
Abstract
Background:
The potential influence of a preoperative anterolateral ligament (ALL) lesion seen on magnetic resonance imaging (MRI) on the mid- and long-term surgical outcomes of anterior cruciate ligament (ACL) reconstruction is still controversial.
Purpose:
To evaluate the clinical outcomes and failure rate of isolated ACL reconstruction at a minimum 5-year follow-up in patients with and without ALL injury diagnosed preoperatively using MRI.
Study Design:
Cohort study; Level of evidence, 2.
Methods:
A prospective cohort of patients with acute ACL injury was divided into 2 groups based on the presence (ALL injury group) or absence (control group) of ALL injury on preoperative MRI. This is a longer-term follow-up study of a previously published study that had a minimum 2-year follow-up. Both groups underwent anatomic isolated reconstruction of the ACL. The Lysholm and subjective International Knee Documentation Committee scores, KT-1000 arthrometer and pivot-shift tests, reconstruction failure rate, incidence of contralateral ACL injury, presence of associated meniscal injury, and presence of knee hyperextension were evaluated. The evaluation at the 5-year follow-up was also compared with the same patient’s evaluation at 2 years of follow-up.
Results:
A total of 156 patients were evaluated. No significant differences were found between the groups in the preoperative evaluation. In the postoperative evaluation, patients in the ALL injury group had a higher reconstruction failure rate (14.3% vs 4.6% for the control group; P = .049) and worse clinical outcomes according to the Lysholm scores (85.0 ± 10.3 vs 92.3 ± 6.6; P < .00001). Although the pivot-shift test results were similar, anteroposterior translation using the KT-1000 arthrometer revealed worse results for the ALL injury group (2.8 ± 1.4 mm vs 1.9 ± 1.3 mm; P = .00018). Patients in the ALL injury group also had an increase in KT-1000 arthrometer values from 2 to 5 years (2.4 ± 1.6 vs 2.8 ± 1.4; P = .038). Patients in the control group had no differences in outcomes from 2 to 5 years of follow-up.
Conclusion:
Combined ACL and ALL injuries were associated with significantly less favorable outcomes than were isolated ACL injuries at a minimum follow-up of 5 years after isolated ACL reconstruction with hamstring autograft. Patients with concomitant ALL injury showed a higher failure rate and worse functional scores. Also, knee stability tended to slightly worsen from 2 to 5 years in cases of associated ALL injury.
The anterolateral ligament (ALL) of the knee has been the subject of in-depth scrutiny, encompassing anatomic, biomechanical, and radiological dimensions.6,26 Clinical investigations have elucidated that combining an ALL reconstruction with anterior cruciate ligament (ACL) reconstruction in high-risk patients yields a diminished risk of failure and enhanced functional outcomes.7,12,27 Rather than debating whether to undertake extra-articular reinforcement, some authors posit that the discussion should focus on the circumstances under which it should be performed. Even though there exists compelling evidence of the advantages conferred by concurrent ALL and ACL reconstruction, there is an unresolved question regarding the potential influence of preoperative magnetic resonance imaging (MRI)–documented ALL injuries on the mid- and long-term surgical outcomes.
The incidence of ALL and anterolateral structure injuries combined with an acute ACL rupture varies in the literature.4,10,11,24 Initial MRI-based investigations reported concomitant injury to the ALL in 40% of patients with ACL ruptures. Monaco et al 21 showed that MRI is highly sensitive, specific, and accurate for the detection of abnormalities of the ALL/anterolateral capsule and shows a high percentage of agreement with surgical findings. The healing potential of the ALL remains an understudied topic. Lee et al 17 scrutinized this parameter and documented poor healing in around 70% of patients after 1 year. Saithna et al, 24 using 3-dimensional MRI protocols, found only a 30.3% healing rate 12 months after injury. The nonhealing of the ALL holds clinical significance, as biomechanical analyses suggest that isolated ACL reconstruction fails to restore normal knee biomechanics in cases of concomitant acute anterolateral structure injuries. 16
A few investigations have indicated less favorable clinical outcomes in the presence of ALL injuries alongside ACL injuries. However, they consist of shorter follow-up or retrospective studies that preclude more robust conclusions.3,15 Our group has previously reported a rerupture rate of 10.2% after isolated ACL reconstruction in the group with associated ALL injury, as opposed to 1.4% in the group with isolated ACL injuries, at a minimum follow-up of 2 years. 25 However, the literature lacks studies on this subject with a longer follow-up.
Thus, the primary objective of this prospective cohort study was to compare clinical and functional outcomes and the failure rate in the same cohort undergoing isolated ACL reconstruction in acute cases, with or without concurrent anterolateral knee structure injuries documented preoperatively using MRI, with a minimum follow-up of 5 years. We hypothesized that patients with a preoperative ALL injury would have worse functional outcomes and a higher failure rate than patients without anterolateral injuries.
Methods
The study was approved by the ethics committee of our institution (internal reference number CAAE 83486118.3.0000.0068), and informed consent was obtained. Between March 2015 and January 2018, patients with an acute ACL injury with indication for surgical treatment were included in a prospective cohort. Patients with associated injuries requiring additional surgical procedures, such as osteotomy, peripheral ligament reconstruction, posterior cruciate ligament reconstruction, or cartilage injury requiring treatment, or in whom the ALL was not visualized on MRI, were excluded from the study. No age limits were established and patients with meniscal injuries were included.
