
Abstract
Background:
Synovial fluid (SF) biomarkers demonstrate time-dependent variation after acute knee injury, and it is postulated that persistently elevated inflammatory markers may mediate worse long-term outcomes.
Purpose:
This study investigated the relationship between biomarkers in SF at the time of meniscectomy and long-term patient-reported outcomes in patients with acute versus chronic meniscal injuries.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
This retrospective analysis included patients who underwent knee SF aspiration on the day of arthroscopic meniscectomy between October 2011 and October 2020 with minimum 4-year follow-up. SF aspirated from the operative knee was analyzed for 10 pro- and anti-inflammatory biomarkers. Patients completed the visual analog scale for pain, Lysholm Knee Questionnaire, Tegner Activity Scale, and Knee injury and Osteoarthritis Outcome Score–Physical Function Short-form (KOOS-PS) before surgery and at follow-up. Patients were categorized as having acute (<6 weeks) or chronic (>1 year) symptoms. K-means clustering analysis was performed using biomarker levels to group patients into distinct cohorts.
Results:
Of 85 patients meeting inclusion criteria, 55 had chronic and 30 had acute meniscal pathology, with 62 (72.9%) completing patient-reported outcome surveys at a mean follow-up of 8.66 years (SD, 2.27). K-means clustering identified 2 distinct biomarker profiles: a high-inflammation cluster and a low-inflammation cluster. The high-inflammation cluster had higher levels of 7 proinflammatory biomarkers as compared with the low-inflammation cluster (P = .015). The low-inflammation cluster predominantly comprised chronic meniscal injuries (89.2%), whereas the high-inflammation cluster was divided between acute and chronic cases. There were no differences in postoperative outcomes between clusters in the overall cohort. However, within the chronic cohort, the high-inflammation cluster exhibited worse postoperative scores on the visual analog scale for pain (P = .035), Lysholm questionnaire (P = .007), KOOS-PS (P = .038), and Tegner scale (P = .049) and had a higher rate of postoperative injections (P = .020) than the low-inflammation cohort.
Conclusion:
In patients with chronic meniscal injury, those with a more proinflammatory SF biomarker profile at the time of meniscectomy had worse outcomes than those who had a low inflammatory profile. In acute meniscal injuries, most patients demonstrate a high inflammatory profile, which was not associated with a difference in long-term outcomes.
Arthroscopic knee interventions for meniscal knee injuries are highly effective in alleviating patient symptoms and restoring knee function.9,10 However, despite restoration of joint biomechanics and initial resolution of pain, a subset of patients with meniscal injury will experience deterioration of outcomes in the long term, potentially attributed to the development of posttraumatic osteoarthritis (PTOA). 22 This degenerative process is mediated by pathologic changes initiated at the time of injury, with variability in clinical progression influenced by factors such as age, sex, activity level, body mass index (BMI), and reinjury. 22
Recent research has highlighted the role of synovial fluid (SF) biomarkers in reflecting physiologic and pathologic changes within the joint.18,24 Elevated concentrations of several proinflammatory markers, including matrix metalloproteinase 3 (MMP-3), interleukin 6 (IL-6), monocyte chemoattractant protein 1 (MCP-1), and macrophage inflammatory protein 1β (MIP-1β), have been observed in patients after acute meniscal injury when compared with healthy controls.4,21 It is theorized that while these acute changes in the SF molecular milieu after injury typically revert to baseline over time, a subset of patients experiences sustained posttraumatic inflammation, leading to degradation of articular cartilage and progression of PTOA.17,20
Several studies have demonstrated that elevations in proinflammatory SF biomarkers after injury are predictive of worse outcomes. Cuéllar et al 7 and Garriga et al 11 examined a range of knee injuries and found that elevations in IL-6 and MCP-1 corresponded to worse pain and functional scores at baseline and 2-year follow-up. Additionally, Moore et al 26 recently reported that a proinflammatory phenotype after knee injury is predictive of worse long-term outcomes, further supporting the role of synovial inflammation in disease progression. However, while significant research has focused on the acute postinjury period, there is limited research into the chronic period after injury and how this may affect long-term outcomes.
Therefore, the purpose of the current study was to investigate the relationship between biomarker levels in SF at the time of meniscectomy and long-term patient-reported outcomes (PROs) in patients with acute versus chronic meniscal injuries. It was hypothesized that patients with higher levels of proinflammatory markers would demonstrate worse PROs at final follow-up. Additionally, it was hypothesized that patients with chronic injuries and persistently elevated inflammatory markers would demonstrate worse outcomes after arthroscopy.
Methods
Study Design
This was a retrospective analysis of a prospectively collected database from an institutional review board–approved study (i15-00929) of patients who underwent knee SF aspiration on the day of arthroscopic knee surgery for isolated meniscal injury at a single institution between July 2011 and October 2020. Patients were included in the study if they were indicated for partial meniscectomy based on persistent pain, mechanical symptoms, physical examination, and imaging and had a minimum 4 years of follow-up. All enrolled patients had SF aspirated from the operative knee before surgical incision, and the concentrations of 10 selected pro- and anti-inflammatory biomarkers were quantified and recorded.
Patients were classified as having either acute meniscal injury, defined as <6 weeks of symptoms, or chronic meniscal injury, defined as a symptom duration >12 months as outlined by Keene et al. 16 Exclusion criteria were as follows: symptom duration from 6 weeks to 12 months, any associated ligamentous injury, concomitant meniscal repair, concomitant cartilage or meniscal transplantation, age <18 years, systemic inflammatory disease, autoimmune disease, intra-articular corticosteroid injection in the 3 months before surgery, previous ipsilateral knee surgery, severe osteoarthritis (Kellgren-Lawrence [KL] grade >3), immunomodulatory drug use, chemotherapy within the past year, insufficient SF aspiration, and insufficient biomarker data.
