
Abstract
Background:
Intra-articular (IA) injections of orthobiologics, such as platelet-rich plasma (PRP) and microfragmented adipose tissue (MFAT), have recently gained attention as treatments for knee osteoarthritis (OA). However, clinical evidence supporting their use remains limited.
Purpose:
To evaluate the effectiveness and safety of IA injections of PRP and MFAT in patients with knee OA and to compare these 2 treatment modalities.
Study Design:
Systematic review and meta-analysis; Level of evidence, 2.
Methods:
A systematic search was conducted in the MEDLINE, Embase, and Cochrane Library databases to identify randomized controlled trials assessing the efficacy and safety of PRP or MFAT injections in knee OA. Outcomes included pain relief (measured by the 100-mm visual analog scale), functional improvement (assessed by the Knee injury and Osteoarthritis Outcome Score and International Knee Documentation Committee subjective score), and safety (assessed by procedure-related adverse events). The minimal clinically important difference was used to evaluate the clinical significance of the treatments, and a meta-analysis was performed to compare PRP and MFAT. Methodological quality was assessed using the Modified Coleman Methodology Score.
Results:
Six randomized controlled trials were included in the analysis. Both PRP and MFAT achieved minimal clinically important difference in most clinical outcomes up to 12 months after injection. The meta-analysis revealed comparable results for pain relief, functional improvement, and safety between the MFAT and PRP groups from 1 to 24 months after treatment. However, at the 6-month mark, MFAT demonstrated a small but statistically significant advantage over PRP in most clinical outcomes. The median Modified Coleman Methodology Score was 73 (range, 70-75).
Conclusion:
IA injections of PRP and MFAT both provided significant clinical benefits and were safe for treating knee OA over a 12-month period. Although no substantial differences were observed between the 2 treatments in most follow-up periods, MFAT showed slightly better pain relief and functional improvement at 6 months. However, further research is needed to confirm these findings and guide clinical practice.
Keywords
Orthobiologics have recently garnered significant attention as a means to address the low intrinsic regenerative potential of the osteoarthritic environment.12,19,30 Among these treatments, blood-derived products such as platelet-rich plasma (PRP) and cell-based therapies containing mesenchymal stromal cells (MSCs) are increasingly used for knee osteoarthritis (OA).12,19 A substantial body of literature supports the effectiveness of PRP,6,32,33,48,50 with high-level studies, including randomized controlled trials (RCTs) and meta-analyses, demonstrating its superiority over placebo, steroid injections, and viscosupplements.6,32,48,50 As PRP has shown the potential to modulate the intra-articular (IA) environment, PRP offers clinically relevant functional improvement and pain relief at short-term follow-up compared with placebo for the treatment of knee OA.7,44
Although the role of PRP in treating OA has become more established, newer cell-based therapies, particularly those derived from adipose tissue, have emerged.12,19,31 Adipose tissue, known for its accessibility and abundance,28,31 is now processed into microfragmented adipose tissue (MFAT) through a point-of-care procedure that preserves cell integrity and tissue microarchitecture without requiring culture expansion or enzymatic treatment.14,22 This process provides an abundant source of stromal cells and growth factors while circumventing strict regulatory requirements.4,51,54
Given the potential of orthobiologics as disease-modifying treatment for knee OA, interest has increased in comparing the regenerative and immunomodulatory effects of MFAT with those of PRP.31,32 However, despite this potential, existing guidelines have yet to endorse orthobiologics for nonoperative knee OA treatment, partly due to a lack of direct comparative evidence between MFAT and PRP. 2
To address this gap, we conducted a systematic review and meta-analysis of RCTs to provide comprehensive information on the effectiveness and safety of IA injections of MFAT and PRP. Our study aimed to directly compare these 2 treatment modalities in patients with knee OA, with the goal of informing clinical decision-making and future guidelines. The hypothesis was that MFAT and PRP would be effective for treating knee OA, with both techniques demonstrating comparable effectiveness and safety.
Methods
Literature Search
This systematic review and meta-analysis adhered to the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines 42 and was registered in the International Prospective Register of Systematic Reviews (registration No. CRD42024533189). A comprehensive search was performed by 2 independent reviewers (J-H.K. and S.K.L.) using PubMed (MEDLINE), EMBASE, and the Cochrane Library, covering studies from inception to April 30, 2024, based on a predefined search strategy. The search used the following keywords: (“adipose*”) AND (“microfragmented” OR “stromal*” OR “adipose tissue”) AND (“platelet rich plasma” OR “PRP”) AND (“knee”) AND (“osteoarthritis”). Bibliographies of the identified studies were manually reviewed to identify additional relevant articles, with no language restrictions applied.
Study Selection
Titles and abstracts were screened by 2 reviewers (J-H.K. and S.K.L.). Full-text articles were reviewed if the abstracts did not provide sufficient data. Discrepancies were resolved by consensus or consultation with a third author (Y-B.P.). Studies were included or excluded based on the Population, Intervention, Comparison, Outcomes, and Study design (PICOS) criteria 37 (Table 1): Population (patients with knee OA), Intervention (IA injection of autologous MFAT), Comparison (IA injection of PRP), Outcomes (clinical outcomes and safety) and Study design (level of evidence [LOE] 1 and 2).
