
Abstract
Background:
Ruptures of the distal biceps tendon (DBT) can affect the range of motion and strength of the elbow, raising concerns for patients seeking to restore normal function and engage in their regular activities, particularly returning to previous levels of sport participation.
Purpose:
To characterize and assess the rate and timing of return to sport (RTS) after DBT repair.
Study Design:
Systematic review; Level of evidence, 4.
Methods:
PubMed, Embase, and Google Scholar (pages 1-20) were searched from database inception to December 6, 2023 for clinical studies reporting RTS outcomes after DBT repair. The extracted data consisted of patient characteristics; information on the incision approach, fixation method, and rehabilitation protocol; and outcome data including RTS rates, patient-reported outcome measure scores, and complications.
Results:
A total of 42 studies, including 1093 patients (1100 elbows), met the inclusion criteria. The mean age of patients was 44.9 years, and 99.2% of patients were male. The mean follow-up time was 31.5 months. Ruptures were acute in 87.6% of cases, the dominant arm was injured in 64.9%, and the cause of the injury was sport related in 43.5%. The overall RTS rate was 91.5%, with 85.2% of patients returning to preinjury levels or higher, at a mean time of 6.3 months. Patients had excellent functional outcomes, irrespective of the incision approach or fixation method, although trends associated with a higher RTS rate were observed with bone tunnel fixation, ≤2 weeks of postoperative immobilization, early initiation of active range of motion postoperatively, and initiation of strengthening at ≤10 weeks. Single-incision repair had higher rates of nerve-related complications and reruptures compared with double-incision repair, and cortical button fixation had a higher rate of nerve-related complications among the fixation methods.
Conclusion:
There was a high rate of RTS after DBT repair at 6 months postoperatively. A positive trend for RTS was observed with respect to rehabilitation protocols favoring earlier active mobility.
A rupture of the distal biceps tendon (DBT) is a relatively rare injury, with an incidence ranging from 1.2 to 2.6 per 100,000 patients.28,49 The majority of DBT ruptures occur in male patients aged between 35 and 55 years, often as a result of an eccentric load on a flexed and supinated forearm.28,49 This mechanism of injury is commonly encountered in weightlifting, physically demanding jobs, and combat and contact sports. 59 Further risk factors for a DBT rupture include age, elevated body mass index, smoking, anabolic steroid use, and corticosteroid use. 55 Age-related degenerative changes have been observed in the DBT in patients aged as young as 35 years and may contribute to spontaneous ruptures. 27 Further, the DBT contains a known vascular watershed region, rendering the area susceptible to ruptures.50,55
Tears of the DBT can be either partial or complete. The most common tear pattern is avulsion of the DBT off of the radial tuberosity; however, intratendinous and intramuscular tears are seen. The treatment of DBT ruptures depends on factors such as the tear pattern and the patient’s lifestyle and aesthetic preferences. However, biomechanical studies have shown that a complete DBT rupture leads to reductions in 30% of peak elbow flexion strength and 40% to 50% of peak forearm supination strength; thus, operative treatment is often recommended.39,41
Surgical repair of the DBT can be through either a single or double incision, each with associated strengths and weaknesses. 17 In addition, fixation to the radial tuberosity can be performed with the use of cortical buttons, suture anchors, bone tunnels, or interference screws. The choice of repair strategy is influenced by the chronicity of the tear, with tendon retraction in chronic cases potentially requiring the use of tendon grafts to bridge the gap to the radial tuberosity. 26 Postoperative rehabilitation of DBT ruptures typically involves a period of immobilization in elbow flexion, followed by a progression of passive and active ranges of motion to strengthening, as determined by the surgeon.
DBT ruptures pose a concern for patients seeking to restore normal function and engage in their regular activities, whether recreational or professional. Previous systematic reviews have indicated that return to work is achievable within 3 to 4 months after surgery, 48 with a longer recovery time expected for return to sport (RTS) in athletes, at around 9 months. 44 The rate, timing, and level of RTS are important factors to understand to appropriately educate patients and set expectations. However, there are no current systematic reviews on the overall rate of RTS for patients within the general population. This study aimed to systematically review the orthopaedic literature to characterize the rate and timing of RTS after DBT ruptures and repair.
Methods
A systematic review was conducted following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. 38
Search Strategy
PubMed, Embase, and Google Scholar (pages 1-20) were searched on December 6, 2023 using predetermined keywords. The keywords “distal biceps,”“rupture,”“tear,”“avulsion,”“detachment,” and “sport” were applied to find articles pertaining to functional and RTS outcomes after DBT repair. Additional articles were identified by searching through reference lists.
Inclusion criteria consisted of (1) DBT repair, (2) reporting of functional outcomes, (3) reporting of RTS outcomes, (4) patients aged ≥18 years, and (5) all levels of play (eg, recreational, semiprofessional, professional). Exclusion criteria consisted of (1) case reports; (2) narrative or systematic reviews; (3) biomechanical, anatomic, radiological, or cadaveric studies; (4) technique articles; (5) conference abstracts; (6) augmentation procedures; and (7) nonoperative outcomes.
Study Screening
There were 2 reviewers (P.B. and M.D.) who independently evaluated all titles and abstracts, and subsequently full-text articles, for eligibility. All articles identified by both reviewers at the title and abstract stage were included. Full texts were evaluated, and disagreements were discussed between the 2 reviewers and resolved by a consensus.
Data Extraction
Relevant data from included studies were extracted into a predetermined data sheet. Extracted data included study characteristics (eg, author, year of publication, level of evidence, sample size), patient characteristics (eg, age, sex, percentage of dominant extremity injuries, time between injury and surgery, percentage of sport-related injuries, type and level of sport), intervention details (eg, incision approach, fixation method, rehabilitation protocol, duration of follow-up), and outcome data (rate of RTS, time to RTS, rate of return to preinjury levels or higher, patient-reported outcome measure scores, and complications). Outcome measures reported included the Disabilities of the Arm, Shoulder and Hand (DASH), the quick version of the DASH (QuickDASH), the Mayo Elbow Performance Score (MEPS), the Oxford Elbow Score (OES), a visual analog scale (VAS), and satisfaction. RTS and functional outcomes were evaluated for the entire cohort, which included both patients engaged in recreational activities and athletes. A subanalysis on RTS outcomes for athletes alone was performed as well.