All patients with a clinical diagnosis of acute ACL injury underwent confirmatory MRI examination in the acute phase (<3 weeks after the injury) and were evaluated for injury of the ALL. The MRI examinations were all performed on 1.5-T scanners (Aera, Siemens Medical Solutions; Espree, Siemens Medical Solutions; Avanto, Siemens Medical Solutions). The MRI protocol included a coronal T1-weighted sequence; sagittal, axial, and coronal T2-weighted sequences with fat saturation; and a sagittal proton density–weighted sequence.
The ALL injury MRI examination criteria used were based on previous studies of this structure and included proximal or distal bone detachment, discontinuation of its fibers, or irregular contour associated with periligamentous edema.11,28 The MRI examinations were evaluated by a musculoskeletal radiologist and a knee surgeon (P.V.P.H. and C.P.H.), both with previous experience in the evaluation of anterolateral knee structures, and correlation tests were performed. Two evaluations were performed per evaluator with a minimum interval of 30 days.
All patients underwent isolated intra-articular anatomic single-bundle ACL reconstruction with autologous 4- or 5-strand hamstring grafts, using the outside-in technique and fixation with absorbable interference screws in the femur and tibia. Most patients underwent the same rehabilitation protocol for isolated ACL reconstruction at our institution. No immobilization device or movement restriction of any type was applied. Patients were encouraged to bear weight on the operated limb as tolerated, and range of motion was initiated on the first postoperative day. In patients who underwent meniscal repair, the rehabilitation included load bearing as tolerated with a knee brace and range of motion restricted from 0° to 90° for 4 weeks. After that, the protocol was similar to that of the other patients. Quadriceps strengthening exercises were allowed from the initial postoperative period. Running activities were started around 4 months after surgery, and the authorization to return to sports without restrictions was made around 8 to 9 months.
Patients were divided into 2 groups according to the presence (ALL injury group) or absence (control group) of an anterolateral injury based on the initial MRI examination performed in the acute phase of the injury. The demographic data of the 2 groups were compared, and the following criteria were evaluated: physical examination before and after surgery, including the KT-1000 arthrometer and pivot-shift tests; failure rate; subjective International Knee Documentation Committee (IKDC) and Lysholm scores; and incidence of contralateral ACL injury. Risk factors such as the presence of associated meniscal injuries in the intraoperative period, intra-articular ACL graft size, and the degree of knee hyperextension, measured using a goniometer at the time of the surgical procedure in the contralateral knee to minimize the effects of the ACL injury on the affected knee, were evaluated. ACL reconstruction failure was considered when the patient had a KT-1000 arthrometer reading of >5 mm or pivot shift test result of 2+ or 3+, or when the graft was torn on postoperative MRI findings. MRI scans were performed only when clinically indicated. The groups were compared with each other at a minimum follow-up of 5 years, and a comparison was also carried out within the same group of patients at 2 25 and 5 years of minimum follow-up. Patients were always evaluated by knee surgeons, knee fellows, and physical therapists at our institution during regular follow-up, the latter 2 being responsible for entering the data into the database. After ACL reconstruction, patients returned for follow-up 1 week, 3 weeks, 6 weeks, 3 months, 6 months, and 1 year postoperatively, and annually after that. During the years the study was performed, a number of different knee fellows and physical therapists were responsible for entering the data into the database. For this study, the evaluators were blinded to the ALL status.
The pre- and postoperative pivot-shift tests were performed by 2 orthopaedic surgeons (M.F.S. and C.P.H.) with experience in physical examination of the knee. The most experienced examiner served as the main examiner, and the least experienced examiner was used to assess interrater agreement. The pivot-shift test was defined according to IKDC classification: normal (0), glide (1), clunk (2), and gross (3). 8 The preoperative pivot-shift test was performed under anesthesia just before surgery, but the postoperative pivot-shift test was not performed under anesthesia because it was done during regular postoperative follow-up visits.
Statistical analysis was performed using the Pearson chi-square and Fisher’s exact tests for categorical variables and the Mann-Whitney test for continuous variables. Statistical significance was considered when the P value was <.05.
Results
A total of 156 patients were evaluated after a minimum follow-up of 5 years. The study flowchart is depicted in Figure 1. This accounts for a loss of 26 patients (14%) in comparison with the minimum 2-year follow-up evaluation. The ALL injury group comprised 91 patients, and the control group consisted of 65 patients. The overall rate of ALL injury was 59.3% in the study sample and 58.3% in the cohort available for 5 years of follow-up. Representative MRI scans of the ALL and control groups are shown in Figure 2.