Patients were asked to complete a survey before their operation and at final follow-up that included visual analog scale for pain (VAS pain), Lysholm Knee Questionnaire, Tegner Activity Scale, and Knee injury and Osteoarthritis Outcome Score–Physical Function Short-form (KOOS-PS). Patients who did not complete follow-up PROs but met all inclusion criteria were included for clustering and follow-up procedure analysis but not for outcome score analysis. Patients who underwent subsequent ipsilateral knee surgery before collection of final outcome scores were excluded from analysis of PROs. Patient demographic factors (age, sex, BMI, smoking status), subsequent ipsilateral knee surgery, and postoperative corticosteroid injections were identified through review of the electronic medical record. Details about the meniscal injury were collected from operative reports including the size of the lesion, location, and tear type. The tear type was classified as simple (1 major tear component—longitudinal, horizontal, or radial), degenerative, bucket-handle, or complex (multiplane combination with ≥2 tear components) as described by Marigi et al. 23 Finally, preoperative radiographs were analyzed to determine KL grade.
SF Collection and Storage
For all patients in the study, SF sampling was performed with an 18-gauge needle and a 20-mL syringe. Samples were obtained after surgical preparation and draping from the superolateral portal site before the surgical incision. The samples were transferred from the syringe to sterile tubes containing a protease inhibitor solution (Halt Protease Inhibitor Cocktail, EDTA-Free; Pierce Biotechnology). The samples were immediately centrifuged at 3820 rpm (2288g) and 20°C for 10 minutes and stored at −80°C until the time of analysis. A minimum of 250 μL of supernatant after centrifugation was required for adequate processing.
Biomarker Analysis
SF samples were analyzed to determine the concentrations of 10 biomarkers that have been suggested to play a role in joint space inflammation and cartilage degradation. 6 Custom and standard precoated multiplex V-PLEX Plus human assay plates (Meso Scale Discovery) were used: human interleukin 1 receptor antagonist (IL-1Ra) kit, human tissue inhibitor of metalloproteinase 1 kit, human regulated on activation, normal T cell expressed and secreted (RANTES) ultrasensitive kit, human matrix metallopeptidase 3 (MMP-3) ultrasensitive kit, human basic fibroblast growth factor (bFGF) kit, human tissue inhibitor of metalloproteinase 2 kit, and MULTI-SPOT Human 4-Plex Assay (IL-6, vascular endothelial growth factor [VEGF], MCP-1, and MIP-1β). The SF samples were thawed and then assayed in duplicate. The plates were read using the QuickPlex SQ 120 Plate Reader/Scanner (Meso Scale Discovery). Discovery Workbench software 4.0 (Meso Scale Discovery) was used to generate a standard curve that was compared with the standard curve provided with each kit. If the results fell within the range determined by the standard curve, they were accepted. 19
Statistical Analysis
Statistical analysis was completed in SPSS Version 29.0.2 (IBM Corp). Biomarker concentrations were log transformed to achieve a normal distribution. Normally distributed continuous variables between cohorts were compared by the 2-sample Student t test. Analyses of covariance were performed to compare groups while controlling for KL grade and BMI. Categorical variables were compared by chi-square analyses. K-means clustering was performed using simple euclidean distance to partition patients into 2 distinct cohorts based on SF biomarker levels. This technique is an unsupervised machine learning algorithm that partitions data into a predefined number of clusters by minimizing the variance within each cluster. For data that are complex and interrelated, such as SF biomarker levels, this technique identifies distinct patterns or subgroups, allowing a complex dataset to be consolidated into smaller groups with similar properties. The minimal clinically important difference (MCID) threshold was calculated by the distribution-based method with a moderate effect size (0.5), according to the following formula: MCID = effect size×SDbaseline, where SD represents the standard deviation of the baseline outcome scores, as defined by Wright et al. 31 An a priori power analysis was conducted using a previously reported MCID of 8.2 after meniscectomy 2 and a standard deviation of 12 with a resulting Cohen d of 0.066. To detect this effect size with 80% power at a significance level of 0.05, a sample size of 74 patients was required (G*Power Version 3.1.9.6).
Results
Patient Demographics and Clustering Analysis
Out of 213 patients who met inclusion for the study, 30 had an acute injury and 55 had a chronic meniscal injury (Figure 1). The total cohort had a mean ± SD age and BMI of 50.06 ± 11.64 years and 29.26 ± 5.87 kg/m2 and was majority male (54.1%). Long-term outcome scores were available for 62 of the 85 patients (72.9%) at a mean follow-up of 8.66 ± 2.27 years. Eight patients went on to have a repeat meniscectomy, 1 of whom required conversion to total knee arthroplasty (TKA). An additional 7 patients underwent TKA without previous repeat meniscectomy. PROs for these patients were excluded from the analysis if recorded after their subsequent surgery.
