
Abstract
Background:
The outcomes of surgical repair for traumatic avulsions of the pyramidalis, anterior pubic ligament, adductor longus complex (PLAC) remain unknown.
Purpose:
To report how surgical repair for PLAC injuries in professional athletes affected return to preinjury level of sporting activity, injury recurrence, patient satisfaction, functional performance, and complications.
Study Design:
Case series; Level of evidence, 4.
Methods:
This retrospective, single-surgeon study included 62 professional athletes. Inclusion criteria for study participation were professional athletes, primary injury within 28 days of surgical intervention, magnetic resonance imaging scan confirming complete avulsion of the proximal adductor longus tendon fibrocartilaginous entheses, patient symptomatic with groin pain and adductor weakness, and surgical intervention undertaken by the senior author. Exclusion criteria were chronic and recurrent adductor injuries; concomitant chronic conditions including osteoarthritis, inguinal hernia, and chronic groin pain; and patient living abroad or not available for follow-up. All study participants underwent surgical repair with suture anchor fixation. A standard rehabilitation protocol was followed postoperatively. The Lower Extremity Functional Scale (LEFS), Marx Activity Rating Scale (MARS), patient satisfaction levels, and time to return to previous level of sport were the primary outcome measures used in this study.
Results:
The mean follow-up time was 4.2 years (range, 2.1-8.1 years) from the date of surgery. The study included 62 professional athletes (52 male, 10 female) with a mean age of 27.2 years (range, 18-36 years) with acute traumatic avulsions of the proximal adductor longus tendon involving the PLAC: type I, 28 patients (45.2%); type II, 24 patients (38.7%); type III, 2 patients (3.3%); type IV, 2 patients (3.3%); type V, 6 patients (9.7%); and type VI, 0 patients (0%). All 62 patients (100%) returned to their preinjury level of sporting activity. The specific level of each sport at which the individuals were performing was not recorded; however, all participants were professional athletes who returned to professional play. The mean time from surgical intervention to return to full sporting activity was 12.3 ± 2.2 weeks (range, 9-18 weeks) with no injury recurrence at 2 years after surgery. Overall, 46 patients (74.2%) were highly satisfied and 16 patients (25.8%) were satisfied with the outcomes of their surgery. Improvements were observed in the mean LEFS (from 49.7 ± 5.2 points preoperatively to 80.2 ± 4.2 points at 2-year follow-up; P < .001). In addition, 48 patients (77.4%) had a LEFS of 75 points, and 12 patients (19.4%) achieved the maximum LEFS score of 80 points at 2-year follow-up. Improvements were also seen in MARS scores (from 3.1 ± 1.2 points preoperatively to 12.8 ± 1.8 points at 2-year follow-up; P < .001). In total, 46 patients (74.2%) achieved a MARS score of 12 points, and 14 patients (22.6%) achieved the maximum MARS score of 16 points at 2-year follow-up. Four patients had postoperative wound complications, and 1 patient had postoperative neuroma-related pain.
Conclusion:
Surgical repair of acute traumatic avulsions of the adductor longus fibrocartilaginous entheses involving the PLAC was associated with early return to preoperative level of sporting function in professional athletes, with no risk of injury recurrence, high levels of patient satisfaction, improvements in functional outcomes, and low risk of postoperative complications at short-term follow-up.
Keywords
Adductor muscle injuries are prevalent in sports, representing 64% of hip and groin region injuries in male professional and recreational athletes.12,18,25 Among the adductor muscle group, the adductor longus muscle is predominantly implicated, accounting for approximately 90% of the injuries.19,21 Although sprains are the dominant type of adductor longus injuries, a prevalence of complete proximal ruptures and avulsions is emerging. 4 Such injuries are associated with prolonged rehabilitation, delayed return to sporting activity, and suboptimal functional outcomes. 18 Furthermore, adductor longus injuries can contribute to the development of chronic groin pain syndrome, a complex condition characterized by persistent pain and tenderness in the pubic and inguinal regions, which may significantly impair function in professional and recreational athletes.6,15 Although this syndrome can ensue from various origins such as pubic osteitis, prostatitis, and inguinal hernias, studies have shown that isolated overuse injuries to the adductor longus muscle or tendon remain the prevailing etiological factor.1,2,13
The most common mechanism of acute adductor longus injury involves an eccentric overload during contraction of the adductor muscles.4,22 Other culpable movements include a combination of extension and external rotation of the hip joint. 20 Consequently, proximal avulsion injuries of the adductor longus tendon are seen more commonly in sports such as football, basketball, and skiing, which involve rapid pivoting, cutting, and twisting.20,21 More recently, magnetic resonance imaging (MRI) studies have shown that proximal avulsion injuries of the fibrocartilage entheses often represent a wider zone of injury within the pyramidalis, anterior pubic ligament, and adductor longus complex (PLAC).16,17 It is possible to stratify the grade of injury to the PLAC by assessing the degree of trauma to these 3 key structures and the surrounding musculature on MRI. 17 Although this classification system provides an important anatomic grading to the PLAC injury, its clinical significance to guiding treatment or long-term prognosis remains undetermined.
