
Abstract
Background:
Multiple factors, such as muscle fatty infiltration (FI), tendon collagen content, and collagen arrangement, determine bone-tendon interface (BTI) healing after rotator cuff (RC) repair.
Purpose:
To evaluate the effects of systemic administration of ezetimibe-atorvastatin (EZE/ATZ) combination on muscle FI and tendon collagen density and arrangement in an RC repair rat model.
Study design:
Controlled laboratory study.
Methods:
A total of 26 male Sprague-Dawley rats were randomly divided equally into control and EZE/ATZ groups and subjected to RC tendon repair surgery. Postoperatively, the EZE/ATZ group rats received a combination of EZE (10 mg/kg/d) and ATZ (20 mg/kg/d) for 4 weeks, after which they were sacrificed. Oil Red O staining was used to assess FI in the supraspinatus muscle. The expression of biomarkers related to muscle atrophy and FI was measured using quantitative real-time polymerase chain reaction. For the qualitative and quantitative analysis of FI-related biomarkers, immunohistochemical staining was performed. Biomechanical and histological analyses were performed to evaluate the quality of BTI healing after RC repair.
Results:
The EZE/ATZ group showed significantly lower FI compared with the control group (P < .001) and significantly downregulated expression of gene markers related to muscle atrophy and FI. On histological analysis, the EZE/ATZ group exhibited increased collagen type I contents, consistent collagen arrangement (P = .005), and significantly higher collagen density (P = .003) compared with the control group. Biomechanical analysis of the BTI healing revealed that the EZE/ATZ group had significantly increased ultimate strength (P = .006) compared with the control group.
Conclusion:
Systemic EZE/ATZ administration suppressed supraspinatus FI by downregulating muscle atrophy–related and FI-related genes after RC repair. Additionally, EZE/ATZ use improved collagen biosynthesis, density, and arrangement at the BTI and significantly increased tensile strength.
Clinical Relevance:
The results of the current study strongly advocate the use of EZE/ATZ to improve shoulder function and tendon healing after RC repair.
Rotator cuff (RC) tears cause severe shoulder pain and limit motor function. RC tear is a fairly common disorder of the shoulder joint, affecting more than half of the population aged ≥50 years, with prevalence rates of up to 80% in individuals aged >80 years. 20 More than 250,000 arthroscopic RC repair surgeries are performed each year in the United States alone. 7 However, despite successful surgical intervention, reported rates of inadequate repair and reinjury are unacceptably high, ranging from 25% to as high as 94%.1,9
Although incomplete healing after RC repair is multifactorial, major contributing factors include fatty infiltration (FI) with muscle atrophy and a decrease in collagen content and arrangement of the bone-tendon interface (BTI) due to an inflammatory response.2,13 Muscle atrophy and FI after massive RC tears further cause muscular weakness and contribute to poor healing of the BTI. 30 Muscle degeneration in RC rupture is due to increased expression of proteolytic pathway–activating E3 ligases, such as muscle atrophy F-box protein (Atrogin-1) and muscle RING-finger protein-1 (MuRF-1), and regulatory mechanisms of peroxisome proliferator–activated receptor gamma (PPAR-γ) and CCAAT/enhancer-binding protein alpha (C/EBP-α), 2 transcription factors that promote adipogenesis.2,5 Another important factor is the inflammatory response during the tendon healing process, which may contribute to cell proliferation and differentiation and determines the collagen contents and arrangement in the BTI. Irregular collagen arrangement forms scar tissue at the BTI, which lacks sufficient tensile strength as the normal tendon, causing a retear. Therefore, pharmacological treatments targeted at regulating muscle degeneration–related genes and inflammatory responses, particularly those that prevent supraspinatus atrophy and FI after RC repair and improve collagen synthesis, density, and alignment, may reduce the risk of retear and improve BTI healing clinical practice.
A combination of ezetimibe and atorvastatin (EZE/ATZ) medications is a common treatment for hyperlipidemia that is used either when low-density lipoprotein cholesterol (LDL-C) levels cannot be managed adequately even with high-dose statins or when it is difficult to maintain high-dose statins owing to side effects such as muscle pain, liver damage, or diabetes. The combination of EZE and statins offers several advantages over statin monotherapy, including greater reductions in LDL-C, reduced risk of cardiovascular events, and reduced potential for muscle-related side effects; consequently, it is endorsed as a suitable option for cholesterol management in adults in both the United States and Europe. 14
EZE and ATZ when used in isolation are known for their antiadipogenesis and inflammation regulation effects; however, the effect of a combination of these drugs on improving tendon healing after RC repair is unexplored. Pure EZE has been reported to induce downregulation of PPAR-γ and C/EBP-α in high fat diet–induced dyslipidemia in rats, thereby reducing hepatocyte lipid accumulation. 22 In contrast, pure ATZ has been shown to increase tendon collagen biosynthesis by increasing prostaglandin E2 production during the acute inflammatory response in an RC suture rat model. Thus, a combination of EZE/ATZ may potentially exert antiadipogenic and collagen biosynthesis–increasing effects simultaneously to improve muscle quality and BTI healing after RC repair. In this context, the current study aimed to investigate the histological and biomechanical effects of EZE/ATZ on BTI healing after RC repair. On the basis of the effects of pure ETZ and ATZ, we hypothesized that systemic EZE/ATZ administration would downregulate muscle degeneration–related genes and reduce supraspinatus FI. Additionally, EZE/ATZ may enhance BTI healing and tendon tensile strength by improving collagen content and arrangement. Abbreviations used in this article are defined in Table 1.
Abbreviations Used
Methods
Animal Model
All animal procedures were approved by the Institutional Animal Care and Use Committee of Kyungpook National University (IACUC No. KNU 2023-0210). A total of 26 male Sprague-Dawley rats (aged 12 weeks) were housed in a specific pathogen-free facility in a controlled environment (maintained at 12-h/12-h light/dark cycle; temperature, 22°C ± 2°C) for 1 week to enable acclimatization; food and water were provided ad libitum. The rats were then randomly divided into a control group and an EZE/ATZ group (n = 13 rats each).
The rats underwent an RC suture surgery, 4 weeks after which the right shoulders were used for biomechanical evaluation, including an ultimate failure load evaluation, and the left shoulders were used for histological evaluation. The proximal one-third of the right supraspinatus muscle was used to measure the expression of biomarkers for muscle atrophy and FI, and the proximal one-third of the left supraspinatus muscle was used for Oil Red O staining to assess FI.
Surgical Procedure
Anesthesia was induced using 5% isoflurane delivered with oxygen at 4 L/min, and intraoperative anesthesia was maintained using 2% isoflurane through a nose cone. The rats’ shoulder hair was appropriately shaved to expose the skin and sterilize it. The RC rupture procedure was then performed as per previously described methods. 33 In brief, the scapula was identified, and a 3- to 4-cm incision was made. Next, the deltoid muscle was incised to expose the supraspinatus tendon, which was separated using Metzenbaum scissors; the area between the tendon and bone was incised sharply using a blade (Figure 1).