Inclusion and Exclusion Criteria Based on PICO a
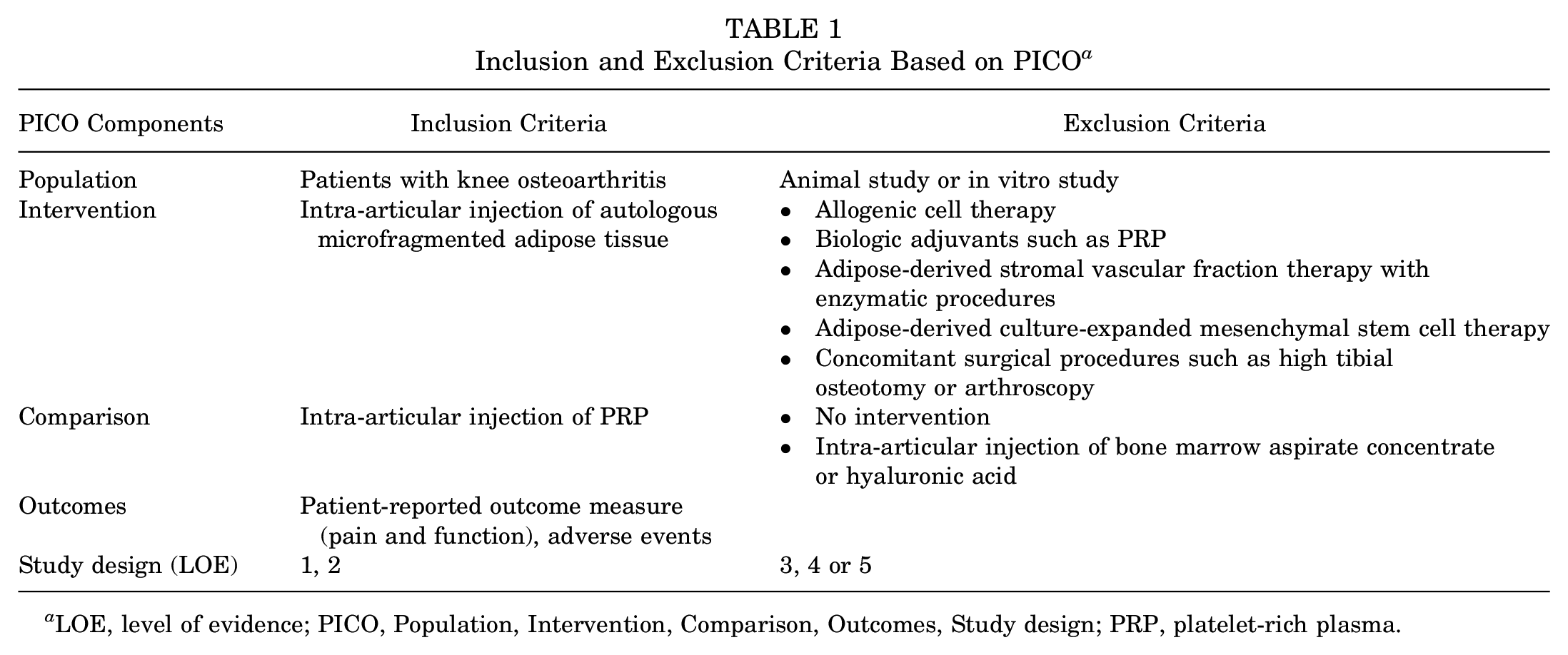
LOE, level of evidence; PICO, Population, Intervention, Comparison, Outcomes, Study design; PRP, platelet-rich plasma.
Assessment of Literature and Methodological Quality
Two independent reviewers (J-H.K. and S.K.L.) evaluated the quality of the included studies. The LOE was assessed according to established criteria from previous publications. 39 The methodological quality was evaluated using the Modified Coleman Methodology Score (MCMS),13,15 which assesses various aspects of study design and execution, including inclusion criteria, sample size calculation, randomization, follow-up, patient analysis, blinding, treatment similarity, treatment description, group comparability, outcome assessment, rehabilitation protocol description, clinical effect measurement, and patient count. The MCMS scores range from 0 to 100, with higher scores indicating a more robust method. Scores were classified as follows: >85, excellent; 70 to 84, good; 55 to 69, fair; ≤54, poor. 15 Disagreements were resolved by consensus or consultation with a third author (Y-B.P).
Assessment of Risk of Bias
Two independent reviewers (J-H.K. and S.K.L.) assessed the risk of bias in the included RCTs using the Cochrane Handbook for Systematic Reviews of Interventions. 27 This tool evaluates bias across several domains: selection, performance, detection, and attrition. Disagreements between reviewers were resolved through discussion or adjudication by a third author (Y-BP).
Nomenclature
MFAT was defined according to the consensus statement on nomenclature by the International Society of Cellular Therapy. 10 The PAW classification system standardizes PRP by categorizing it based on platelet concentration (P1-P4, relative to baseline level), activation status (A– or A+), and white blood cell content (W– or W+), and the system was used to categorize PRP as leukocyte-poor (LP) or leukocyte-rich (LR), as established in previous studies.17,36,47 LP-PRP is defined as PRP with a leukocyte concentration equal to or below that of the baseline whole blood, whereas LR-PRP is defined as PRP with a leukocyte concentration above the baseline whole blood. 20
Data Extraction
The same reviewers independently extracted data from the included studies. Disagreements were resolved through discussion or consultation with a third author (Y-B.P). Collected data included study characteristics (author, year of publication, country, sample size, and LOE), patient characteristics (mean age, sex proportion, mean body mass index, follow-up duration, and OA grading), and intervention details (MFAT and PRP). Outcome measures for pain (100-mm visual analog scale [VAS] score), function (Knee injury and Osteoarthritis Outcome Score [KOOS] and International Knee Documentation Committee [IKDC] subjective score), and safety (procedure-related pain or swelling, adverse events [AEs], and serious AEs) were recorded using a predefined data form. For missing data, we first attempted to contact the study authors. If contact failed, we estimated missed values using methods outlined in the Cochrane guidelines. 27
Statistical Analysis
The primary objectives of this systematic review were to evaluate the clinical significance of MFAT and PRP and to compare their effectiveness in terms of pain relief, functional improvement, and safety. Clinical outcomes were assessed by comparing postinjection values with preinjection values using formulas from the Cochrane guidelines. 27 The minimal clinically important difference (MCID) was used to assess clinical significance based on pooled data from the included studies.8,16,34,45,52 When feasible, meta-analysis was conducted to calculate the standardized mean difference (MD) with 95% CIs for continuous variables and the risk ratio with 95% CIs for dichotomous variables. If meta-analysis could not be performed due to insufficient data, a qualitative description of the outcomes was provided. Publication bias was not assessed, as it was deemed unnecessary with <10 studies in comparison. 27 Heterogeneity was evaluated using I2 statistics to estimate the proportion of variation due to differences between studies. 41 Fixed-effects meta-analysis was used to pool outcomes across studies. Forest plots, constructed with RevMan Version 5.4 (The Cochrane Collaboration), were used to display outcomes, pooled effect estimates, and overall summary effects. Statistical significance was set at P < .05.
Results
Identification of Studies
The initial electronic search identified 348 studies, and 1 additional study was identified from a manual search. After removal of 109 duplicates, 240 studies remained. Of these, 217 were excluded based on title or abstract, and 17 were excluded after full-text review. Ultimately, 6 RCTs4,5,18,24,31,55 were included in this systematic review (Figure 1).
