
Abstract
Background:
Asymmetric landing kinetics 6 months after anterior cruciate ligament reconstruction (ACLR) are associated with higher risk of second anterior cruciate ligament injury. Little is known about landing kinetics after ACLR with an all–soft tissue quadriceps tendon (QT) autograft despite its increasingly common use in young, active patients.
Purpose/Hypothesis:
The purpose of this study was to compare landing kinetics during a bilateral drop vertical jump (DVJ) 6 months after ACLR in participants who had undergone primary ACLR with a QT or bone–patellar tendon–bone (BTB) autograft. The hypothesis was that patients with a QT autograft will experience more asymmetry during a bilateral DVJ than patients with a BTB autograft 6 months after ACLR. In addition, greater impact force asymmetry will be associated with worse patient-reported outcome measures.
Study Design:
Controlled laboratory study.
Methods:
Participants who underwent primary unilateral ACLR with a QT or BTB autograft between May 2022 and December 2023 were prospectively recruited to undergo DVJ assessment and patient-reported outcome measures 6 months after ACLR. DVJ assessment was completed using force-sensing insoles. Peak impact force, average loading rate, and impulse data were collected at 100 Hz.
Results:
Forty-four participants (22 BTB, 22 QT) completed DVJ assessment and International Knee Documentation Committee (IKDC) and Anterior Cruciate Ligament–Return to Sport After Injury (ACL-RSI) surveys at 6 ± 1 months after ACLR. Graft source groups did not differ by age (P = .884), sex (P = .531), mass (P = .872), height (P = .572), months since surgery (P = .683), or lateral (P = .637) or medial (P = .416) meniscal tear treatment rate. On average, participants with a QT autograft demonstrated 26.2% greater contralateral limb peak impact force (P = .004), 18.4% lower peak impact force limb symmetry index (P = .009), 18.5% lower involved limb impulse (P < .001), and 15.1% lower impulse limb symmetry index (P < .001) when compared with participants with a BTB autograft. Graft source groups did not differ in IKDC score (P = .333) or ACL-RSI score (P = .070). Neither IKDC nor ACL-RSI score was strongly associated with any kinetic variables.
Conclusion/Clinical Relevance:
Participants with a QT autograft exhibit greater asymmetry in landing kinetics when compared with participants with a BTB autograft 6 months after ACLR, and landing kinetics were not associated with IKDC or ACL-RSI score.
Keywords
After anterior cruciate ligament (ACL) injury, surgical reconstruction aims to reduce knee joint laxity, restore normal knee function, and prevent secondary injury to the meniscus and articular cartilage with the goal of return to preinjury levels of activity. 8 However, up to 30% of patients who undergo ACL reconstruction (ACLR) experience a contralateral or ipsilateral ACL injury within 2 years of the index ACLR.5,28,29 As the rate of ACLR has been increasing, clinicians have worked to develop a variety of assessments to evaluate readiness for return to sport (RTS) and risk of second ACL injury.9,10,22 Unfortunately, the assessments that now make up standard RTS criteria do not consistently or accurately identify athletes who are at high risk of second ACL injury. 30 This discrepancy may be a result of the current battery of assessments, which includes tasks that (1) require subjective judgment by the clinician, as objective measurements can be technologically challenging and cost prohibitive, or (2) are objective but do not meaningfully predict risk of second injury. 24 There has recently been increased interest in the feasibility of objectively assessing limb kinetics during tasks that correlate with second ACL injury, such as the drop vertical jump (DVJ).18,21 It is crucial to learn how to implement tasks such as this in the clinical environment to better understand the risk factors of second ACL injury, how to easily assess patients for these risk factors, and how surgical decision-making may help reduce this risk.
