
Abstract
Background:
The management of pain after shoulder surgery typically includes the use of cryotherapy and the prescription of opioid analgesics. Much focus has been placed lately on the opioid epidemic, which in part is fueled by excessive prescription of opioid medication. Previous studies have found a combination of cryotherapy and compression effective at reducing analgesic consumption and increasing recovery in patients undergoing knee and spine surgery; however, efficacy in patients undergoing shoulder surgery has not been evaluated.
Purpose:
To evaluate the effectiveness of a cryo–pneumatic compression device on postoperative shoulder pain, narcotic use, and quality of life when compared with standard care cryotherapy.
Study Design:
Randomized controlled trial; Level of evidence, 2.
Methods:
In total, 200 patients older than 18 years scheduled for unilateral shoulder surgery were enrolled. Patients were randomized to receive either postoperative cryo–pneumatic compression or standard care. The intervention group received a cryo–pneumatic device, while the standard care group received the treating surgeon’s preferred method of postoperative care, including standard cryotherapy. Narcotic use was evaluated by the number of oral morphine milligram equivalents consumed during the postoperative period, as well as the time to cessation of narcotic use. Patient-reported outcome measures consisted of a numeric rating scale pain score, 36-item Short Form Survey, patient experience assessed using the net promoter score, and adverse events. Outcomes were evaluated at 2, 6, and 12 weeks postoperatively.
Results:
Patients receiving cryo–pneumatic compression reported a significant decrease in opioid consumption when compared with standard care (oral morphine milligram equivalents median, 56.1 vs 112; P = .02468). A significant increase in self-reported function was seen in the cryo–pneumatic compression group at 2 weeks when compared with standard care (mean, 61.2 vs 54.2; P = .0412).
Conclusion:
In patients undergoing unilateral shoulder surgery, the use of cryotherapy with pneumatic compression, when compared with standard care, resulted in significantly decreased opioid consumption as well as increased function at 2 weeks.
Registration:
NCT04185064 (ClinicalTrials.gov identifier).
Elective shoulder surgery is one of the most commonly performed orthopaedic surgeries and is increasing in volume rapidly given recent advancements in surgical techniques. 8 Pain management after shoulder surgery typically involves the prescription of pain medication, typically in the form of opioid analgesics, and occasionally the use of adjunct cryotherapy. Lately, much focus has been put on the opioid epidemic, which in part is fueled by excessive prescription of opioid medications.3,11 Recent studies have indicated that orthopaedic surgeons are among the highest opioid prescribers.7,12 This is especially critical considering that opioid-naïve patients undergoing shoulder surgery are at an increased risk of long-term dependence. 6 With the increasing number of shoulder surgeries performed, identifying ways to reduce opioid consumption postoperatively is imperative for orthopaedic surgeons to reduce opioid prescriptions.
Cryotherapy is commonly used after shoulder surgery to decrease swelling and inflammation, as well as to help alleviate postoperative pain.4,10,14,15 Cold can be applied in many forms, from ice packs to more complex cryotherapy devices. Previous studies have found a combination of cryotherapy and compression to be effective at reducing analgesic consumption and increasing recovery in patients undergoing knee and spine surgery; however, efficacy in patients undergoing shoulder surgery has not been evaluated.1,2,9,13 The aim of this study was to evaluate the effectiveness of a cryo–pneumatic compression device on postoperative shoulder pain, narcotic use, and quality of life when compared with standard care.
Methods
This study was a multicenter, unblinded randomized controlled trial evaluating clinical outcomes after the use of cryo–pneumatic compression or standard care after shoulder surgery. Before initiation of the study, ethics approval was obtained (approval No. MOD00604707) and the study was registered at ClinicalTrials.gov (NCT04185064). Patient randomization was established by creation of a randomization list created in R Version 4.0.2 (R Foundation for Statistical Computing) using the package randomizeR by a research coordinator not involved in the treatment of patients (S.A.P.). Block randomization was performed using blocks of 8 patients, and no stratification was performed.