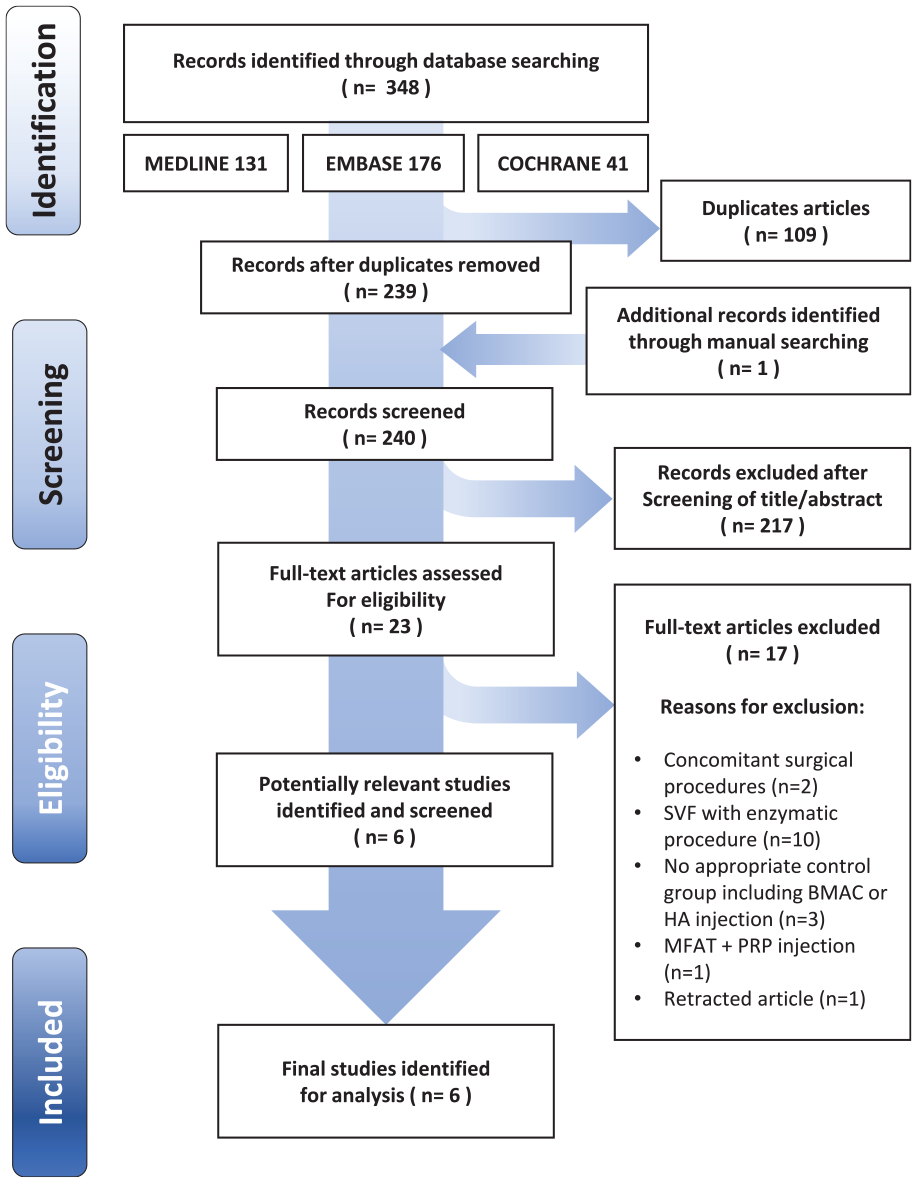
PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) flow diagram for the identification and selection of studies. BMAC, bone marrow aspirate concentrate; HA, hyaluronic acid; MFAT, microfragmented adipose tissue; PRP, platelet-rich plasma; SVF, stromal vascular fraction.
Study Characteristics
A total of 415 knees with OA were included. Four RCTs included patients with Kellgren-Lawrence (K-L) grade 1 to 4,4,5,31,55 whereas 2 RCTs included patients with K-L grade 1 or 2.18,24 Follow-up periods varied: 1 RCT 5 had a follow-up of up to 6 months, 3 RCTs up to 12 months,4,18,31 and 2 RCTs up to 24 months24,55 (Table 2). Among the 6 RCTs, 3 studies4,5,55 compared MFAT with LR-PRP, and the remaining 3 studies18,24,31 compared MFAT with LP-PRP. All studies used the Lipogems system (Lipogems International SpA) for mechanical agitation of adipose tissue (Table 3). The study by Dallo et al 18 was excluded from the meta-analysis due to overlapping data with the study by Gobbi et al, 24 which had a longer follow-up period. Additionally, data from Baria et al 5 were included in the meta-analysis up to 6 months, whereas data from the follow-up study by Baria et al 4 were included for the 12-month period due to reduced sample size.
Study Design and Demographic Characteristics of Included Studies a
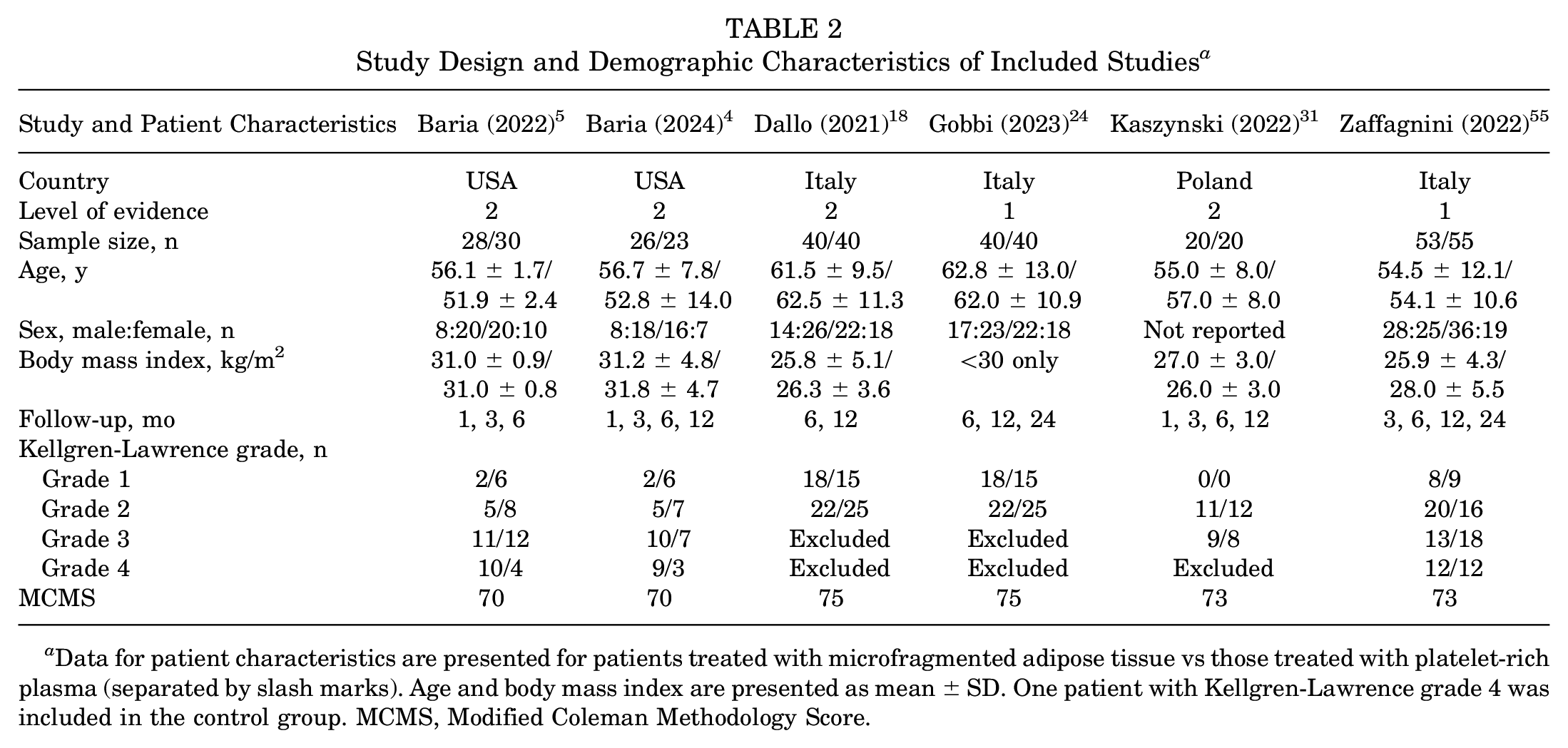
Data for patient characteristics are presented for patients treated with microfragmented adipose tissue vs those treated with platelet-rich plasma (separated by slash marks). Age and body mass index are presented as mean ± SD. One patient with Kellgren-Lawrence grade 4 was included in the control group. MCMS, Modified Coleman Methodology Score.
