
Abstract
Background:
The effectiveness and safety of matrix-associated autologous chondrocyte implantation with an autologous periosteal flap (pMACI) remain unclear. The Japanese Ministry of Health, Labor, and Welfare requires postmarketing surveillance of all patients undergoing pMACI using the tissue-engineered product JACC.
Purpose:
To evaluate the effectiveness and safety of pMACI for large articular cartilage defects (≥4 cm2) in the knee joint using real-world data analysis.
Study Design:
Case series; Level of evidence, 4.
Methods:
Data were collected from patients who underwent pMACI between 2012 and 2019, with 2 years of follow-up. The primary outcomes were the Lysholm knee score and Knee injury and Osteoarthritis Outcome Score (KOOS) at 6, 12, and 24 months. Adverse events were assessed by physical examination, magnetic resonance imaging, and/or arthroscopy.
Results:
Overall, 232 knees in 225 patients who presented with trauma (198 knees) or osteochondritis dissecans (34 knees) in the medial (132 knees) and lateral (44 knees) femoral condyle, patella (25 knees), trochlea (86 knees), and tibial plateau (4 knees) were included. The mean age of the patients was 40.9 ± 15.0 years, with mean cartilage defects of 5.6 ± 2.4 cm2 in size. Concomitant surgeries, such as osteotomy (50 knees), ligament reconstruction (27 knees), meniscal procedures (28 knees), osteochondral autograft transplantation (24 knees), and microfracture (14 knees), were performed in 113 (48.7%) knees. The minimal clinically important difference in the Lysholm knee score and KOOS Symptoms subscale was achieved in 79.7% and 63.5% of patients, respectively, and the Patient Acceptable Symptom State was achieved in 90.1% and 73.7%, respectively. Substantial clinical benefit was achieved in the KOOS Sports/Recreation and Quality of Life subscales at 39.6% and 37.8%, respectively. Knees that underwent concomitant microfracture had significantly worse KOOS values than the remainder of the cohort. Complications, including effusion (16.8%), graft delamination (14.7%), knee contracture (9.1%), graft hypertrophy (8.2%), and ossification (3.4%), were observed in 86 (37.1%) knees. Osteochondritis dissecans was significantly associated with graft hypertrophy and ossification, whereas concomitant surgery was significantly associated with delamination and contracture. Treatment failure required additional cartilage procedures in 11 (4.7%) knees.
Conclusion:
Treatment of large cartilage defects (≥4 cm2) with pMACI resulted in improved outcome scores in approximately 75% of patients. However, complications occurred in one-third of patients, and 4.7% required reoperation.
The lack of vessel and nerve supplies negatively affects the repair of large articular cartilage defects. 15 Brittberg et al 6 developed autologous cultured chondrocyte implantation (ACI), treating their first patients in 1987, and reported long-term outcomes in 1994. The first generation of ACI (also known as periosteal ACI [pACI]) involved injecting chondrocytes expanded by monolayer cultivation into the defect and covering it with an autologous periosteal flap from the tibia. 6 Multiple studies have shown the efficacy and safety of pACI at mid- and long-term follow-up. # However, concerns about maintaining the chondrocyte phenotype in cultivation, risk of cell leakage from the defect, and uneven cell distribution during implantation remain to be resolved.17,34 These issues might be associated with the reported evidence in some systematic reviews for the absence of difference in the long-term clinical outcomes between pACI and microfracture (MF).12,20,37
A matrix-associated ACI (MACI) was envisaged to resolve this discrepancy. Bayesian network meta-analysis revealed that MACI demonstrated a better effect among ACI procedures. 24 The benefits of this procedure include maintenance of the chondrocyte phenotype during cultivation, a low risk of cell leakage, and cell distribution during implantation.25,26 MACI covered with autologous periosteum (pMACI) was developed by Ochi et al33,34 in 2001. Chondrocytes were embedded in atelocollagen gel, cultured for 4 weeks, transplanted, and covered with autologous periosteum. Basic science has suggested that this method can effectively alleviate previous concerns.17,33,46 The resulting product, JACC (Japan Tissue Engineering), was created according to the method of Ochi et al33,34 and underwent clinical trials that produced good clinical and magnetic resonance imaging (MRI) outcomes up to 6 years after implantation, with minimal adverse events (AEs).1,44,45 In 2013, JACC was approved by the Japanese Ministry of Health, Labor, and Welfare (MHLW) for use in pMACI for treating traumatic cartilage defects or osteochondritis dissecans (OCD) in the knee joint (excluding osteoarthritis), in which the affected area was ≥4 cm2. The treatment is covered for use under the National Health Insurance scheme. Although the autologous periosteum was replaced with a collagen membrane as a cover for ACI or MACI in other countries, the use of the collagen membrane was not allowed in Japan until 2019.
Since the introduction of JACC, the MHLW has required postmarketing surveillance for all patients treated with pMACI prepared with the JACC culture. The Pharmaceuticals and Medical Device Agency manages postmarketing surveillance protocols. The agency gathers data from all hospitals performing pMACI in Japan, providing an extensive resource of real-world data in routine clinical practice for generating real-world evidence. Thus, this study aimed to use these data to clarify the risks and benefits of pMACI in treating large cartilage defects.
Methods
Study Design
This retrospective multicenter case series analysis was based on real-world data. The study was performed under the control of the Japanese MHLW, based on ordinance number 38 of March 23, 2005. The surveillance results were reexamined and submitted to the Japanese regulatory authority, the Pharmaceuticals and Medical Device Agency. An independent analysis was conducted using data from the reexamination. The authors, except for KS, belong to a third-party committee that analyzed the data. Individual institutions provided ethics approval for this study. All patients provided informed consent to their health institutions for the collection and use of their surveillance data.