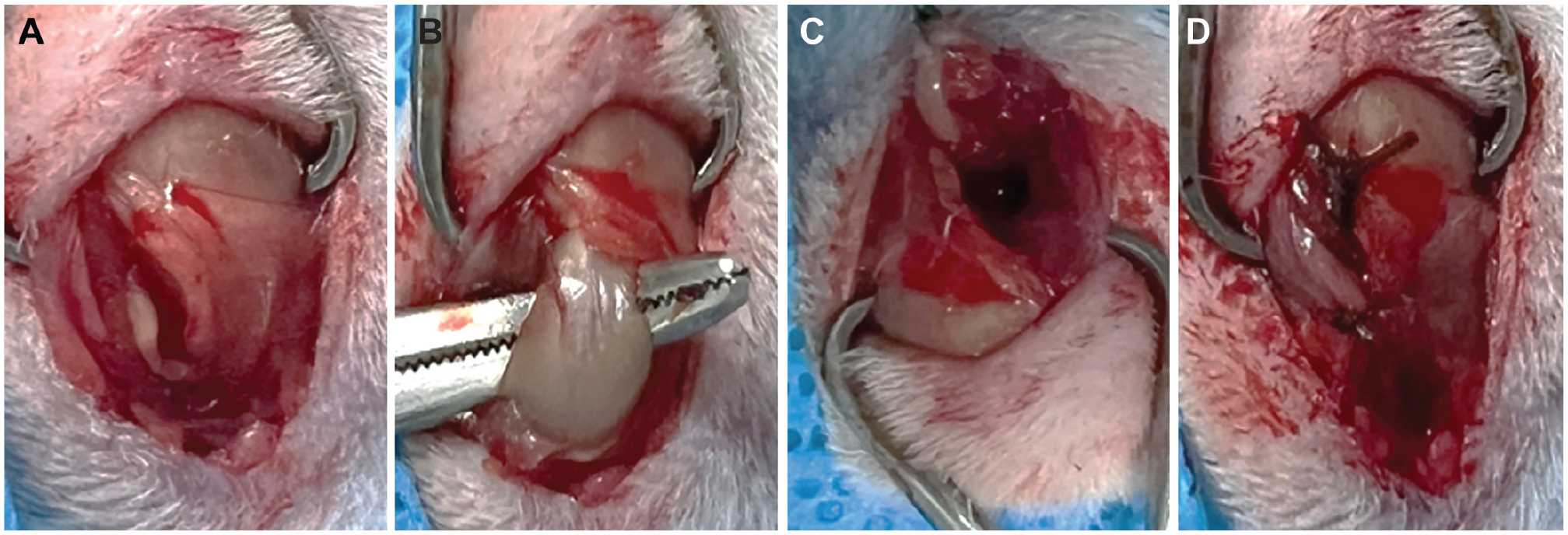
The rotator cuff rupture procedure performed on the rat model. (A) A 3- to 4-cm skin incision was made along the shoulder blades bilaterally to expose the deltoid muscles. (B) In the same direction, a 2- to 3-cm incision was made on the deltoid muscle to expose the supraspinatus tendon. (C) The exposed supraspinatus was fixed using a clamp, and the bone-tendon interface was sharply incised using a knife. (D) The greater tuberosity was widely exposed to create 2 parallel bone tunnels, and the supraspinatus tendon was repaired using a single-row technique using No. 3-0 Ethibond (Ethicon).
The severed supraspinatus tendon was sutured to the tuberosity using Ethibond (Ethicon). After the repair surgery, the EZE/ATZ group received EZE (10 mg/kg/d) plus ATZ (20 mg/kg/d) (Atomibe tablet; Ildong Pharmaceutical) orally for 4 weeks. Rats in the control group received 1 mL of saline solution. For postoperative analgesia, all rats were administered 2 mg/mL of acetaminophen orally for 3 days. Four weeks after the surgery, all mice were sacrificed, and the repaired tendon-bone segment was harvested.
Quantitative Real-Time Polymerase Chain Reaction
Total RNA was isolated from the proximal third of the repaired supraspinatus tendon and then reverse transcribed to cDNA using ReverTra Ace qPCR RT Master Mix (Toyobo). Primer sequences of Atrogin-1, MuRF-1, PPAR-γ, and C/EBP-α genes are presented in Table 2.
Primer Sequences for the Quantitative Real-Time Polymerase Chain Reaction
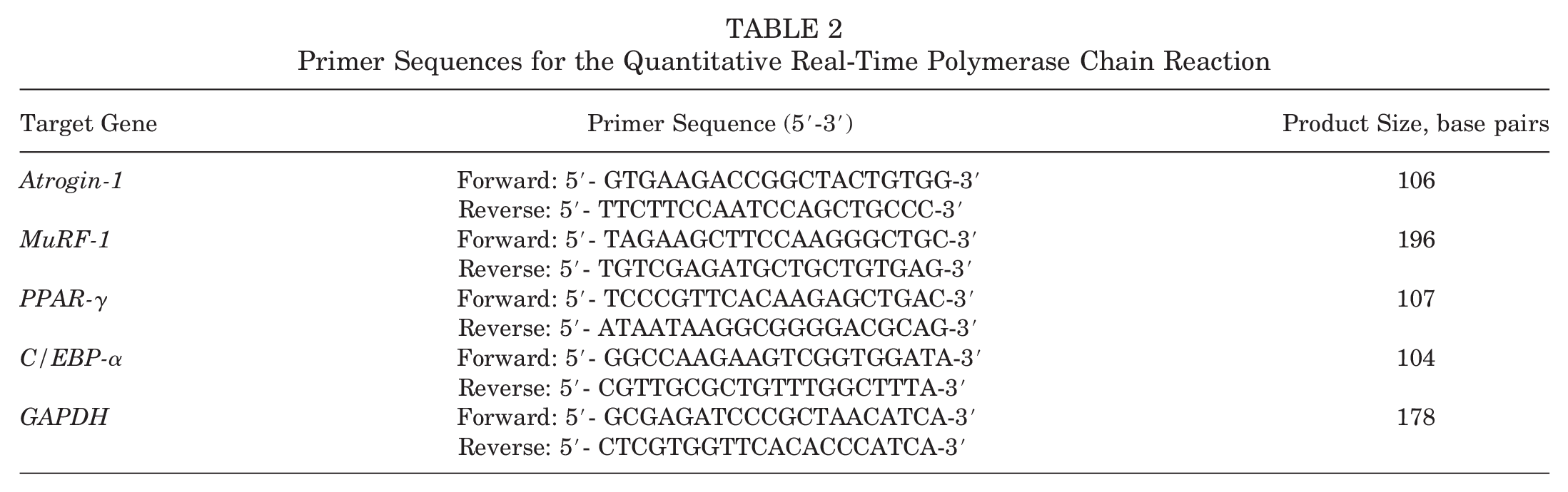
The advanced general-purpose SYBR Green Supermix (Bio-Rad) was used for expression analysis, and the expression of target genes was measured using the CFX96 Touch Real-Time Polymerase Chain Reaction detection system (Bio-Rad). The following polymerase chain reaction temperature conditions were used: 95°C for 30 seconds, 40 cycles of 95°C for 15 seconds, and 60°C for 30 seconds. The expression values of the final target genes were normalized to those of glyceraldehyde 3–phosphate dehydrogenase using the 2−ΔΔ CT method. 34
Oil Red O Staining
Qualitative and quantitative analyses of supraspinatus FI induced by RC tears were conducted using histological visualization of adipocytes and triglycerides performed via Oil Red O staining. Four weeks after surgery, RC supraspinatus tendon-bone segments were harvested from both shoulders of rats. The proximal one-third of the supraspinatus was transversely incised using a knife, and the specimen was frozen at −80°C. Frozen sections were cut into 8- to 10-mm slices, fixed with 10% formalin, washed with tap water followed by washing with 60% isopropanol, stained with lipid (Oil Red O) staining kit (MAK194; Sigma-Aldrich), and then counterstained with hematoxylin. 10 FI was quantified using light microscopy and ImageJ software (public domain JAVA image processing program; US National Institutes of Health).