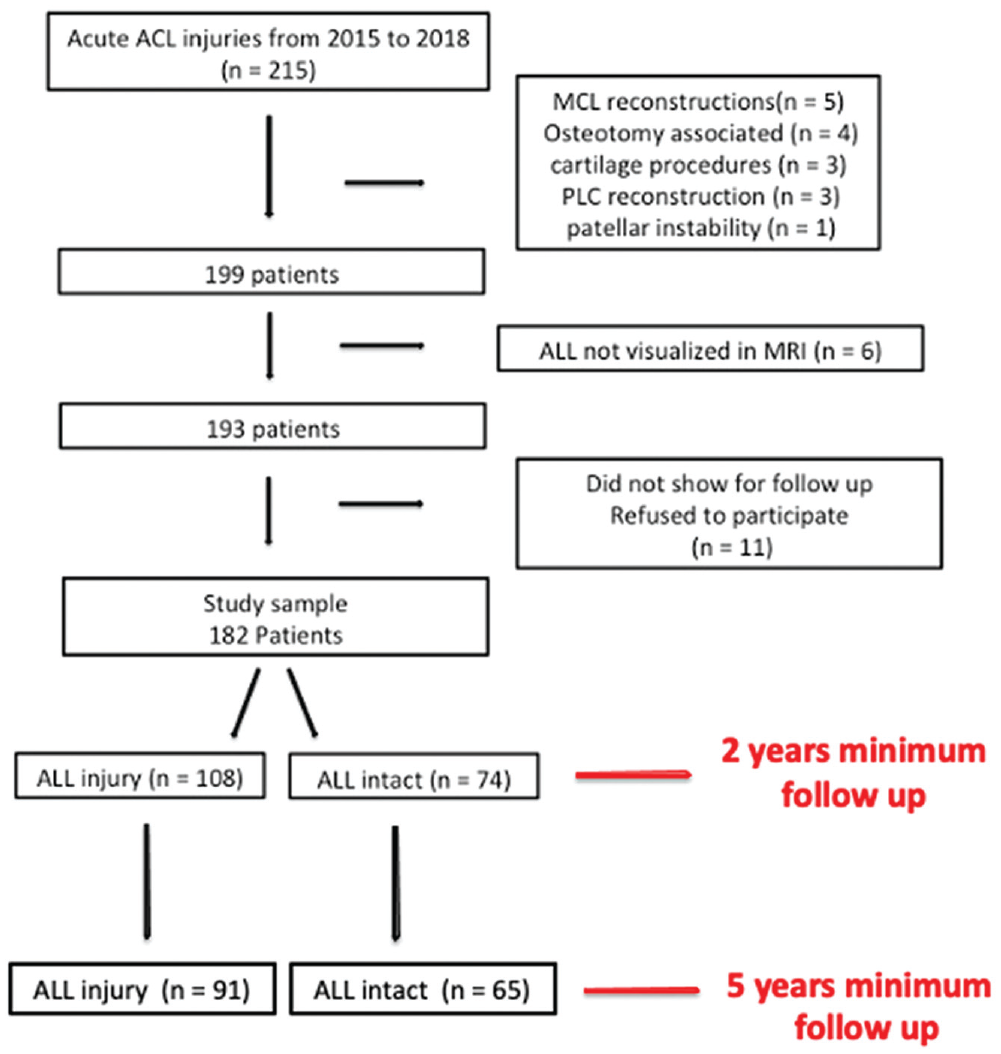
Flowchart of the study. ACL, anterior cruciate ligament; ALL, anterolateral ligament; MCL, medial collateral ligament; MRI, magnetic resonance imaging; PLC, posterolateral corner.
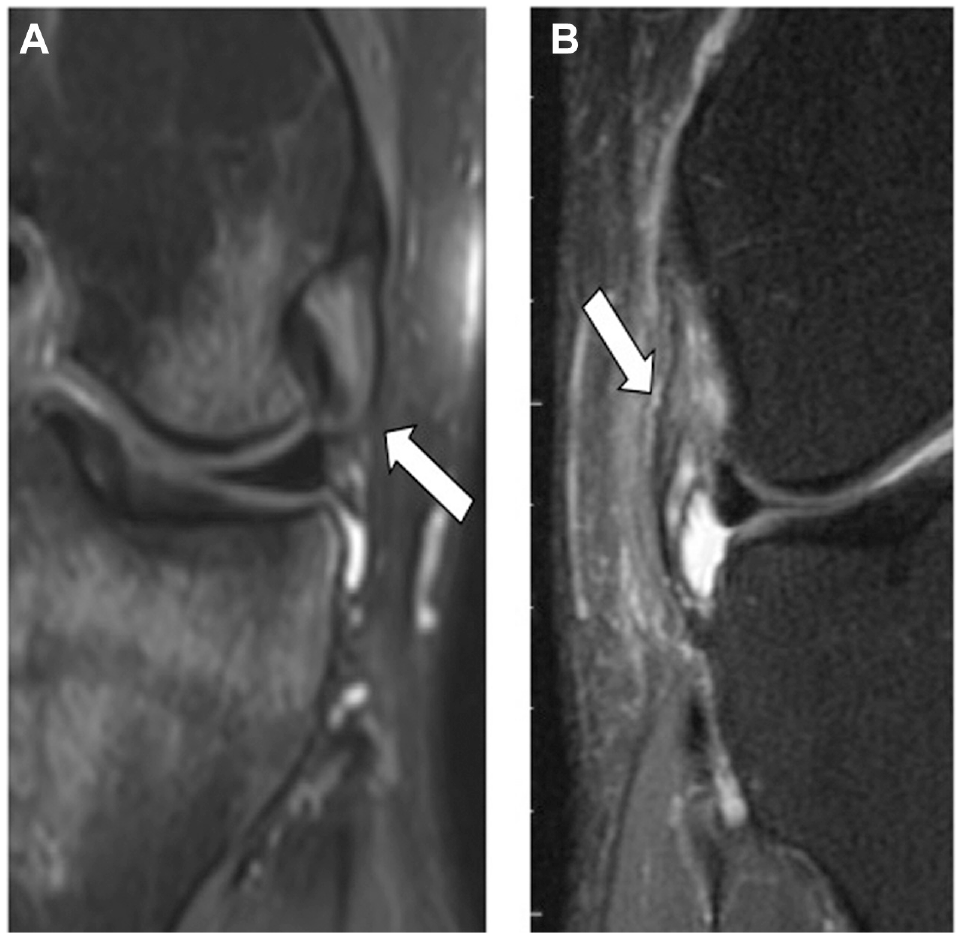
Coronal T2-weighted magnetic resonance imaging scans with fat saturation of left knees depicting (A) normal and (B) abnormal anterolateral ligaments (ALLs). The normal ALL (arrow in A) is thin, has a homogeneous signal, and does not present peripheral edema. The abnormal ALL is thickened and irregular, with areas of attenuation (arrow in B), and has peripheral edema. (Reproduced from Sobrado et al. 25 )
The groups exhibited no significant differences in age, sex, duration of injury until surgical treatment, follow-up duration, intra-articular ACL graft diameter, knee hyperextension, preoperative pivot-shift grade, and preoperative KT-1000 arthrometer values (Table 1).