Participants
Patients eligible for this analysis underwent pMACI between July 27, 2012, and July 26, 2019, and had follow-up data for 2 years. This study included patients with traumatic cartilage defects or OCD of the knee joint where the defect area was ≥4 cm2. Patients with osteoarthritis, a history of autoimmune disease, a history of hypersensitivity to antibiotics or animal-derived ingredients, or a positive preoperative allergy test for fetal bovine serum and atelocollagen used in the manufacturing process of JACC were excluded.
Graft Preparation and Implantation
The grafts were prepared with JACC according to the method of Ochi et al33,34 with some modifications. Approximately 400 mg of cartilage tissue was harvested arthroscopically from the nonweightbearing areas of the knee joint and sent to Japan Tissue Engineering. Cartilage tissue was subjected to enzymatic digestion, and chondrocytes were isolated and embedded in an atelocollagen gel. They were cultured in a 3-dimensional manner for 4 weeks. Before shipping, the sterility, absence of mycoplasma and endotoxins, cell counts, cell viability, and cartilage matrix content were measured.
Implantation was performed on receipt of the graft at the institution. Medial or lateral parapatellar arthrotomy was performed under tourniquet control. The chondral lesion was debrided from the intact surrounding cartilage until the subchondral bone was exposed44,45 (Figure 1, A and B). The graft was implanted into the defect, and the autologous periosteal flap from the proximal medial tibia was sutured to this position (Figure 1, C and D). The joint capsule, retinaculum, and skin were sutured separately.
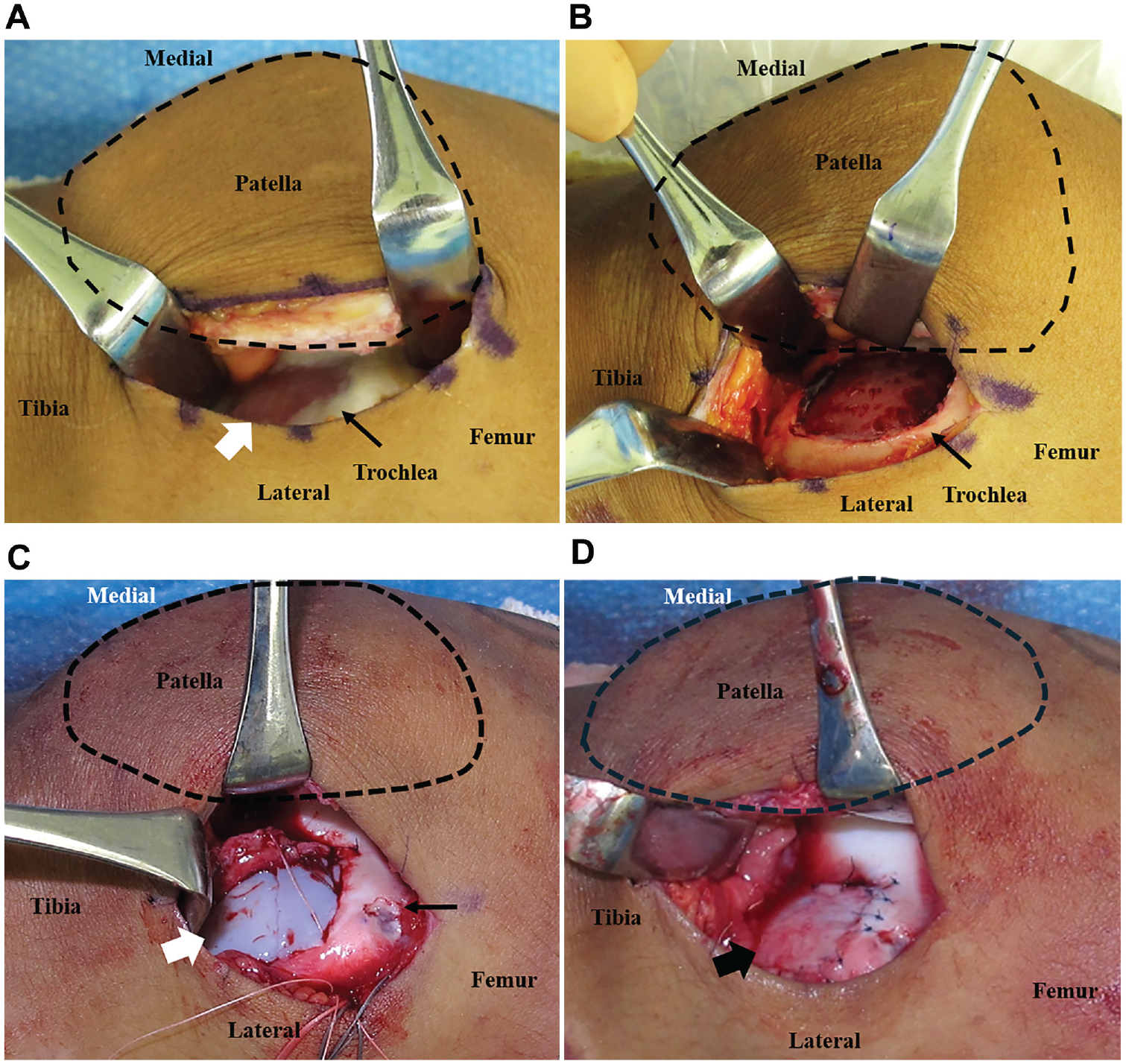
Implantation of JACC with an autologous periosteal flap in a 14-year-old boy with osteochondritis dissecans of the left trochlea. (A) The chondral lesion on the left trochlea (7.5 cm2, white arrow) was exposed by medial retraction of the patella (black dotted circle) via a lateral parapatellar approach. (B) The chondral lesion was debrided from intact surrounding cartilage (12 cm2). (C) The JACC (white arrow) was implanted into the defect. The black arrow indicates the cartilage-harvesting site of the lateral femoral condyle. Sutures were used to pull out the autologous periosteum. (D) An autologous periosteum (black arrow) was sutured to the rim surrounding the normal cartilage.