Protocol Details for the Interventions in Included Studies a
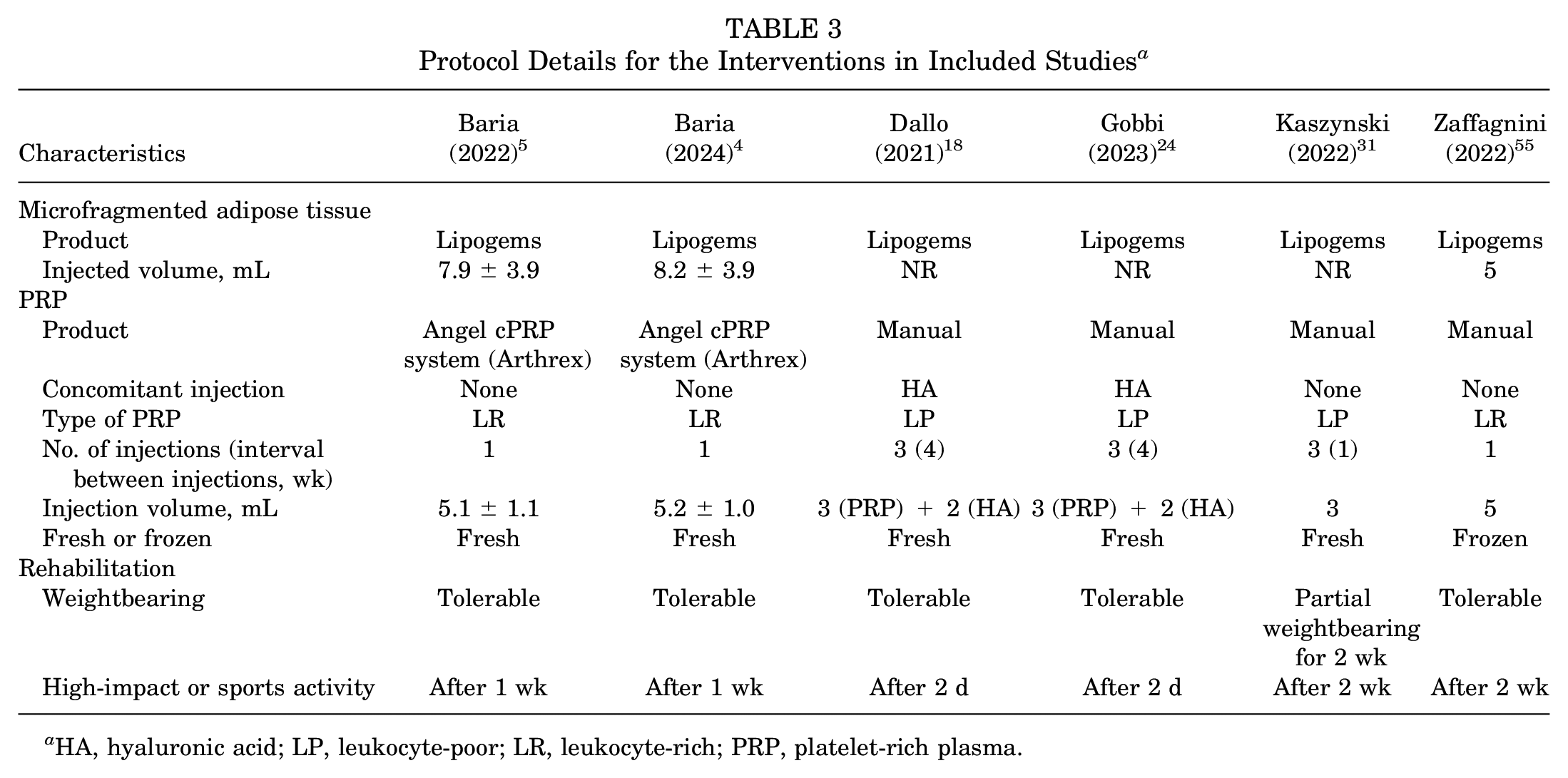
HA, hyaluronic acid; LP, leukocyte-poor; LR, leukocyte-rich; PRP, platelet-rich plasma.
Assessment of Literature and Methodological Quality and Risk of Bias
Two studies24,55 were classified as LOE 1 and the remaining 4 studies4,5,18,31 as LOE 2. All included studies4,5,18,24,31,55 were assessed as high quality based on the MCMS, with a median score of 73 (range, 70-75). The risk of bias was low across all studies, with no high-risk areas identified (see the Appendix Figure, available in the online version of this article).
Clinical Significance Based on MCID Achievement
The pooled analysis demonstrated that clinical improvements surpassed the MCID for all outcome measures from 1 to 12 months after both MFAT and PRP IA injections (Figure 2). At 24 months, improvements in the MFAT and PRP groups fell below the MCID for several measures, including the 100-mm VAS, KOOS-Symptom, KOOS-Sport, KOOS-Pain, KOOS–Activity of Daily Living, and IKDC subjective scores.

