
Abstract
Background:
Arthroscopic labral repair has been shown to result in favorable short- and midterm outcomes; however, the durability of outcomes specifically in older patients remains underreported.
Purpose:
To (1) report prospectively collected hip preservation rates and patient-reported outcome measures (PROMs) at a minimum 10-year follow-up in patients aged ≥40 years after primary hip arthroscopy with labral repair and (2) perform a matched analysis comparing patients aged ≥40 years with patients aged <40 years.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
Data were prospectively collected and retrospectively reviewed on all patients who underwent primary hip arthroscopy between February 2008 and December 2011. Patients aged ≥40 years who underwent labral repair were included. Preoperative and minimum 10-year follow-up scores were collected for multiple PROMs. Propensity score matching was utilized to compare these patients with a cohort of patients <40 years.
Results:
Of the 113 hips eligible, 91 hips (80.5%) on 85 patients (6 bilateral) had a minimum 10-year follow-up. There were 58 women (68%) and 27 men (32%) with a mean age and body mass index of 47.8 years and 25.8, respectively. The hip preservation rate for patients aged ≥40 years was 78%, with 20 patients requiring arthroplasty during the study period. There was significant improvement in all PROMs from baseline to minimum 10-year follow-up with high rates of achieving the minimal clinically important difference and Patient Acceptable Symptom State clinical outcome thresholds. In total, 69 patients aged ≥40 years were propensity matched to 107 patients <40 years. Patients ≥40 tended to have a lower hip preservation rate (81.2% vs 91.6%; P = .06), while patients in the younger cohort had significantly higher rates of secondary hip arthroscopy (14% vs 3%; P = .02). Improvement in PROMs was comparable between the groups.
Conclusion:
Patients ≥40 years who underwent primary hip arthroscopy with labral repair demonstrated a hip preservation rate of 78%, significant and durable improvement in PROMs, and high rates of satisfaction at a minimum 10-year follow-up. Matched analysis with patients <40 years revealed comparable improvement in patient-reported outcomes between the 2 groups, with a tendency to a higher level of arthroplasty in patients ≥40 years.
Femoroacetabular impingement syndrome (FAIS) is a clinical entity driven by atypical bony morphology on the acetabular and/or femoral head that results in abnormal distribution of contact stresses, which can lead to labral and cartilage pathology. 21 With improvement in both intraoperative technique and anchor technology, labral repair has become the gold standard for labral treatment with up to 80% of hip arthroscopies including it as a procedure. 52
Despite advances in diagnostic and surgical techniques, increasing age has been identified as a negative predictor of outcomes at 2 and 5 years after primary hip arthroscopy.13,15,26,40 Age >40 years has been a consistent threshold for identifying an older patient cohort; however, there are several studies in the literature focusing on older patient groups, aged >50 and >60 years.8,18,24,48,53 Although age alone should not preclude arthroscopic labral repair, as multiple studies have shown outcome improvements and modest rates of conversion to total hip arthroplasty in patients >40 years in short- and midterm outcome follow-ups, there is presently minimal data regarding the long-term durability of labral repair focused on this population.8,46
The purpose of this study was to (1) report minimum 10-year survivorship and outcomes in patients aged ≥40 years who underwent primary arthroscopic treatment of FAIS and labral tears and (2) perform a subanalysis comparing outcomes with a control group of patients aged <40 years. We hypothesized that (1) the study group would demonstrate favorable survivorship and significant improvements in all PROMs at a minimum 10-year follow-up and (2) patients aged ≥40 years would exhibit similar PROMs but lower survivorship than patients <40 years.
Methods
Patient Selection
Patient data were prospectively collected and retrospectively reviewed for all patients who underwent primary hip arthroscopy for FAIS and labral tearing with the senior surgeon (B.G.D.) between February 2008 and December 2011. A cutoff age of 40 years was utilized as this is the most common threshold for older populations in the hip preservation literature.18,24,26 Patients were considered eligible if they were aged ≥40 years and underwent primary hip arthroscopy with labral repair for a clinical and radiographic diagnosis of femoroacetabular impingement with preoperative outcome forms completed. Preoperative and minimum 10-year follow-up scores for patient-reported outcome measures (PROMs) were recorded (Figure 1). Exclusion criteria were labral debridement, workers’ compensation, Tönnis grade >1, or previous ipsilateral hip surgery or conditions (fracture, lateral center-edge angle [LCEA] <18°, avascular necrosis, or Legg-Calve-Perthes disease). The design of the study was a case series of participants ≥40 years of age with a subsequent propensity-matched cohort subanalysis of patients <40 years.
