
Abstract
Background:
Despite the growing volume of neighborhood-level health disparity research, there remains a paucity of prospective studies investigating the relationship between Area Deprivation Index (ADI) and functional outcomes for patients undergoing hip arthroscopy.
Purpose:
To investigate the relationship between neighborhood-level socioeconomic status and functional outcomes after hip arthroscopy.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
A retrospective analysis of prospectively collected data was performed on patients aged ≥18 years with minimum 1-year follow-up who underwent hip arthroscopy for the treatment of symptomatic labral tears. The study population was divided into ADILow and ADIHigh cohorts according to ADI score: a validated measurement of neighborhood-level socioeconomic status standardized to yield a score between 1 and 100. Patient-reported outcome measures (PROMs) included the modified Harris Hip Score, Nonarthritic Hip Score, Hip Outcome Score–Activities of Daily Living, Hip Outcome Score–Sports-Specific Subscale, 33-item International Hip Outcome Tool, visual analog scale for pain, and patient satisfaction.
Results:
A total of 228 patients met inclusion criteria and were included in the final analysis. After patients were stratified by ADI score (mean ± SD), the ADILow cohort (n = 113; 5.8 ± 3.0; range, 1-12) and ADIHigh cohort (n = 115; 28.0 ± 14.5; range, 13-97) had no differences in baseline patient demographics. The ADIHigh cohort had significantly worse preoperative baseline scores for all 5 PROMs; however, these differences were not present by 1-year follow-up. Furthermore, the 2 cohorts achieved similar rates of the minimal clinically important difference for all 5 PROMs and the Patient Acceptable Symptom State for 4 PROMs. When controlling for patient demographics, patients with higher ADI scores had greater odds of achieving the minimal clinically important difference for all PROMs except the 33-item International Hip Outcome Tool.
Conclusion:
Although hip arthroscopy patients experiencing a greater neighborhood-level socioeconomic disadvantage exhibited significantly lower preoperative baseline PROM scores, this disparity resolved at 1-year follow-up. In fact, when adjusting for patient characteristics including ADI score, more disadvantaged patients achieved greater odds of achieving the minimal clinically important difference. The present study is merely a first step toward understanding health inequities among patients seeking orthopaedic care. Further development of clinical guidelines and health policy research is necessary to advance care for patients from disadvantaged communities.
As medicine continues to emphasize the importance of holistic, patient-centered care, it is imperative that orthopaedic surgeons understand the influence of social determinants of health (SDOH) on patient outcomes.11,13 SDOH is an umbrella term that encompass a patient's economic stability, access to quality education, health care accessibility, neighborhood and built environment, and sense of community. 53 This combination of individual, institutional, and environmental factors may significantly influence a patient's ability to access quality health care, trust one's medical provider, or adequately follow postoperative instructions. 4 Together, these health inequities can accumulate over an individual's lifetime and contribute to higher rates of complications, readmission, and mortality for various types of surgery, ranging from anterior cruciate ligament reconstruction and rotator cuff repair to total knee arthroplasty.17,19,24,42,52,54,60
In orthopaedics, studies investigating the relationship between SDOH and postoperative outcomes have primarily utilized large databases, such as the National Inpatient Sample, the American College of Surgeons’ National Surgical Quality Improvement Program, or the PearlDiver database.1,3,5,6,21,23,39,45 A limitation with these studies, however, is that they lack prospective functional outcomes, patient satisfaction, and complications beyond 90-day follow-up. 7 Conversely, most nondatabase studies that collect patient-reported outcome measures (PROMs) focus on a single social determinant, such as race, ethnicity, insurance status, income, education level, employment status, or socioeconomic status (SES).12,38,43,46 Although the effect of these individual-level SDOH factors account for some variance in patient outcomes and warrant further exploration, neighborhood-level factors such as environment and accessibility to social services also play a key role in influencing overall health. 32 These limitations led to the development of the Area Deprivation Index (ADI), a validated score funded by the National Institutes of Health that calculates neighborhood-level socioeconomic disadvantage according to a composite measure of 17 census variables across the following domains: income, education, employment, and housing quality. 18
The potential of the ADI to guide health disparity research and improve health care accessibility has led to its widespread utilization in orthopaedic surgery research. 25 Recent studies have explored the association between ADI score and patient outcomes such as prolonged hospital stay, postoperative complications, and the Patient-Reported Outcomes Measurement Information System—a validated measurement of physical function, pain interference, depression, and anxiety.37,49,50 Despite the growing volume of neighborhood-level health disparity research, there remains a paucity of high-quality prospective studies investigating the relationship between ADI and functional outcomes for patients undergoing hip arthroscopy. The primary purpose of the present study was to examine whether patients from neighborhoods with greater socioeconomic disadvantage experienced inferior functional outcomes. Secondary outcomes consisted of rates of achieving the minimal clinically important difference (MCID) or Patient Acceptable Symptom State (PASS),9,35,44,57 patient satisfaction, likelihood of choosing the same treatment again, and rates of revision hip arthroscopy or conversion to total hip arthroplasty. We hypothesized that patients experiencing greater neighborhood-level socioeconomic disadvantage would report worse preoperative baseline PROM scores and postoperative outcomes.