Nonoperative treatment of proximal adductor longus avulsion injuries is associated with highly variable times for return to preinjury level of sporting activity, residual groin pain, and risk of retears with return to running or kicking activities. 18 More recently, studies have reported on the surgical repair of acute proximal adductor longus avulsion injuries and reported high levels of return to sporting activity with low risk of complications at short-term follow-up.3,4,9,10,14,18,23,24 However, these trials combined acute and chronic proximal avulsion injuries. Injuries to the surrounding anatomic structures, including the PLAC complex, were not reported, and/or patients did not receive standardized postoperative rehabilitation protocols for return to sporting activity. A paucity of evidence is available regarding the outcomes of surgical repair of acute adductor longus avulsion injuries involving the PLAC complex in relation to return to preinjury level of sporting activity, functional outcomes, and risk of injury recurrence.
The purpose of this study was to report the outcomes of surgical repair of the PLAC complex regarding return to preinjury level of sporting activity, injury recurrence, patient satisfaction, functional performance, and complications in professional athletes. The specific activity level of each sport at which the individuals were performing was not recorded; however, it was hypothesized that surgical repair of acute traumatic avulsions of the PLAC would allow an early return to preoperative level of sporting function among these professional athletes.
Methods
Patient Selection
This retrospective case series study included 62 professional athletes undergoing surgical repair for acute proximal avulsion injuries of the PLAC. All operative procedures were performed by a single surgeon (F.S.H.) between November 2015 and November 2021. Study patients underwent MRI to confirm a proximal avulsion injury of the PLAC and to establish any concurrent surrounding injuries (Figure 1). In 2017, Schilders et al 16 published a classification system for grading proximal adductor avulsion injuries as part of a wider injury pattern involving the PLAC. All MRI scans were reviewed to establish the grade of PLAC injury using this classification system. All MRI scans were reviewed by the senior author (F.S.H.).
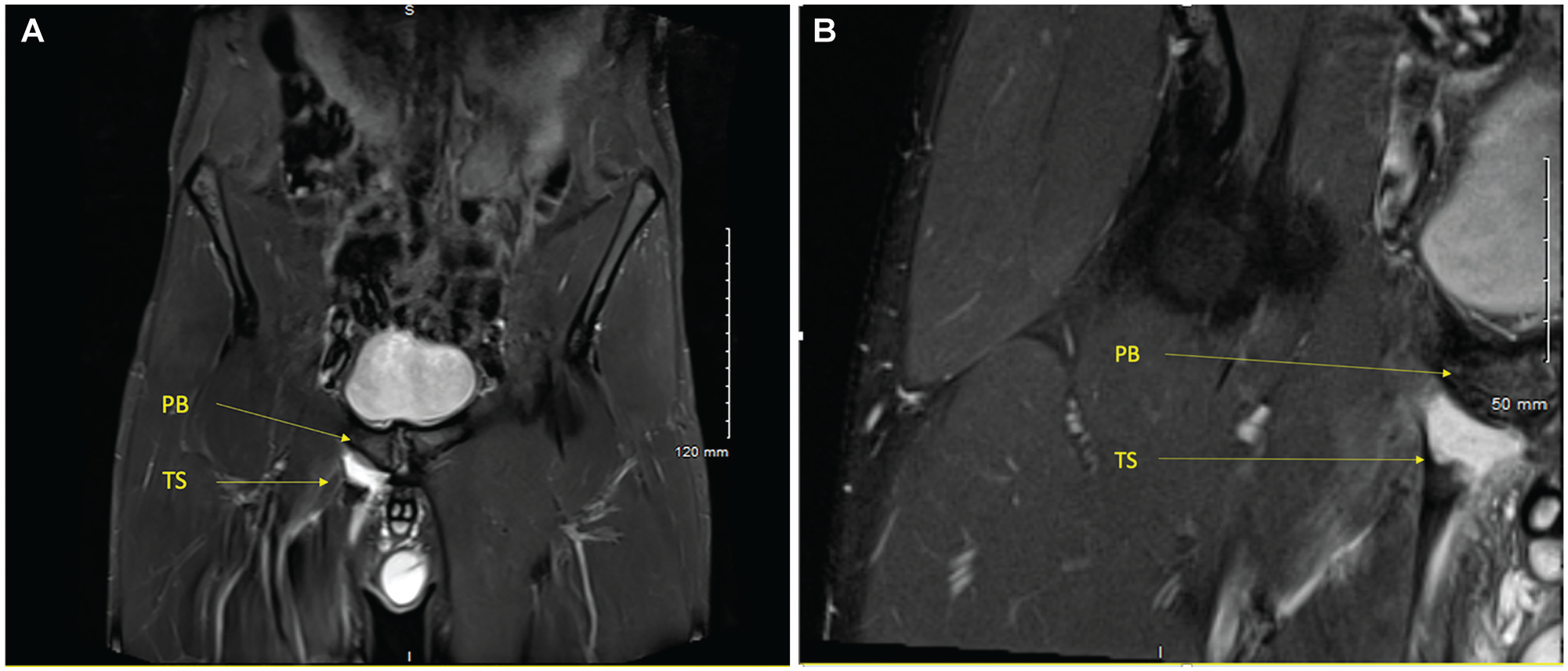
