
Abstract
Background:
Augmented repair is an alternative strategy for the treatment of acute ligament and tendon injuries that imparts time-zero biomechanical strength to allow early loading, thereby protecting the repaired structures during the early healing process.
Purpose:
To investigate the biomechanical properties and biological healing process after suture repair of acute anterior cruciate ligament (ACL) tears with polyethylene terephthalate (PET) augmentation and compare the findings with those obtained without PET augmentation.
Study Design:
Controlled laboratory study.
Methods:
A total of 48 rabbits were assigned to 3 groups: a PET-augmented group, a nonaugmented suture repair group, and a natural (control) group. All 3 groups were evaluated at 4, 12, and 16 weeks after surgery. Biomechanical performance was assessed using tensile strength testing, and ACL healing and maturation were assessed using histological assessments.
Results:
The PET-augmented group showed less anterior knee laxity at 30° of knee flexion and superior structural continuity compared with the suture group. ACL repair with PET augmentation yielded recovery of the maximum tensile load as early as 4 weeks compared with that of the natural group (110.5 ± 6.5 vs 129.0 ± 8.6 N, respectively; P = .29) and a gradual improvement in linear stiffness from 4 weeks (58.4 ± 3.9 N/mm) to 16 weeks (83.1 ± 5.1 N/mm; P = .04), approaching that of the natural group (106.7 ± 5.8 N/mm). Furthermore, histological analyses revealed that in the PET-augmented group, the ACL healed back to the proximal insertion as early as 4 weeks with angiogenesis and collagen regeneration, and the increased ligament maturity score indicated a gradual healing process from 4 to 16 weeks.
Conclusion:
Compared with nonaugmented repair, repair augmented with a PET band enhanced early ACL stability and supported healing of ACL tears in a rabbit model.
Clinical Relevance:
The biomechanical and histological findings support subsequent clinical investigations using PET augmentation in patients with acute ACL tears.
Anterior cruciate ligament (ACL) repair is a potential surgical treatment option for some ACL tears.34,47,55,61 Primary ACL repair was the standard surgical technique for ACL tears until the 1980s, when controversial midterm and long-term outcomes, such as healing failure, retears, knee instability, and impairment of activities of daily living, were reported.3,64,72 Several factors have been proposed to improve the prognosis of ACL repair. However, the rates of failure and structural laxity of the ACL range from 40% to 100%,17,32,60 posing a major challenge to the clinical application of ACL repair.
Considering the challenges associated with ACL repair, various arthroscopic techniques have been introduced, particularly for proximal ACL ruptures.2,69 Recent improvements in mechanical and biological augmentation, as well as in patient selection, have resulted in a resurgence in the interest in ACL repair.18,26 Dynamic intraligamentary stabilization has been used to compare primary repair procedures in a controlled study. 36 In a systematic review, Ahmad et al 2 concluded that dynamic intraligamentary stabilization may be an effective modality for the treatment of acute proximal ACL tears. Murray et al49,50 used a bioactive scaffold to bridge the gap between torn ligament ends and reported superior short-term outcomes. Ribbans et al 43 reported internal bracing as an alternative technique for ACL repair that reinforces the ligament with suture augmentation and provides secondary stabilization for the injured knee.5,6 Overall, although reconstruction is still the gold standard, with the support of both biomechanical and biological augmentation, ACL repair is re-emerging as a viable alternative in orthopaedics. 62 Among these techniques, biomechanical augmentation has the potential to improve mechanical stability and protect the repaired ACL from excessive elongation during the early healing stages26,44; therefore, it has garnered significant attention.
Various types of scaffolds have been developed for augmented repair.7,39,65 Polyethylene terephthalate (PET), a nondegradable polyester polymer, is widely used to repair ligament and tendon injuries.11,41 Notably, the ligament advanced reinforcement system (LARS), which is composed of PET, has shown superior mechanical properties and a low immune response.16,45,70 Recent studies have reported that the LARS can restore knee stability and improve functional outcomes in reconstructed ACLs.13,20
In this study, we evaluated the early healing process after PET-augmented repair in a rabbit model of acute ACL tears. We hypothesized that repair augmented with a PET band could enhance the biomechanical stability of the repaired ACL and potentially promote ACL healing compared with suture repair without PET augmentation.
Methods
Study Design
This study was approved by our Institutional Animal Care and Use Committee. A total of 48 male 6-month-old New Zealand rabbits (skeletally mature; weighing 2.0-3.0 kg) with healthy and intact hindlimbs were used in this study. A random hindlimb from each rabbit was treated with repair augmented with a PET band (PET-augmented group; n = 21) or suture repair (suture group; n = 21). All animals in the PET-augmented group and suture group were randomly euthanized immediately after surgery (n = 3) or at 4 (n = 6), 12 (n = 6), and 16 weeks (n = 6) postoperatively. There were 6 healthy rabbits that served as controls (natural group). The outcome measures included anterior-posterior (AP) laxity testing (n = 6), gross examination (n = 6), tensile testing (n = 3), and histological analysis (n = 3).
Surgical Procedure
After the induction of general anesthesia, medial parapatellar arthrotomy was performed, and the ligamentum mucosum was released (Figure 1, A1 and B1). The ACL was cut close to the femoral insertion (Figure 1, A2 and B2). A laxity test was performed to verify functional loss of the ACL. A modified Kirchmayr suture (3-0 Prolene; Ethicon), which has shown superior ultimate failure loads, was applied at the proximal side of the tibial ACL stump, as described previously (Figure 1, A3 and B3). 56 For repair augmented with the PET band, a 1-mm drill pin was placed in the tibia using a commercial drill guide with the tunnel entrance posterior to the intermeniscal ligament and in the middle of the tibial insertion of the ACL. A femoral tunnel was created using a 1-mm drill pin at the center of the femoral insertion of the ACL. Then, a 1-mm knitted PET band (Ligatech) was threaded through the tibial tunnel and fixed with a titanium interference screw (1.5 mm × 4 mm). The other side of the PET band was threaded through the femoral tunnel using sutures. The PET band was tightened at full extension and fixed to an EndoButton (Ligatech) by knots, and the sutures of the ligament stump were fixed to the EndoButton at 45° of knee flexion. Cyclic knee motion was performed to confirm that the ligament stump was close to the femoral insertion (Figure 1, A4, A5, B4, and B5). Finally, all the knees were closed in layers. For suture repair, a modified Kirchmayr suture was applied to the proximal side of the tibial ACL stump (Figure 2, A1 and B1), and the sutures were threaded through the femoral tunnel and fixed with an EndoButton (Figure 2, A2, A3, B2, and B3). After 1 week of plaster immobilization, all animals were returned to their cages and allowed to move without any restrictions.