Graft choice during ACLR affects postoperative rehabilitation and clinical outcomes. Patients who receive a hamstring tendon autograft, bone–patellar tendon–bone (BTB) autograft, and quadriceps tendon (QT) autograft experience different donor site morbidity profiles, strength recovery timelines, and joint mechanics during loading tasks after primary ACLR.6,37 For example, during a bilateral DVJ, a common movement that exposes athletes to high risk of ACL injury, 21 athletes who undergo ACLR with a BTB autograft land with greater vertical ground-reaction force in the involved limb than those with a hamstring tendon autograft. 43 This difference may be because the BTB graft harvest disrupts the extensor mechanism,25,43 which has been shown to cause increased anterior knee pain and decreased quadriceps strength.6,37 Importantly, post-ACLR DVJ asymmetries appear to be related to differences in quadriceps strength,12,16,17,38 and recent findings have shown that quadriceps strength is inferior in patients with a QT autograft during post-ACLR rehabilitation. 14 However, little is known about landing kinetics after ACLR with a QT autograft despite its increasing use in the treatment of young, physically active patients. 3
Previous research indicates that young athletes who exhibit >90% limb symmetry index (LSI) in knee-loading variables such as vertical ground-reaction force during a bilateral DVJ are more likely to pass RTS testing. 21 In addition, greater between-limb asymmetry in knee extensor moment before RTS clearance is associated with an elevated risk of second ACL injury after RTS. 31 Six months after ACLR, this landing asymmetry is common and associated with future cartilage degeneration and meniscal abnormalities.40,41 However, measuring extensor moment requires 3-dimensional motion analysis, an approach that is not translatable to the clinical rehabilitation setting owing to prohibitive costs and its advanced training requirements. 23 Loadsol force-sensing insoles are an emerging technology that utilizes an in-shoe insole synced to a mobile application to collect real-time impact forces, which are analogous to ground-reaction forces, 39 without advanced processing or training. Importantly, force-sensing insoles have been validated against traditional force plates for landing tasks in a post-ACLR population. 23 Therefore, this technology may allow rehabilitation clinicians to objectively assess biomechanical asymmetries during landing to provide real-time feedback to patients, advance RTS testing, and assess risk for future injury.
The purpose of this study was to compare landing kinetics during a bilateral DVJ 6 months after ACLR in participants who had undergone primary ACLR with a QT or BTB autograft. We hypothesized that patients with a QT autograft would exhibit more limb-loading asymmetries than patients with a BTB autograft during a bilateral DVJ 6 months after ACLR. In addition, we hypothesized that, in line with previous findings, 35 greater asymmetry in impact forces would be associated with worse patient-reported outcome measures (PROMs).
Methods
The current study was a multisite cross-sectional subanalysis incorporating data from 2 ongoing longitudinal studies investigating lower extremity biomechanics after ACLR. Both studies were approved by their institutional review boards (Western-Copernicus Group Institutional Review Board 20216925 and University of Virginia Institutional Review Board 220225). All adult participants provided written informed consent before participation. All minor participants provided written assent and 1 parent or guardian provided written consent before participation.
Participants
Participants were recruited from 2 sports medicine practices 6 ± 1 months after ACLR. Recruited patients were between the ages of 13 and 40 years and underwent ACLR with a QT or BTB autograft between May 2022 and December 2023 (Figure 1). Participants were not randomized into graft groups, and graft type was determined through a joint decision-making process between surgeons and their patients. Participants were excluded if they (1) had evidence of radiographic osteoarthritis (Kellgren-Lawrence grade >1); (2) had a history of ipsilateral or contralateral knee surgery; (3) had a lower extremity fracture at the time of ACL injury; (4) had inflammatory arthritis, immunodeficiency, or articular cartilage damage greater than 3A; or (5) underwent multiligamentous reconstruction or subtotal meniscectomy at the time of ACLR. Postoperative rehabilitation was not standardized among patients, and patients had the ability to attend physical therapy at the clinic of their choosing; however, standard protocols were provided by surgeons to guide rehabilitation.