Characteristics of the Groups and Preoperative Data a
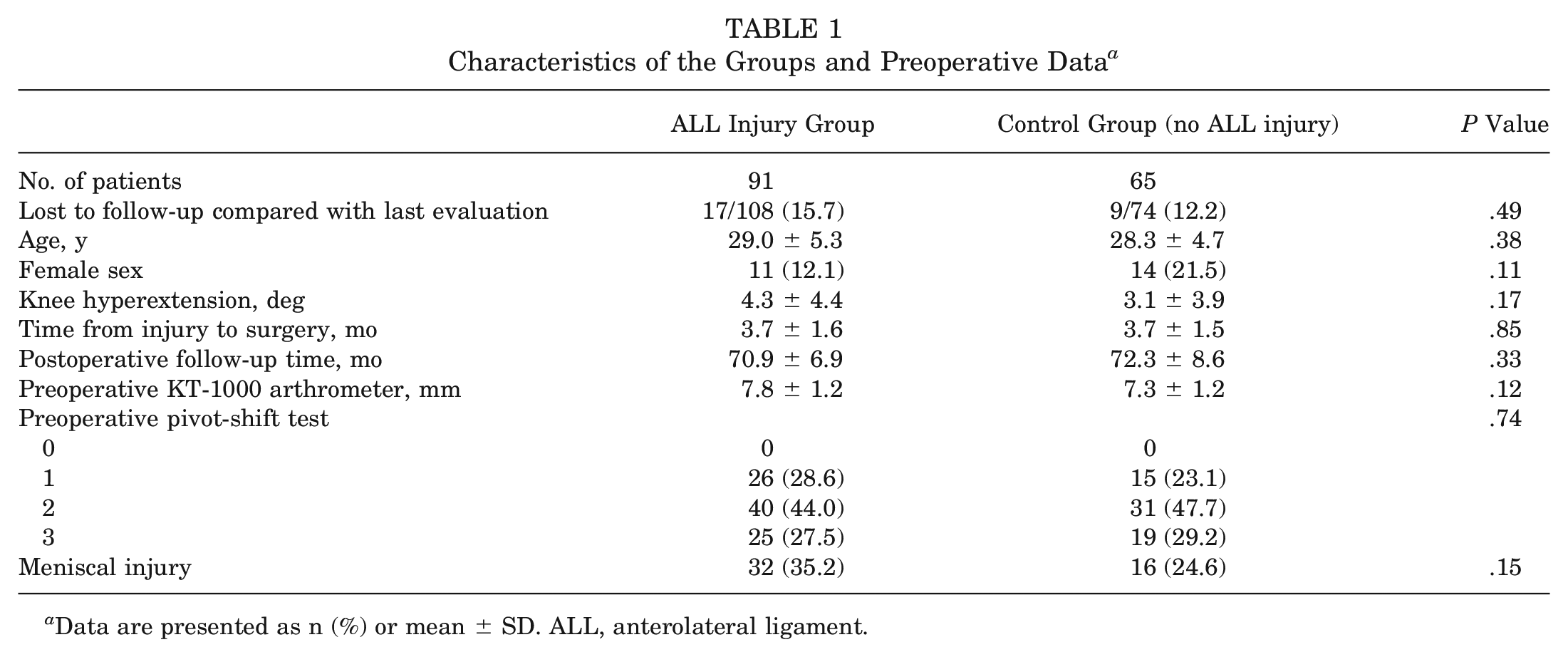
Data are presented as n (%) or mean ± SD. ALL, anterolateral ligament.
The prevalence of meniscal injury also did not display significant disparities between the groups. A meniscal injury was found in 32 patients (35.2%) from the ALL injury group and 16 (24.6%) from the control group (P = .15). The type of treatment for these injuries likewise exhibited no significant differences (P = .09) between the groups: repair was performed in 19 patients, and partial meniscectomy was carried out in 29 patients (Table 2).
