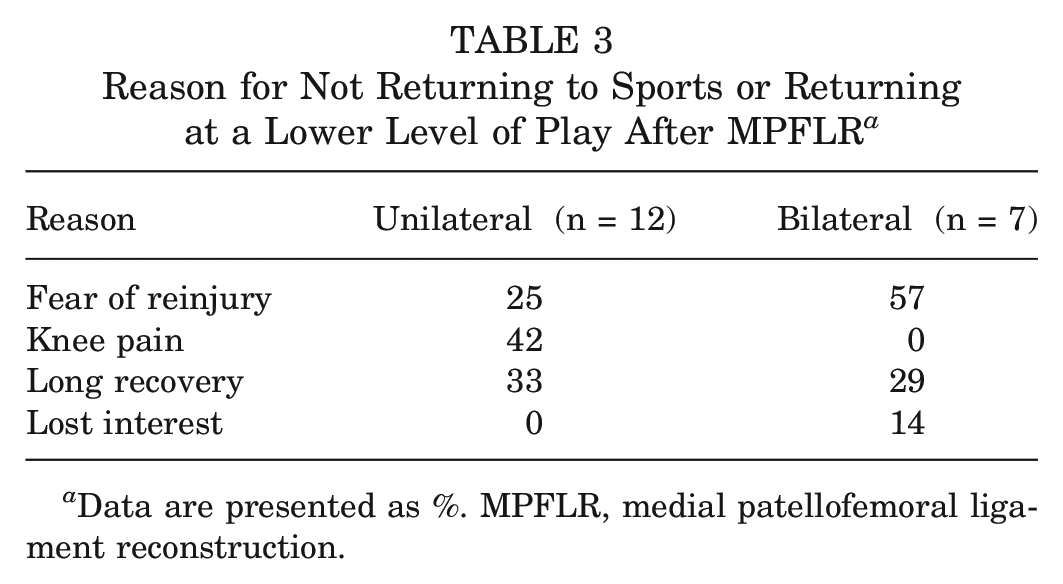
Data are presented as %. MPFLR, medial patellofemoral ligament reconstruction.
Complications and PROs After MPFLR a
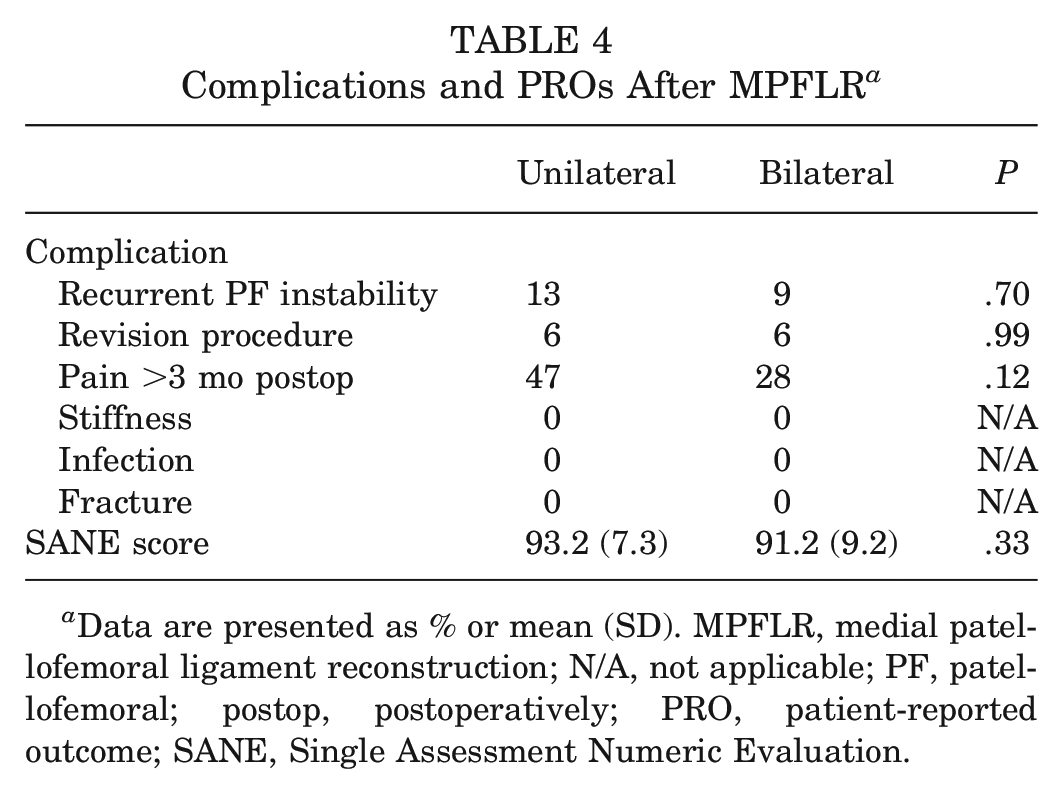
Data are presented as % or mean (SD). MPFLR, medial patellofemoral ligament reconstruction; N/A, not applicable; PF, patellofemoral; postop, postoperatively; PRO, patient-reported outcome; SANE, Single Assessment Numeric Evaluation.