Concomitant Surgeries
Osteochondral autograft transplantation (OAT) or MF was performed for smaller cartilage defects that were not treated by pMACI. Additionally, ligament reconstruction was performed to treat ligament tears, meniscal repair or partial meniscectomy was performed to treat meniscal tears, and osteotomies were performed for tibiofemoral malalignment with varus or valgus deformity >5° or patellofemoral malalignment with a tibial tuberosity–trochlear groove distance >15 to 20 mm.
Postoperative Rehabilitation
As previously reported,1,33,34,44,45 a lightweight brace was used to immobilize the knee for 2 weeks, followed by continuous passive movement. For patellofemoral lesions, motion was restricted for up to 4 weeks. Partial weightbearing was introduced 3 weeks postoperatively and gradually increased to full muscle training by 8 weeks, according to the individual institution's protocol, defect site and size, and concomitant procedures.
Assessment of Effectiveness and Safety
The effectiveness of pMACI was evaluated with the Lysholm knee score (LKS) and Knee injury and Osteoarthritis Outcome Score (KOOS) 41 before surgery and 6, 12, and 24 months after pMACI. For safety evaluation, patients underwent MRI at the same time periods to assess the graft integrity using a 1.5-T or 3.0-T scanner with fast spin-echo proton density–weighted sequences, with or without fat suppression, and T2-weighted imaging in the coronal and sagittal planes. 8
Effectiveness was demonstrated by the number and ratio of cases that achieved the minimal clinically important difference (MCID)16,18,22 between the pre- and postoperative differences using the cutoff points of LKS and KOOS by Ogura et al, 35 the Patient Acceptable Symptom State (PASS) using the cutoff points by Chahal et al, 7 and the substantial clinical benefit (SCB) 10 using the cutoff points by Ogura et al. 35 The chronological effects of diseases and concomitant surgeries on LKS and KOOS were also evaluated.
Safety was assessed by recording the number of AEs, which were defined as undesired, unintended signs (eg, abnormal laboratory test values); MRI and/or arthroscopic evidence of graft delamination; graft hypertrophy; effusion; ossification detected on radiographs; knee contracture (≥5°); and symptoms or illness, with or without a causal relationship with the product. Graft delamination included delamination of the periosteal membrane, underlying graft tissue, or both. The effects of diseases and concomitant surgeries on the incidence of AEs were also evaluated. Treatment failure was defined as a requirement for reoperation due to graft delamination or failure of graft filling after pMACI. 28
Statistical Analysis
SAS Version 9.4 (SAS Institute Inc) was used for all statistical analyses. Demographic data are presented as means and standard deviations. A power analysis was performed using a Monte Carlo simulation to evaluate the validity of the sample size. A mixed-effects model for repeated measures (MMRM) was used to compare the LKS and KOOS values at each time point in the overall cohort and by disease and concomitant surgery. The models included fixed effects for disease or concomitant surgeries, time points, and disease or concomitant surgeries by time point interactions. Missing data were not imputed in the MMRM analysis. In another analysis, the last observation carried forward method was used to impute missing values for LKS and the KOOS Symptoms, Pain, Activities of Daily Living, Sports/Recreation, and Quality of Life (QOL) subscales. The Student or Welch t test was used for continuous data, and the Fisher exact test was used for categorical data to evaluate differences in patient characteristics between the group assessing the efficacy of pMACI and the group without scores. The Fisher exact test was used to evaluate differences in the AE ratios between diseases or concomitant surgeries, and the group assessing the efficacy of pMACI and the group without scores.
All tests were 2-sided, and no adjustments were made to the multiple comparisons. Statistical significance was set at P < .05.
Results
Study Population
This study initially included 344 knees in 335 patients (mean age, 40.6 years; range, 11-74 years; 187 men and 148 women) from 98 institutions. However, knees without LKS preoperatively, 6 months postoperatively, or both (47, 49, and 16 knees, respectively) were excluded, and 232 knees in 225 patients (mean age, 40.9 years; range, 12-74 years; 126 men and 106 women) were included in the final analysis (Figure 2). The power analysis confirmed the validity of our sample size for the main MMRM analysis for LKS and KOOS 2 years after implantation (power, 100%). The Student t test, Welch t test, and Fisher exact test showed no significant differences in patient characteristics between the group assessing the efficacy of pMACI and the group without scores, except for patellofemoral malalignment (3.0% vs 10.7%; P = .0052).

Study flowchart. “Meniscal procedure” indicates meniscal suture and/or resection. “Multiple surgeries” includes osteotomy and meniscal procedure (8 knees), ligament reconstruction and meniscal procedure (6 knees), osteotomy and osteochondral autograft transplantation (OAT) (4 knees), meniscal procedure and OAT (3 knees), meniscal procedure and microfracture (MF) (2 knees), osteotomy and ligament reconstruction (1 knee), osteotomy and OAT and MF (1 knee), ligament reconstruction and OAT (1 knee), and ligament reconstruction and meniscal procedure and MF (1 knee). OCD, osteochondritis dissecans; pMACI, matrix-associated autologous chondrocyte implantation with an autologous periosteum.
Osteochondral defects were caused by traumatic injury (trauma) in 198 knees and OCD in 34 knees, and the mean lesion sizes before and after debridement were 5.6 ± 2.4 cm2 and 5.9 ± 2.5 cm2, respectively (Table 1). Concomitant surgeries, such as osteotomy, ligament reconstruction, meniscal procedure, OAT, and MF, were performed in 113 (48.7%) knees. Table 2 presents the timing of concomitant surgeries. As shown in Figure 2, patients were divided into 7 groups according to concomitant surgeries for evaluation.