Biomechanical Analysis
The reattached supraspinatus tendon-bone segment of the right shoulder was appropriately resected. The biomechanical analysis procedures were performed as per a previous study. 33 Briefly, the cross-sectional area (CSA) and width of the middle part of the supraspinatus tendon were measured using the Digimatic Micrometer (MDC-25SB; Mitutoyo). The collected samples were fixed in the universal testing machine (OTT-03; Oriental TM) along the anatomic direction, and a 20-kg load cell was used to determine failure, failure mode (insertion rupture or intermediate material failure), and breakage. The ultimate strength parameters were measured at a load of 10 mm/min. Interstitial tears suggested relatively weak BTI healing, and intermediate substance tears suggested strong BTI healing.
Histological Analysis
All left RC supraspinatus tendon-bone portion specimens collected from both groups were histologically assessed to quantify the degree of BTI regeneration. The collected samples were fixed in 10% neutral buffered formalin (pH 7.4) and embedded in paraffin. Paraffin blocks were cut into 4 µm–thick sections, deparaffinized, and rehydrated. 32 Randomly selected sample slides were stained with hematoxylin-eosin and Masson trichrome. Two investigators (J.P.Y. and S.J.P.), who were blinded to the group identity, performed the analysis. Each tissue slide was photographed under a microscope (Leica DM IL LED; Leica Microsystems) using an imaging system equipped with LAS software (Version 4.8; Leica Microsystems). Whole slides were used to assess areas with increased cellularity and vascularity, the proportion of collagen fibers, and the level of maturation in the BTI structures. 17
As per previous studies, histopathology scores were based on (1) cell morphology, (2) collagen arrangement, (3) collagen density, (4) vascularity, and (5) cellularity. 12 For quantitative analysis, cell morphology is traditionally defined based on the shape and size of the nucleus and the cytoplasmic area. Hypercellularity was defined as the presence of >30 nuclei per field of view, whereas hypocellularity was defined as <20 nuclei per field of view. Collagen arrangements were defined as segregation and loss of boundaries within collagen fiber bundles, overall tissue expansion, and disruption of normal polarization patterns. Vascularity was evaluated by examining the area occupied by prominent blood vessels flowing between the fiber bundles. 12 All specimens were independently scored by 2 pathologists (S.J.P. and D.H.K., each with at least 10 years of experience) who were blinded to group allocation to minimize observer error.
Immunohistochemistry
To evaluate the reduction of supraspinatus PPAR-γ protein contents and BTI regenerative activity, we used immunohistochemistry to assess the amount of PPAR-γ and collagen type I (collagen I). The detailed method for immunohistochemistry is similar to that described in a previous study. 19 Briefly, all samples were treated with 10% normal serum and 1% bovine serum albumin (BSA) in Tris-buffered saline (TBS) to prevent the binding of nonspecific antibodies. The sections were then treated with primary antibodies diluted in TBS with 1% BSA. For detection of primary antibodies, enzyme-linked secondary antibodies were applied to the slides and diluted in TBS with 1% BSA. Finally, the images were evaluated using a light microscope and ImageJ software.
Statistical Analysis
The preliminary power analysis was based on a previous study evaluating RC healing in rats after pharmacological intervention.18,21,35 Using G*Power 3.1.9.7 (Heinrich-Heine-Universität Düsseldorf), we calculated the minimum sample numbers for each of the FI (effect size, 2.20; sample size, 7 shoulders), 11 molecular expression (effect size, 2.70; sample size, 5 shoulders), 18 histology (effect size, 1.69; sample size, 11 shoulders), 21 and biomechanical (effect size, 1.81; sample size, 10 shoulders) 35 tests using a power of 0.80 and an alpha error probability of <.05. Therefore, to check for unexpected variability, we randomly divided a total of 26 rats into an EZE/ATZ group and a control group, with 13 rats in each group.
All statistical analyses were performed using SPSS Statistics for Windows (Version 12.0; SPSS Inc); P values of <.05 were considered statistically significant. Data are presented as mean and standard deviation. The differences in FI, biomechanics, and histological tendon healing among the 2 groups were analyzed using independent-samples t tests.
Results
EZE/ATZ Significantly Suppressed Supraspinatus FI After RC Tear
FI in the supraspinatus muscle was confirmed in both groups at 4 weeks after repair. After 4 weeks of treatment, the CSA (P < .001) and wet weight (P < .001) of the supraspinatus muscle in the EZE/ATZ group were significantly suppressed compared with those in the control group (Figure 2).