No significant differences were observed between cohorts for postoperative complications (Table 4). Also, 13% of participants had recurrent patellofemoral instability after unilateral MPFLR compared with 9% after bilateral MPFLR (P = .70). For both cohorts, 6% of participants underwent a revision procedure for recurrent instability. Knee pain was recorded in postoperative clinic notes >3 months after surgery in 47% of participants after unilateral MPFLR and 28% after each procedure in bilateral MPFLR (P = .12). Greater than two-thirds of recorded knee pain in both groups was documented as mild and/or resolved spontaneously by the following clinic appointment. We did not record any instances of postoperative fracture, infection, or prolonged knee stiffness in either cohort.
Results from exploratory outcomes obtained from preoperative imaging are shown in Table 5. We found that participants undergoing bilateral MPFLR had a higher CDI compared with those undergoing unilateral MPFLR (1.3 vs 1.2, respectively; P = .005). This resulted in 66% of the bilateral MPFLR cohort's being categorized as having patella alta as opposed to just 38% of the unilateral MPFLR cohort (P = .04). In regard to trochlear dysplasia, the Dejour classification trended toward significance, with most participants undergoing unilateral MPFLR classified as having Dejour A/B, while most participants’ knees in the bilateral MPFLR were classified as having Dejour C/D (P = .06). The lateral trochlear inclination angle did not demonstrate a significant difference between cohorts (bilateral, 7.4° vs unilateral, 6°; P = .47). As expected, based on matched cohorts for concomitant procedures, there was no difference in the TT-TG distance between groups, and both had 19% of knees measuring as high TT-TG states (>20 mm).
Preoperative Imaging Measurements and Anatomic Characteristics a
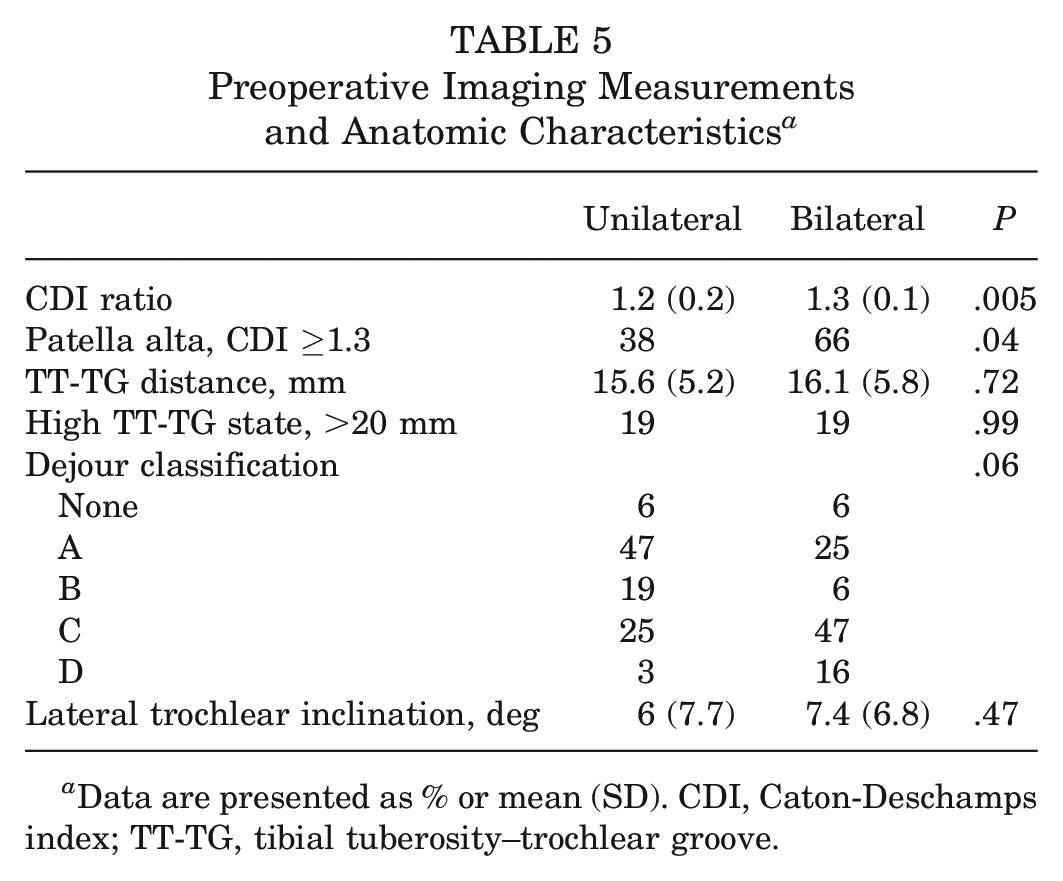
Data are presented as % or mean (SD). CDI, Caton-Deschamps index; TT-TG, tibial tuberosity–trochlear groove.