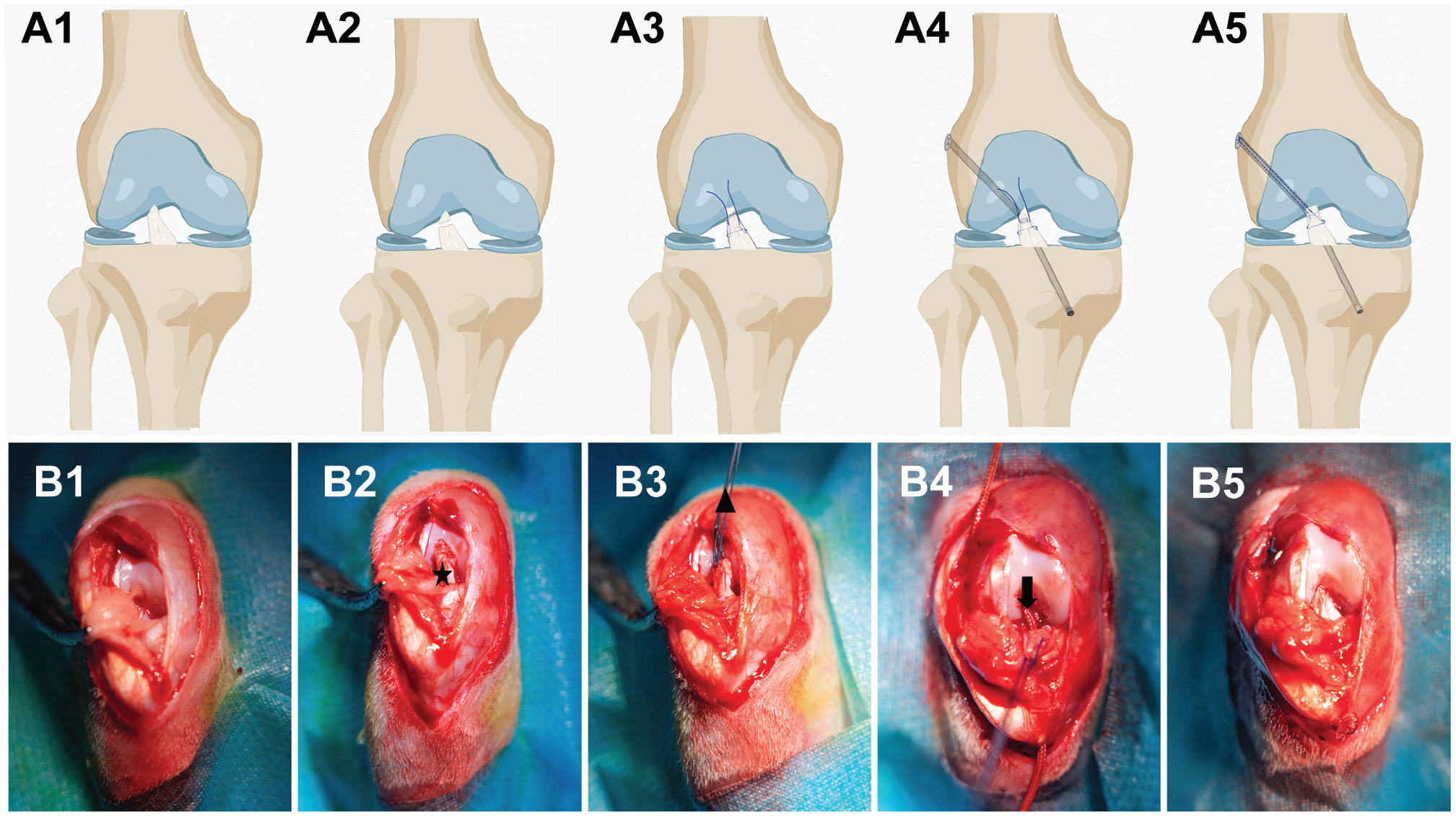
Surgical procedure of repair augmented with the PET band. (A) Schematic diagram. (B) Repair augmented with the PET band in rabbits. Star: anterior cruciate ligament stump; triangle: suture; arrow: PET band.
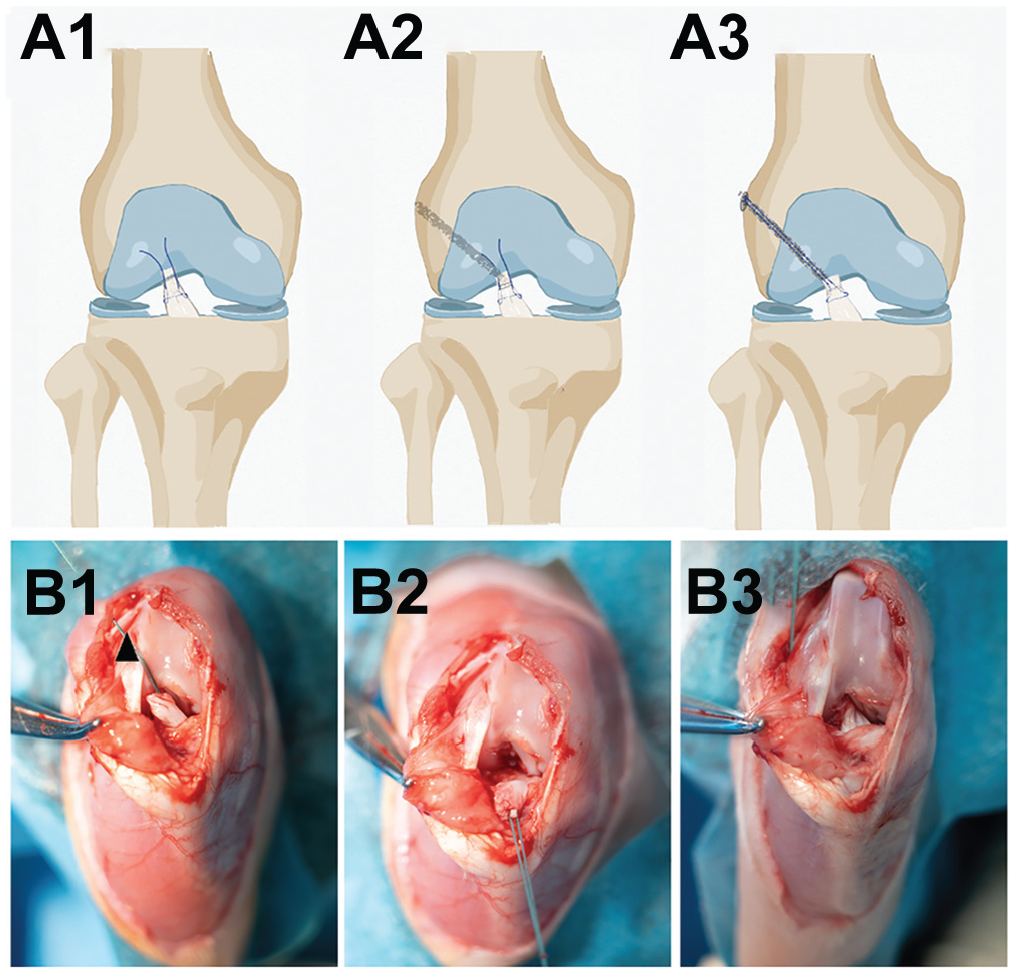
Surgical procedure of suture repair. (A) Schematic diagram. (B) Suture repair in rabbits. Triangle: suture.
AP Laxity Testing and Gross Examination
After euthanasia, AP laxity testing was performed with the knee flexed at 30°. The knees were supported using custom fixtures and rigidly attached to an electronic digital caliper. A fixed AP-directed shear load was applied to the tibia. The displacement data were acquired by 2 independent investigators.