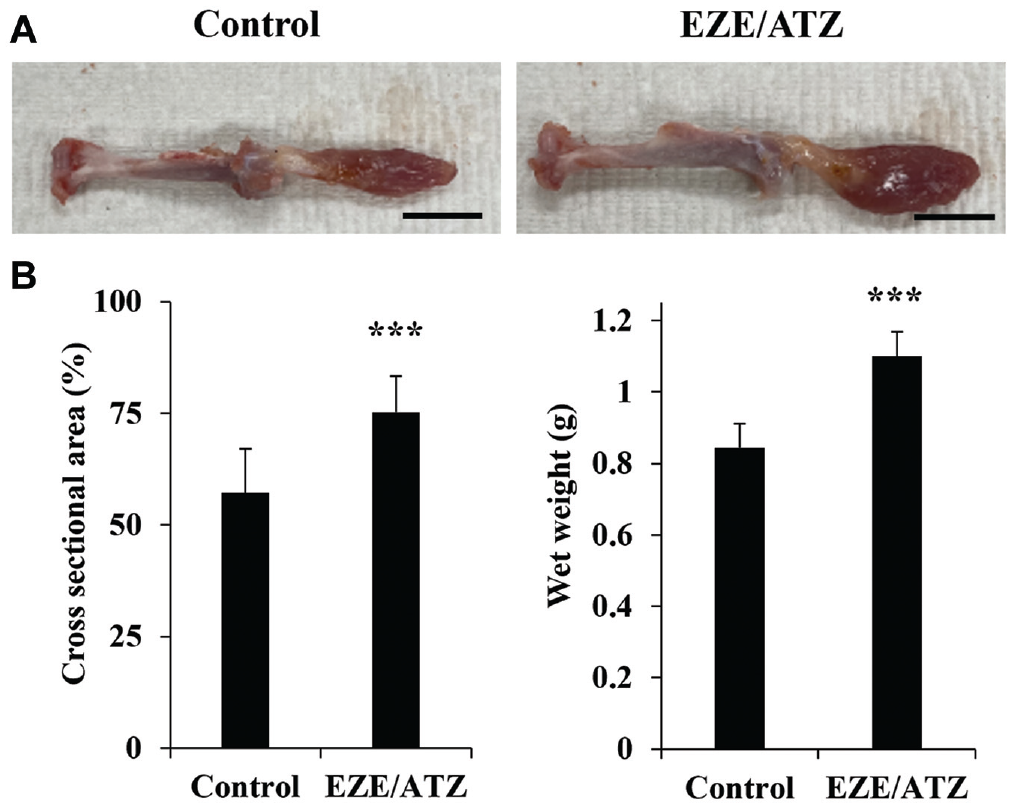
Cross-sectional area (CSA) and wet weight of the supraspinatus muscle at 4 weeks after rotator cuff rupture. (A) Images of collected bone-tendon-muscle samples from the control and ezetimibe/atorvastatin (EZE/ATZ) groups. (B) CSA quantitative value and sample wet weight of the supraspinatus. CSA measurements were calculated using ImageJ software using Oil Red O images. Wet weight was measured at the time of sample collection after individual euthanasia. Error bars represent the standard deviation (n = 13). Bar, 10 mm. ***P < .001.
Supraspinatus FI was mainly noted at the muscle-tendon junction and in the central rather than in the distal part of the muscle. Quantitative analysis showed that the EZE/ATZ group showed significantly lower FI (1.49% ± 1.54%) compared with the control group (16.27% ± 4.92%; P < .001) (Figure 3). In the immunohistochemistry staining analysis of PPAR-γ, a representative molecular marker of FI, the supraspinatus marker protein contents of the EZE/ATZ-treated group were significantly suppressed (P = .032) compared with those of the control group (Figure 3). These results suggest that administration of EZE/ATZ after tendon repair can prevent RC supraspinatus atrophy and FI.
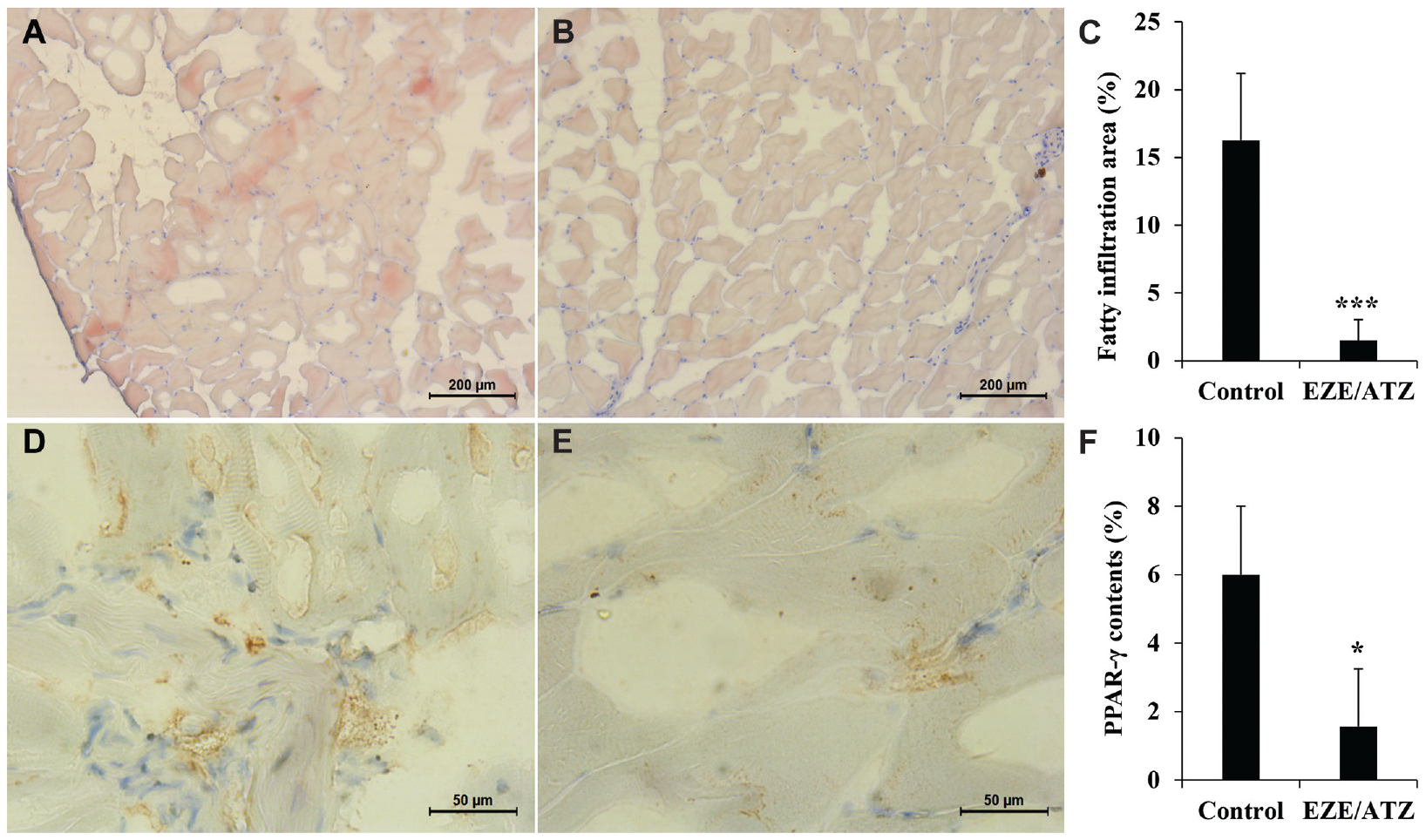
Oil Red O and immunohistochemistry staining of the supraspinatus. The supraspinatus muscle was collected 4 weeks after rotator cuff repair surgery, and fatty infiltration (FI) of the (A) control and (B) ezetimibe/atorvastatin (EZE/ATZ) groups was qualitatively analyzed using Oil Red O staining. (C) Quantitative muscle FI analyzed using ImageJ (n = 13). Immunohistochemistry staining images of peroxisome proliferator–activated receptor gamma (PPAR-γ) in (D) control group and (E) EZE/ATZ group. (F) Quantitative analysis of PPAR-γ protein contents (n = 8). *P < .05. ***P < .001. Error bars represent the standard deviation.
