
Abstract
Background:
Recent biomechanical evidence for adjustable suture anchor (ASA)–based posterior medial meniscus root (PMMR) fixation has shown promising results compared with conventional transtibial pull-out repair (TPOR). However, ASA fixation has not been evaluated in human tissue to 100,000 cycles.
Hypothesis:
ASA repair would lead to increased primary fixation strength and less cyclic displacement than conventional TPORs.
Study Design:
Controlled laboratory study.
Methods:
A total of 32 human medial menisci were used, 8 of which were intact specimens and served as native controls. For the others, PMMR tears were created and repaired using 3 different techniques (n = 8 group). Two conventional PMMR repairs were prepared consisting of two No. 2 simple sutures (TSS) and two No. 2 sutures in a Mason-Allen (MA) configuration, all tied over a cortical button. The knotless ASA repair was fixed in MA with repair sutures tensioned at 120 N (MA-120). The repairs’ initial force, stiffness, and relief displacement from the tensioned state toward repair unloading (2 N) were measured after fixation. All repair constructs were loaded for 100,000 cycles, with displacement and stiffness measured, and finally were pulled to failure.
Results:
The TPORs demonstrated similar primary fixation and cyclic loading behavior except for initial cyclic displacement (cycle 10). The ASA repair provided a higher initial repair load (P < .001) and stiffness (P < .001) with relief displacement similar to conventional TPORs. Lower initial cyclic displacement (P < .011; cycle 10) with overall higher repair stiffness (P < .011) resulted in significantly lower displacement (P < .001) throughout testing for ASA repair. Although both TPORs were completely loose after 100,000 cycles, the ASA repair achieved near-native dynamic meniscal stabilization. The TSS repair had lower overall ultimate load (P < .001) and ultimate stiffness (P < .023) compared with the ASA repair. All repairs had lower ultimate stiffness and loads than the native meniscus (P < .001).
Conclusion:
The ASA repair resulted in improved primary PMMR fixation that was stiffer with less cyclic displacement than conventional TPORs and approached that of the human meniscal function after 100,000 load cycles in a cadaveric model. However, all repair techniques had lower ultimate strength than the native human PMMR.
Clinical Relevance:
Knotless ASA meniscus root fixation resulted in higher tissue compression and less displacement in a cadaveric model; however, future clinical series with surveillance imaging will define the overall significance of healing rates.
Posterior medial meniscus root (PMMR) tears have been shown to adversely affect knee function by increasing contact stress and decreasing contact area.1,13,18,26 Untreated meniscus root tears are associated with meniscal extrusion, increased pain, and articular cartilage degeneration, leading to chondral lesion formation and subchondral insufficiency fracture similar to a functional, subtotal meniscectomy.17,19,38 The 2 most common techniques reported in the literature for PMMR fixation are transtibial pull-out repair (TPOR) and suture anchor repair to restore meniscal anatomy and function and prevent clinically observed degenerative joint changes.1,8,12,22
Previous biomechanical studies have quantified the stabilization potential of various PMMR repair techniques within a cyclic loading range of 1000 cycles.3,9,15,16,25,31-33 A recent porcine study demonstrated superior primary fixation with higher tissue compression and cyclic displacement to match the native menisci for a newly developed, tensionable, knotless adjustable suture anchor (ASA) providing aperture fixation in contrast to other TPORs. 3 Although using more homogeneous porcine tissue allows for better comparability of the test results, 14 the stiffer meniscus tissue and higher bone quality compared with human tissue may alter the results in terms of translating findings into clinical practice for direct relevance and understanding of clinical implications. 36 Furthermore, postoperative rehabilitation protocols suggest a period of 4 to 8 weeks of partial weightbearing for meniscal healing; longer term assessments would be warranted.28,37,39 Test protocols with more rehabilitative loading are required to provide qualitative evidence of the effect of prolonged cyclic loading on gradual deformation. 42 Although the meniscus-suture interface has been identified as the primary contributor to increased cyclic displacement, with the 2-simple suture (TSS) and Mason-Allen (MA) techniques having the most favorable biomechanical characteristics,10,15,25 the ASA implant has not been evaluated in weaker human tissues under prolonged cyclic loading. It is currently unknown whether the previously reported levels of primary fixation and displacement underestimate what would be observed biomechanically and clinically in humans and how the ASA repair compares to clinical conventional TPORs fixed in weaker bone.
This study aimed to evaluate and compare the initial repair load, stiffness, and relief displacement directly after fixation of the 2 most relevant, clinical, fixed TPOR techniques with knotless ASA fixation in a biomechanical, full-construct human model. In addition, the cyclic displacement and stiffness during prolonged repetitive loading over 100,000 cycles and the ultimate load and stiffness during pull-to-failure testing of all repairs were compared. It was hypothesized that primary PMMR fixation with the tensionable ASA implant would provide a higher initial repair load and greater resistance against displacement during cyclic loading than previously described conventional TPORs.
