
Abstract
Background:
Previous studies have attempted to determine prognostic factors for predicting the occurrence of noncontact anterior cruciate ligament (ACL) injuries. However, studies on risk factors for noncontact ACL injuries in Asian female soccer players are limited.
Purpose:
To identify intrinsic risk factors for noncontact ACL injuries among young female Asian soccer players.
Study Design:
Cohort study; Level of evidence, 2.
Methods:
This study evaluated 145 female Japanese soccer players for potential risk factors for noncontact ACL injury during the preseason medical assessment. In total, 25 variables were examined—including anthropometric data, joint range of motion, muscle flexibility, muscle strength, and balance measurements. Participants were monitored throughout a single season for noncontact ACL injuries diagnosed by physicians.
Results:
Noncontact ACL injuries occurred in 13 knees of 13 players (9%). Lower hamstring-to-quadriceps ratio (0.44 ± 0.07 vs 0.50 ± 0.10; P = .04), greater knee extension muscle strength (3.2 ± 0.5 vs 2.7 ± 0.5 N·m/kg; P < .01), and longer playing experience (10.8 ± 3 vs 8.1 ± 4.2 years; P = .02) were significantly associated with new-onset noncontact ACL injuries in young female soccer players. No statistically significant between-group differences were found for any other variables.
Conclusion:
New-onset noncontact ACL injury in young female soccer players was significantly associated with lower hamstring-to-quadriceps ratio, greater knee extension muscle strength, and longer soccer experience. These findings will help develop strategies for preventing noncontact ACL injuries among female soccer players.
Keywords
Anterior cruciate ligament (ACL) injuries are highly likely to occur in sports involving cutting, jumping, pivoting, accelerating, and decelerating motions, such as soccer, basketball, handball, and rugby. ACL injuries, in particular, can result in a prolonged absence from the game and have the longest absence among common soccer injury diagnoses. 7 Interest in women's soccer has grown significantly in recent years, leading to a corresponding increase in female soccer players. A meta-analysis revealed that ACL injury incidence is higher in female athletes than in male athletes in various sports. 19 A significant sex discrepancy exists in the incidence of ACL injury among soccer athletes, with female athletes having an incidence rate that is 2 to 9.6 times greater than that of their male counterparts.4,19,20 Therefore, reducing ACL injuries in female soccer players is of considerable interest.
The mechanisms underlying ACL injuries in soccer are classified as contact and noncontact injuries. Although contact ACL injuries are challenging to prevent, noncontact injuries—including those caused by indirect contact—may be reduced if risk factors are identified. A video analysis of the ACL mechanism and situational pattern of injury in professional female soccer players revealed that approximately 90% of injuries involve no direct contact with the knee, with noncontact injuries being highly prevalent. 14
Several risk factors increase the risk of ACL injuries. Intrinsic risk factors for female athletes include general joint laxity, 29 bony anatomies,23,25,29 decreased fatigue resistance, 1 imbalance of hip abductor strength,12,17,22 and decreased hip external rotational strength. 12 The body of evidence has been compiled from studies on several sports—including soccer, handball, basketball, and volleyball.1,12 Although numerous studies have investigated the risk factors for ACL injury in female athletes, most have been conducted in Europe and North America, and few data are available on Japanese athletes. 22 Data need to be collected from Asia, especially Japan, to investigate the effect of differences in skeletal structure and physique on the risk of sports injuries, including ACL injury. In Japan, few prospective studies have evaluated female soccer players, particularly those that have analyzed multiple factors.
Therefore, we designed a prospective study to determine whether these intrinsic risk factors identified in Western studies are also risk factors for ACL injuries in Japanese female soccer players. Furthermore, this study investigated whether other risk factors previously not considered are associated with ACL injuries, particularly in Japanese female soccer players. This study aimed to identify the intrinsic risk factors for noncontact ACL injuries in young female soccer players. This study hypothesized that some factors—including general joint laxity or imbalance of hip abductor strength—reported in Europe and North America are also relevant in assessing the risk of noncontact ACL injury in young female Japanese soccer players.
Methods
This prospective cohort study assessed female high school and collegiate soccer players during the 2018 to 2020 seasons as part of the Prospective Study of Predictors of Sports Injuries: UTokyo Sports Science Institute Sports Injury Prevention Project.27,28 Data on risk factors were collected during a preseason medical assessment for each of the 3 years, and all participants were monitored for injuries during a single soccer season. Our institution's ethics committee approved the protocol, and written consent was obtained from all participants.