Coronal magnetic resonance imaging sequences (T2-weighted, short-TI inversion recovery [STIR], 5 mm slice thickness plane). (A) Adductor longus avulsion injury of a 25-year-old soccer player with a stump retraction of 2.1 cm. (B) Closer view of total avulsion of right proximal adductor longus tendon; at the site of lesion, a fluid collection attributed to a sero-hematoma is observed. PB, pubic bone; TS, tendon stump.
Inclusion criteria for study participation were as follows: professional athletes, primary injury within 28 days of surgical intervention, MRI scan confirming complete avulsion of the proximal adductor longus tendon fibrocartilaginous entheses, patient symptomatic with groin pain and adductor weakness, and surgical intervention undertaken by the senior author. Exclusion criteria were chronic and recurrent adductor injuries; concomitant chronic conditions, including osteoarthritis, inguinal hernia, and chronic groin pain; and patient living abroad or unavailable for follow-up. The study was reviewed by the hospital review board, which advised that further approval was not required. Written informed consent for participation was obtained from all study patients.
Surgical Technique
All procedures were performed by a single surgeon (F.S.H.), with the patient in supine position under general anesthesia. A preoperative dose of intravenous antibiotics was administered on induction. The affected limb was abducted and positioned into the figure-of-4 position (Figure 2A). After careful skin preparation and draping, the anterior superior iliac spine and pubic tubercle were marked. A parainguinal incision measuring 3 to 4 cm was made just distal to the inguinal crease (Figure 2B). Manual palpation was used to identify the retracted adductor longus tendon, followed by blunt subcutaneous dissection and hematoma evacuation. The distal stump of the adductor longus tendon was identified, mobilized, and secured with a nonabsorbable polyester suture (No. 5 Ethibond Excel) (Figure 2C). Fluoroscopy was not used in this procedure.
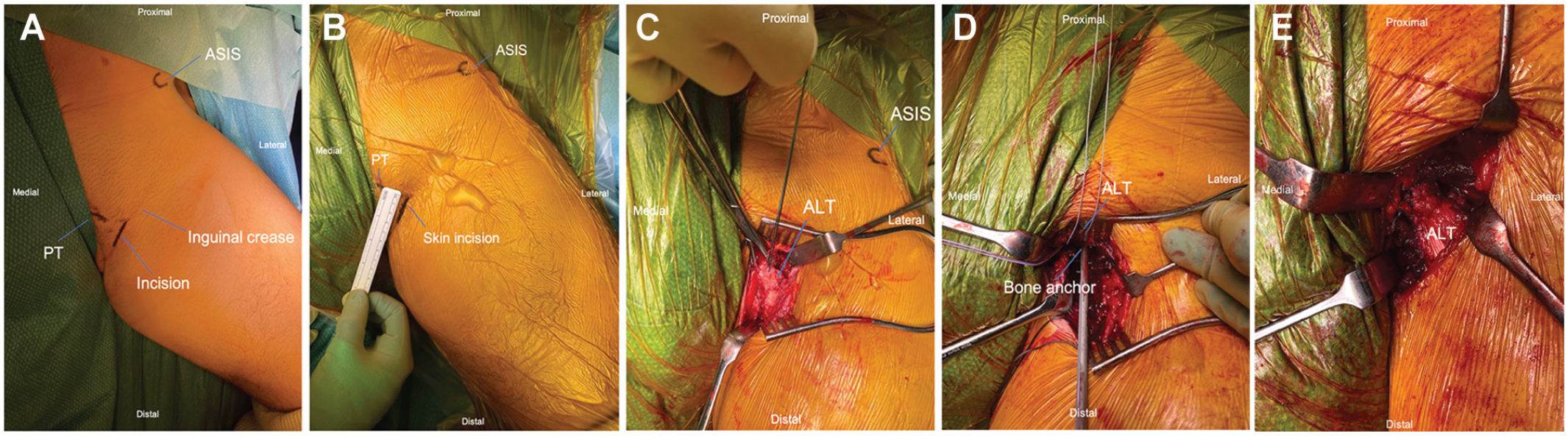
Intraoperative photographs. (A) Patient position on operating table in neutral rotation. (B) Landmark marking for surgical incision over injured area. (C) Adductor longus tendon (ALT) looped with a nonabsorbable polyester suture and tensioned. (D) Suture insertion in the symphysial surface with bone anchor docked into pubic bone. (E) ALT sutured to the anchors and reattached to the pubic bone, further reinforced with stay sutures to the periosteum. ASIS, anterior superior iliac spine; PT, pubic tubercle.