Methods
Specimen
A total of 32 paired fresh-frozen human cadaveric tibias with attached menisci (9 male and 7 female specimens; mean ± SD age, 57.7 ± 9.3 years) were provided by the Science Care donor bank. All tissues were frozen at −20°C and thawed at room temperature overnight before biomechanical testing. After soft tissue removal and axial sectioning of the tibia 14 cm below the joint line, the medial meniscus was visually inspected to ensure structural integrity with no noticeable macroscopic degenerative changes. Twelve paired human specimens were equally distributed in a balanced incomplete block design into 3 groups with no statistical difference in age for primary fixation and cyclic testing of various TPOR techniques of PMMR tears (Figure 1). Using a balanced incomplete block diagram is a statistical model that benefits from paired specimen similarity when analyzing 3 treatment groups. Eight additional samples were used for a reference native meniscus control group.
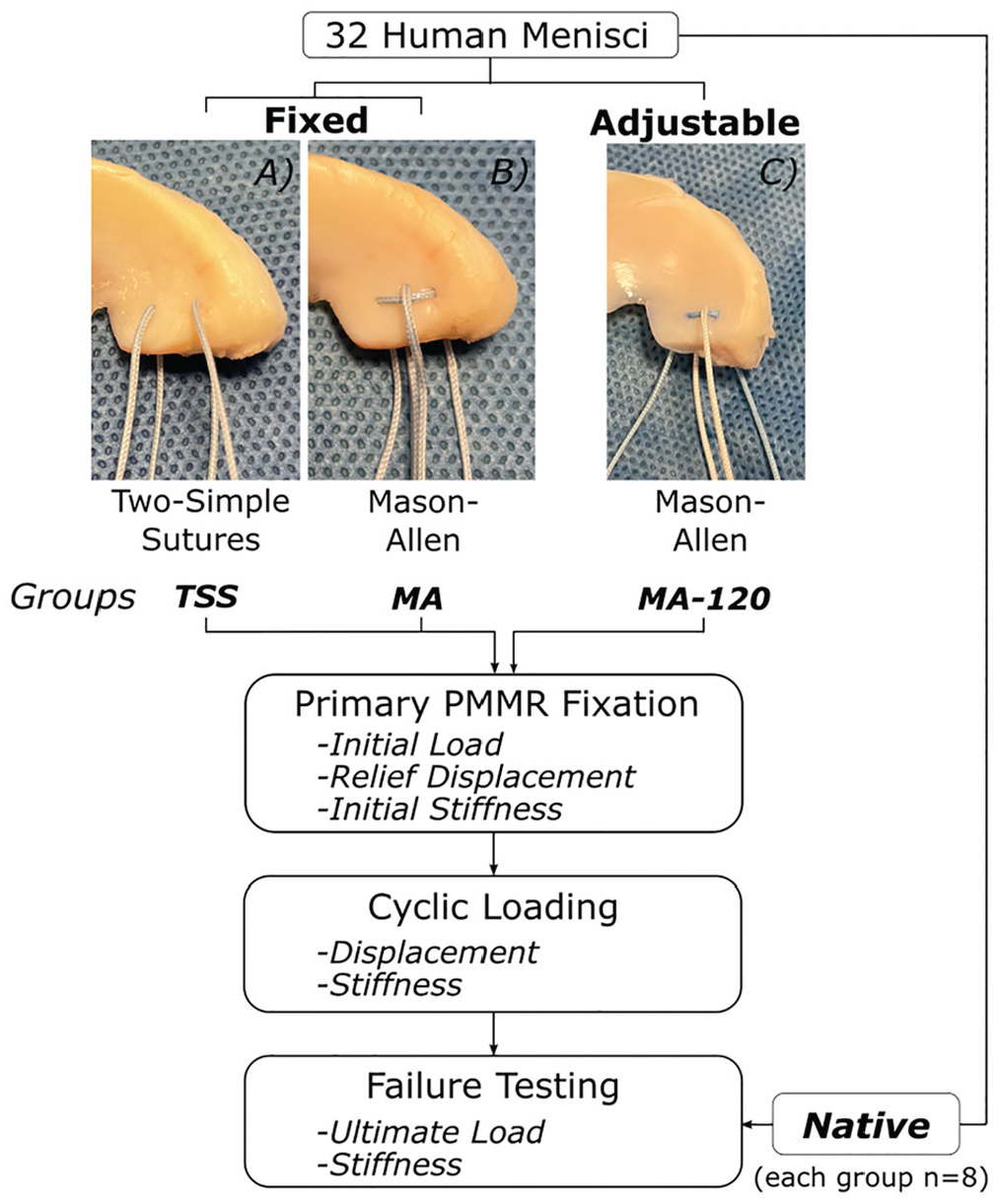
Schematic illustration of the 2 fixed groups (A, 2 simple sutures; B, Mason-Allen sutures) tied over a cortical button and the knotless adjustable suture repair (C, Mason-Allen sutures) with testing algorithm and outcome variables. PMMR, posterior medial meniscus root; MA, Mason-Allen; MA-120, MA with 120 N of tension applied during adjustable fixation; TSS, 2 simple sutures.