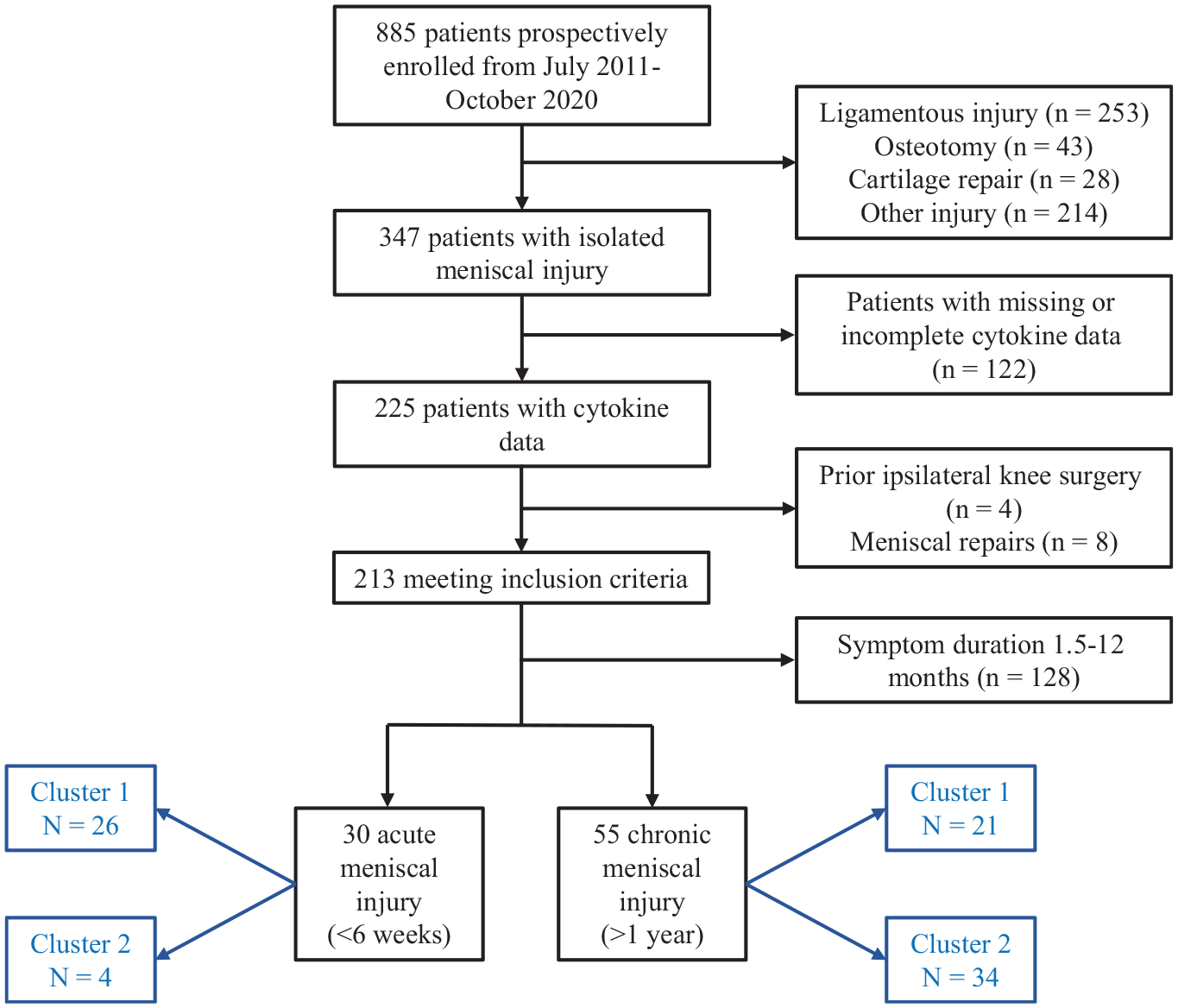
Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) diagram of included patients.
Of the total cohort of 85 patients, the K-means clustering analysis of SF biomarkers identified 2 distinct clusters: cluster 1 consisted of 47 individuals, and cluster 2 consisted of 38 individuals. Cluster 1 (“high-inflammation” phenotype) had significantly higher log-transformed levels of several biomarkers when compared with cluster 2 (“low-inflammation” phenotype), including IL-6, MCP-1, MIP-1β, VEGF, IL-1Ra, MMP-3, and bFGF (Table 1). The age, sex, BMI, smoking status, laterality, and KL grade were not significantly different between clusters. The low-inflammation phenotype had a significantly higher proportion of chronic cases than the high-inflammation phenotype (89.5% vs 44.7%; P < .001). The majority (86.7%) of patients who were acutely injured were in the high-inflammation phenotype, whereas those who were chronically injured were divided between the high (38.2%) and low (61.8%) cohorts.
Baseline Demographics and Cytokine Profiles of Entire Cohort by Inflammation Cluster a
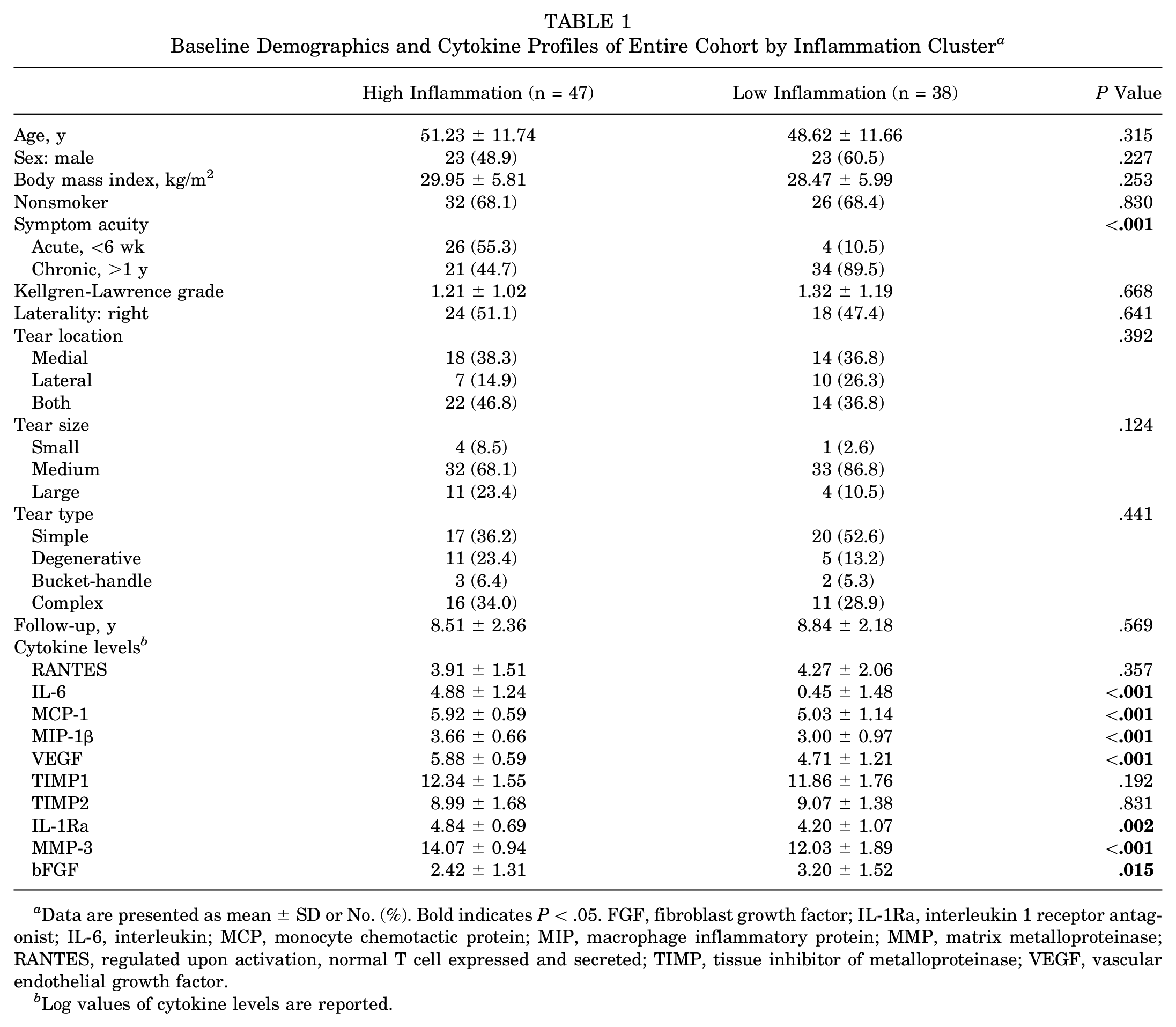