Meniscal Treatment and Graft Diameter a
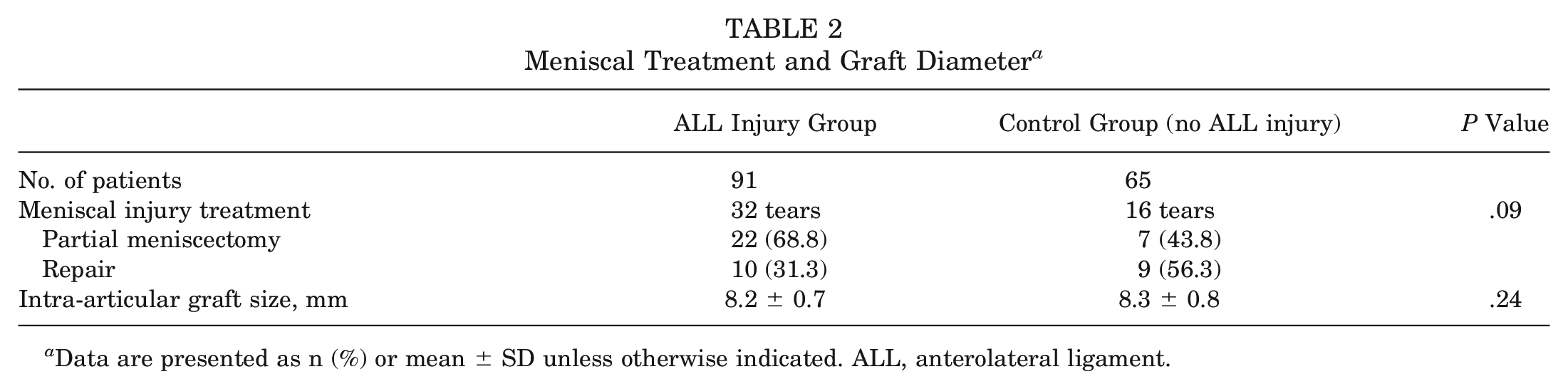
Data are presented as n (%) or mean ± SD unless otherwise indicated. ALL, anterolateral ligament.
On final evaluation, patients in the control group (no ALL injury) demonstrated superior postoperative outcomes on the Lysholm scale (P < .00001), albeit not in the IKDC functional scales (P = .10), after a mean follow-up period of 70.9 ± 6.9 months for the ALL injury group and 72.3 ± 8.6 months for the control group (P = .33). Assessment of anteroposterior (AP) translation by the KT-1000 arthrometer revealed worse results for the ALL injury group (2.8 ± 1.4 mm) compared with the control group (1.9 ± 1.3 mm) (P = .00018). The pivot-shift test did not reveal any difference between the 2 groups (P = .77). The rate of contralateral ACL injury within the entire cohort was 10.3% (n = 16), with no significant variance between the groups (P = .47). The rate of reconstruction failure in the entire cohort was 10.3% (n = 16), with 14.3% (n = 13) in the ALL injury group and 4.6% (n = 3) in the control group. This difference was statistically significant (P = .049). The contralateral ACL injury rate in the entire cohort was also 10.3% (n = 16), with 8.8% (n = 8) in the ALL injury group and 12.3% (n = 8) in the control group. It did not differ between the groups (Table 3).
Postoperative Clinical Results a
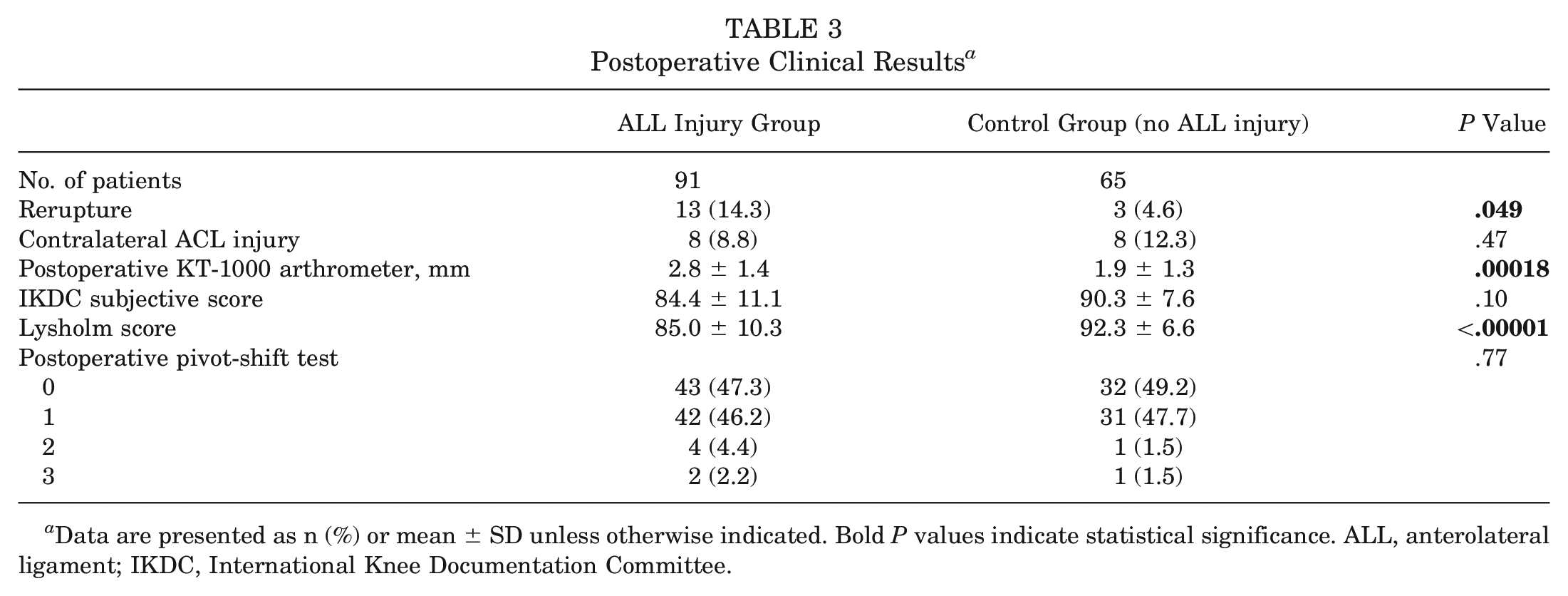
Data are presented as n (%) or mean ± SD unless otherwise indicated. Bold P values indicate statistical significance. ALL, anterolateral ligament; IKDC, International Knee Documentation Committee.