Methods
Study Population
Institutional review board approval (2019P002191/2013P001442) was obtained to perform a retrospective analysis of prospectively collected data on patients who underwent hip arthroscopy for the treatment of symptomatic labral tears secondary to femoroacetabular impingement. All patients were treated by a single fellowship-trained surgeon (S.D.M.) at a large academic hospital in New England between May 2014 and October 2023. Before surgery, all patients presenting to the clinic with hip pain underwent preoperative evaluation consisting of hip and pelvis radiographs (ie, anteroposterior pelvic and Dunn lateral views), a physical examination with provocative testing of the labrum, and assessment for impingement-related symptoms (eg, pain and/or limited range of motion with flexion, adduction, and internal rotation or flexion, abduction, and external rotation).14,30 Patients indicating positive clinical and radiographic findings underwent magnetic resonance arthrography to evaluate for labral pathology, a diagnostic intra-articular hip joint/corticosteroid injection, and a minimum 3 months of nonoperative management that included formal physical therapy. Patients with persistent hip pain consented for hip arthroscopy and were offered enrollment in this study. 40
Area Deprivation Index
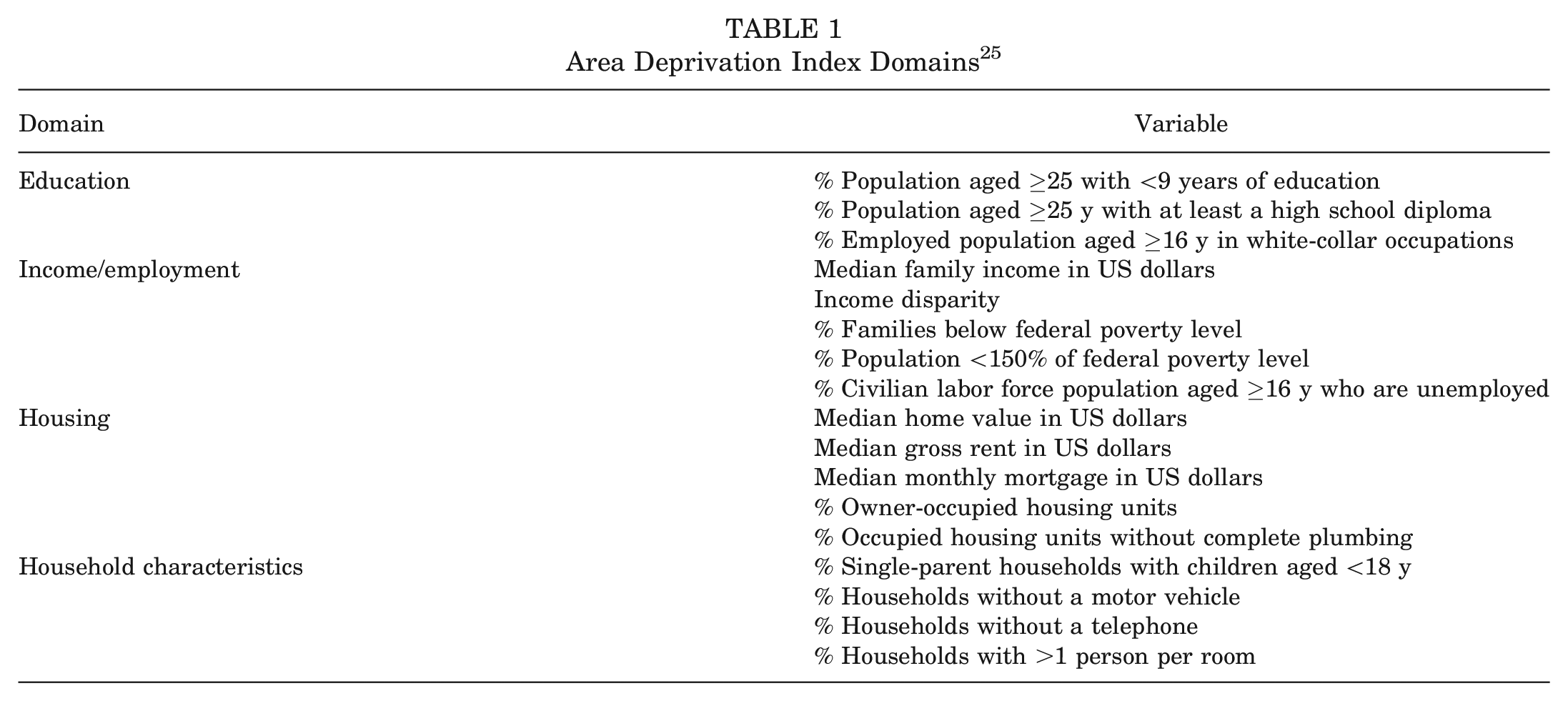
The ADI is a validated score that measures neighborhood-level socioeconomic disadvantage. Originally developed by the Health Resources and Services Administration and later refined, adapted, and validated by the Center for Health Disparities Research at the University of Wisconsin–Madison, the ADI grades census block groups by the following neighborhood-level domains: income, education, employment, and housing quality (Table 1).18,33 Once scored, census block groups are normalized and provided as an ADI national percentile ranking from 1 to 100, with a census block with an ADI of 1 indicating the lowest level of “disadvantage” and 100 indicating the highest level of disadvantage. By utilizing patient addresses, census block groups were assigned and their ADI scores collected.
Area Deprivation Index Domains 25
Patient Selection
Among our study population, patients in the present study were aged ≥18 years, underwent primary hip arthroscopy for the treatment of symptomatic labral tears secondary to femoroacetabular impingement (cam, pincer, or mixed), had complete preoperative baseline and minimum 1-year postoperative PROMs, and resided in the New England region of the United States. Patients were excluded if they received labral debridement, demonstrated advanced hip osteoarthritis (Tönnis >1), had radiographic evidence of hip dysplasia (lateral center-edge angle <20°), underwent previous surgery of the ipsilateral hip/leg, or resided in a neighborhood missing from the ADI ranking (Figure 1). 18
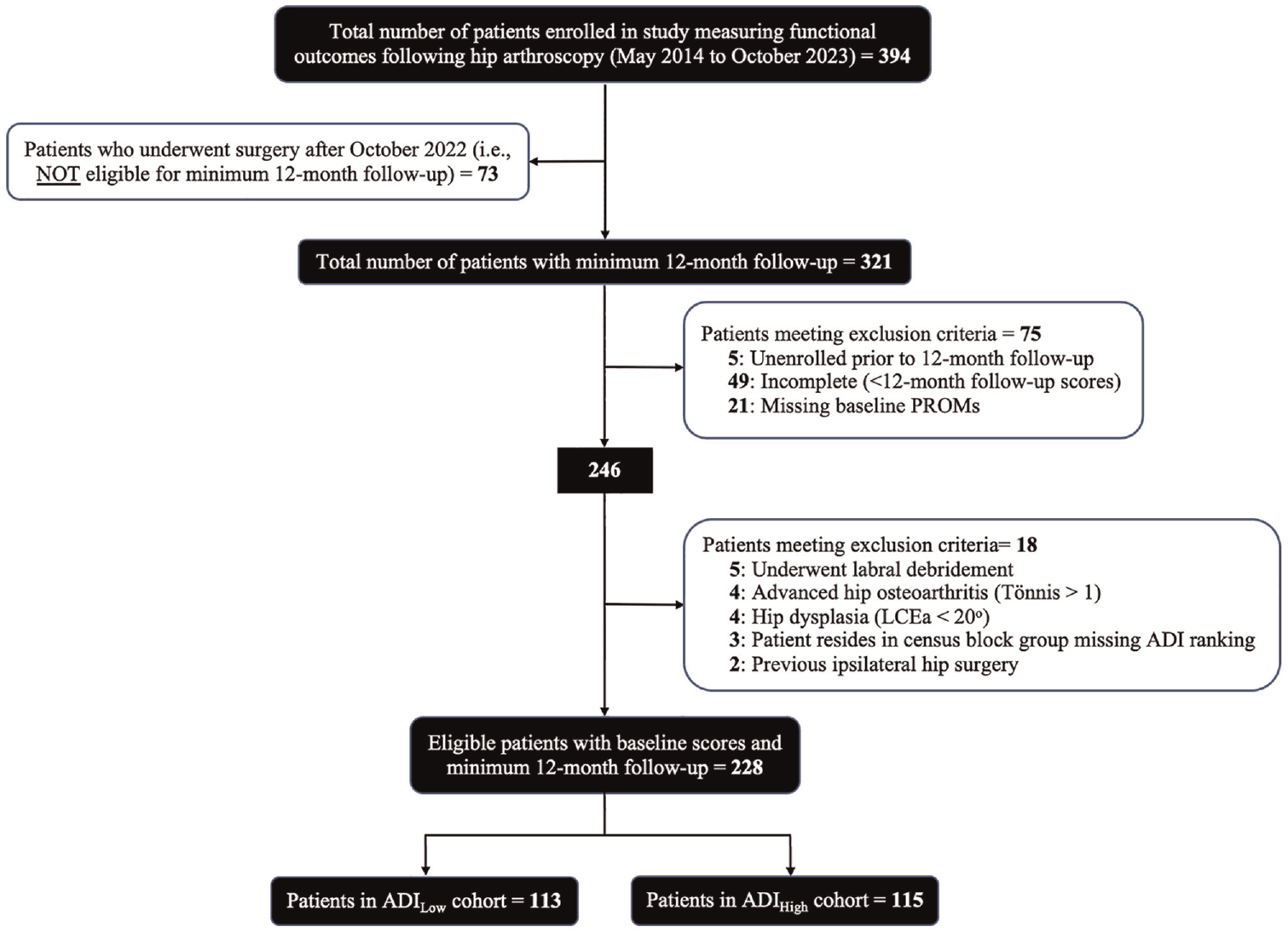
Flowchart detailing eligibility/selection criteria of patients with minimum 1-year follow-up. ADI, Area Deprivation Index; LCEA, lateral center-edge angle; PROM, patient-reported outcome measure.
