
Abstract
Background:
There is growing interest in sagittal plane malalignment as a risk factor for patellofemoral chondral wear and, correspondingly, as an important measure to correct when performing certain tibial tubercle osteotomy (TTO) procedures. However, a radiographic method to measure anteriorization after TTO has not been described.
Purpose:
To develop and validate a radiographic method of measuring anteriorization after TTO.
Study Design:
Cross-sectional study (diagnosis); Level of evidence, 3.
Methods:
Patients treated by 2 high-volume sports medicine surgeons at a single institution who underwent a TTO from 2015 to 2023 with available pre- and postoperative radiographic and magnetic resonance imaging (MRI) scans were identified. Approximately 10 mm and 0 mm of operative anteriorization were targeted for the anteromedializing and straight distalizing TTOs, respectively. Two methods to assess anteriorization after TTO on lateral knee radiographs were developed, using the preoperative to postoperative difference in distance between the anterior-most aspect of the tibial tubercle and either the center of the tibial shaft or the anterior tibial plateau. To validate the radiographic techniques, intraclass correlation coefficients (ICCs) were calculated between each method of radiographic measurement and the gold standard MRI measurement (preoperative to postoperative difference in sagittal tibial tubercle–trochlear groove distance).
Results:
There were 70 patients (52 [74%] women) with a mean age of 31.5 ± 9.2 years. The mean anteriorization amount among the 57 anteriorizing TTOs was 4.9 ± 2.5 mm on the x-ray (XR) shaft technique, 4.6 ± 2.6 mm on the XR plateau technique, and 5.3 ± 2.7 mm on MRI (P = .35). The mean anteriorization amount among the 13 straight distalizing TTOs was 0.1 ± 2.5 mm on the XR shaft technique, −0.3 ± 2.2 mm on the XR plateau technique, and 0.6 ± 2.6 mm on MRI (P = .66). There was excellent agreement with MRI for both the XR shaft (ICC, 0.89) and XR plateau (ICC, 0.82) techniques. Interrater reliability was excellent for both techniques (ICC, 0.94-0.95).
Conclusion:
Anteriorization after TTO can be measured using routine pre- and postoperative radiographs. Additionally, the amount of anteriorization achieved with modern anteromedializing TTO techniques was less than that traditionally targeted. Moving forward, surgeons can assess the amount of anteriorization achieved during TTO on standard radiographs, while researchers may investigate the potential role of anteriorization on postoperative outcomes.
Keywords
Patellofemoral (PF) malalignment is a well-known risk factor for PF pain, chondromalacia, and/or instability. These conditions account for substantial disease burden, especially among young women.10,33 While these conditions can often be managed nonoperatively, the tibial tubercle osteotomy (TTO) is a versatile surgical treatment option when nonoperative measures fail. 31 Depending on the patient’s specific pathology, TTOs can be adapted to improve patellar tracking within the trochlea and/or reduce the PF contact forces on the articular cartilage. 31
Traditionally, the majority of clinical focus has been on axial (ie, patella alta) and coronal (ie, a lateralized tibial tubercle) plane PF malalignment as risk factors for PF symptoms. Specifically, a lateralized tibial tubercle (as frequently measured by an increased tibial tubercle–trochlear groove [TT-TG] distance) and increased patellar height (as frequently measured by the Caton-Deschamps Index [CDI], among other techniques) have been associated with increased chondral wear and/or instability.13,20,26,31 As such, these measures figure prominently into surgical planning, and the success of various TTO surgeries at improving these measures has been studied at length.16,19
Recently, however, there has been growing interest in sagittal plane malalignment as a risk factor for PF chondral wear, as well as an increasingly important measure to surgically correct when performing cartilage restoration procedures. As described by Lansdown et al, 18 the sagittal TT-TG (sTT-TG) is a method for assessing the relative amount of posteriorization of the tibial tubercle relative to the trochlea. Decreased sTT-TG (ie, increased posteriorization) has been shown to be associated with increased PF chondral wear in several recent studies.15,18,25,32 These results have spurred focus on the importance of anteriorization in many TTO procedures (ie, when unloading the PF cartilage is a goal of surgery) and stimulated a renewed interest in straight anteriorizing TTOs.28,32 To date, however, there are little data on how sagittal plane alignment changes after various TTO techniques, nor is there any currently described method to measure this parameter from routine pre- and postoperative radiographs. Therefore, the purpose of this study was to develop and validate a radiographic method of measuring anteriorization after TTO. We hypothesized that we would be able to develop a radiographic technique that yielded excellent agreement compared with a magnetic resonance imaging (MRI) gold standard.