In native specimens, the medial menisci were detached from the tibia by dissection of the meniscocapsular tissue and the anterior meniscotibial ligament, leaving only the posterior meniscus root intact. In repair specimens, the menisci were released entirely from the tibia by additional cutting of the posterior meniscotibial ligament at 5 mm lateral to the margin of the posterior horn.
In all specimens, the medial tibial plateau was cut 1 cm medial to the PMMR insertion to provide sufficient space for the meniscus to be clamped. In repair specimens, a transtibial tunnel was created from the anterolateral cortex to the PMMR footprint using a drill guide and a 2.4-mm drill.3,16
The tibia was embedded in a custom-made aluminum cylinder using a bicomponent embedding material (RenCast; Huntsman Advanced Materials) in line with the tibia’s long axis and 3 cm distal to the predetermined exit of the tibial tunnel axis to leave sufficient space for suture repair knot tying. Specimens were kept moist with physiological saline solution during specimen preparation and testing.
Repair Techniques
Three different suture repair groups were prepared for biomechanical testing as previously described, including 2 fixed suture repairs (Figure 1, A and B) and 1 knotless, tensionable ASA repair implant (SutureLoc; Arthrex) (Figure 1C). 3 The conventional fixed TPOR techniques were selected because they are considered the most relevant clinical methods, with the lowest reported cyclic displacement for the TSS technique and the highest reported ultimate failure strength for the MA meniscus root fixation.15,25 The fixed MA group served as a reference group for the adjustable ASA group despite differences in the suture fixation method. A suture passer (Knee Scorpion; Arthrex) was used for suture shuttling through the meniscus to replicate the typical arthroscopic surgical technique.
For the TSS technique, two separate No. 2 nonabsorbable braided sutures (FiberWire; Arthrex) were stitched through the meniscus (Figure 1A). The locations for suture passing through the meniscus were defined as 5 mm medial to the lateral edge of the posterior meniscus horn, with 1 suture positioned adjacent to the meniscocapsular junction and the other suture positioned 5 mm more anteriorly.3,15
For the fixed MA technique, a horizontal mattress suture was created using a No. 2 nonabsorbable braided suture (FiberWire) with the suture loop portion on the superior meniscus surface. A second No. 2 nonabsorbable braided suture (FiberWire) was then passed through the meniscus just medial to and in the center of the horizontal suture loop (Figure 1B).
The adjustable MA repair technique used a double-loaded, all-suture anchor implant consisting of two No. 2 nonabsorbable repair sutures with corresponding shuttle sutures and a soft anchor with an anchor-deploying suture loop. The adjustable implant was retrieved via a transtibial drill hole and passed from proximal to distal but with the soft anchor positioned just below the proximal cortex. Pulling on the tibial-sided, anchor-deploying suture loop at 150 N using a digital force gauge (Mark-10 M7-50; Bronx-Systems) with slight initial manual countertension on the distal repair sutures locked the anchor sheath within the tibial tunnel beneath the tibial plateau for meniscus root fixation proximally, rather than distal suspensory fixation at the distal end of the tunnel with the other conventional TPOR techniques. A horizontal mattress suture was created with a first No. 2 nonabsorbable braided repair suture, and the second repair suture was stitched through the meniscus immediately medial to and in the center of the horizontal suture loop. The repair sutures were passed transtibially, with each corresponding shuttle suture passing through an integrated “Chinese finger” locking mechanism located within the anchor body. The repair suture tension was adjusted to reattach the meniscus root. All meniscus-suture configuration techniques were performed by the first author (S.B.).
Primary Fixation
A slotted aluminum metal plate (5 mm in thickness) with a central hole (2.4 mm in diameter) was secured by screw side-action grips (Instron) equipped with serrated grip jaw faces to the test machine actuator (ElectroPuls E10000; Instron). The embedded tibia was rigidly secured over a bottom mount to the baseplate with the transtibial tunnel aligned with the actuator axis (Figure 2A). An initial distance of 8 mm between the metal undersurface and bony surface allowed for measurement of the initial load on the repair and the impingement-free translation of the actuator to a relative repair unloading position of 2 N after fixation. 4 The repair sutures of the fixed groups were passed through the tibial tunnel and the holes of the tibial button (TightRope Button; Arthrex). After the suture-meniscus interface was preconditioned with a manual pull of 50 N for 5 seconds measured by the test machine’s load cell (1-kN; Instron), fixed TPORs were secured by manual knotting of 2 suture couples and the adjustable group by applying 120 N (MA-120) of tension to each loop-shortening strand using a digital force gauge (Mark-10 M7-50; Bronx-Systems). 3 Each suture couple was fixed with 4 alternating counteractive half-hitch knots over the button; the adjustable implant was kept knotless. In the MA configurations, the horizontal suture was fixed first. Preconditioning the suture-meniscus interface provided proper fixation conditions for comparative analysis and reduced settling effects before cyclic testing.