EZE/ATZ Suppressed the Expression of Atrogin-1, MuRF-1, PPAR-γ, and C/EBP-α
At 4 weeks after repair, the expressions of Atrogin-1, MuRF-1, PPAR-γ, and C/EBP-α were significantly lower in the EZE/ATZ group than in the control group (P < .001, P < .001, P < .001, and P < .01, respectively) (Figure 4), indicating a possible FI-inhibitory effect of EZE/ATZ induced via downregulation of genes related to muscle atrophy and FI.
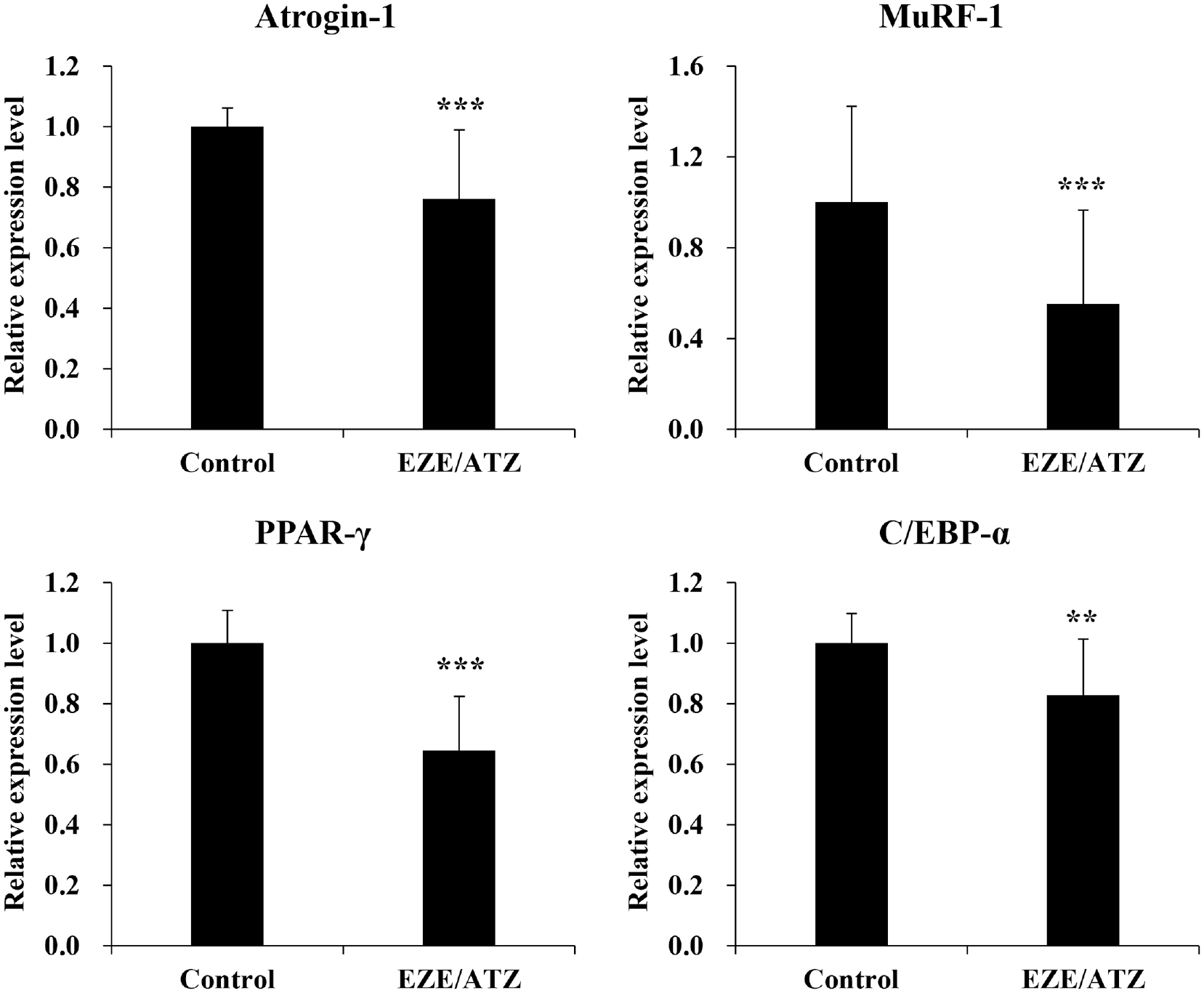
Mean expression level of gene markers related to muscle atrophy (Atrogin-1 and MuRF-1) and fatty infiltration (PPAR-γ and C/EBP-α) in rat models of rotator cuff repair. The marker expression levels were confirmed via quantitative real-time polymerase chain reaction in the proximal part of the supraspinatus muscle. Expression values of each gene were normalized by GAPDH. Error bars represent the standard deviation (n = 13). **P < .01.***P < .001. Atrogin-1, muscle atrophy F-box protein; C/EBP-α, CCAAT/enhancer-binding protein alpha; EZE/ATZ, ezetimibe/atorvastatin; GAPDH, glyceraldehyde 3-phosphate dehydrogenase; MuRF-1, muscle RING-finger protein-1; PPAR-γ, peroxisome proliferator–activated receptor gamma.
EZE/ATZ Enhanced the Collagen Density and Arrangement in the BTI
On histological scoring of the BTI at 4 weeks after surgery, the EZE/ATZ group exhibited consistently significant collagen arrangement (P = .005) and higher collagen density (P = .003) compared with the control group (Table 3). In contrast, no significant between-group differences were observed for cell morphology (P = .695), cellularity (P = .263), and vascularity (P = .379).
