
Abstract
Background:
Trochlear dysplasia is present in 68% to 85% of patients with recurrent lateral patellofemoral instability (LPI) compared with 3% to 6% of healthy controls. Trochlear dysplasia has been associated with medial patellofemoral ligament (MPFL) graft failure and lower quality-of-life (QOL) outcome scores. The correction of trochlear dysplasia with trochleoplasty is indicated in patients with recurrent LPI and high-grade trochlear dysplasia with a trochlear bump and a significant J-sign.
Purpose:
To assess the clinical and patient-reported outcomes after patella-stabilizing surgery, including thin flap sulcus deepening trochleoplasty, and to explore the influence of pathoanatomic variables on postoperative QOL scores in patients who have undergone patellar stabilization, including trochleoplasty.
Study Design:
Case series; Level of evidence, 4.
Methods:
A total of 63 consecutive knees in 46 patients with recurrent LPI and high-grade trochlear dysplasia who underwent MPFL reconstruction with thin flap trochleoplasty were followed for 2 years postoperatively. Clinical outcomes and Banff Patellofemoral Instability Instrument (BPII) 2.0 scores were collected prospectively. The t test was used to determine changes in QOL. Multiple linear regression was conducted to determine significant pathoanatomic variables that affected outcomes after MPFL reconstruction.
Results:
Overall, 63 knees with a mean follow-up of 32.9 ± 17.0 months (range, 12-84 months) were included. All patients had preoperative high-grade trochlear dysplasia (Dejour type B: 46%; Dejour type D: 54%), with a mean trochlear bump height of 6.1 ± 1.8 mm (range, 3.2-10.5 mm). The BPII 2.0 score increased significantly from preoperatively (29.3 ± 12.4) to postoperatively (71.8 ± 17.4) (P < .001), with a large effect size (Cohen d = −2.41). There was 1 redislocation (1.6%) and 3 reoperations (4.8%). Persistent apprehension and the J-sign were present in 8.5% and 13.6% of the knees, respectively. Multiple linear regression analysis demonstrated no statistically significant predictive relationship between the 24-month postoperative BPII 2.0 score and the preoperative BPII 2.0 score, tibiofemoral rotation, the Beighton score, or trochlear bump height (R = 0.47; R2 = 0.22; F = 5.23; P = .13).
Conclusion:
Thin flap trochleoplasty combined with MPFL reconstruction in patients with recurrent LPI and high-grade trochlear dysplasia resulted in low redislocation and reoperation rates at a mean of 33 months. Disease-specific QOL scores were statistically significantly improved from preoperatively to postoperatively.
Keywords
A lateral patellofemoral dislocation is a significant knee injury. Recurrent lateral patellofemoral instability (LPI) is treated with medial patellofemoral ligament (MPFL) reconstruction, and in the presence of pathoanatomic risk factors, concomitant procedures can be performed to improve the anatomy and biomechanics of the patellofemoral joint. Trochlear dysplasia is present in 68% to 85% of patients with recurrent patellar instability compared with 3% to 6% of healthy controls.15,36 In cadaveric studies and computational modeling, trochlear dysplasia was the most important factor contributing to increased lateral patellar translation.3,29,35 Clinically, trochlear dysplasia has been documented as one of the common reasons for recurrent instability9,15 and MPFL graft failure.1,17,37 Furthermore, an association has been demonstrated between high-grade trochlear dysplasia and lower quality-of-life (QOL) scores, especially with a trochlear bump >5 mm.23,25
Trochlear dysplasia can be corrected with trochleoplasty, a procedure in which excess bone from the femur is removed, creating a trochlear groove. Trochleoplasty, in addition to MPFL reconstruction, is indicated in patients with recurrent lateral patellar instability and high-grade trochlear dysplasia (Dejour types B and D) with a supratrochlear spur >5 mm and a significant J-sign. 34 It is a well-established procedure in Europe, with a 2019 meta-analysis of 29 case series including only 2 studies originating from North America and the remainder being from Europe. 27
Currently, the most commonly used technique for high-grade trochlear dysplasia in the setting of LPI with a trochlear bump is sulcus deepening trochleoplasty. 34 It can be performed by creating a thick osteochondral V-shaped flap, as described by Dejour and Saggin, 14 or a thin U-shaped flap, as described by von Knoch et al. 40 An arthroscopic version of thin flap trochleoplasty has also been described.7,39 The senior author (L.A.H.) has performed the thin flap technique since 2013 for patients requiring trochleoplasty with minimal cartilage damage.