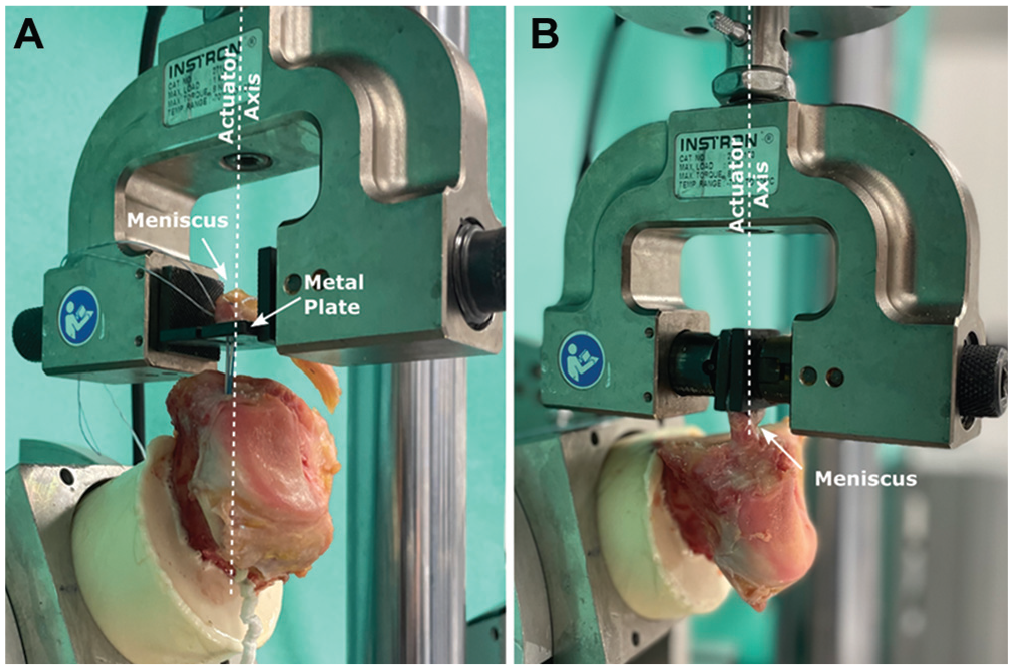
Biomechanical setup for (A) primary fixation of the transtibial pull-out meniscus root repair in line with the actuator axis and (B) cyclic loading applied aligned with the circumferential fibers of the meniscus.
As in a previous study, the initial load, relief displacement, and initial stiffness were defined as primary outcomes after final fixation. 3 The initial load quantified the tissue compression exerted by the suture repair. The actuator movement from the initial fixation state toward repair unloading until reaching a residual load of 2 N corresponds to the relief displacement. The initial stiffness represents the linear inclination between the initial load position and the loading point with 5 N of tension on the repair during construct unloading. All tests were performed at room temperature, and soft tissue was kept moist with a physiological saline solution.
Cyclic and Failure Testing
For cyclic testing, the meniscus root was reapproximated directly to the tibia, both oriented to clamp the peripheral portion of the medial meniscus 1 cm lateral to the repair sutures (repair groups) or the tibial insertion of the root ligament (native group) and to apply tensile loading in line with the circumferential fibers of the PMMR (Figure 2B). The meniscus was fixed in the same manner as for primary fixation, with suture knotting over the button for fixed groups or adjustable suture tensioning (120 N) using the digital force gauge. The specimen-protect feature of the test machine was activated during meniscal clamping with the screw side action grips to maintain a constant tension of 2 N on the repair. The same meniscus and knotless adjustable repair implant from the primary fixation were used for cyclic testing. Similar to the cyclic loading procedure in the previous study, 3 new repair sutures for the fixed groups were threaded with a needle through the same meniscal punctures so that the same meniscus could be used throughout the test as for the adjustable repair constructs.
After the specimen was precycled between 2 and 10 N for 10 cycles at 0.5 Hz, cyclic loading was applied at a test frequency of 1.5 Hz for 100,000 cycles between 5 and 30 N. The test parameters used in this study are consistent with those used in other studies evaluating the biomechanical performance of meniscal repair systems.3,5-7,11,27,34 A saline drip irrigation system maintained constant hydration during cyclic loading. The final load-to-failure test was performed at a rate of 0.5 mm/s. The native specimens were pulled to failure immediately after precycling to provide information about the ultimate strength and the time-zero native meniscal behavior in order to quantify and qualify the stabilization potential of various PMMR repairs. The load-displacement curves of all native specimens below the load threshold of 32 N were pooled to represent the native meniscal behavior. Native stiffness was determined within the linear portion of the load-displacement curve in a load range of 200 to 350 N.