Outcomes
ADI scores of patients meeting inclusion criteria were normalized to a relative mean percentile of 50%, and the top and bottom halves of patients were stratified into 2 cohorts: ADIHigh (most socioeconomic deprivation) and ADILow (least socioeconomic deprivation), respectively. The primary outcomes were the modified Harris Hip Score (mHHS), Hip Outcome Score–Activities of Daily Living (HOS-ADL), Hip Outcome Score–Sports-Specific Subscale (HOS-SSS), Nonarthritic Hip Score (NAHS), 33-item International Hip Outcome Tool (iHOT-33), and visual analog scale (VAS) for pain. Questionnaires were completed before surgery and at 3, 6, and 12 months after surgery. Secondary outcomes consisted of rates of achieving the MCID or PASS,9,35,44,57 patient satisfaction, likelihood of choosing the same treatment again, and rates of revision hip arthroscopy or conversion to total hip arthroplasty.
Abbreviated Surgical Technique
After administration of general anesthesia, the patient was positioned supine on a hip distraction table (Advanced Supine Hip Positioning System; Smith & Nephew) with a well-padded perineal post. To preserve the iliofemoral ligament and zona orbicularis, intra-articular access was facilitated via the puncture capsulotomy technique with anterolateral, anterior, midanterior, and Dienst portals, as previously described.2,10,22 In efforts to mitigate neurovascular complications and maintain ambient intra-articular temperatures for chondrolabral junction preservation, sparing use of intermittent traction and pulsed intra-articular lavage, respectively, were applied.28,34,36,51,56 Acetabular and femoral osteoplasty was performed as indicated without violation of the chondrolabral junction. 56 Repair was performed for small, discrete, linear tears that had adequate healthy tissue amenable to suture anchor fixation. If the labrum was irreparable owing to the indication of complex tears, tears involving the chondrolabral junction, or degenerative labral tissue, labral augmentation via capsular autograft was performed.34,36 After labral repair or augmentation, traction was fully released to ensure restoration of the hip suction seal and formation of an anatomic “in-round” repair. 51
Notably, during the study period, the senior surgeon's method of treating full-thickness chondral flaps, focal Outerbridge grade ≥2 lesions, and/or chondrolabral junction breakdown shifted from microfracture (May 2014 to November 2016) to a standardized method of bone marrow aspirate concentrate augmentation (December 2016 to October 2023).20,26,27,55 There was no other notable variation in surgical technique by the senior surgeon (S.D.M.) within the study period. All costs associated with bone marrow aspirate concentrate were covered by the Conine Family Fund for Joint Preservation (a philanthropic organization without affiliations to industry), ensuring equitable patient access.
Postoperative Rehabilitation
All patients followed the same 5-phase patient-guided rehabilitation protocol. 31 Because of the minimally invasive puncture capsulotomy technique that does not disrupt the iliofemoral ligament, postoperative use of a hip brace or continuous passive motion therapy was not necessary. Patients who experienced slow improvements were allowed to begin formal physical therapy at 6 months postoperatively. Those with significant persistent pain or lack of function underwent revision hip arthroscopy or conversion to total hip arthroplasty.
Statistical Analysis
Pearson χ2 test and Fisher exact test were used to compare categorical variables; 2-sample t tests were used to compare continuous variables. A multivariable-adjusted logistic regression analysis, controlling for ADI score (1-100), age, sex, body mass index, laterality, and Tönnis grade, was performed to predict achievement of clinically meaningful thresholds. ADI was used on a continuous 1-100 scale to best indicate a patient's odds of achieving the MCID/PASS, which would improve the study's generalizability for patients across communities with a range of ADI scores. The threshold for statistical significance was set to .05. All statistical analyses were performed using Stata software (Version 18.0; StataCorp).
Results
Study Population
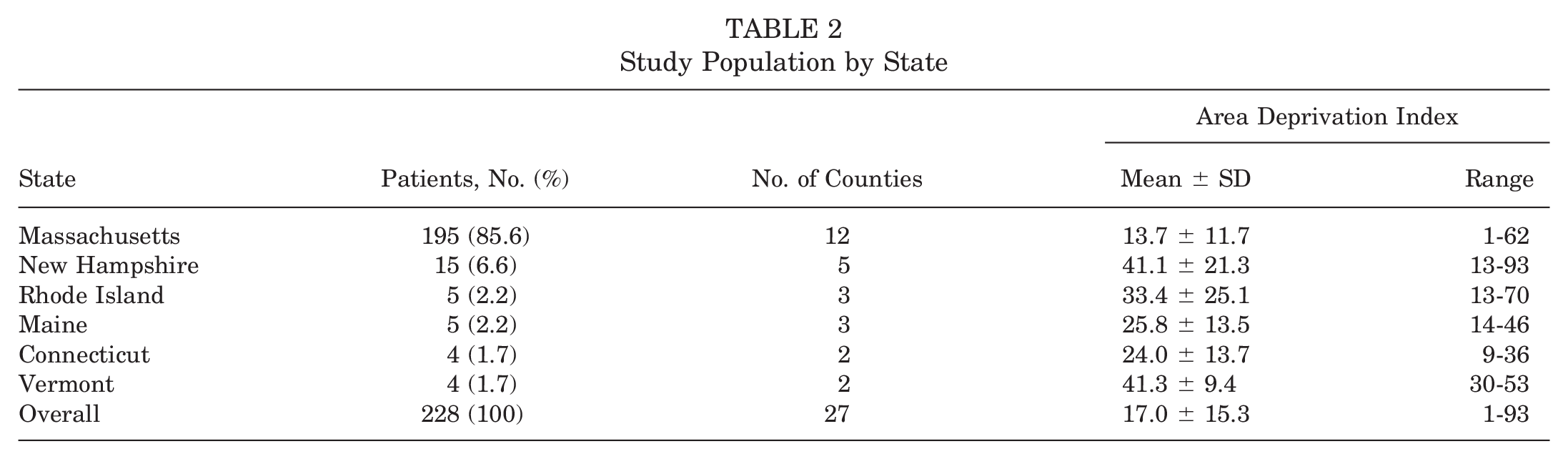
Of the 321 patients prospectively enrolled in the present study who underwent primary hip arthroscopy for the treatment of symptomatic labral tears secondary to femoroacetabular impingement and had a minimum 12-month follow-up, 228 (71.0%) met inclusion/exclusion criteria and were included in the final analysis. Of these patients, 113 were allocated to the ADILow cohort and 115 to the ADIHigh cohort (Figure 1). When stratified by state, most patients resided in Massachusetts (n = 195; 85.6%), followed by New Hampshire (n = 15; 6.6%), Rhode Island (n = 5; 2.2%), Maine (n = 5; 2.2%), Connecticut (n = 4; 1.7%), and Vermont (n = 4; 1.7%). The mean ± SD ADI score across all patients (n = 228) was 17.0 ± 15.3 (range, 1-93). Patients from Massachusetts exhibited the lowest overall ADI score (least socioeconomic disadvantage; 13.7 ± 11.7; range, 1-62), while patients from New Hampshire (41.1 ± 23.1; range, 13-93) and Vermont (41.3 ± 9.4; range, 30-53) exhibited the highest (most socioeconomic disadvantage) (Table 2). The average ADI score by county ranged from 6 to 67. Figure 2 represents the normalized distribution of ADI scores by county, stratified and color coded by decile ranking.