After the animals were euthanized, the knee cavity was exposed, and the gross appearance of the ACL was recorded. The intra-articular section of the ACL was evaluated by assessing structural continuity and tissue morphology.
Tensile Testing
Biomechanical properties, including maximum tensile load and linear stiffness, were assessed using tensile testing. Tensile testing was performed using a biomechanical testing machine (ElectroForce 3520-AT; TA Instruments) immediately after surgery and at 4, 12, and 16 weeks postoperatively. The specimens were fixed using a component of the testing apparatus to ensure that the applied load was directed along the longitudinal axis of the ACL. Before tensile testing, 10 cycles of longitudinal preloading at 1 N were applied to the specimens for preconditioning. The maximum tensile load was recorded at an elongation speed of 5 mm/min until mechanical failure. 80 Linear stiffness was calculated from the linear portion of the load-deformation curve. The samples were kept moist with saline solution throughout testing.
Histological Analysis
After euthanizing the rabbits, the femur-ACL-tibia complex was immediately fixed in paraformaldehyde, decalcified in ethylenediaminetetraacetic acid solution, and embedded in paraffin. The embedded samples were sectioned at a thickness of 5 µm along the sagittal plane of the knee. Hematoxylin and eosin (H&E), Sirius Red, collagen type I (COL-I; ab6308 [Abcam]), Masson, and CD31 (ab13420 [Abcam]) staining were performed using standard protocols. The sections were observed using an inverted light microscope (IX71SBF-2; Olympus), and digital images were acquired using DP Manager (Olympus). The ACL was divided into proximal, middle, and distal thirds. 61 Maturation of the proximal ACL was evaluated using a previously validated ligament maturity scoring system proposed by Watkins and modified by Ide et al. 28 Overall, 6 parameters, including cellularity, proportion of cells resembling tenocytes, proportion of parallel cells, vascularity, proportion of large-diameter fibers characteristic of mature ligament fibers, and proportion of parallel fibers, were evaluated semiquantitatively. In the natural group, the proximal ACL was assigned the total ligament maturity score of 28. Ligament-bone healing was assessed on the basis of a previously reported histological scoring system for ligament-bone healing, which evaluated the cellular morphological characteristics of interface tissue, the extent of surrounding fibrocartilage tissue, and the interface tissue transition from the bone to ligament. Ligament-bone healing in the natural group was assigned the total score of 12.14,29 ImageJ software (National Institutes of Health) was used for further quantitative analysis by an independent observer who was blinded to the group allocation and intervention.
Statistical Analysis
All quantitative results were expressed as mean ± standard deviation. One-way analysis of variance with the Tukey test and unpaired t test was used to compare significant differences between the groups at different time points. Prism software (Version 8.1; GraphPad) was used for statistical analyses. P < .05 was considered statistically significant.
Results
Biomechanical Properties
The mean maximum tensile load of the PET bands was 146.5 ± 10.53 N, and the mean linear stiffness was 15.6 ± 0.57 N/mm. Biomechanical properties, including linear stiffness and maximum tensile load, were assessed using tensile testing in the PET-augmented and natural groups. The biomechanical properties were evaluated immediately after surgery in the suture and PET-augmented groups. As shown in Figure 3, the maximum tensile load (64.70 ± 15.62 vs 34.64 ± 5.17 N, respectively; P = .011) and linear stiffness (52.69 ± 14.09 vs 26.69 ± 4.38 N/mm, respectively; P = .012) in the PET-augmented group were significantly higher than those in the suture group (Figure 3). Because all suture repair cases failed, the suture group was excluded from further assessments. All the specimens failed in the proximal part of the ligament (Figure 4A). As shown in Figure 4B, linear stiffness in the PET-augmented group was 58.4 ± 3.9 N/mm at 4 weeks (P = .003), 66.4 ± 6.6 N/mm at 12 weeks (P = .006), and 83.1 ± 5.1 N/mm at 16 weeks (P = .04), indicating a gradual increase from 4 to 16 weeks that approached the value of the healthy ACL in the natural group (106.7 ± 5.8 N/mm). Moreover, the maximum tensile load in the PET-augmented group was 110.5 ± 6.5 N at 4 weeks (P = .29), 121.0 ± 3.5 N at 12 weeks (P = .79), and 120.2 ± 13.3 N at 16 weeks (P = .76), which was not significantly inferior to that of the natural group (129.0 ± 8.6 N) (Figure 4C). Thus, the PET-augmented group exhibited a progressive increase in linear stiffness postoperatively and showed recovery of the maximum tensile load as early as 4 weeks.
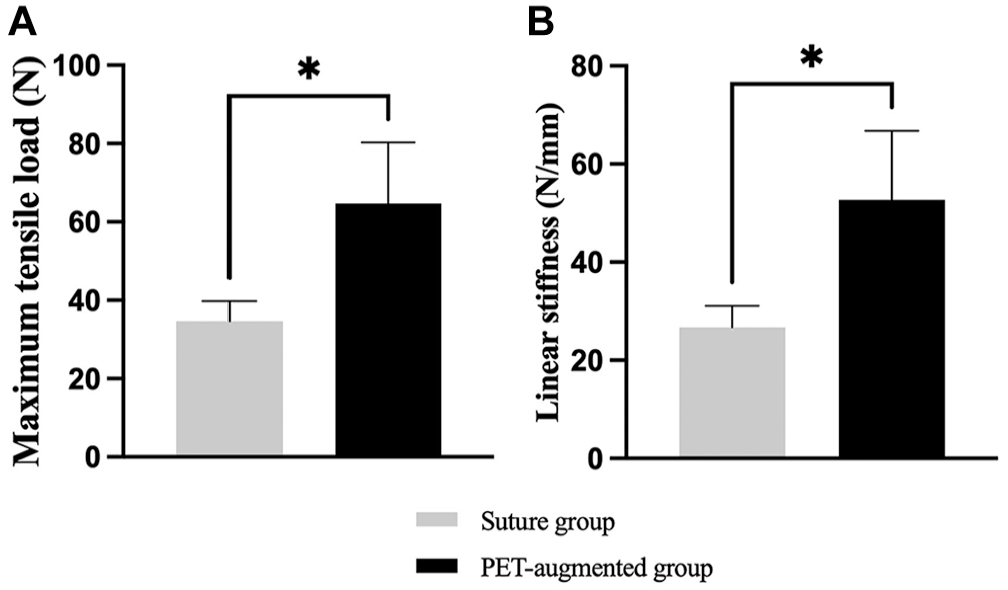
(A) Maximum tensile load and (B) linear stiffness immediately after surgery. *P < .05.
