
Abstract
Background:
Fresh osteochondral allograft (OCA) transplantation is an established treatment option for patients with chondral or osteochondral lesions of the knee. Predictably positive outcomes are seen in situations of focal or isolated cartilage defects. However, OCA transplantation may also be performed in more complex joint salvage situations in young patients.
Purpose:
To evaluate survivorship and outcomes in patients who underwent OCA transplantation for large bipolar lesions of the knee.
Study Design:
Case series; Level of evidence, 4.
Methods:
Fresh OCAs were implanted for bipolar chondral lesions in 86 patients (89 knees) between 1983 and 2020. A total of 37 male and 52 female knees with a mean patient age of 37.9 years (range, 14.5-66.0 years) were treated. Surgical indications included degenerative chondral lesions, osteoarthritis, osteochondritis dissecans, traumatic chondral injuries, and previous failed OCAs. The clinical evaluation included the modified Merle d’Aubigné-Postel score, International Knee Documentation Committee (IKDC) score, and Knee Injury and Osteoarthritis Outcome Score (KOOS). Outcomes were collected during outpatient clinic visits or via mail. The minimum follow-up was 2 years. Additional procedures after OCA transplantation were documented. OCA failure was defined as a reoperation that involved removal of the allograft.
Results:
There were 81 knees (91.0%) that had undergone previous surgery, with a mean of 3.2 previous procedures (range, 1-11). The mean treated defect surface area was 16.7 cm2. Graft failure occurred in 31 knees (34.8%). Reoperations (including failures) occurred in 46 knees (51.7%). The mean time to failure was 4.8 years. Survivorship of the bipolar OCA was 73.8% at 5 years, 66.6% at 10 years, and 58.9% at 15 years. Among the 58 knees (65.2%) in which the OCA was still in situ, the mean follow-up was 11.3 years (range, 2.1-27.6 years). The mean modified Merle d’Aubigné-Postel score improved from 12.4 to 14.8 points; 64.3% of knees (36/56 with available data) were considered successful with a score ≥15. The mean IKDC pain score improved from 6.3 to 4.0, and the mean IKDC function score improved from 2.9 to 6.2. The KOOS symptoms, pain, activities of daily living, sports/recreation, and quality of life subscores all increased postoperatively by a mean of 19.7, 25.9, 27.1, 35.4, and 36.4, respectively.
Conclusion:
OCA transplantation is a salvage treatment option for large bipolar cartilage lesions of the knee with acceptable survivorship and significant clinical improvement in a challenging patient population.
Keywords
Articular cartilage injuries of the knee are common and have limited innate healing capacity. Symptoms may include persistent pain, catching, and persistent swelling that limit the ability to participate in sports and exercise. If identified early in the setting of focal isolated defects, cartilage restoration techniques such as subchondral marrow stimulation, autologous chondrocyte implantation, osteochondral autograft transplantation, and fresh osteochondral allograft (OCA) transplantation have been shown to have high success rates, yielding improvements in pain and function.1,7,14,16,18 However, cartilage disease progression can lead to defect enlargement, extension into the subchondral bone, and development of multifocal or bipolar lesions. Concomitant or staged off-loading osteotomy is a commonly used procedure to treat overpressure in a symptomatic compartment. Although options such as unicompartmental and total knee arthroplasty are effective procedures for patients with end-stage arthritis, their usage in younger and more active patients remains limited because of concerns for long-term survivorship. The ideal cartilage treatment for complex large or bipolar chondral defects remains unclear, as clinical success has been less predictable.5,6,10,12,15 There are limited previous studies that have reported on bipolar OCA transplantation, and they have generally included small sample sizes, have had a short-term follow-up, and have reported inconsistent graft survivorship rates. Our group previously reported on the early outcomes of 48 knees (46 patients) that underwent bipolar OCA transplantation, 12 and survivorship was 64.1% at 5 years.
For the treatment of complex cartilage conditions, OCA transplantation offers immediate restoration of the articular cartilage ultrastructure in a single-stage procedure. OCA transplantation restores mature articular cartilage and the underlying subchondral bone for host tissue fixation to the graft via creeping substitution. Chondrocyte viability and extracellular matrix integrity directly affect postoperative outcomes, and their preservation is critical. Additional benefits include the lack of donor site morbidity, the ability to address concurrent subchondral bone marrow lesions, accelerated recovery, and long-term durability. Additionally, OCA transplantation may be performed in the revision setting or in situations in which other cartilage repair procedures have failed.
The purpose of this study was to assess long-term survivorship and self-reported outcomes in patients who underwent OCA transplantation for large bipolar lesions of the knee. This study’s aim was accomplished by following up on a previously published midterm outcomes report on the same patients 12 as well as including more patients to provide a larger cohort. We hypothesized that patients would have acceptable graft survivorship and improved outcomes at midterm to long-term follow-up in this challenging clinical scenario.
Methods
An institutional review board–approved prospective OCA registry was used to collect data on all patients undergoing fresh OCA transplantation at our institution. We identified 99 knees (96 patients) who underwent OCA transplantation for large bipolar lesions in the knee between 1983 and 2020. Of those, 10 knees (10 patients) were excluded because they did not have a minimum follow-up of two years, resulting in 89 knees (86 patients) included in the present midterm report. All 48 knees (46 patients) included in our original report 12 were included in the current study as well as an additional 40 knees (39 patients) who met the inclusion criteria since the original study was conducted. In addition, one knee (one patient) who was originally excluded from the early-term report due to a lack of follow-up was later contacted and included in the present report (Figure 1).
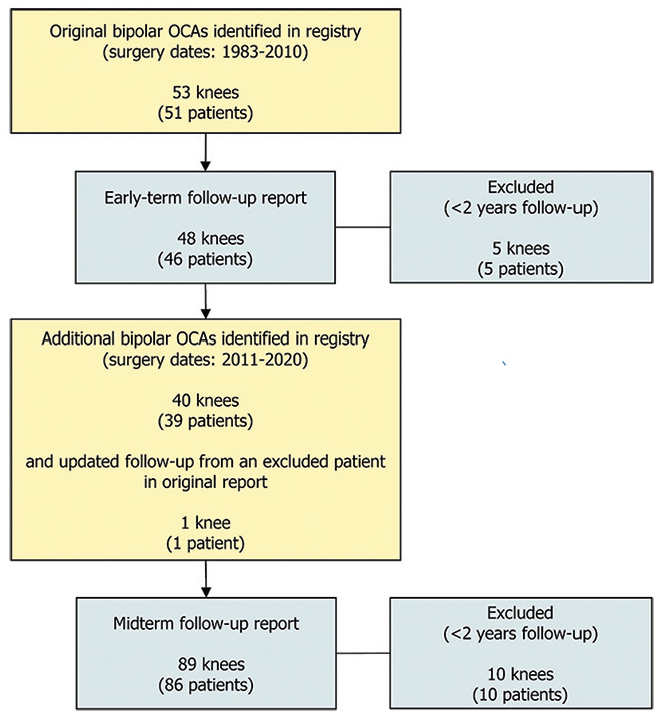
Patient population flowchart.