Data are presented as mean ± SD or No. (%). Bold indicates P < .05. FGF, fibroblast growth factor; IL-1Ra, interleukin 1 receptor antagonist; IL-6, interleukin; MCP, monocyte chemotactic protein; MIP, macrophage inflammatory protein; MMP, matrix metalloproteinase; RANTES, regulated upon activation, normal T cell expressed and secreted; TIMP, tissue inhibitor of metalloproteinase; VEGF, vascular endothelial growth factor.
Log values of cytokine levels are reported.
PRO Analysis for Entire Cohort
The high-inflammation phenotype had significantly lower preoperative scores on the KOOS-PS (52.00 ± 18.12 vs 64.73 ± 17.49; P = .035) and Tegner scale (1.92 ± 1.18 vs 3.11 ± 1.37; P < .001) as compared with the low-inflammation cohort when controlling for degree of osteoarthritis and BMI. There were no significant differences in postoperative VAS pain, Lysholm, KOOS-PS, or Tegner scores between cohorts (Table 2).
Pre- and Postoperative Outcome Scores of Entire Cohort by Inflammation Cluster a
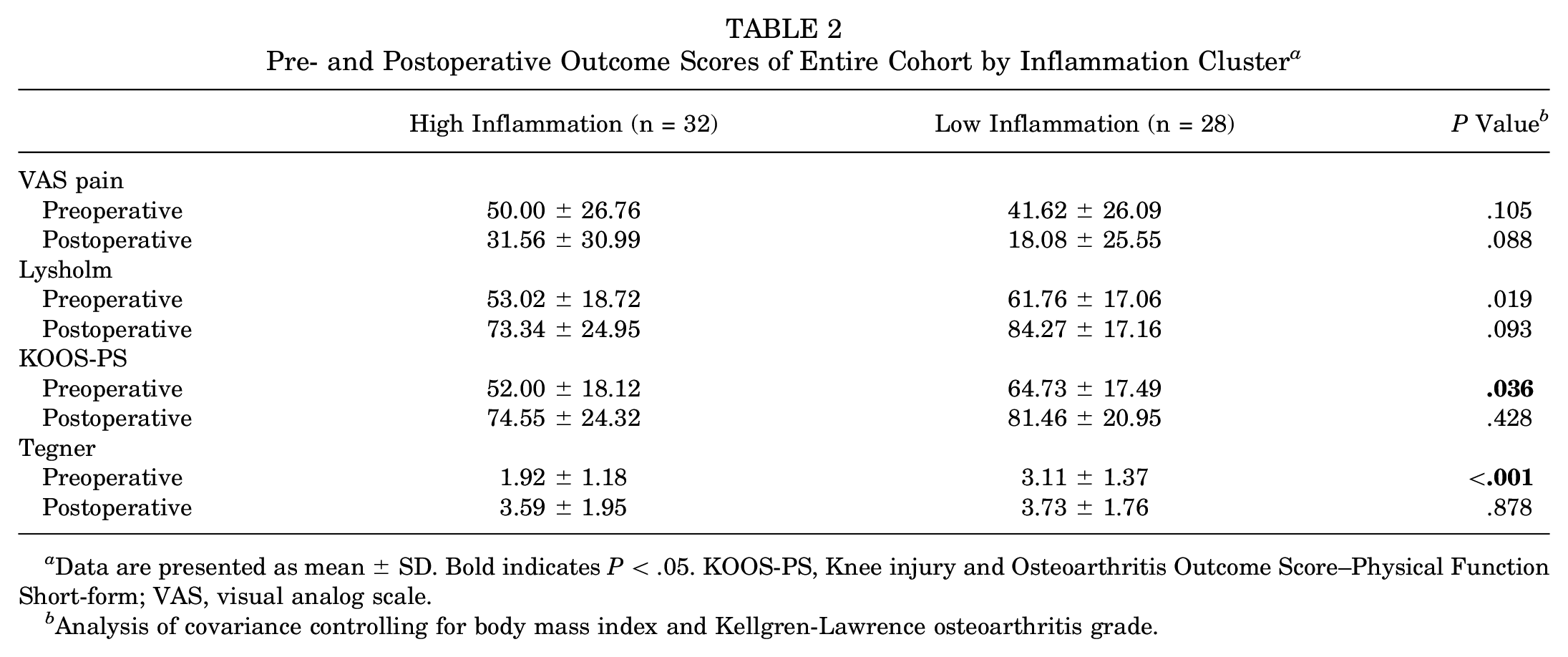
Data are presented as mean ± SD. Bold indicates P < .05. KOOS-PS, Knee injury and Osteoarthritis Outcome Score–Physical Function Short-form; VAS, visual analog scale.