Summary of Patient Characteristics a
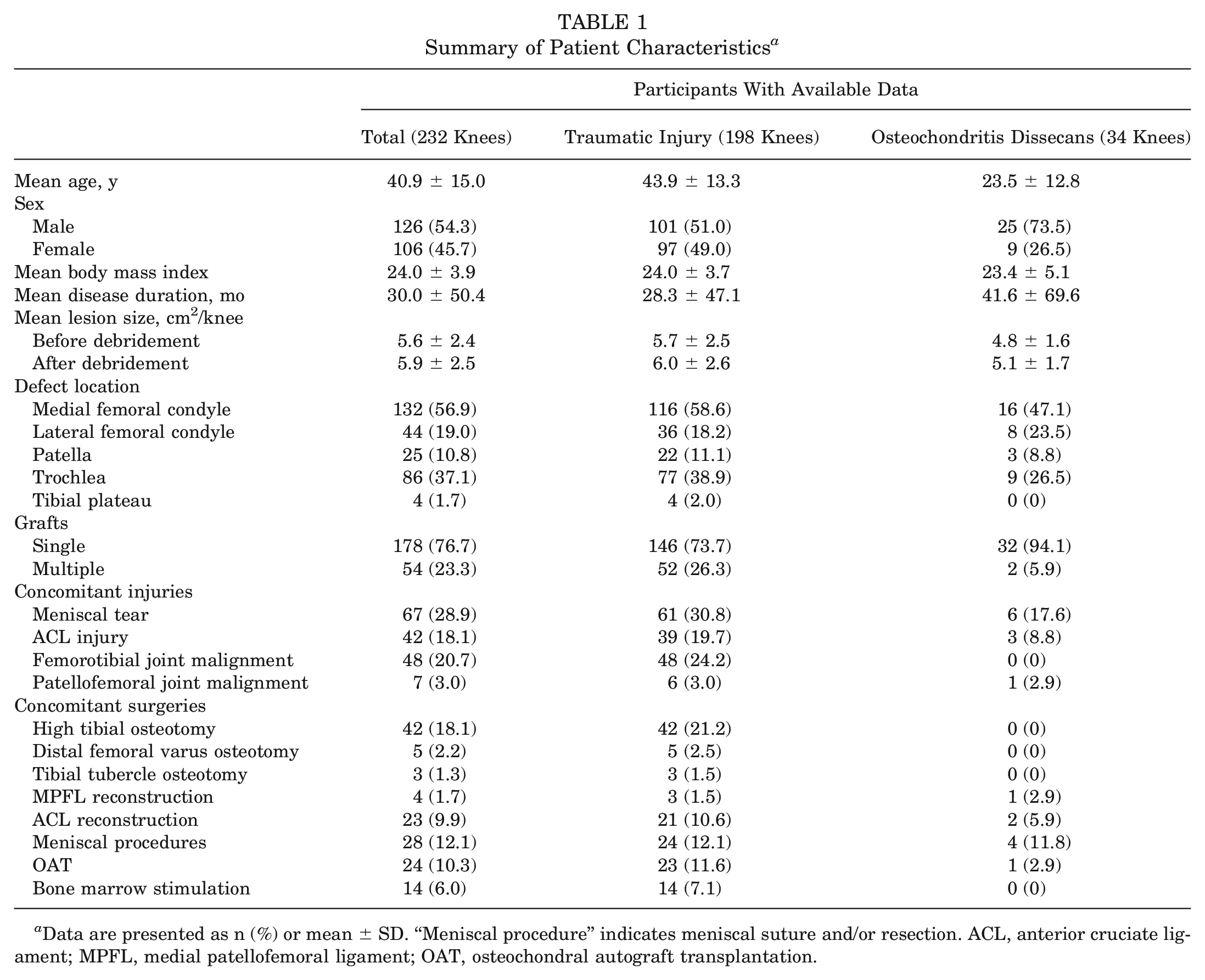
Data are presented as n (%) or mean ± SD. “Meniscal procedure” indicates meniscal suture and/or resection. ACL, anterior cruciate ligament; MPFL, medial patellofemoral ligament; OAT, osteochondral autograft transplantation.
Timing of Concomitant Surgeries a

Data are presented as number of knees. “Meniscal procedure” indicates meniscal suture and/or resection. MF, microfracture; OAT, osteochondral autograft transplantation; pMACI, matrix-associated autologous chondrocyte implantation with an autologous periosteum.
Evaluation of Clinical Scores
Changes in the LKS and KOOS scores in the total, trauma, and OCD groups are shown in Figure 3. The mean LKS values in the total, trauma, and OCD groups significantly improved from 59.0 ± 19.3, 57.2 ± 19.2, and 69.3 ± 16.4 points preoperatively to 87.5 ± 12.2, 86.2 ± 12.5, and 94.8 ± 7.0 points, respectively, 24 months postoperatively (P < .0001). The mean overall KOOS values in the total, trauma, and OCD groups significantly improved from 54.2 ± 18.9, 53.4 ± 19.1, and 60.4 ± 15.5 points preoperatively to 75.2 ± 17.6, 73.4 ± 17.7, and 87.1 ± 12.1 points, respectively, 24 months postoperatively (P < .0001).