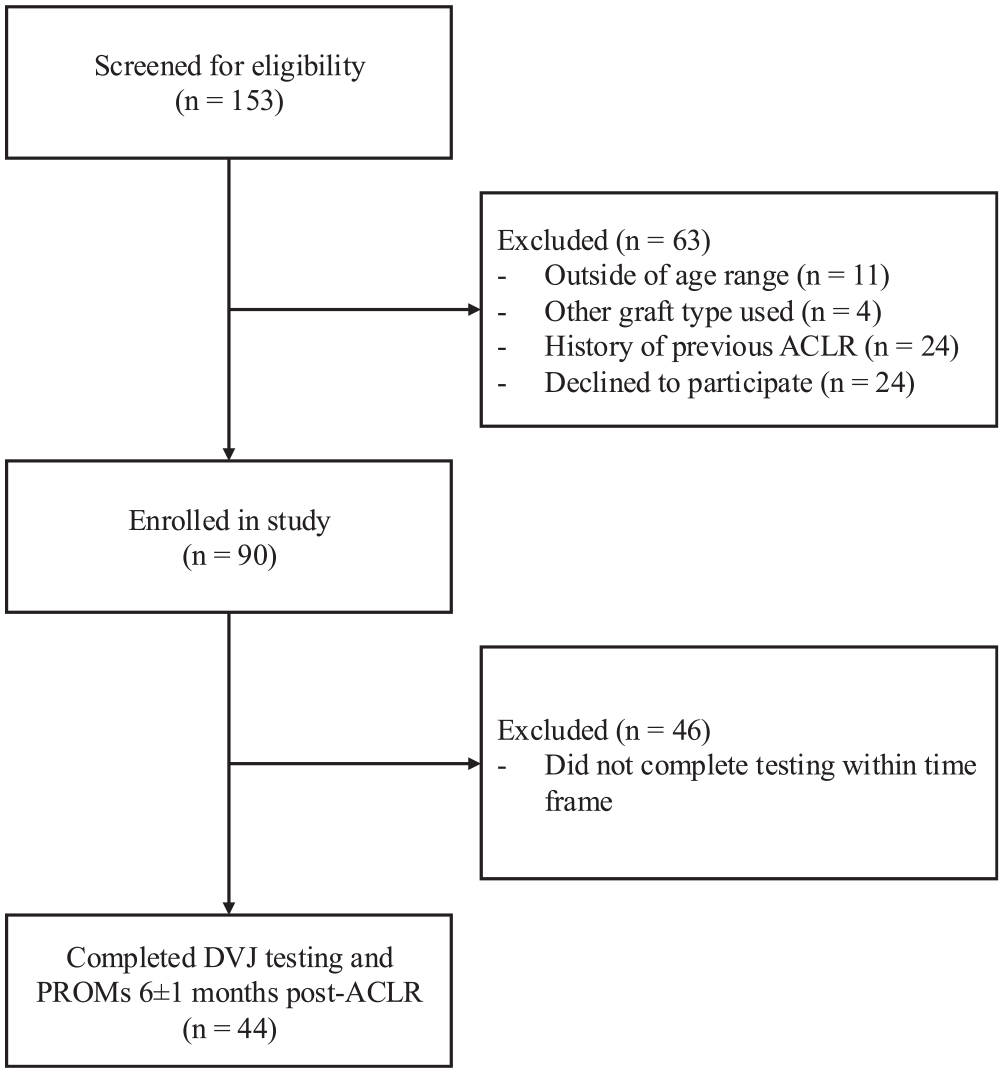
STROBE flowchart depicting screening, inclusion, and exclusion of participants. ACLR, anterior cruciate ligament reconstruction; DVJ, drop vertical jump; PROM, patient-reported outcome measure.
Surgical Technique
ACLR was performed by 1 of 10 fellowship-trained surgeons at 2 institutions. For the QT harvest, a 3- to 4-cm longitudinal incision was made, ending at the superior pole of the patella. Either a 9- or 10-mm double-bladed knife (Arthrex) was used to harvest the graft in line with the longest aspect of the tendon. The tendon was then excised off the superior pole of the patella with a No. 15 scalpel and dissected proximally. Depending on surgeon preference, either a partial- or full-thickness graft was obtained. A QT cutter (Arthrex) was then used to complete the harvest. The goal was to obtain a graft length of at least 65 mm and a tendon diameter between 9 and 10 mm. The tendon defect was closed with the knee in flexion in all cases with an absorbable suture.
For the patellar tendon harvest, an 8-cm incision was made along the medial aspect of the patellar tendon. Subcutaneous dissection was carried down to the paratenon, which was incised with a No. 15 scalpel and dissected medially and laterally to expose the underlying patellar tendon. The central 10 mm of the patellar tendon was then incised with a fresh No. 10 scalpel. A sagittal saw and curved osteotome were used to harvest a bone block 10 × 20 mm on the patellar and tibial sides. The harvest sites were bone grafted with autogenous bone, and the peritenon was closed with an absorbable suture.
After diagnostic arthroscopy, any meniscal pathology was treated. The femoral and tibial tunnels were drilled independently. After graft passage, femoral and tibial fixation was performed according to surgeon preference. In all cases, the patient’s limb was placed in a hinged knee brace locked in extension before being woken from anesthesia.
