
Abstract
Background:
Glenoid and humeral head bone defects are common in chronic shoulder instability. The talus, and more specifically, the subtalar joint, has been proposed as a unique allograft from which bipolar bone loss can be addressed. However, there are few biomechanical data or joint reconstruction analyses of the glenoid using the posterior facet of a subtalar joint allograft (STA).
Purpose:
To compare the contact mechanics of an STA versus a coracoid graft (Latarjet procedure) versus a distal tibial allograft (DTA) for anatomic glenoid reconstruction.
Study Design:
Controlled laboratory study.
Methods:
A total of 8 fresh-frozen, unpaired cadaveric specimens underwent repeated-measures biomechanical testing in 5 stages: native (intact) state, bone loss (30% glenoid bone defect), Latarjet procedure, glenoid reconstruction using a DTA, and glenoid reconstruction using an STA. A compressive load of 440 N was applied to the glenohumeral joint when the humerus was mounted to a dynamic tensile testing machine in 3 shoulder positions: 30° of abduction, 60° of abduction, and 60° of abduction with 90° of external rotation (ER). Average contact pressure, contact area, and peak contact pressure were determined from the sensors. Surface area and surface congruency were calculated using a custom script. Data were analyzed using analysis of variance.
Results:
There was a significantly higher surface area with glenoid reconstruction using the DTA (859 ± 78 mm2; P = .005) than with glenoid reconstruction using the STA (806 ± 88 mm2; P < .001) and the Latarjet procedure (692 ± 91 mm2). Surface congruency was significantly better with reconstruction using the DTA (2.0 ± 0.3 mm; P = .003) or the STA (1.9 ± 0.3 mm; P = .004) than with the Latarjet procedure (2.6 ± 0.4 mm). In all shoulder positions, the average contact pressure in the bone loss state was significantly higher than that in the native state (P < .05). All repair states restored average contact pressure to the native state at 60° of abduction and 60° of abduction with 90° of ER. There was less contact area after the Latarjet procedure than in the native state at 30° and 60° of abduction (P = .009 and P = .040, respectively). There was no significant difference in contact area and peak contact pressure after reconstruction with the DTA or STA compared with the native state.
Conclusion:
Anatomic glenoid reconstruction using a DTA or STA restored average contact pressure, peak contact pressure, and contact area at 60° of abduction and 60° of abduction with 90° of ER in a cadaveric model. In addition, surface congruency and surface area improved over the traditional Latarjet procedure.
Clinical Relevance:
The STA showed comparable contact mechanics and surface geometry to the DTA. Further research is needed to determine the in vivo clinical outcomes of this new alternative graft.
Keywords
Erosion of the anterior glenoid rim is commonly associated with anterior glenohumeral instability, and it is considered a risk factor for recurrent instability after shoulder stabilization procedures. 5 Multiple bony reconstruction techniques have been developed to address glenoid bone loss (GBL), including the coracoid process, iliac crest, or distal tibia, such as the distal tibial allograft (DTA).15,17,24 Proponents of the Latarjet procedure cite the “triple blocking effect” as a reason for its success. 21 Specifically, the sling effect helps to restore stability and results in bony reconstruction. 10 Previous literature has reported good clinical outcomes after the Latarjet procedure for short- to long-term periods.14,21 However, the Latarjet procedure is nonanatomic and noncartilaginous and is associated with unique complications such as nonunion, osteolysis, and coracoid fractures as well as technical difficulties if revision surgery is required. 12 Furthermore, there are still some concerns with the risk of progression to instability arthropathy or osteoarthritis. 4
Exploring reconstruction techniques with free bone block transfer, the iliac crest autograft is a valid and safe option in the short term for substantial GBL. However, it has been associated with the considerable risk of recurrent instability, nonunion, graft lysis, and persistent pain at the donor site. 20 For this reason, alternative allograft options, such as the DTA, iliac crest allograft, or femoral head allograft, were introduced for anatomic glenoid reconstruction. 30 Recent systematic reviews have shown comparable outcomes and complications between free bone block autografts and allografts for managing GBL.9,30 Among free bone block techniques, the DTA has demonstrated many clinical and biomechanical advantages, including the absence of donor site morbidity, repair of a significant glenoid defect, excellent articular congruency with the humeral head, and the restoration of native glenohumeral biomechanics, and is a robust treatment option after a failed Latarjet procedure.23,24,26 However, there are limited studies on long-term outcomes and availability of different grafts in some areas of the world. The osteochondral allograft of the talus has been proposed as an optimal graft choice for humeral head reconstruction7,13,19 and with which bipolar bone loss at the humerus and glenoid can be addressed simultaneously. An anthropometric analysis was performed that showcased a surface similar to the native humeral head's superior dome and a radius of curvature of the subtalar joint that perfectly matched that of the previously validated DTA. 13 Additionally, the features and characteristics of the subtalar joint were found to be similar to those of the glenoid bone.
However, to date, there is a paucity of biomechanical data or surface analyses regarding the effects of a subtalar joint allograft (STA) in glenoid reconstruction. Therefore, this study aimed to compare the contact mechanics and surface profiles of the posterior facet of the STA, a new alternative graft option for anatomic glenoid reconstruction, with a coracoid graft (Latarjet procedure) and a DTA. It was hypothesized that anatomic glenoid reconstruction using an STA would provide contact mechanics and surface profiles similar to those with reconstruction using a DTA and would be superior to the Latarjet procedure with a coracoid graft.