Statistical Analysis
Quantitative statistical analysis was performed using Stata statistical software (Version 14.1; StataCorp).
Results
Literature Search
The initial literature search resulted in 629 articles. After the removal of 159 duplicate studies, 470 articles were screened for inclusion and exclusion criteria. Then, 102 studies were evaluated, and full texts were assessed for eligibility. Overall, 42 clinical studies were included in this systematic review, as demonstrated in Figure 1. §
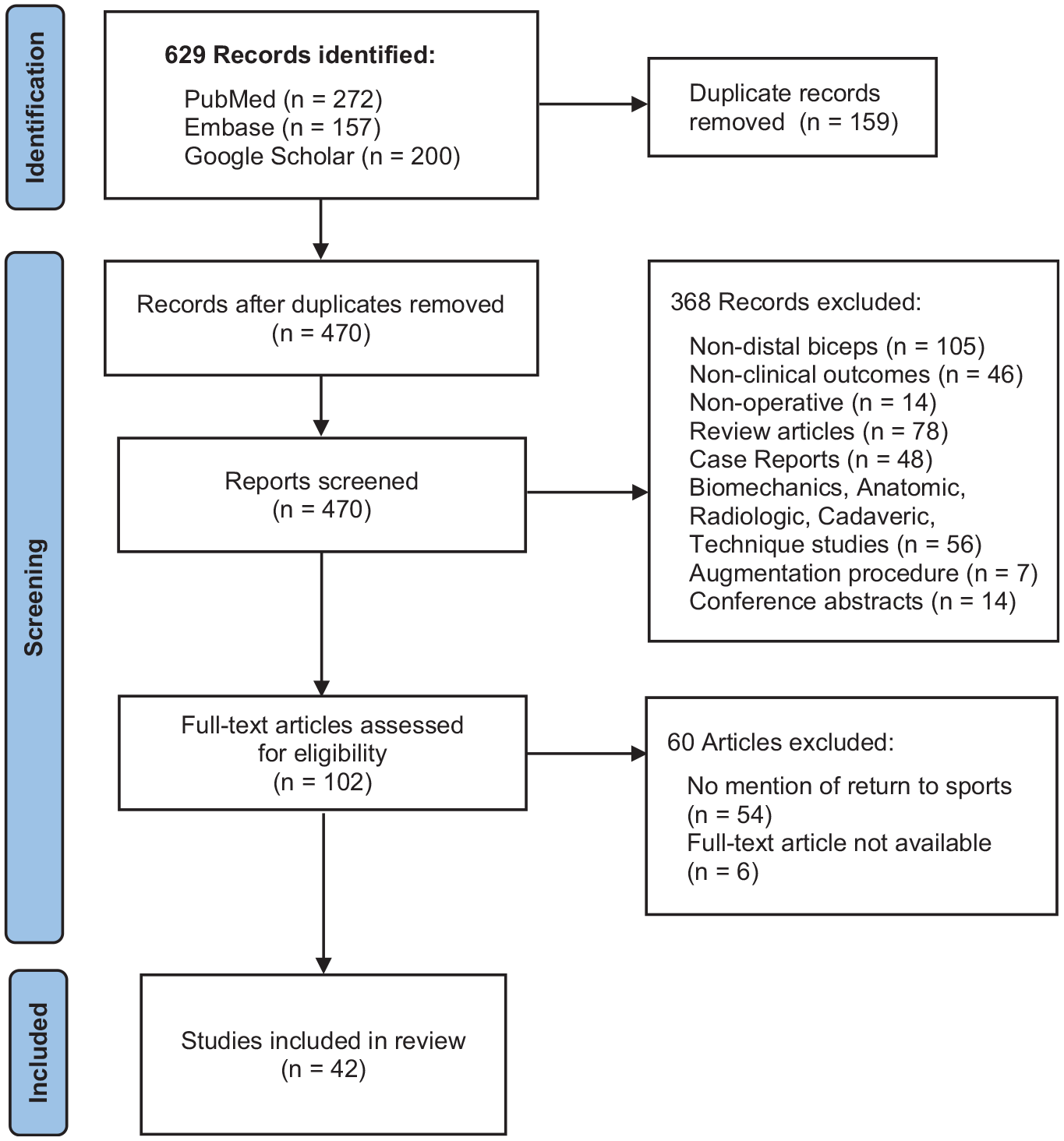
Outline of PRISMA search strategy. PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
Characteristics of Studies
A total of 42 studies, including 1093 patients (1100 elbows) who underwent DBT repair, met the inclusion criteria. The median sample size of the included studies was 21 patients (range, 4-108). The majority of patients were male (99.2%), with a mean age of 44.9 years (range, 27.4-56.5 years) and a mean follow-up of 31.5 months (range, 7.4-84.0 months). The median time from the injury to surgery was 13.1 days (range, 3.8-259.0 days), and ruptures were acute in 87.6% (558/637) of cases. The dominant arm was injured in 64.9% (522/804) of patients, and the cause of the injury was sport related in 43.5% (210/483). Of all the patients, 169 (15.5%) were reported to be athletes. The study characteristics and patient characteristics are illustrated in Table 1.