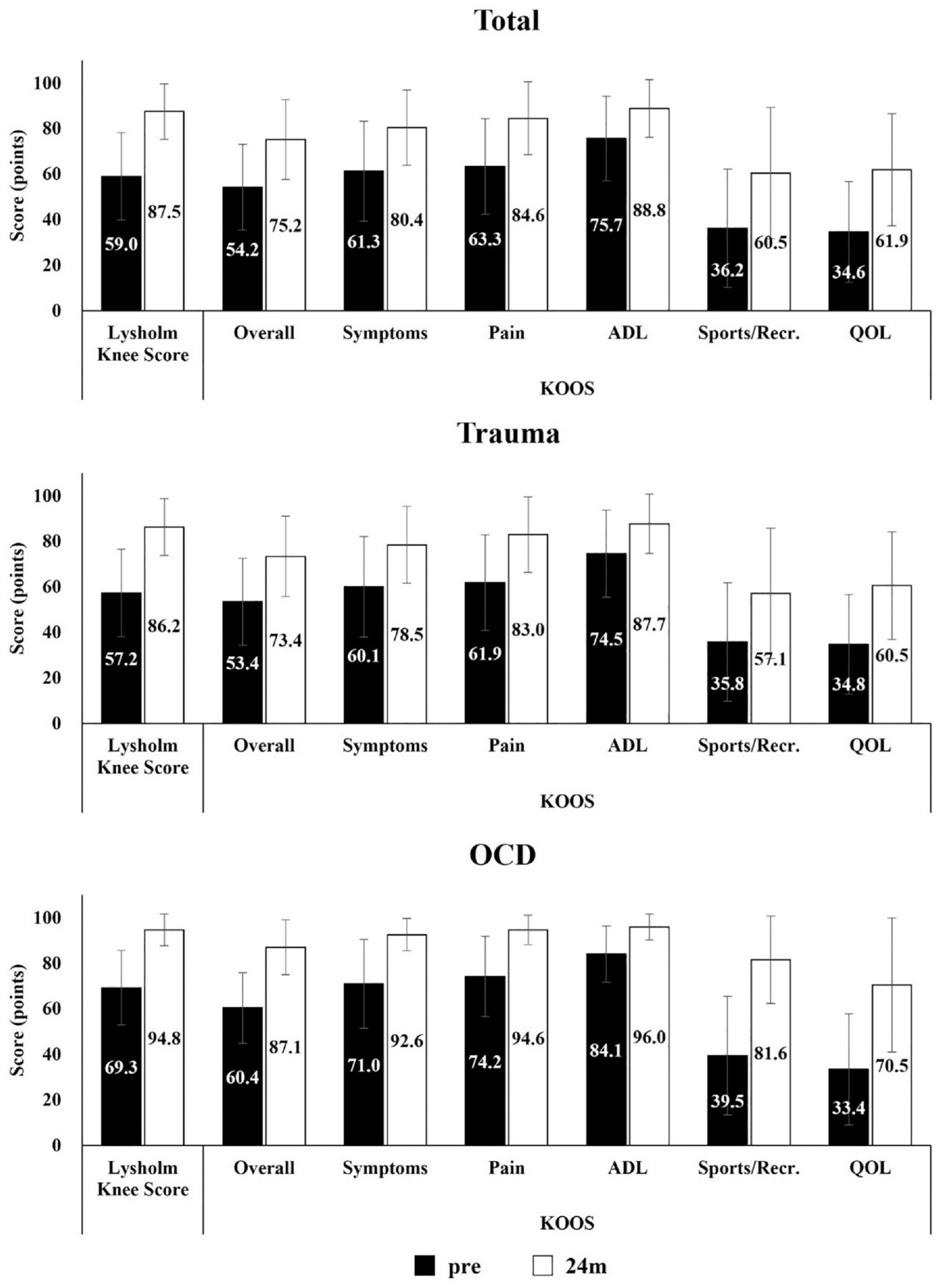
Changes in Lysholm knee score and Knee injury and Osteoarthritis Outcome Score (KOOS) in the total, trauma, and osteochondritis dissecans (OCD) groups. Before (pre) and 24 months (24 m) after implantation. Scale bar: mean ± SD. ADL, Activities of Daily Living; QOL, Quality of Life; Sports/Recr., Sports/Recreation.
The overall effectiveness of pMACI is shown in Table 3. The MCID in LKS and the KOOS Symptoms subscale was achieved in 79.7% and 63.5% of patients, respectively, and the PASS in 90.1% and 73.7%, respectively. However, the SCB in the KOOS Sports/Recreation and QOL subscales was achieved in 39.6% and 37.8% of patients, respectively.
Optimal Change Score Cutoff and Patients Achieving MCID, PASS, or SCB a

ADL, Activities of Daily Living: KOOS, Knee injury and Osteoarthritis Outcome Score; LKS, Lysholm knee score; MCID, minimal clinically important difference; PASS, Patient Acceptable Symptom State; QOL, Quality of Life; SCB, substantial clinical benefit; Sports/Recr., Sports/Recreation.
Each subscale of the KOOS had missing values for the change and final scores, as the study included patients with LKS scores preoperatively and 6 months postoperatively.
Chronological Effects of Diseases on pMACI Effectiveness
Figure 4 shows the changes in the mean LKS and KOOS scores in the trauma and OCD groups. The LKS and KOOS values in all domains were significantly greater 2 years postoperatively compared with preoperatively in both groups (P < .005). There were no significant differences in the changes in LKS between the groups. Improvements in the KOOS Sports/Recreation and QOL subscales were significantly earlier and better in the OCD group than in the trauma group, except for QOL at 24 months (Sports/Recreation difference at 6, 12, and 24 months: P = .0113, P = .0047, and P = .0107, respectively; QOL difference at 6, 12, and 24 months: P = .0301, P = .0346, and P = .0517, respectively).