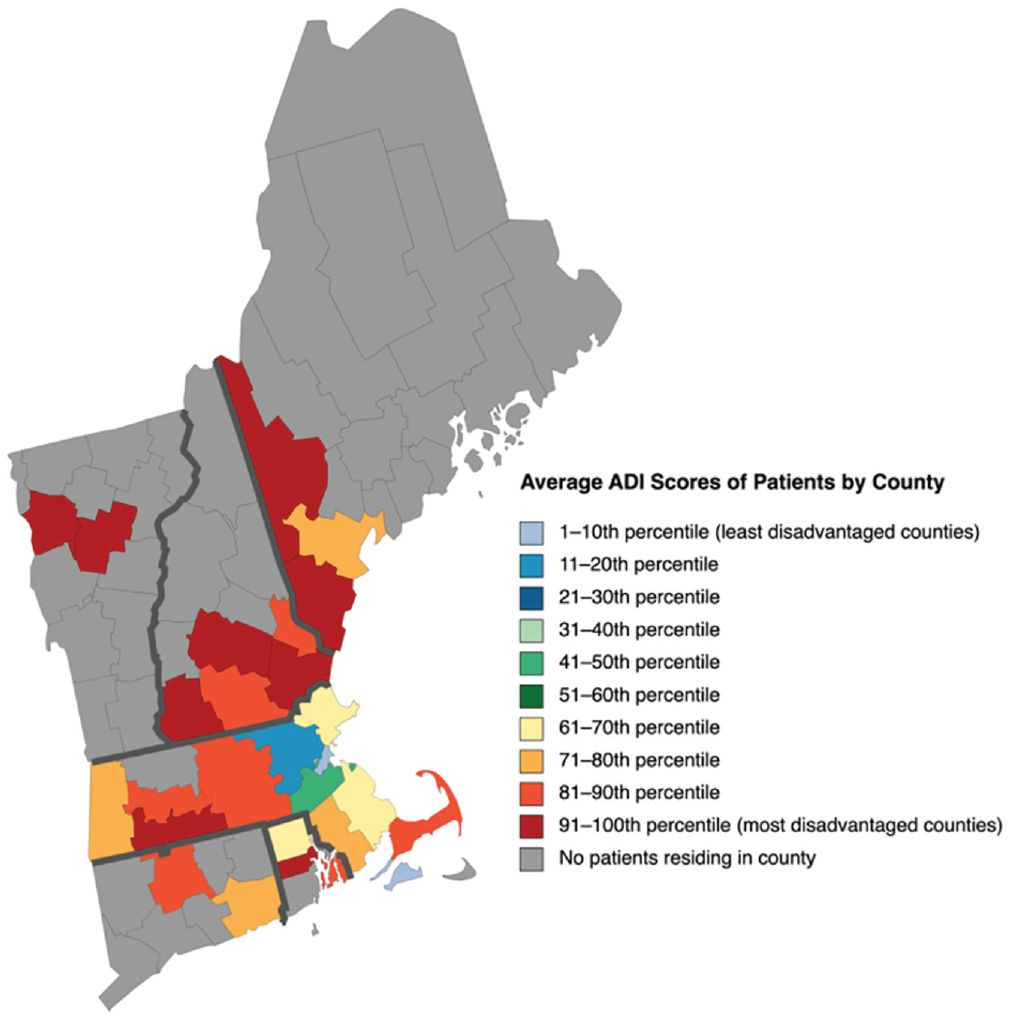
Normalized distribution of Area Deprivation Index (ADI) scores by county, stratified and color-coded by decile ranking.
Study Population by State
Subgroup Descriptive Differences
The ADILow cohort (n = 113; 1st-50th percentiles) had an ADI score of 5.8 ± 3.0 (range, 1-12) while the ADIHigh cohort (n = 115; 51st-100th percentiles) had a score of 28.0 ± 14.5 (range, 13-93). When patient baseline demographics were examined, besides ADI score (P < .001), the ADILow and ADIHigh cohorts had no differences in age, body mass index, sex, Tönnis grade, laterality, labral management, and additional chondral treatment. A complete breakdown of baseline demographics is found in Table 3.
Patient Demographics and Surgical Management a
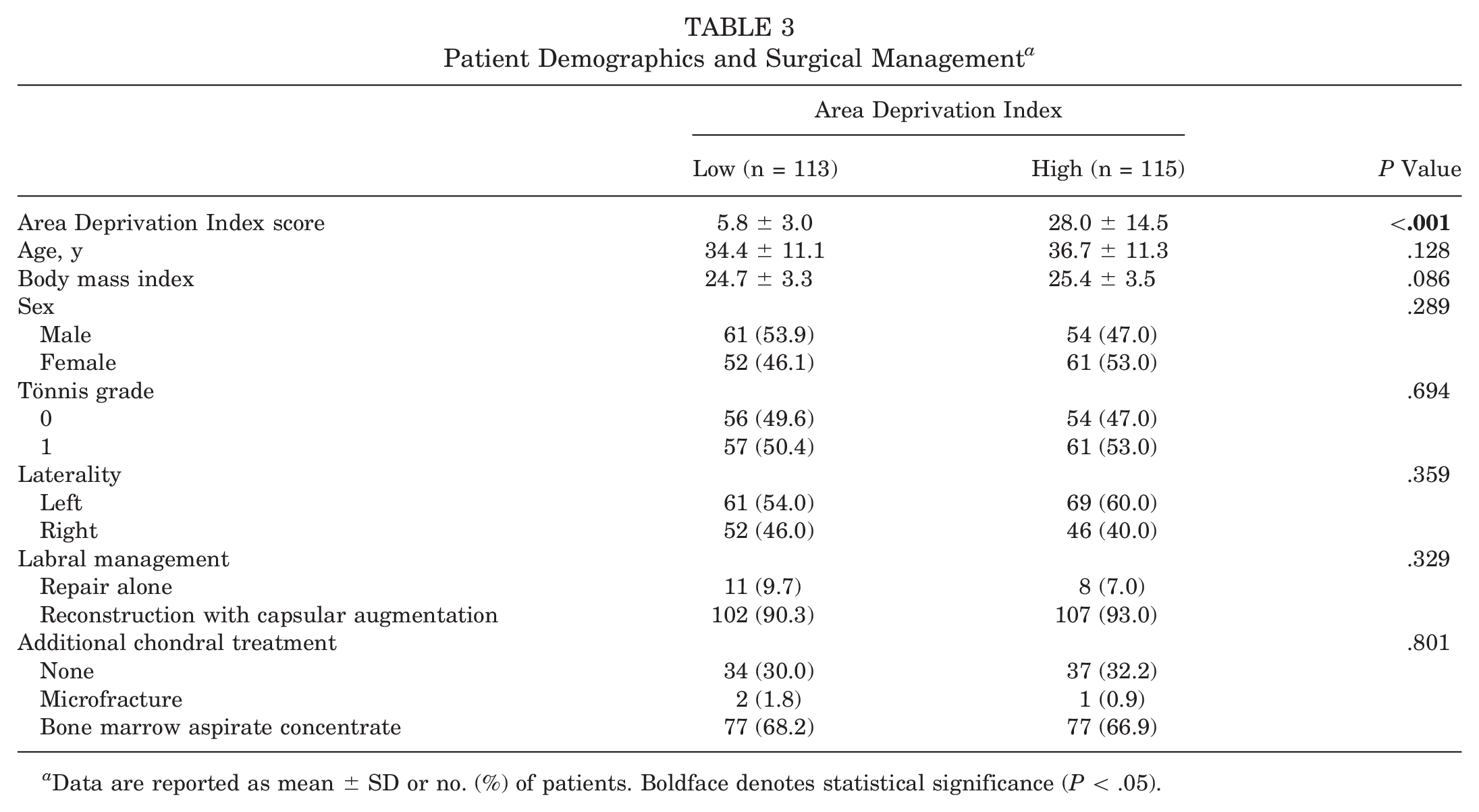
Data are reported as mean ± SD or no. (%) of patients. Boldface denotes statistical significance (P < .05).