Study and Patient Characteristics a
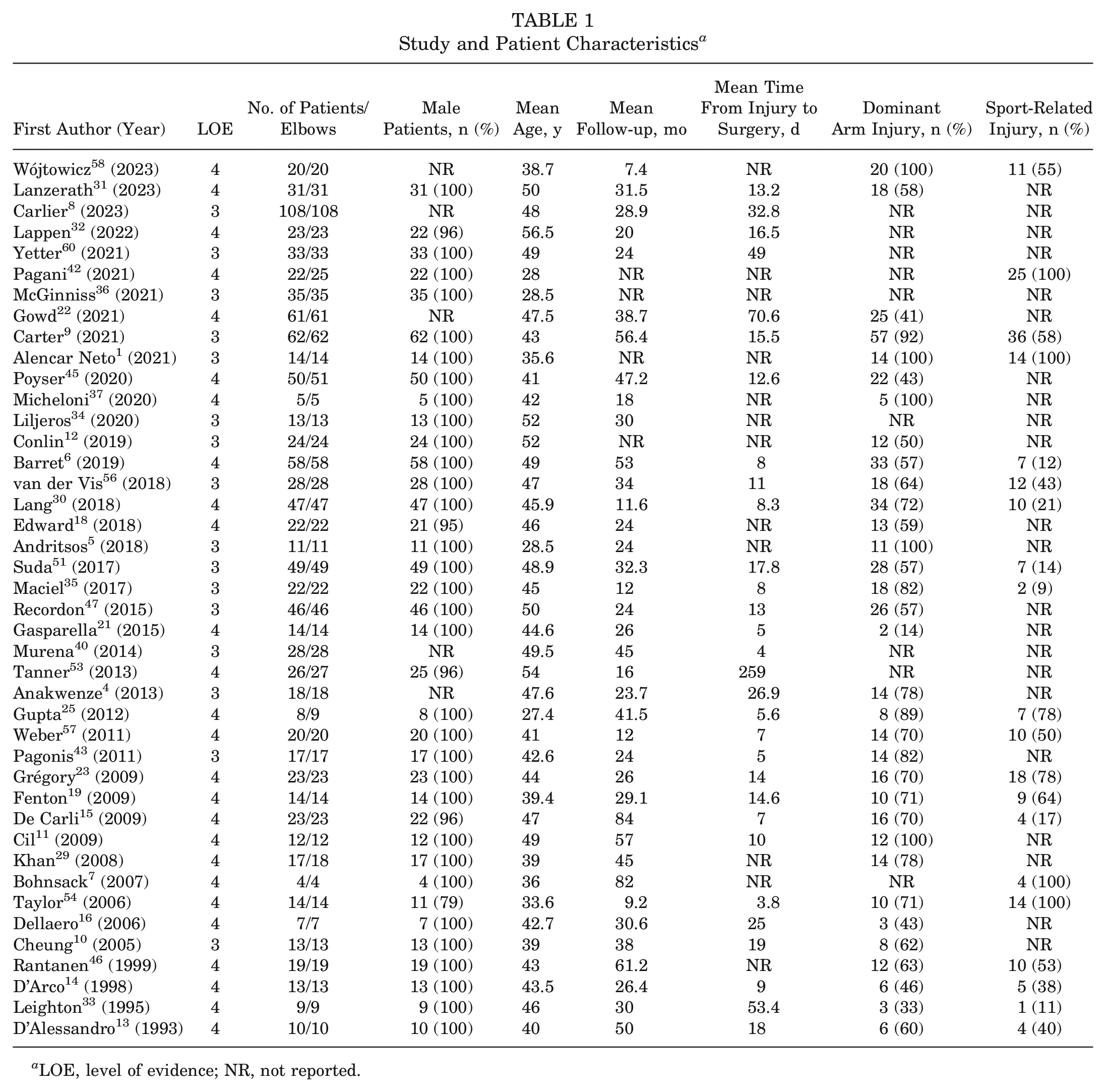
LOE, level of evidence; NR, not reported.
Surgical Technique and Rehabilitation
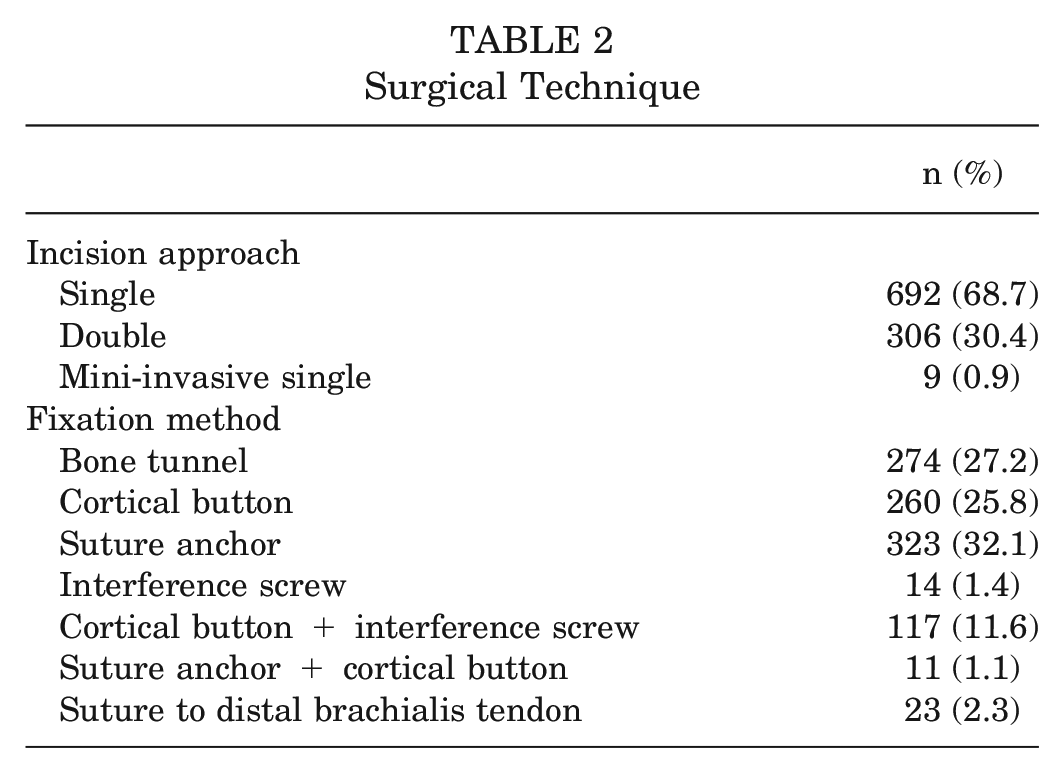
The distribution of patients by surgical technique is presented in Table 2. Of the 38 studies that reported the surgical technique, including 1007 patients (92.1%), pooled data found that single-incision repair was performed in 68.7% of patients and double-incision repair was performed in 30.4%. For the method of fixation, 27.2% of cases involved bone tunnels, 25.8% involved cortical buttons, 32.1% involved suture anchors, 1.4% involved interference screws, and 11.6% involved a combination of cortical buttons and interference screws.