Methods
Specimen Preparation
A total of 8 fresh-frozen, unpaired cadaveric shoulders (mean age, 51.7 years [range, 53-63 years]; 4 female, 4 male) were assessed in this study. The specimens used were donated to a tissue bank for medical research and purchased by our institution. Using cadaveric specimens does not require institutional review board approval at our institution. Specimens were excluded if they were aged >65 years and there was any history of injuries, surgery, osteoporosis, osteoarthritis, or any other shoulder joint abnormalities. The shoulders were thawed at room temperature overnight before testing. All skin, subcutaneous tissue, and muscles were dissected to the glenohumeral joint. The capsule was identified and sharply excised to expose the humerus and glenoid with the labrum. The scapula was potted in polymethyl methacrylate (PMMA; Fricke Dental) with the glenoid positioned parallel to the floor to ensure that the joint experienced compressive loads rather than shearing forces during testing. The corresponding humeral shaft was also potted in a cylindrical mold using PMMA.
Study Design
A repeated-measures experimental design was employed to adequately compare the contact mechanics and surface geometry of the native (intact) state, a bone loss state (30% anterior glenoid bone defect), the Latarjet procedure state, a reconstruction state using a DTA, and a reconstruction state using an STA. The native and bone loss states were tested first and second, respectively, and the Latarjet procedure and reconstruction states were tested in a randomized order.
Surgical Technique
One certified orthopaedic sports medicine surgeon performed the surgical procedures for all specimens (P.G.). Below are descriptions for each stage of this study.
(1) Native (intact) state (Figure 1A).
(2) Bone loss state: A digital caliper was used to measure the anterior-posterior and superior-inferior diameters of the glenoid with the labrum attached. Dimensions were obtained based on viewing the glenoid as a clock, with the superior portion of the glenoid equivalent to 12 o'clock. To simulate a critical-sized glenoid defect, a 30% glenoid defect (maximum width of anterior-posterior diameter) was planned and cut from the 3-o’clock position (right shoulder) parallel to the long axis of the glenoid using an oscillating saw. 25 We chose 30% of the glenoid bone defect because it represents severe GBL that is indicated for glenoid reconstruction using the free bone block technique 25 (Figure 1B).
(3) Latarjet procedure: A coracoid graft was harvested at 23 mm proximal to the anterior tip of the coracoid process using an oscillating saw. The inferior edge of the coracoid was corticated to facilitate graft fixation. Next, the coracoid bone block was placed flush with glenoid cartilage as much as possible and then was fixed in the traditional 3- to 5-o’clock position (right shoulder and superior position) using two 3.75-mm cannulated, partially threaded titanium screws (Arthrex) (Figure 1, C and D).
(4) Anatomic glenoid reconstruction using a DTA: A fresh DTA (JRF Ortho) was prepared using a technique described by Liles et al. 18 The DTA was prepared at the lateral surface with a 10° angle cut to restore the normal curvature of the glenoid using a workstation (Arthrex) (Figure 2A). The graft size was 10 mm wide and 23 mm long (Figure 2B). After graft preparation, the DTA was fixed to the glenoid bone and placed flush with articular cartilage of the glenoid to achieve an anatomic position using two 3.75-mm cannulated, partially threaded titanium screws (Arthrex) (Figure 2, C and D).
(5) Anatomic glenoid reconstruction using an STA: A fresh STA (JRF Ortho) was prepared using the same technique as described above (Figure 3, A and B). The graft size was 10 mm wide and 23 mm long. Next, the STA was placed flush with articular cartilage of the glenoid in the same manner and fixed using two 3.75-mm cannulated, partially threaded titanium screws (Arthrex) (Figure 3, C and D).
For every state of glenoid reconstruction, the surgeon checked and secured the fixation site before surface analysis and biomechanical testing.
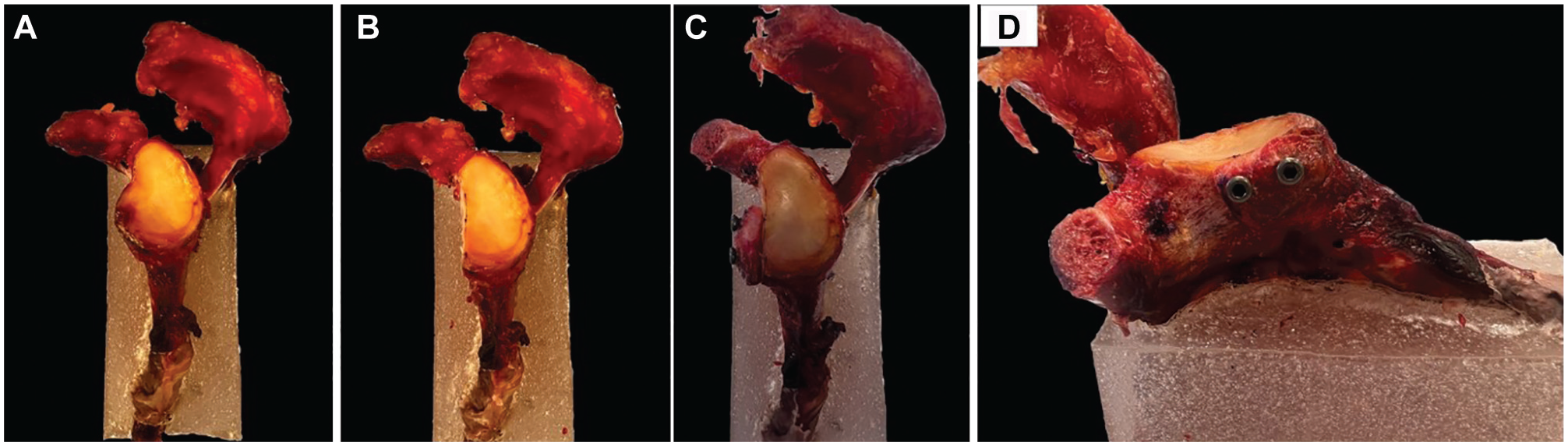
The surgical technique in a left cadaveric shoulder during each stage. (A) Anteroposterior (AP) view of the intact glenoid in the native state. (B) Creation of a critical-sized glenoid defect (30% glenoid defect) in the bone loss state. (C) AP view and (D) lateral view of the Latarjet procedure: the coracoid bone block (23 mm in size) was fixed and placed flush with the glenoid (traditional 3- to 5-o’clock position) using two 3.75-mm cannulated, partially threaded titanium screws.