Surgical procedures were performed by 1 of 3 surgeons, with the majority (69/89 [77.5%]) performed by the senior author (W.D.B.). Fresh allograft tissue, which met the criteria of the American Association of Tissue Banks, was obtained within 24 hours after donor death. Since 1983, there have been no essential changes in the graft recovery process. All grafts were recovered aseptically, and no terminal sterilization was performed to maintain chondrocyte viability. The recovered specimen was processed and maintained at 4°C until the time of implantation. All grafts were implanted within 28 days of donor death. Donor-recipient matching was based solely on size and anatomic location, with a match considered appropriate when the tibial width, as measured on radiography or magnetic resonance imaging, was within 2 mm of the direct measurement of the donor tibial width. No blood matching, tissue matching, or immunosuppressive therapy was utilized.
The surgical technique used in this study has been previously described. 12 Briefly, the patient was placed in a supine position, and a midline incision was performed. Patellofemoral and medial compartment lesions were approached through medial parapatellar arthrotomy. Lateral compartment lesions were approached either through lateral or medial arthrotomy, depending on the details of the surgical treatment. The topographic characteristics of the recipient defect were noted to determine whether a shell, plug, or combined (shell and plug) allograft was appropriate. In the setting of bipolar tibiofemoral procedures, hemi–tibial plateaus with an attached meniscal graft were utilized for tibial OCA transplantation. Patellofemoral OCA transplantation was performed with either shell or combined (shell and plug) grafts for the treatment of patellar and/or trochlear lesions (Figure 2). After bony preparation, the allograft specimen was cut to match the recipient articular surface. Grafts were set with a press-fit technique with or without supplemental absorbable pin or screw stabilization (Figure 3). Hemi–tibial plateau allografts were uniformly fixed with 3.0-mm metal screws in the anterior and lateral margins of the graft.
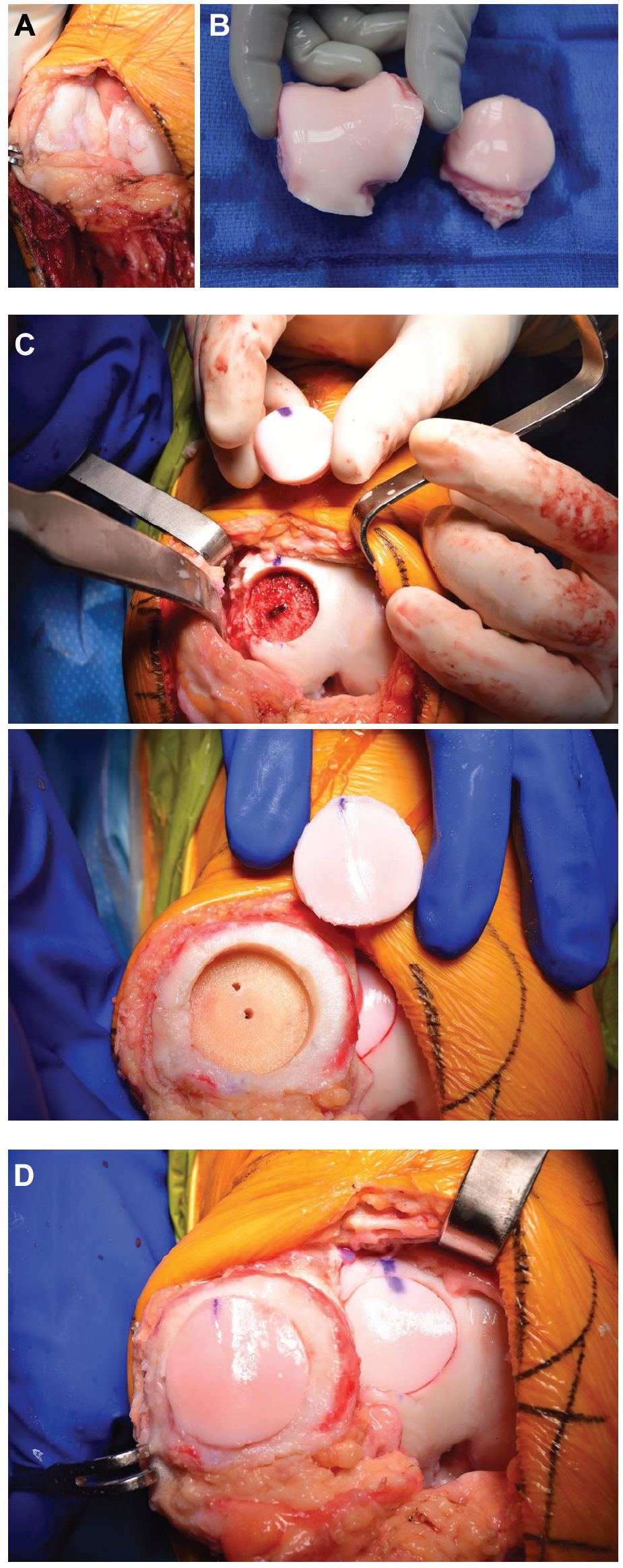
Bipolar patellofemoral osteochondral allograft in a right knee, viewed via medial parapatellar arthrotomy. (A) Intraoperative view of the patella (left) and trochlea (right), demonstrating diffuse chondral disease. (B) Trochlear and patellar allograft tissue. (C) Harvested trochlear (top) and patellar (bottom) plug graft and prepared recipient sites. (D) After insertion of the graft using a press-fit technique with no additional fixation.