Methods
This was a retrospective review of patients undergoing TTO by 2 experienced PF surgeons (S.M.S., A.H.G.) at a single institution from 2015 to 2023. Inclusion criteria consisted of all TTO patients for whom pre- and postoperative MRI scans and calibrated lateral knee radiographs were available. Given that sTT-TG can vary substantially with knee flexion, 21 any patients whose knees were in >10° of flexion on MRI were excluded (n = 9). Additionally, patients without satisfactory lateral radiographs pre- and postoperatively—defined as having the posterior aspects of the femoral condyles superimposed or within 5 mm and clearly depicting the PF and tibiofemoral joints (to account for abduction/adduction)5,14—were excluded (n = 2). Patients with excessive metal artifact preventing visualization of the anterior tubercle on postoperative MRI were excluded (n = 2). Finally, patients undergoing concurrent PF joint arthroplasty, high tibial osteotomy, and/or distal femur osteotomy were excluded (n = 3), as these procedures prevented assessment of anteriorization from the TTO. There were no other exclusion criteria.
After extensive development of various ways to radiographically measure anteriorization, 2 methods were proposed for formal assessment. The first strategy used the proximal anatomic axis of the tibial shaft as a reference (shaft technique), with this line determined similarly to how it is determined in the measurement of posterior tibial slope.4,14,37 In particular, the distance from the most anterior portion of the tibial tubercle to the center of the tibial shaft was measured on pre- and postoperative lateral knee radiographs, with the difference between these measurements (postoperative minus preoperative) representing the anteriorization amount. To obtain the center of the shaft reference line, 2 circles were drawn encompassing the anterior and posterior cortices of the tibial shaft 5 cm and 15 cm distal to the plateau, respectively, and the line bisecting the center of these circles represented the center of the tibial