Regarding the ALL group, the postoperative KT-1000 arthrometer measurements increased from 2.4 ± 1.6 mm to 2.8 ± 1.4 mm when comparing the 2-year and 5-year minimum follow-up periods. No differences were observed in other variables examined (Table 4). In the control group, there were no changes in postoperative clinical results when comparing evaluations with minimum follow-ups of 2 years and 5 years for ACL reconstruction across all studied variables (Table 5).
Postoperative Clinical Results Comparing Evaluation With Minimum 2-Year and 5-Year Follow-ups for ACL Reconstruction in Cases of Associated ALL injury a
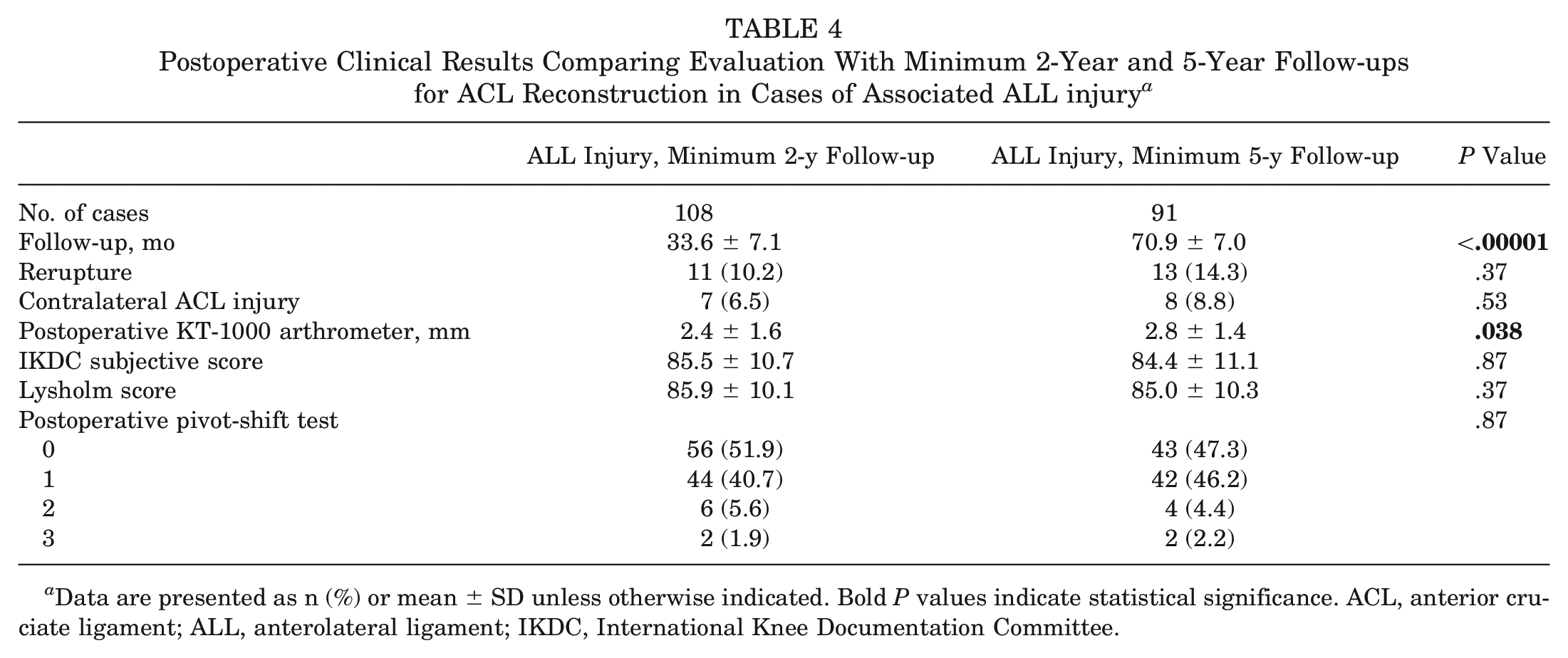
Data are presented as n (%) or mean ± SD unless otherwise indicated. Bold P values indicate statistical significance. ACL, anterior cruciate ligament; ALL, anterolateral ligament; IKDC, International Knee Documentation Committee.