Patient Selection
Patients older than 18 years scheduled for open or arthroscopic unilateral primary or revision shoulder surgery at 5 hospitals in Ontario, Canada, were approached by board-certified orthopaedic surgeons (M.K., P.M., V.V., J.H.) for participation between December 2019 and February 2023. The exclusion criteria for the study were (1) patients undergoing bilateral surgery; (2) patients who were pregnant or nursing; (3) patients who did not believe they could comply with the study protocol; (4) patients generally unfit for surgery; (5) patients with specific treatment preferences; (6) patients who were unable to complete questionnaires because of language barriers, decreased mental capacity, and/or neuropsychological problems; (7) social factors precluding study follow-up; and (8) an inability or unwillingness to provide informed consent.
The randomization list was generated before enrollment of the first patient in the study and was accessible only by the research coordinator. Written informed consent was obtained before the surgical procedure, and the patients were randomized centrally by a research coordinator uninvolved with patient care. Given the nature of the treatments, blinding of patients and treatment providers was not possible.
A 50-patient, nonrandomized prospective cohort of patients who would receive a cryo–pneumatic compression device at a cost to themselves or their insurer was planned; however, this cohort was not initiated because of the extended timeline of the randomized controlled trial recruitment caused by COVID-19 pandemic–related hospital and operating room shutdowns that were experienced in Ontario during the study period.
Intervention Group
The intervention group received a cryo–pneumatic compression device, which consisted of a Game Ready GRPro 2.1 system with a Game Ready ATX shoulder wrap (Avanos Medical Inc.). The device provides continuous cold and intermittent pneumatic compression therapy to the shoulder joint and surrounding soft tissues.
Cryo–pneumatic compression was applied to the patient in the operating room at the conclusion of the surgical procedure and was used in the recovery room for 45 minutes to 1 hour. For postoperative days 1 and 2, the patient was instructed to use the device as cold as comfortable (34°F; adjustable to 50°F) on the low-compression setting for 30 minutes on and 60 minutes off throughout the day, and as needed at night. For postoperative days 3 to the end of usage, the patient was instructed to use the device as cold as comfortable on the medium-compression setting for a minimum of twice per day. The patients received a standard arm sling as well as the treating surgeon’s standard postoperative medications and physical therapy per their standard practices.
Standard Care Group
The standard care group received the treating surgeon’s preferred method of postoperative care, which could consist of rest, ice, and compression using standard ice packs or bags of ice, a cryocuff, or other such devices. There were no limitations to the type of cryotherapy that could be used in the standard care group, with the exception of a cryo–pneumatic compression device. The standard care intervention was used per the treating surgeon’s standard recommendations to patients. As with the intervention group, patients received their normal arm sling, postoperative medications, and physical therapy per their treating surgeon and physical therapist’s standard practices.
Clinical Outcomes
The primary outcome in this study was patient-reported numeric rating scale (NRS) pain score at 12 weeks, rated on a scale ranging from 0 (no pain) to 10 (worst possible pain). Narcotic usage after surgery was evaluated by the number of oral morphine milligram equivalents (OMME) during the postoperative period, as well as the time to cessation of narcotic use. Narcotic usage was collected using a patient drug diary that was completed by the patient during the postoperative period. Patient-reported outcome measures (PROMs) consisted of quality of life using the 36-item Short Form Survey (SF-36) and its subscales, reported on scales of 0 to 100, with higher values representing better outcomes; patient experience assessed using the net promoter score; and adverse events. Narcotic usage was collected after patients completed their use of the medication, while PROMs and adverse events were collected at 2, 6, and 12 weeks postoperatively.
Statistical Analysis
Data were analyzed as intention to treat. A convenience sample size of 200 patients was selected based on the feasibility of recruiting this number of patients in a 12-month period and was expected to provide adequate power to detect differences between groups for the NRS pain measure.