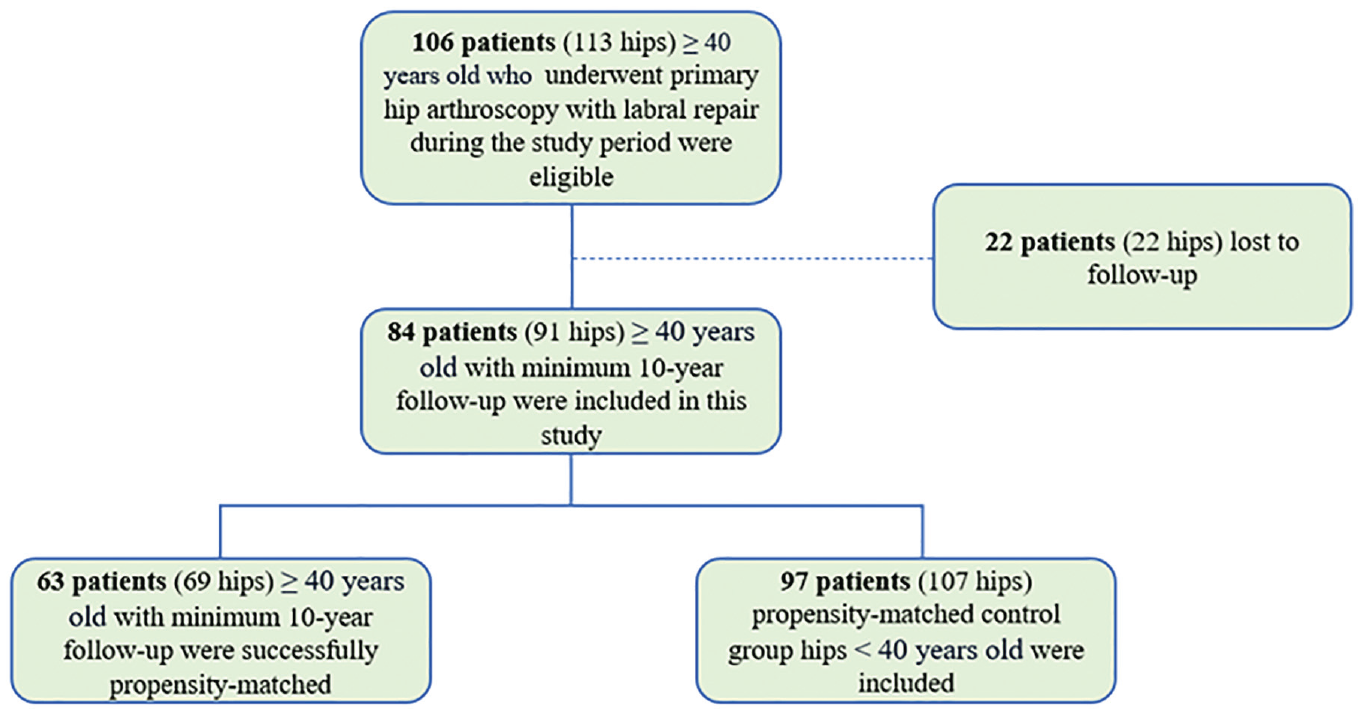
Flow diagram for patients included in the study.
Participation in the American Hip Institute Hip Preservation Registry
All patients participated in the American Hip Institute Hip Preservation Registry. Even though the present study represents a unique analysis, midterm data on some patients in this study may have been reported in other studies. 13 All data collection and reporting received institutional review board approval.
Clinical and Imaging Assessment and Surgical Indications
The senior author (B.G.D.) examined each patient's medical history and performed a comprehensive physical examination and imaging review that included assessments of the range of motion, gait, and signs of FAIS. 20 Radiographic measurements including the alpha angle, LCEA, anterior center-edge angle, Tönnis angle, and Tönnis grade were recorded as previously described.13,34 Osteoarthritis was assessed on the images using the Tönnis classification. 29 Acetabular lateral coverage was evaluated using the LCEA modified by Ogata et al. 45 The alpha angle was determined using the method established by Nötzli et al, 44 and cam morphology was defined by alpha angle >55°. Magnetic resonance arthrography (1.5 T) was used to assess additional extra- and intra-articular pathology including labral and chondral pathology. 22 Patients were instructed to attempt nonsurgical treatment for a minimum of 3 months. If nonsurgical treatments failed, patients were recommended for hip arthroscopy.
Surgical Assessment and Technique
All arthroscopies were performed by the senior surgeon. Patients were situated in the supine position on a traction table with access gained in the anterolateral, mid-anterior, and distal anterolateral accessory portals where femoroplasty and acetabuloplasty were performed as previously described (see Appendix 1, available in the online version of this article).31,33,37 Labral tears were evaluated using the Seldes classification. 50 The acetabular labrum articular disruption classification was utilized to assess chondrolabral junction damage. 51 The Outerbridge classification was used to evaluate femoral and acetabular chondral injury with a grade >2 used to identify severe cartilage damage. 18 Ligamentum teres damage was graded by the Domb 36 and Villar classifications. 23 Labral tears were treated with repair, 37 through a base refixation or a controlled-tension anatomic loop stitch placed through a distal anterolateral accessory portal.14,35,47 Capsular management strategies were evolving during the study period, with capsular release performed earlier followed by direct side-to-side repair occurring later in the study period. 17 Plication of the interportal capsulotomy was also performed for hips at risk of instability and borderline dysplasia defined by an LCEA <25°. 27
Rehabilitation Protocol
All patients were placed in a hip brace (DonJoy VersaRom; Enovis) for stability and placed on a personalized postoperative rehabilitation protocol as previously described (see Appendix 2, available online).2,16
Surgical Outcome Tools
Patients completed the modified Harris Hip Score (mHHS), 3 Non-Arthritic Hip Score (NAHS), 11 Hip Outcome Score–Sport-Specific Subscale (HOS-SSS), 38 and visual analog scale (VAS) for pain preoperatively within 1 month of their surgical date. 10 Postoperatively, patients completed questionnaires at 3 months, 1 year, and annually thereafter. The minimal clinically important difference (MCID) 43 and validated Patient Acceptable Symptom State (PASS) thresholds for postoperative hip arthroscopy outcomes were used to evaluate clinically relevant outcomes.7,9,49 Using a distribution-based method, as validated by Norman et al, 43 we calculated the MCID for all PROMs at the 10-year time point. Additionally, using threshold values from previously published literature, the numbers of patients who met the PASS for the mHHS (74 points), NAHS (85.6 points), VAS (2.16 points), and HOS-SSS (75 points) were documented.7,9,49 The hip preservation rate, also referred to as arthroplasty-free rate, was defined to include all hips that had not undergone arthroplasty, while the secondary arthroscopy rate was used to count all hips that required revision arthroscopy during the follow-up period.