Postoperative Clinical Results Comparing Evaluation With Minimum 2-Year and 5-Year Follow-ups for ACL Reconstruction in Cases of Nonassociated ALL Injury a
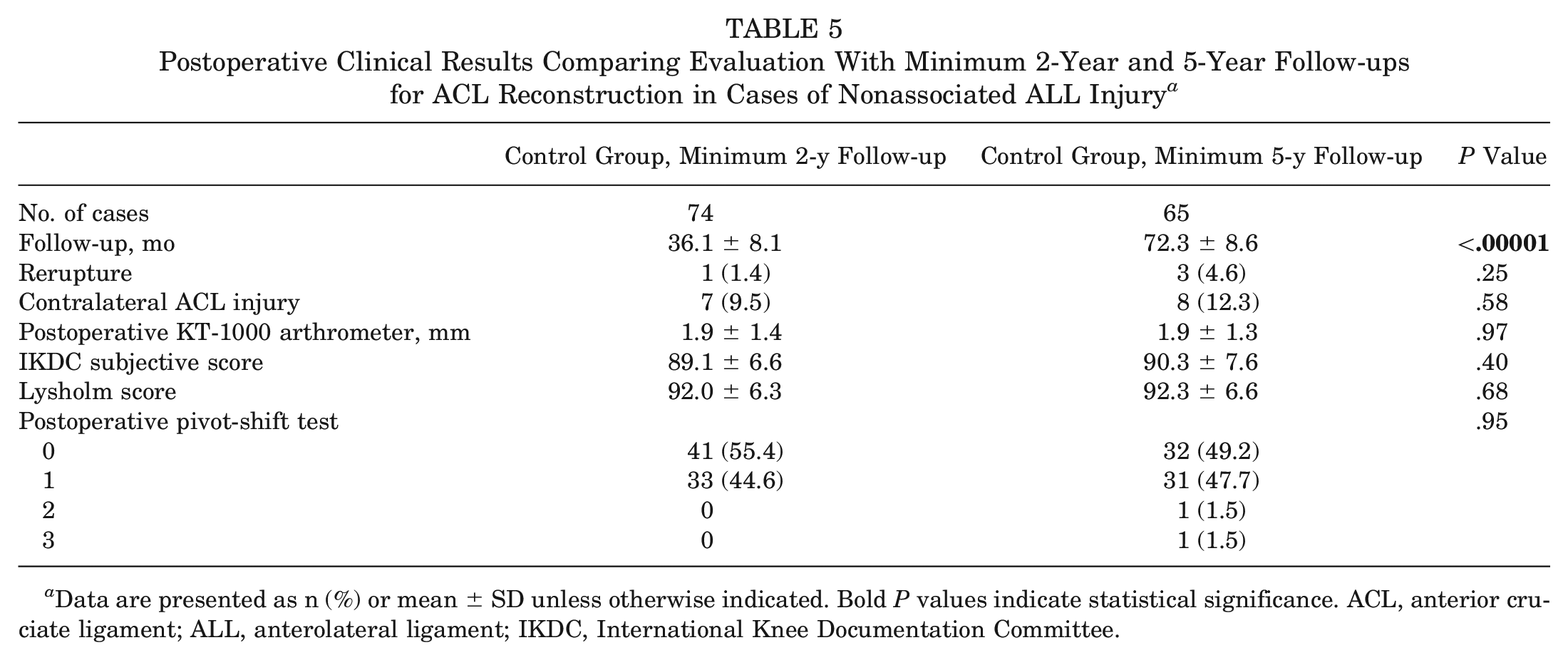
Data are presented as n (%) or mean ± SD unless otherwise indicated. Bold P values indicate statistical significance. ACL, anterior cruciate ligament; ALL, anterolateral ligament; IKDC, International Knee Documentation Committee.
The interrater agreement for ALL injuries on MRI ranged from 0.71 to 0.82 (kappa test), and the agreement between the 2 reviews by the same evaluator ranged from 0.73 to 0.83. The interexaminer agreement for the pivot-shift test was 0.654 (kappa test), which was considered substantial agreement. These data were reported in the 2-year follow-up results of this cohort. 25
Discussion
The most important finding of this study was that patients with an ALL injury on preoperative MRI performed in the acute phase after an ACL injury showed a higher rerupture rate, increased AP laxity on KT-1000 arthrometer test, and a worse Lysholm score than patients with a normal anterolateral complex at a minimum 5-year follow-up after an isolated ACL reconstruction performed with hamstring graft. Also, knee instability measured by the KT-1000 arthrometer worsened from 2 to 5 years of follow-up in the ALL injury group.
These conclusions build on the findings of the 2-year follow-up study of Sobrado et al, 25 which reported a failure rate of 10.2% for the ALL injury group and 1.4% for the control group (P = .029), highlighting the potential adverse effect of an associated untreated anterolateral injury on the outcomes of ACL reconstruction. They also noted inferior scores on the Lysholm scale (P < .001) and IKDC functional scale (P = .035) after a mean follow-up period of 33.6 ± 7.1 months for the ALL injury group and 36.1 ± 8.1 months for the control group. Consistently, in the present evaluation, we have also identified a higher failure rate in the ALL injury group (14.3% vs 4.6% for the control group), but over an extended follow-up period.
The failure rate of 14.3% in the ALL injury group compares with those of well-recognized high-risk factors for ACL reconstruction failures, including young athletes (15.6%), hyperlaxity (21%), high-demand patients (11%), and ACL revision surgery (14.7%).7,12,13,29 Consequently, we believe this finding supports the case for considering the inclusion of ALL injury assessment on MRI as an additional risk factor for ACL reconstruction failure. Even though there is no mandatory risk factor that obligates an associated anterolateral reconstruction combined with the intra-articular ACL reconstruction, a few studies have attempted to reach consensus about the possible indications for this combined procedure. Despite some variations, until now, the most accepted indications have been revision ACL reconstruction, young patients involved in pivoting sports, hyperlaxity, and high-grade anterolateral rotatory instabilities.1,2,6,26 According to the data presented in this study, the presence of an ALL injury on an MRI scan should be considered in determining when to perform an ALL reconstruction.