Patient-Reported Outcome Measures
Before the jump-landing assessment, participants completed 2 PROMs—the International Knee Documentation Committee (IKDC) 15 and the ACL–Return to Sport After Injury (ACL-RSI) 42 —to assess knee-related function and psychological readiness for RTS via an online survey platform (REDCap). The IKDC 15 is an 18-item form scored from 0 to 100, with higher scores representing fewer symptoms, greater knee function, and higher sport-related activity. The IKDC has been validated to be responsive to various knee conditions, and normative data have been established by sex and age. 1 The ACL-RSI 42 is a 12-item scale scored from 0 to 100, with higher scores representing a greater psychological readiness to RTS after ACL injury. To date, it is the only scale developed for this purpose, and the ACL-RSI score can predict RTS outcomes.2,19
Limb-Loading Assessments
Participants completed a bilateral jump-landing assessment in a rehabilitation clinic under the supervision of a study team member. Before the landing assessment began, the force-sensing insoles were inserted into the participant’s shoes and calibrated using the standardized protocol described by Renner et al. 36 After calibration, the participant was weighed (newtons) using the force-sensing insoles to ensure that the sensors were correctly assessing the patient’s weight. Impact force data were collected at 100 Hz.
Participants were allowed to practice the jump-landing task before data collection and were encouraged to rest before trials in which landing forces were collected. After participants indicated that they were ready for data collection, they were asked to stand on top of a 30-cm box positioned one-half of their body height away from a landing target marked on the floor. They were asked to jump out to the landing target and, once in contact with the ground, immediately complete a vertical jump for maximum height. Participants were allowed to move their arms freely during this motion and were encouraged to land as close to the landing target as possible after the maximum vertical jump. All participants completed a minimum of 3 acceptable landing trials and a maximum of 5. Landing trials were considered acceptable if (1) the participant was deemed to have correctly followed instructions, (2) visual inspection of the force-time data were consistent with typical data from a landing task, and (3) the participant was able to execute all phases of the landing without losing balance or prematurely ending the trial. Additional trials were not completed because the jump-landing assessment was included as part of a longer clinical assessment and the assessors feared accumulation of fatigue if additional trials were included.
Study team members who supervised the jump-landing task were not blinded to participants’ graft types. To ensure consistency between sites, the same investigators were responsible for data collection at each site. Participants were intentionally recruited from each site, as one site more heavily favored the QT autograft while the other more heavily favored the BTB autograft for primary unilateral ACLR.
Data quality was monitored in real time, and the jump-landing data were recollected if there were any perceived issues. Data were normalized to participant body weight, and the variables of interest were peak impact force (PIF), average loading rate (ALR), and impulse. Impulse was calculated as the area under the force-time curve from heel- strike to toe-off, and ALR was calculated as the slope of the middle 60% of the first jump landing using the method presented by Goss and Gross. 11 LSIs (percentage) were calculated for each biomechanical variable (equation 1):

Data were exported from the force-sensing insole mobile application and processed using a custom processing program developed by Peebles et al. 33 PIF data were not filtered, per the recommendations of Renner et al. 36
Statistical Analysis
Descriptive statistics were calculated for demographics, surgical characteristics, PROMs, and biomechanical variables of interest. Continuous demographic variables and surgical characteristics were compared between graft source groups using 1-way analysis of variance (ANOVA), while categorical variables were compared between groups using χ2 tests. IKDC and ACL-RSI scores were compared between graft source groups using 1-way ANOVAs. Involved limb, contralateral limb, and LSI for PIF, ALR, and impulse were compared between graft source groups using separate ANOVAs. Given that there were no significant differences between groups for participant age or sex, we opted not to control for these factors in our analysis. We also chose not to control the effect of site, given that the sites were chosen because they preferred specific graft sources for primary ACLR. However, we did run a sensitivity analysis in which we removed patients with the low-frequency graft source at each site and repeated the graft comparisons for IKDC, ACL-RSI, and landing kinetics. Cohen d effect sizes and 95% confidence intervals were calculated to estimate the standardized magnitude of difference between graft sources for each kinetic variable. Relationships among IKDC score, ACL-RSI score, and LSI for each biomechanical variable were assessed using Pearson product-moment correlation coefficients. Correlations were interpreted as very weak (r = 0-0.19), weak (r = 0.20-0.39), moderate (r = 0.40-0.59), strong (r = 0.60-0.79), or very strong (r = 0.80-1.0). The a priori alpha level was P < .05 for all analyses. Statistical analysis was completed using an open-source statistical package (Version 2.2.5; Jamovi), and data visualizations were completed using the ggplot package in R Studio (Version 2023.06.0+421).