Discussion
In this retrospectively matched cohort study with prospectively collected primary outcome data, we found a significant decrease in RTS rates for pediatric patients after bilateral MPFLR when compared with unilateral MPFLR. While just 69% of patients returned to sports after bilateral MPFLR, compared with 94% after unilateral MPFLR, there was no difference in the level of play achieved postoperatively among those who returned to sports.
Recently, Li et al 14 published RTS rates after bilateral and unilateral MPFLR that were not statistically different (62% vs 72%, respectively). However, the mean ages of patients in their study were 25 and 22 years for their bilateral and unilateral MPFLR cohorts, respectively. It is unclear from their study design whether they were measuring return to organized sports as opposed to return to general athletic activities. Compared with adult patients, adolescents typically have increased opportunities for participation in organized sports. Time away from sports can have a greater effect on future participation as their peers continue to advance during rapid neuromuscular development and acquisition of sport-specific skills. Therefore, it may be expected that RTS outcomes would differ in a pediatric or adolescent population. In addition, their finding of just 72% of patients returning to sports after unilateral MPFLR is lower than that in previous reports, which may account for not finding a significant difference between their cohorts.16,21 However, their reported RTS rate after bilateral MPFLR of 62% was similar to our finding of 69%.
More broadly, Platt et al 21 performed a systematic analysis and meta-analysis on RTS after MPFLR. They included 23 articles and 786 patients in the final analysis. They found that 92.8% of patients returned to sports at a mean of 6.7 months, of whom 71.3% returned to at least the same preinjury level. Patients who underwent MPFLR with a concomitant osteotomy had lower RTS rates compared with those without an osteotomy (86.9% vs 95.4%); nonetheless, this was not significant on metaregression analysis. The most common reason for patients who returned at a lower level of play was fear of reinjury (39.7%). They did not report any data on patients with unilateral versus bilateral MPFLR. Liu et al 16 reported on RTS data of 91 patients within a retrospective case series who underwent unilateral or bilateral MPFLR without concomitant osteotomy or distal patellar tendon realignment procedures. They found that 94.5% of patients returned to sports and 74% attained at least preoperative levels of play. They did not perform a subgroup analysis on unilateral versus bilateral outcomes. Our findings of 94% of patients returning to sports after unilateral MPFLR were consistent with the reported values by Platt et al and Liu et al; however, our data showed that patients RTS at a much lower rate after a subsequent MPFLR on the contralateral knee. It is unclear how many patients underwent bilateral MPFLR in the studies above and how that may have affected their results.
Similar to the above studies, we also found fear of reinjury in both of our cohorts contributing to either not returning to sports or returning at a lower level, with 57% in the bilateral cohort and 25% in the unilateral cohort citing this as the primary reason. This highlights the growing evidence of psychological influence on RTS outcomes after MPFLR and other knee reconstructive procedures.7,9,12 More work is needed to determine whether targeted interventions to increase confidence in postoperative knee performance can improve patient outcomes.