Statistical Analysis
Descriptive statistics for continuous variables are reported as means, medians, standard deviations, and ranges. Categorical variables are reported as totals and percentages. Chi-square and Fisher exact tests were used to compare categorical data. Continuous variables were assessed for normality using the Shapiro-Wilk test and assessed for variance using the F test. A 2-tailed t test was used to assess normally distributed data sets with equal variance, and Wilcoxon signed-rank, Mann-Whitney U, or Welch tests were used to analyze nonparametric data where appropriate.
An a priori power analysis was conducted to determine the required sample sizes in each propensity-matched group to obtain a minimum of 80% power using a 1:2 matching ratio. Based on an expected mean difference in the mHHS of 8 points and standard deviation of 10, the power analysis determined that 19 patients aged >40 years and 39 patients aged <40 years were required (G*Power).12,19,30 For the process of propensity matching, hips in the study group can only be matched with a control group hip once. Previous studies have shown that the optimal method for controlled group comparison is greedy matching without replacement.1,6 A caliper of 0.1 times the standard deviation of the logit propensity scores was used. Greedy matching without replacement was used to match patients aged ≥40 years with patients aged <40. 5 Patients who were outside the caliper (propensity range) were excluded from analysis to ensure no differences between groups due to commonly cited confounding factors. 4
A Cox proportional hazards regression analysis was performed to report hazard ratios (HRs) of preoperative factors influencing 10-year conversion to arthroplasty in patients aged ≥40 years. Kaplan-Meier analysis was performed to assess conversion to arthroplasty and secondary hip arthroscopy. Kaplan-Meier analyses comparing the matched cohorts were assessed using a Mantel-Cox log-rank test. Analysis was performed using JMP and propensity matching with RStudio (Version 1.3.959; posit.co). The threshold for statistical significance was P < .05.17,22,25 Groups were matched in a 1:2 ratio by sex, body mass index, Tönnis grade, LCEA, and capsular treatment.
Results
Patient Characteristics and Radiographic Measurements
Of the 113 hips (106 patients) aged ≥40 years that were eligible for analysis, 91 hips (80.5%) had a minimum 10-year follow-up. Within this study cohort, there were 58 women (68.2%) and 27 men (31.8%), with a median age of 46.3 years (IQR, 44.1-51.5 years) and median body mass index of 25.1 (IQR, 22.3-29.2). There were 6 bilateral subjects all of which were in female patients. Characteristics of the study cohort are presented in Table 1. With a stratified age analysis, there were 27 hips (30%; 27 patients) >50 years and 2 hips (2%) >60 years. There were no preoperative differences in the 22 hips that were lost to follow-up (see Appendix Table A1, available online).
Patient Characteristics and Radiographic Data (N = 91 hips) a

Values are presented as n (%) or mean ± SD (range). BMI, body mass index; LCEA, lateral center-edge angle.
Intraoperative Findings and Surgical Procedures
Radiographic measurements, intraoperative findings, and surgical procedures are presented in Table 2. A total of 35 hips (38%) had severe cartilage damage of the acetabulum, while 13 hips (14%) had severe cartilage damage of the femoral head identified during diagnostic arthroscopy. When stratified by age, 14 patients (14/27, 52%) aged >50 years had severe acetabular cartilage damage compared with 21 patients (21/64, 33%) between 40 and 50 years of age (P = .09). Two patients (7.4%) >50 years had severe femoral head chondral damage compared with 11 patients (17%) between 40 and 50 years (P = .21). All hips received labral repair, while 75% underwent femoroplasty and 86% underwent acetabuloplasty for cam and pincer deformities. A total of 34 hips (37%) received capsular repair or plication.
Intraoperative Findings and Surgical Management (N = 91 hips) a

Values are presented as n (%) or mean ± SD. ALAD, acetabular labral articular disruption.
Patient-Reported Outcome Measures
The study cohort demonstrated significant improvements in all PROMs from preoperatively to a minimum 10-year follow-up (P < .001) (Figure 2). Median postoperative 10-year satisfaction with surgery was 9 of 10 (IQR, 8-10) and the VAS hip pain score was 2 (IQR, 0-3.9). Patients achieved MCID and PASS at high rates for all PROMs (Table 3).