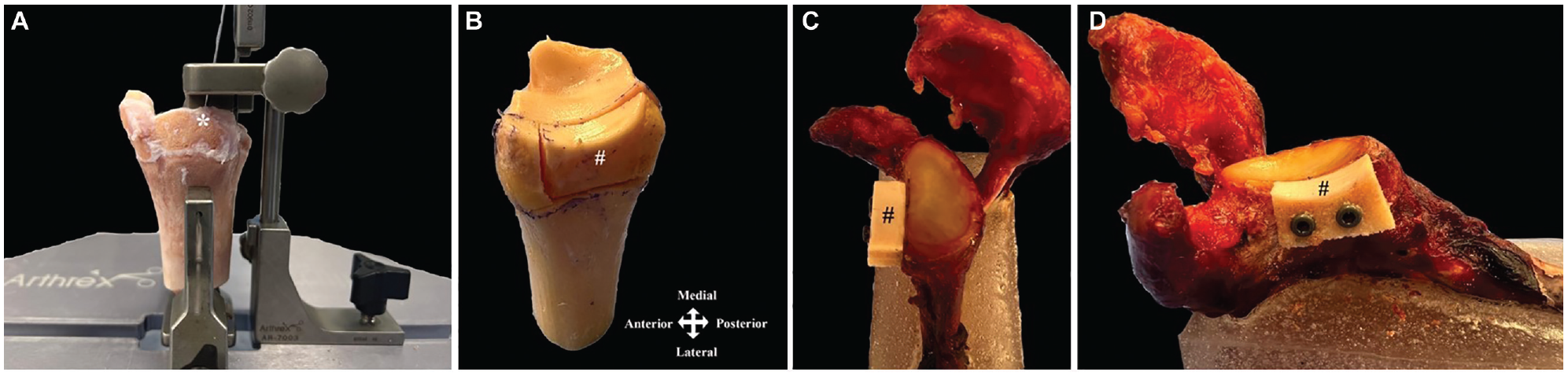
The distal tibial allograft (DTA) in a left cadaveric shoulder. (A) The DTA was prepared at the lateral surface with a 10° angle cut (*) to restore the normal curvature of the glenoid using a workstation. (B) The graft size was 10 mm wide and 23 mm long (#). (C) Anteroposterior view and (D) lateral view of anatomic glenoid reconstruction using the DTA: the DTA was fixed using two 3.75-mm cannulated, partially threaded titanium screws.
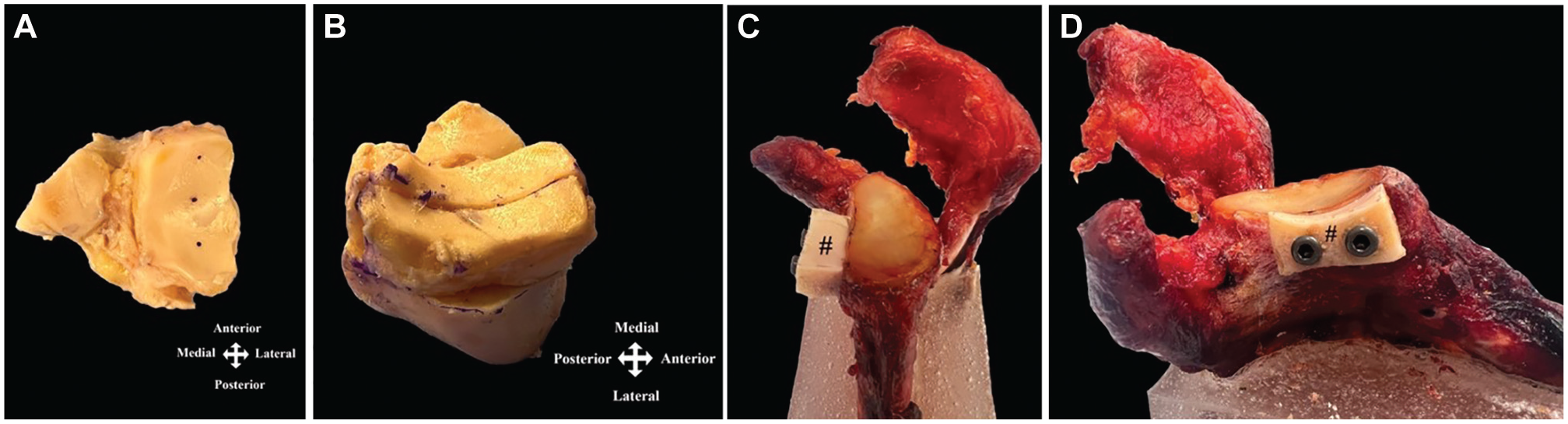
The subtalar joint allograft (STA) in a left cadaveric shoulder. (A) The inferior surface of the STA had a similar morphology as the glenoid surface. (B) The STA was prepared the same as the distal tibial allograft, with a size of 10 mm wide and 23 mm long. (C) Anteroposterior view and (D) lateral view of anatomic glenoid reconstruction using the STA (#): the STA was fixed using two 3.75-mm cannulated, partially threaded titanium screws.