Baseline characteristics were performed using descriptive statistics reported by group as mean and standard deviation for continuous variables and count with percentage for categorical variables. The normality of data was tested using the Shapiro-Wilk test and visualization of residual Q-Q plots. For continuous outcome measures, normally distributed data were analyzed using a 1-way analysis of variance with factors of group for OMME consumed and time to cessation of narcotics, and a 2-way repeated-measures analysis of variance with factors of time and group for PROMs. Nonnormally distributed data were analyzed using a Mann-Whitney U test for OMME consumed and time to cessation of narcotics, and a generalized linear model with factors of time and group for PROMs. Adverse events were analyzed using a Pearson chi-square test. All statistical analyses were conducted in R Version 4.3.1 (R Foundation for Statistical Computing).
Results
Patient information is summarized in Table 1. A total of 200 patients were enrolled in this study, of whom 102 were randomized to the cryo–pneumatic compression group and 98 to the standard care group. Sixteen patients were lost to follow-up in the cryo–pneumatic compression group, and 38 in the standard care group (Figure 1). No statistically significant differences were found between the groups with respect to patient characteristics and operative data. The mean ages in the cryo–pneumatic compression and standard care groups were 55.8 ± 14.5 years and 54.1 ± 14.9 years, respectively, and there were more men than women. In both groups, rotator cuff repair was the most common surgery type (n = 100; 50%), followed by stabilization, labral repair, or superior labral anterior-posterior repair (n = 38; 19%).
Patient Characteristics a
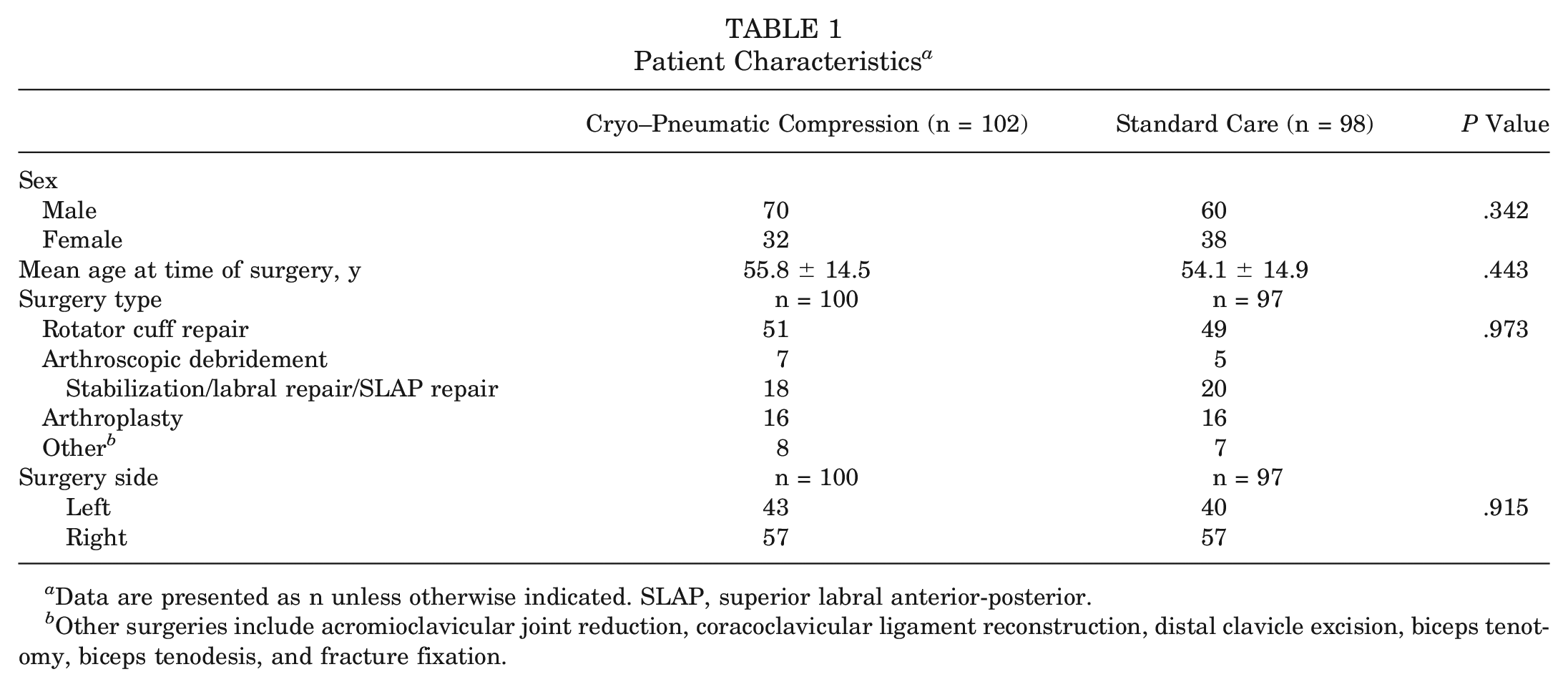
Data are presented as n unless otherwise indicated. SLAP, superior labral anterior-posterior.