shaft (Figure 1), consistent with well-defined techniques for posterior tibial slope.4,14,37 The second strategy used the most anterior aspect of the tibial plateau as a reference (plateau technique). Specifically, the anatomic axis was defined as above. Next, a line was drawn parallel to the anatomic axis and tangent to the anterior-most point of the tibial tubercle. Finally, the distance from the anterior tubercle tangent line to the most anterior portion of the tibial plateau was measured. The difference between these measurements pre- and postoperatively (postoperative minus preoperative) again represented the anteriorization amount (Figure 2).
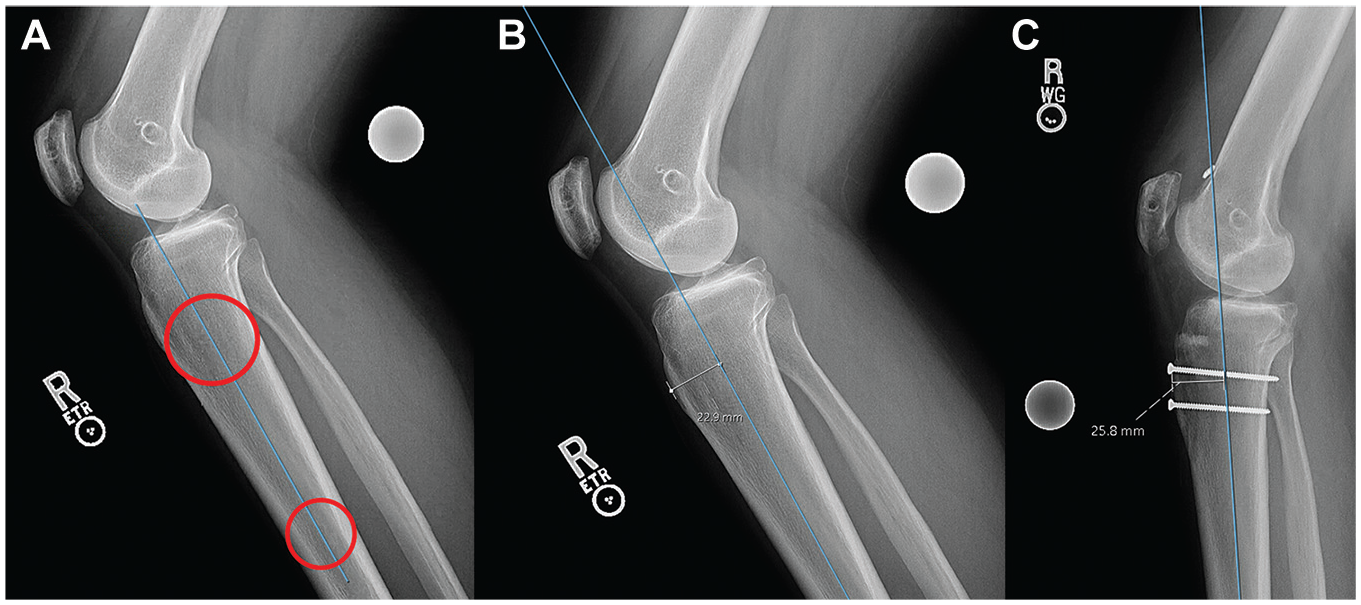
Shaft (proximal anatomic axis) anteriorization measurement. (A) Two circles, one at 5 cm from the tibial plateau and one 15 cm from the tibial plateau, are drawn. A line that bisects the 2 circles is then used as the reference point. (B) The anterior distance is measured as the distance from the line drawn in part A to the most anterior aspect of the tibial tubercle (22.9 mm). (C) Utilizing the methods explained in parts A and B, the postoperative XR is measured with a distance of 25.8 mm. The anteriorization amount is then calculated (postoperative minus preoperative): 25.8 − 22.9 = 2.9 mm.
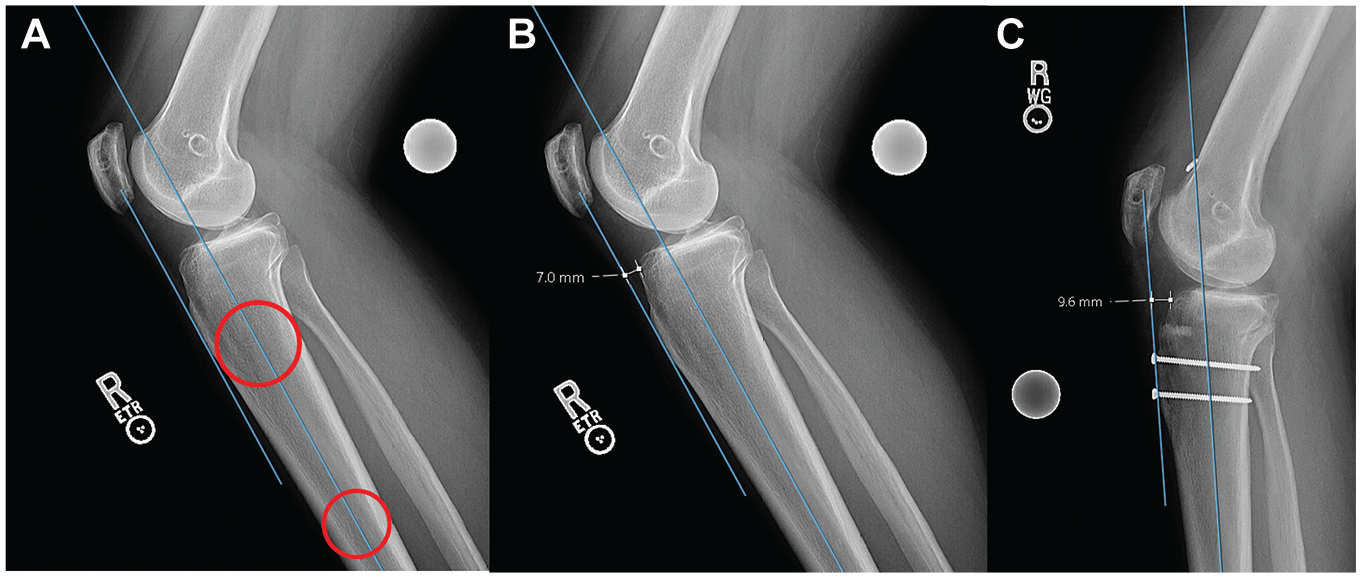
Anterior plateau anteriorization measurement. (A) First, the anatomic axis of the proximal tibia is determined. Two circles, one at 5 cm from the tibial plateau and one 15 cm from the tibial plateau, are drawn, with the line that bisects these circles representing the anatomic axis. Second, a line is drawn parallel to the anatomic axis and tangential to the anterior-most aspect of the tibial tubercle. (B) The distance from the anterior aspect of the tibial plateau to the tangential line is measured as 7.0 mm. (C) Utilizing the methods explained in parts A and B, the postoperative XR is measured with a distance of 9.6 mm. The anteriorization amount is then calculated (postoperative minus preoperative): 9.6 − 7.0 = 2.6 mm.