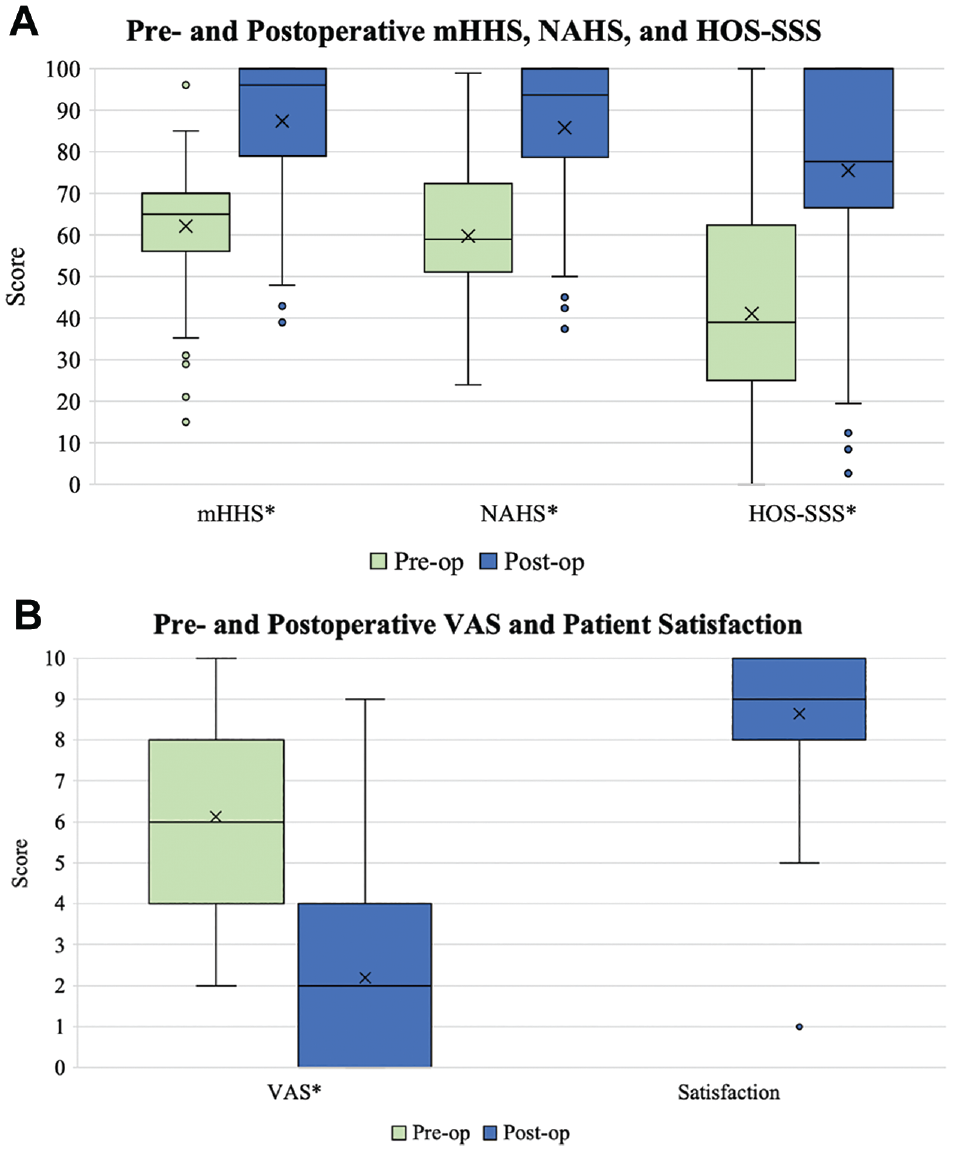
Box-and-whisker plots depicting (A) preoperative and minimum 10-year postoperative patient-reported outcome scores for the modified Harris Hip Score (mHHS), Non-Arthritic Hip Score (NAHS), and Hip Outcome Score–Sport-Specific Subscale (HOS-SSS) and (B) visual analog scale (VAS) and patient-reported satisfaction scores in patients aged ≥40 years. The X within the box indicates the mean. The box represents the interquartile range, with the horizontal line depicting the median and the boundaries of the box indicating the first and third quartiles. The whiskers of the plot are set to 1.5 times the interquartile range. Outliers are depicted as dots. *Statistically significant improvement from preoperatively to postoperatively (P < .05).
Clinically Relevant Outcome Threshold Achievement a

Values are presented as n (%). HOS-SSS, Hip Outcome Score–Sport-Specific Subscale; MCID, minimal clinically important difference; mHHS, modified Harris Hip Score; NAHS, Non-Arthritic Hip Score; PASS, Patient Acceptable Symptom State; VAS, visual analog scale.
Hip Preservation Analysis
There were 20 patients (22%) who required arthroplasty during the study period at a mean of 39.9 ± 30.5 months, with a hip preservation rate of 78%. Nineteen patients underwent total hip arthroplasty, and 1 patient underwent hip resurfacing. Four patients underwent a revision arthroscopy for labral retear at a mean of 32.9 ± 30.1 months, with 1 patient who required a revision hip arthroscopy at 10.8 months undergoing total hip arthroplasty at 38.3 months. Taken together, 23 hips required reoperation during the study. There were 9 patients aged >50 years who required arthroplasty compared with 11 patients between 40 and 50 years of age who required arthroplasty (33% vs 17%; P = .10). The patients >50 years of age required arthroplasty sooner than patients between 40 and 50 years (24.2 ± 17.0 months vs 52.8 ± 33.0 months; P = .04). A Cox proportional hazards regression model was constructed using preoperative and intraoperative variables that identified acetabuloplasty (HR, 0.21; P = .03), Tönnis grade 1 (HR, 3.34; P = .07), preoperative alpha angle (HR, 12.7; P = .06), and severe femoral head chondral injury (Outerbridge grade >2, HR, 3.53; P = .08) as the strongest predictors of conversion to total hip arthroplasty (remaining variables P > .10) (see Appendix Table A2, available online). Kaplan-Meier curves for conversion to arthroplasty as well as revision arthroscopy are presented in Figure 3.