Surgical Technique
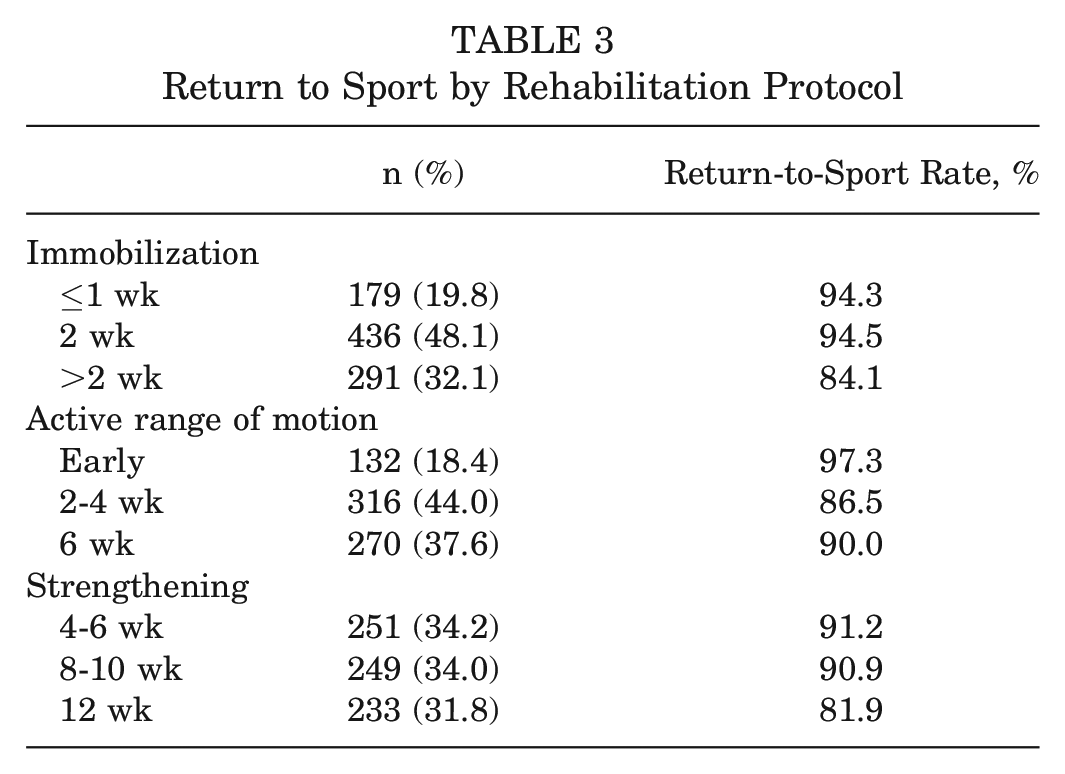
Rehabilitation protocols varied across 35 studies, including 906 patients. The distribution of patients by rehabilitation protocol is presented in Table 3. The majority of patients were immobilized for ≤2 weeks postoperatively (67.9%). Active range of motion was initiated on the first postoperative day in 18.4% of patients, within 2 to 4 weeks in 44.0%, and at week 6 in 37.6%. Strengthening was initiated within 4 to 6 weeks in 34.2% of patients, within 8 to 10 weeks in 34.0% of patients, and at week 12 in 31.8% of patients. The rehabilitation protocol of each study is summarized in the Appendix (available in the online version of this article).
Return to Sport by Rehabilitation Protocol
RTS Outcomes
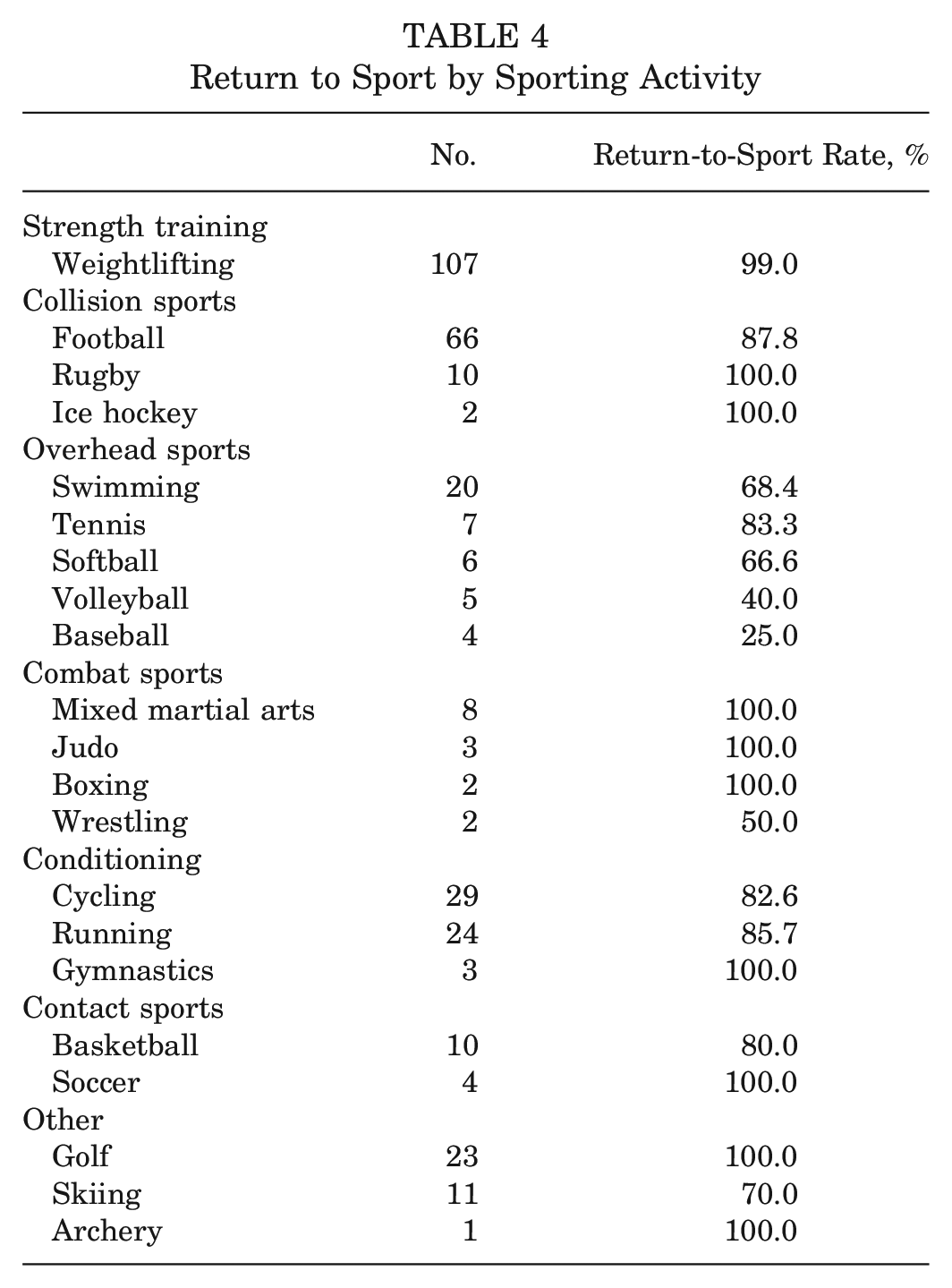
The overall RTS rate for all patients was 91.5%, with 85.2% (506/594) of patients returning to preinjury levels or higher. The mean time to RTS was reported in 18 studies and was found to be 6.3 months (range, 3.0-12.55 months). Rates of RTS by sporting activity are presented in Table 4. Of the 169 athletes specifically, the RTS rate was found to be 96.4%, with 92.9% (130/140) of athletes returning to preinjury levels or higher. The mean time to RTS in athletes was reported in 9 studies and was found to be 9.4 months (range, 3.0-12.55 months).