Surface Analysis
The border of the glenoid was defined by creating fiducial markers inferoposterior, inferoanterior, and superoanterior of the glenoid. Another fiducial marker was created on the acromion. The scapula was explanted from the humerus and rigidly secured to a fixture adjacent to the laser scanner. The 4 fiducial markers for each testing state were digitized with the point tip of a coordinate measuring machine (Romer Absolute Arm; Hexagon) to define the global location of the glenoid relative to the coordinate frame of the machine. With the scapula still rigidly secured to the fixture, a laser scanner attachment for the Romer Absolute Arm (HP-L-8.9; manufacturer-reported accuracy, 0.04 mm; Hexagon) was used to record a 3-dimensional digitized point cloud of the glenoid surface in the same coordinate frame of the machine. This process was repeated for each testing state.
The laser scanning data were processed using custom software (MATLAB Version R2021a; The MathWorks) script. All point clouds were trimmed to the marked boundaries of the glenoid surface. The point cloud computed the surface area for each specimen and testing state. To determine the surface congruency of the bone loss state, the Latarjet procedure state, and the reconstruction states relative to the intact state, the point cloud of each nonintact testing state was registered to the point cloud of the intact state using an iterative closest point algorithm. Surface congruency was calculated as the root mean square deviation in normal distance between registered points from the nonintact specimen to the intact specimen. A reconstruction surface that is perfectly congruent to the intact surface would yield a root mean square deviation of zero. The higher the root mean square deviation, the worse the congruency between surfaces.
Biomechanical Testing
The potted humerus was secured within a custom fixture that enabled the humerus’ position to be adjusted during testing. This fixture was clamped to the base platform of a dynamic tensile testing system (ElectroPuls E10000; Instron) with the potted scapula secured to the end effector of the testing system. Using a handheld goniometer, the researcher positioned the specimen such that the glenoid would be loaded with pure compression toward the anterior portion of the glenoid and the humerus would be in neutral flexion (Figure 4). Testing was repeated with the humerus in 3 positions relative to the scapula, and the order of testing these positions was randomized:
(1) 30° of abduction (neutral internal/external rotation) with the bicipital groove oriented anteriorly,
(2) 60° of abduction (neutral internal/external rotation) with the bicipital groove oriented anteriorly, and
(3) 60° of abduction with 90° of external rotation (ER).
A thin, flexible electronic pressure sensor (K-Scan Model 5051; 5000 psi; Tekscan) was inserted between the humeral head and the glenoid. The anterior and posterior ends of the sensor were sutured and tethered to screws anchored to the humerus to ensure consistent placement of the sensor during all trials and the reproducibility of pressure measurements. The sensor allowed the measurement of pressure from 0.1 to 35 MPa with an accuracy of 0.1 MPa. The sensor was 0.1 mm thick, comprising a sensing area of 55.9 × 55.9 mm and a spatial resolution of 0.1 mm. The sensor was calibrated by performing manufacturer-defined adjustments at 20% and 80% of the expected maximum pressure. A power calibration was performed per the manufacturer's specifications. A new pressure sensor was utilized for each specimen.
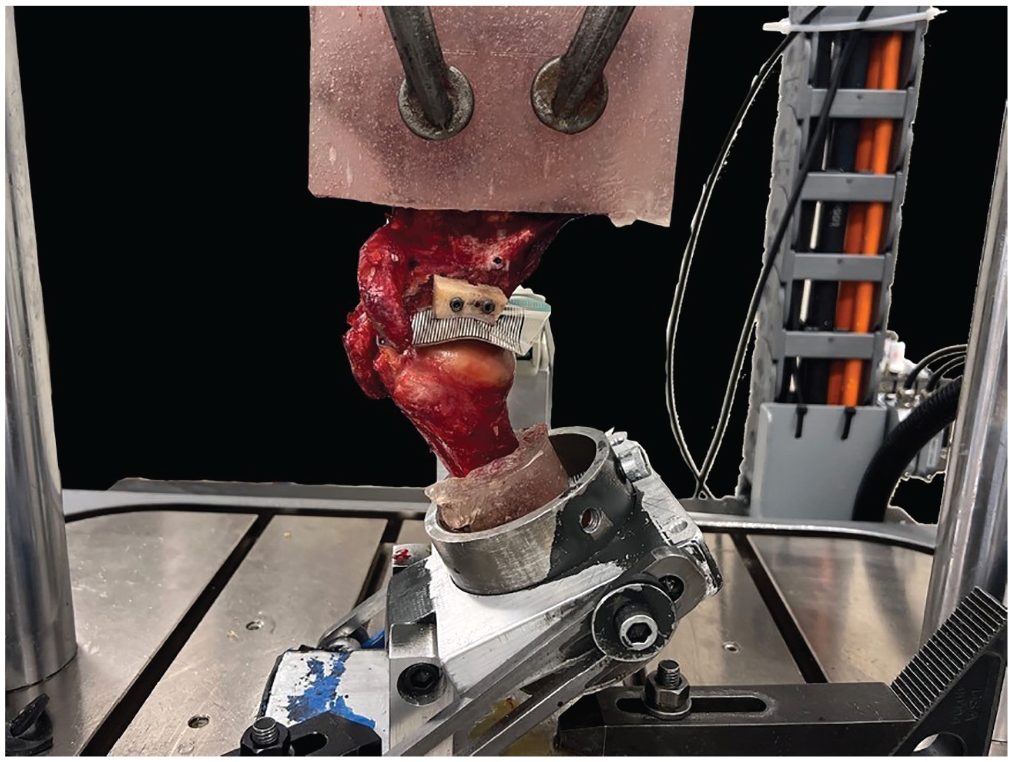
Biomechanical testing. The potted humerus was secured within a custom fixture that enabled the humerus’ position to be adjusted during testing. This fixture was clamped to the base platform of a dynamic tensile testing system. A thin, flexible electronic pressure sensor was inserted between the humeral head and the glenoid.