Clinical improvements after MFAT or PRP intra-articular injection from 1 to 24 months. (A) 100-mm VAS, (B) KOOS-Pain, (C) KOOS-Symptom, (D) KOOS-ADL, (E) KOOS-Sports, (F) KOOS-QoL, (G) IKDC subjective score. ADL, Activity of Daily Living; IKDC, International Knee Documentation Committee; KOOS, Knee injury and Osteoarthritis Outcome Score; MCID, minimal clinically important difference; MFAT, microfragmented adipose tissue; PRP, platelet-rich plasma; QoL, Quality of Life; VAS, visual analog scale.
Pain Improvement (100-mm VAS and KOOS-Pain)
No significant differences in pain improvement were observed between the 2 groups at most follow-up periods. However, at 6 months, the MFAT group showed significantly greater improvements in 100-mm VAS (MD, 5.55; 95% CI, 1.2-9.9; I2 = 10%; Z = 2.5; P = .01) and KOOS-Pain (MD, 3.61; 95% CI, 0.31-6.91; I2 = 0%; Z = 2.15; P = .03) compared with the PRP group (Figure 3).
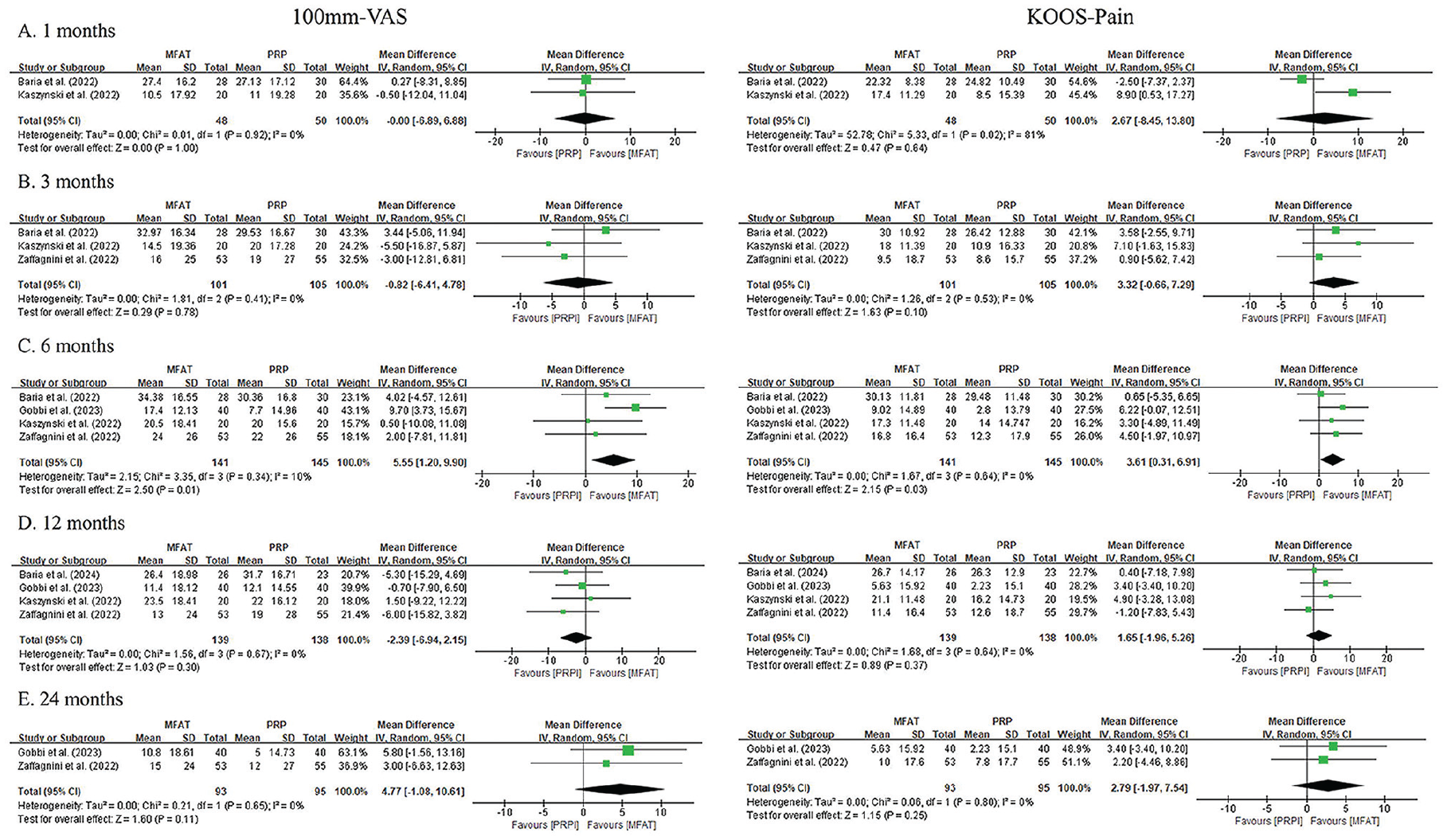
Forest plots of improvement in 100-mm VAS and KOOS-Pain at 1 (A), 3 (B), 6 (C), 12 (D), and 24 (E) months after intra-articular injection of MFAT versus PRP. Squares represent the mean difference in outcomes, with the size of the square being proportional to the sample size. IV, inverse variance; KOOS, Knee injury and Osteoarthritis Outcome Score; MFAT, microfragmented adipose tissue; PRP, platelet-rich plasma; VAS, visual analog scale.
Functional Improvement (KOOS and IKDC Subjective Score)
Significant functional improvements were observed only at specific follow-up periods: 6 and 12 months for KOOS-Symptom and 6 months for KOOS–Quality of Life (QoL) and IKDC subjective scores. The MFAT group had significantly greater improvements in KOOS-Symptom at 6 months (MD, 5.31; 95% CI, 1.72-8.89; I2 = 12%; Z = 2.9; P = .004) and 12 months (MD, 3.68; 95% CI, 0.33-7.02; I2 = 1%; Z = 2.9; P = .03) (Figure 4). Similarly, improvements in KOOS-QoL (MD, 4.74; 95% CI, 0.79-8.69; I2 = 0%; Z = 2.35; P = .02) and IKDC subjective scores (MD, 4.22; 95% CI, 0.4-8.03; I2 = 0%; Z = 2.16; P = .03) were significantly higher in the MFAT group at 6 months (Figures 5 and 6).