The study participants included 151 young female soccer players from 3 soccer teams (1 high school and 2 collegiate teams) in Japan. No players were injured at the start of the study, and none reported a history of lower limb musculoskeletal injuries over the preceding 3 months. All participants underwent preseason medical checkups and completed a questionnaire that was used to collect data on age, years of soccer experience, injury history, and medication. In addition to anthropometric measurements, preseason data from 5 physical screening tests were used—including joint laxity, joint range of motion (ROM), muscle flexibility, muscle strength, and balance. Each participant's ACL injury history was recorded as soon as informed consent was obtained, and this process continued until the end of the season. Consequently, each player generated only 1 set of measurement data. The latest data were used for players who participated in the medical assessment more than once.
Anthropometric Measurements
Body weight and height were measured at the preseason medical checkup, and body mass index was calculated. Body composition parameters were estimated using InBody 270 (Biospace Co, Ltd), a multifrequency impedance analyzer that records a player's lean soft tissue mass (skeletal muscle mass), body fat mass, and percentage body fat. In addition, the height of each player's navicular tubercle was measured as a flat-foot index.
Joint Laxity and Flexibility
General Joint Laxity Testing
Each player underwent general joint laxity testing using methods published by the University of Tokyo, as described by Watanabe et al. 30 The test was used to evaluate 7 conditions—thumb-to-forearm position, elbow hyperextension of ≥15°, shoulder hyperrotation, hip hyper-external rotation of ≥90° while standing, knee hyperextension of ≥10°, ankle hyperdorsiflexion of ≥45° in knee flexion, and trunk flexion with both palms touching the floor and knees fully extended.26-28 A point value of 0.5 was given each time the designated laxity measurements on both the right and left sides of the tested joints (wrists, elbows, shoulders, knees, and ankles) were surpassed, whereas 1 point was scored for each of the trunk and hip for a maximum possible score of 7 points.
Joint ROM
As described previously, joint ROM was measured for internal hip rotation, ankle dorsiflexion, and knee extension.2,3 The passive hip internal rotation angle in the prone position was used to measure internal hip rotation. The dorsiflexion angle of the weightbearing ankle at knee flexion was used to measure ankle dorsiflexion. The knee hyperextension angle was measured in the standing position with the quadriceps engaged for knee extension.
Muscle Flexibility
Muscle flexibility tests were performed bilaterally on the iliopsoas, quadriceps femoris, hamstring, gastrocnemius, and soleus muscles using previously described methods.10,15,27,28
Iliopsoas. The flexibility of the iliopsoas was measured by determining the hip joint angle formed when the participants passively flexed their opposite hip joint in a supine position.
Quadriceps. The flexibility of the quadriceps was measured by asking the participants to grasp their lower leg proximal to the ankle and pull it toward the buttocks while in a prone position.
Hamstrings. Hamstring muscle flexibility was measured by asking the participants to bring the hip to 90° of flexion in the supine position. A researcher (S.Takei) measured the angle between the vertical line to the floor while holding the participant's heel and the tibia's long axis after maximal extension of the knee joint.
Gastrocnemius. For the gastrocnemius flexibility test, the active dorsiflexion angle of the ankle joint was measured during maximum dorsiflexion in the supine position, with the knee extended.
Soleus. For the soleus flexibility test, the active dorsiflexion angle of the ankle joint was measured by asking the participant to perform maximal dorsiflexion while in the prone position with the knee at 90° of flexion.
Muscle Strength Tests
Isometric Knee Extension and Flexion
The Cybex Humac Norm (Computer Sports Medicine Inc) was used to measure isometric muscle strength during knee flexion and extension. The player pedaled on a stationary exercise bicycle for 5 minutes before the measurement. A randomized order of measurement was used for the test, which involved isometric contraction with knee flexion and extension at 70° (Figure 1). The highest peak torque was recorded. Strength measurements were normalized to body weight. Furthermore, the hamstring-to-quadriceps (H/Q) muscle strength ratio was calculated.

Knee extension and flexion strength testing.
Isometric Hip Abduction
Isometric assessments of hip abductor strength using a handheld dynamometer have excellent intra- and intertester reliability. 21 Hip abductor strength was measured isometrically using a handheld dynamometer (μTAS F-1; Anima Industry Inc). Participants lay next to a wall in the supine position with neutral hips, both knees extended, and arms crossed over their chest. The participants were asked to abduct their legs maximally for 5 seconds, with 1 minute of rest between contractions, and the peak force generated was recorded. The dynamometer was placed on the lateral epicondyle of the femur, and the distance between the lateral epicondyle and hip center was measured. The highest peak torque was recorded. Strength measurements were recorded after normalizing to body weight.