Functional Outcomes
When mean preoperative baseline PROM scores were compared between groups, a lower ADI score (ADILow) was associated with significantly higher scores as compared with a higher ADI score (ADIHigh) for all 5 PROMs: mHHS (66.3 ± 13.1 vs 61.8 ± 14.9; P = .017), HOS-ADL (74.5 ± 17.7 vs 67.6 ± 18.7; P = .005), HOS-SSS (47.8 ± 24.1 vs 41.1 ± 23.7; P = .034), NAHS (68.2 ± 16.8 vs 63.0 ± 17.3; P = .023), and iHOT-33 (43.8 ± 16.9 vs 38.6 ± 17.4; P = .024). At 1-year follow-up, however, these disparities in PROM scores resolved, with both groups reporting similar functional outcomes (Table 4). Notably, there were no differences in VAS pain level between ADI groups at any time point. Patients in the ADILow and ADIHigh cohorts reported similar levels of patient satisfaction and rates of answering yes when asked, “Yes/no—would you receive the same treatment again?” Last, no patient in either ADI cohort underwent revision hip arthroscopy or conversion to total hip arthroplasty at 1-year follow-up.
Patient-Reported Outcome Measures a
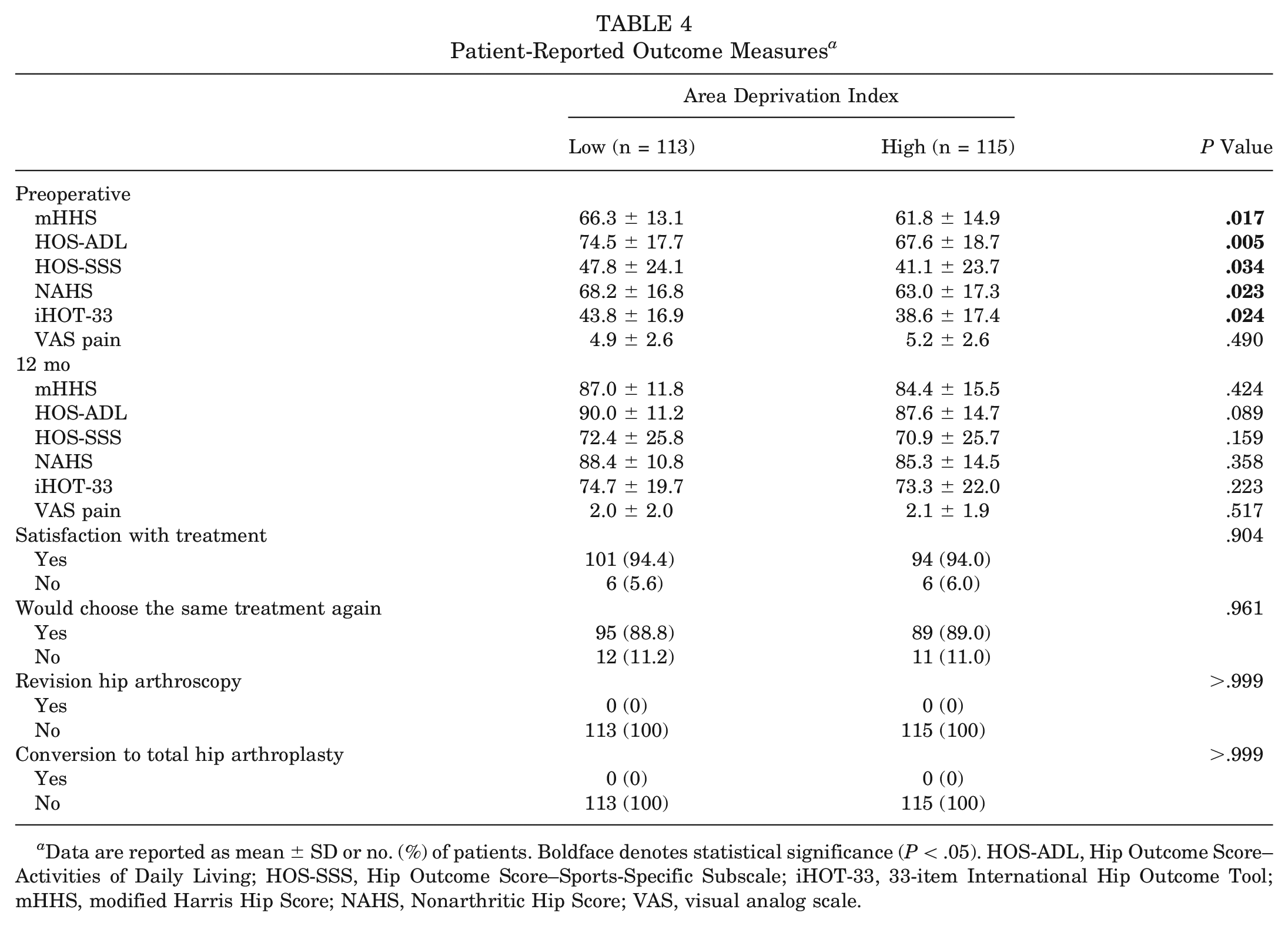
Data are reported as mean ± SD or no. (%) of patients. Boldface denotes statistical significance (P < .05). HOS-ADL, Hip Outcome Score–Activities of Daily Living; HOS-SSS, Hip Outcome Score–Sports-Specific Subscale; iHOT-33, 33-item International Hip Outcome Tool; mHHS, modified Harris Hip Score; NAHS, Nonarthritic Hip Score; VAS, visual analog scale.