Results
Forty-four participants (22 BTB autograft, 22 QT autograft) completed PROMs and jump-landing assessment at 6 ± 1 months after ACLR. Graft source groups did not differ by age, sex, mass, height, months since surgery, or treatment rate for lateral or medial meniscal tear (Table 1).
Participant Demographics and Surgical Characteristics Between Graft Sources a
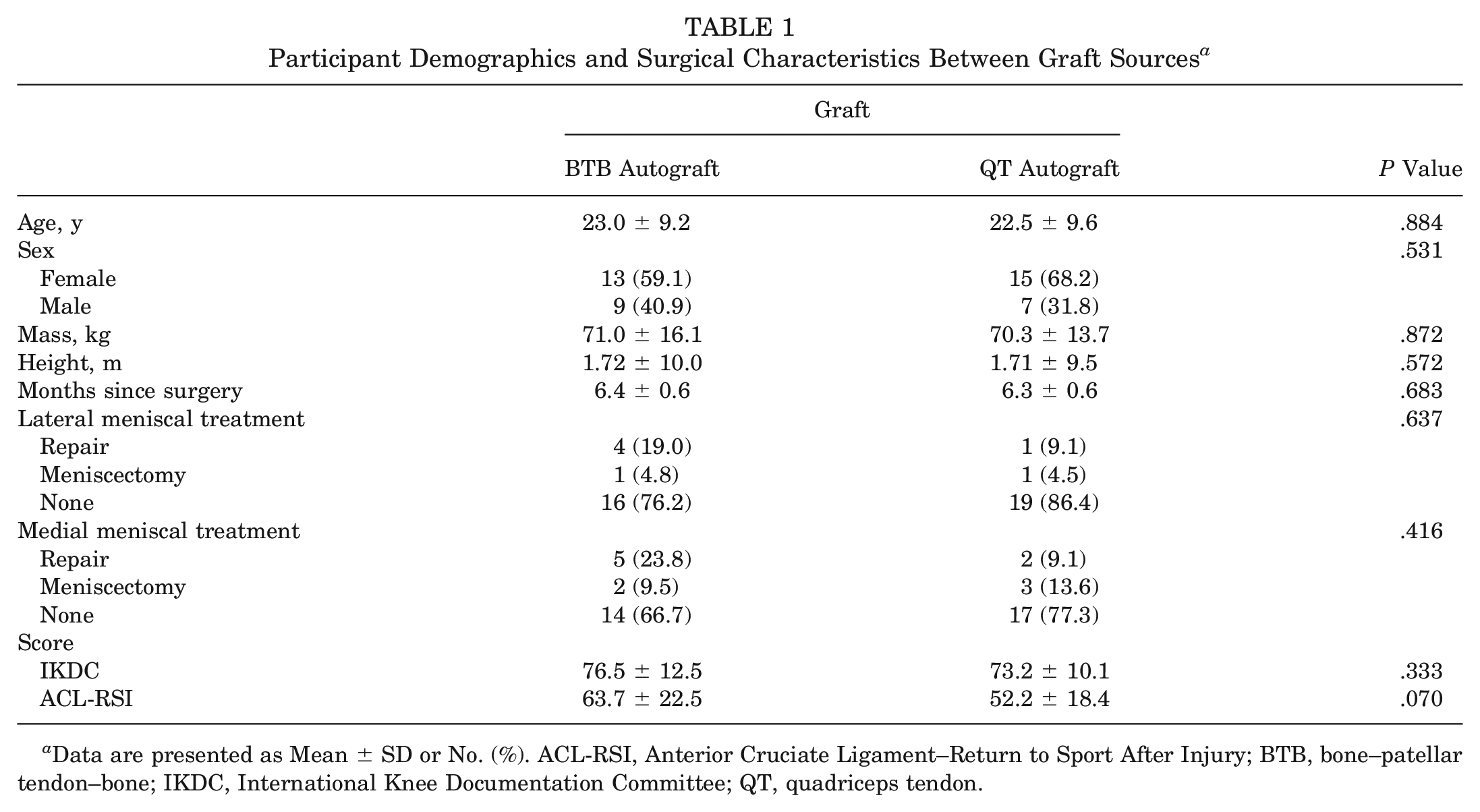
Data are presented as Mean ± SD or No. (%). ACL-RSI, Anterior Cruciate Ligament–Return to Sport After Injury; BTB, bone–patellar tendon–bone; IKDC, International Knee Documentation Committee; QT, quadriceps tendon.