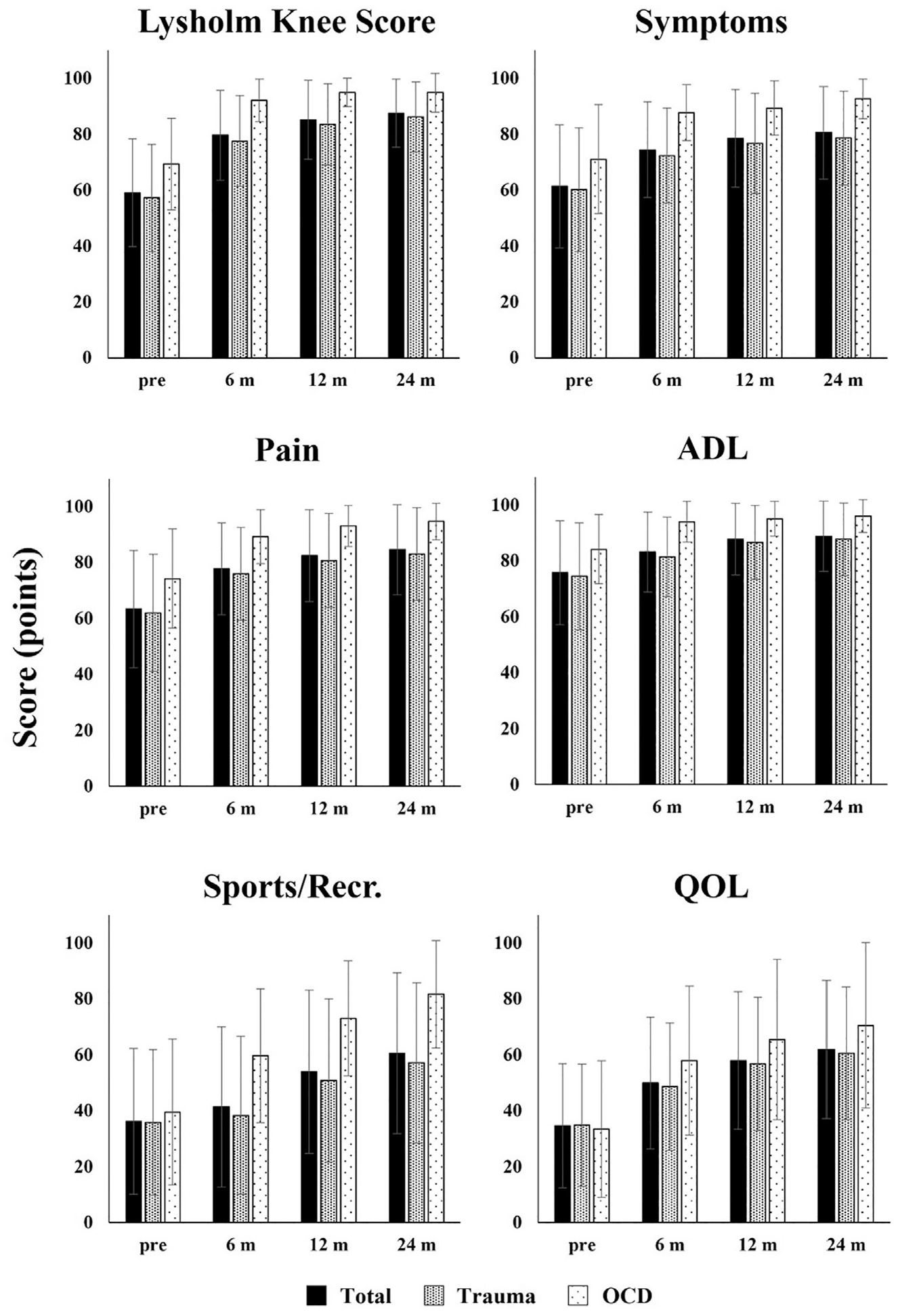
Chronological changes in the Lysholm knee score and Knee injury and Osteoarthritis Outcome Score in the total, trauma, and OCD groups. Before (pre) and 6, 12, and 24 months (m) after implantation. Scale bar: mean ± SD. ADL, Activities of Daily Living; QOL, Quality of Life; Sports/Recr., Sports/Recreation.
Chronological Effects of Concomitant Surgeries on the Effectiveness of pMACI
Figure 5 shows the mean LKS and KOOS scores for the concomitant surgeries. Significant improvements were observed in all domains except for the pMACI with MF subgroup, which showed improvement only in the LKS. Differences between preoperative and 24-month KOOS Symptoms, Sports/Recreation, and QOL subscales in the pMACI with MF subgroup were significantly lower than those in the pMACI-alone subgroup (Symptoms difference, P = .0490; Sports/Recreation difference, P = .0125; QOL difference, P = .0361). The difference in KOOS Symptoms in the pMACI with OAT subgroup was significantly higher than that in the pMACI-alone subgroup (P = .0468).