The purpose of this study was to assess the clinical and patient-reported outcomes after patella-stabilizing surgery, including thin flap sulcus deepening trochleoplasty. A secondary purpose was to explore the influence of pathoanatomic variables on postoperative QOL scores in patients who have undergone patellar stabilization, including trochleoplasty.
Methods
Between 2013 and 2021, a total of 63 consecutive thin flap trochleoplasty procedures were performed in 46 patients (17 bilateral). The indication for surgery was recurrent LPI in extension, in the setting of high-grade trochlear dysplasia, with a significant J-sign. A significant J-sign was defined as grade 3 or 4 according to the J-sign classification 18 or bayonet or “L” shaped according to Donell et al. 16 The approach to surgical management in this study cohort was designed to be consistent with the Lyon protocol.12,14 The Dejour classification was used to classify trochlear dysplasia. 14 Type A represents a shallow but concave trochlea with a crossing sign seen on lateral radiographs but without a significant trochlear bump. Type B indicates a flat trochlear groove with a crossing sign and a trochlear bump. Type C has a flat trochlea and asymmetric trochlear facets identified with a double contour sign. Type D exhibits a “cliff” shape and all the radiographic signs (crossing sign, double contour sign, and trochlear bump). Type A is characterized as low-grade dysplasia, and types B, C, and D are considered high-grade dysplasia. Trochleoplasty was considered for Dejour types B to D dysplasia. Tibial tubercle osteotomy (TTO) was considered when the tibial tubercle–to–posterior cruciate ligament distance was >20 mm (medializing) or the Caton-Deschamps index was >1.3 (distalizing). All patients were treated with MPFL reconstruction using an autograft or allograft. 2
Patient history, demographic characteristics (age, sex, and body mass index), and pathoanatomic risk factors were assessed preoperatively. Clinical factors included the Beighton score, femoral anteversion, and tibial external rotation. Radiological measurements included trochlear dysplasia (Dejour classification), trochlear bump height (in mm), patella alta (Caton-Deschamps index), and tibiofemoral rotation (in degrees). Trochlear bump height and patella alta were measured on true lateral radiographs with a <3-mm condylar overlap. 26 Tibiofemoral rotation was assessed by measuring the angle between the posterior femoral and tibial condylar lines on 3-dimensional computed tomography. 42 Clinical outcomes from a clinical knee examination, knee range of motion testing (with a goniometer), the lateral patellar apprehension test, 22 and the J-sign classification 28 were collected preoperatively and postoperatively. Patients were assessed at 3 weeks and 3, 6, 12, and 24 months postoperatively. Information regarding complications, recurrence of patellar instability, and reoperations was collected prospectively. The Banff Patellofemoral Instability Instrument (BPII) 2.0 was completed preoperatively and at 1 and 2 years postoperatively. The BPII 2.0 is a disease-specific QOL patient-reported outcome measure (PROM) validated for patellar instability and was previously found to be reliable and responsive.21,24 It contains 23 questions in 5 domains, each scored on a 100-mm visual analog scale. The BPII 2.0 score is calculated with a maximum of 100, with higher scores indicating better QOL. Ethical approval for this study was obtained from the University of Calgary.
Surgical Technique
Thin flap trochleoplasty was performed in all cases through lateral parapatellar arthrotomy. Lateral retinacular lengthening was incorporated into the approach by creating a plane between the lateral retinaculum and the capsular layer. Arthrotomy was performed, and proximal extension through the distal lateral quadriceps tendon was performed when necessary to facilitate exposure. The patella was subluxated medially and maintained in this position with Steinmann pins in the medial femoral metaphysis. The center of the native trochlea was marked, as well as the center of the projected new groove, which was lateralized to align with the femoral notch. Using sharp curved osteotomes, a thin osteochondral flap was raised with a distal hinge, leaving 3 to 4 mm of bone with the chondral layer.