Load-displacement data during cyclic loading and pull-to-failure testing were recorded continuously using data acquisition software (WaveMatrix; Instron) at a sampling rate of 750 Hz. Metrics for comparison data included cyclic displacement and stiffness at 10, 100, 1000, 10,000, 25,000, and 100,000 cycles and ultimate failure load with failure mode noted. Cyclic displacement represents plastic deformation (laxity) during force-controlled loading and is a relative valley measurement in relation to the test machine actuator position after precycling. Cyclic stiffness represents the linear slope of the hysteresis valley and peak data.
Statistical Analysis
Different suture repair techniques and devices were independent variables, and all metrics for comparison were dependent variables. Initial repair tension and stiffness, relief displacement, cyclic displacement and stiffness, and ultimate failure load and stiffness were primary outcome variables. A sample size of n = 8 was selected based on previous studies comparing the biomechanical performance of various PMMR repair techniques.3,16,25
Statistical analyses were performed using Sigma Plot Statistics for Windows, Version 13.0 (Systat Software). The statistical analysis included a 1-way analysis of variance (ANOVA) with a Holm-Sidak post hoc test performed for a significant pairwise analysis of primary outcome variables. Significance was defined as P≤ .05, and the desired power level was set at 0.8. The Shapiro-Wilks test confirmed that each data set followed a normal distribution. A nonparametric test (Kruskal-Wallis) was used for data sets that failed this test. For Kruskal-Wallis tests that found significance, a post hoc test according to the Dunn method was conducted to analyze the differences further.
Results
Primary Fixation
The initial repair load and stiffness with statistical analysis results are shown in Figure 3 for all repair groups. Overall, the fixed PMMR repairs demonstrated similar primary fixation behavior with lower (P < .001) initial repair load and initial stiffness compared with the ASA group. Nevertheless, the relief displacement of TSS (0.83 ± 0.18 mm) and MA (0.75 ± 0.20 mm) was similar to that of MA-120 (0.87 ± 0.22 mm), without significance.
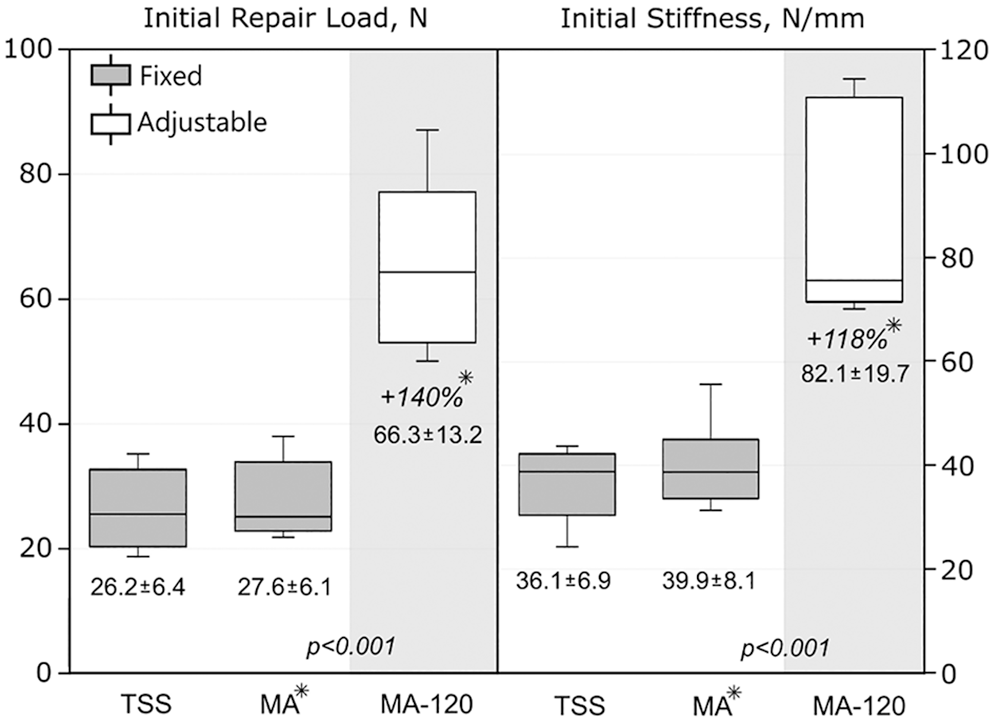
Boxplot with mean ± standard deviation values of initial repair load and stiffness, statistical analysis (different background shadings indicate statistical significance levels), and percentage deviation between adjustable and fixed Mason-Allen repair (asterisks with italic values). MA, Mason-Allen; MA-120, MA with 120 N of tension applied during adjustable fixation; TSS, 2 simple sutures.