Given that it is the currently utilized technique and has been validated in a cadaveric setting,1,15,18,19,21,25,34 change in sTT-TG on MRI was used as the gold standard for anteriorization amount. Sagittal TT-TG was measured using the standard methodology as described by Lansdown et al. 18 Specifically, using the axial proton-density MRI sequence, we identified the anterior-most aspect of the tibial tubercle. Next, the anterior surface of the trochlear cartilage was identified at the nadir of the trochlear groove. Finally, the distance between these 2 points along a line perpendicular to the posterior condylar axis was measured, representing the sTT-TG. The difference between the pre- and postoperative sTT-TGs (postoperative minus preoperative) represented the anteriorization amount (Figure 3).
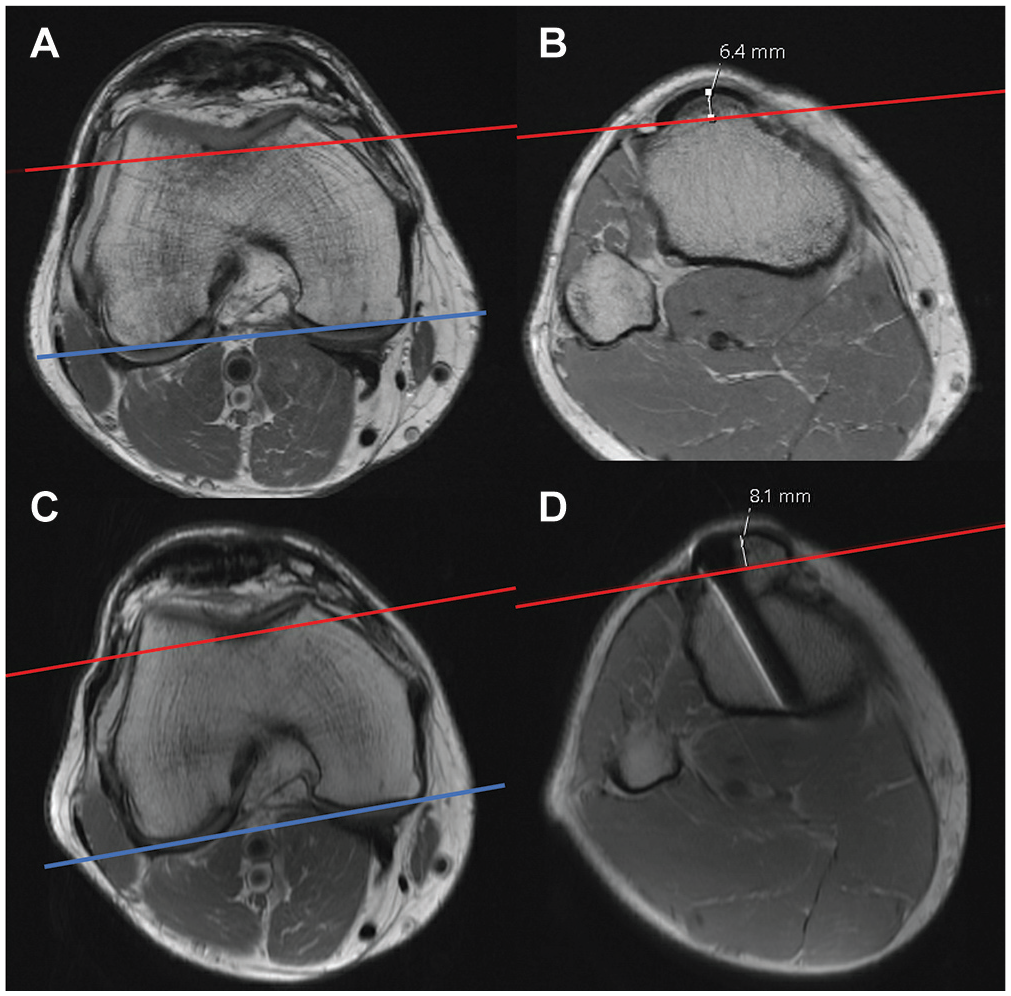
Magnetic resonance imaging (MRI) anteriorization measurement. (A) Using the axial proton-density MRI sequence, we identify the anterior surface of the trochlear cartilage at the nadir of the trochlear groove. A line parallel to the posterior condyles (blue line) at the nadir of the trochlear cartilage is drawn (red line). (B) Next, the anterior-most aspect of the tibial tubercle is identified. The distance between the red line and the anterior-most aspect of the tibial tubercle is measured, representing the sagittal tibial tubercle–trochlear groove distance. (C) Similar steps are taken marking the nadir of the trochlear groove on the postoperative MRI scan. (D) The anteriorization amount is then calculated (postoperative minus preoperative): 8.1 mm − 6.4 mm = 1.7 mm.