A high-speed bur was used to remove excess bone comprising the trochlear bump and to establish the trochlear groove. The osteochondral flap was carefully thinned with the bur until it was malleable and then molded in the newly formed groove and fixed with 2 to 3 polylactic acid copolymer SmartNail implants (ConMed) (Figure 1). The periosteum was reapproximated with 3-0 Vicryl interrupted sutures (Ethicon). The arthrotomy site was closed by suturing the anterior capsular layer to the posterior lateral retinaculum layer, thus performing lateral retinacular Z-lengthening. When necessary, the distal lateral quadriceps tendon was closed with absorbable sutures. When TTO was completed concomitantly, it was performed before trochleoplasty. 13 MPFL reconstruction was performed as the final procedure using a gracilis tendon autograft or allograft with 2 anchors at the patella and a bioabsorbable screw on the femur. 26
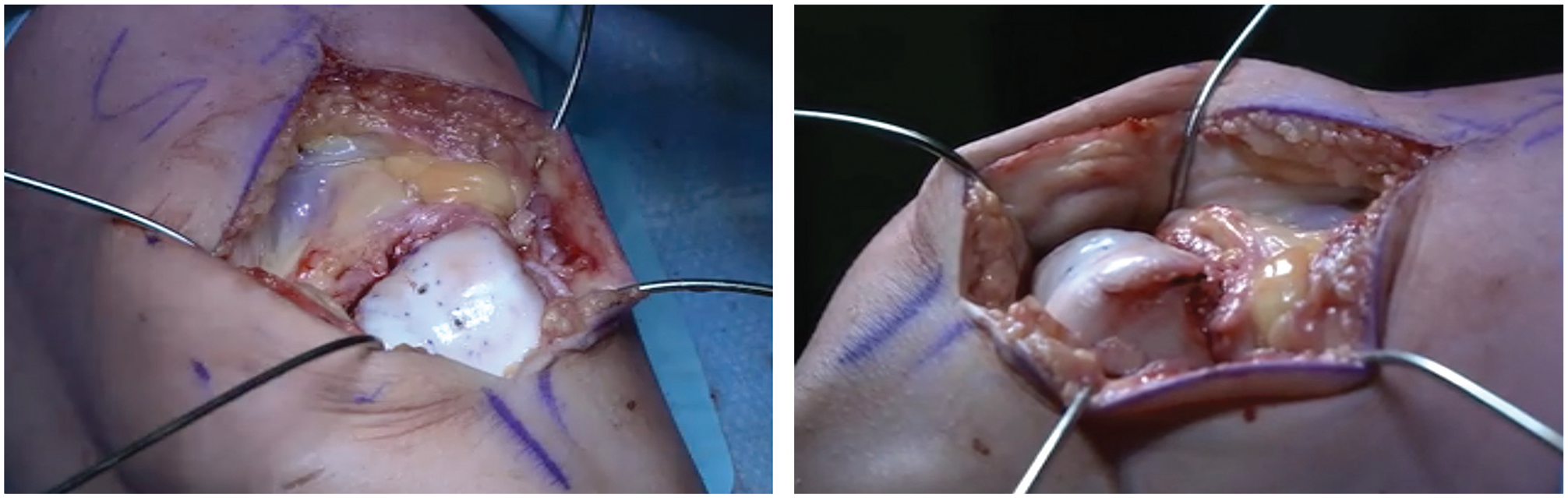
Superior and lateral views of completed thin flap trochleoplasty.
Postoperative Rehabilitation
Postoperative rehabilitation was phase based, consistent with the MPFL reconstruction protocol. Phase 1 (0-3 weeks) allowed patients to bear weight as tolerated with a range of motion brace and crutches as needed. Range of motion was not restricted, and gradual quadriceps activation exercises were encouraged. If TTO was performed, the protocol was modified to include 6 weeks of reduced range of motion, with weightbearing allowed as tolerated. Phase 2 (3-12 weeks) allowed weaning of the range of motion brace and crutches, with increasing focus on core, gluteal, hamstring, and quadricep strengthening. Phase 3 (12-24 weeks) focused on improving proprioception and balance along with single-leg strengthening exercises. Running and plyometric exercises were commenced in this phase. A gradual return to sport was initiated in phase 4 (24 weeks to 2 years). Sport-specific exercises were included to maximize strength, balance, and proprioception. 5
Statistical Analysis
Percentages, means, standard deviations, and ranges were calculated for the cohort. Floor and ceiling effects were calculated for the preoperative and 24-month postoperative BPII 2.0 scores to ensure that this trochleoplasty population demonstrated content validity for use of the PROM. A dependent-samples t test was used to determine if there was a change in BPII 2.0 scores from preoperatively to 24 months postoperatively. The effect size (Cohen d) was calculated. Multiple linear regression was used to explore the presence of any predictive relationship between the 24-month postoperative BPII 2.0 score and the preoperative BPII 2.0 score, tibiofemoral rotation, the Beighton score, and trochlear bump height. These variables were selected because they have previously demonstrated some relationship to outcomes after MPFL reconstruction.20,25,43,44 These variables also incorporated multiple factors, including lower limb rotation, tissue quality, trochlear dysplasia, and QOL, which includes biopsychosocial factors. All analyses were conducted using SPSS (Version 29; IBM).