The footprint of the adductor on the pubis was prepared for reattachment, and two to three 5.5-mm suture anchors were inserted in the symphysial surface (Figure 2D). A tension-free reattachment of tendon to bone was undertaken using a modified Mason-Allen stitch, with the tendon parachuted down to bone with the free end of the bone anchor suture. The repair was further reinforced with periosteal sutures (No. 5 Ethibond) (Figure 2E). The spermatic cord and femoral bundle, which lie proximally and laterally, respectively, were protected throughout the procedure. Copious wound irrigation with normal saline was then performed, and absorbable sutures were used to perform a layered closure of the overlying fascia, subcutaneous fat, and skin. The surgical technique did not change over the course of the study (between November 2015 and November 2021).
Postoperative Rehabilitation
All patients were discharged home on the day of surgery with a standardized milestone-based rehabilitation program. All patients were advised to mobilize partial weightbearing (50% weightbearing) with crutches for 4 weeks after surgery. No brace was used. This was supervised by an experienced sports physical therapist and divided into 4 distinct phases 8 :
Phase I (postoperative phase, 0-3 weeks): avoid infection; maintain body mass at preinjury level; perform deadlift, hip thrust, and single-joint exercises 3 times per week; perform concentric and isometric abdominal and hip strengthening exercises 5 times per week.
Phase II (introductory loading, 3-6 weeks): pain-free range of motion at baseline levels in all planes; adductor squeeze test pain-free and at 80% of unaffected side; flexion, abduction, and external rotation (FABER) test at 90% symmetry without any apprehension; adductor strength at 80% symmetry of unaffected leg with hand-held dynamometry testing; side-lying adductor raise performed and sustained for 5 seconds; and unbreakable manual muscle abduction testing in side-lying at middle and inner range.
Phase III (advanced loading, 6-10 weeks): pain-free range of motion at baseline levels in all planes; adductor squeeze test pain-free and same as unaffected side; symmetrical adductor strength with hand-held dynamometry testing; symmetrical, pain-free FABER test without any apprehension; symmetrical adductor strength with hand-held dynamometer; and technical competence in linear skipping and lateral force projection drills.
Phase IV (return-to-play reconditioning, 11-14 weeks): match external load demands of a training week; sprint at 95% of personal maximum velocity on 2 occasions; complete games-specific tasks confidently and competently; and match positional training loads standards in training for 2 consecutive weeks.
Outcome Measures
All patients were reviewed in the outpatient clinic or virtually by the operating surgeon at regular intervals until complete resumption of return to professional play. All study outcomes were collected by a specialist nurse at most recent follow-up via face-to-face consultations, telephone calls, or email correspondence due to the wide geographical distribution of the athletes. Return to preinjury sporting activity function and patient satisfaction were recorded.
Return to Preinjury Sporting Activity Function
The ability to return to full preinjury level of sporting activity was recorded. Return to sport means returning to preinjury level of sport but not necessarily at preinjury level of performance. All patients were professional athletes who were cleared to return to professional competitive sport. This was confirmed with the team doctors or physical therapists in all cases. If appropriate, the time interval from surgical intervention to return to full preinjury level of sporting activity was recorded.
Patient Satisfaction
Patient satisfaction was recorded via the Musculoskeletal Outcomes Data Evaluation and Management System, which scores patient satisfaction on a scale of 1 to 5 (1, very unsatisfied; 2, unsatisfied; 3, neutral; 4, satisfied; 5, very satisfied). 7
Functional Performance and Complications
All study patients completed the Lower Extremity Functional Scale (LEFS) and Marx Activity Rating Scale (MARS) preoperatively and at the most recent follow-up.5,11 The LEFS is a validated and effective questionnaire for assessing specific lower limb function. It is an 80-point scale with 20 questions (4 points per question) and a minimum clinical difference of 9 points. 5 The MARS measures patient activity level and knee function independent of age, sex, and type of sporting activity. Scores of 0 to 4 are assigned to 4 activities: running, changing direction, decelerating, and pivoting, with a total score of 16 points. 11
Complications
All complications with their respective treatments and outcomes during the follow-up period were recorded.