Landing Kinetics
BTB and QT autograft groups differed in PIF and impulse but not ALR. There were no significant differences between graft source groups for involved limb PIF, but participants with a QT autograft demonstrated significantly greater contralateral limb PIF and significantly lower PIF LSI when compared with participants with a BTB autograft. There were no significant differences between graft source groups for involved limb ALR, contralateral limb ALR, or ALR LSI. The QT autograft group demonstrated significantly lower involved limb impulse and impulse LSI as compared with the BTB autograft group, but there were no significant differences in contralateral limb impulse between groups (Table 2).
Landing Kinetics Between Graft Sources a
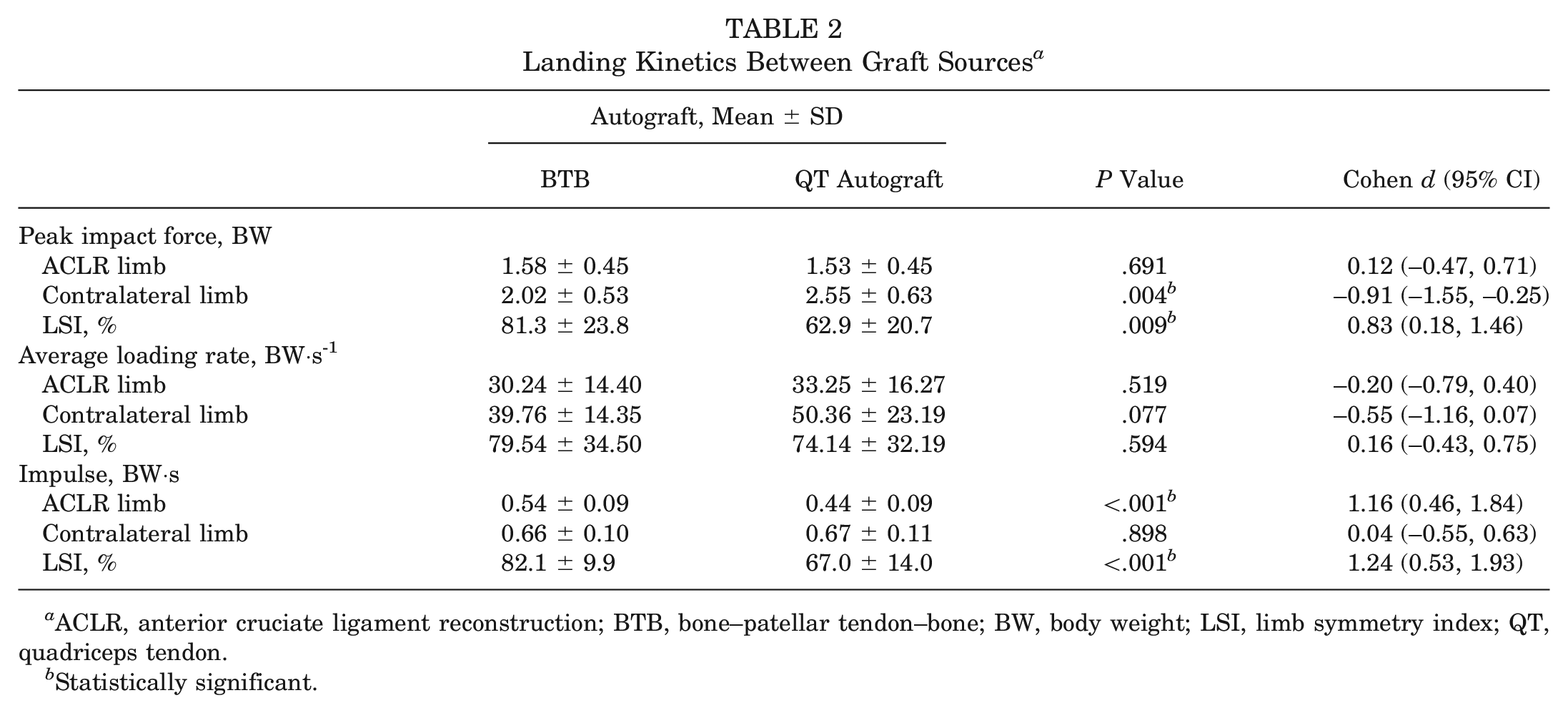
ACLR, anterior cruciate ligament reconstruction; BTB, bone–patellar tendon–bone; BW, body weight; LSI, limb symmetry index; QT, quadriceps tendon.
Statistically significant.