Results
Between 2013 and 2021, a total of 63 consecutive thin flap trochleoplasty procedures were performed in 46 patients (17 bilateral). The mean age at the time of surgery was 22.0 years (range, 14-45 years), and the mean body mass index was 23.7 ± 5.2 kg/m2. The mean follow-up was 32.9 ± 17.0 months (range, 12-84 months). One patient was lost to follow-up after the 12-month visit; 2 patients underwent patellar stabilization on their contralateral knee after completing the 12-month BPII 2.0 and were not sufficiently recovered for us to evaluate the 24-month BPII 2.0 score for their primary knee. There were 37 female (80%) and 9 male (20%) patients. Generalized ligamentous laxity, defined as a Beighton score ≥4, was evident in 65% of patients. All patients had preoperative high-grade trochlear dysplasia (Dejour type B: 46%; Dejour type D: 54%), and the mean trochlear bump height was 6.1 ± 1.8 mm (range, 3.2-10.5 mm).
Previous Procedures
Overall, 17 patients had undergone procedures other than isolated arthroscopic surgery before trochleoplasty. Procedures performed before and concomitant with trochleoplasty are listed in Table 1.
Procedures Performed Before and Concomitant With Trochleoplasty a
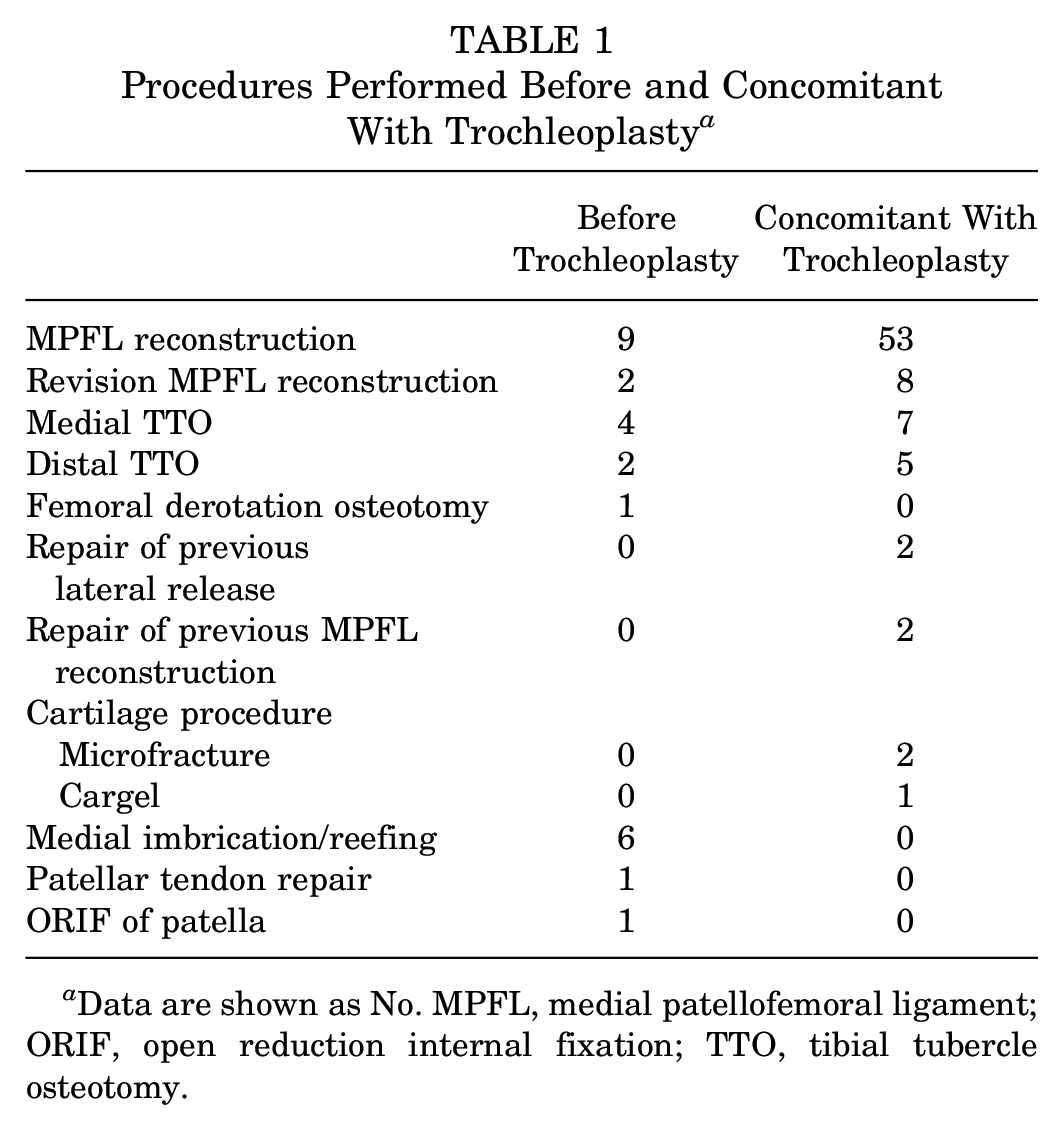
Data are shown as No. MPFL, medial patellofemoral ligament; ORIF, open reduction internal fixation; TTO, tibial tubercle osteotomy.
PROM Scores
There were no floor or ceiling effects evident in the preoperative or postoperative BPII 2.0 scores, indicating content validity of the measure in this trochleoplasty cohort. The BPII 2.0 score demonstrated a statistically significant increase from preoperatively (29.3 ± 12.4 [range, 3.7-74.5]) to 24 months postoperatively (71.8 ± 17.4 [range, 33.7-99.1]) (t = 18.32; P < .001). The Cohen d was calculated as −2.41, indicating a large effect size.
Complications and Reoperations
The recurrence of patellofemoral dislocations was present in 1 knee (1.6%), which suffered atraumatic failure at 3 years after trochleoplasty and MPFL reconstruction. This patient demonstrated a recurrence of the J-sign in terminal extension with an increased femoral internal torsion of 33°. Femoral derotation osteotomy and revision MPFL reconstruction were performed with good results.