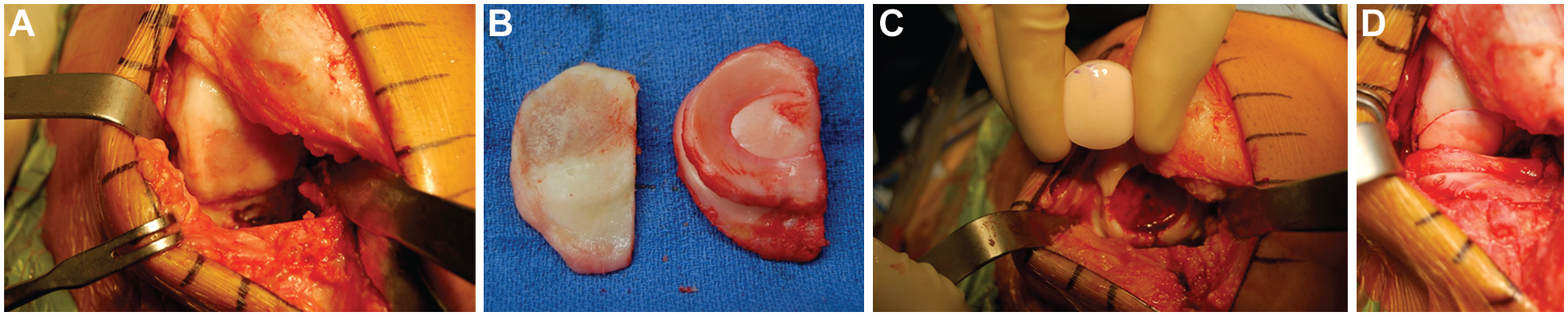
Bipolar tibiofemoral osteochondral allograft in a right knee, viewed via lateral parapatellar arthrotomy. (A) Intraoperative view of the lateral component with a full-thickness femoral condyle lesion. Note that the tibial surface has already been resected. (B) Resected lateral tibial plateau (left) and prepared tibial allograft with an attached meniscus. (C) Femoral plug allograft and prepared femoral defect. (D) Lateral compartment after insertion of the femoral condyle and tibial plateau with meniscal allografts.
Postoperative care included formal physical therapy for all patients with 12 weeks of protected weightbearing. Patients were placed in a range of motion brace until radiographic signs of graft incorporation were noted at follow-up. Patellofemoral grafts were limited to 0° to 30° of flexion initially, followed by the progression to full range of motion once quadriceps function was adequate, as determined by the patient’s ability to perform an active straight-leg raise without lag. We routinely did not restrict patients in their postoperative activity after this surgery.
The primary outcome in this study was OCA failure, defined as graft removal during revision OCA transplantation, conversion to arthroplasty, arthrodesis, or patellectomy. Preoperative and postoperative patient-reported outcomes were recorded and included the International Knee Documentation Committee (IKDC) score, the Knee Injury and Osteoarthritis Outcome Score (KOOS), and the modified Merle d’Aubigné-Postel score. Patient-reported outcomes were collected at follow-up clinic visits as well as via mail for those unable to travel to an in-person visit. Patients’ most recent outcome scores were used for the study. The minimum follow-up was 2 years.
Statistical Analysis
Data were summarized using frequencies and percentages for categorical variables and means ± standard deviations for continuous variables. The Kaplan-Meier method was used to calculate graft survivorship. The Wilcoxon signed-rank test was used to assess the change in patient-reported outcomes from preoperatively to latest follow-up. Univariate analysis was performed to determine which patient characteristics and graft-related factors differed between patients who experienced OCA failure and those who did not. Variables that were statistically significant in univariate analysis were included in full logistic regression to determine the factors predictive of graft failure. A final logistic regression model was built that included the variables most predictive of graft failure while adjusting for all other variables in the model. A P value of .05 was used to determine statistical significance. Data were analyzed using SPSS (Version 29.0; IBM).
Results
The mean patient age was 37.9 years (range, 14.5-66.0 years), with 41.6% of patients being male. The most common primary diagnoses were degenerative chondral lesions and osteoarthritis (Table 1). A diagnosis of a degenerative chondral lesion was made when symptoms persisted for longer than 18 months without a discrete identifiable episode leading to the lesion. A diagnosis of osteoarthritis was made when patients demonstrated radiographic signs of joint space narrowing. According to the modified Fairbank-Ahlbäck radiographic classification of osteoarthritis, 11 5% of knees had grade 0 (no changes), 38% had grade I (sharpening of edges, flattening of condyles, sclerosis, or initial formation of osteophytes but no joint space narrowing), 23% had grade II (<50% joint space narrowing), and 34% had grade III (≥50% joint space narrowing). Of the 89 knees, 81 (91.0%) had undergone previous surgical interventions, with a mean of 3.2 (range, 1-11) previous procedures per patient. Among patients who had undergone a previous surgical intervention, 24.7% had 1 previous procedure, 19.8% had 2 previous procedures, and 55.4% had ≥3 previous procedures.