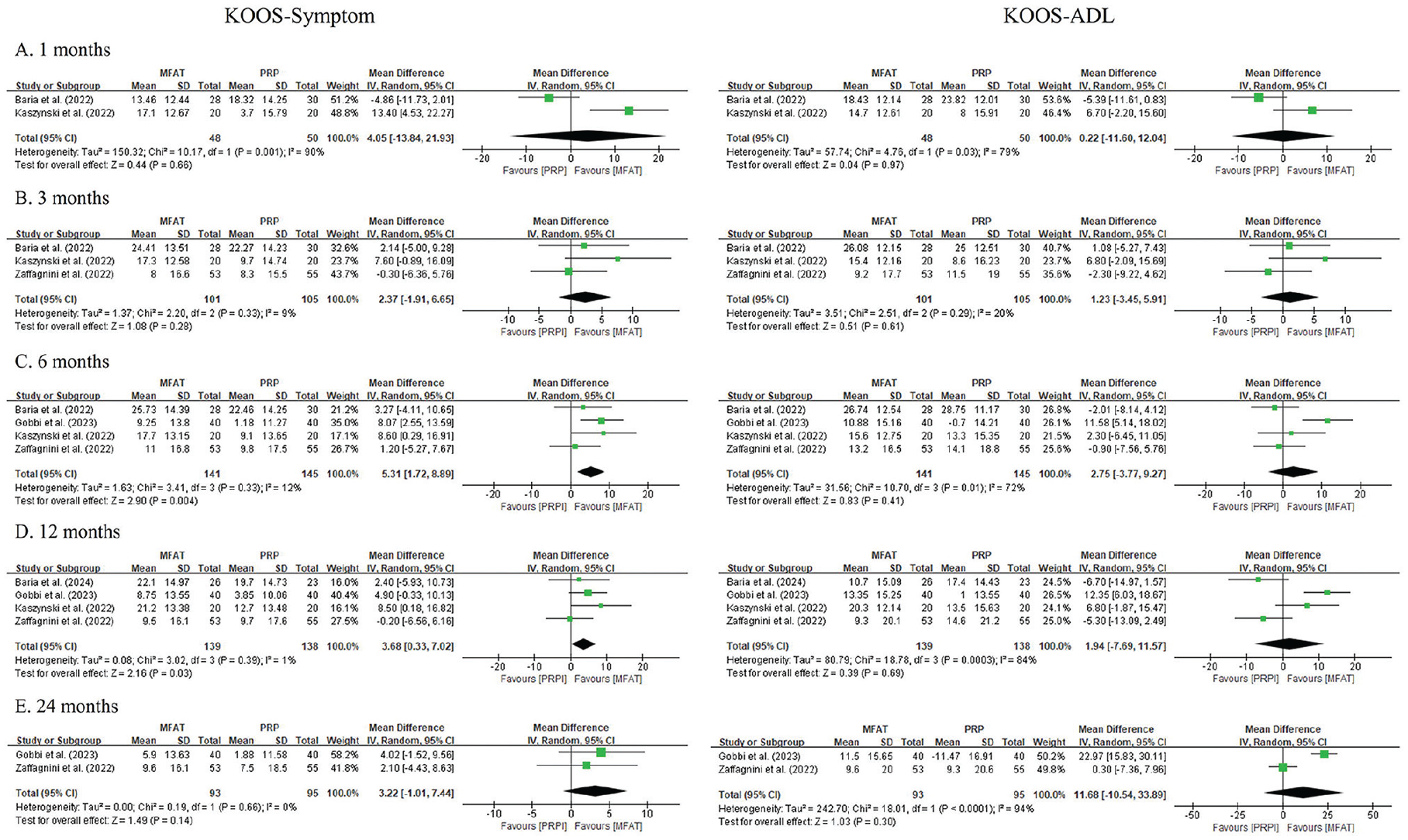
Forest plots of improvement in KOOS-Symptom and KOOS-ADL at 1 (A), 3 (B), 6 (C), 12 (D), and 24 (E) months after intra-articular injection of MFAT versus PRP. Squares represent the mean difference in outcomes, with the size of the square being proportional to the sample size. ADL, Activity of Daily Living; IV, inverse variance; KOOS, Knee injury and Osteoarthritis Outcome Score; MFAT, microfragmented adipose tissue; PRP, platelet-rich plasma.
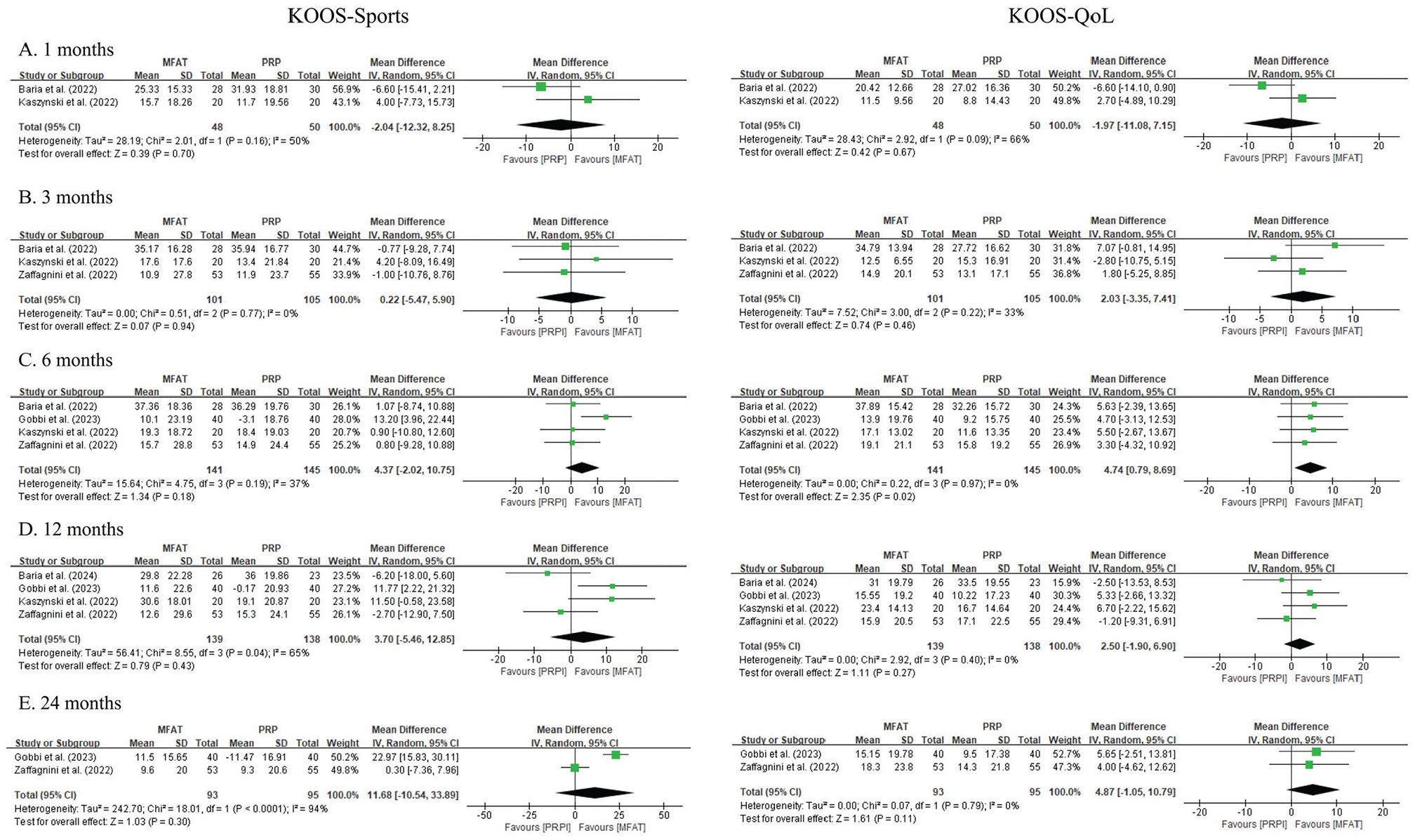
Forest plots of improvement in KOOS-Sports and KOOS-QoL at 1 (A), 3 (B), 6 (C), 12 (D), and 24 (E) months after intra-articular injection of MFAT versus PRP. Squares represent the mean difference in outcomes, with the size of the square being proportional to the sample size. IV, inverse variance; KOOS, Knee injury and Osteoarthritis Outcome Score; MFAT, microfragmented adipose tissue; PRP, platelet-rich plasma; QoL, Quality of Life.