Histological Scoring of the Bone-Tendon Interface 4 Weeks After Surgery a
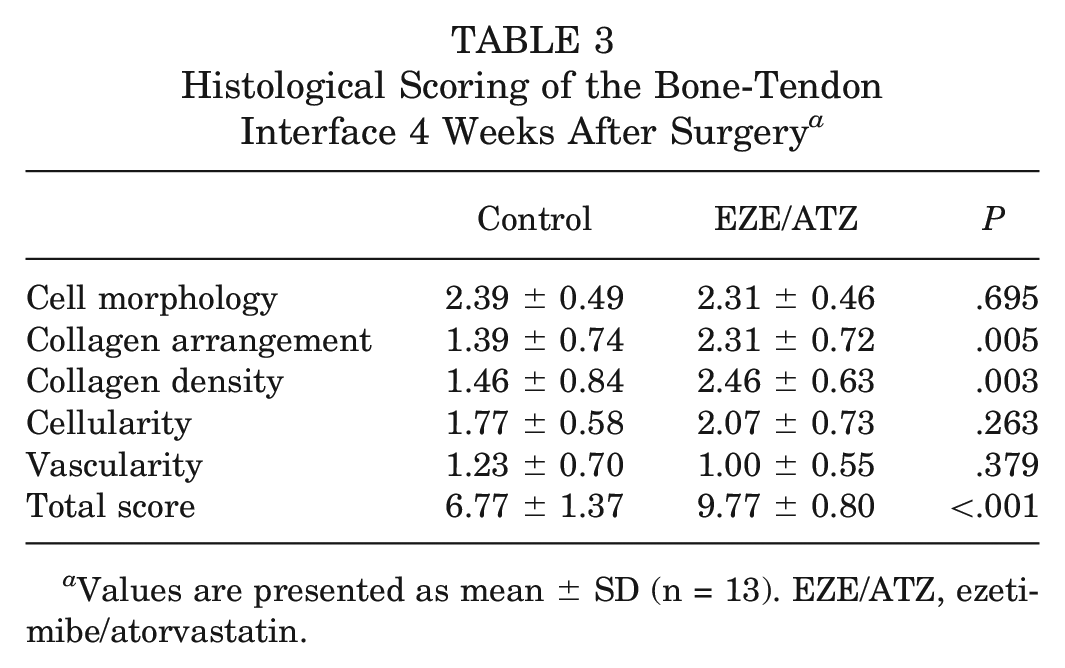
Values are presented as mean ± SD (n = 13). EZE/ATZ, ezetimibe/atorvastatin.
Due to the consistent collagen arrangement (P = .005) and higher collagen density (P = .003), the total score (P < .001) was also significantly higher for the EZE/ATZ group than for the control group. Additionally, the ratio of collagen I in the supraspinatus of the EZE/ATZ group (12.53 ± 1.83) was significantly higher than that of the control group (2.31 ± 1.16) (P < .001).
These findings suggested that EZE/ATZ significantly improved healing in the RC supraspinatus and BTI compared with the control group (Figure 5).
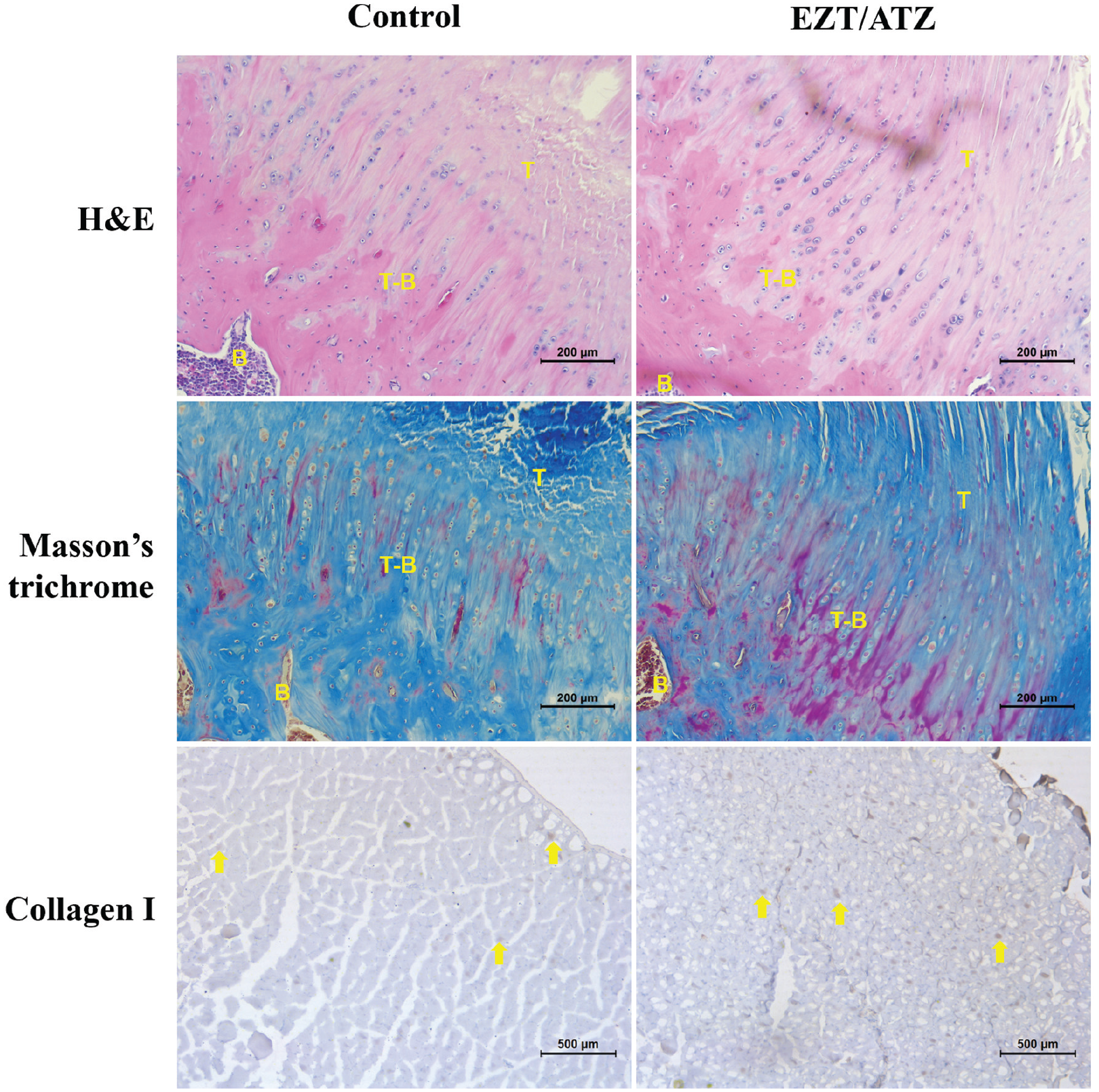
Histological analysis of the bone-tendon interface (BTI) and the proximal supraspinatus muscle treated with statins. BTI sections were harvested from the left shoulder of the rat 4 weeks after rotator cuff repair. These samples were evaluated for collagen arrangement, density, vascularity, and cellularity using hematoxylin and eosin (H&E) and Masson trichrome staining (n = 13). Collagen type I contents of the supraspinatus were seen using immunohistochemistry staining 4 weeks after surgery (n = 11). Stained slides were imaged under an optical microscope (original magnification, ×50). B, bone; EZT/ATZ, ezetimibe/atorvastatin; T, tendon; T-B, tendon-bone interface. Yellow arrows represent collagen type I proteins.