Patient Characteristics a
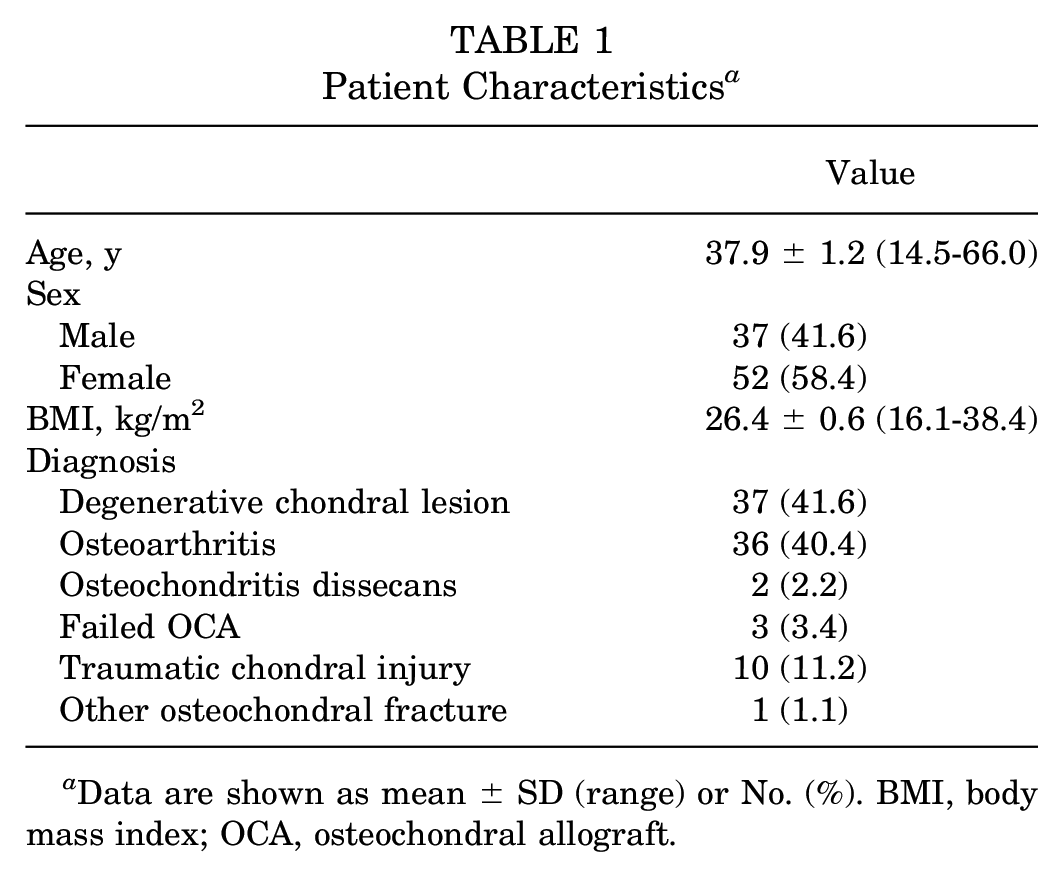
Data are shown as mean ± SD (range) or No. (%). BMI, body mass index; OCA, osteochondral allograft.
Of the 89 knees included in this series, 39 cases of bipolar OCA transplantation were performed in the patellofemoral compartment, 20 cases were performed in the medial compartment, 24 cases were performed in the lateral compartment, and 6 cases were multicompartmental (Table 2). There were 2 patients (2 knees) who had bipolar grafts in the patella, trochlea, and femoral condyle (1 lateral and 1 medial). The allograft type was a plug, shell, or combined in 34, 33, and 22 of cases, respectively. The mean graft surface area was 16.7 cm2 (range, 4.2-41.0 cm2). Concomitant procedures were performed in 39 knees, with the majority consisting of hardware removal (Table 3). Overall, 3 knees (3.4%) underwent concomitant off-loading osteotomy (1 distal femoral, 1 high tibial, and 1 tibial tubercle). Additionally, 3 knees underwent a staged bilateral procedure.
Allograft Characteristics a
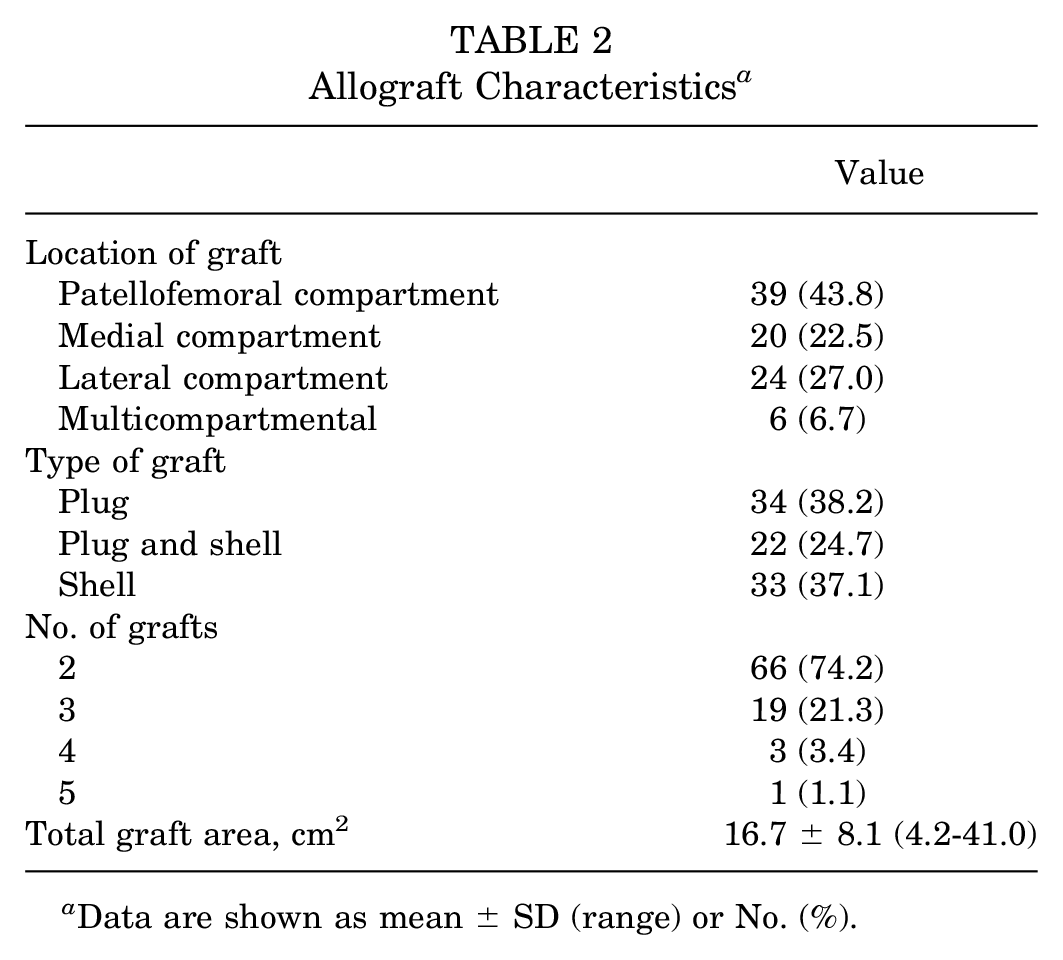
Data are shown as mean ± SD (range) or No. (%).