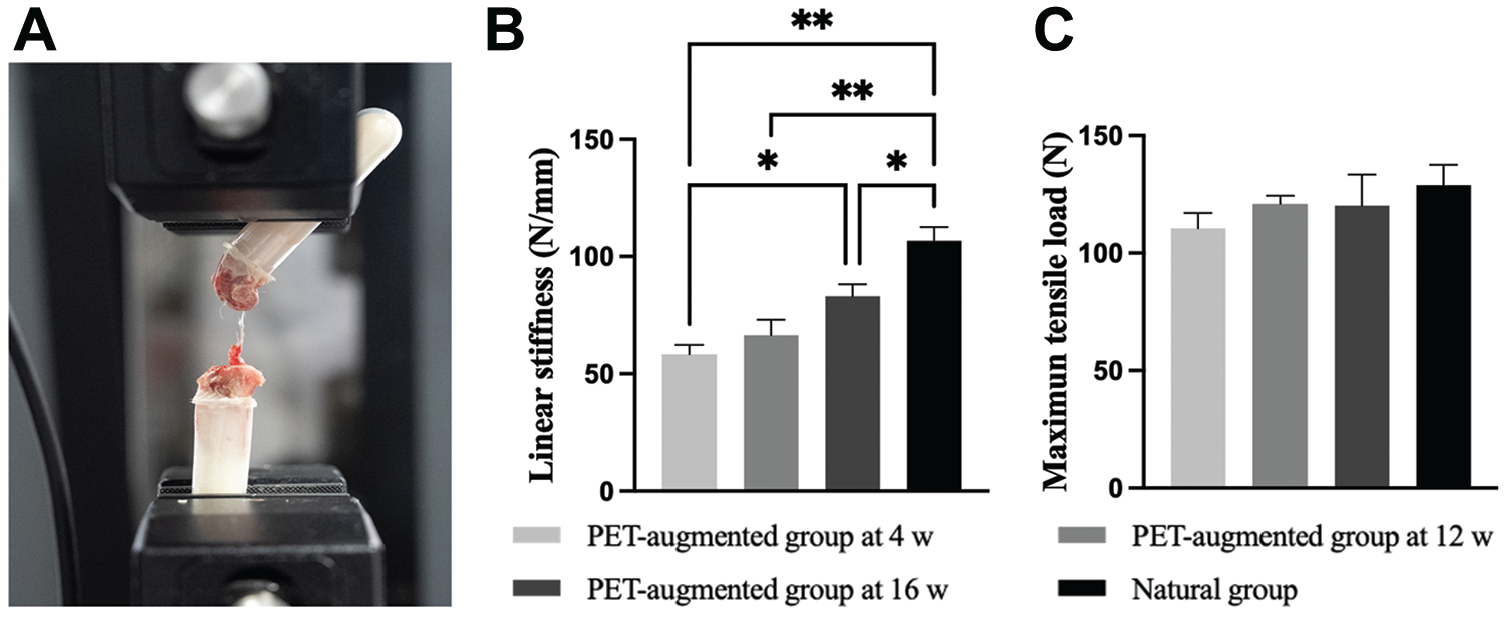
(A) Representative image of tensile testing in the PET-augmented group. (B) Linear stiffness and (C) maximum tensile load in the PET-augmented and natural groups. *P < .05. **P < .01.
Knee Laxity
AP laxity testing was performed to assess knee laxity in the PET-augmented, suture, and natural groups. As shown in Figure 5, knee laxity in the groups did not differ significantly immediately after surgery. At 4 weeks, the PET-augmented group showed significantly lower AP displacement at 30° of knee flexion compared with the suture group (1.11 ± 0.25 vs 4.16 ± 0.79 mm, respectively; P = .0006). This difference continued at 12 weeks (1.04 ± 0.12 vs 3.83 ± 0.67 mm, respectively; P = .0004) and 16 weeks (1.37 ± 0.29 vs 3.95 ± 0.54 mm, respectively; P = .0003). The suture group showed higher AP displacement than the natural group at 4 weeks (4.16 ± 0.79 vs 0.92 ± 0.18 mm, respectively; P = .0005), 12 weeks (3.83 ± 0.67 vs 0.90 ± 0.22 mm, respectively; P = .0003), and 16 weeks (3.95 ± 0.54 vs 0.99 ± 0.13 mm, respectively; P = .0001). However, no significant difference was observed between the PET-augmented and natural groups at 4 weeks (1.11 ± 0.25 vs 0.92 ± 0.18 mm, respectively; P = .89), 12 weeks (1.04 ± 0.12 vs 0.90 ± 0.22 mm, respectively; P = .90), and 16 weeks (1.37 ± 0.29 vs 0.99 ± 0.13 mm, respectively; P = .45) (Figure 5). Thus, the knees in the PET-augmented group demonstrated less AP laxity at 30° of knee flexion than those in the suture group.
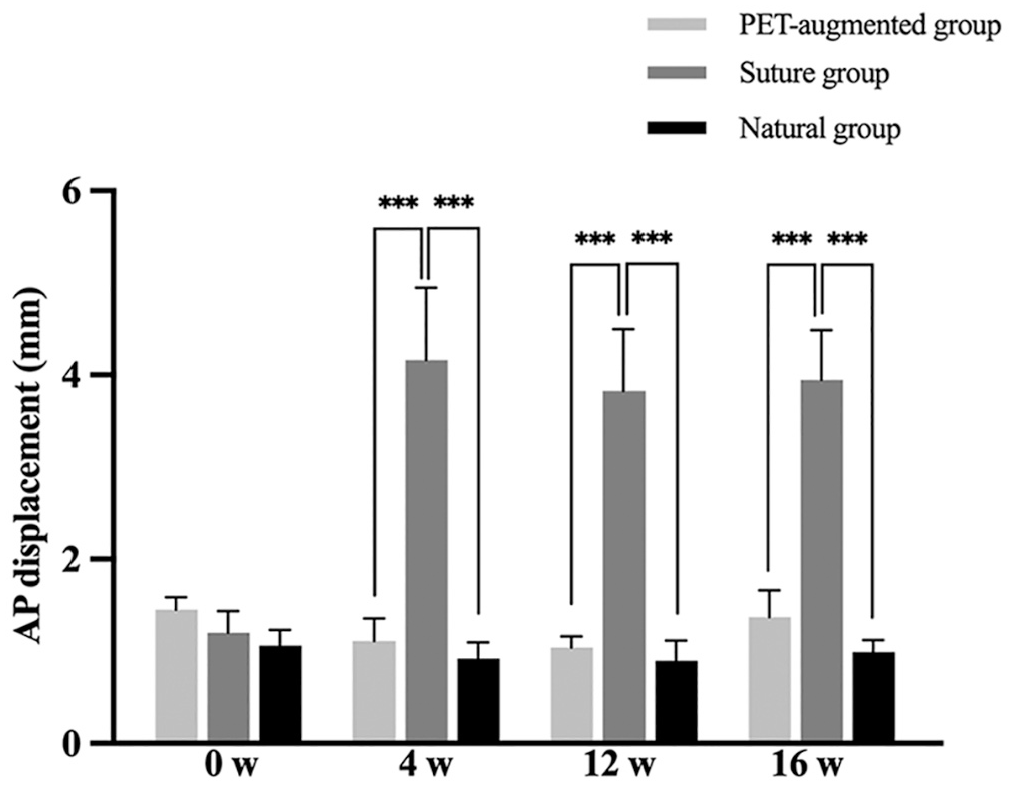
Anterior-posterior laxity testing at 0, 4, 12, and 16 weeks. ***P < .001.