Analysis of covariance controlling for body mass index and Kellgren-Lawrence osteoarthritis grade.
Chronic Cohort Subanalysis
Among the chronic cohort subanalysis comparing the high- and low-inflammation phenotypes, the high-inflammation cohort was significantly older than the low-inflammation cohort (55.64 ± 7.08 vs 48.04 ± 12.17 years; P = .014). There was no significant difference in sex, BMI, smoking status, KL grade, laterality, or location of meniscal tear between groups (Table 3).
Baseline Demographics of Chronic Subcohort by Inflammation Cluster a
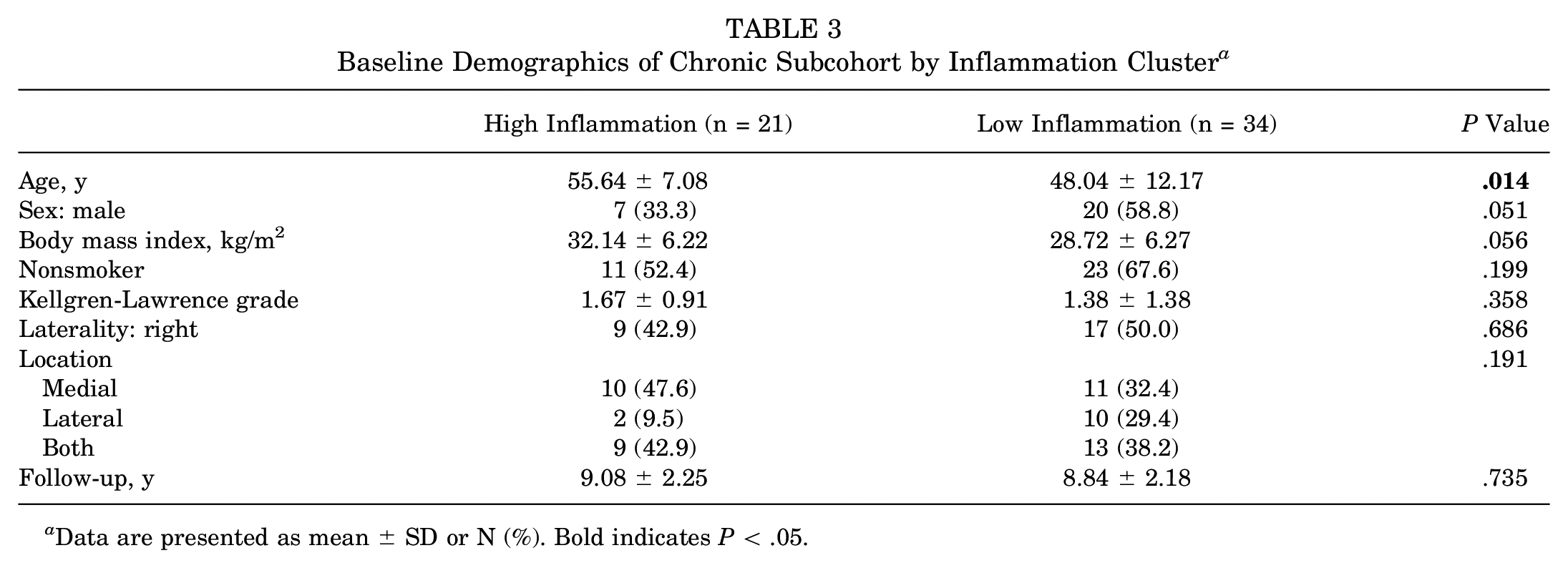
Data are presented as mean ± SD or N (%). Bold indicates P < .05.
In the subanalysis of patients who were chronically injured, the high-inflammation cohort had significantly higher preoperative VAS pain (63.00 ± 26.38 vs 43.64 ± 25.23; P = .023) and lower preoperative Lysholm (48.25 ± 21.77 vs 60.27 ± 17.28; P = .031) when compared with the low-inflammation cohort. There was no significant difference in preoperative Tegner or KOOS-PS when controlling for degree of osteoarthritis and BMI (Table 4).