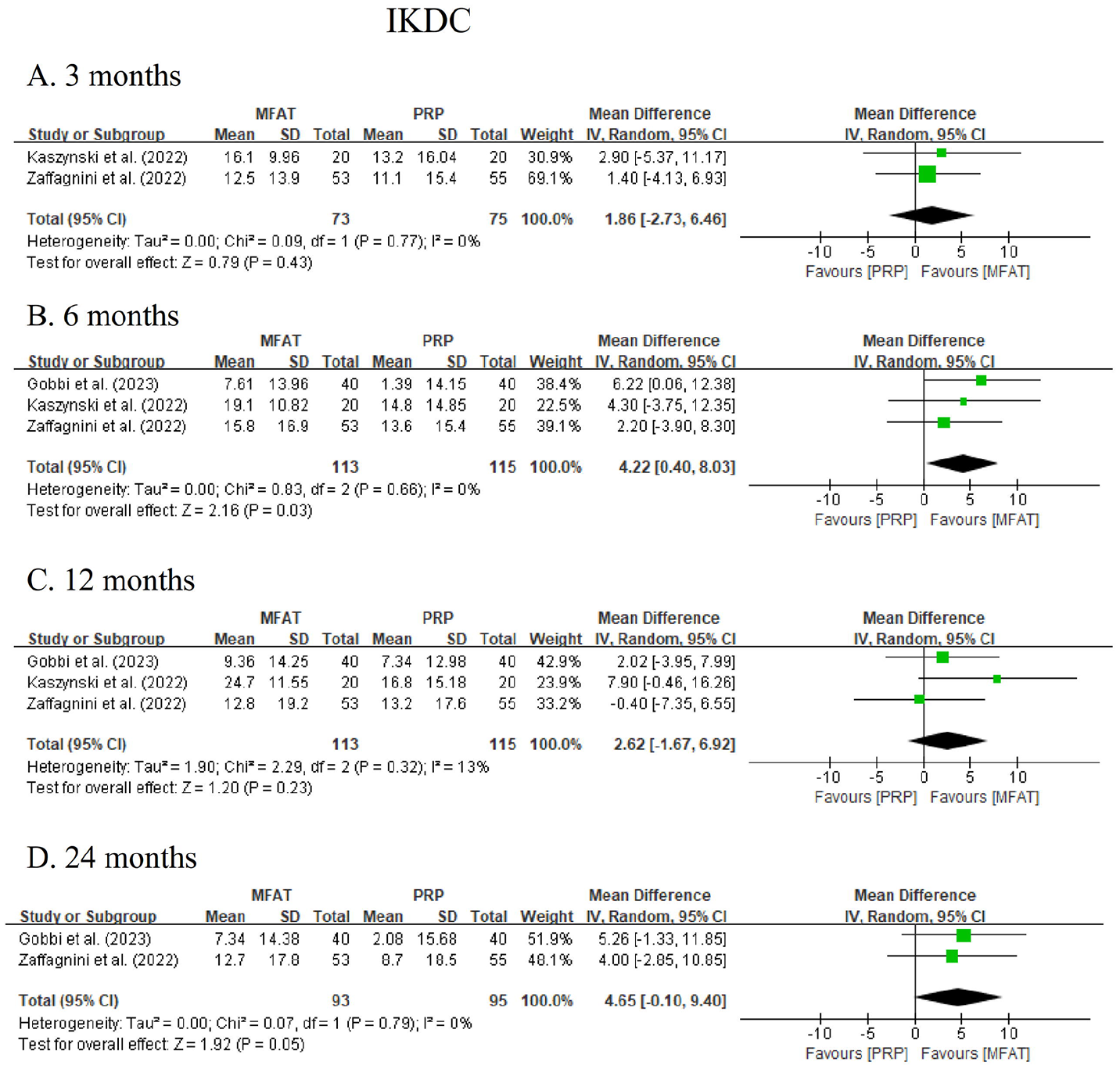
Forest plots of improvement in IKDC subjective scores at 3 (A), 6 (B), 12 (C), and 24 (D) months after intra-articular injection of MFAT versus PRP. Squares represent the mean difference in outcomes, with the size of the square being proportional to the sample size. IKDC, International Knee Documentation Committee; IV, inverse variance; MFAT, microfragmented adipose tissue; PRP, platelet-rich plasma.
Safety
Procedure-related AEs were reported in 3 studies.4,24,55 The pooled analysis showed no significant difference in AEs between the MFAT group (odds ratio, 10.3%; 95% CI, 0.6% to 21.2%) and the PRP group (odds ratio, 12.9%; 95% CI, –0.4% to 26.1%; P = .08). All AEs, which included pain and/or swelling at the injection site, resolved within a few days. No serious procedure-related AEs were reported.
Discussion
The principal findings of this meta-analysis demonstrate that MFAT and PRP offered clinically significant effectiveness and safety in treating knee OA, as measured by MCID achievement. Although both treatments showed similar improvements in pain and function, MFAT resulted in significantly better pain relief and functional enhancement than PRP at the 6-month follow-up.