Gross Appearance
The gross appearance was observed, and structural continuity of the ACL was assessed in the PET-augmented and suture groups. ACL healing back to the femoral intercondylar notch was considered to indicate the recovery of structural continuity. 51 In the PET-augmented group, the ACL healed back to the femoral intercondylar notch at 4 weeks, and a large amount of reddish tissue was formed (Figure 6A). At 12 weeks, reddish tissue decreased and white tissue appeared in the PET-augmented group (Figure 6B). At 16 weeks, reddish tissue disappeared, and white tissue was covered by transparent membrane-like tissue (Figure 6C). In the suture group, the ACL failed to heal back to the femoral intercondylar notch, and the ACL stump was clearly observed from 4 to 16 weeks (Figure 6, D-F). Overall, all ACLs in the PET-augmented group showed the recovery of structural continuity, whereas all ACLs in the suture group lost structural continuity. Thus, structural continuity of the ACL was recovered by the formation of regenerative tissue in the PET-augmented group.
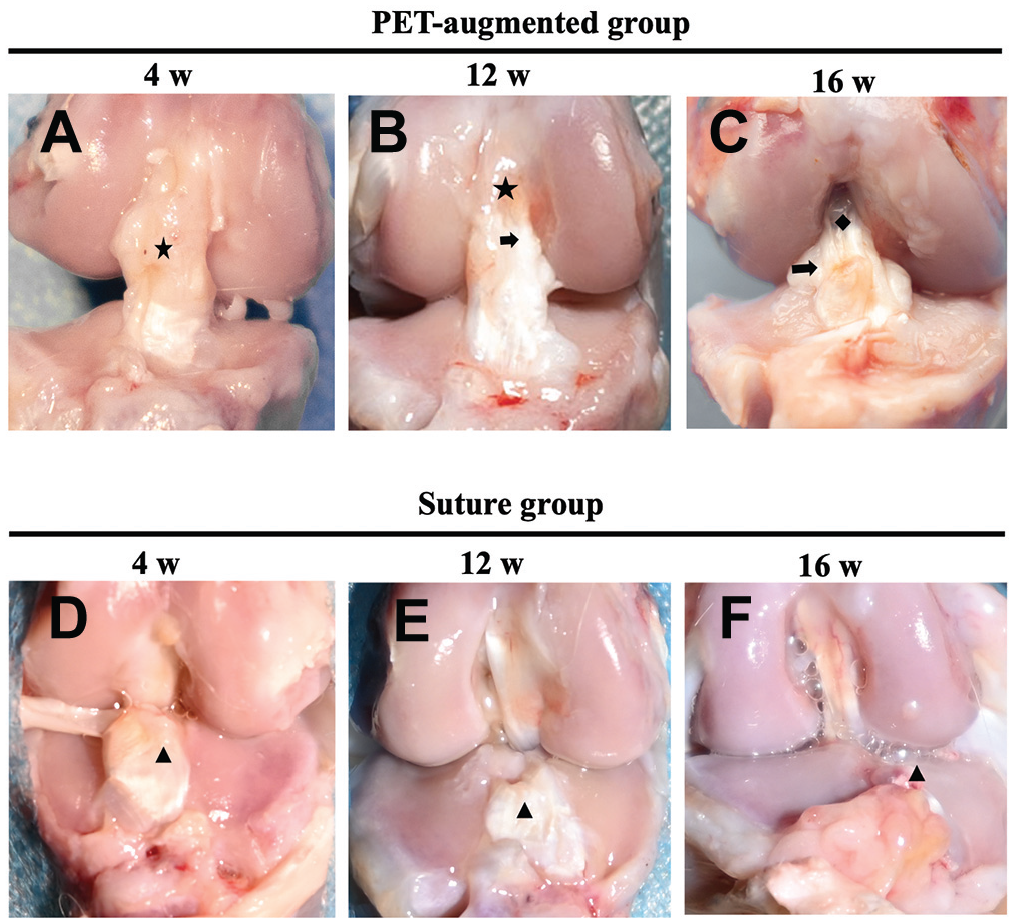
(A-C) Representative images of the gross appearance of the anterior cruciate ligament (ACL) in the PET-augmented group. (D-F) Representative images of the gross appearance of the ACL in the suture group. Star: reddish tissue; arrow: white tissue; square: transparent membrane-like tissue; triangle: ACL stump.
Histological Staining
Ligament Maturity Assays
H&E, Sirius Red, and COL-I staining were used to assess the collagen organization, components, and content of the proximal ACL in the PET-augmented and natural groups (Figure 7). On the basis of the results of H&E, Sirius Red, and COL-I staining, a ligament maturity scoring system was used to assess maturation of the proximal ACL.
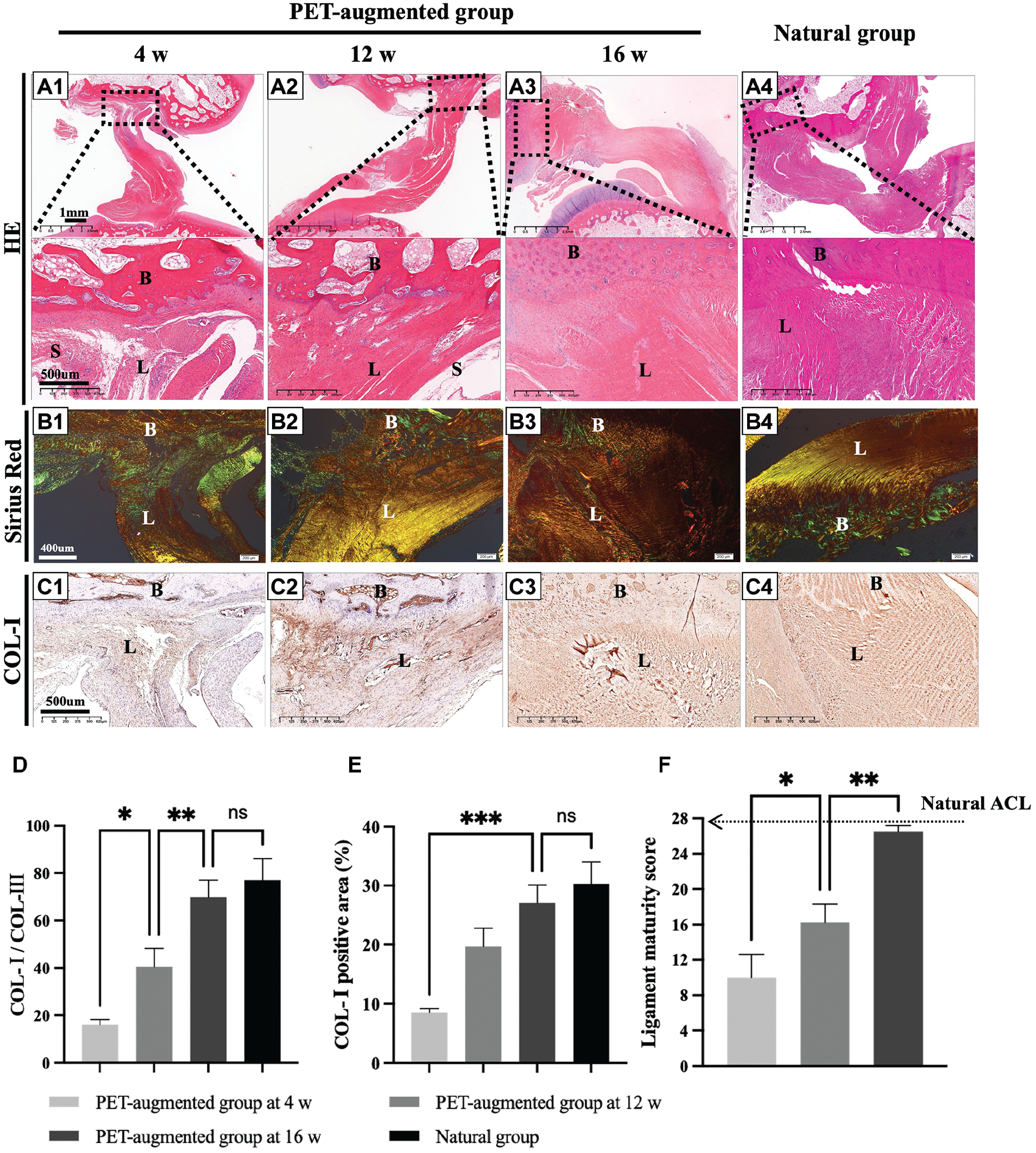
(A1-A4) Representative hematoxylin and eosin (H&E) staining images of the proximal anterior cruciate ligament (ACL). (B1-B4) Representative Sirius Red staining images of the proximal ACL. (C1-C4) Representative collagen type I (COL-I) staining images of the proximal ACL. (D) The COL-I area/collagen type III (COL-III) area at the proximal ACL. (E) COL-I–positive area at the proximal ACL. (F) The ligament maturity score of the proximal ACL. B, bone; L, ligament; S, synovial membrane. *P < .05. **P < .01. ***P < .001. ns: P > .05.