As the goal of this study was to develop a radiographic method for measuring anteriorization after TTO regardless of type or indication, all TTO types that are performed by the senior surgeons (S.M.S., A.H.G.) were included. Specifically, depending on symptomatology and alignment, patients underwent either anteromedializing TTO (AMZ-TTO), straight distalizing TTO (TTO-d), or AMZ-TTO with distalization (AMZ-TTO-d). The specific surgical techniques have been described in detail previously.27,30 For anteriorizing TTOs (ie, AMZ-TTO and AMZ-TTO-d), roughly 10 mm of anteriorization was typically targeted. For TTO-ds, no change in sagittal plane alignment was targeted (ie, 0 mm of anteriorization/posteriorization). In general, patients with painful PF chondromalacia and/or recurrent patellar instability underwent AMZ-TTO if they had coronal plane malignment due to a lateralized tibial tubercle (ie, TT-TG, ≥15) without significant patella alta (CDI, <1.3), TTO-d if they had patella alta (ie, CDI, ≥1.3) without coronal plane malignment (ie, TT-TG, <15), and AMZ-TTO-d if they had combined coronal plane malignment (ie, TT-TG, ≥15) and patella alta (ie, CDI, ≥1.3). During the study period, excessive posteriorization alone was not recognized as an indication for TTO in the authors’ practices.
Electronic medical records were reviewed to collect numerous patient factors. Demographic factors collected included age, sex, body mass index, laterality, smoking status, and osteotomy type. The primary outcome measures were the agreements in anteriorization measurement between each proposed radiographic technique and the MRI gold standard. Secondary outcomes included agreement between the 2 proposed radiographic techniques, as well as measuring the mean amount of anteriorization after TTO procedures.