Return to Sport by Sporting Activity
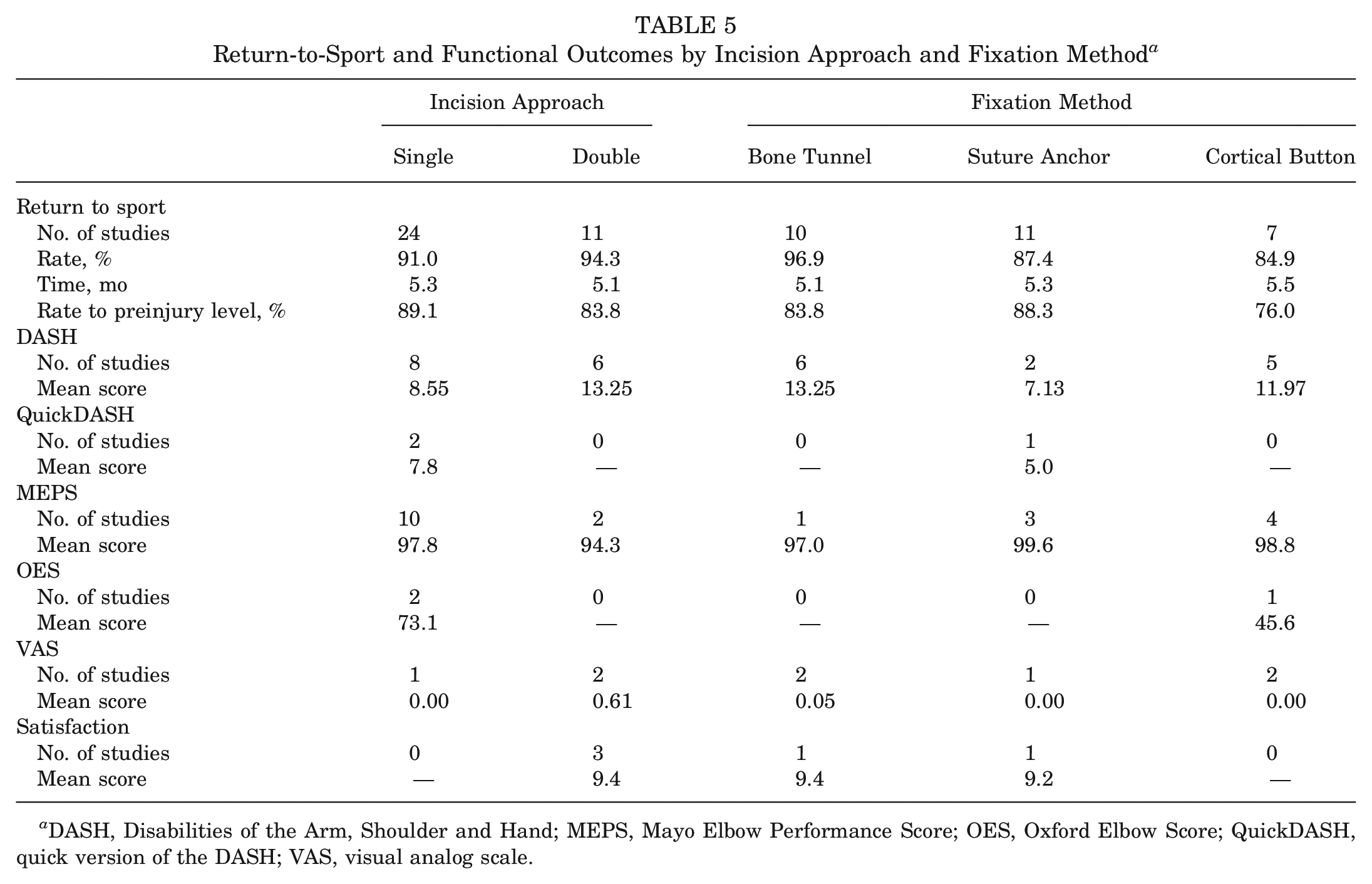
While RTS outcomes were similar between single- and double-incision approaches, there was a higher trend in the rates of RTS and return to preinjury levels of sport in patients with bone tunnel fixation (96.9% and 83.8%, respectively) compared with those with suture anchor fixation (87.4% and 88.3%, respectively) and cortical button fixation (84.9% and 76.0%, respectively) (Table 5). There was also a positive trend for high RTS rates in patients with early initiation of active range of motion after surgery (97.3%) and a negative trend in patients who had prolonged immobilization for >2 weeks (84.1%) and delayed initiation of strengthening at week 12 (81.9%) (Table 3).
Return-to-Sport and Functional Outcomes by Incision Approach and Fixation Method a
DASH, Disabilities of the Arm, Shoulder and Hand; MEPS, Mayo Elbow Performance Score; OES, Oxford Elbow Score; QuickDASH, quick version of the DASH; VAS, visual analog scale.
Functional Outcomes
Functional outcomes reported in studies varied: DASH scores were reported in 15 studies, ∥ QuickDASH scores in 5 studies,8,9,56,58,60 MEPS scores in 12 studies, ¶ OES scores in 4 studies,9,40,56,58 VAS scores in 8 studies,6,8,32,35,47,53,56,60 and satisfaction scores in 6 studies.9,12,45,47,58,60 The mean DASH score (n = 348) was 10.25, the mean QuickDASH score (n = 251) was 4.8, the mean MEPS score (n = 358) was 96.8, the mean OES score (n = 138) was 58, the mean VAS score (n = 345) was 0.3, and the mean satisfaction score (n = 236) was 9.52.