Statistical Analysis
Paired t tests were used to compare study outcomes found to be normally distributed, whereas the Mann-Whitney U test was used for continuous outcomes found not to be normally distributed. Categorical outcomes were compared with the Fisher exact test. Statistical significance was set at P < .05 for all analyses, and all statistical analysis was performed with SPSS software (Version 24; IBM Corp).
Results
Return to Function and Recurrence of Injury
All 62 study patients (100%) returned to their professional level of sporting activity. Baseline characteristics, demographic data, and grade of PLAC injury for the study population are presented in Tables 1 and 2. Mean time from surgical intervention to return to full professional sporting activity was 12.3 ± 2.2 weeks (range, 9-18 weeks). At the most recent follow-up, all 62 study patients (100%) were still participating at their preinjury professional level of sporting activity with no injury recurrence. Mean follow-up time was 4.2 years (range, 2.1-8.1 years) from date of surgery. No study patients were lost to follow-up during the study period.
Patient Characteristics and Baseline Data (N = 62) a
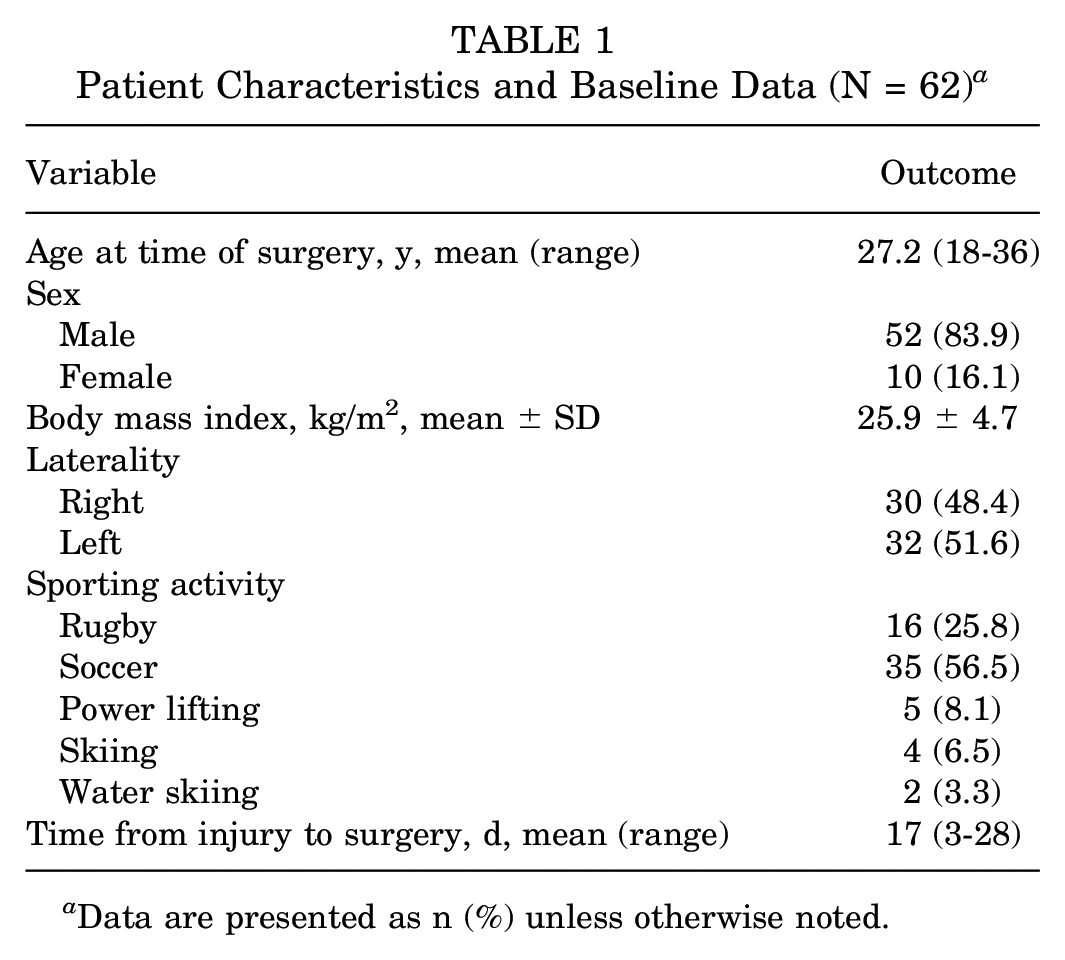
Data are presented as n (%) unless otherwise noted.