Statistical Analysis
Anteriorization measurements were performed in random order by 2 trained physicians (N.H.V., N.P.L.). The raters were blinded to their corresponding measurements for the other parameters (eg, when obtaining the postoperative shaft measurement, the raters were unaware of what they measured for the preoperative shaft measurement, the pre- or postoperative plateau measurement, or the MRI measurements). Similarly, the raters were blinded from each other’s measurements. The means of the 2 raters’ measurements were calculated, and these means were then used to assess the agreement between techniques. Specifically, to assess performance of the proposed XR measurements in comparison with the MRI gold standard, intraclass correlation coefficients (ICCs) were calculated comparing MRI with (1) the XR shaft technique and (2) the XR plateau technique. In addition, to assess agreement between the 2 radiographic measures with each other, the ICC of the radiographic techniques was calculated. For each of the 3 measurement techniques, ICCs were calculated to assess interrater reliability between the 2 raters. Finally, to assess intrarater reliability, 1 rater repeated measurements on a random sample of 20 patients at least 30 days after the initial assessment. Consistent with historical standards, scores ≥0.75 were considered to represent excellent agreement, 0.6 to 0.74 good, 0.4 to 0.59 fair, and <0.4 poor.7,14,21 To further contextualize the results, standard Pearson correlation coefficients (R) were also calculated between techniques. Categorical variables are presented as number (percent). Continuous variables are reported as mean ± standard deviation. One-way analysis of variance was used to assess for differences in mean anteriorization values between measurement techniques. All radiological measurements were made in the Sectra IDS7 (Sectra Medical Systems AB) picture archiving and communication system. All statistics were performed in SAS Version 9.4 (SAS Institute), and a P value <.05 was considered statistically significant. This study was approved by our institutional review board.
Results
Patient Sample
There were 70 patients meeting inclusion criteria, including 41 (58.6%) undergoing AMZ-TTO, 13 (18.6%) undergoing TTO-d, and 16 (22.9%) undergoing AMZ-TTO-d. The mean age was 31.5 ± 9.2 years. There were 52 (74%) women and 18 (26%) men. The mean body mass index was 27.2 ± 5.7 kg/m2. Additional demographic data are listed in Table 1.
Baseline Demographic Data Among the 70 Included Patients a

Continuous data are presented as mean (SD). Categorical data are presented as n (%). AMZ, anteromedializing; BMI, body mass index; Dist, straight distalizing; Dist+AMZ, anteromedializing with distalization.
Anteriorization After TTO
The mean anteriorization amount among the 57 anteriorizing TTOs (AMZ-TTO or AMZ-TTO-d) was 4.9 ± 2.5 mm on the XR shaft technique, 4.6 ± 2.6 mm on the XR plateau technique, and 5.3 ± 2.7 mm on MRI (Table 2). These values did not significantly differ between measurement techniques (P = .35). The mean anteriorization amount among the 13 TTO-ds was 0.1 ± 2.5 mm on the XR shaft technique, −0.3 ± 2.2 mm on the XR plateau technique, and 0.6 ± 2.6 mm on MRI. These values did not significantly differ between techniques (P = .66).
Magnitude of Anteriorization After TTO as Determined by Various Imaging Techniques a

Data are presented as mean (SD) in millimeters. MRI, magnetic resonance imaging; TTO, tibial tubercle osteotomy.
Validation of Radiographic Measurements of Anteriorization
Both proposed radiographic techniques for measuring anteriorization demonstrated excellent agreement and correlation with the MRI gold standard (Table 3). Specifically, the XR shaft technique demonstrated an ICC with the MRI gold standard of 0.89 and a correlation coefficient of 0.90 (P < .001). The XR plateau technique demonstrated an ICC with the MRI gold standard of 0.82 and a correlation coefficient of 0.84 (P < .001). The radiographic techniques also had high agreement (ICC, 0.91) and correlation (R = 0.91; P < .001) with each other.
ICCs and Pearson Correlation Coefficients (R) With Corresponding P Values for the Agreement in Measurement Between the Various Imaging Modalities a

ICC, intraclass correlation coefficient; MRI, magnetic resonance imaging.
ICC scores ≥0.75 represent excellent agreement, 0.6-0.74 good, 0.4-0.59 fair, and <0.4 poor. 7
P values correspond to the R values only.
Inter- and Intrarater Reliability
In terms of interrater reliability, all 3 measurements of anteriorization were highly reproducible with excellent interrater agreement (Table 4). Specifically, the ICCs were 0.950 for the XR shaft technique, 0.939 for the XR plateau technique, and 0.942 for the MRI technique. Similarly, intrarater reliability was excellent, with ICCs of 0.989 for the XR shaft technique, 0.975 for the XR plateau technique, and 0.973 for the MRI technique.
ICCs for the Agreement Between (ie, Interrater Reliability) and Within (ie, Intrarater Reliability) Raters for the Various Imaging Techniques a

ICC scores ≥0.75 represent excellent agreement, 0.6-0.74 good, 0.4-0.59 fair, and <0.4 poor. 7 ICC, intraclass correlation coefficient; MRI, magnetic resonance imaging.