The dynamic tensile testing system applied a compressive load of 440 N to the joint at a rate of 44 N/s and held this load for 30 seconds. This served as an approximate maximum load for the simulation of in vivo glenohumeral loading conditions during the shoulder's range of motion in activities of daily living. 8 Average contact pressure, peak contact pressure, and contact area were recorded. This process was repeated for each humerus position and each testing state, with the humerus in the same position for all testing states.
Statistical Analysis
A power analysis (G*Power 3.1; Heinrich Heine University Düsseldorf) based on the data from a previous study by Frank et al 6 showed that 8 specimens were required to make pairwise comparisons between groups (effect size f = 1.42; power = 0.8; α = .05). In this study, the primary outcomes were average contact pressure (MPa), contact area (mm2), and peak contact pressure (MPa). The data were assessed for a normal distribution using the Shapiro-Wilk test. The mean and standard deviation were used to describe continuous data. Also, 2-way repeated-measures analysis of variance was conducted to evaluate (1) whether there was a significant interaction between states (ie, native, bone loss, Latarjet, DTA, and STA) and shoulder positions (ie, 30° of abduction, 60° of abduction, and 60° of abduction with 90° of ER) for the outcome variables and (2) the effects of states and shoulder positions on the outcome variables. If the P value was <.05, a pairwise comparison of the means was conducted using the Bonferroni method. Statistical analyses were performed using R (Version 4.3.1; R Foundation for Statistical Computing). P < .05 was considered to be statistically significant.
Results
Surface Analysis
Surface analysis of the glenoid in the bone loss state exhibited a significantly lower surface area compared with the other states. Anatomic glenoid reconstruction using the DTA showed a significantly higher surface area than that in the native state. However, there was no significant difference in the surface area between the native state and after the Latarjet procedure as well as after anatomic glenoid reconstruction using the STA. In addition, there was a significantly higher surface area in the DTA state compared with the STA and Latarjet procedure states (Figure 5A).
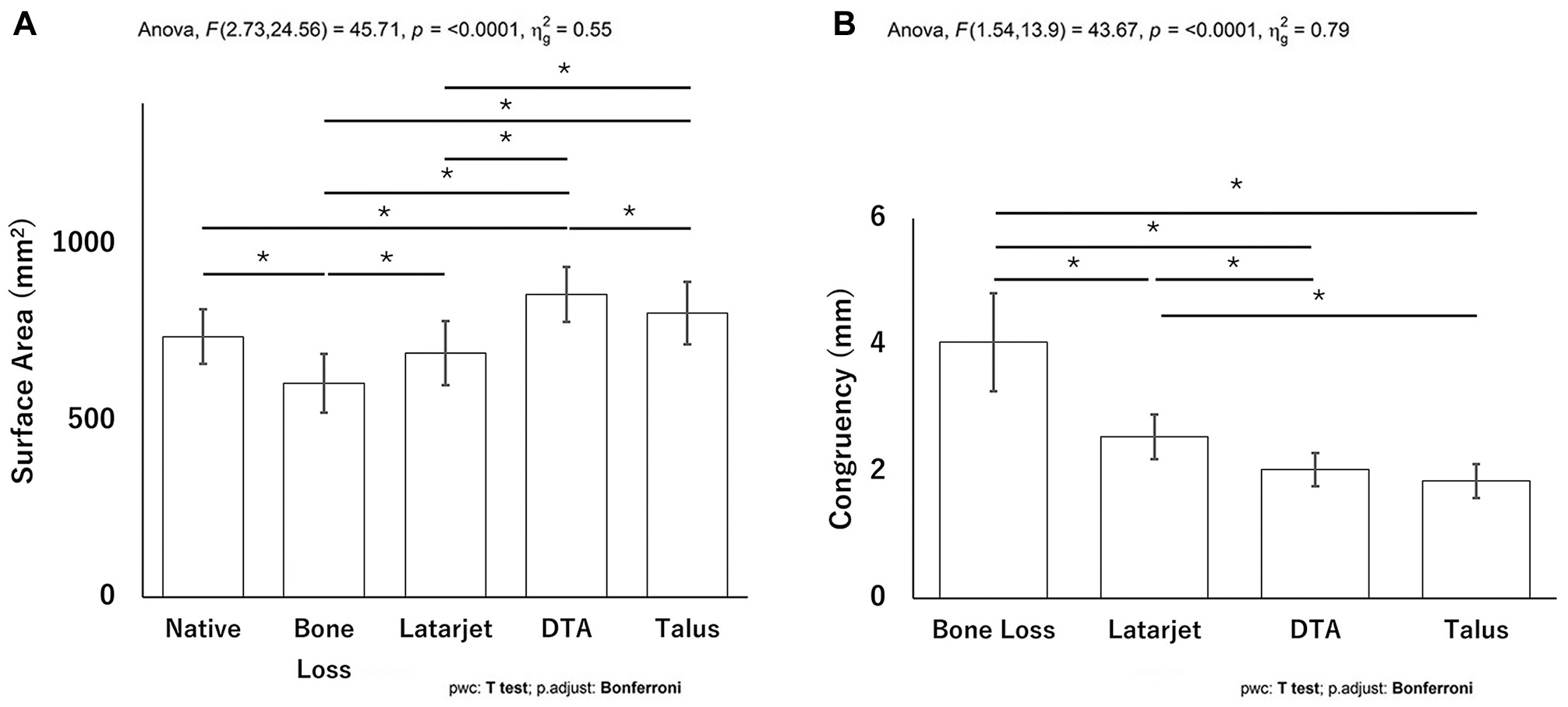
(A) Surface area (mm2) and (B) surface congruency (mm) in the different stages of the study: native, bone loss, Latarjet procedure, distal tibial allograft (DTA), and subtalar joint allograft (STA). The asterisk (*) denotes a statistically significant difference between 2 states (Bonferroni test for pairwise comparisons).