Cyclic Testing
The progressions of construct stiffness over displacement for all groups at variable load cycles are shown in Figure 4. The ANOVA showed significant differences between MA-120 and the 2 fixed groups for displacement and construct stiffness at variable load cycles. The fixed groups had a lower initial construct stiffness, resulting in a higher final repair displacement after a continuous increase in stiffness over the load cycles. Less initial displacement combined with increasing resistance to displacement led to overall significantly lower displacement (P < .001) for the ASA MA meniscus-suture repair fixation. Apart from the cyclic displacement at the beginning (cycle 10; P < .002), no other significant difference was found between the 2 fixed groups.

Mean stiffness over displacement progression with statistical analysis throughout loading over 100,000 cycles with initial (cycle 10) and final (cycle 100,000) percentage deviation of primary outcome variables between adjustable and fixed Mason-Allen repair. MA, Mason-Allen; MA-120, MA with 120 N of tension applied during adjustable fixation; TSS, 2 simple sutures.
The biomechanical, time-zero, native PMMR tensile behaviors tested under simulated hoop-stress loading in line with the circumferential fibers were merged to establish a functional zone of the native human meniscus (Figure 5). Representative hysteresis curves of each repair group at the end of testing were used to quantify and qualify the stabilization potential of the tested repair techniques to the native meniscus reference model. Although the hysteresis curve of the adjustable groups was close to the native meniscal function, a completely loose state was assessed for fixed, conventional PMMR fixation groups.
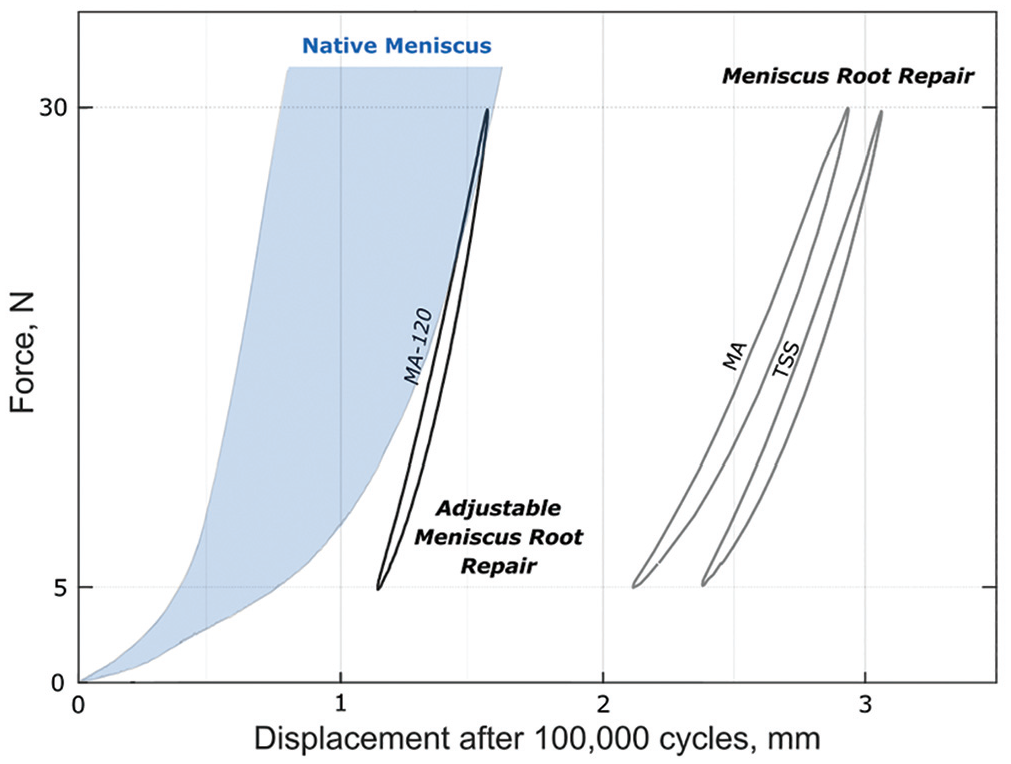
Representative hysteresis curves of suture-based meniscus root repair groups at the end of the test (100,000 cycles) show the final loading situation of the adjustable and fixed repairs in relation to the native meniscus. MA, Mason-Allen; MA-120, MA with 120 N of tension applied during adjustable fixation; TSS, 2 simple sutures.
Pull to Failure
None of the specimens failed during cyclic testing. The ultimate failure load of both MA suture-based repairs was significantly higher (P < .001) compared with TSS (Figure 6). The ultimate stiffness of the adjustable repair (MA-120) was considerably higher than that of the TSS. However, the native human meniscus had significantly higher ultimate failure load (P < .001) and stiffness (P < .001) compared with all repair techniques. Suture cut-through of the meniscus was the common failure mode for all repair groups.