Other surgeries include acromioclavicular joint reduction, coracoclavicular ligament reconstruction, distal clavicle excision, biceps tenotomy, biceps tenodesis, and fracture fixation.
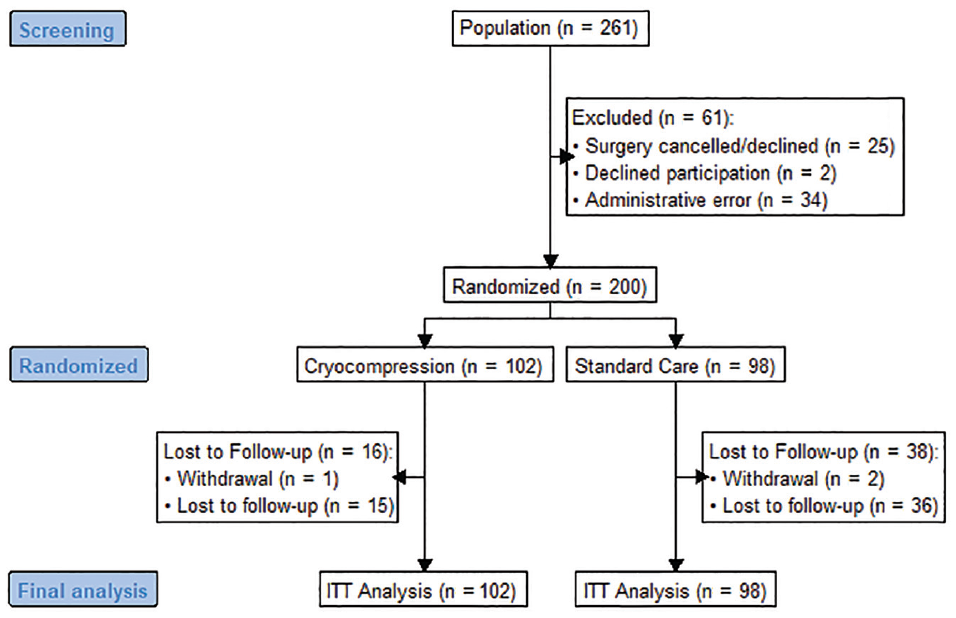
CONSORT (Consolidated Standards of Reporting Trials) diagram. ITT, intention to treat.
Because of an administration error at a site, the first 34 patients did not have any data collected, which resulted in retraining and a restart of recruitment at the site. A post hoc analysis of characteristics comparing these patients with the included patients from this site showed no significant differences in age (P = .42), sex (P > .99), type of surgery (P = .49), or side of surgery (P = .53), indicating that the study population would be representative of these patients as well, and they would likely experience similar outcomes and not change the results of the study
Patients in the standard care group most commonly used a cryocuff for their postoperative cryotherapy (43%), followed by ice packs (30%), and finally no cryotherapy (6%), with 21% of patients not reporting on their cryotherapy use. Of patients in the cryo–pneumatic compression group, 5% used the device for <1 week or not at all. Four of the 5 study sites applied both standard care cryotherapy and cryo–pneumatic compression therapy in the operating room for use in the postanesthesia care unit, while the fifth site did not apply either standard care cryotherapy or the cryo–pneumatic compression device for postanesthesia care unit use.