Balance Tests
Double- and single-leg stance balance was assessed using a 1 m Footscan (RSscan International) pressure plate with 8192 resistive sensors, a pixel resolution of 5.08 × 7.62–mm, and a sampling frequency of 250 Hz, as previously described.5,6 First, participants performed a 30-second trial of barefoot double-leg standing balance with arms crossed over the chest and eyes open. Next, participants performed a 30-second trial of single-leg standing balance, similar to the double-leg standing balance test, but alternating between the left and right legs after a 30-second rest interval. The total distance that the center of pressure shifted during the 30-second interval of both tests was considered the balance parameter.13,22
ACL Injury Diagnosis
ACL injuries were directly diagnosed by an orthopaedic team physician (S.Taketomi). The diagnosis, date of injury, injury site, and mechanism of injury (contact or noncontact) were documented for each injury. Direct contact with the lower extremity was considered a contact mechanism, whereas indirect contact (contact not involving the injured knee/lower extremity) and no contact were considered noncontact mechanisms. Physical examination and magnetic resonance imaging were used to diagnose injuries. Only injuries sustained during soccer practice or matches were considered.
Statistical Analysis
All statistical analyses were performed using BellCurve for Excel (SSRI Co Ltd). Parameters, except for the lower limbs, were compared between injured and uninjured players. The lower limb parameters were compared between the injured players’ injured limbs and the means of uninjured players’ limbs. In addition, they were compared between the dominant leg of the injured and uninjured players. Unpaired 2-tailed Student t test and the Mann-Whitney U test were used to assess continuous and nonparametric variables. P < .05 was considered statistically significant. A post hoc power analysis of the significant risk factors—including years of soccer experience (effect size, 0.65), knee extension muscle strength (effect size, 0.99), and H/Q ratio (effect size, 0.56)—yielded a power of 1 for all and was calculated at α = .05.
Results
ACL injuries occurred in 13 knees of 13 players (incidence, 9%). All ACL injuries were noncontact injuries. Three ACL injuries occurred during matches, and the remaining 10 occurred during training. The timing of injury was preseason for 3 players, early season for 5 players, and late season for 5 players. Six players had a history of ACL injury and were excluded from the analysis. No players who underwent the medical assessment were lost to follow-up during the injury registration period. Hence, 145 players (13 injured and 132 uninjured players) were assessed (Figure 2). Of the 13 injured players, 7 sustained ACL injuries in the dominant leg and 6 in the nondominant leg. The positions of players are described in Table 2. Injured players were significantly more likely to have more years of soccer experience (10.8 [95% CI, 8.6-12.5] vs 8.1 [95% CI, 7.4-8.9] years; P = .02; Cohen d = 0.65 (Table 1). No significant between-group differences were found for any other variables (Tables 1 and 3). The knee extension muscle strength of the injured limb in injured players was significantly greater than the mean knee extension muscle strength of both limbs in uninjured players (3.2 N·m/kg [95% CI, 2.8-3.5 N·m/kg] vs 2.7 N·m/kg [95% CI, 2.6-2.8 N·m/kg]; P < .001; Cohen d = 0.84). The H/Q ratio of the injured limb of injured players was lower than that of the mean H/Q ratio of both limbs of the uninjured players (0.44 [95% CI, 0.39-0.48] vs 0.50 [95% CI, 0.48-0.51]; P = .04; Cohen d = 0.60) (Table 4). Participants with greater knee extension muscle strength in the dominant leg (3.2 N·m/kg [95% CI, 2.9-3.5 N·m/kg] vs 2.8 N·m/kg [95% CI, 2.7-2.9 N·m/kg]; P = .03; Cohen d = 0.65) were more likely to sustain noncontact ACL injuries (Table 5).