Concomitant Procedures a
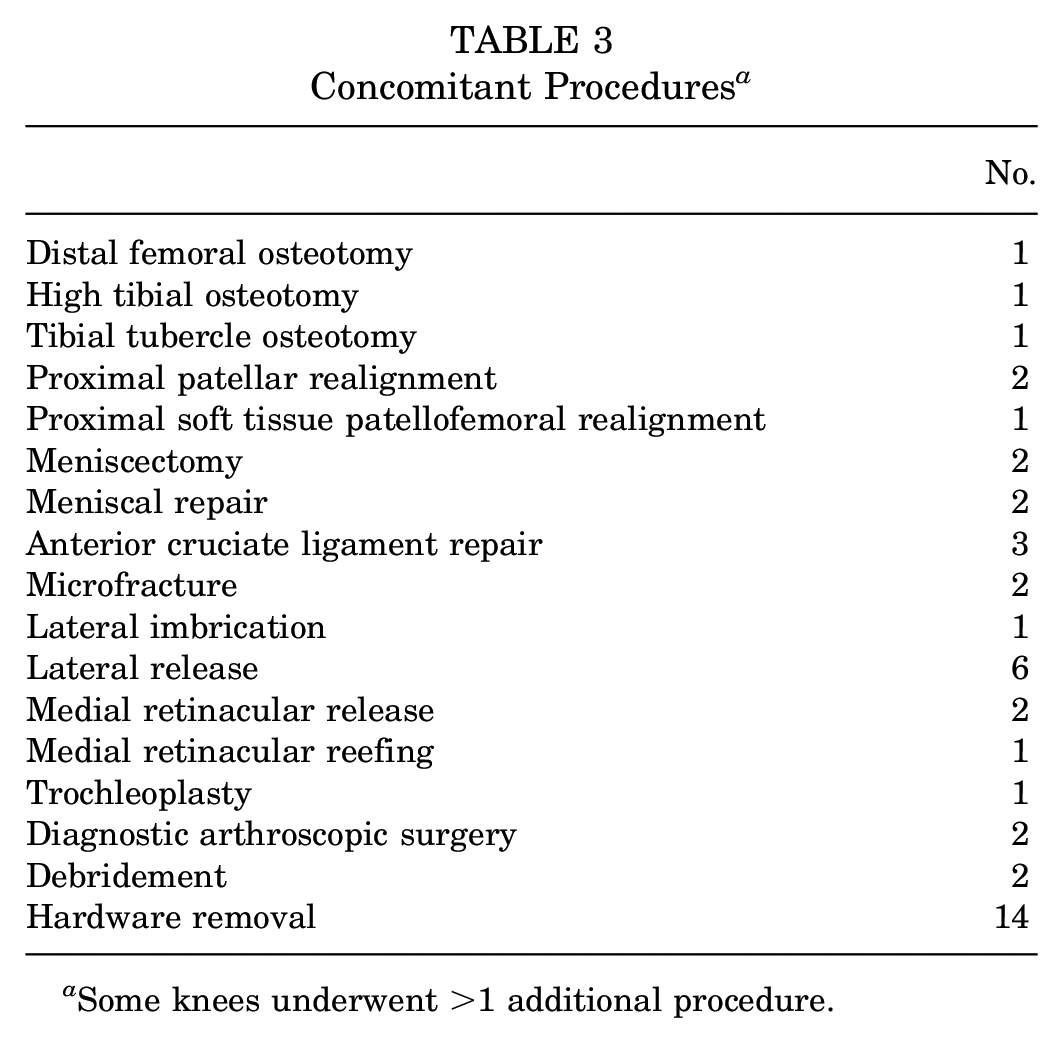
Some knees underwent >1 additional procedure.
At latest follow-up, 46 of the 89 knees (51.7%) underwent a reoperation after OCA transplantation, of which 31 (34.8%) were defined as OCA failure with a mean time to failure of 4.8 years (Table 4). Most failures (23/31 knees [74.2%]) underwent conversion to arthroplasty (19 total arthroplasty, 2 unicompartmental arthroplasty, and 2 patellofemoral arthroplasty) (Table 4). Among the 31 failures, 22 had been previously identified and reported in our original early follow-up report, and 9 were identified since the previous report was published. Overall, 29.0% of failures occurred in the patellofemoral compartment, 25.8% occurred in the medial compartment, and 45.2% occurred in the lateral compartment. Among the 39 patellofemoral compartment grafts, the failure rate was 23.1%; among the 20 medial compartment grafts, the failure rate was 40.0%; and among the 24 lateral compartment grafts, the failure rate was 58.3% (P = .19). None of the six multicompartmental grafts failed.
Reoperations a

Some knees underwent >1 reoperation. OCA, osteochondral allograft.
OCA survivorship was 73.8% at 5 years, 66.6% at 10 years, and 58.9% at 15 years (Figure 4). Univariate analysis identified that body mass index (BMI), patient sex, diagnosis, anatomic location treated, total graft area, and graft fixation technique (plug vs shell) were associated with OCA failure (Table 5). Patient age, previous surgery, number of previous surgeries, and number of grafts showed no increase in the failure rate. Logistic regression models were built using the variables that were statistically significant in univariate analysis. The final regression model showed that patients with increasing BMI, a diagnosis of osteoarthritis, and shell grafts were more likely to experience OCA failure compared with patients without these characteristics, after holding all other variables in the model constant (Table 6).
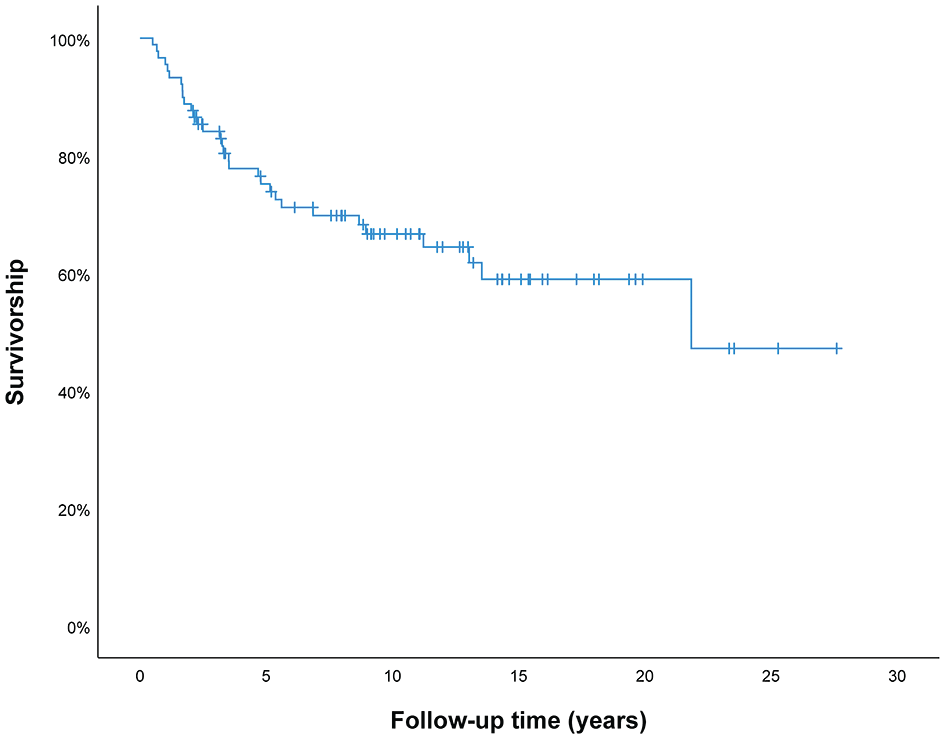
Survivorship of the bipolar osteochondral allograft was 73.8% at 5 years, 66.6% at 10 years, and 58.9% at 15 years.