Postoperative Narcotic Consumption
After the cessation of narcotics, patients in the cryo–pneumatic compression group demonstrated a significant reduction in the amount of narcotics consumed (median, 56.1 OMME; IQR, 66.1 OMME) when compared with standard care (median, 112 OMME; IQR, 99.4 OMME) (P = .02468) (Figure 2). The time to cessation of narcotics was shorter in the cryo–pneumatic compression group (median, 4 days; IQR, 5 days) when compared with the standard care group (median, 6 days; IQR, 4.5 days), although this did not reach statistical significance (P = .1534).
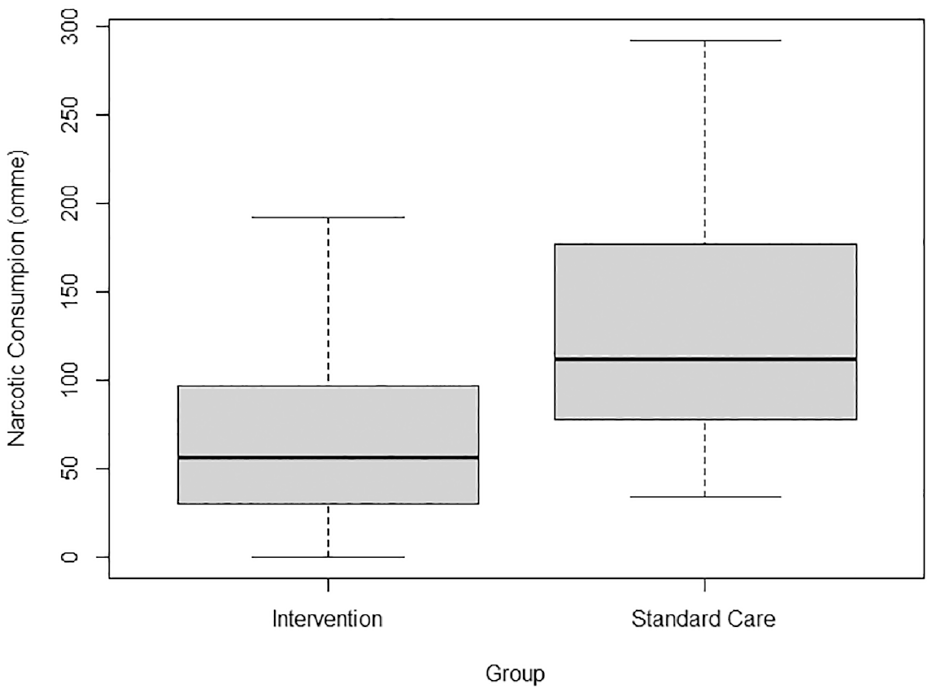
Narcotic consumption over the postoperative period. OMME, oral morphine milligram equivalents.
Patient-Reported Outcome Measures
A significant increase in self-reported function (SF-36 Physical Function subscale) was seen in the cryo–pneumatic compression group at 2 weeks when compared with standard care (mean, 61.2 ± 21.2 vs 54.2 ± 22.9; P = .0412) (Table 2). No significant difference was seen in patient NRS pain scores or any other SF-36 subscale scores at any time point during the study follow-up (Table 2). Net promoter scores were higher in the cryo–pneumatic compression group at 2 and 6 weeks postoperatively and were comparable at 12 weeks postoperatively.