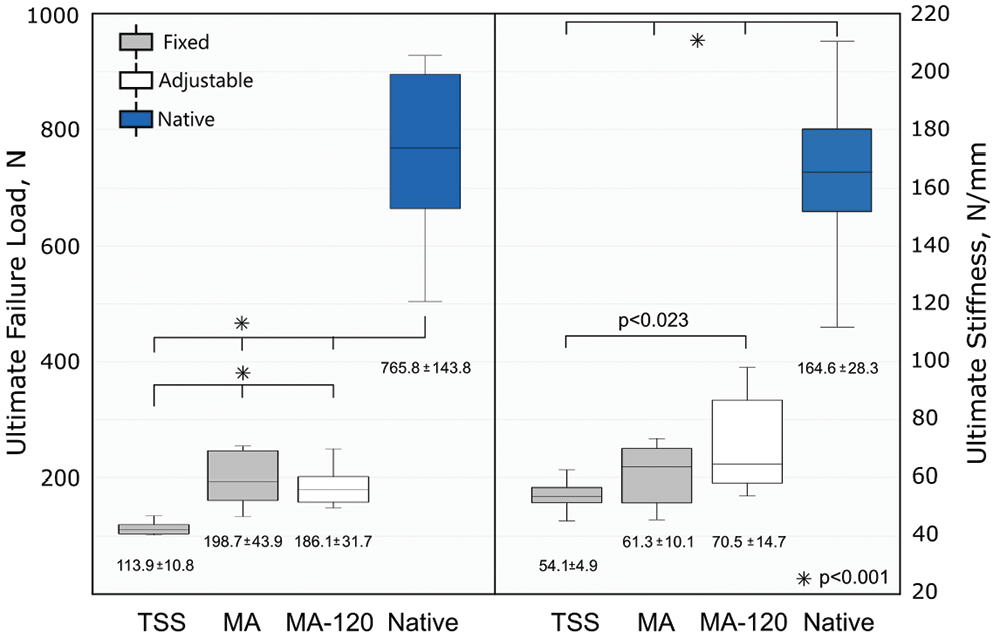
Boxplot with mean ± standard deviation values of ultimate load and stiffness during pull to failure with statistical analysis of meniscal repairs and native meniscus. MA, Mason-Allen; MA-120, MA with 120 N of tension applied during adjustable fixation; TSS, 2 simple sutures.
Discussion
The results of this study confirm our hypothesis that repair suture tensioning with the ASA implant would result in significantly higher initial repair load and stiffness of the meniscus tissue compared with the conventional TPOR techniques when knotting the repair suture over a button in a cadaveric model. The study also showed that the overall stiffer ASA repair restricted displacement throughout testing that nearly approximated the native human meniscal function in the cyclic load range, whereas both conventional TPORs were looser. Apart from the initial cyclic displacement, no other significant difference was found between TSS and MA during load cycling. 25 None of the groups exceeded the 3-mm threshold for displacement that has been reported to compromise meniscal function, 40 but the final peak displacement approached this threshold for the conventional TPORs. Although the adjustable and fixed meniscus root repair with the MA configuration achieved higher ultimate failure than TSS, all repair techniques showed inferior ultimate strength to the native human PMMR.
In recent years, several studies have evaluated the effect of the suture configuration, suture selection, or tunnel position on PMMR fixation.3,9,15,16,25,31-33 Biomechanical evidence shows that anatomic meniscus root repair using 2 repair sutures in a more complex MA configuration is superior to a simple suture configuration and improves TPOR meniscal refixation and articular contact mechanics. 20 Direct meniscus root refixation at its tibial insertion site using a suture anchor has been proposed as an alternative repair option to conventional TPOR, and despite promising biomechanical and clinical results,16,21,30,35 the need for an accessory posterior medial portal with an antegrade delivery technique and the risk of neurovascular structural damage have prevented clinical widespread use. The latest ASA repair technique, using a retrograde transtibial approach for implant insertion, provides aperture tibial plateau fixation and suture repair tensioning, which overcomes the apparent limitations of previous anchor techniques. A recent porcine biomechanical study showed that the ASA implant with manual tensioning of the repair sutures significantly improved primary surgical PMMR fixation and reduced cyclic displacement compared with conventional TPORs. To the best of our knowledge, this study was the first to evaluate the primary fixation of the novel ASA implant and the 2 most clinically relevant fixed repair techniques for meniscus root repair tested over prolonged cyclic loading of 100,000 cycles in a human meniscal cadaveric model.