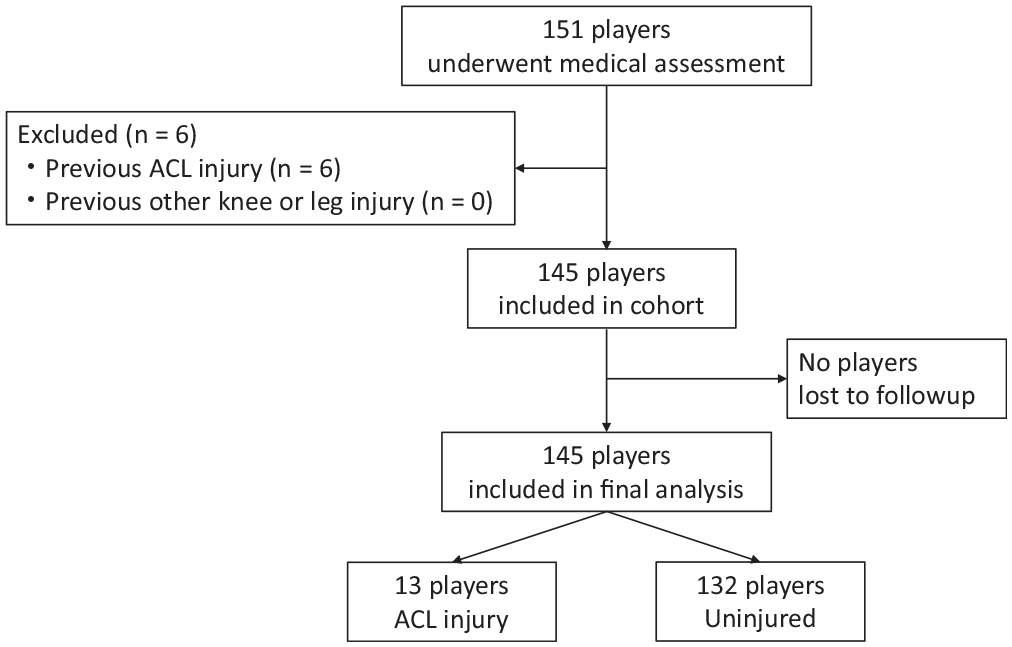
Flow chart for patient inclusion and exclusion. ACL, anterior cruciate ligament.
Characteristics of Players Evaluated a
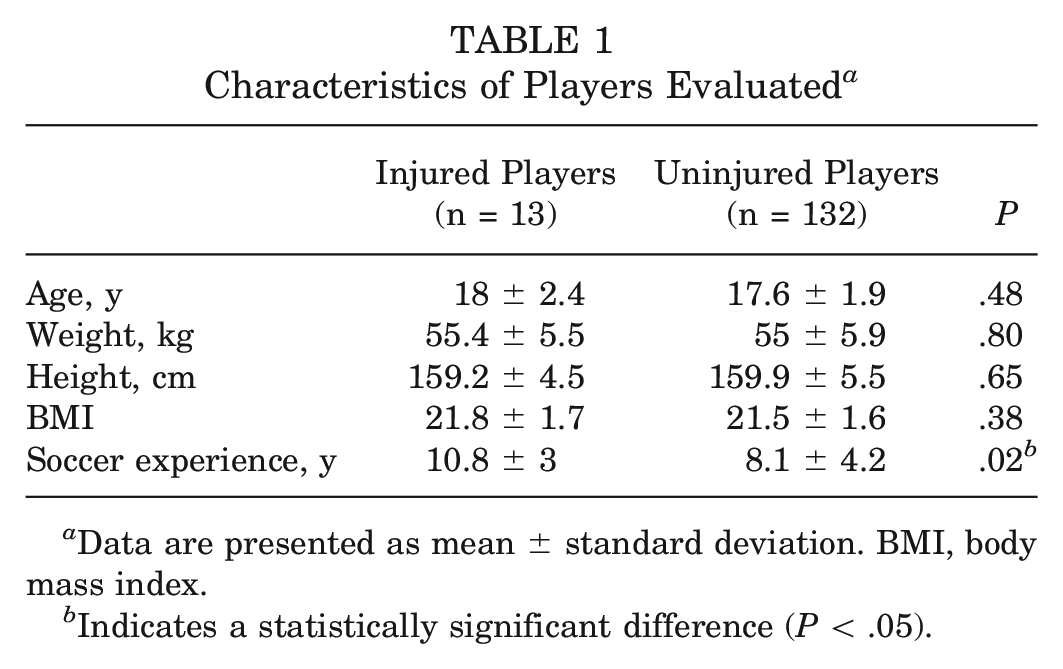
Data are presented as mean ± standard deviation. BMI, body mass index.
Indicates a statistically significant difference (P < .05).