There were 3 reoperations (4.8%), with 2 on the same patient, including arthroscopic wash out surgery for an intra-articular postoperative infection as well as a subsequent arthroscopic debridement and manipulation under anesthesia. The patient recovered favorably, with a 2-year BPII 2.0 score of 73.9. The patient who underwent a concomitant cartilage restoration procedure with Cargel (Smith & Nephew) developed hypertrophic cartilage and underwent arthroscopic surgery and debridement, followed by a resolution of symptoms with a 2-year BPII 2.0 score of 72.3.
At 24 months postoperatively, all knees demonstrated a stable MPFL on clinical examination. Knee range of motion was not restricted, with all patients demonstrating ≥135°. At the final follow-up, persistent apprehension to lateral patellar translation was evident in 8.5% (5/59) of the knees. A persistent J-sign was evident in 13.6% (8/59) of the knees; however, in all cases, it was no longer classified as significant.
Regression Analysis
Simple multiple linear regression was used to explore evidence of a predictive relationship between the 24-month postoperative BPII 2.0 score and the preoperative BPII 2.0 score, tibiofemoral rotation, the Beighton score, and trochlear bump height. There were no statistically significant relationships between the 24-month postoperative BPII 2.0 score and the included variables (R = 0.47; R2 = 0.22; F = 5.23; P = .13).
Discussion
This study demonstrated that thin flap sulcus deepening trochleoplasty and MPFL reconstruction as components of the surgical management of patients with recurrent LPI and high-grade dysplasia with minimal cartilage damage had low redislocation (1.6%) and reoperation (4.8%) rates at a mean of 33 months after patellar stabilization. At 2 years postoperatively, there were no knee range of motion limitations, and all patients demonstrated a stable MPFL on clinical examination. There was a statistically significant improvement in QOL scores from preoperatively to 2 years postoperatively, with a large effect size. This trochleoplasty series, the first reported in Canada and one of the few in North America, showed that trochleoplasty, in combination with MPFL reconstruction, was both effective and reliable, with a low complication rate, in this cohort of complex patients.