We did not discover convincing evidence in our secondary and exploratory outcomes that explains why patients returned to sports at lower rates after bilateral MPFLR. There were no significant differences in postoperative complications between cohorts, and the only significant difference in preoperative imaging measurements was a higher CDI ratio in patients who underwent bilateral MPFLR. As groups were matched primarily by concomitant procedures, there were no additional procedures in the bilateral group that addressed patellar height. However, the significance of this finding is questionable because the absolute difference in the CDI ratio between cohorts was just 0.1. Although our bilateral cohort trended toward a higher Dejour classification for trochlear dysplasia, we found no difference in lateral trochlear inclination angles between groups. Furthermore, trochlear dysplasia is a known risk factor for persistent patellofemoral instability,4,13,24,25 but we found no difference in recurrent instability or revision procedures. This also undercuts trochlear dysplasia as an explanation for poorer RTS outcomes after bilateral MPFLR. It is possible that anatomic differences between groups contributed to lower RTS rates; nonetheless, we found no compelling evidence that these differences were major underlying causes for lower RTS rates in the bilateral group. Despite the difference in RTS rates, patients in both cohorts overall perceived their knees to be doing well with similar SANE scores, rating their current knee function as >90 out of 100. Another area for future research is seeking a better understanding of other factors that contribute to RTS outcomes.
Orthopaedic surgeons utilize personal experience from their training and practice along with data reported in the literature to guide discussions with patients on postoperative outcomes and rehabilitation. Although >90% of patients returned to sports in some capacity after MPFLR per previous reports, it is important to note that just over two-thirds of patients regained the same level or higher levels of play.15,16,21 Although these data are useful when counseling patients and their families, it was not previously clear whether it also applied to patients after bilateral MPFLR. It stands to reason that patients may have poorer outcomes after bilateral MPFLR given that the theoretical risks for complications are doubled and they also have longer postoperative rehabilitation time that equates to increased time away from sports. To this point, Hiemstra et al 8 studied a cohort of 224 patients who underwent an isolated MPFLR, and they reported that patients with bilateral symptoms had significantly lower PROs compared with those with only unilateral symptoms. The difference in outcome scores between the 2 groups exceeded the minimally important difference on the patellofemoral instability–specific scale used in the study. Their findings of lower quality of life with bilateral symptoms add to our work demonstrating worse outcomes after bilateral MPFLR. A better understanding of these clinically important outcomes for pediatric patients after bilateral MPFLR can assist surgeons in preoperative counseling and management of postoperative expectations on recovery and rehabilitation.
The limitations of our study include use of retrospective cohorts and heterogeneity of the concomitant surgical procedures. Although we prospectively collected primary outcome data, the retrospective design of the study introduced a potential for recall bias. However, we expect that patients will accurately remember whether they did or did not RTS after surgery, even if they completed their recovery period several years ago. However, the level of play they returned to has a higher risk for recall bias. Although our data suggest that there is no difference in the level of sports attained among those able to RTS in either cohort, it is important to be cautious in the interpretation of these results. Our study was powered to detect a difference in whether or not patients could RTS but not specifically how they return. Likewise, this study was underpowered for the secondary outcomes, which limits our ability to contextualize our findings. We also had variable time from the procedure to the collection of RTS outcomes, but among patients in both cohorts who returned to sports, the mean time to return to play was far earlier than the earliest time point of data collection—at least 1 year after the surgery or the second procedure for the bilateral cohort. It is unknown how our results would be affected by a prospective study design or a longer follow-up period. Because of the limited potential patient population for bilateral MPFLR, we included patients who had concomitant pathology from the patellar instability events or unrelated pathology identified on preoperative imaging that warranted surgical intervention at the time of MPFLR. To account for this heterogeneity, we matched patients primarily on the concomitant procedures. In addition, because of the difference in skeletal maturity among participants, we categorized patients who underwent combined tibial tubercle osteotomy or Roux-Goldthwait procedures together as distal patellar tendon realignment procedures. Although both are described techniques for reducing recurrent patellofemoral instability for patients with high TT-TG distances, there are no comparative outcome studies between these procedures. 17 Although the additional pathology and procedures could affect RTS rates, matching participants reduces this effect and allows for a broader application of the findings— considering the range and frequency of concomitant procedures performed in the setting of patellar instability.
Conclusion
We found that pediatric patients had a lower RTS rate after bilateral MPFLR when compared with a retrospectively matched unilateral MPFLR cohort. Fear of reinjury was a commonly cited reason for not returning to sports. Future work should be aimed at confirming these findings using a prospective study design and determining causes for lower RTS rates after bilateral MPFLR as potential targets for intervention.
Footnotes
Submitted September 7, 2023; accepted February 2, 2024.
One or more of the authors has declared the following potential conflict of interest or source of funding: E.A.C. and L.M.S. have received support for education from Pinnacle/Arthrex. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.