As shown in Figure 7A1, the H&E-stained images showed that the ACL in the PET-augmented group healed back to the femoral end at 4 weeks, and collagen was arranged randomly and organized loosely. At 12 weeks, denser and more organized collagen was observed (Figure 7A2). At 16 weeks, the collagen organization in the PET-augmented group was similar to that in the natural group (Figure 7, A3 and A4).
The Sirius Red staining results are shown in Figure 7B1 to 7B4, with the yellow area indicating COL-I and the green area indicating collagen type III (COL-III). 12 The COL-I/COL-III area ratio in the PET-augmented group significantly increased from 4 weeks (1.2 ± 0.1) to 16 weeks (6.1 ± 1.1) (P = .001). At 16 weeks, the COL-I/COL-III area ratio in the PET-augmented group was comparable with that in the natural group (6.1 ± 1.1 vs 6.4 ± 1.2, respectively; P = .97) (Figure 7D), indicating similar collagen compositions in the 2 groups.
In Figure 7C1 to 7C4, the COL-I–positive area is brown in color. The COL-I–positive area 12 in the PET-augmented group gradually increased from 4 weeks (8.5 ± 0.7) to 16 weeks (27.1 ± 3.1) (P = .0002). The COL-I–positive area in the PET-augmented group was comparable with that in the natural group at 16 weeks (27.1% ± 3.1% vs 30.3% ± 3.7%, respectively; P = .54). These findings suggest that the COL-I content of the proximal ACL in the PET-augmented group was comparable with that in the natural group at 16 weeks (Figure 7, D and E).
As shown in Figure 7F, the ligament maturity score in the PET-augmented group significantly improved from 4 weeks (10.0 ± 2.6) to 12 weeks (16.2 ± 2.1; P < .05) to 16 weeks (26.5 ± 0.6; P < .05) and gradually approached that in the natural group (28.0 ± 0.0; P = .005). Therefore, the PET-augmented group showed promising potential for postoperative ligament maturation.
Ligament-Bone Healing Assays
Masson staining was used to assess maturation of the ligament-bone interface in the PET-augmented and natural groups (Figure 8). A histological scoring system for ligament-bone healing was used for quantitative analysis. As shown in Figure 8A1, only fibrovascular tissue was observed in the PET-augmented group at 4 weeks. At 12 weeks, Sharpey-like fibers were visible in the PET-augmented group, but no obvious formation of fibrocartilage was observed (Figure 8A2). At 16 weeks, fibrocartilage partially surrounded by collagen fibers in an organized arrangement was observed in the PET-augmented group (Figure 8A3). In the natural group, intact fibrocartilage was surrounded by collagen fibers and inserted into the bone (Figure 8A4). The ligament-bone healing score in the PET-augmented group significantly improved from 4 weeks (2.7 ± 1.5) to 12 weeks (6.0 ± 0.8; P < .05) to 16 weeks (8.7 ± 0.6; P < .05) and gradually approached that in the natural group (12.0 ± 0.0; P = .01) (Figure 8C). Therefore, the PET-augmented group showed great potential for postoperative healing of the ligament-bone interface.
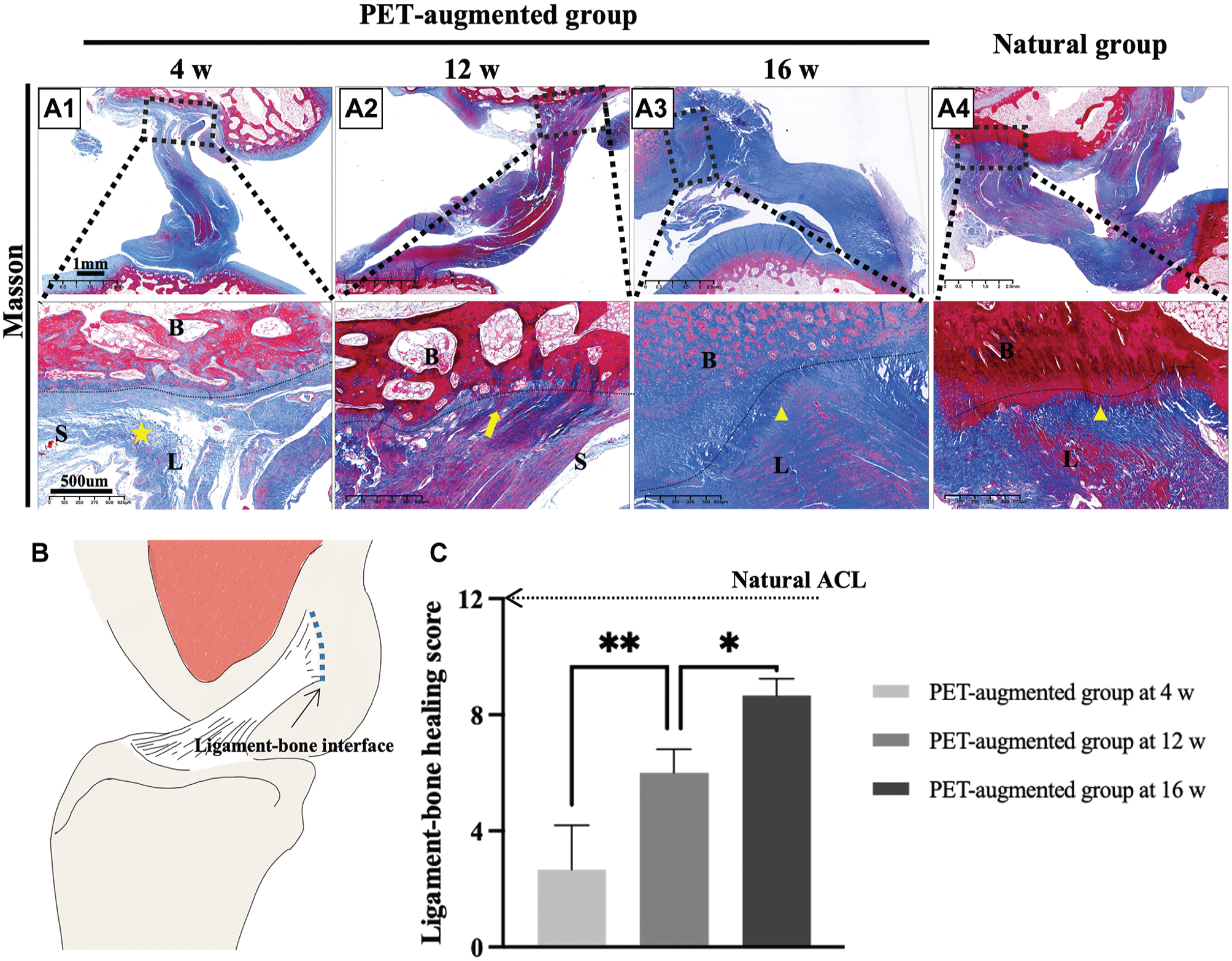
(A) Representative Masson staining images at the ligament-bone interface. (B) Schematic diagram. (C) Ligament-bone healing score. B, bone; L, ligament; S, synovial membrane. Star: fibrovascular tissue; arrow: Sharpey-like fibers; triangle: fibrocartilage. *P < .05. **P < .01.