Position of Players a
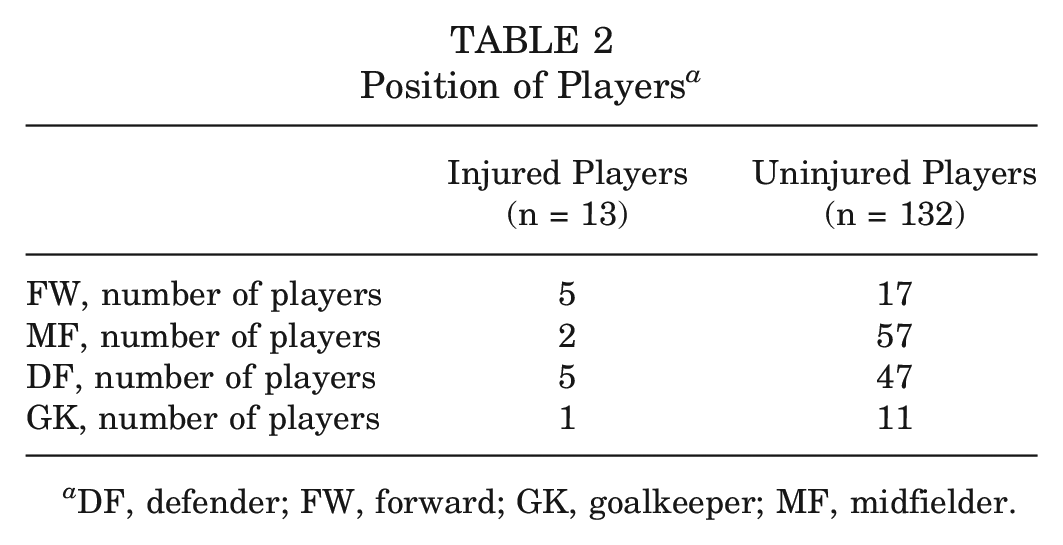
DF, defender; FW, forward; GK, goalkeeper; MF, midfielder.
Anthropometric, Joint Laxity, and Double-Leg Balance Measurements for the Injured and Uninjured Groups a
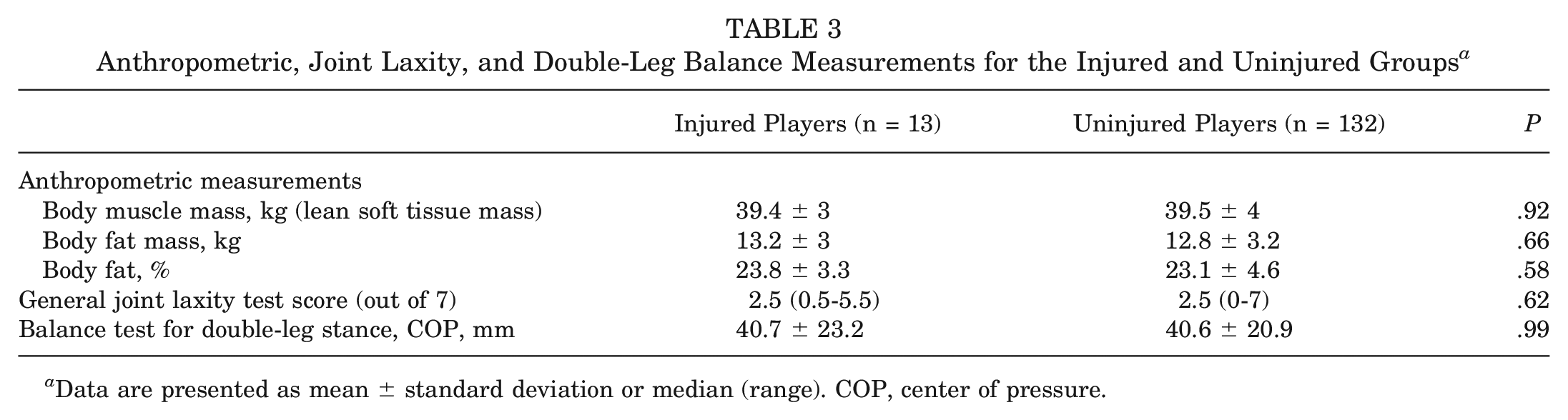
Data are presented as mean ± standard deviation or median (range). COP, center of pressure.