The available literature on trochleoplasty remains sparse, with mainly small to medium case series. This research has been summarized in 2 recent meta-analyses. Hiemstra et al 27 analyzed 29 studies, including 998 patients undergoing trochleoplasty. PROMs were included in 13 studies, and scores significantly improved from preoperatively to the final follow-up in all studies. 27 The redislocation rate was 0% in most studies but ranged from 0% to 27%. 27 The reoperation rate was significant but very heterogeneous between the studies, reflecting the “complex nature” of these patients. 27 Davies et al 11 included 12 contemporary series of 702 trochleoplasty procedures with a mean follow-up ranging from 0.88 to 8.3 years. The redislocation rate ranged from 0% to 8%. 11 Although the data regarding the safety and efficacy of trochleoplasty for patients with LPI and high-grade dysplasia are accumulating, the reporting of outcomes is inconsistent, making comparisons between studies difficult.
Subsequent to these systematic reviews, more case series have been published, adding 355 cases with a clinical follow-up to the trochleoplasty literature. These case series are summarized in Table 2 and report short- to medium-term follow-up. Substantial variability in the reporting of outcomes after trochleoplasty is also evident in these recent studies.
Recent Case Series Reporting Outcomes of Trochleoplasty a
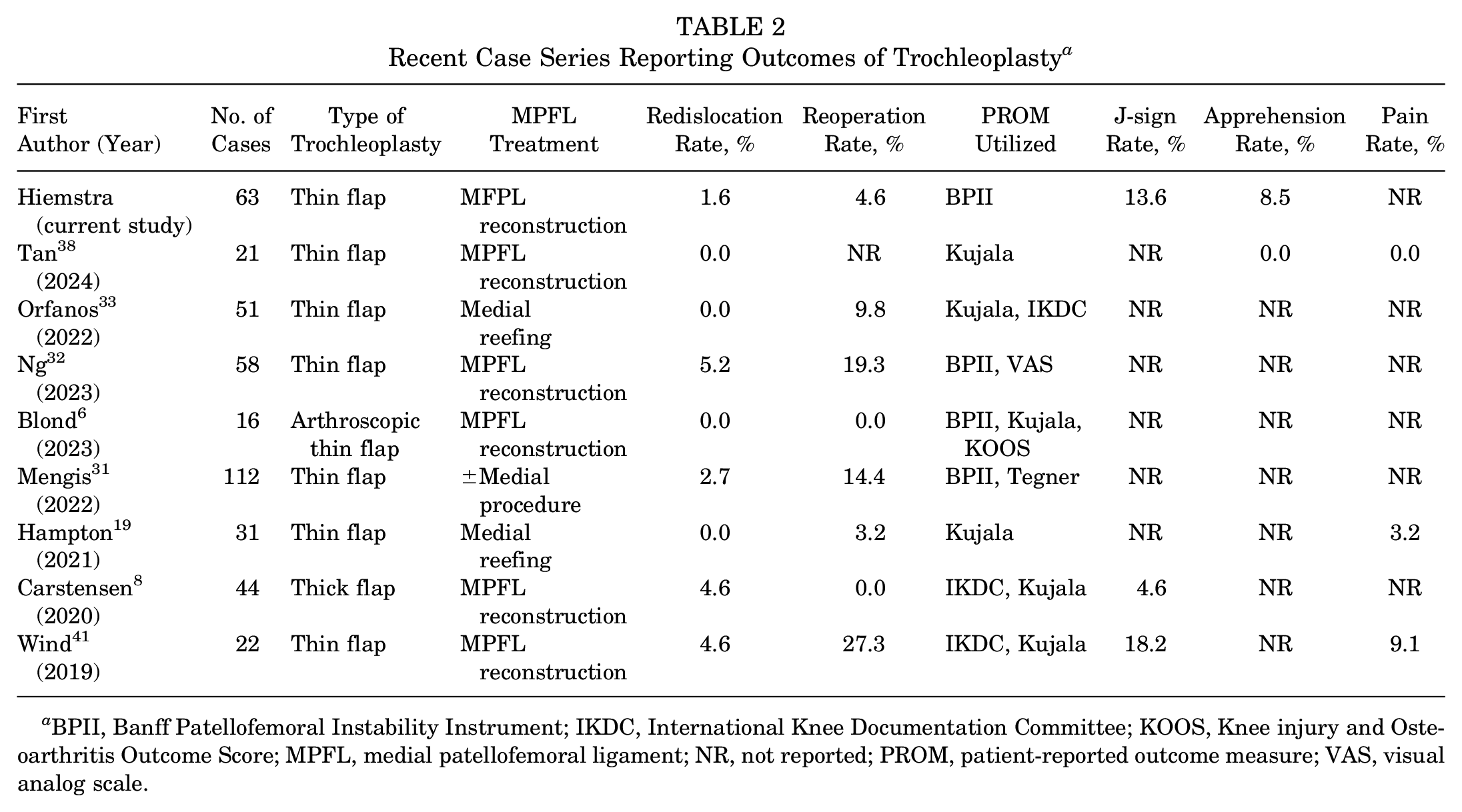
BPII, Banff Patellofemoral Instability Instrument; IKDC, International Knee Documentation Committee; KOOS, Knee injury and Osteoarthritis Outcome Score; MPFL, medial patellofemoral ligament; NR, not reported; PROM, patient-reported outcome measure; VAS, visual analog scale.