Angiogenesis Assays
Blood vessels play a crucial role in the ligament healing process by providing the nutrients and oxygen necessary for ligament repair. 66 CD31 is a marker of blood vessels. 12 Blood vessels were quantified using CD31 staining in the proximal, middle, and distal thirds of the ACL in the PET-augmented and natural groups, which were marked in brown (Figure 9A). As shown in Figure 9B, the blood vessel count in the proximal ACL increased at 4 weeks and gradually decreased from 4 to 16 weeks in the PET-augmented group, whereas little variation was noted in the middle and distal ACL. Additionally, at 4 weeks, the PET-augmented group exhibited a significantly higher blood vessel count in the proximal ACL compared with the natural group (88.7 ± 21.5 vs 38.0 ± 9.9, respectively; P = .01), while the same difference was not observed in the middle and distal ACL (Figure 9C). This suggests that active angiogenesis occurred in the proximal ACL at 4 weeks in the PET-augmented group. 67
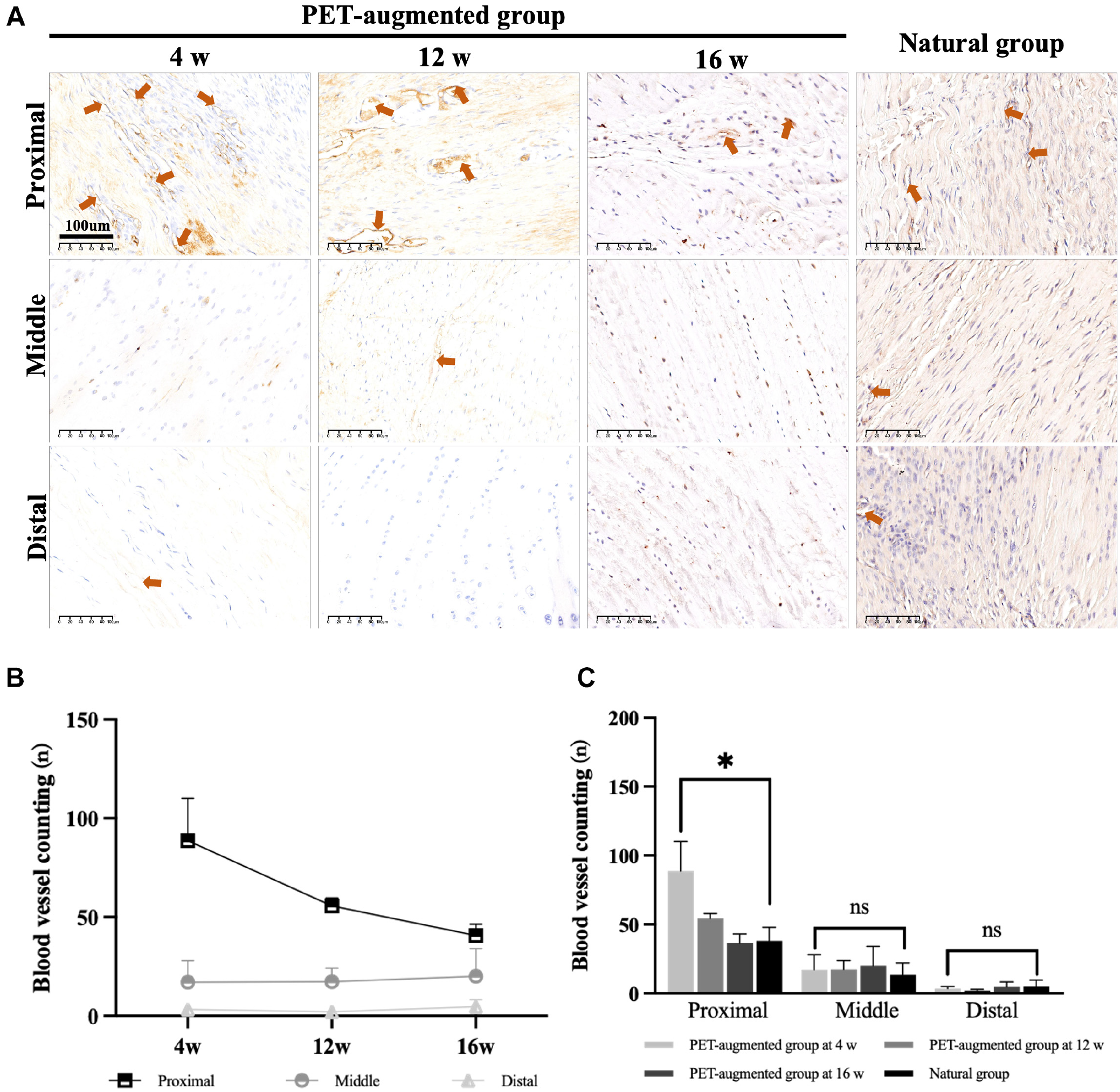
(A) Representative CD31 staining images in the proximal, middle, and distal thirds of the anterior cruciate ligament (ACL) in the PET-augmented and natural groups. (B) Changes in the blood vessel counts of the proximal, middle, and distal ACL in the PET-augmented group over time. (C) Quantitative comparison of blood vessel counts. Arrow: blood vessel. *P < .05. ns: P > .05.
Discussion
In this study, ACL repair augmented with a PET band led to significant improvements in mechanical performance and biological healing compared with suture repair alone. Stability under the maximum tensile load was similar to that of the native ACL at all time points assessed. Biological healing, as evaluated by histological assessments, showed expected improvements over time in terms of cellularity, collagen content, organization, and vascularity.