PROM Improvement From Baseline
When overall improvement was assessed in PROM and VAS pain scores at 1-year follow-up as compared with baseline, there were no significant differences between the ADILow and ADIHigh cohorts (Table 5).
Δ Patient-Reported Outcome Measure Improvement From Baseline a
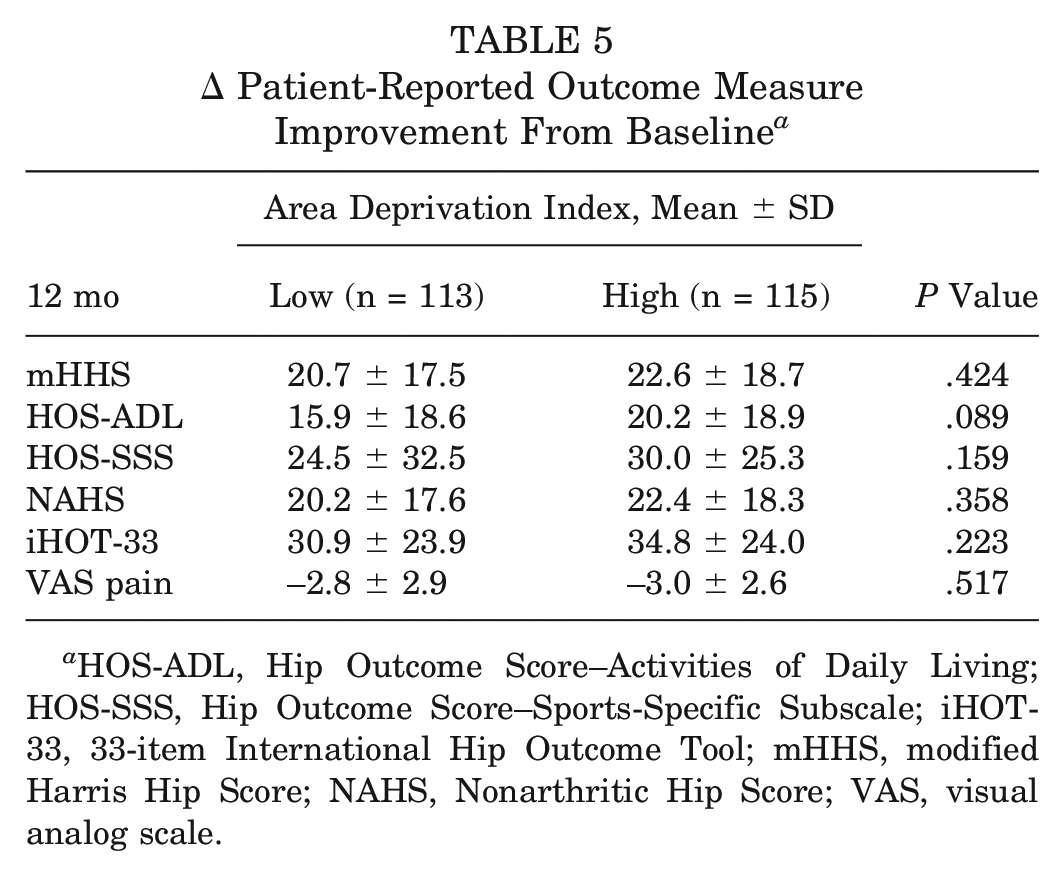
HOS-ADL, Hip Outcome Score–Activities of Daily Living; HOS-SSS, Hip Outcome Score–Sports-Specific Subscale; iHOT-33, 33-item International Hip Outcome Tool; mHHS, modified Harris Hip Score; NAHS, Nonarthritic Hip Score; VAS, visual analog scale.
Rates of Achieving Clinically Meaningful Outcomes
There was a minimal number of differences in MCID and PASS achievement rates at 1-year follow-up for the mHHS, HOS-ADL, HOS-SSS, NAHS, or iHOT-33 (Table 6). Specifically, at 1-year follow-up, rates of achieving the HOS-ADL MCID for the ADILow and ADIHigh cohorts were 60.2% and 76.3% (P = .009). All other rates of achieving clinically meaningful outcomes were insignificant. Multivariate logistic regression, however, showed that at 1-year follow-up, patients with higher ADI scores had significantly increased odds of attaining the MCID for nearly all PROMs when controlling for ADI score, age, body mass index, sex, laterality, and Tönnis grade. Younger age was associated with greater odds of attaining the MCID for all PROMs (eg, the odds of achieving the MCID for mHHS decreased by 6% for every 1 additional year of age). Finally, female sex increased the odds of the MCID for the mHHS (odds ratio [OR], 3.48; P = .002), HOS-ADL (OR, 2.59; P = .004), and iHOT-33 (OR, 2.19; P = .032). Similarly, younger age and Tönnis grade were significant predictors for achieving the PASS for 4 and 3 PROMs, respectively. Patients with Tönnis grade 1 had lower odds of achieving the PASS for the HOS-SSS (OR, 0.55; P = .043), NAHS (OR, 0.43; P = .016), and iHOT-33 (OR, 0.46; P = .011) (Table 7).
Unadjusted Rates of Achieving the MCID and PASS at 12 Months a
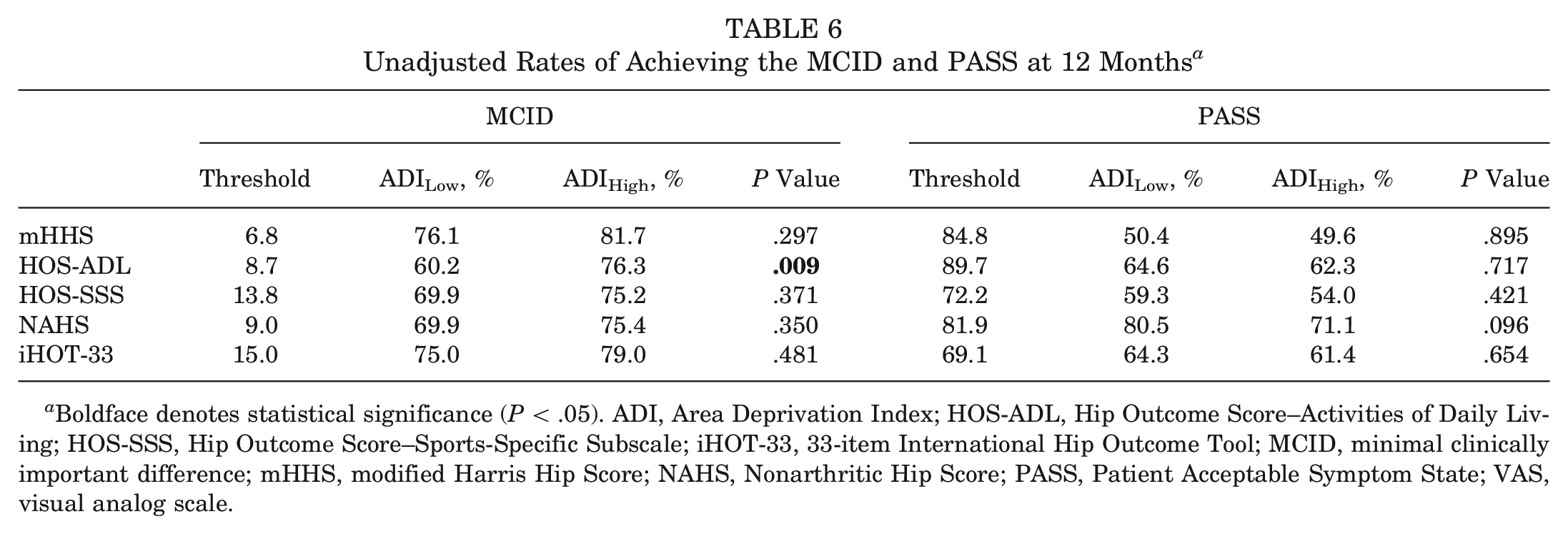
Boldface denotes statistical significance (P < .05). ADI, Area Deprivation Index; HOS-ADL, Hip Outcome Score–Activities of Daily Living; HOS-SSS, Hip Outcome Score–Sports-Specific Subscale; iHOT-33, 33-item International Hip Outcome Tool; MCID, minimal clinically important difference; mHHS, modified Harris Hip Score; NAHS, Nonarthritic Hip Score; PASS, Patient Acceptable Symptom State; VAS, visual analog scale.