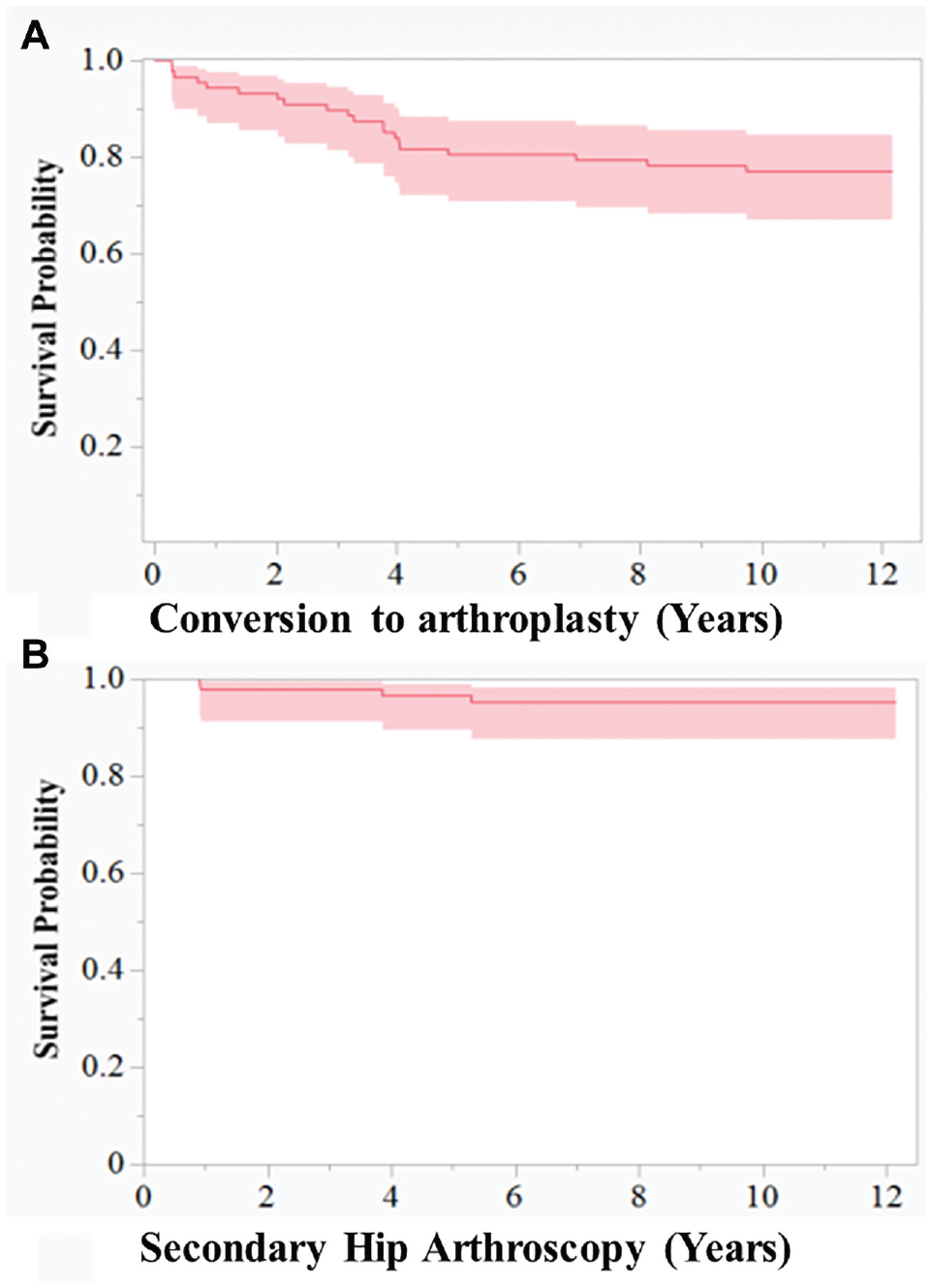
Kaplan-Meier analysis depicting timing of (A) arthroplasty and (B) secondary hip arthroscopy from the index surgery. Shaded areas represent 95% confidence intervals.
Propensity-Matched Subanalysis
Patients aged ≥40 years were matched in a 1:2 ratio to patients aged <40 years for further analysis. A total of 69 hips (63 patients) aged ≥40 years were successfully matched to 107 hips (97 patients) aged <40 years. Because of the rigorous matching criteria used to minimize the potential effect of confounding factors, the groups were unable to be perfectly matched in a 1:2 ratio. The median age of the older cohort was 45.5 years (IQR, 44-50 years; range, 40.1-62.2 years), while the median age of the younger cohort was 26.7 years (IQR, 20-32 years; range, 14.2-39.8 years). There were no differences in characteristics (other than age), radiographic measurements, or patient follow-up. There were no differences in severe chondral pathology (Outerbridge grade >2) of either the acetabulum or femoral head identified during arthroscopy (Table 4). Patients aged ≥40 years had a higher prevalence of ligamentum teres damage (P < .001) and underwent ligamentum teres debridement at higher rates (54% vs 35%; P = .02) as well as higher rates of femoroplasty (74% vs 57%; P = .03). Patients <40 years had higher rates of acetabuloplasty (94% vs 84%; P = .04) as well as iliopsoas release (52% vs 28%; P = .002).