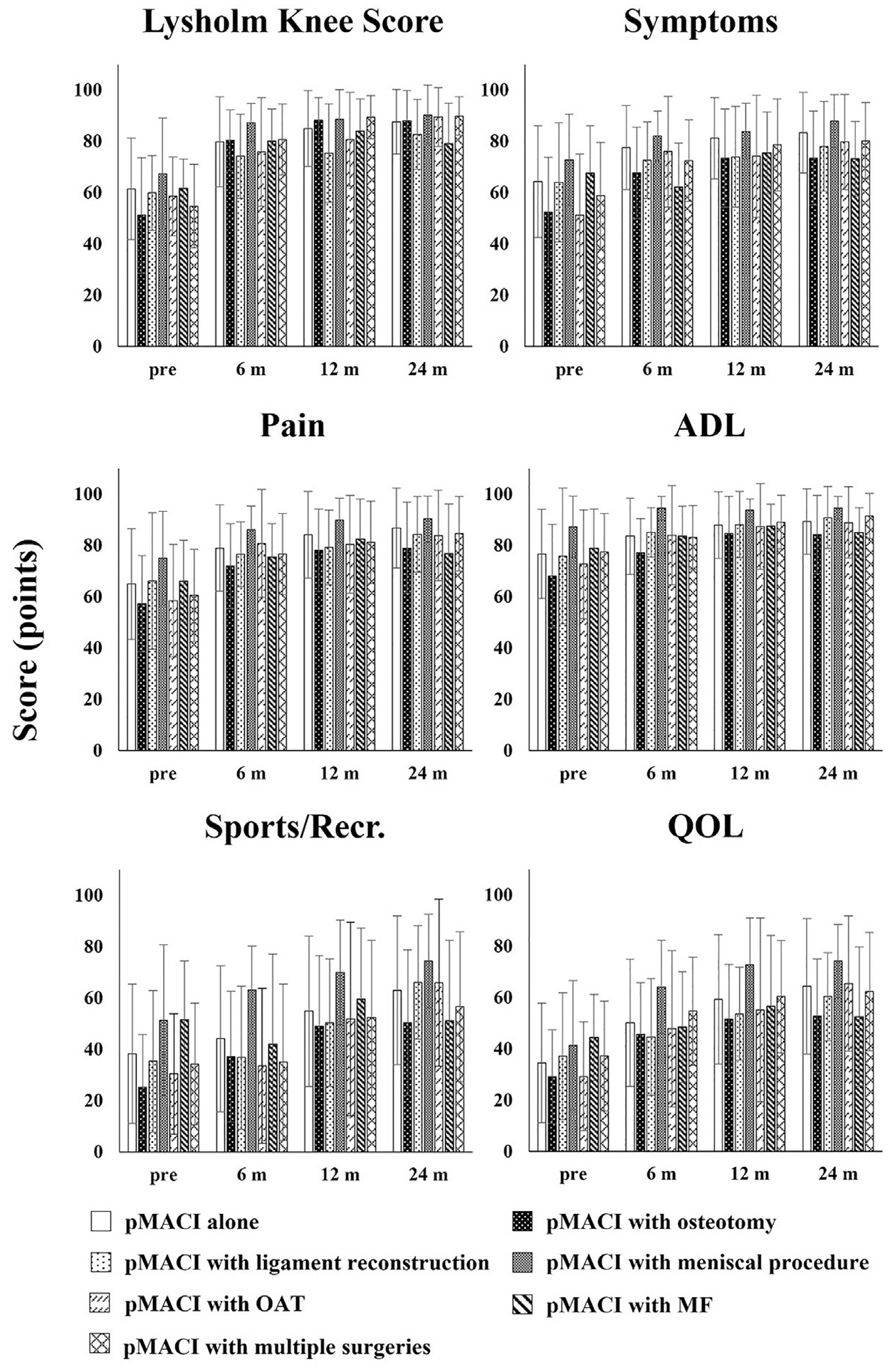
Lysholm knee score and Knee injury and Osteoarthritis Outcome Score regarding concomitant surgeries. Before (pre) and 6, 12, and 24 months (m) after implantation. Scale bar: mean ± SD. ADL, Activities of Daily Living; MF, microfracture; OAT, osteochondral autograft transplantation; pMACI, matrix-associated autologous chondrocyte implantation with an autologous periosteum; QOL, Quality of Life; Sports/Recr., Sports/Recreation.
Adverse Events
Overall, 86 (37.1%) knees in 86 patients experienced AEs. The most frequently reported AEs were effusion (16.8%), graft delamination (14.7%), knee contracture (9.1%), graft hypertrophy (8.2%), and ossification (3.4%) (Table 4).
Adverse Events of pMACI a

pMACI, matrix-associated autologous chondrocyte implantation with an autologous periosteum.
Other events: joint loose body (3 knees); procedural pain, surgical site infection, cartilage defect at the boundary between the normal cartilage and transplantation, new cartilage defect, and crepitus (2 knees each); synovitis, instability, cellulitis, swelling, pyrexia, patellar fracture, extraskeletal ossification, lateral graft overgrowth, and osteonecrosis (1 knee each).
The Fisher exact test revealed that OCD was significantly associated with graft hypertrophy (20.6% vs 6.1%; P = .0108) and ossification (11.8% vs 2.0%; P = .0177), whereas concomitant surgery was significantly associated with overall AEs (46.0% vs 28.6%; P = .0067), the most frequently reported AEs (45.1% vs 25.2%; P = .0016), delamination (20.4% vs 9.2%; P = .0248), and knee contracture (15.0% vs 3.4%; P = .0024).
Among the 86 knees, 26 required arthroscopic debridement as repeated surgery, and 7 required other treatments, such as medication (n = 2), surgical wound debridement (n = 2), immobilization (n = 1), puncture (n = 1), and prolonged rehabilitation (n = 1), to treat AEs. Reoperations such as OAT (n = 8), MF (n = 4), and revision pMACI concomitant with high tibial osteotomy (n = 1) were required for recovery in 13 knees. Two of the 13 knees underwent reoperation for a new cartilage defect. Neither total nor unicompartmental knee reconstruction was needed. Thus, 11 (4.7%) knees in 11 patients experienced treatment failure.
In the initially included group (344 knees in 335 patients), in which safety was checked at each consultation in all cases, 121 (35.2%) knees in 120 patients showed AEs such as effusion (n = 49, 14.2%), graft delamination (n = 50, 14.5%), knee contracture (n = 26, 7.6%), graft hypertrophy (n = 29, 8.4%), and ossification (n = 9, 2.6%). No apparent differences were observed in the AE ratios between the initially included and pMACI efficacy assessment groups. The Fisher exact test showed no significant difference in the incidence of the most frequently reported AEs between the group assessing the efficacy of pMACI and the group without scores.