There was improved surface congruency after the Latarjet procedure, reconstruction using the DTA, and reconstruction using the STA compared with the bone loss state. Moreover, anatomic glenoid reconstruction using the DTA or STA yielded improved surface congruency over the Latarjet procedure. However, there was no significant difference in surface congruency between the DTA and STA states (Figure 5B).
Average Contact Pressure
The average contact pressure, contact area, and peak contact pressure in all states and all shoulder positions (30° of abduction, 60° of abduction, and 60° of abduction with 90° of ER) are listed in Appendix Table A1 (available in the online version of this article). In all shoulder positions, the average contact pressure in the bone loss state was significantly higher than that in the native state. At 30° of abduction, the average contact pressure was significantly increased after the Latarjet procedure and reconstruction using the STA; however, there was no significant difference compared with reconstruction with the DTA. The study exhibited no significant difference in average contact pressure after the Latarjet procedure, reconstruction using the DTA, or reconstruction using the STA compared with the native state at 60° of abduction and 60° of abduction with 90° of ER (Figure 6).

Bar chart showing the mean and standard deviation of the average contact pressure (MPa) in different states at each flexion angle. The asterisk (*) denotes a statistically significant difference between 2 states (Bonferroni test for pairwise comparisons).
Contact Area
There was a significantly decreased contact area in the bone loss state compared with the native state in all shoulder positions (30° of abduction, 60° of abduction, and 60° of abduction with 90° of ER). The study exhibited less contact area after the Latarjet procedure than in the native state at 30° and 60° of abduction. In addition, there was no significant difference in the contact area between the native state and after anatomic glenoid reconstruction with either the DTA or STA (Figure 7).

Bar chart showing the mean and standard deviation of the contact area (mm2) in different states at each flexion angle. The asterisk (*) denotes a statistically significant difference between 2 states (Bonferroni test for pairwise comparisons).
Peak Contact Pressure
The study showed significantly increased peak contact pressure in the bone loss state and after the Latarjet procedure compared with the native state at 60° of abduction. Overall, there was no significant difference in peak contact pressure between the native state and after anatomic glenoid reconstruction with the DTA or STA (Figure 8).