Patient-Reported Outcome Measures a
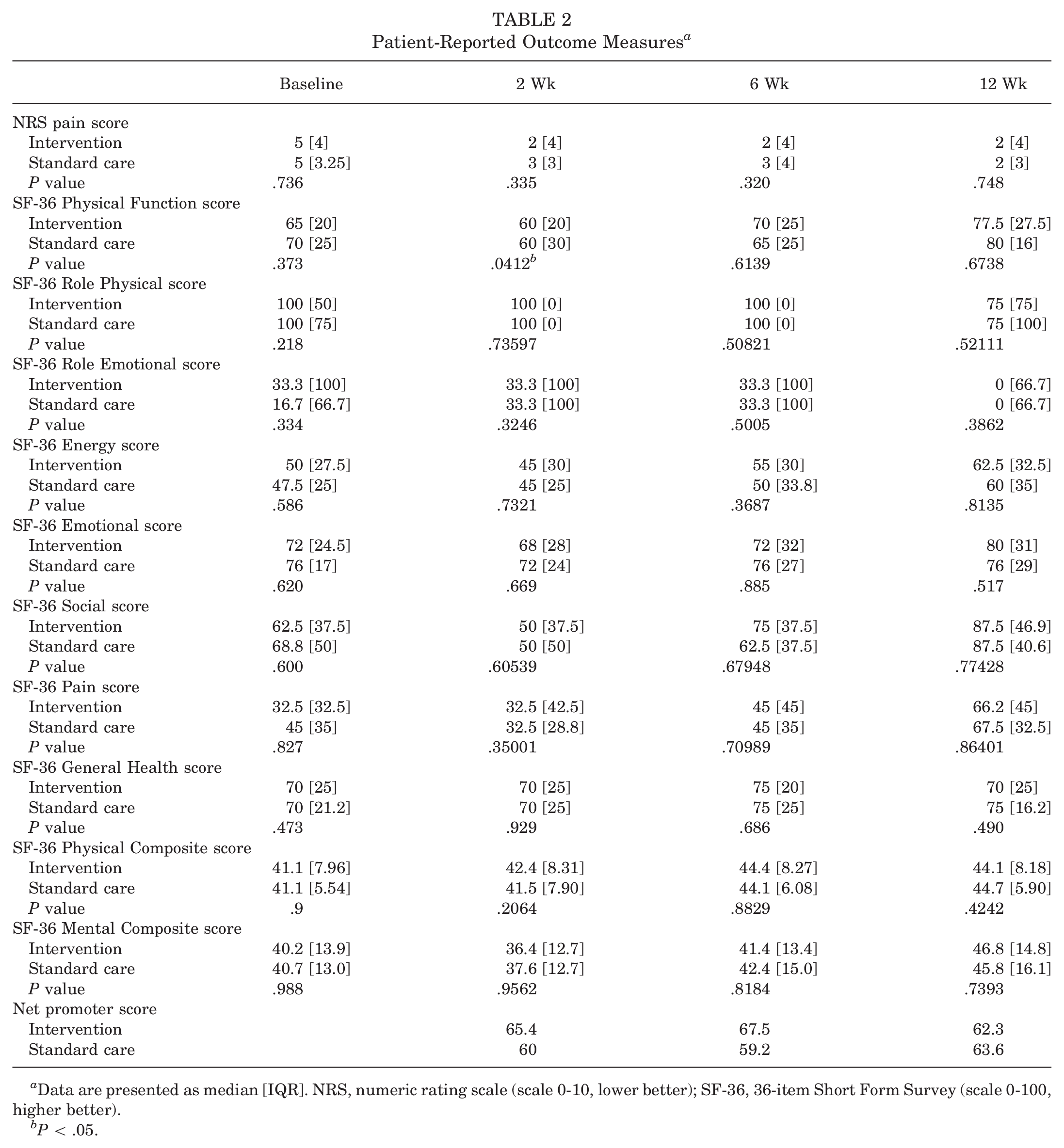
Data are presented as median [IQR]. NRS, numeric rating scale (scale 0-10, lower better); SF-36, 36-item Short Form Survey (scale 0-100, higher better).
P < .05.