Propensity-Matched Comparison Between Patients Aged ≥40 With Those Aged <40 Years a

Values are presented as n (%) or mean ± SD. Boldface type indicates statistical significance (P < .05). ALAD, acetabular labral articular disruption; BMI, body mass index; LCEA, lateral center-edge angle.
Outcomes Comparison Between Propensity-Matched Groups
Both groups experienced significant improvements in all PROMs from preoperatively to a minimum 10-year follow-up (P < .001) (Table 5). Postoperative mHHS, NAHS, and HOS-SSS were all significantly higher for the age <40-year cohort (P < .05), but there were no differences in improvement between groups. The preoperative VAS score for pain was significantly higher in patients aged <40 years, and this group had greater improvement in VAS score for pain (P = .01). The median 10-year postoperative VAS hip pain score was 1.9 (IQR, 0-3.5) for the older group compared with 1.3 (IQR, 0-3) for younger patients. The median 10-year postoperative satisfaction score was 9 of 10 (IQR, 8-10) for both groups. Both groups achieved an MCID or PASS for the NAHS and HOS-SSS at similar rates (Table 6). However, patients aged <40 years achieved PASS for the mHHS at significantly higher rates (88% vs 75%; P = .04).
Patient-Reported Outcome Measures for the Propensity-Matched Groups a

Values are presented as mean ± SD (range). For the Hip Outcome Score–Sport-Specific Subscale (HOS-SSS), postoperative scores were obtained in 46 and 86 hips for patients aged ≥40 and <40 years, respectively. Boldface type indicates statistical significance (P < .05). mHHS, modified Harris Hip Score; NAHS, Non-Arthritic Hip Score; VAS, visual analog scale.
Rates of Achieving Psychometric Thresholds for the Propensity-Matched Groups a

Values are presented as n (%). For the Hip Outcome Score–Sport-Specific Subscale (HOS-SSS), postoperative scores were obtained in 46 and 86 hips for patients aged ≥40 and <40 years, respectively. Boldface type indicates statistical significance (P < .05). MCID, minimal clinically important difference; mHHS, modified Harris Hip Score; NAHS, Non-Arthritic Hip Score; PASS, Patient Acceptable Symptom State; VAS, visual analog scale.
Hip Preservation Rate Between Propensity-Matched Groups
The hip preservation rate for the 69 matched patients ≥40 years was 81.2% (56 hips), with 13 patients converting to total hip arthroplasty at a mean of 38.0 months. One patient required secondary hip arthroscopy at 63.6 months postoperatively, while 1 patient who required arthroplasty at 38.3 months underwent a previous revision hip arthroscopy at 10.8 months. The hip preservation rate for the 107 patients <40 years was 91.6%, with 9 patients converting to arthroplasty at a mean of 61.5 months. Fifteen patients (14%) required revision arthroscopy at a mean of 41.0 months. There were 3 patients <40 years of age who underwent revision hip arthroscopy at a mean of 24.6 ± 22.3 months who eventually required a total hip arthroplasty at a mean of 67.2 ± 35.5 months. Patients ≥40 years of age had a lower hip preservation rate (81.2% vs 91.6%; P = .06), while patients <40 years of age had a significantly greater rate of revision hip arthroscopy (14% vs 3%; P = .02). There were no differences regarding time to secondary surgery found between groups (P > .05). Kaplan-Meier analyses are presented in Figure 4, with greater rates of arthroplasty in the ≥40-year age group (Mantel-Cox test: P = .08) and significantly greater rates of revision hip arthroscopy in the younger cohort (Mantel-Cox test: P = .02).
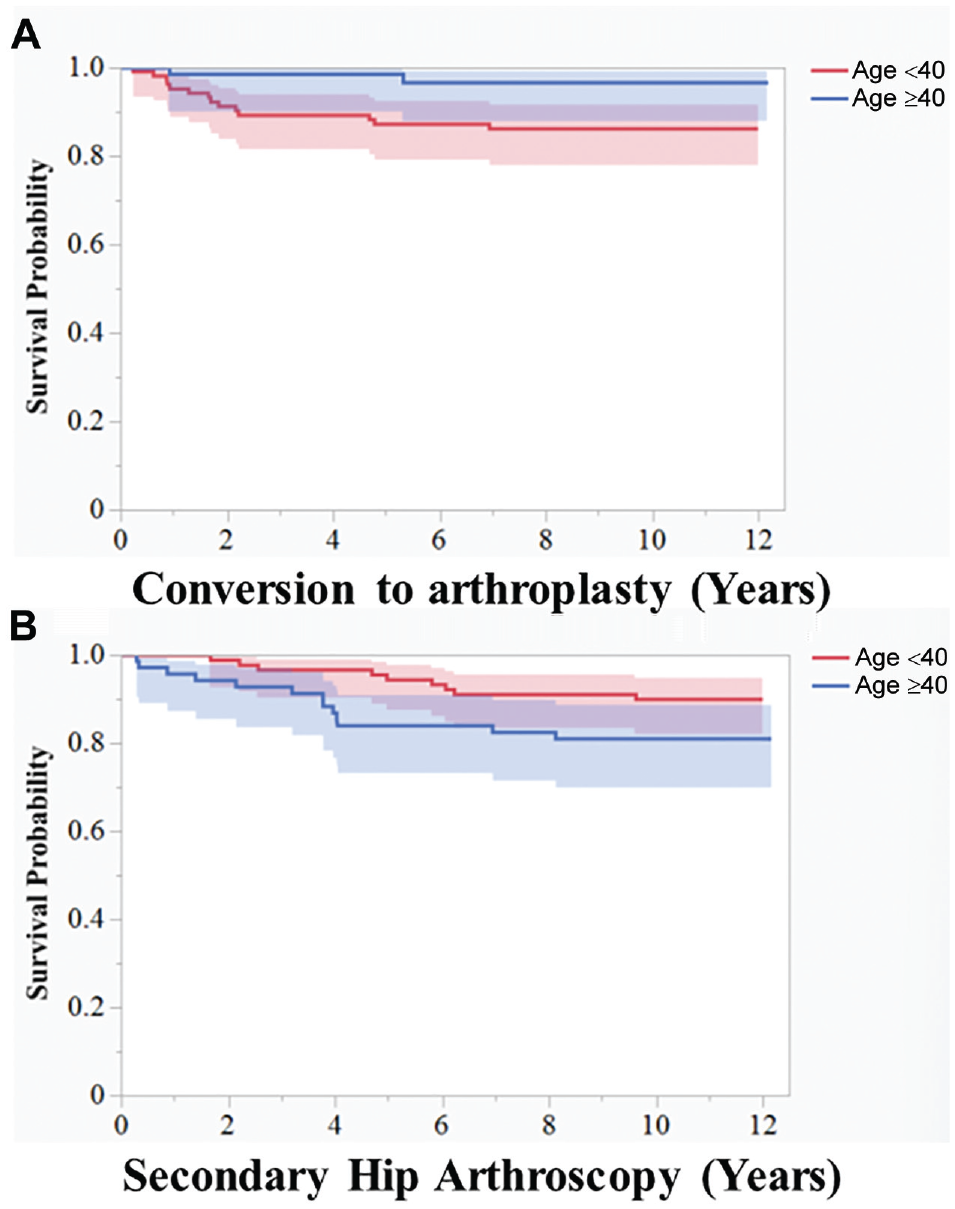
Kaplan-Meier analyses depicting timing of (A) arthroplasty and (B) secondary hip arthroscopy comparing patients aged ≥40 years (blue shading) with patients aged <40 years (red shading). There were (A) greater rates of arthroplasty in the ≥40-year group (Mantel-Cox test: P = .08) and (B) significantly greater rates of revision hip arthroscopy in the <40-year cohort (Mantel-Cox test: P = .02).