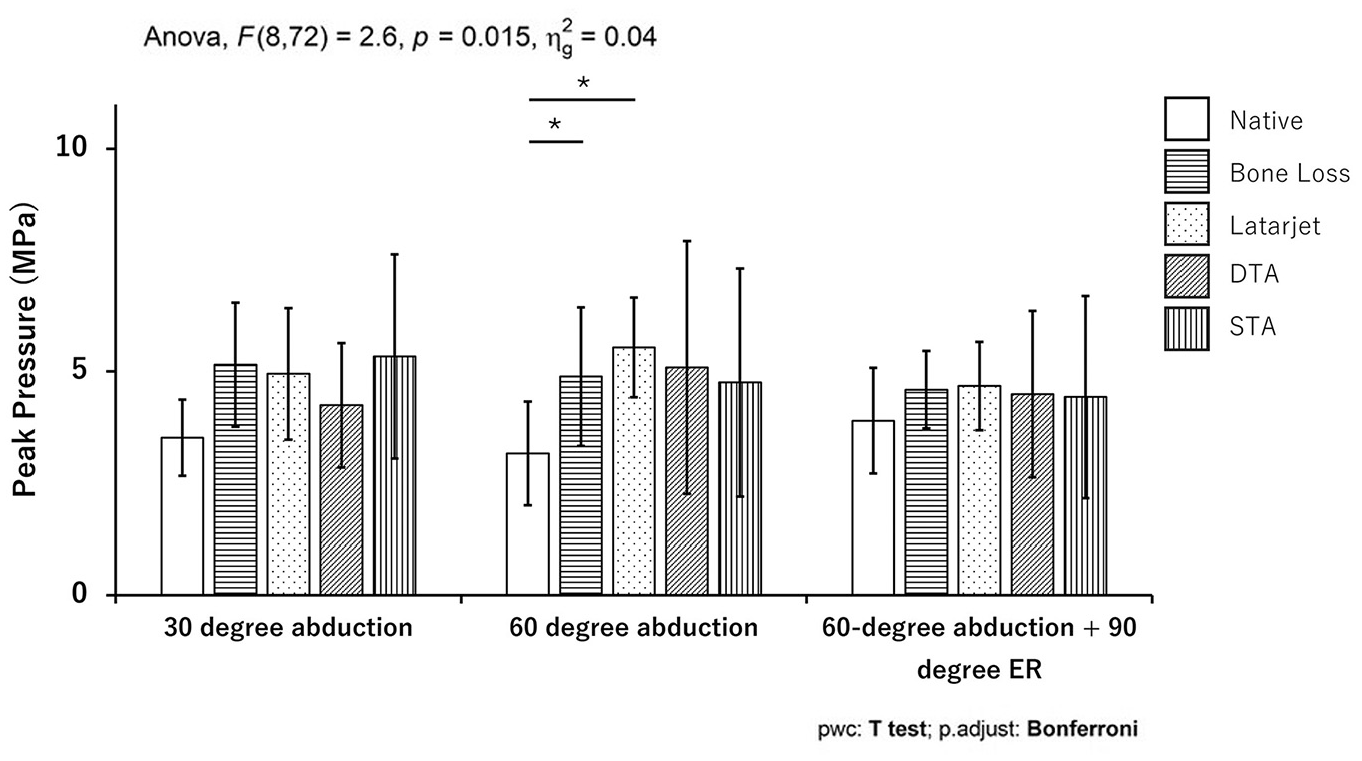
Bar chart showing the mean and standard deviation of the peak contact pressure (MPa) in different states at each flexion angle. There was a statistically significant interaction between states and flexion angles for peak contact pressure according to 2-way repeated-measures analysis of variance. The asterisk (*) denotes a statistically significant difference between 2 states (Bonferroni test for pairwise comparisons).
Discussion
The study's most important findings were that the Latarjet procedure and anatomic glenoid reconstruction using an STA restored the physiological surface area, while reconstruction using a DTA resulted in a supraphysiological surface area in a cadaveric model. Furthermore, reconstruction with a DTA and STA improved surface congruency over the Latarjet procedure. Moreover, while all stabilization techniques substantially improved average contact pressure compared with the defect condition, reconstruction using the DTA was most favorable in maintaining the average contact pressure similar to the native state, particularly in lower degrees of abduction. Additionally, reconstruction with the DTA and STA preserved the contact area, similar to the native state, better than the Latarjet procedure. Finally, the Latarjet procedure induced a higher peak contact pressure at 60° of abduction compared with the native state. This finding may be because, in the Latarjet procedure state, poor congruency of the coracoid graft to the native humeral head may lead to humeral head contact on the coracoid and on a smaller posterior region of the native glenoid. In these cases, the contact area between the humerus and glenoid decreases, and contact pressure increases from the native state and even, for 1 specimen in this study, from the bone loss state. The DTA and STA reconstruction states were not significantly different from the native state.
Historically, the Latarjet procedure has demonstrated favorable outcomes in addressing critical GBL; more recently, alternative autograft techniques involving free bone block transfer, such as iliac crest autografts, distal clavicle autografts, or scapular spine autografts, have been explored.16,28 However, these grafts have the inherent limitation of not reconstructing the cartilaginous surface of the native glenoid, which may be attributed to the premature onset of postoperative osteoarthritis. 28 Recent studies have explored allografts in providing a cartilaginous surface, such as the DTA and the STA.7,13,23 The STA is of particular interest because of its potential for simultaneous use in cases of concurrent humeral head bone loss and GBL with a single graft, which are highly prevalent in patients with primary instability (33%) as well as recurrent instability.13,22 While there exists a paucity of biomechanical data on surface area, contact area, contact pressure, and surface congruency of the STA, reconstruction using an STA for bipolar bone loss theoretically addresses a clinically significant challenge by reducing the costs associated with using 2 separate allografts.