In terms of functional scales, our cohort revealed lower Lysholm scores (85.0 vs 92.3, difference of 7.3 points; P < .00001) but no significant difference in IKDC scores (P = .10) within this population (ALL injury). These findings are consistent with the results reported of Sobrado et al, 25 Castelli et al, 3 and Melugin et al. 18 Castelli et al reported inferior IKDC (93.1 vs 97.3, difference of 4.2 points) and Lysholm (94.7 vs 99, difference of 4.3 points) scores for the group with ALL injuries in a study involving 62 patients. In a similar study, Melugin et al, comparing patients with ACL injuries with and without a Segond fracture, also found a statistically significant difference in IKDC scores (86.5 vs 93.0, difference of 6.5 points; P = .03) in favor of patients without a Segond fracture. It could be argued that the magnitude of improvement in Lysholm scores may not be clinically significant, considering the minimal clinically important difference of 8.9 for the Lysholm score, even though it is statistically significant. 22 The minimal clinically important difference for the IKDC is 16.7 in ACL reconstruction patients. However, in the context of the comprehensive findings of this study, it can be asserted that an ALL injury is associated with significantly less favorable outcomes after ACL reconstruction.
The ALL injury group also exhibited a greater anterior knee translation value in the postoperative KT-1000 arthrometer test (2.8 ± 1.4 mm vs 1.9 ± 1.3 mm for the control group; P = .00018). The ALL serves as a secondary stabilizer of the knee, and its injury may have contributed to the long-term increase in postoperative AP translation. 19 This heightened AP laxity could have also played a role in the poorer subjective scores, such as those on the Lysholm questionnaire. In relation to the pivot-shift test, we observed no disparities in the pre- and postoperative assessments between both groups. Biomechanical studies have reported a correlation between anterolateral injury and rotatory instability, which would be expected in our study.19,20 Clinical studies have also shown that preoperative anterolateral injuries have a strong correlation with higher grades in the pivot-shift test. 14 However, it is a subjective maneuver influenced by various factors that may vary in magnitude based on the presence of meniscal injury, bone morphology, other peripheral injuries, and ligamentous hyperlaxity. 5 Also, as a wide range of lesions were considered, some smaller ones may have only a minor influence in rotation, and that may be why the preoperative pivot-shift test results were similar between the groups. Moreover, our postoperative physical examinations were conducted on nonanesthetized patients, which may have impacted the results, despite the presence of 2 experienced examiners and a satisfactory level of correlation between them.
Another important finding of this study was the worsening of anterior knee instability from a minimum of 2 to a minimum of 5 years of follow-up in the ALL injury group. Biomechanical studies have already shown that an isolated ACL reconstruction cannot restore knee biomechanics in the presence of combined ACL and anterolateral tears. 16 Because the ALL has a low healing potential, according to studies by Lee et al 17 and Saithna et al, 24 it is possible that progressive loosening of the ACL over time may have occurred given the lack of stability of the lateral capsular structures. After 2 years, it is possible to consider that the ligamentization of the ACL reconstruction is complete, in the way loosening would not be expected after that period. According to these findings, it is possible to infer that the healing process of the ACL might take >2 years or the residual capsular laxity can cause gradual attenuation of the ACL from repetitive microtrauma. This finding needs to be further studied. Even with the worsening of the knee AP translation, the IKDC and Lysholm scores presented the same results between groups. As they are subjective scales, this small change in KT-1000 arthrometer values may not have had the capacity to change patients’ perception of knee function.
The use of hamstring grafts only can be considered a limitation, as it is not possible to completely extrapolate these results to other types of graft, such as the patellar tendon and the quadriceps tendons. Nevertheless, the present study has strengths because it is prospective, has a relevant number of patients operated on with a similar technique, and had a minimum follow-up >60 months, which has not been previously reported in the literature. The loss to follow-up can also be considered a limitation, although a percentage of around 12% to 15% is acceptable. Moreover, the fact that the lesions were not stratified by location and severity is another important limitation of this study. The postoperative pivot-shift test was not performed under anesthesia, and this can also create some bias in the reported results.
The study findings support that an acute MRI-identified ALL injury is associated with an increased risk of ACL reconstruction failure and poorer clinical outcomes in terms of the Lysholm score and AP laxity. These results were evident at the 2-year assessment and persisted after a minimum follow-up of 5 years. ALL reconstruction has demonstrated its effectiveness in reducing the incidence of ACL reconstruction reinjuries in various contexts,7,9,12,23 and its potential application should be explored further in patients with this imaging finding. According to the findings of this study, an MRI detection of an ALL lesion during the preoperative period should be considered as a possible further indication for adding a lateral extra-articular procedure to the ACL reconstruction surgery.
Conclusion
Combined ACL and ALL injuries were associated with significantly less favorable outcomes than were isolated ACL injuries at a minimum follow-up of 5 years after isolated ACL reconstruction with hamstring autograft. Patients with concomitant ALL injury showed a higher failure rate and worse functional scores. Also, knee stability tends to slightly worsen from 2 to 5 years in cases of associated ALL injury.
Footnotes
Submitted January 15, 2024; accepted May 17, 2024.
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.