Discussion
The principal findings of the current study are as follows: (1) anteriorization after TTOs can be measured simply from routine pre- and postoperative radiographs, (2) this radiographic technique to measure anteriorization results in high inter- and intrarater agreement, and (3) the anteriorization amount achieved after anteriorizing procedures may be less than that typically targeted. These findings have a number of implications for the sports medicine surgeon and the role of anteriorization on outcomes after TTO.
The most important contribution of this study was the demonstration of a radiographic method to assess anteriorization using routine pre- and postoperative radiographs. Anteriorization is a critical component of many TTO surgeries in the setting of chondral wear. As described by Maquet, 22 the PF joint experiences a compressive joint reactive force from the pull of the quadriceps muscle and the counterforce from the patellar tendon. He demonstrated that anteriorizing the tubercle 20 mm can reduce this force up to 50%. While the Maquet procedure has generally fallen out of favor due to wound complications and nonunion,23,28 the principle of anteriorization remains a critical component of many TTO techniques performed today, including the anteromedializing, Fulkerson-type, 11 TTO, and modern techniques for straight anteriorizing TTOs. 28 Indeed, expert consensus suggests that when performing cartilage repair on bipolar PF cartilage lesions, concurrent anteriorization should be strongly considered to “unload” or protect the cartilage repair. 6 This belief is supported by biomechanical data demonstrating the ability of anteriorizing TTOs to reduce PF contact forces. For example, in cadaveric studies, Beck et al 3 demonstrated that AMZ-TTOs reduce trochlear contact pressures, while Lamplot et al 17 recently demonstrated that AMZ-TTOs reduce patellar contact pressures in patients with PF dysplasia. Similarly, Rue et al 29 found that straight anteriorizing TTOs reduce trochlear contact pressures by 20% to 32%. Ultimately, anteriorization is an increasingly important consideration in the surgical planning of, and postoperative assessment after, TTO, and the currently described technique to measure this on radiographs will greatly increase clinicians’ ability to evaluate this important parameter after surgery, as most patients do not undergo MRI postoperatively.
We propose that the tibial shaft XR method be the preferred method for adoption. Compared with the plateau method, the shaft method had somewhat higher agreement with MRI (ICC, 0.89 vs 0.82). It is possible that by the reference line being the center of the anatomic axis, this measurement is less susceptible to small rotational changes, improving accuracy. Moreover, while where to choose the anterior-most part of the tibial plateau could require a degree of subjectivity given the varying morphologies of anterior proximal tibias (eg, where the tibia starts to round into plateau vs the flat part of the plateau), the assessment of the center of the tibial shaft is performed in an entirely objective manner. As such, we believe the tibial shaft technique is best suited to measure anteriorization moving forward in clinical and research applications.
There are several potential advantages to measuring anteriorization using radiographs compared with MRI scans. First, radiographs are much more readily available and cost-effective, as pre- and postoperative radiographs are already performed as a routine aspect of clinical care to assess osteotomy healing. Second, radiographic measurement is less affected by metal artifact; 2 patients had to be excluded from this study because the anterior aspect of the tubercle was not visible because of the metal artifact induced by the screws on MRI. This is never a problem when performing the proposed measurements on radiographs. Third, while it cannot be assessed in the current study and would likely require cadaveric analysis, the radiographic technique may actually be more accurate for measuring anteriorization than MRI. Specifically, MRI measurement of sTT-TG is greatly affected by knee flexion. 21 Although we excluded patients who had >10° of flexion on MRI, even small changes in knee flexion change the sTT-TG measurement, and it is possible that some of the discrepancy in radiographic and MRI results is because of small (ie, <10°) changes in knee flexion angle between MRI studies. In contrast, the proposed radiographic techniques are unaffected by knee flexion angle. To be sure, radiographic measurements may be affected by rotational changes; at worst, however, a lateral knee radiograph can be readily repeated to improve alignment if needed.