Pre- and Postoperative Outcome Scores of Chronic Cohort by Inflammation Cluster a
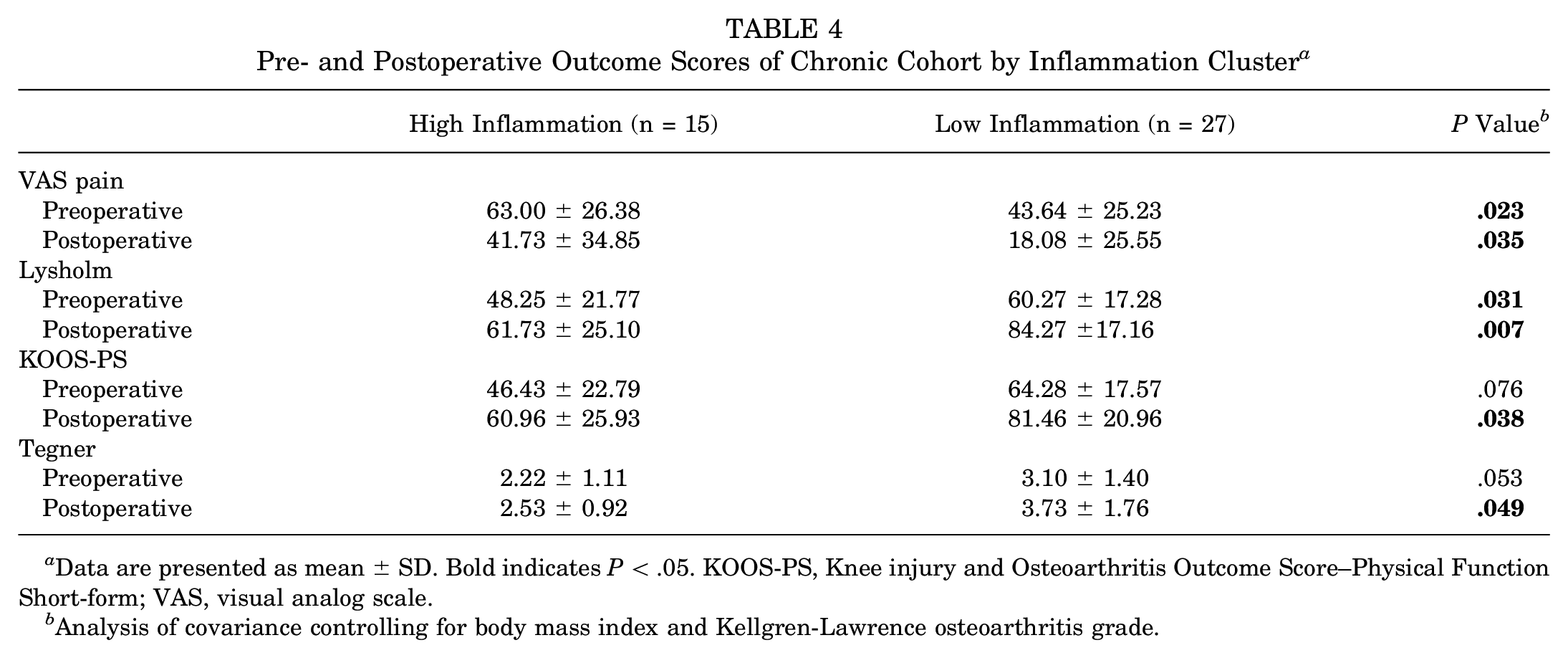
Data are presented as mean ± SD. Bold indicates P < .05. KOOS-PS, Knee injury and Osteoarthritis Outcome Score–Physical Function Short-form; VAS, visual analog scale.
Analysis of covariance controlling for body mass index and Kellgren-Lawrence osteoarthritis grade.
With respect to postoperative scores, the high-inflammation phenotype cohort had significantly higher levels of VAS pain at final follow-up (41.73 ± 34.85 vs 18.08 ± 25.55; P = .035) when controlling for degree of osteoarthritis and BMI. Additionally, the high-inflammation phenotype had significantly lower scores on the Lysholm questionnaire (61.73 ± 25.10 vs 84.27 ± 17.16; P = .007), KOOS-PS (60.96 ± 25.93 vs 81.46 ± 20.96; P = .038), and Tegner scale (2.53 ± 0.92 vs 3.73 ± 1.76; P = .049) at final follow-up.
Achievement of MCID by Inflammation Cluster
The distribution-based MCID was calculated for the Lysholm and KOOS-PS scoring systems using the entire patient cohort. The calculated threshold for the Lysholm MCID was 9.5 and for the KOOS-PS it was 9.2. As compared with the high-inflammation group, a significantly higher proportion of patients in the low-inflammation group met the Lysholm MCID (70.3% vs 33.3%; P = .020) and the KOOS-PS MCID (74.1% vs 33.3%; P = .010) (Figure 2).
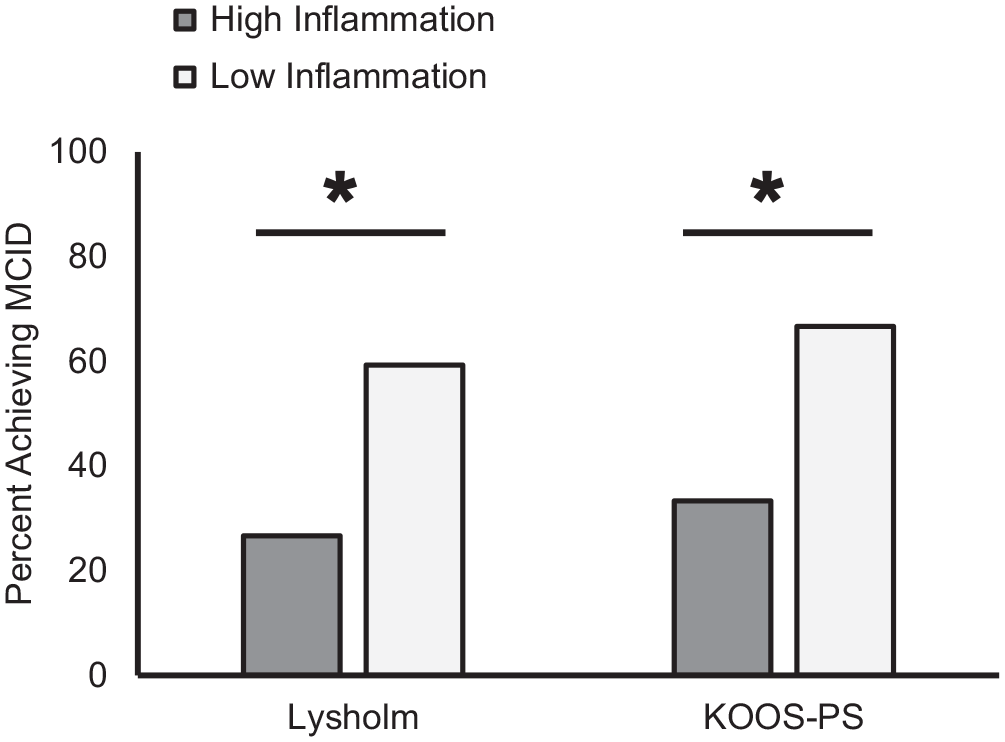
Comparison of achievement of MCID for Lysholm and KOOS-PS scoring systems by high- and low-inflammation groups. *P < .05. KOOS-PS, Knee injury and Osteoarthritis Outcome Score–Physical Function Short-form; MCID, minimal clinically important difference.