A closer examination of the PROMs in these more recently published case series demonstrated that all studies reported improved scores from preoperatively to postoperatively after trochleoplasty and MPFL reconstruction (Table 3).
PROM Scores for Recent Case Series Reporting Outcomes of Trochleoplasty a
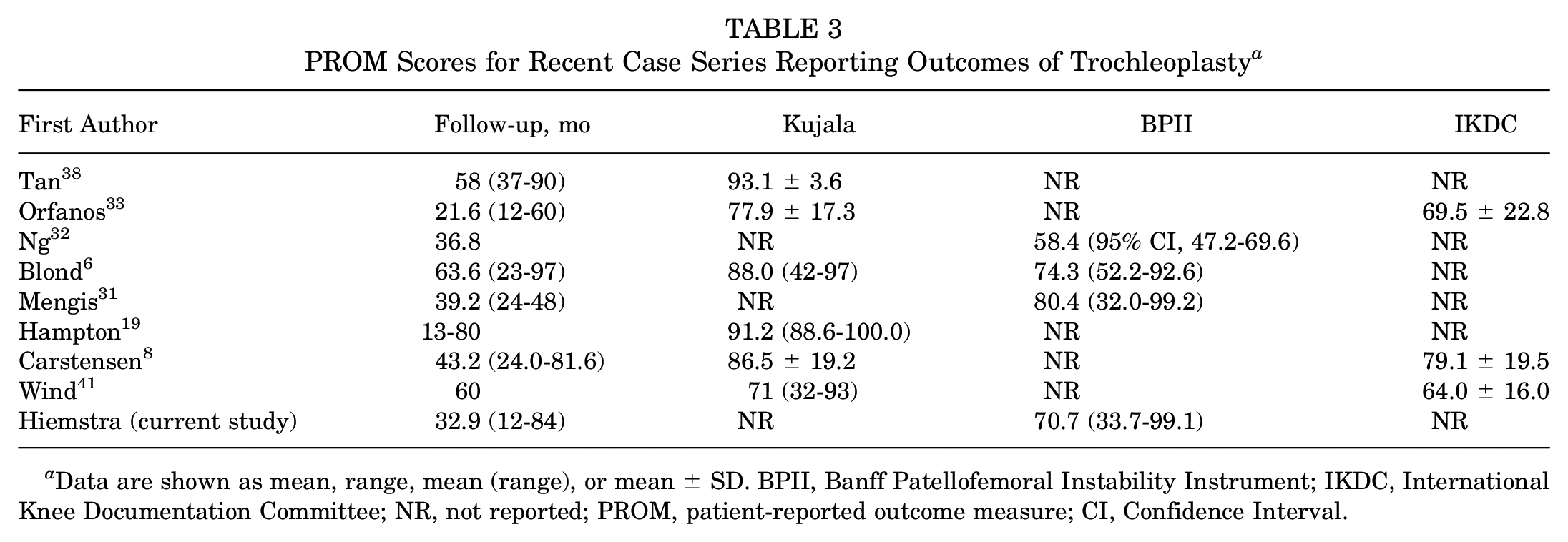
Data are shown as mean, range, mean (range), or mean ± SD. BPII, Banff Patellofemoral Instability Instrument; IKDC, International Knee Documentation Committee; NR, not reported; PROM, patient-reported outcome measure; CI, Confidence Interval.