Pyramidalis–Anterior Pubic Ligament–Adductor Longus Complex (PLAC) Classification of Study Patients (N = 62) a
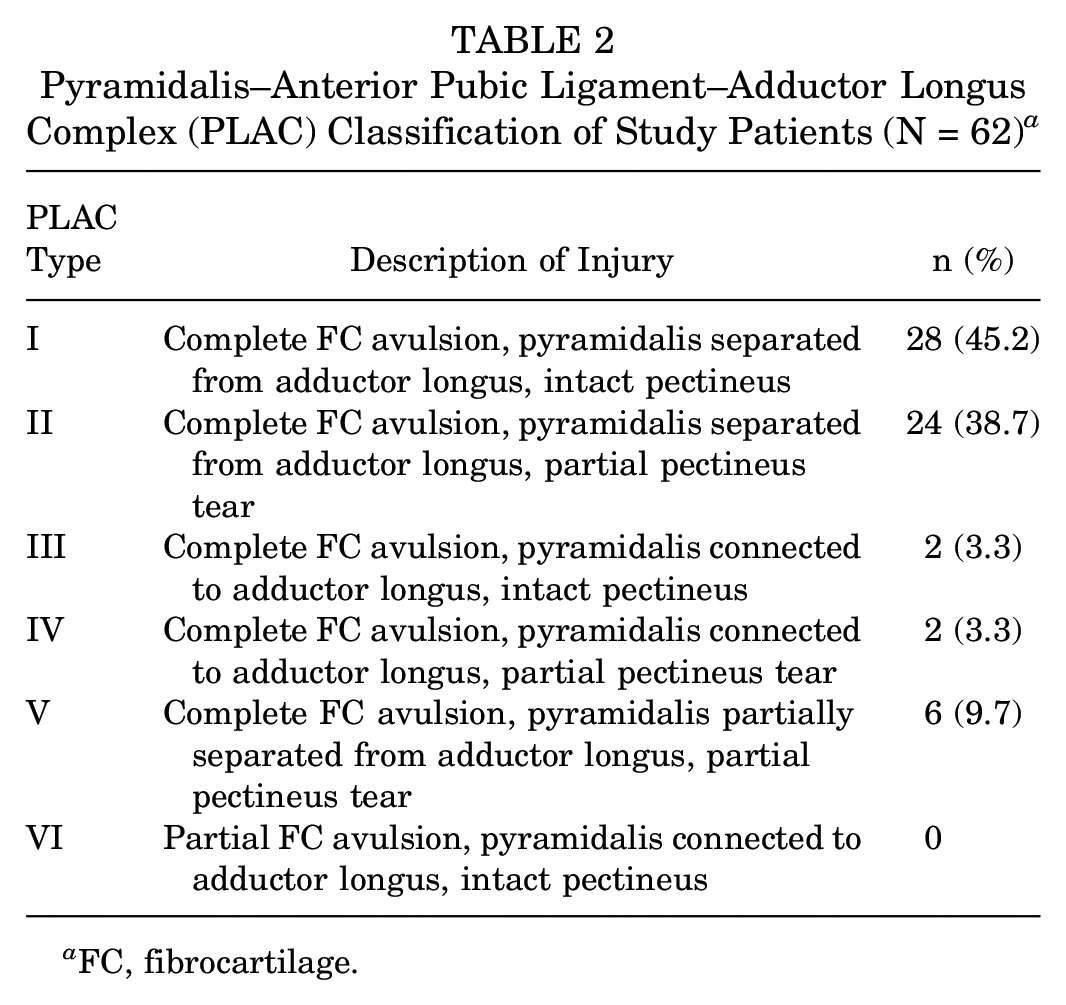
FC, fibrocartilage.
Patient Satisfaction
Surgical repair of acute proximal adductor longus avulsion injuries involving the PLAC was associated with 46 patients (74.2%) being highly satisfied and 16 patients (25.8%) being satisfied with the outcomes of their surgery at 2-year follow-up. No study patients were neutral, unsatisfied, or highly unsatisfied with the outcome of their surgery.
Functional Performance
The mean LEFS score improved from 49.7 ± 5.2 points preoperatively, to 80.2 ± 4.2 points at 2-year follow-up (P < .001). In addition, 48 patients (77.4%) had a LEFS of 75 points and 12 patients (19.4%) achieved the maximum LEFS score of 80 points at 2-year follow-up. The mean MARS scores improved from 3.1 ± 1.2 points preoperatively, to 12.8 ± 1.8 points at 2-year follow-up (P < .001). A total of 46 patients (74.2%) achieved a MARS score of 12 points, and 14 patients (22.6%) achieved the maximum MARS score of 16 points at 2-year follow-up.