Multivariate Logistic Regression for Attainment of the MCID and PASS at 1-Year Follow-up a
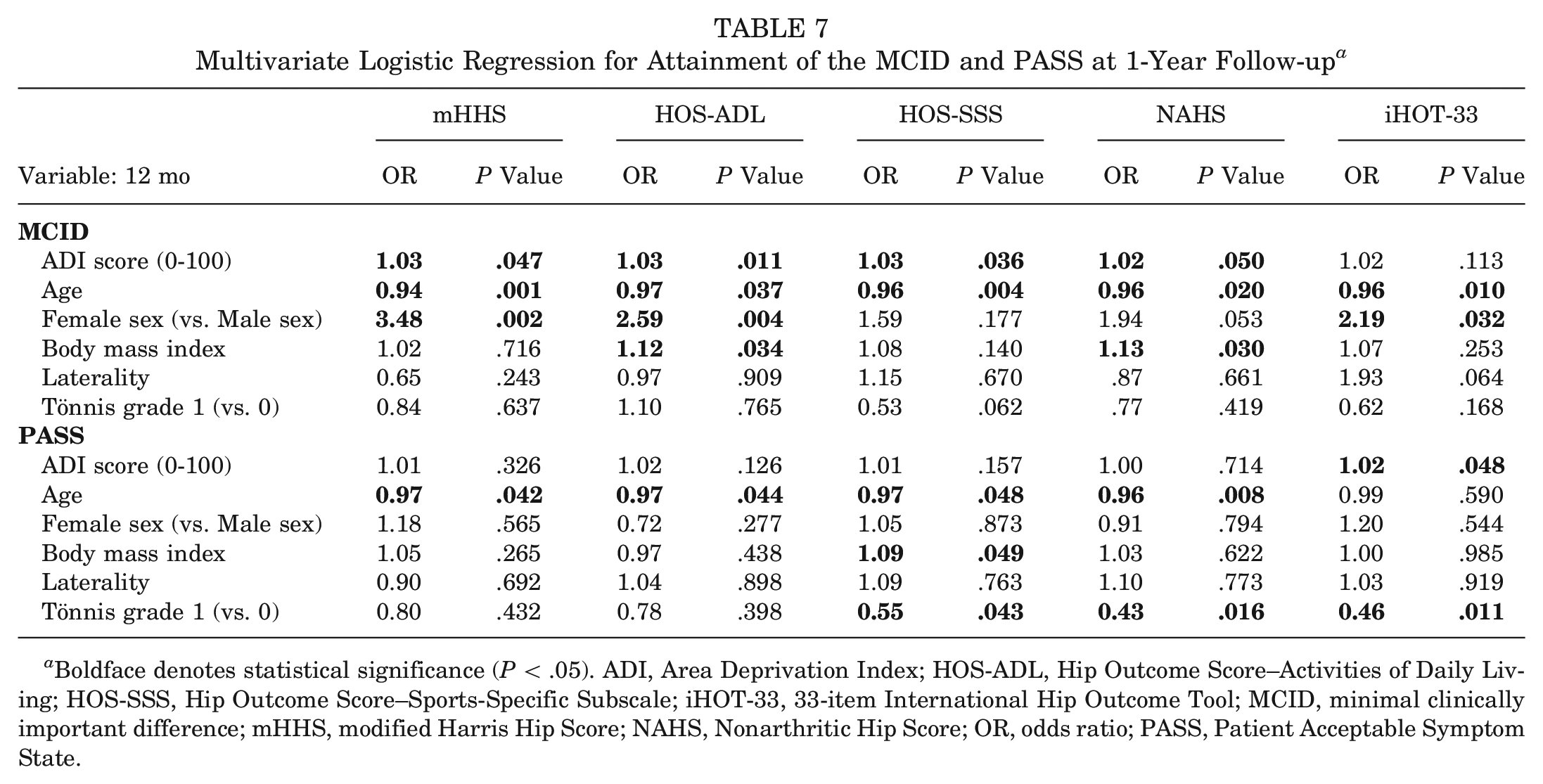
Boldface denotes statistical significance (P < .05). ADI, Area Deprivation Index; HOS-ADL, Hip Outcome Score–Activities of Daily Living; HOS-SSS, Hip Outcome Score–Sports-Specific Subscale; iHOT-33, 33-item International Hip Outcome Tool; MCID, minimal clinically important difference; mHHS, modified Harris Hip Score; NAHS, Nonarthritic Hip Score; OR, odds ratio; PASS, Patient Acceptable Symptom State.
Discussion
In the present study, we found that ADIHigh patients reported significantly worse preoperative baseline scores for all 5 PROMs (mHHS, HOS-ADL, HOS-SSS, NAHS, iHOT-33); however, these differences resolved by 1-year follow-up. Furthermore, patients in the ADILow and ADIHigh cohorts achieved similar rates of the PASS for all 5 PROMs and the MCID for 4 PROMs. When controlling for patient demographics, patients with higher ADI scores had greater odds of achieving the MCID for all PROMs except the iHOT-33 (OR, 1.02; P = .113). Together, these findings disproved our hypothesis that patients from neighborhoods with greater socioeconomic disadvantage experience inferior functional outcomes after surgery and lower rates of achieving clinically meaningful thresholds. Despite the growing volume of orthopaedic health equity research examining how SDOH influence patient outcomes, the present study is the first to explore the relationship between ADI and PROMs after hip arthroscopy.
The utilization of ADI in health disparity research has garnered significant attention in recent years.8,15,16,25,50 As compared with traditional social proxies that examine individual aspects of a patient's life, such as race and insurance, ADI score captures a patient's lived environment through assessing neighborhood-level education, income/employment, housing, and household characteristics. 25 Incorporating these socioeconomic factors into 1 metric may provide a more holistic understanding of a patient's environment and ability to access resources. Epidemiologic investigations, for example, have extensively explored the effect that socioeconomic indices can have on health care delivery, research, and clinical practice, finding that ADI is a predictor for economic risks and multimorbidity.8,15 A 2022 study on Early Head Start, a federally funded program that serves socioeconomically disadvantaged pregnant women and families with young children, found that living in a more disadvantaged neighborhood was associated with economic hardships and pressures, perceptions of decreased neighborhood safety, and lower perceived social status. 15 These day-to-day social stressors and poverty-related experiences are strongly linked to an increased risk for posttraumatic stress disorder, anxiety, and depression. 48 Together, the social and psychological stressors that disadvantaged patients experience may have manifested in ADIHigh patients having significantly worse scores for all 5 baseline PROMs. Having this quantitative assessment of functional outcomes, in addition to previous qualitative population health studies, further adds to the relationship among neighborhood disadvantage, mental health, and physical health.