Patient and Allograft Characteristics by OCA Failure and Nonfailure a
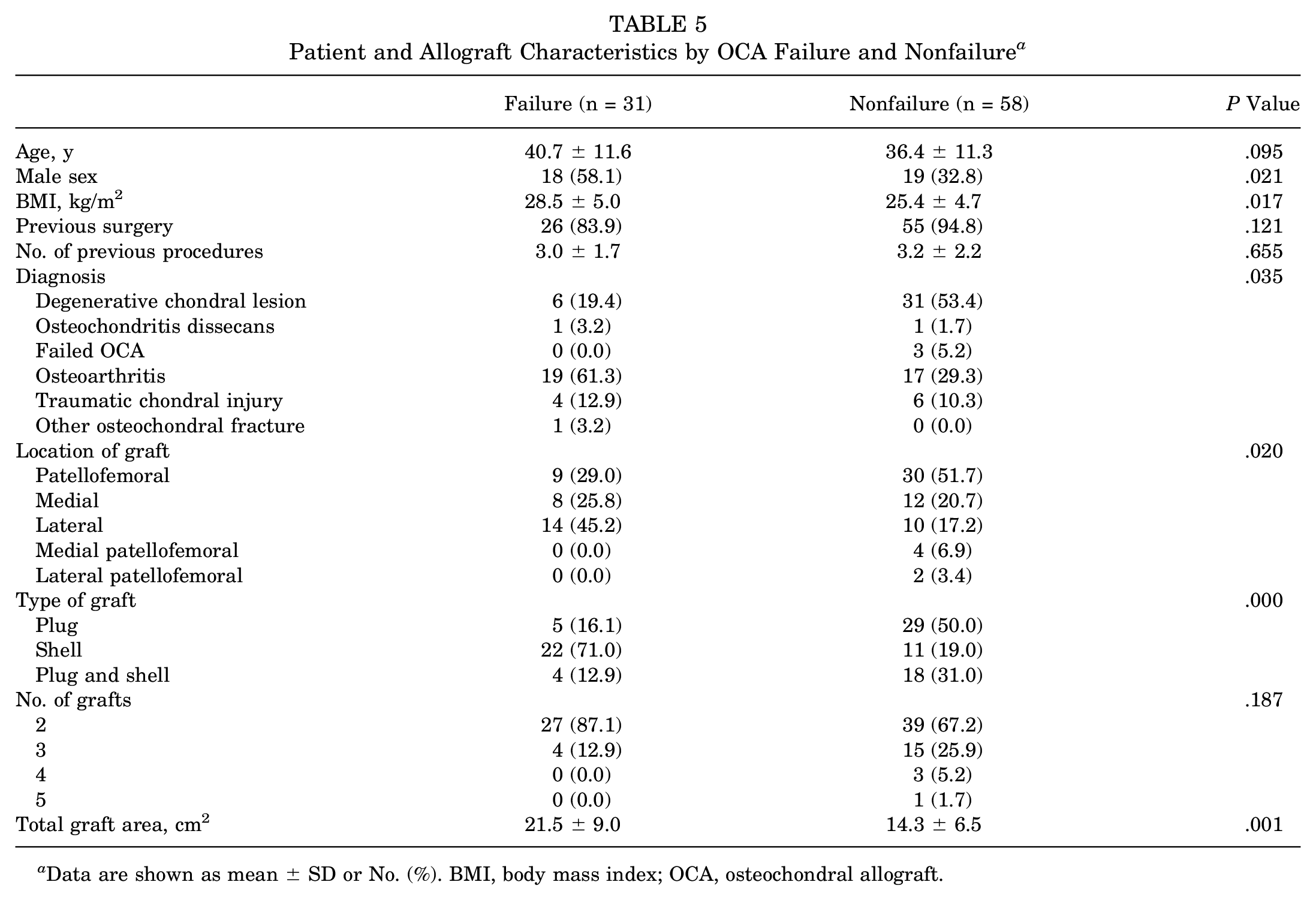
Data are shown as mean ± SD or No. (%). BMI, body mass index; OCA, osteochondral allograft.
Variables Predicting OCA Failure a
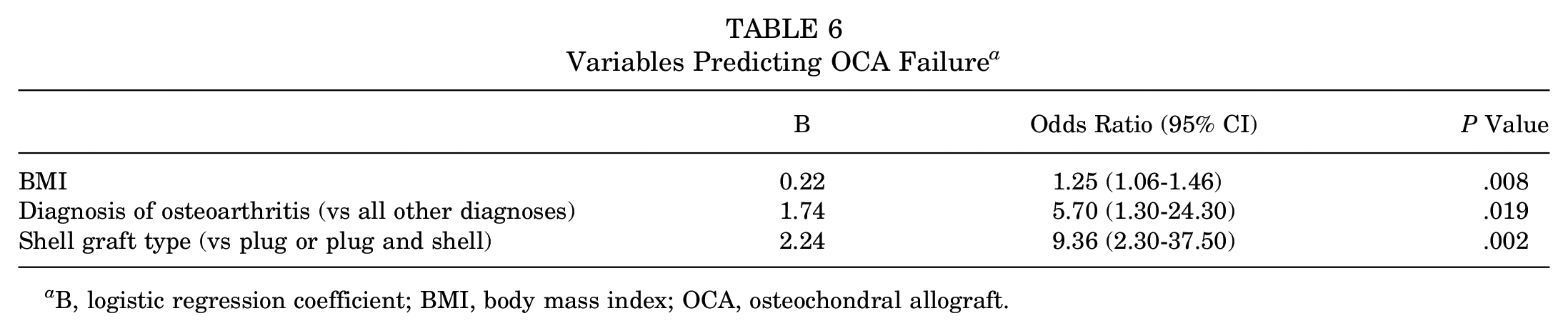
B, logistic regression coefficient; BMI, body mass index; OCA, osteochondral allograft.