Complications
Five patients had postoperative complications during the follow-up period. This included 1 patient with wound breakdown that required a return to surgery for washout and primary closure. Three patients developed postoperative wound infections. Two of these 3 patients were treated successfully with oral antibiotics. The third patient underwent surgical washout of a superficial wound collection and primary wound closure, with retainment of the suture anchors. These patients had no further complications. One additional patient had neuroma-related pain around the operative site. This resolved with physical therapy and an ultrasound-guided corticosteroid injection. This was not associated with any functional deficit, and the patient returned to preinjury level of professional sporting play at 18 weeks after the date of surgery. No further complications were observed at 2-year follow-up.
Discussion
Surgical repair of acute traumatic avulsions of the PLAC enabled professional athletes to return to their preoperative level of sporting function with no episodes of injury recurrence at short-term follow-up. Operative intervention was associated with high levels of patient satisfaction, improved functional outcome scores compared with preoperative values, and low risk of postoperative complications at 2-year follow-up.
All athletes were able to return to their preinjury level of professional sporting play at 12.3 ± 2.2 weeks (range, 9-18 weeks) after surgery. These findings are consistent with previous studies on surgical repair of isolated adductor longus avulsion injuries reporting return to sporting activity at 8 to 16 weeks after surgery.14,18,24 Rizio et al 14 reviewed outcomes in 2 professional football players undergoing surgical repair of proximal adductor longus avulsion injuries and found that both players returned to full sporting activity by the third postoperative month.
Tansey et al 23 prospectively reviewed outcomes in 15 professional athletes undergoing surgical reattachment of proximal adductor avulsion injuries, with 7 of these patients receiving additional mesh reinforcement of the posterior inguinal wall. These injuries were not classified as PLAC injuries but were type IV injuries involving the rectus abdominis and therefore the inguinal canal. The authors reported that the mean time for return to sporting activity was 13 weeks (range, 10-21 weeks). Similar to the current study, Tansey et al found no risk of recurrence at short-term follow-up. In the current study, we found only 2 cases of type IV PLAC injuries, and neither case had inguinal canal disruption that would have required mesh repair.
The MRI findings of the current study support those from recent studies showing that proximal adductor longus injuries commonly represent a wider injury pattern to the PLAC.16,17 The majority of patients had PLAC type I and II injuries where the pyramidalis muscle was separated from the adductor longus tendon with an intact or partial tear of the pectineus muscle respectively. The pyramidalis is a small triangular muscle, located anterior to the rectus abdominis in the midline. The inferior origin of the muscle is the pubic crest and anterior pubic ligament, and superiorly it inserts into the linea alba (Figure 3). The proximal adductor longus tendon attaches to the anterior pubic ligament and its fibrocartilage is anchored to the anterior pubic body, inferior to the pubic crest. In addition, the pectineus muscle originates from the lacunar ligament and linea ileopectinea and blends together with the adductor muscle at their superior margin. This complex anatomic arrangement explains the potential for proximal adductor longus avulsion injuries to involve more complex trauma to the entire PLAC and the adjacent pectineus muscle. 17
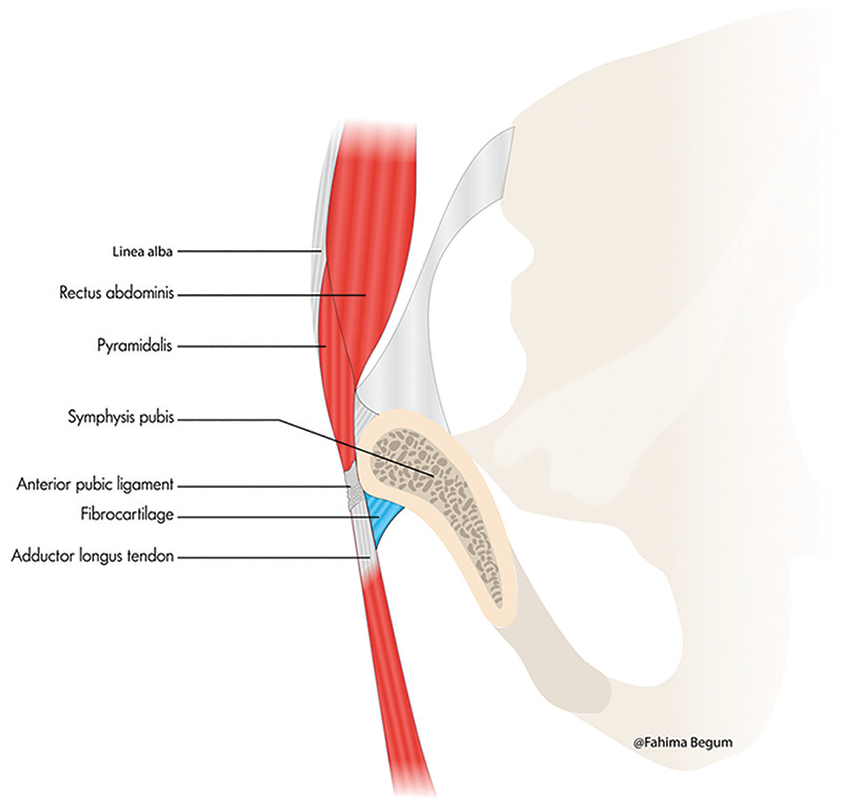
Diagram illustrating the anatomy of the pyramidalis, anterior pubic ligament, and adductor longus complex (PLAC) and the relationship between the pyramidalis, the anterior pubic ligament, and the adductor longus tendon.