Adverse Events
No significant difference was seen in adverse events between the 2 groups, with 6 adverse events experienced by patients during the study, 4 in the standard care group and 2 in the cryo–pneumatic compression group (Fisher exact P = .4379) (Table 3). None of the adverse events were judged as related to the postoperative cryotherapy for either group.
Adverse Events a

Data are presented as n (%).
Discussion
We conducted a prospective, multicenter, unblinded randomized controlled trial comparing cryo–pneumatic compression with standard care in the postoperative treatment of patients undergoing unilateral primary or revision shoulder surgery. The study indicated a decrease in postoperative opioid consumption in the patients receiving cryo–pneumatic compression, as well as an increase in patient-reported function at 2 weeks. There was also a trend toward a shorter time to cessation of opioids; however, this did not reach significance. No differences were found in NRS pain or other subscales of the SF-36 at any time point.
Because of the current epidemic of opioid overdose and the risks associated with opioid use, there is a concerted effort to reduce the reliance on these medications for pain management. Multimodal opioid-sparing protocols using alternative forms of nonopioid medications have provided reductions in postoperative opioid consumption.5,16 The opioid use reductions demonstrated in this study suggest that cryo–pneumatic compression in conjunction with multimodal opioid-sparing protocols further reduces the reliance on narcotic medications.
Patients in this study demonstrated no difference in NRS pain at any time point, however. It may be that patients in the standard care group showed similar pain scores at 2 weeks because of their consumption of more opioid medication, which may have helped to lower their perceptions of pain to levels similar to those of the cryo–pneumatic compression group. Additionally, a lack of significant difference between groups at 6 and 12 weeks could also be attributed to the patients being beyond the immediate postoperative period, in which pain is generally highest. As the protocol indicated use of the cryo–pneumatic compression device for 2 weeks, an additional 4 and 8 weeks beyond its use may see patients from both groups in a similar stage of recovery not affected by cryotherapy modality.
There are several strengths to the present trial. The study did not exclude patients based on the type of surgery or condition and included revision surgeries, which provides excellent generalizability of the results. Additionally, the multicenter study design also strengthens the generalizability of this study as patients received procedures in different settings, with different anesthetic protocols, from different surgeons. The outcomes of this study, including opioid use, function, pain, and quality of life, are important for patients undergoing shoulder surgery.
Limitations
The current trial has several limitations. First, given the nature of the interventions it was not possible to blind the patients or surgeons as the cryotherapy was applied by the surgeon after the procedure. The operating surgeon was also the person who collected the postoperative data forms, and as such the outcome assessors could not be blinded. Second, the outcome of opioid consumption was collected by patient reporting by use of a drug diary, which has the potential for biased reporting. Third, the study only included patients undergoing unilateral shoulder surgery, so extrapolation to patients undergoing bilateral surgery may be limited. Fourth, the administration error at the single site including the first 34 patients resulted in those patients not having any data collected, which resulted in retraining and a restart of recruitment at the site. As these were consecutive patients from both groups, this likely had little effect on the outcomes of the study because the a priori sample size of 200 patients was still met for the final analysis. The post hoc analysis that was performed showed no significant difference between the groups, indicating that the study population would be representative of these patients as well, and they would likely experience similar outcomes and not change the results of the study. Fifth, missing data on the type of standard care used in 21% of patients limits the results because if these patients did no form of cryotherapy, they may have experienced worse outcomes than if they had used some form of standard care, thus impacting the differences seen between groups. Finally, because of the COVID-19 pandemic and related shutdowns of healthcare resources, in-person follow-up was not always available, and email and telephone follow-ups were relied on, which likely contributed to an increase in patient loss to follow-up.
Conclusion
In patients undergoing unilateral shoulder surgery, the use of a cryo–pneumatic compression device, when compared with standard care, resulted in a significant decrease in opioid consumption postoperatively as well as increased function at 2 weeks postoperatively; however, further research is warranted to confirm the findings of this study given the stated limitations.
Footnotes
Submitted January 25, 2024; accepted June 11, 2024.
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.