Follow-up Procedures by Inflammation Cluster
Overall, 8 patients converted to TKA: 6 (12.8%) in the high-inflammation group and 2 (5.3%) in the low-inflammation group (P = .239). Eight patients went on to have repeat meniscectomies: 5 (10.6%) in the high-inflammation group and 3 (7.9%) in the low-inflammation group (P = .667). There was no difference in overall reoperations between groups (10 in high inflammation vs 5 in low inflammation; P = .329). Eighteen patients (21.2%) required corticosteroid injections for subsequent pain in the operative knee at a median 3.69 years (IQR, 2.73-5.41) after surgery. While there was no significant difference in the rate of postoperative injections between the high- and low-inflammation groups overall (25.5% vs 15.8.0%; P = .274), within the chronic cohort, those in the high-inflammation group had a significantly higher rate of postoperative injections as compared with the low-inflammation group (42.9% vs 14.7%; P = .020).
Comparison of Acute and Chronic Meniscal Injuries
An additional subanalysis was performed to evaluate any differences in outcomes between patients who were chronically and acutely injured. There was no difference in pre- or postoperative VAS pain, KOOS-PS, or Lysholm scores between patients who were acutely versus chronically injured when controlling for BMI and KL grade (Table 5). However, the chronically injured group had a higher baseline Tegner score (2.74 ± 1.37 vs 1.93 ± 1.30; P = .013) and lower postoperative Tegner score (3.26 ± 1.59 vs 4.53 ± 2.15; P = .042) than the acutely injured group. There was no significant difference in conversion to TKA, repeat meniscectomy, postoperative injections, and overall reoperations between the patients who were acutely and chronically injured.
Comparison of Pre- and Postoperative Outcome Scores Between Acute and Chronic Meniscal Injuries a
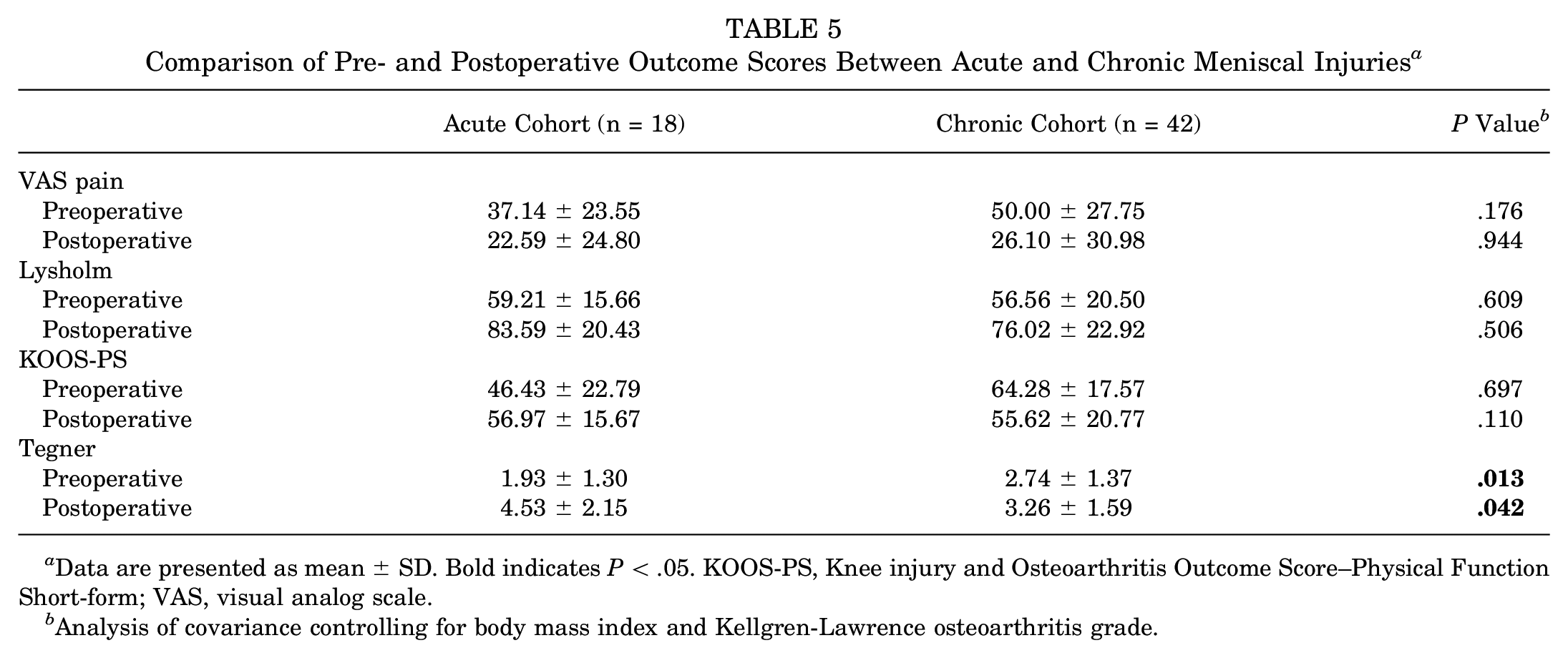
Data are presented as mean ± SD. Bold indicates P < .05. KOOS-PS, Knee injury and Osteoarthritis Outcome Score–Physical Function Short-form; VAS, visual analog scale.