Upon review of orthopaedic investigations on the shoulder, hip, hand, and knee, there exists conflicting evidence for whether disadvantaged patients experienced worse outcomes. A 2023 study by Shaikh et al 49 assessing arthroscopic rotator cuff repair among patients at 6-month follow-up found that the more disadvantaged patients had significantly lower odds of achieving the MCID for all included domains of the Patient-Reported Outcomes Measurement Information System: physical function (OR, 0.31; P = .001), pain interference (OR, 0.21; P = .001), and depression (OR, 0.28; P = .001). Rahman et al 41 investigated patients at 90-day follow-up in the Michigan Arthroplasty Registry Collaborative Quality Initiative database who underwent total knee arthroplasty. When the cohort was stratified by upper and lower 50th percentiles, patients with higher ADI scores had higher odds of periprosthetic joint infection, all-cause reoperation, aseptic revision, hospital readmission, and visits to the emergency department. Conversely, a 3-month follow-up study assessing patients who underwent carpal tunnel release found no association between ADI or Distressed Communities Index and postoperative score on the QuickDASH (shortened version of the Disabilities of the Arm, Shoulder and Hand) or score improvement. 59 Additionally, a 2021 study by Saks et al 47 on hip arthroscopy patients found no association between Social Deprivation Index and patient-reported outcomes for the mHHS, NAHS, VAS for pain, iHOT, satisfaction, and secondary surgery at baseline and 2-year follow-up. When clinically meaningful thresholds were assessed for the mHHS, NAHS, and VAS for pain, there were no significant differences in the MCID and PASS among all Social Deprivation Index quartiles. In the present investigation of 228 patients undergoing hip arthroscopy, our findings showed that ADIHigh patients had worse baseline PROMs but achieved equivalent outcomes to ADILow patients for the mHHS, HOS-ADL, HOS-SSS, NAHS, iHOT-33, VAS for pain, patient satisfaction, and rates of achieving the MCID or PASS. When adjusting for patient characteristics using multivariate logistic regression, however, disadvantaged patients showed greater odds of achieving clinically meaningful thresholds, with every point increase in ADI score leading to 2%-3% higher odds of the MCID. Together, our findings with previous studies show great variation in the relationship between socioeconomic indices and postoperative outcomes at short-term follow-up.41,47,49,59
This lack of consensus across previous literature, particularly among hip arthroscopy investigations, 47 calls into question if there exists a better method to holistically assess a patient's level of social disadvantage. Wang and Geng 58 performed structural equation modeling and found that higher SES is strongly related to better physical health and healthier lifestyles. Furthermore, lifestyle was a significant mediator between SES and physical health, as well as SES and psychological health, indicating that SES has direct effects on health through lifestyle behaviors. Additionally, one must consider the direct relationship among SES, health care accessibility, and health. Increased poverty, for example, may prevent patients from accessing care, but this lack of health care may further worsen a patient's health, preventing one from returning to work and affording basic needs (eg, food, housing, medication, transportation). A similar cycle can be applied to rural or remote communities that offer limited access to care owing to the rising physician shortages. 29
We believe that the present study's findings may be attributed to disparities in health care accessibility. As we hypothesized, patients experiencing greater neighborhood-level disadvantage had worse baseline PROMs. A potential explanation for this is that disadvantaged patients experience greater SDOH and have less access to medical resources such as physical therapists or primary care physicians, causing their preoperative function to decrease over time. After surgery, however, all patients were provided the same postoperative rehabilitation protocol, had equal access to follow-up appointments, and were prescribed physical therapy as needed. This equitable access to high-quality postoperative care may have led to ADIHigh patients achieving similar 1-year PROMs and higher odds of the MCID as compared with ADILow patients. Together, this supports an important consideration for the potential relationship between health care accessibility and functional outcomes. Given the complex and intertwined relationship among SES, health care accessibility, healthy lifestyle behavior, and overall health, the present study is merely a first step toward understanding the relationship between health inequities and outcomes for patients seeking orthopaedic care. Further development of clinical guidelines and health policy research is necessary to advance care for patients from disadvantaged communities.
Limitations
This study has several limitations that must be considered. First, all findings pertain to those of a single experienced senior surgeon (S.D.M.) who had performed >1000 hip arthroscopy procedures before May 2014. Thus, these outcomes may not be generalizable to other surgeons, especially regarding capsular management, methods of labral reconstruction, and treatment of chondrolabral/chondral injury.10,26,34,36 Second, ADI score is constructed using 5-year data from the American Community Survey, indicating that these data pertain only to a neighborhood's level of SES between 2016 and 2021. 33 This assessment of SES at a single time point may not account for potentially important changes in a community's demographics across the surveillance period. Third, utilizing a patient's zip code to identify and classify level of SES disadvantage may have introduced bias into our findings, especially for patients residing in areas with high heterogeneity or vastly changing demographics. 49 This may result in an ADI score that is not representative of all individuals living in that area. Fourth, the mean ADI scores for the ADILow cohort (n = 113; 5.8 ± 3.0; range, 1-12) and ADIHigh cohort (n = 115; 28.0 ± 14.5; range, 13-97) were both low, signifying a relatively affluent patient population. Fifth, all patients in the final investigation resided in the New England region of the United States and may not be representative of patients from all geographic regions. Sixth, neighborhood characteristics beyond ADI score were not assessed (eg, rurality or medically underserved area/population). This is an important consideration for future investigations as patients from urban areas may do worse than patients from rural areas. Seventh, race/ethnicity and insurance status were not compared between cohorts as there was a general lack of diversity within the study population. Future research investigating the relationship among ADI score, race/ethnicity or insurance status, and PROMs is a crucial next step toward understanding the association between SDOH and orthopaedic surgery outcomes. Finally, as described in previous literature, a potential concern ubiquitous in clinical care is that implicit biases toward disadvantaged patients may have influenced the physician-patient relationship or health care–related decision-making.
Conclusion
Although patients who underwent hip arthroscopy while experiencing a greater neighborhood-level socioeconomic disadvantage exhibited significantly lower preoperative baseline scores, this disparity resolved at 1-year follow-up. In fact, when adjusting for patient characteristics including ADI score, more disadvantaged patients achieved greater odds of achieving the MCID. The present study is merely a first step toward understanding health inequities among patients seeking orthopaedic care. Future research expanding this investigation to multiple institutions around the United States and internationally is warranted to improve the generalizability of the present study's findings. Last, further development of clinical guidelines and health policy research is necessary to advance care for patients from disadvantaged communities.
Footnotes
Submitted January 25, 2024; accepted June 11, 2024.
One or more of the authors has declared the following potential conflict of interest or source of funding: The Conine Family Fund for Joint Preservation provided research support. S.D.M. has received support for education from Kairos Surgical and a gift from Allergan. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.