A detailed analysis of the surface area in the present study indicated that the DTA state demonstrated the highest surface area, surpassing physiological levels. This finding aligns with previous research, which has shown that glenoid reconstruction with a DTA yields a significantly larger glenohumeral contact area than the Latarjet procedure with coracoid bone blocks in both 60° of abduction and the ABER (abduction and ER) position. 2 Interpreting these results, the supraphysiological surface area with reconstruction using the DTA may have mixed implications. While it may imply more robust initial reconstruction, there is concern regarding potential friction in the subscapularis tendon during anterior glenoid reconstruction. However, this may have limited clinical significance compared with the Latarjet procedure, which has been associated with notable radiographic structural changes, including marked thinning, rerouting of the subscapularis tendon, and slight fatty degeneration of the muscle, which clinically may translate into a decline in internal rotation after the Latarjet procedure. 27 Additionally, the Latarjet procedure may alter the position of the scapula because of pectoralis minor tenotomy and transfer of the conjoint tendon, and dissection of the coracoacromial ligament during the Latarjet procedure may lead to increased superior translation of the humeral head. 29
Analysis underscored the efficacy of bone block stabilization procedures, which restored the average contact pressure to the native state at 60° of abduction and 60° of abduction with 90° of ER. This is particularly relevant, given that previous studies have shown that anteroinferior glenohumeral contact pressure increases by 300% to 400% in the setting of 30% glenoid defects. 11 This high contact pressure may predispose to focal loading and early-onset osteoarthritis, as evidenced by findings of glenohumeral arthritis in patients undergoing the Latarjet procedure. Mizuno and colleagues 21 found that at a mean follow-up time of 20 years, 23.5% of patients undergoing the Latarjet procedure had developed glenohumeral arthritis. The fact that reconstruction using the DTA maintained an average contact pressure similar to the native state, particularly in lower degrees of abduction, emphasizes potentially superior biomechanical performance over the Latarjet procedure. 2 Our study showed a similar trend for peak contact pressure in which the Latarjet procedure induced higher peak contact pressure than reconstruction using the DTA or STA. These findings might be explained by the fact that the DTA and STA possess a robust cartilaginous surface that is highly congruent with the area of GBL.13,24 Regarding surface congruency, reconstruction with the DTA and STA provided superior biomechanical results compared with the Latarjet procedure, which might improve the ability to restore the native anatomy and biomechanics of the glenoid more closely. 24 These findings align with previous anthropometric studies, which have demonstrated glenoid-like morphological characteristics of these grafts, with a radius of curvature of the STA of 21.51 ± 2.30 mm and a radius of curvature of the DTA of 22.8 ± 3.3 mm, resulting in an acceptable fit in 94% of cases. 3
In terms of the clinical implications of these findings, it has to be acknowledged that there is long-standing clinical experience and outcome data for the Latarjet procedure demonstrating sustained long-term success and favorable return-to-play rates of up to 94%.1,14,21 Similarly, while a newer technique, clinical outcomes after reconstruction using a DTA have been positive, indicating favorable restoration of glenohumeral stability and biomechanics with few complications.9,18,26 The findings of this study in regard to reconstruction with an STA warrant further exploration, especially in cases of bipolar bone loss in which a single graft could be utilized, potentially reducing costs and enhancing graft availability. However, special considerations must be addressed regarding graft harvesting. Donors with posttraumatic, osteoarthritic, or surgical changes to the distal tibia around the midfoot or hindfoot may have to be excluded.
The current study had several limitations. First, there was no active or passive loading on the rotator cuff or the periscapular muscles to reflect in vivo muscle activity. Second, as this was a cadaveric study, the compliance of soft tissue, particularly the glenohumeral capsule, may be different than in vivo. In addition, the thickness and biomechanical properties of the capsule may be different between specimens. It is difficult to standardize and may allow for variability in results. Third, we removed all soft tissue such as the capsulolabral complex and ligament, and there was no load applied to the conjoint tendons to simulate the sling effect of the Latarjet procedure. Fourth, we made a vertical glenoid cut to create the bone defect to reduce bias; however, this may not be representative of a true glenoid bone defect. Furthermore, the humerus was loaded in pure compression in the same anterior portion of the glenoid through all testing states, and the contact location was not changed for the humerus’ position, which is not physiological. Finally, the parameters measured reflect conditions at time zero and do not account for any remodeling of the cartilage surface or block resorption. Additional in vivo studies may be beneficial to understand the effects such as stability, in vivo resorption, outcomes, or risk of failure.
Conclusion
Anatomic glenoid reconstruction using the DTA or STA restored average contact pressure, peak contact pressure, and contact area at 60° of abduction and 60° of abduction with 90° of ER. In addition, surface congruency and surface area improved over the traditional Latarjet procedure. The STA showed comparable contact mechanics and surface geometry to the DTA. Further research is needed to determine the in vivo clinical outcomes of this new alternative graft.
Supplemental Material
sj-pdf-1-ajs-10.1177_03635465251315487 – Supplemental material for Biomechanical Evaluation and Surface Analysis of Glenoid Reconstruction Using a Subtalar Joint Allograft for Significant Glenoid Bone Loss in Recurrent Shoulder Instability: A Novel Alternative Graft Option
Supplemental material, sj-pdf-1-ajs-10.1177_03635465251315487 for Biomechanical Evaluation and Surface Analysis of Glenoid Reconstruction Using a Subtalar Joint Allograft for Significant Glenoid Bone Loss in Recurrent Shoulder Instability: A Novel Alternative Graft Option by Phob Ganokroj, Justin F.M. Hollenbeck, Marco Adriani, Ryan J. Whalen, Amelia H. Drumm, Alexander R. Garcia, Wyatt H. Buchalter, Trevor J. McBride, Marco-Christopher Rupp and CAPT Matthew T. Provencher in The American Journal of Sports Medicine
Footnotes
Acknowledgements
The authors thank the Steadman Philippon Research Institute's digital media team for the illustrations and Ms Narumol Sudjai from Siriraj Hospital, Faculty of Medicine, Mahidol University, for statistical analysis.
Submitted June 13, 2024; accepted December 2, 2024.
One or more of the authors has declared the following potential conflict of interest or source of funding: M.T.P. has received royalties from Arthrex, Arthrosurface, Responsive Arthroscopy, and Anika Therapeutics; consulting fees from Arthrex, the Joint Restoration Foundation, Zimmer Biomet, and Arthrosurface; grants from the United States Department of Defense, the National Institutes of Health, and DJO; and honoraria from Flexion Therapeutics. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.