Lower Limb Parameters of Injured and Uninjured Limbs of Both Injured and Uninjured Groups a
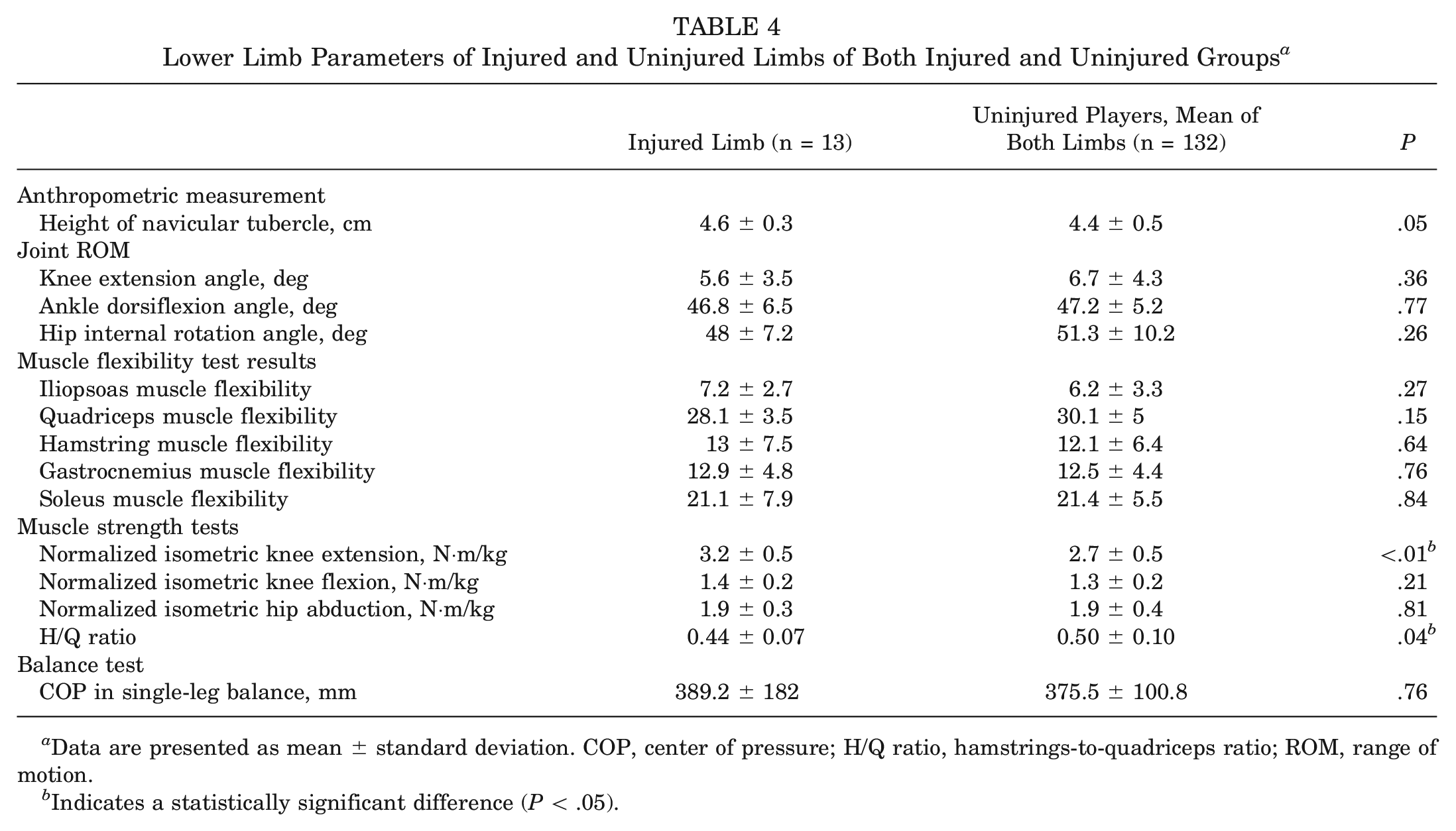
Data are presented as mean ± standard deviation. COP, center of pressure; H/Q ratio, hamstrings-to-quadriceps ratio; ROM, range of motion.
Indicates a statistically significant difference (P < .05).
Lower Limb Parameters of the Dominant Leg of Injured and Uninjured Players a

Data are presented as mean ± standard deviation. COP, center of pressure; H/Q ratio, hamstrings-to-quadriceps ratio; ROM, range of motion.
Indicates a statistically significant difference (P < .05).
Discussion
This study demonstrated that a lower H/Q ratio, greater knee extension muscle strength, and longer soccer experience were significantly associated with new-onset noncontact ACL injury in young Japanese female soccer players. This is the first prospective cohort study to identify a lower H/Q ratio as an intrinsic risk factor for noncontact ACL injury in female soccer players. Contrary to our hypothesis, such risk factors as general joint laxity or imbalance of hip abductor strength for noncontact ACL injuries identified in Western female athletes were not associated with new-onset ACL injuries in this study.