The mean follow-up of the 58 knees that had grafts remaining in situ at latest follow-up was 11.3 years (range, 2.1-27.6 years); 81.0% had a minimum 5-year follow-up, and 55.2% had a minimum 10-year follow-up. Most patients (51/58 [87.9%]) reported being satisfied or extremely satisfied with the results of OCA transplantation at latest follow-up. The IKDC score showed a significant improvement from preoperatively to postoperatively (all P < .001) for all subscales including pain, function, and total (Table 7). Patients had a similar improvement on the KOOS subscales for symptoms, pain, quality of life, activities of daily living, and sports/recreation (all P < .001). At latest follow-up, the modified Merle d’Aubigné-Postel score increased by 2.4 points from preoperatively (P < .001).
Patient-Reported Outcome Scores a
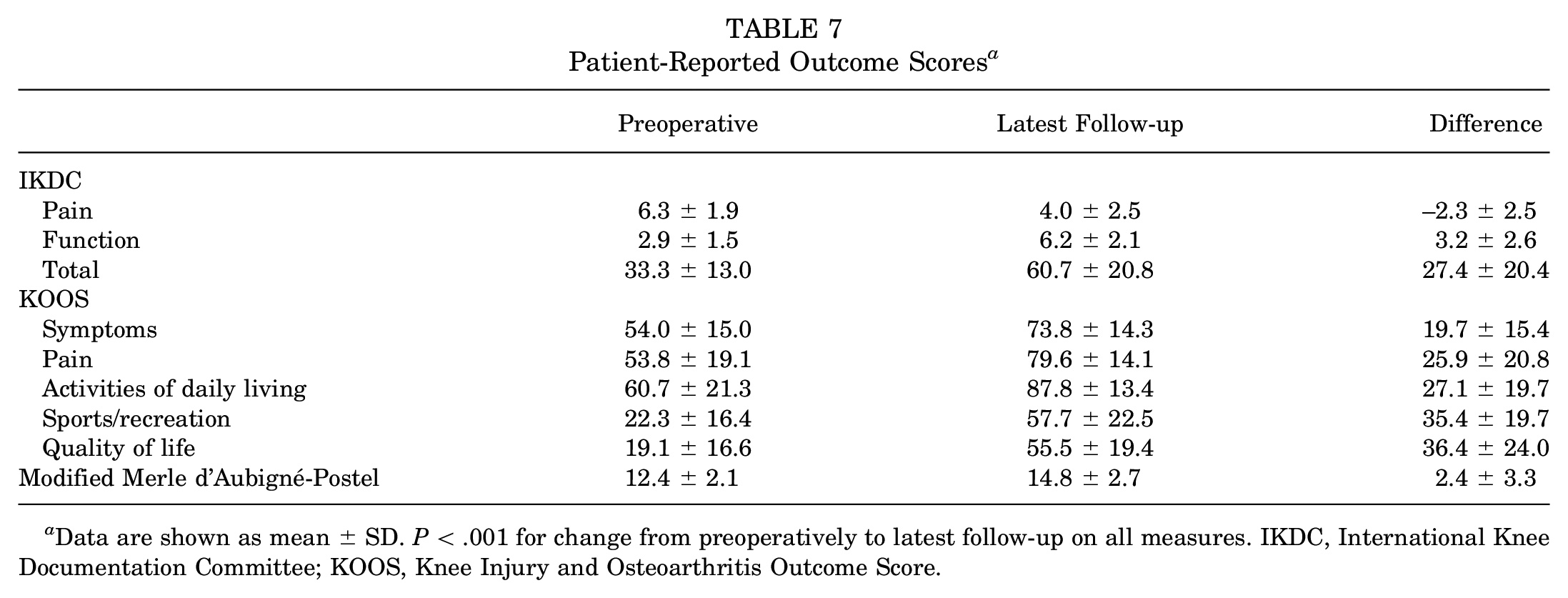
Data are shown as mean ± SD. P < .001 for change from preoperatively to latest follow-up on all measures. IKDC, International Knee Documentation Committee; KOOS, Knee Injury and Osteoarthritis Outcome Score.
Discussion
In this study, patients undergoing bipolar OCA transplantation for reciprocal cartilage lesions in the knee had a graft survivorship of 66.6% at 10 years. Reoperations occurred in 46 knees (51.7%), of which 31 knees were considered allograft failures. However, despite these findings, patients routinely reported improved clinical outcomes, as assessed by IKDC, KOOS, and modified Merle d’Aubigné-Postel scores, during their postoperative care. Additionally, 87.9% reported being satisfied or extremely satisfied with the result of OCA transplantation at their latest follow-up.
The optimal management of large reciprocal osteochondral lesions of the knee in young patients remains challenging. Although arthroplasty has been shown to be fundamentally successful with high survivorship, it may not be an ideal surgical option for a patient with a relatively young age or high activity demands. A recent registry study by Castagnini et al3 focused on primary total knee arthroplasty in a young population and showed a cumulative survivorship of 90% in the first 8 years, which declined to 83.5% at 10 years. An 8.8% revision rate was noted at final follow-up, with aseptic loosening being the leading cause of revision. 3 Additional studies have confirmed similar findings, with younger patients undergoing total knee arthroplasty having higher rates of aseptic loosening within 2 years of the index procedure (52.5% vs 29%, respectively) as well as higher rates of reoperations (17.7% vs 9.7%, respectively) and component re-revision (11.4% vs 6%, respectively) compared with a traditional older cohort. 19 These differing results may help support the role of cartilage repair as an alternative option for a curative or bridging procedure in a younger population suffering from debilitating cartilage disease of the knee.