Discussion
The present analysis found that patients aged ≥40 years who underwent primary hip arthroscopy with labral repair demonstrated a hip preservation rate of 78%, sustained improvement in PROMs, and high rates of clinically relevant outcome achievement at a minimum 10-year follow-up. Matched analysis with a cohort of patients <40 years of age revealed comparable postoperative improvement and satisfaction, with increased rates of arthroplasty for patients ≥40 years and increased rates of revision hip arthroscopy for patients <40 years.
Available long-term outcomes of patients undergoing hip arthroscopy are sparse, with limited focus on older patient populations. A recent systematic review by Lee and colleagues 32 analyzing 12 studies after hip arthroscopy with minimum 10-year outcomes found revision hip arthroscopy rates ranging from 4.5% to 24% and arthroplasty rates ranging from 0% to 44.1%. The authors report lower 10-year hip preservation rates in studies with a mean age ≥35 years (n = 9), ranging from 56% to 86%, with older age identified as an independent risk factor for conversion to arthroplasty in 5 studies. These findings are confounded by variable rates of preexisting osteoarthritis, acetabular coverage, and labral repair, and no study directly compared a matched group of older patients with a younger cohort. Similar to previous reports, we found preexisting arthritis, identified radiographically as Tönnis grade >0 and intraoperatively as femoral head Outerbridge grade >2, as independent predictors of conversion to arthroplasty; however, these did not reach significance in a multivariate hazard regression model. Interestingly, acetabuloplasty was found to be a significant protective factor against arthroplasty (HR, 0.21), indicating that osseous correction may affect long-term outcomes. This was reinforced by a recent study by Nepple et al, 42 who found that long-term clinical outcomes and arthroplasty-free rates were improved in patients receiving femoroplasty during hip arthroscopy compared with those who did not (hip preservation rate, 78% vs 41%; P = .002). It is important to note that hip preservation was dramatically evolving during and after the study period, so long-term outcomes with standardized and modern techniques will be a valuable resource demanding future study.
In addition to satisfactory hip preservation rates, patients ≥40 years also reported durable therapeutic gain by maintaining significant improvement in postoperative outcome scores and achieving high rates of clinically relevant outcome thresholds 10 years after hip arthroscopy with labral repair. In 8 studies with 10-year follow-up using PROMs, there was significant postoperative improvement maintained in all hip-specific outcome measures. 32 Furthermore, the authors found that 10-year rates of achieving clinically relevant outcomes for the mHHS across 5 studies ranged from 72% to 89% and from 62% to 87% for the MCID and PASS, respectively. These are consistent with the MCID (81%) and PASS (78%) rates for the mHHS reported in the present study in patients ≥40. Younger patients may achieve higher rates of clinically relevant outcome thresholds, with Menge et al 41 reporting mHHS MCID and PASS rates of 89% and 84%, respectively, as well as HOS-SSS MCID and PASS rates of 94% and 90%, respectively, in a cohort of adolescent patients with 10-year follow-up. Despite the outcomes differences with a younger patient cohort, minimum 10-year follow-up data have shown low levels of median hip pain and high rates of median satisfaction between the older and younger groups in this study. Taken together, patients aged ≥40 years undergoing hip arthroscopy with labral repair had comparable clinical and functional outcomes compared with younger cohorts in this study and the available literature.