This study found that surgical repair of these injuries was associated with high levels of patient satisfaction among professional athletes at short-term follow-up. This may be attributable to acute surgical repair of the adductor longus tendon for early restoration of the muscle to its natural working length. Lempainen et al 9 retrospectively reviewed outcomes in 40 male patients who had undergone surgical repair of complete proximal adductor longus tears at mean 11 months of follow-up. Of the 40 patients, 23 (57.5%) reported excellent outcomes, 13 (32.5%) reported good outcomes, and 4 (10%) deemed their outcomes as moderate. Athletes reporting excellent outcomes had undergone surgery sooner after the injury compared with athletes reporting good or moderate outcomes (2.4 ± 1.8 vs 11.4 ± 11.0 weeks, respectively; P < .01). Delays in surgical attachment of the avulsed adductor tendon may lead to muscle atrophy and fibrosis of scar tissue to adjacent anatomic structures.4,18 Failed nonoperative treatment may lead to chronic pain and decreased function, which may be career-threatening complications in elite athletes. 18
In the current study, surgical repair of PLAC injuries was associated with improvements in functional outcome scores at short-term follow-up. Bharam et al 4 conducted a prospective case series on 6 professional athletes undergoing suture anchor fixation of proximal adductor avulsion injuries with minimum 2-year follow-up. Those authors reported improvements in the mean Hip Outcome Score Activities of Daily Living subscale (postoperative vs preoperative: 99.0 vs 43.2, respectively; P < .001), Hip Outcome Score Sport-Specific subscale (98.9 vs 8.3, respectively; P < .001), and modified Harris Hip Score (97.1 vs 44.6, respectively; P < .001). Best et al 3 reviewed outcomes in 14 patients with adductor longus avulsion injuries undergoing nonoperative treatment for stump retraction <2 cm and suture anchor repair for stump retraction >2 cm. Their study revealed that 6 of the 7 patients in the surgical group rated their postinjury sporting level as 100% at 21.7 ± 12.3 months of follow-up, whereas only 4 of the 7 patients in the nonsurgical group achieved this at 15.1 ± 6.0 months of follow-up.
The current study has some important limitations that must be acknowledged when interpreting the findings. It was not possible to include a control group undergoing nonoperative treatment because all patients were professional athletes with complete avulsions who preferred surgical intervention to facilitate return to preinjury level of sporting function with minimal risk of injury recurrence or functional compromise. Repeat imaging with MRI was not used to assess healing at the operative site; therefore, asymptomatic recurrent injuries may not have been detected. All study participants were professional athletes, and so the generalizability of these findings to the nonathletic population remains unknown. Because all study participants were professional athletes, this study measured the effect of surgical management on whether the athletes returned to their respective professional sports and how long this time took, and specific activity levels were not measured. Additionally, all surgeries in this study were performed by the primary surgeon; thus, the repeatability of the findings with this technique remains to be explored. Despite these limitations, this is the largest case series on the surgical treatment of these complex injuries and provides important prognostic information on return to preinjury levels of sporting activity, patient satisfaction, functional progress, and risk of complications at short-term follow-up. The findings will facilitate more informed discussion between medical professionals and patients in relation to postoperative rehabilitation and planning for return to sporting activity.
Conclusion
Surgical repair of acute traumatic avulsions of the PLAC enabled return to preoperative level of sporting function with no episodes of injury recurrence at short-term follow-up. Operative intervention was associated with high levels of patient satisfaction, improved functional outcome scores compared with preoperative values, and low risk of complications at 2-year follow-up.
Footnotes
Submitted February 6, 2024; accepted March 31, 2025.
The authors have declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.