The reproducibility of the measurements for anteriorization observed in this study can be benchmarked by other recent studies on sTT-TG. For example, among 6 cadaveric specimens imaged at varying flexion angles, MacLean et al 21 reported ICCs for MRI measurement of sTT-TG ranging from 0.95 to 0.98. In a study of 47 patients with cartilage restoration and 94 patients who underwent meniscectomy being assessed for sTT-TG on MRI, Kaplan et al 15 found an ICC of 0.93 between their raters. In a computed tomography–based study of sTT-TG (termed “anteroposterior TT-TG”) on 22 symptomatic and 22 asymptomatic knees, Tanaka et al 34 found an ICC of 0.82 for this measure. These interrater reliabilities are similar to what was achieved in the current study validating radiographic anteriorization measurements for both the shaft-based (ICC, 0.95) and plateau-based (ICC, 0.94) techniques. Similarly, these reference values demonstrate how accurate the shaft-based XR technique was (ICC, 0.89) in comparison with the MRI gold standard. That is, a different measurement technique on a different imaging modality was able to achieve agreement at a similar level to what has been achieved historically for raters performing the same measurement on the same imaging modality. Taken together, these results demonstrate that the proposed radiographic technique for measuring anteriorization is both accurate and reproducible.
Interestingly, a secondary finding of this study was that the anteriorization amount achieved as determined on postoperative imaging generally tended to be lower than that aimed for intraoperatively. Traditionally, surgeons aim for a goal of 10 to 15 mm of anteriorization,8,9,12,18 which is supported by biomechanical studies suggesting a minimum of 10 mm of anteriorization is needed to appreciably reduce PF contact forces.2,24 Despite a goal of approximately 10 mm typically being sought by the operating surgeons of this study, the mean anteriorization amount achieved for the anteriorizing TTOs was only about 5 mm. These results raise questions about either the validity of the traditional 10-mm anteriorization goal being necessary for clinical benefit or the relative biomechanical benefit that may or may not exist from the magnitude of anteriorization being achieved in the in vivo setting with current surgical techniques. The proposed measurement technique may enable future research to better assess the role of anteriorization amount on clinical outcomes after TTO.
Limitations
Although this study has numerous strengths including its novelty, high interrater reliability, and large sample size, it is not without limitations. While we assessed 2 specific techniques for measuring anteriorization on radiographs based on the most promising proposals generated in an extensive development process, other methods are theoretically conceivable. Next, although results were consistent across 2 experienced PF surgeons in the current study, the secondary outcome that the anteriorization amount was less than aimed for intraoperatively may not generalize to other surgeons or techniques. The vast majority of MRI scans in this study were performed with advanced metal suppression technology, 36 and the osteotomy screws were generally not placed at the anterior apex of the shingle; nevertheless, 2 patients had to be excluded due to metal artifact preventing anteriorization measurement. Finally, while this was a retrospective study, this is only a minor limitation as we did not attempt to prognosticate outcomes from these measurements. 35
Conclusion
Anteriorization after TTO can be reliably measured using routine pre- and postoperative radiographs. We propose that measuring the distance between the anterior tibial tubercle and the central tibial shaft may be the most reproducible method. Moreover, we found that the anteriorization achieved with the modern AMZ-TTO techniques used in this study was less than the anteriorization that historical standards believed to be necessary for biomechanical benefit. Moving forward, surgeons can assess the amount of anteriorization achieved during TTO on standard radiographs, while researchers may investigate the potential role of anteriorization on postoperative outcomes.
Footnotes
Submitted August 10, 2024; accepted January 29, 2025.
One or more of the authors has declared the following potential conflict of interest or source of funding: A.H.G. has received speaking fees from Bioventus and Organogenesis; research support from Cartiheal, JRF, Moximed, Organogenesis, and Vericel; consulting fees from JRF, Moximed, Smith & Nephew, Flexion Therapeutics, and Vericel; nonconsulting fees from Linvatec and Pacira Pharmaceuticals; honoraria from Fidia Pharma; and royalties from Organogensis; he also holds stock or stock options in Engage and Stryker. S.M.S. has received consulting fees from Smith & Nephew, Miach, Vericel, and Flexion Therapeutics; research support from Miach and Vericel; and honoraria from JRF; she also holds stock or stock options in Engage and Stryker. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.