EZE/ATZ Improved the Ultimate Mechanical Strength of the BTI After RC Repair
On biomechanical analysis of BTI healing, the EZE/ATZ group showed significantly increased load to failure (P = .040) and ultimate strength (P = .006) compared with the control group (Figure 6). However, no significant differences were found between the 2 groups in terms of CSA (P = .958) and elongation (P = .686), suggesting that systemic administration of EZE/ATZ can improve collagen density and arrangement at BTI, thereby significantly enhancing tensile strength.
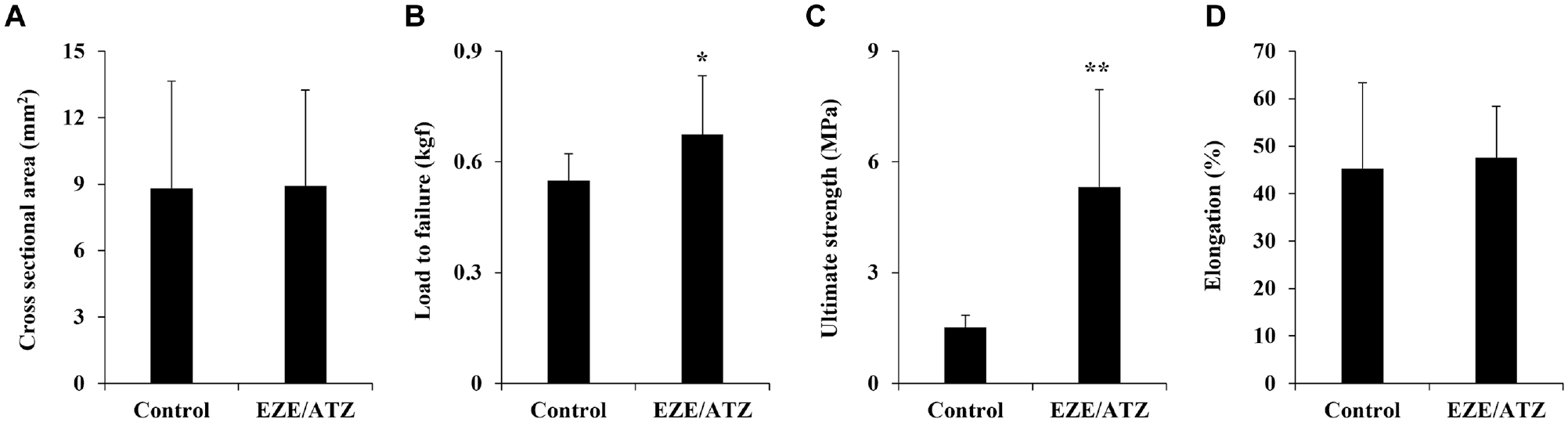
Biomechanical analysis of the bone-tendon interface treated with statins. Four weeks after rotator cuff repair, the bone-tendon segment was harvested from the right shoulder of the rat. The collected samples were fixed in the universal testing machine along the anatomic direction, and the failure rate was measured at a load of 10 mm/min using a 20-kg load cell. The outcome variables were (A) cross-sectional area, (B) load to failure, (C) ultimate strength, and (D) elongation. EZE/ATZ, ezetimibe/atorvastatin. Error bars represent the standard deviation (n = 13). *P < .05. **P < .01.
For quantitative analysis of unidirectional arrangement of the BTI collagen fiber, picrosirius red staining images were analyzed using FiberFit software.15,27 Compared with the control group, the EZE/ATZ group showed a narrower histogram of fiber angles at BTI (Figure 7, A and B) and had a quantitatively higher collagen alignment index, an indicator of collagen fiber unidirectional alignment (Figure 7C).
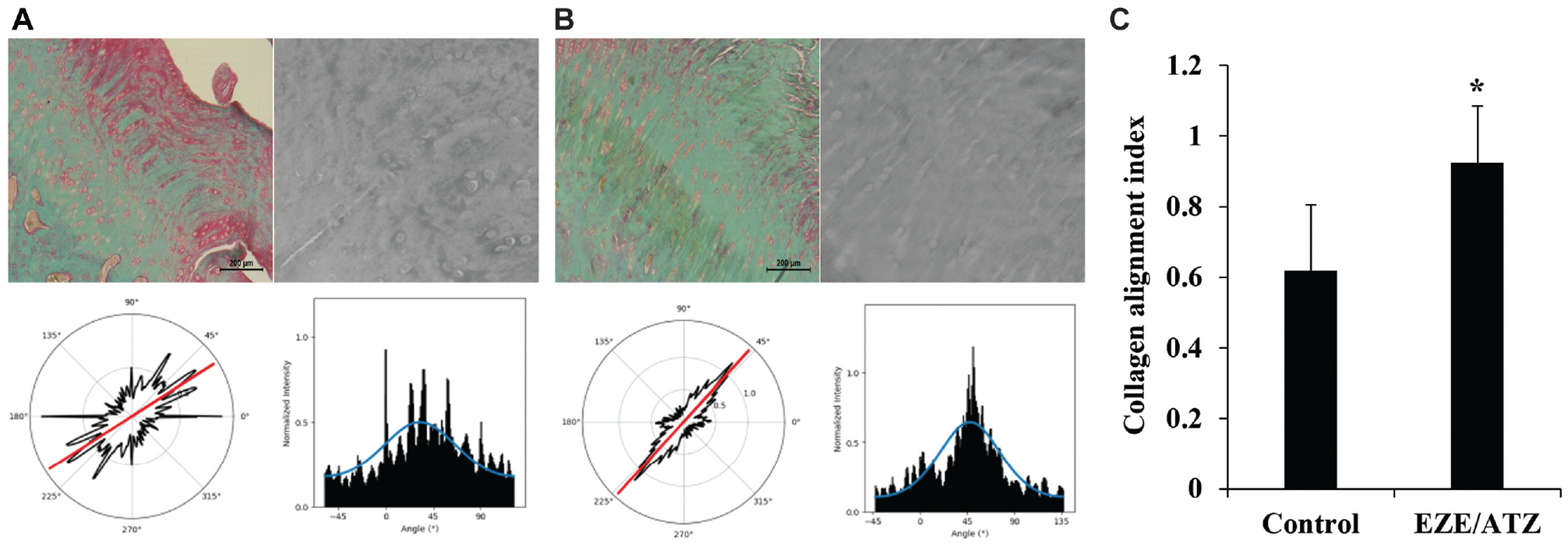
Qualitative and quantitative analysis of bone-tendon interface collagen fiber orientation using FiberFit software. Picrosirius red images of (A) control and (B) ezetimibe/atorvastatin (EZE/ATZ) groups and histograms of fiber angles analyzed using FiberFit software. (C) Quantitative analysis of collagen alignment index. The collagen alignment index represents the dispersion of fibers and has no units. Lower values are more disordered, whereas higher values indicate more aligned collagen. Error bars represent the standard deviation (n = 13). *P < .05.