Despite established success, hip preservation in an older population must be approached with care. Horner et al 26 analyzed 9954 patients aged >40 years across 17 studies and reported hip preservation rates of 81.9%, 76.9%, and 75.0% for those aged >40, >50, and >60 years, respectively, with a short-term follow-up averaging 25.0 months. Griffin et al 24 performed a similar review in patients >40 years of age, with favorable results in 7 of 8 of the included studies and a hip preservation rate of 81.5% at a mean follow-up of 32.9 months. With a longer follow-up of 10 years, we report a hip preservation rate of 78% for patients aged ≥40 years. With a subgroup analysis of the ≥40-year cohort, hip preservation rates of 83% for patients between ages 40 and 50 years and 67% for patients aged >50 years were found. Furthermore, we found that patients >50 years of age had a 52% rate of severe acetabular chondral damage compared with 33% for the group between 40 and 50 years of age. Confounding factors such as higher levels of preexisting radiographic arthritis as well as intraoperative chondral damage in an older population may play a larger role in conversion to arthroplasty than age alone.28,39,51
Strengths
There are several strengths in the present study. First, this study adds to the knowledge of long-term outcomes after labral repair in older age groups, which to date has been limited. Propensity score matching was utilized to minimize the effects of potential confounding factors, diminishing the risk of type 2 error. Furthermore, the use of multiple validated functional hip outcome scores designed to assess outcomes in active patients with nonarthritic hips limits the potential ceiling effect and increases the generalizability of results. Finally, multiple clinical psychometric tools were utilized to assess the achievement of clinically relevant outcomes. 25
Limitations
As this was a nonrandomized study, confounding variables may have influenced results. Although data were prospectively collected, the data were analyzed retrospectively. Additionally, analysis was based on patients operated on by a single high-volume hip preservation surgeon, which may limit generalizability or lead to nonreproducible findings. Furthermore, surgical techniques evolved substantially over the study period, which may affect applicability for more modern techniques and approaches. The study was not powered to evaluate subgroup differences in the age-stratified population between the 40- to 50-year age group and >50-year age group, and younger patients were more likely to receive revision arthroscopy while older patients were more likely to undergo arthroplasty, which may reflect a bias to continue to pursue joint preservation for the younger cohort. The management of the hip capsule was also evolving during the study period, resulting in a lower rate of capsular closure compared with more recent trends in hip arthroscopy using modern techniques. Finally, although conversion to arthroplasty was used as a proxy for osteoarthritis progression, an independent radiographic analysis of progressive osteoarthritis was not performed, which may be of benefit for future studies.
Conclusion
Patients ≥40 years who underwent primary hip arthroscopy with labral repair demonstrated a 10-year hip preservation rate of 78%, durable therapeutic gain in PROMs, and high rates of achievement of the MCID or PASS. Matched analysis with patients <40 years of age revealed comparable improvement in patient-reported outcomes between the 2 groups with higher rates of arthroplasty in patients aged ≥40 years.
Supplemental Material
sj-pdf-1-ajs-10.1177_03635465241270291 – Supplemental material for Ten-Year Outcomes in Patients Aged 40 Years and Older After Primary Arthroscopic Treatment of Femoroacetabular Impingement With Labral Repair
Supplemental material, sj-pdf-1-ajs-10.1177_03635465241270291 for Ten-Year Outcomes in Patients Aged 40 Years and Older After Primary Arthroscopic Treatment of Femoroacetabular Impingement With Labral Repair by Benjamin G. Domb, Jade S. Owens, Ajay C. Lall, W. Taylor Harris and Benjamin D. Kuhns in The American Journal of Sports Medicine
Footnotes
Submitted December 27, 2023; accepted June 3, 2024.
One or more of the authors has declared the following potential conflict of interest or source of funding: This study was funded by Arthrex (IIRR-01507). B.G.D. has had ownership interests in the American Hip Institute, Hinsdale Orthopaedics, SCD#3, North Shore Surgical Suites, and Munster Specialty Surgery Center; has received research support from Arthrex, the Kauffman Foundation, and Stryker; consulting fees from Adventist Hinsdale Hospital, Arthrex, Medacta, Stryker, and SI-BONE; educational support from Arthrex, Breg, Medacta, and Medwest Associates; speaking fees from Arthrex; honoraria from Medacta; travel and lodging payments from Arthrex, Medacta, and Stryker; food and beverage payments from Arthrex, Medacta, Stryker, DJO Global, and Zimmer Biomet; and royalties from Amplitude, Arthrex, DJO Global, Medacta, Stryker, and Orthomerica. B.G.D. is medical director of hip preservation at St. Alexius Medical Center; and board member for the American Hip Institute Research Foundation, AANA Learning Center Committee, Journal of Hip Preservation Surgery, and Journal of Arthroscopy. The American Hip Institute Research Foundation funds research and is where this study was performed. A.C.L. has received support for education from Arthrex, Medwest, and Smith & Nephew; research support from Arthrex, Stryker, and Medacta; hospitality payments from Smith & Nephew, Stryker, Zimmer Biomet, and Arthrex; and consulting fees from Arthrex, Stryker, and Graymont Medical. A.C.L. is the co–medical director of hip preservation at St. Alexius Medical Center, a clinical instructor at the University of Illinois College of Medicine, and a member of the AANA Learning Center Committee. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.