Functional outcome scores based on the incision approach and fixation method are presented in Table 5. The single-incision approach showed a mean DASH score of 8.55 and a mean MEPS score of 97.8 compared with 13.25 and 94.3, respectively, for the double-incision approach, suggesting excellent functional performance with both. While the trends in MEPS and VAS scores were similar, suture anchor fixation had slightly lower DASH scores (7.13) compared with bone tunnel fixation (13.25) and cortical button fixation (11.97).
Complications
Complications were documented in 35 studies, involving 946 patients (Table 6). There were a total of 182 complications (19.2%), of which 129 were nerve-related injuries: 112 had sensory neurapraxia (61.5%), and 17 had an unresolved nerve injury (9.3%). There were a total of 21 reoperations (2.2%), of which 11 were due to a rerupture of the DBT (52.4%), 6 due to radioulnar synostosis (28.6%), 2 due to heterotopic ossification (9.5%), and 2 due to an unresolved nerve injury (9.5%).
Complications and Reoperations by Incision Approach and Fixation Method a
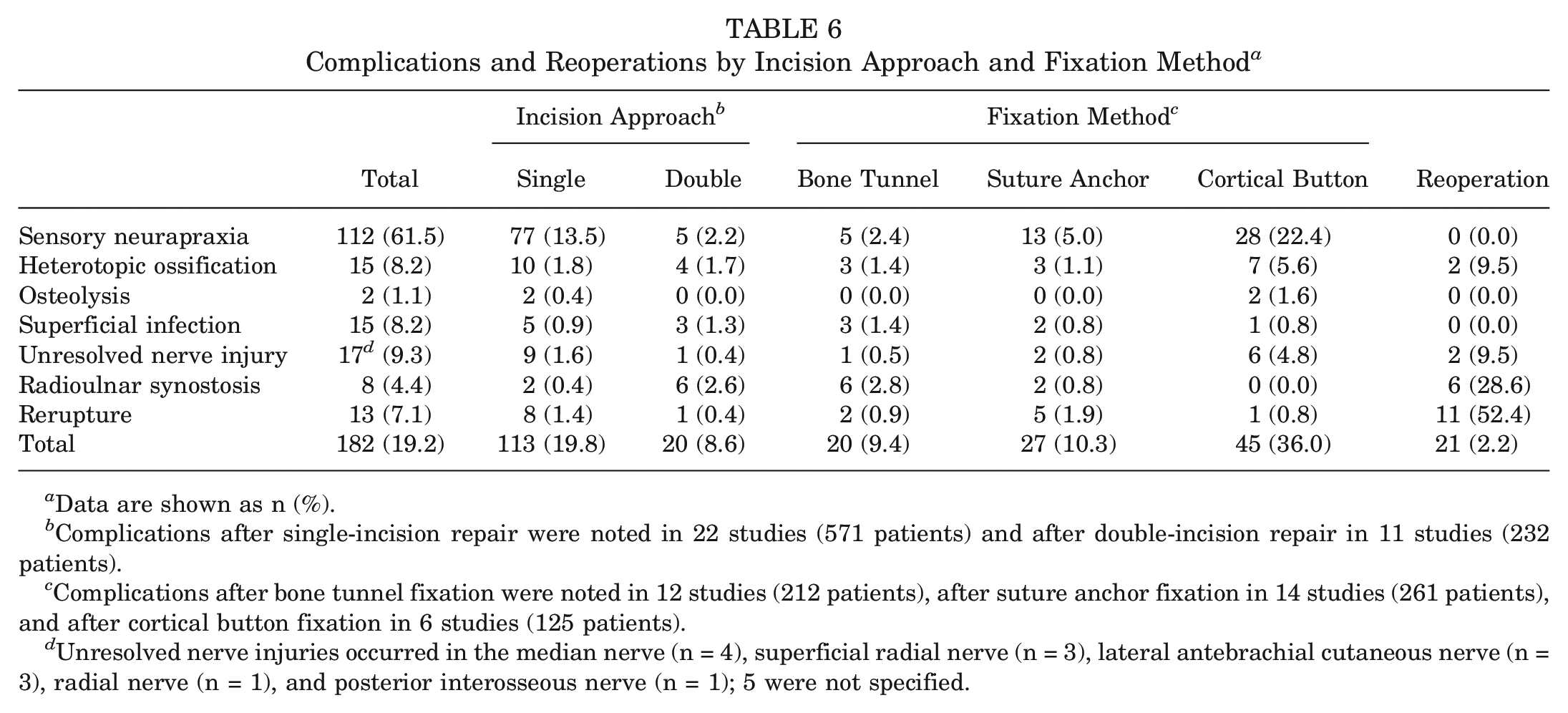
Data are shown as n (%).
Complications after single-incision repair were noted in 22 studies (571 patients) and after double-incision repair in 11 studies (232 patients).
Complications after bone tunnel fixation were noted in 12 studies (212 patients), after suture anchor fixation in 14 studies (261 patients), and after cortical button fixation in 6 studies (125 patients).
Unresolved nerve injuries occurred in the median nerve (n = 4), superficial radial nerve (n = 3), lateral antebrachial cutaneous nerve (n = 3), radial nerve (n = 1), and posterior interosseous nerve (n = 1); 5 were not specified.
The single-incision approach was found to have a higher total complication rate (19.8%) compared with the double-incision approach (8.6%), with higher rates of sensory neurapraxia (13.5% vs 2.2%, respectively), unresolved nerve injuries (1.6% vs 0.4%, respectively), and reruptures (1.4% vs 0.4%, respectively). While the rates of heterotopic ossification were similar, the double-incision approach had a higher rate of radioulnar synostosis than the single-incision approach (2.6% vs 0.4%, respectively). Cortical button fixation had the highest complication rate among fixation methods (36.0%), with higher rates of sensory neurapraxia (22.4%), unresolved nerve injuries (4.8%), and heterotopic ossification (5.6%). In all studies reviewed, the cortical button was placed bicortically. Bone tunnel fixation and suture anchor fixation had similar total complication rates of 9.4% and 10.3%, respectively; bone tunnel fixation had the highest rate of radioulnar synostosis of 2.8%; and suture anchor fixation had the highest rate of reruptures of 1.9%.