Patient-Reported Outcome Measures
Graft source groups did not differ in IKDC score or ACL-RSI score (Table 1). Among all participants, IKDC score was weakly associated with contralateral limb impulse and impulse LSI but no other kinetic variables (Table 3). Among the BTB autograft group, the IKDC score was not associated with any kinetic variable, but among the QT autograft group, IKDC score was moderately associated with contralateral limb PIF and contralateral limb impulse. Among all participants, ACL-RSI score was weakly associated with PIF LSI and impulse LSI, but there were no associations between ACL-RSI score and kinetic variables among participants with a BTB or QT autograft alone.
Association Between Patient-Reported and Kinetic Outcomes a

Data are presented as Pearson product-moment correlation coefficients. ACLR, anterior cruciate ligament reconstruction; ACL-RSI, Anterior Cruciate Ligament–Return to Sport After Injury; BTB, bone–patellar tendon–bone; BW, body weight; IKDC, International Knee Documentation Committee; LSI, limb symmetry index; QT, quadriceps tendon.
P < .05.
Sensitivity Analysis
There was a significant association between research site and graft source (P < .001), as site 1 enrolled 90.9% of patients with a QT autograft (n=20) while site 2 enrolled 86.4% with a BTB autograft (n = 19). When we compared graft source groups after removing low-frequency grafts from each site, our findings were consistent with the primary analyses. There were no significant differences between grafts for IKDC score (P = .179) or ACL-RSI score (P = .051). Contralateral PIF (P < .001) and loading rate (P = .009) as well as ACLR limb impulse (P < .001) were significantly different between graft source groups. Additionally, PIF LSI (P = .004) and impulse LSI (P < .001) were significantly different between graft source groups.
Discussion
The most important finding of this study was that participants who undergo ACLR with an all–soft tissue QT autograft exhibit greater PIF and impulse asymmetry during a bilateral DVJ than those with a BTB autograft (Table 2). This finding was novel, as only 1 previous study has assessed jump-landing kinetics in participants 6 months after ACLR with an all–soft tissue QT autograft, and it found no difference when compared with a BTB autograft. 26 In addition, this previous study utilized a laboratory-based 3-dimensional motion analysis system, while the current study leveraged force-sensing insoles, a clinically feasible technology, and participants underwent testing in the clinical environment.
Our finding that participants with QT autografts exhibit greater PIF and impulse asymmetry as compared with participants with BTB autografts is clinically significant, as asymmetric landing patterns before patients RTS have been associated with higher risk of second ACL injury after RTS, cartilage degeneration, and meniscal abnormalities.31,40,41 While Paterno et al 31 observed this association between risk of second ACL injury and asymmetric knee extensor moment, it is important to note that knee extensor moment can be reliably predicted through ground-reaction forces,7,32 which were recorded in the current study. Our QT and BTB autograft groups demonstrated no difference in involved limb PIF, but the QT autograft group demonstrated significantly greater uninvolved limb PIF, thereby creating more side-to-side PIF asymmetry when compared with the BTB autograft group (Table 2). This may be indicative of a compensatory mechanism being used by these participants with a QT autograft, as greater impact forces during a DVJ have been shown to be associated with a stiff landing pattern after ACLR 20 and with higher risk of ACL injury. 13 While nonsignificant, the lower ACL-RSI scores reported by these patients with a QT autograft may be indicative of this compensatory mechanism owing to a maladaptive psychological response. 4 Additionally, in the uninvolved limb, increased impact forces have been observed during landing in patients after ACLR as compared with healthy controls, and it has been hypothesized that increased reliance on the uninvolved limb during landing may place patients at higher risk of contralateral injury. 27
Our findings regarding impulse symmetry mirror our PIF symmetry results. Like PIF symmetry, impulse symmetry can be a surrogate for knee extensor moment symmetry in clinical settings,23,34 and we found that the QT autograft group exhibited greater impulse asymmetry than the BTB autograft group (Table 2). This may also indicate a compensatory mechanism being utilized by patients with a QT autograft, as their lower involved limb impulse, as compared with their counterparts with a BTB autograft, may indicate an inability to appropriately transfer momentum during landing. While our study did not directly measure second injury, future work should use tools such as force-sensing insoles to correlate asymmetries in landing kinetics with second injury among various autograft groups to evaluate whether these differences in landing kinetics truly do put patients with a QT autograft at higher risk of a second ACL injury.