Notably, ACL repair with PET augmentation achieved successful healing, while direct suturing failed. The immediate biomechanical properties of the repaired ACL after surgery are considered the main reason for this variation in failure rates. Repair augmented with a PET band significantly increased the maximum tensile load and linear stiffness of the healing ACL, suggesting that PET-enhanced mechanical stability may support early healing. Additionally, the relatively high failure rate observed in the suture group could be attributed to the unique anatomic features and gait of rabbits. Previous studies have indicated a greater posterior slope of the tibial plateau in rabbits than in humans, 8 implying a heightened risk of reinjuries in rabbit ACL repair models. Moreover, the mean ultimate stress of the rabbit ACL is 69 ± 7 MPa, 52 which is markedly higher than that of the human ACL. 9 Thus, the rabbit ACL may experience increased loading during normal activities compared with the human ACL, which could be ascribed to differences in gait (hopping vs walking) and knee flexion angles (increased flexion in rabbits).
Vascularity is considered crucial in the healing process of ligaments because blood vessels provide necessary nutrients and oxygen, 66 reflecting the potential for, and state of, ACL healing after repair. 67 The PET-augmented group showed an abundant expression of an angiogenic protein (CD31) in the proximal ACL at 4 weeks, indicating the vascularity of the repaired ACL. This may be one reason for satisfactory ACL healing in this group. 66 The indications for ACL repair are generally based on the location of the tear and ACL tissue quality. 22 However, our study provided additional evidence from a biological standpoint, showing that abundant angiogenesis of the proximal ACL indicates the potential for healing. Notably, the indications for ACL repair continue to evolve, possibly owing to advances in tissue engineering and materials science. For instance, Murray et al 50 expanded the indications to include patients with at least 50% of the length of the ACL attached to the tibia using scaffolds incorporating autologous blood or platelet-rich plasma. Therefore, ACL repair may have a broad range of clinical applications in the future.
The direct insertion site of the ACL consists of a transition zone characterized by ligaments, unmineralized fibrocartilage, mineralized fibrocartilage, and bone tissue.15,57 Healing of repaired or reconstructed tissue occurs through fibrovascular scar formation rather than true regeneration of the native tissue architecture of the bone-ligament interface. 4 Over the past decade, basic research has explored strategies to biologically enhance ligament-bone healing through the use of growth factors, cell-based therapies, and various delivery methods.27,37,38,40,42,77,78 Immune interventions, exosome therapy, and other approaches also hold promise for promoting ACL healing.23,74,76,79 However, compared with biological augmentation, the understanding of biomechanical augmentation remains limited. Bachmaier et al5,6 found that internally braced ACL repair increased overall stabilization and restricted gap formation. Kokubun et al 35 utilized a nylon scaffolding structure to prevent abnormal tibiofemoral subluxation and promote collagen regeneration. These results underscore the importance of biomechanical augmentation in optimizing healing. On the basis of the findings of previous studies, this study evaluated mechanical performance and biological healing through histological assessments at multiple time points. A detailed analysis of ACL healing and mechanical improvements will lay the foundation for future research.
The application of PET materials in sports medicine has shown great potential, particularly with products such as the LARS, bio-knotless anchors, and Trevira hochfest gaining product clearance.20,58,75 However, selecting suitable grafts for augmented ACL repair remains challenging. ACLs endure cyclic loads of approximately 300 N, approximately 1.5 million times annually, with a maximum tensile load of 1730 N and a linear stiffness of 242 N/mm. In contrast, common PET suture tapes, such as Trevira hochfest, offer a maximum tensile load of only 68.3 N and a linear stiffness as high as 1886 N/mm, 21 which may not provide sufficient mechanical support and may result in persistent stress shielding, 53 hindering the healing process. The PET band used in this study demonstrated a high ultimate load capacity and appropriate linear stiffness, showing promising results for the augmentation of ACL repair in rabbits. Therefore, in clinical applications, PET bands should achieve both higher ultimate loads and suitable linear stiffness for optimal performance. Additionally, similar to other PET medical materials, the PET band lacks tissue induction properties, leading to poor host integration after implantation and raising concerns about its long-term effectiveness. Current tissue-engineering strategies, including surface modifications, hybrid fibers, and specialized fiber shapes,10,31,71 may be key methods for addressing these limitations. Consequently, the application of PET bands in ACL repair requires further investigation.
Although ACL reconstruction is considered the standard treatment approach for ACL injuries, ACL repair offers several theoretical advantages. For example, minimally invasive repair techniques allow shorter surgical times, preserve proprioception, and avoid donor site morbidities.1,54,68 However, major challenges persist, with limited evidence of the ability of repair to fully restore tissue structure or mechanical strength, raising concerns regarding long-term outcomes. Furthermore, despite comparable anterior tibial translation and International Knee Documentation Committee scores postoperatively, ACL repair has still shown a higher failure rate.19,24,25,33,36,46,48,63 However, if repair fails, reconstruction remains an alternative.
This study had some limitations. First, the gait pattern of rabbits is different from that of humans because of the use of 4 limbs for weightbearing rather than 2 limbs30,59,73; this difference precluded the complete simulation of clinical conditions, such as all of the suture repair cases failing. Second, findings at time points longer than 16 weeks in repair augmented with a PET band have not been investigated, and healing after 16 weeks needs to be verified in further studies. Additionally, owing to the lack of available measuring instruments for AP laxity testing, this test was performed as reported in previous studies. 30 A customized device for quantitative measurements of knee laxity will be necessary in future studies. Finally, multiple factors affect the prognosis of ACL repair in clinical practice, including the tear site, quality of the torn ends, patient age, and presence of the synovium. However, these factors were not addressed in our study, indicating the need for further research to comprehensively understand their implications.
Conclusion
Repair augmented with a PET band demonstrated the potential to support knee stability and restore structural continuity of the ACL at up to 16 weeks of follow-up in a rabbit model of acute ACL tears. Moreover, the ACL showed the potential for healing and maturation after PET-augmented repair.
Authors
Han Gao, MD, Luyi Sun, MD, Chengxuan Yu, MD, Mingru Huang, MD, Sijia Feng, MD, Dandan Sheng, PhD (Department of Sports Medicine, Huashan Hospital, Fudan University, Shanghai, China); Michael Tim Yun Ong, MD, Fu Sai Chuen Bruma, MD, PhD (Department of Orthopaedics and Traumatology, Faculty of Medicine, The Chinese University of Hong Kong, Hong Kong Special Administrative Region, China); Xing Yang, MD, Yuefeng Hao, MD, PhD (Department of Orthopedics, Affiliated Suzhou Hospital of Nanjing Medical University, Suzhou, China); Christer Rolf, MD, PhD (Division of Orthopedics and Biotechnology, Department of Clinical Science, Intervention and Technology, Karolinska Institute, Stockholm, Sweden); and Shiyi Chen, MD, PhD, Yunxia Li, MD, Jun Chen, PhD (Department of Sports Medicine, Huashan Hospital, Fudan University, Shanghai, China).
Footnotes
Submitted May 29, 2024; accepted January 10, 2025.
One or more of the authors has declared the following potential conflict of interest or source of funding: This work was supported by the National Key R&D Program of China (2021YFA1201303), Clinical Research Plan of SHDC (SHDC2022CRT021), and National Natural Science Foundation of China (82172511). AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.