Comparative Studies
Overall, 9 studies assessed RTS and functional outcomes among various study groups. There were 5 studies that compared fixation methods, with 4 reporting similar outcomes between different techniques.22,30,45,47,56 Lang et al 30 found no difference in the ability to RTS after DBT repair by bone tunnels, suture anchors, and cortical buttons; Recordon et al 47 reported no difference in functional outcomes between cortical button fixation and bone tunnel fixation; and both van der Vis et al 56 and Poyser et al 45 found no difference between suture anchor fixation and cortical button fixation. In contrast, in their multivariate analysis, Gowd et al 22 found a decreased likelihood of RTS to the same or better preinjury level with suture anchor fixation compared with cortical button fixation. As for the incision approach, Gowd et al 22 also found an increased time to RTS with the single-incision approach (6.55 months) compared with the double-incision approach (4.85 months). Murena et al 40 compared standard and mini-invasive single-incision approaches and found a positive trend in strength recovery, time to RTS, and DASH scores with the mini-invasive approach, although OES and MEPS scores were similar. Conlin et al 12 showed that repair of the bicipital aponeurosis in conjunction with DBT repair led to a faster return to recreational activities compared with isolated DBT repair (77% returned within 6 months vs 36% in the isolated DBT repair group). Moreover, 2 studies compared DBT repair in the acute and chronic settings and reported similar functional outcomes, irrespective of the time to surgery.4,8 Carlier and Pierreux 8 compared primary repair of acute (135 patients) and chronic (75 patients) DBT tears and demonstrated no significant difference in short- and long-term MEPS and QuickDASH scores, recovery of strength in flexion and supination, and rates of complications, although the acute repair group had a higher rate of asymptomatic heterotopic ossification than the chronic repair group (17% vs 4%, respectively).
Discussion
The principal finding of this study was the high RTS rate in patients after DBT repair. This systematic review found that 91.5% of all patients were able to RTS after a mean 6.3 months, with the majority returning to preinjury levels or higher. High rates of RTS and excellent functional outcomes were generally uniform across all incision approaches and fixation methods. Trends in the rate of RTS were observed in relation to the rehabilitation protocol, with higher return rates seen in those with ≤2 weeks of immobilization, early initiation of active range of motion exercises, and initiation of strengthening exercises between 4 and 10 weeks. The complication rate for patients included in this review was 19.2%, with the majority of these being sensory neurapraxia. The tendon rerupture rate was 1.4%. Reoperations occurred for reruptures, radioulnar synostosis, unresolved nerve injuries, and heterotopic ossification, with an overall rate of 2.2%.
This is the first systematic review that encompasses all available data on RTS after DBT repair in the orthopaedic literature. Given that weightlifting, contact sports, and combat sports often contribute to the occurrence of DBT ruptures, as evidenced by 43.5% of the patients in this review, knowledge of the timing and rate of RTS is essential for patients engaging in these activities, whether recreationally or professionally. The RTS rate in athletes specifically was considerably high at 96.4%. This was similar to a previous systematic review on RTS outcomes by Pitsilos et al 44 that evaluated 10 studies, including 157 athletes, reporting a rate of 97.5% that was independent of surgical technique or rehabilitation program. On the other hand, the time to RTS was higher in athletes at a mean 9.4 months compared with the overall mean time of 6.3 months. However, this may have been influenced by 2 studies that analyzed return to play in National Football League (NFL) players after DBT repair, with both reporting a late mean time to return to play of 11.46 and 12.55 months.36,42 This may be because of the small number of games in an NFL season, making return to play in the same season highly unlikely. While the rate of return to play in NFL players within 1 year was high, Pagani et al 42 showed that only 56% of players who undergo DBT repair remain in the NFL at 2 years. Moreover, Gowd et al 22 recommended that athletes with injuries to their dominant side should receive careful advice, as patients were found to have a decreased likelihood of RTS to the same level as well as a prolonged time to return to play in their multivariate analysis.
DBT repair can be performed through a single- or double-incision approach using various methods of fixation. Within the literature, functional outcomes have been shown to be similar, irrespective of the incision approach or fixation method.2,24 In our review, similar results were found between patients undergoing single- and double-incision repair in the rate, timing, and level of RTS. Radioulnar synostosis had a higher incidence with double-incision repair; however, single-incision repair had a much higher total complication rate, with higher rates of nerve-related injuries and reruptures. Similar results were demonstrated in a systematic review evaluating complications after DBT repair by Amarasooriya et al, 3 indicating a higher incidence of posterior interosseous nerve, lateral antebrachial cutaneous nerve, and superficial radial nerve injuries as well as a significantly higher rate of reruptures with single-incision repair. While an overall positive trend in the RTS rate was shown in favor of bone tunnel fixation, several comparative studies assessing different fixation methods reported no difference in functional and RTS outcomes.30,45,47,56 Grewal et al 24 performed a randomized controlled trial and demonstrated no difference in outcomes between single-incision repair with 2 anterior suture anchors and double-incision repair with bone tunnels. Despite differences seen in RTS and functional outcomes between surgical techniques, these differences were small and likely not clinically relevant. The differences in MEPS and DASH scores among surgical techniques did not achieve the minimal clinically important difference.20,52 However, cortical button fixation exhibited a higher total complication rate, particularly nerve-related injuries. In the systematic review by Amarasooriya et al, 3 cortical button fixation had a significantly higher rate of lateral antebrachial cutaneous nerve injuries compared with suture anchor fixation and bone tunnel fixation, although no significant difference in the rates of reruptures and posterior interosseous nerve injuries was seen between the fixation methods. Interestingly, a trend for high RTS rates was observed with respect to rehabilitation protocols that favored ≤2 weeks of immobilization, early initiation of active range of motion exercises, and initiation of strengthening exercises between 4 and 10 weeks. This may suggest that delays in active mobility may affect RTS outcomes in patients. Further research with high-quality clinical trials is warranted to explore and evaluate the effect of incision approach, method of fixation, and rehabilitation protocol on RTS and functional outcomes.