We found no strong associations between biomechanical variables and PROMs (Table 3), which was unexpected given the associations previously found between landing kinetics and ACL-RSI score at this time point. 35 In the absence of associations between PROMs and DVJ asymmetries among the entire cohort or either graft group, factors other than self-reported function and psychological readiness must be considered as potentially driving the observed differences in knee kinetics. While our study did not directly examine quadriceps strength differences between graft groups, it may be possible that quadriceps strength is driving these observed differences between graft groups. Previous studies have found a relationship between post-ACLR DVJ asymmetries and asymmetry in quadriceps strength,12,16,17,38 and it has recently been reported that quadriceps strength is inferior in patients with a QT autograft versus a BTB autograft during post-ACLR rehabilitation. 14 Therefore, perhaps difficulty in regaining quadriceps strength and delays in rehabilitation attributed to this difficulty could be driving our observed between–graft group differences in landing kinetics. Future studies should measure quadriceps strength alongside landing kinetics to determine whether an association between them exists and could be driving differences between patients with QT and BTB autografts after ACLR. While our study was, unfortunately, unable to capture this assessment owing to lack of an appropriate isokinetic dynamometer at 1 site, the inclusion of these tests in future studies may elucidate potential interventions to reduce loading asymmetry before patients RTS.
Importantly, our use of force-sensing insoles is clinically translatable, as they are less expensive than traditional force plates and do not require advanced training. In patients post-ACLR, PIF and impulse measurements collected from force-sensing insoles during landing have been strongly associated with force plate vertical ground-reaction force symmetry as measured by force plates and knee extensor moment symmetry as measured by 3D motion capture. 23 Given that post-ACLR loading asymmetry during jump landing is associated with a higher risk of second ACL injury, 31 patients may benefit from the inclusion of objective testing of loading asymmetry, and our study indicates that force-sensing insoles are suitable to accomplish this in the clinical rehabilitation setting, thereby allowing for early, direct intervention to improve outcomes. In the future, tools such as force-sensing insoles could be incorporated into RTS testing to objectively evaluate who may be at higher risk of second ACL injury. Future research should aim to determine clinical thresholds for landing kinetic variables that are predictive of second ACL injury to maximize the clinical utility of data derived from tools such as force-sensing insoles.
This study was not without limitations. First, it was conducted at multiple sites and included multiple surgeons, thereby creating potential variation in surgical techniques. While this may affect the internal validity of our results, it would also serve to increase their generalizability. Additionally, because each site in this study primarily contributed patients of 1 graft source, there is a possibility that surgeon-specific factors such as experience and technique may have confounded our results. Our study may have also been underpowered, with 22 participants in each graft cohort. However, now that preliminary effect sizes have been established using force-sensing insoles, future studies should be more adequately powered to make comparisons of landing forces between ACLR limbs. Our study also analyzed only a single time point (6 ± 1 months after ACLR), and longitudinal data were not collected. Yet, because aberrant landing patterns at this specific time point have been associated with an increased risk of second injury, 31 our results help guide clinical decision-making. Next, the 100-Hz sampling rate of force-sensing insoles is lower than that of traditional force plates. Nevertheless, traditional force plates are not as easy to use in the clinical setting, and force-sensing insoles at 100 Hz have been validated against force plates.23,36 In addition, given the lack of an isokinetic dynamometer at 1 site, we were unable to measure quadriceps strength, even though a relationship between post-ACLR DVJ asymmetries and decreased quadriceps strength has been previously found.12,16,17,38 This reduces our ability to determine what other modifiable traits may be causing our noted differences in loading asymmetry between graft groups. Last, we did not evaluate postoperative outcomes (ie, RTS and second ACL injury), as this study was intentionally conducted before the RTS period to capture biomechanical data at a time when patients are still in contact with the health care team and intervention is possible. Therefore, we cannot make conclusive claims on the clinical effect of our observed differences in landing kinetics.
Conclusion
Our results demonstrate that participants with a QT autograft exhibit greater asymmetry in landing kinetics when compared with participants with a BTB autograft 6 months after ACLR. However, landing kinetics were not associated with PROMs within our sample. Importantly, our study also demonstrates that force-sensing insoles appear to be a suitable tool for use in the clinical setting for the testing of DVJ asymmetries before RTS clearance.
Footnotes
Submitted April 17, 2024; accepted November 7, 2024.
One or more of the authors has declared the following potential conflict of interest or source of funding: E.S.C. has received consulting fees from Avanos, research support from Arthrex, and hospitality payments from Supreme Orthopedic Systems. C.M.K. has received consulting fees from Inova Health. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.