Several studies have investigated the association between ACL injury risk and the H/Q ratio. Three studies16,22,24 focused on female athletes, 1 on male 26 athletes, 1 on both male and female athletes, 8 and 1 on military cadets. 29 However, only 1 study reported an association between ACL injury and the H/Q ratio. 26 A recent systematic review concluded that the H/Q ratio is limited in predicting ACL injuries. 11 However, Myer et al 16 studied female soccer and basketball players and found that the H/Q ratio of female athletes with noncontact ACL injuries tended to be lower than that of uninjured female athletes, although the difference was insignificant. Only 1 study on male American football players reported a lower H/Q ratio as a risk factor for noncontact ACL injury. 26 Conversely, no study has identified a low H/Q ratio as a risk factor for ACL injury in female athletes. The present study is perhaps the first to report a low H/Q ratio as a significant risk factor for ACL injury in female athletes. The aforementioned article on male American football players and our present study were conducted in Japan 26 ; therefore, the H/Q ratio may be an essential risk factor in Asian or Japanese female athletes. The differences between the results of previous studies from Europe and North America and this study may be due to differences in spinal-pelvic alignment by race and ethnicity. Asian people, including Japanese, have a smaller angle of lumbar lordosis and a more posteriorly tilted pelvis compared with other racial groups. 31 Thus, the hamstring muscle may be looser and less powerful in Asian people, and conversely, the quadriceps muscle may be more powerful, resulting in a lower H/Q ratio. This difference in pelvic tilt between Asian people and those of other races and ethnicities may have caused the H/Q ratio to emerge as a risk factor for ACL injury in this study. Specifically, the results of the present study showed that high quadriceps strength and low H/Q ratio were risk factors for noncontact ACL injuries in female soccer players. Because a longer playing experience was also a risk factor, athletes at higher levels of competition with strong quadriceps but insufficient matching hamstring strength may be at particular risk. In soccer, noncontact ACL injuries commonly occur because of various motions, such as when a player does not decelerate when defending. 14 In this example, an imbalance in strength between the quadriceps and hamstring muscles may be the cause; in other words, weaker hamstring muscles relative to the quadriceps muscles, which contract strongly during deceleration, may lead to a failure of knee control. Combined with the finding that female athletes appeared to rely more on their quadriceps muscles in response to anterior tibial translation, 9 the results of this study indicate that ACL injuries may be prevented through adequate hamstring strength training in female soccer players, particularly those with high quadriceps muscle strength.
Greater knee extension strength was a risk factor in the comparison between the injured limb of injured players and the mean of both lower limbs of uninjured players, as well as in the comparison between the dominant leg of injured players and the dominant leg of uninjured players. The results of the comparisons indicate that these characteristics may be specific to individual players who sustain ACL injuries. However, a lower H/Q ratio was a risk factor only in the comparison between the injured limb of the injured players and the mean of both lower limbs of the uninjured players, indicating that a lower H/Q ratio may be characteristic of the injured limb rather than that of the player.
The present study also showed a significant association between a longer soccer experience and new-onset noncontact ACL injury in female soccer players. A longer athletic career would mean more opportunities to compete at a higher level of competition and participate in higher-intensity training and, therefore, more opportunities to encounter situations that might cause ACL injury. Few reports have examined the association between athletic history and ACL injury risk. Beynnon et al 4 assessed a large cohort of high school and collegiate athletes who engaged in multiple sports and found that collegiate athletes had a higher risk of ACL injury. The study found that the incidence of noncontact ACL injury increases with the level of competition. In contrast, a study on male American football players reported a higher risk of ACL injury during preseason training for athletes with ≤3 years of athletic experience than for athletes with ≥4 years of experience. 18 Because of these contradictory reports, further studies must confirm a longer athletic experience as a risk factor for noncontact ACL injury.
General joint laxity, a known risk factor for ACL injury in female athletes as identified in a study conducted in the United States, 29 was not associated with new-onset noncontact ACL injury in the present study. One possible reason for the discrepancy between the results of this study and those of previous reports is that the risk of ACL injury differs somewhat between Japanese and Western athletes. Hip abductor strength was not associated with new noncontact ACL injury in this study. Previous studies conducted on female basketball and handball players in Japan have reported high hip abductor strength as a risk factor for ACL injury,17,22 whereas a study conducted on Iranian athletes, who are similar in physique to European people in Asia, contradicts this, indicating that low hip abductor strength is a risk factor for ACL injury. 12 However, the association between hip abductor strength and ACL injury remains unclear. The absolute number of players with noncontact ACL injuries was small (13 players); thus, the study results cannot conclude that general joint laxity and hip abductor strength are not associated with noncontact ACL injuries in female soccer players. Further extensive prospective cohort studies, particularly on Japanese and Asian players, are required for confirmation.