Despite concerns over its validity for patients with patellofemoral instability, the Kujala score remains the most common PROM utilized in this patient population. It was created primarily as an anterior knee pain score and only has one question pertaining to instability. Continued concerns with ceiling effects associated with the Kujala score persist in patients with LPI, as indicated in the range of scores presented in Table 3. There has been increasing use of the BPII 2.0 since its publication in 2013, and it remains the only disease-specific QOL PROM for patients with LPI.
Complication and failure rates in the present cohort are consistent with the literature and complement the growing body of research supporting the idea that trochleoplasty with MPFL reconstruction is safe and effective.4,43 The persistence of a positive J-sign or lateral apprehension is not systematically reported in the literature but is important to consider. However, both clinical outcomes are challenging to quantify because of their coarse dichotomous scales.22,28 The development of more nuanced and technical assessments will be required to enable a more thorough analysis of these clinical signs. In a recent systematic review of 12 studies, including 702 trochleoplasty cases, a persistent J-sign was present in 0% to 12% of patients (5 studies), while persistent apprehension was present in 0% to 29% of cases (7 studies). 11 In the current cohort, J-sign and apprehension rates at 2 years were 13.6% and 8.5%, respectively. Possible causes of a persistent J-sign include unaddressed pathoanatomic risk factors and deficits in neuromuscular control. The persistence of apprehension is more complex, and while this could indicate unaddressed pathoanatomic risk factors, pain catastrophizing, kinesiophobia, and psychological components are potential factors in ongoing apprehension in some patients. 22
Regression analysis exploring predictive relationships between the 2-year postoperative BPII 2.0 score and the preoperative BPII 2.0 score, trochlear bump height, the Beighton score, and tibiofemoral rotation revealed no significant results. These variables represent a range of risk factors that have been demonstrated to influence patient outcomes after patellofemoral stabilization. The variables include the different pathoanatomy inherent to this population, including disorders of collagen, trochlear dysplasia, rotational abnormalities, and patient QOL and function. The lack of a statistical relationship is not surprising, given that trochleoplasty and MPFL reconstruction correct many of these preoperative factors. However, one recent article demonstrated that the preoperative BPII 2.0 score was predictive of achieving the minimal clinically important difference postoperatively in a cohort of patients with complex LPI. 10 Therefore, this regression analysis should be considered exploratory, as much larger cohorts will be required to show any predictive relationships with a degree of certainty.
The strengths of this study include the prospective collection of data in this large series of consecutive cases. However, there are some limitations to note. First, this is a cohort from a single surgeon specializing in patellofemoral disorders. Thus, the results from this study cannot be generalized to surgeons with lower volumes of patella-stabilizing surgery. Also, because another procedure was performed with trochleoplasty (MPFL reconstruction ± TTO), it is impossible to appreciate each surgical correction’s effect on the reported outcomes. However, a recent study concluded that adding TTO to MPFL reconstruction did not alter patient-reported outcomes, 30 and a systematic review determined that trochleoplasty in isolation or in combination resulted in similar outcomes in recurrent LPI. 11 Lastly, multivariate regression analysis would be more robust with a larger number of cases. Multicenter studies with standardized techniques and data collection will be needed to identify the risk factors for poorer outcomes after trochleoplasty.
Conclusion
Trochleoplasty combined with MPFL reconstruction, with or without TTO, in patients with recurrent lateral patellar instability and high-grade trochlear dysplasia with minimal cartilage damage resulted in low redislocation and reoperation rates at a mean of 33 months. There were no knee range of motion limitations. The persistence of apprehension was evident in 8.5% of knees, and a J-sign of reduced severity was evident in 13.6% of knees. Disease-specific QOL scores (BPII 2.0) were significantly improved, with a large effect size. Despite the technical challenges, based on the results of this study, this technique should be considered as a component of surgical care for patellofemoral stabilization in carefully selected patients.
Footnotes
Acknowledgements
The authors thank and acknowledge the valuable support of the members and staff of the Banff Sport Medicine Foundation toward the successful completion of this research undertaking.
One or more of the authors has declared the following potential conflict of interest or source of funding: L.A.H. has received research funding from Smith & Nephew, Pendopharm, and ConMed; has received consulting fees from Smith & Nephew, Pendopharm, Sanofi, and ConMed; and holds stock or stock options in PrecisionOS. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.