Compared with previous repair displacement studies using lower level cyclic loading (1000 cycles),3,9,15,16,31-33 the increase in load cycles to 100,000 in this study may better represent the suggested postoperative rehabilitation period of 4 to 8 weeks of partial weightbearing for meniscal healing.28,37,39 Therefore, the current test results can be only partially compared with the available literature, as no study has reported the cyclic loading response after 100,000 cycles. Although displacement after the first load cycle did not differentiate the primary fixation strength between variable TPORs,24,25,42 significant increased initial load and stiffness of the ASA fixation technique may refine the perspective of primary surgical fixation. The overall lower stiffness of conventional TPORs may explain relief displacement values similar to those of ASA repair with considerably higher initial loads in this study. The current results of initial repair loads are consistent with a previous porcine study 3 showing similar loads for corresponding repair techniques and a limited amount of tension (<30 N) achieved by indirect PMMR refixation with knotting of the transtibial sutures over a button. Currently, no critical tension threshold for meniscal reapproximation is available, but inadequate meniscus root stabilization due to reduced repair stiffness or increased micromotion under repetitive loads could clinically compromise PMMR healing and long-term contact pressure and mechanics for function.10,21,30 According to Feucht et al, 16 suture anchor placement close to the joint line improved the PMMR fixation to resist meniscal deformation better and reduce displacement at the repair site compared with conventional TPOR. The more complex MA suture pattern is considered to improve the meniscus tissue reapproximation to the bone at higher tension levels by reducing the risk of suture cut-through and stress on the meniscus tissue due to optimized load distribution.29,38 A stiffer meniscus and higher bone quality of porcine tissue may explain slight differences in the repair stiffness and displacement with the ASA repair placed in more variable human tissue.2,14 All meniscus root repairs in human tissue were less stiff than those in porcine tissue after 1000 load cycles. 3 Consistent with other studies, the MA repair achieved higher ultimate failure strength.15,25 The failure load of all repairs was inferior to that of the native PMMR attachment3,16,23 and higher than the forces acting on the repaired PMMR during the early postoperative period of limited weightbearing. 41 Given the complete recovery after loading situations within the linear-elastic loading range, 43 time-zero properties are most often considered to adequately characterize the native meniscus for baseline comparisons with repair groups.
Limitations
Several limitations of this study must be recognized when interpreting these results. The mean age of human donors was older than that of middle-aged patients undergoing a PMMR repair and could cause lower stability due to the age-dependent, reduced quality of the meniscus tissue. However, these menisci displayed no damage. Patients with meniscus root injuries often experience degeneration of the meniscus, which reduces the stability of the tissue, before a tear occurs. Therefore, the quality of the tissue in patients with meniscal tears could be worse than that in patients without injuries. In this respect, the preparations used contain factors that have the opposite effect on stability to those seen in a clinical setting. However, suture anchor fixation in weaker human bone is likely to represent worse bony fixation conditions, so implant behavior in weaker tissue quality should overestimate the implant performance compared with PMMR repairs in the clinic.
Furthermore, due to age- and sex-related effects between groups, inconsistent structural tissue properties may influence the biomechanical outcome. In contrast to variable in vivo loading conditions in the human knee during daily activities, a simulated meniscal hoop stress load was applied in line with the circumferential fibers to achieve near-physiologic testing conditions with the complete meniscus released from the meniscocapsular junction and secured in customized clamps. Therefore, the obtained time-zero biomechanical performance of various PMMR repairs may differ from device behavior in the clinical setting. Variable tension of the repair depending on the surgeon’s experience or slight differences in suture pattern in variable menisci (size and quality) or bone tunnel length may influence mechanical performance and clinical outcome in practice. Although various suturing techniques for PMMR fixation with the ASA implant can be performed in the operating room, the present biomechanical work focused only on the performance of the suture-meniscus repair in the MA configuration. In addition, this study did not consider the effects of gradual biological healing during partial weightbearing rehabilitation that would occur with meniscus root repair and patient clinical outcomes.
Conclusion
The ASA repair resulted in improved primary PMMR fixation that was stiffer with less cyclic displacement than conventional TPORs and approached that of the human meniscal function after 100,000 load cycles in a cadaveric model. However, all repair techniques had lower ultimate strength than the native human PMMR.
Footnotes
Submitted July 23, 2024; accepted December 2, 2024.
One or more of the authors has declared the following potential conflict of interest or source of funding: Arthrex provided research support for this study. S.B. and C.A.W. are employees of Arthrex. A.J.K., P.A.S., C.W.N., and A.B. are consultants for Arthrex and have received consulting fees, speaking fees, compensation for services other than consulting, and royalties from Arthrex. A.J.K. has received honoraria from Joint Restoration Foundation, royalties from Responsive Arthroscopy, and a grant from DJO. P.A.S. has received compensation for services other than consulting from Kairos Surgical and support for education from United Orthopedics. C.W.N. has received support for education from Arthrex, Elite Orthopedics, and Medinc of Texas; compensation for services other than consulting from Synthes GmbH; and consulting fees from Vericel Corporation and Arthrex. A.B. has received hospitality payments from GE Healthcare, speaking fees from Synthes GmbH and Arthrex, and consulting fees from Collagen Matrix and Arthrex. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.