Achieving balance between quadriceps and hamstrings is crucial to prevent ACL injuries in female soccer players. Thus, the quadriceps and hamstrings should be concurrently targeted during training.
Limitations
First, the study results are not generalizable to all soccer players because of the small number of participants. Furthermore, our study cohort was a convenience sample of 3 amateur teams of relatively young age playing at a high level of competition. However, given the scarcity of prospective cohort studies on Japanese female soccer players, this study provides valuable preliminary data. Second, multivariate analysis was not performed in this study; the 3 risk factors were identified from univariate analysis. Also, >30 incidents of noncontact ACL injuries were needed to perform a multivariate analysis of these 3 factors. However, current data on ACL injury incidents and the statistical power were insufficient to perform this analysis. Third, this study only assessed isometric muscle strength in knee extension and flexion. Although isokinetic testing would have added additional information and allowed comparison with other studies that utilized isokinetic testing, the time and personnel constraints of the medical checkups made such evaluations difficult. Fourth, uninjured players included players with injuries other than ACL injuries, which may have introduced bias. Fifth, data on the exposure and ground surface during games and training sessions were unavailable. Data on the period of rest due to injury were also unavailable. Finally, this study did not include data on the number of training sessions and matches per player. This last item would have been a valuable bias because those who practice and play more often have a higher risk of injury.
Conclusion
Lower H/Q ratio, greater knee extension muscle strength, and longer soccer experience were significantly associated with new-onset noncontact ACL injury in young female soccer players in this study. These findings will help develop strategies for preventing noncontact ACL injuries among female soccer players.
Authors
Shuji Taketomi, MD, PhD (Department of Orthopaedic Surgery, Faculty of Medicine, The University of Tokyo, Tokyo, Japan); Kohei Kawaguchi, MD (Department of Orthopaedic Surgery Faculty of Medicine, The University of Tokyo, Tokyo, Japan; the University of Tokyo Sports Science Initiative [UTSSI], Tokyo, Japan); Yuri Mizutani, MD, (UTSSI, Tokyo, Japan); Seira Takei, MD, PhD (UTSSI, Tokyo, Japan); Ryota Yamagami, MD (Department of Orthopaedic Surgery, Faculty of Medicine, The University of Tokyo, Tokyo, Japan); Kenichi Kono, MD, PhD (Department of Orthopaedic Surgery, Faculty of Medicine, The University of Tokyo, Tokyo, Japan); Ryo Murakami, MD (Department of Orthopaedic Surgery, Faculty of Medicine, The University of Tokyo, Tokyo, Japan); Takahiro Arakawa, MD (Department of Orthopaedic Surgery, Faculty of Medicine, The University of Tokyo, Tokyo, Japan); Tomofumi Kage, MD, PhD (Department of Orthopaedic Surgery, Faculty of Medicine, The University of Tokyo, Tokyo, Japan); Takashi Kobayashi, MD (Department of Orthopaedic Surgery, Faculty of Medicine, The University of Tokyo, Tokyo, Japan); Yuri Furukawa, MD (Department of Orthopaedic Surgery, Faculty of Medicine, The University of Tokyo, Tokyo, Japan); Yusuke Arino, MD (Department of Orthopaedic Surgery, Faculty of Medicine, The University of Tokyo, Toyo, Japan); Sayaka Fujiwara, MD, PhD (UTSSI, Tokyo, Japan; Department of Rehabilitation Medicine, The University of Tokyo, Tokyo, Japan); Sakae Tanaka, MD, PhD (Department of Orthopaedic Surgery, Faculty of Medicine, The University of Tokyo, Tokyo, Japan); and Toru Ogata, MD, PhD (UTSSI, Tokyo, Japan; Department of Rehabilitation Medicine, The University of Tokyo, Tokyo, Japan).
Footnotes
Submitted March 22, 2024; accepted July 22, 2024.
One or more of the authors has declared the following potential conflict of interest or source of funding: This study was funded by scholarship donations from the East Japan Railway Company and Shimamura-Syoukai and grants from the Nakatomi Foundation, Japan Sports Medicine Foundation, Japan Sport Council, Japanese Orthopaedic Society for Sports Medicine, Watanabe Memorial Foundation for the Advancement of New Technology, Japan Keirin Autorace Foundation, Japan Society for the Promotion of Science (KAKENHI 20K11358), Japan Orthopaedics Traumatology Foundation, and Japanese Orthopaedic Society of Knee, Arthroscopy and Sports Medicine. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.