Several factors may be associated with a decreased rate of RTS. Edward et al 18 reported that 10 of 22 patients felt restricted from full sporting activity because of fear (n = 7), perceived weakness (n = 6), pain (n = 5), and restricted range of movement (n = 4). Similarly, Wójtowicz et al 58 observed that among the 4 patients who did not return to full activity, all reported a fear of reinjuries, and 2 experienced pain during physical activity. The fear of reinjuries or reruptures appears to be a prevalent limiting factor hindering RTS: Suda et al 51 showed that 21 patients (42.9%) stopped sport activities mainly because of concerns of a rerupture, and Weber et al 57 reported that 8 patients (40.0%) altered their sport behavior during the activities that led to the DBT injury. Poor mental health scores may affect RTS, as shown by Yetter et al 60 in which 88.9% (8/9) of patients with a Veterans RAND 12-item Health Survey mental component summary score <50 reported difficulty with RTS, in contrast to only 8.3% (2/24) of patients with a score ≥50. Gowd et al 22 found a delay in the treatment of a DBT injury to be associated with a decreased rate of RTS to the same or better level. However, other studies have shown similar functional outcomes, irrespective of the time to surgery, with no differences in MEPS and QuickDash scores, range of motion, and rate of complications.4,8
This study has several strengths. We performed a systematic review under the PRISMA guidelines, which allowed us to collate all the available literature on RTS in patients undergoing the surgical management of DBT ruptures, irrespective of patient characteristics, surgical technique, and rehabilitation program. Our study included a substantial number of patients with a robust follow-up, which enabled us to provide estimates on RTS timing and rates for the general population and athletes specifically. Nevertheless, this study has a number of limitations, namely, the low quality of evidence of the studies included, which were all level 3 or 4. There was heterogeneity in the patient-reported outcome measures used (DASH, QuickDASH, MEPS, etc), and numerous studies lacked data on the time to RTS and the level at which patients returned. There was also wide heterogeneity in the incision approach, method of fixation, and rehabilitation protocol. Some studies employed various incision approaches and methods of fixation without providing separate data for each group; this limited our ability to draw conclusions with regard to the effects of different surgical techniques on RTS and functional outcomes. We were unable to obtain individual study data to perform more detailed statistical analyses to compare incision approaches, fixation methods, rehabilitation protocols, and acute versus chronic tears.
Conclusion
After DBT repair, the overall RTS rate was 91.5%, with a mean time to RTS of 6.3 months. There was a 85.2% rate of return to preinjury levels or higher. In athletes specifically, the RTS rate was 96.4%, with 92.9% returning to preinjury levels or higher at a mean of 9.4 months. Although patients had excellent functional outcomes with surgical management, trends associated with a higher RTS rate included bone tunnel fixation, ≤2 weeks of postoperative immobilization, early initiation of active range of motion postoperatively, and initiation of strengthening at ≤10 weeks. Further high-quality, comparative clinical trials are needed to assess the effect of incision approach, fixation method, and rehabilitation protocol on the rate and timing of RTS particularly because this injury is often seen in athletes.
Supplemental Material
sj-pdf-1-ajs-10.1177_03635465241295618 – Supplemental material for Return to Sport After Distal Biceps Tendon Repair: A Systematic Review
Supplemental material, sj-pdf-1-ajs-10.1177_03635465241295618 for Return to Sport After Distal Biceps Tendon Repair: A Systematic Review by Peter Boufadel, Mohammad Daher, Ryan Lopez, Mohamad Y. Fares, Jad Lawand, Adam Z. Khan and Joseph A. Abboud in The American Journal of Sports Medicine
Footnotes
Submitted January 22, 2024; accepted May 7, 2024.
One or more of the authors has declared the following potential conflict of interest or source of funding: A.Z.K. has received support for education from Arthrex, Medical Device Business Services, and Elite Orthopaedics and hospitality payments from Stryker and Exactech. J.A.A. has received research support from Arthrex, Lima, Orthofix, Zimmer, and the Department of Defense; consulting fees from Bioventus, DJ Orthopedics, Enovis, Globus Medical, Stryker, Encore Medical, Wright Medical, Pacira, Trice Medical, OsteoCentric Technologies, and Zimmer; royalties from DJ Orthopedics, Enovis, Globus Medical, OsteoCentric Technologies, Smith & Nephew, Stryker, Zimmer, Encore Medical, and Integra LifeSciences; and publishing royalties from SLACK, Wolters Kluwer, and Lippincott Williams & Wilkins. He is also a board or committee member for Pacira, Orthobullets, and Shoulder360 and holds stock or stock options in Aevumed, OBERD, Orthobullets, Atreon Orthopedics, OTS Medical, restor3d, and Shoulder JAM. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
An online CME course associated with this article is available for 1 AMA PRA Category 1 Credit™ at https://education.sportsmed.org/Public/Catalog/Home.aspx?CourseSearch=1&Criteria=9&Option=25. In accordance with the standards of the Accreditation Council for Continuing Medical Education (ACCME), it is the policy of The American Orthopaedic Society for Sports Medicine that authors, editors, and planners disclose to the learners all financial relationships during the past 12 months with any commercial interest (A ‘commercial interest’ is any entity producing, marketing, re-selling, or distributing health care goods or services consumed by, or used on, patients). Any and all disclosures are provided in the online journal CME area which is provided to all participants before they actually take the CME activity. In accordance with AOSSM policy, authors, editors, and planners’ participation in this educational activity will be predicated upon timely submission and review of AOSSM disclosure. Noncompliance will result in an author/editor or planner to be stricken from participating in this CME activity.
An online CME course associated with this article is available for 1 AMA PRA Category 1 Credit™ at https://education.sportsmed.org/Public/Catalog/Home.aspx?CourseSearch=1&Criteria=9&Option=25. In accordance with the standards of the Accreditation Council for Continuing Medical Education (ACCME), it is the policy of The American Orthopaedic Society for Sports Medicine that authors, editors, and planners disclose to the learners all financial relationships during the past 12 months with any commercial interest (A ‘commercial interest’ is any entity producing, marketing, re-selling, or distributing health care goods or services consumed by, or used on, patients). Any and all disclosures are provided in the online journal CME area which is provided to all participants before they actually take the CME activity. In accordance with AOSSM policy, authors, editors, and planners’ participation in this educational activity will be predicated upon timely submission and review of AOSSM disclosure. Noncompliance will result in an author/editor or planner to be stricken from participating in this CME activity.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.