Although OCA transplantation is a relatively complex procedure, it has been increasingly adopted over the last decade likely because of improved access to OCA tissue and positive clinical outcomes. 2 Despite improvements in technique, long-term outcomes are still affected by primary surgical indications and the severity of disease, particularly when comparing focal chondral defects versus large reciprocal cartilage lesions. OCA transplantation for the treatment of focal osteochondritis dissecans lesions has been shown to have high survivorship, 93% at 10 years postoperatively, with high patient satisfaction. 16 In comparison, Stannard and Cook 17 found that bipolar lesions were 3.8 times more likely to fail in comparison to unipolar lesions. Although a previous systematic review showed an 86.7%, 78.7%, and 72.8% likelihood of graft survival at 5, 10, and 15 years, respectively, many of the included studies demonstrated a significantly higher failure rate among bipolar defects. 8 Gowd et al 10 published a recent review of bipolar OCA transplantation including 4 studies confirming these findings, with 24.3% (37/152) total failures and a mean time to failure of 2.7 to 4.1 years. These and other studies demonstrate the challenges associated with the treatment of more advanced cartilage disease and arthritis using osteochondral grafting.
Ogura et al 15 reported the outcomes of 57 patients undergoing autologous chondrocyte implantation for the treatment of bipolar chondral defects in the tibiofemoral compartment. There were 30 patients in their cohort who underwent concomitant off-loading osteotomy at the time of cartilage repair. Survival was 80% at 5 years and 76% at 10 years postoperatively, with improved outcomes when a collagen membrane was used. A high satisfaction rate of 91% was reported at a mean of 8.3 years postoperatively. Minas et al 13 reported a 92% success rate when utilizing autologous chondrocyte implantation in the setting of early arthritis with or without concomitant osteotomy as well as improved outcomes at 5 years postoperatively. Cook et al 6 reported a 77.6% graft retention rate and high satisfaction in patients treated with bipolar OCA transplantation with meniscal allograft transplantation at 2-year follow-up.
Our group previously reported the outcomes of 48 knees (46 patients) that underwent OCA transplantation for the treatment of bipolar knee chondral or osteochondral defects. 12 Survivorship of the bipolar OCA was 64.1% at 5 years. The current study is a larger series including the previously evaluated patients and an additional 40 knees, as well as one knee from the previous report that was originally lost to follow-up, for a total of 89 knees. We found similar failure and reoperation rates to those of the previous study. Despite the current failure rate of 34.8%, pain and function scores improved from preoperatively to postoperatively in those with allografts remaining in situ. Improvements noted at final follow-up met the patient acceptable symptomatic state threshold for the KOOS but not the IKDC score. However, the change in KOOS and IKDC scores (from preoperatively to latest follow-up) met the minimal clinically important difference cutoffs as reported by Chahal et al. 4 Clinical outcome scores among patients who had the graft in situ may have been influenced by the relatively high reoperation rate after OCA transplantation. The mean graft area of 16.7 cm2 among patients in this study reflects the very different nature of these patients compared with “typical” cartilage restoration candidates. To our knowledge, the current study is the largest cohort to date with a mean follow-up of greater than 10 years specifically focusing on bipolar lesions of the knee. Patients with surviving grafts reported a significant improvement on all outcome measures. The cause of failure remains unknown, although it is likely multifactorial and dependent on both biological and mechanical factors. This study supports previous claims that bipolar lesions reflect a higher burden of arthritic disease 9 because osteoarthritic lesions showed a 5.7 times increase in the failure rate. Other factors including graft type and BMI should be regarded when considering OCA transplantation, given its higher reported failure rates.
This study has many limitations including the potential bias secondary to the retrospective nature of the study. It is possible that the patients lost to follow-up impacted our results. Patients with unfavorable outcomes may be underrepresented if the reason behind the loss to follow-up was seeking outside care. However, it is also plausible that patients with excellent outcomes were less inclined to continue orthopaedic care. While attributing causes to patient attrition is outside the purview of our study, it does highlight the complex nature of the patient population and a significant challenge for assessing outcomes of this rare procedure. Although we reported a long mean follow-up of 11.3 years, much of the data were obtained via telephone or mailed questionnaires. Given that patients travel from far distances to undergo this particular procedure at our institution, long-term in-person follow-up visits were not practical for many patients. This contributed to subjective findings without supportive radiographic evidence to evaluate graft status or progressive asymptomatic disease. Our results may have been affected by the wide range in the length of follow-up, as longer term follow-up may be influenced by other confounding factors such as those associated with aging. Further studies may consider a comparison group undergoing other commonly performed procedures for osteochondral lesions of the knee with supportive long-term radiographic analysis. We did not assess OCA failure based on the preoperative modified Fairbank-Ahlbäck radiographic classification because we believe that it is beyond the scope of the study. We think that this would be a good idea for a future study looking at the outcomes of OCA transplantation by osteoarthritis classification. Additionally, there was great heterogeneity in the patient population in terms of cause of damage, number and type of previous procedures, and concomitant procedures; however, this is representative of the unique patient population that would qualify for bipolar OCA transplantation. Moreover, only 3 knees underwent concomitant osteotomy at the time of OCA transplantation, which did not allow us to perform a subgroup analysis on this variable.
Conclusion
Overall, our results support previous literature with higher rates of failure among bipolar lesions of the knee in comparison to focal lesions. However, despite the higher failure rates in this challenging patient population, significant improvements on subjective outcome measures and high satisfaction may support the use of OCA transplantation in young patients who are less than optimal candidates for arthroplasty. Finally, patients with increasing BMI, a diagnosis of osteoarthritis, and shell grafts were predisposed to OCA failure, as identified with a logistic regression model.
Footnotes
Submitted August 7, 2023; accepted November 19, 2024.
One or more of the authors has declared the following potential conflict of interest or source of funding: This study was supported by a grant from the Scripps Clinic Medical Group. T.S.B. has received hospitality payments from Stryker and support for education from Smith & Nephew and MicroMed. T.W. has received consulting fees from Bioventus and Miach Orthopaedics, hospitality payments from Arthrex, research support from Miach Orthopaedics, support for education from Evolution Surgical, and holds stock or stock options in Overture Orthopaedics. J.C.M. has received consulting fees from JRF Ortho. W.D.B. holds ownership or investment in OrthAlign; has received intellectual property royalties from DePuy Synthes, Zimmer Biomet, Smith & Nephew, and Encore Medical; and has received consulting fees from JRF Ortho, Arthrex, DePuy Synthes, DePuy Orthopaedics, OrthAlign, Encore Medical, Medical Device Business Services, Bioventus, Smith & Nephew, and Insight Medical Systems. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.