Knee OA is increasingly recognized as a disorder of the knee joint environment, rather than merely a “wear and tear” disease. 35 The OA process begins with molecular and metabolic disturbances in joint tissues, leading to cartilage degradation and joint inflammation. 35 In this context, orthobiologics have emerged as potential disease-modifying treatments for knee OA.12,19 The platelets in PRP, as well as the MSCs and stromal vascular fractions (SVFs) in MFAT, are activated to release a variety of growth factors and cytokines. The bioactive substances released from PRP, MSCs, and SVFs have been extensively studied and are known to promote tissue healing and modulate inflammatory processes.1,23,26,46 This meta-analysis supports the clinical effectiveness of IA injections of MFAT and PRP in knee OA, with improvements in all outcome measures exceeding the MCID from 1 to 12 months after injection. If future studies provide further robust evidence, IA injections of MFAT and PRP could become alternatives to hyaluronic acid or corticosteroids, which are currently recommended for knee OA in established international guidelines.2,3,11 Furthermore, these orthobiologic treatments may represent an important initial step toward achieving the goal of disease-modifying therapies for knee OA.
The meta-analysis found that IA injections of MFAT and PRP resulted in comparable clinical improvements over a 2-year follow-up period, consistent with findings from RCTs that reported similar outcomes between the 2 treatments.4,5,18,24,31,49,53,55 However, a noteworthy finding from this meta-analysis revealed that MFAT provided significantly greater pain relief and functional improvement than PRP at 6 months after injection. This outcome may be due to the method of calculating mean clinical improvement by comparing mean postinjection scores to mean baseline scores and calculating their standard deviations based on the Cochrane guidelines. 27 Additionally, minor variations in the included RCTs may have contributed to these significant differences when data were pooled for analysis. Furthermore, adipose tissue contains approximately 25,000 times more reparative cells than peripheral blood, 43 which may explain the superior regenerative and immune-modulatory effects of MFAT compared with PRP, which lacks MSCs. 38 This is consistent with findings from Zaffagnini et al, 55 who reported better outcomes with MFAT in patients with moderate to severe OA, and from Boric et al, 9 who observed significant increases in glycosaminoglycan levels in articular cartilage after MFAT IA injection. 9
The growing interest in minimally manipulated approaches, driven by strict regulations, highlights additional advantages such as ease of collection, handling, and minimally invasive procedures. PRP has garnered significant support for the treatment of knee OA, with some experts considering it the first-line IA injection therapy among orthobiologics. MFAT, a 1-step treatment that minimally manipulates adipose tissue, preserves the structural properties and integrity of the tissue, maintains the adipose “niche,” and supports the microenvironment and function of MSCs. Despite the significant difference in clinical outcomes between the 2 groups at 6 months after injection, the difference was too small to reach MCID threshold for clinical significance. All RCTs except one 24 reported clinical outcomes exceeding the MCID for both MFAT and PRP.4,5,31,55 Additionally, both treatments were safe, with a low incidence of mild AEs and no significant difference in safety between the 2 groups. Given its clinical effectiveness and safety, PRP is simpler to administer, requires no additional training (eg, lipoaspiration), is less expensive, and is easier to repeat as needed.6,32,45 It has been reported that PRP has several advantages over MFAT including less invasiveness, resource requirement, and cost for procedure. 40 However, more evidence is required for MFAT due to the limited literature available, which hampers a robust comparison between MFAT and PRP. In this regard, PRP may be considered as an initial treatment option due to its advantages, whereas MFAT can be used for patients requiring rapid improvement or those who have shown an inadequate response to PRP therapy. In summary, both MFAT and PRP are effective, safe, and viable nonoperative treatments for knee OA.
Limitations
This study has several limitations. First, the number of studies and sample sizes were relatively small, as MFAT is a relatively new treatment modality. Second, the meta-analysis included heterogeneous patient populations, including variations in K-L grade, body mass index, and intervention protocols. It would be valuable to identify significant factors influencing clinical effectiveness in the future. However, this meta-analysis could not determine whether OA severity (K-L grade) or leukocyte presence in PRP (LR-PRP or LP-PRP) affected outcomes due to the limited number of included studies. Meanwhile, recent studies have suggested that leukocyte concentration in PRP may not affect clinical efficacy, and PRP or MFAT injections may be more effective in patients with milder OA.21,29,34,55 Third, the short-term follow-up of the included studies does not guarantee the long-term safety of orthobiologics such as PRP or MFAT. Therefore, high-quality studies with longer follow-up periods are necessary to establish the long-term efficacy and safety of these treatments. Despite these limitations, meta-analytic approaches have proven valuable in addressing the limitations of individual study sizes, encompassing diverse populations, and providing insights that surpass those of any single study. 25 This review underscores the scientific community’s growing interest in nonoperative therapeutic approaches, which may contribute to a new paradigm in the treatment of knee OA.
Conclusion
IA injections of PRP and MFAT both provided significant clinical benefits and were safe for treating knee OA over a 12-month period. Although no substantial differences were observed between the 2 treatments in most follow-up periods, MFAT showed slightly better pain relief and functional improvement at 6 months. However, further research is needed to confirm these findings and guide clinical practice.
Supplemental Material
sj-tif-1-ajs-10.1177_03635465251337759 – Supplemental material for Microfragmented Adipose Tissue as an Alternative to Platelet-Rich Plasma for Intra-articular Injection in Knee Osteoarthritis: A Systematic Review and Meta-analysis of Randomized Controlled Trials
Supplemental material, sj-tif-1-ajs-10.1177_03635465251337759 for Microfragmented Adipose Tissue as an Alternative to Platelet-Rich Plasma for Intra-articular Injection in Knee Osteoarthritis: A Systematic Review and Meta-analysis of Randomized Controlled Trials by Yong-Beom Park, Seul Ki Lee, Kang-Il Kim, Je-Hyun Yoo, Taehoon Jung and Jun-Ho Kim in The American Journal of Sports Medicine
Footnotes
Submitted August 23, 2024; accepted February 21, 2025.
The authors have declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
An online CME course associated with this article is available for 1 AMA PRA Category 1 Credit™ at https://education.sportsmed.org/Public/Catalog/Home.aspx?CourseSearch=1&Criteria=9&Option=25. In accordance with the standards of the Accreditation Council for Continuing Medical Education (ACCME), it is the policy of The American Orthopaedic Society for Sports Medicine that authors, editors, and planners disclose to the learners all financial relationships during the past 12 months with any commercial interest (A ‘commercial interest’ is any entity producing, marketing, re-selling, or distributing health care goods or services consumed by, or used on, patients). Any and all disclosures are provided in the online journal CME area which is provided to all participants before they actually take the CME activity. In accordance with AOSSM policy, authors, editors, and planners’ participation in this educational activity will be predicated upon timely submission and review of AOSSM disclosure. Noncompliance will result in an author/editor or planner to be stricken from participating in this CME activity.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.