Discussion
This study revealed favorable outcomes in approximately 75% of the patients, while one-third experienced AEs, 11.2% required repeat surgery, and 4.7% required additional cartilage procedures. The responders achieved the above-optional PASS in 90.1% of LKS, 73.7% of KOOS Symptoms, and 83.0% of KOOS Pain due to pMACI. These outcomes were equivalent to or greater than those reported by Chahal et al. 7 Their cartilage repair techniques included osteochondral allograft (43%), ACI (12%), MF (12%), chondroplasty/debridement (31%), and particulated articular cartilage allograft (3%) for chondral lesions (2.7 ± 1.6 cm2).
However, pMACI enabled responders to achieve the optional SCB in the KOOS Sports/Recreation and QOL subscales at 39.6% and 37.8%, respectively, despite an MCID in 79.7% of LKS and 63.5% of KOOS Symptoms. Based on the cutoff points of Ogura et al, 35 responders achieved the above-optional SCB in the KOOS Sports/Recreation and QOL subscales at 58.3% and 50.6%, respectively, suggesting that pMACI achieved only two-thirds or three-fourths of responders reported by Ogura et al. 35
Compared with previous studies, ** few studies have reported the outcomes of ACI limited to large cartilage defects (≥4 cm2) in the knee joint. A phase 2 study of MACI with spheroid technology for cartilage defects (mean, 5.6 cm2; range, 4-10 cm2) showed significant improvement in the mean KOOS values at 2 years postoperatively. 30 A phase 3 study of hydrogel-based ACI for cartilage defects (mean, 4.8 cm2; range, 4-12.5 cm2) showed improved KOOS values ≥10 points in 93% of patients at 2 years postoperatively. 29 Their previous studies29,30 lacked the LKS, MCID, PASS, and SCB evaluations. The effectiveness of MACI should also be evaluated individually. The current study provides significant information about responders to MACI.
Graft delamination was the critical AE in 14.7% of knees. This study demonstrated a relatively higher rate of graft delamination than previous reports,13,49 suggesting that observation might be attributable to the use of autologous periosteum and the inclusion of surgeons who did not perform many pMACI procedures or to new traumatic injuries. Statistical analysis showed that concomitant surgeries affected graft delamination. Harris et al 13 suggested that graft delamination might be due to new traumatic injury (eg, through noncompliance with rehabilitation) or atraumatic flap formation secondary to insufficient integration into the normal surrounding peripheral cartilage or underlying subchondral bone. A firm surface and good stability are necessary to prevent graft delamination and failure after pMACI, which can be controlled using a collagen membrane.
Graft hypertrophy was another critical AE demonstrated in 19 (8.2%) knees with pMACI. In previous studies, the incidence has ranged from 4.2% to 38.1% in pACI, †† 0% to 9% in ACI covered with type I/III collagen (cACI),2,11,13 and 1% to 30% in MACI.2,9,13,48,49 Migliorini et al 24 found that graft hypertrophy doubled in pACI recipients. Periosteal ACI is reported to be more likely to induce graft hypertrophy because of growth factors and chondrocyte precursor cells in the inner cambium layer. 21 This might be explained by the fact that, in this study, OCD significantly induced graft hypertrophy compared with a traumatic injury.
Ossification after pMACI may be a specific issue. Eight (3.4%) knees exhibited ossification, with an open epiphysis observed in 5 (62.5%), indicating a high risk of bone formation due to expanded chondrocytes in the periosteal flap. Statistical analysis demonstrated that OCD significantly induced ossification, and that an artificial membrane without risk should be used to prevent it. Therefore, Japanese surgeons should switch to more advanced MACI procedures to use collagen membranes.
This study is not without limitations. First, this analysis required clinical follow-up. Second, not having a control or reference group for comparison is a limitation. Many concomitant surgeries and different sites and pathologies have been included, which reduced the ability to analyze subgroups. Additional studies to address these issues and long-term durability, along with trials using innovative MACI techniques that address periosteum-related issues, might therefore result in changes in real-world data compared with the original form of pMACI.
Conclusion
Treatment of large cartilage defects ≥4 cm2 with pMACI resulted in improved outcome scores in approximately 75% of patients. However, complications occurred in one-third of patients, and 4.7% required reoperation.
Footnotes
Acknowledgements
The authors thank all clinical investigators and patients for their participation in the study. Keisuke Higashimoto (Japan Tissue Engineering Co., LTD.) and Yuko Maeda (Japan Tissue Engineering Co., LTD.) provided medical writing assistance, and Norichika Matsuki (Japan Tissue Engineering Co., LTD.) provided statistical analysis assistance, which Japan Tissue Engineering Co., LTD. funded.
Submitted November 9, 2023; accepted August 13, 2024.
One or more of the authors has declared the following potential conflict of interest or source of funding: Y.U. is a consultant who receives institutional support from Japan Tissue Engineering Co., LTD. (Japan). Y.U. has received institutional support from Pfizer Japan, Inc. (Japan), Eli Lilly Japan KK (Japan), Ono Pharmaceutical Co., LTD. (Japan), Daiichi Sankyo Co., LTD. (Japan), Shionogi & Co., LTD. (Japan), Kaken Pharmaceutical Co., LTD. (Japan), Chugai Pharmaceutical Co., LTD. (Japan), Mochida Pharmaceutical Co., LTD. (Japan), Nippon Zoki Pharmaceutical Co., LTD. (Japan), Seikagaku Corporation (Japan), Taisho Pharmaceutical Holdings Co., LTD. (Japan), Hisamitsu Pharmaceutical Co., Inc. (Japan), and Stryker (Japan). R.K. is a consultant who receives institutional support from Medacta International (Japan) and Japan Tissue Engineering Co., LTD. (Japan). R.K. has received institutional support from Zimmer Biomet (Japan), Smith & Nephew (Japan), and Hirosaki Life Science Innovation, Inc. (Japan). AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.