Discussion
We found that the combination of EZE/ATZ was effective in suppressing FI in the supraspinatus and improving BTI healing after RC repair. The inhibitory effect of EZE/ATZ on fat invasion was evident both at the physical level (minimal presence of adipose tissue in the muscle FI analysis) and at the molecular level (suppressed expression levels of PPAR-γ and C/EBP-α). This is further corroborated by the decreased expression of muscle atrophy–related markers, Atrogin-1 and MuRF-1. EZE/ATZ also improved collagen arrangement and density within the BTI. These structural changes likely contributed to the enhanced ultimate strength of the tendon-bone segment, as determined via biomechanical comparisons.
The hyperlipidemia treatment guidelines of the Understanding Statin Use in America and Gaps in Education recommend the use of lipid-lowering drugs to lower LDL-C to <55 mg/dL in patients at high risk of cardiovascular disease. 6 High-dose statins are often prescribed to achieve this goal; however, they are associated with an increased risk of myopathy, a muscle-related side effect. 23 Lately, practice has shifted toward reducing the dose of pure statins in the treatment of dyslipidemia and using them in combination with EZE to alleviate muscle-related side effects. 24 In patients with cardiovascular diseases who are intolerant to pure statins, a combined administration of EZE with statins serves as an alternative to high-dose statin therapy; this approach alleviates the side effects while maintaining the lipid-lowering effect. In our study, the EZE/ATZ combination therapy resulted in the inhibition of FI in the muscle, increased expression of collagen I, and improved collagen density and arrangement during tendon remodeling, supporting the use of EZE/ATZ over pure high-dose statins.
Muscle atrophy and FI are common pathological changes after massive RC rupture. The outcomes of our study aligned with our initial hypothesis, demonstrating the favorable effects of EZE/ATZ on muscle degeneration and BTI healing. EZE/ATZ treatment led to a notable reduction in the expression of adipogenic markers, such as PPAR-γ and C/EBP-α, which was consistent with the observed decrease in FI in the supraspinatus tissue visualized via Oil Red O staining. The underlying molecular mechanism may involve the EZE-induced inhibition of the mammalian target of rapamycin complex 1 (mTORC-1) signaling by activating adenosine monophosphate-activated protein kinase (AMPK), leading to the downregulation of adipogenesis-related genes. 15 However, unlike EZE, the FI-inhibitory effect of ATZ is unknown. A previous clinical study has shown no differences in rupture rate and FI after RC repair in patients with hyperlipidemia treated with pure statins. 1 Surely, the 2 drugs may have a synergistic effect in regulating the relevant markers, but further research is warranted to verify these results. Therefore, systemic EZE/ATZ administration after RC repair probably suppresses muscle FI by downregulating adipogenesis-related genes via the EZE-induced AMPK/mTORC-1 signaling.
In a previous animal study, standard-dose ATZ was found to enhance tendon healing by stimulating proinflammatory cyclooxygenase-2/prostaglandin E2 mediators during the acute inflammatory phase after tendon injury. 9 Stimulation of the inflammatory response can accelerate the tendon repair process by encouraging angiogenesis and collagen synthesis. 13 Furthermore, in vitro experiments confirmed that standard-dose ATZ increased the proliferation, adhesion, and migration of tendon cells, which are associated with improved biomechanical properties. 9 This was also observed in our study in the form of increased collagen content and improved collagen density and alignment via systemic administration of EZE/ATZ containing standard-dose ATZ. These improvements in collagen density and alignment may help increase the postoperative shoulder range of motion and reduce the risk of retear at the BTI.
The unacceptably high rates of retear rate at the BTI in the RC tears remain a clinical challenge. Healing of the RC tendon is a complex process that requires effective management via multiple therapeutic targets, such as controlling inflammation, controlling cell proliferation, and strengthening collagen arrays. There is concern that the use of nonsteroidal anti-inflammatory drugs to relieve pain and inflammation after tendon repair may have detrimental effects on BTI healing.4,8,26 Additionally, the effectiveness of platelet-rich plasma and stem cell therapy for promoting cell proliferation and high-quality tendon remodeling has not yet been fully established.3,25,29,31 According to previous research, ATZ has been shown to improve tendon healing by modulating the acute inflammatory response after tendon injury. 9 In the current study, our findings show that EZE/ATZ offers promising results in improving BTI healing via multiple steps, namely regulating genes related to muscle atrophy and FI and enhancing collagen density and arrangement after cell proliferation. These findings strongly advocate the use of EZE/ATZ in patients who have RC rupture and hyperlipidemia and highlight the importance of developing treatments targeting different aspects of the disease.
Several limitations to this study must be acknowledged. First, the effect of EZE/ATZ in lowering LDL-C in the body may be beneficial for patients at risk for atherosclerotic cardiovascular disease but may potentially cause myopathy and tendon complications depending on the type and dose of statin used. 16 Further preclinical and clinical studies are needed to characterize the relationship between the lipid-lowering effects of statins and RC disease. Second, hyperlipidemia is a known risk factor for RC rupture and BTI healing. 28 Therefore, further investigation is needed to determine how systemic administration of EZE/ATZ affects the BTI healing mechanism after RC repair in patients with hyperlipidemia. Third, the rat model of acute RC rupture used in this study does not truly replicate the chronic degenerative RC rupture commonly observed in humans. RC ruptures in humans are often associated with intrinsic degenerative changes in the torn tendon, tendon contracture, and osteoporosis of the shoulder tuberosity. Nonetheless, the postoperative healing process is generally similar for both acute and chronic tears. 9
Conclusion
Despite the limitations, the current study provides important insight into the healing mechanisms and safety of systemic EZE/ATZ administration after RC surgery. On the basis of these results, we can suggest that the combination of statins and EZE may inhibit FI in RC tendons and improve tendon healing. These results may help researchers design clinical trials using this combination therapy in patients with hyperlipidemia who have RC rupture or other tendon diseases.
Footnotes
Submitted January 25, 2024; accepted September 16, 2024.
One or more of the authors has declared the following potential conflict of interest or source of funding: This work was supported by a grant from the National Research Foundation of Korea (NRF), funded by the Republic of Korea government (MSIT) (NRF-2022R1A2C1005374). This research was supported by a grant from the Korea Health Technology R&D Project through the Korea Health Industry Development Institute (KHIDI), funded by the Ministry of Health & Welfare, Republic of Korea (grant No. HR22C1832). AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto. All animal procedures were approved by the Institutional Animal Care and Use Committee of Kyungpook National University, Daegu, Republic of Korea (IACUC No. KNU 2023-0210).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.