Analysis of covariance controlling for body mass index and Kellgren-Lawrence osteoarthritis grade.
Discussion
The most important findings from the present study are that in patients with chronic meniscal injuries, elevated inflammatory biomarker levels in knee SF at the time of arthroscopic surgery were predictive of worse long-term outcomes. While the majority of patients who had acutely injured menisci demonstrated a high-inflammation profile, this profile was not itself a predictor of poor long-term outcomes. Rather, only those with a high-inflammation pattern and a chronic meniscal injury were predisposed to worse outcomes, lower achievement of MCID, and higher injection rates at long-term follow-up. These findings suggest that patients with persistently high inflammatory markers after injury may be at risk for worse outcome scores at long-term follow-up, thus underscoring the detrimental effects of chronic inflammation after knee injury.
Most patients with an acute meniscal injury demonstrated a proinflammatory biomarker profile, with 86.7% of patients falling into the high-inflammation cluster. Key elevated biomarkers in this cohort were IL-6, MCP-1, MIP-1β, VEGF, IL-1Ra, MMP-3, and bFGF. Elevation of these cytokines, chemokines, and matrix metalloproteinases after meniscal injury is consistent with previous findings by Clair et al 19 and Liu et al 21 that showed elevated IL-6, MCP-1, MIP-1β, and MMP-3 in meniscal injury when compared with healthy contralateral knee controls. Additionally, Ali et al 1 demonstrated that growth factors such as VEGF were significantly higher after acute meniscal injury and declined with time after injury. Similar findings have been demonstrated for other acute knee injuries, such as ACL tear and tibial plateau fracture, with an initial surge of biomarkers such as IL-6, MIP-1β, and MMP-3 at the time of injury, followed by a gradual decline until up to 6 months posttrauma.3,13-15,30 This surge of inflammatory biomarkers after acute injury is a well-documented phenomenon that is physiologic rather than pathologic. Accordingly, it follows that the acutely injured group with elevated biomarkers was not at an elevated risk for worse outcome scores.
In contrast to the patients with acute meniscal tear who mostly expressed the high inflammatory phenotype, those with chronic meniscal injury were split between low- and high-inflammation phenotypes. Among this chronic cohort, those with a high-inflammation phenotype at the time of operation had worse preoperative pain and outcome scores. This is consistent with findings by Cuellar et al, 5 which demonstrated that an increased concentration of several proinflammatory biomarkers, including MCP-1, MIP-1β, and IL-6, was associated with more painful knees after meniscal injury. Studies in animal models have suggested that elevated levels of inflammatory biomarkers may contribute to increased sensation of pain due to cytokine-induced sensitization of nociceptors,8,27,29 which innervate the outer third of the meniscus. 12 This may explain a causative relationship between elevated inflammatory biomarkers and increased preoperative pain scores as well as lower functional scores. The differential effects on outcomes in those with a high inflammatory phenotype in the acute setting versus the chronic setting therefore may be related to a pathologically long duration.
While the relationship between increased inflammatory biomarkers and increased patient pain at the time of fluid aspiration has been established, there are limited data regarding the predictive ability of these biomarkers for long-term outcomes. Previous studies by Kingery et al 18 and Cueller et al 6 demonstrated that levels of biomarkers aspirated at the time of surgery correlated with short- and midterm outcome scores, but the underlying mechanism for this relationship is still unclear. One proposed theory of increasing interest involves the relationship between inflammatory cytokines and chemokines and posttraumatic osteoarthritis. After injury, there is an acute surge of cytokines, chemokines, and growth factors, which lead to cartilage remodeling and tissue healing.25,28,32 However, while most patients experience a decrease in proinflammatory markers and return to homeostasis, it is theorized that a subset of patients continues to experience sustained posttraumatic inflammation, resulting in degradation of the cartilage matrix, pathologic joint remodeling, and progression to PTOA.17,20 This delineation between an acute physiologic inflammatory response and chronic pathologic inflammation is evidenced by the findings in this study. While there was no difference in outcome scores between the high- and low-inflammation cohorts overall, among those with a chronic injury, the high-inflammation phenotype had significantly worse long-term pain, worse outcomes scores, and higher rate of postoperative injections. This suggests that it is the chronic nature of the injury and inflammation, rather than the inflammatory response itself, that contributes to poor outcomes.
These findings have clinical implications for the treatment of patients with chronic meniscal injuries and high-inflammatory profiles. Identifying patients with elevated proinflammatory biomarkers could help set appropriate expectations regarding postoperative recovery. Additionally, as targeted anti-inflammatory and biologic therapies continue to be explored, this research may help identify populations that could benefit from such interventions. Finally, patients with high-inflammatory profiles may warrant closer postoperative monitoring and potentially earlier intervention, such as physical therapy modifications or adjunct anti-inflammatory treatments, to optimize recovery and mitigate the risk of poorer long-term outcomes. However, further research is necessary to determine the efficacy of these approaches in improving patient outcomes.
Limitations
The results of this study must be understood through the context of its limitations. While the data reported provide insight into the intra-articular conditions of patients with meniscal pathology during the acute and chronic periods, they represent only a snapshot of a multifaceted and constantly evolving SF microenvironment. While this study focused on 10 biomarkers that our research team and other experts have determined to be clinically relevant, many other biomarkers may be involved in an inflammatory response and are potential avenues for future study. In addition, as patients were aspirated only at the time of surgery, the current study is limited to 1 time point for each patient. This makes determining a temporal relationship between biomarkers difficult and allows only for extrapolation of time points among different patients. Future studies are needed that correlate changes in SF biomarker values at multiple time points with PROs and the development of osteoarthritis. This study is also limited by its retrospective design, which introduces potential selection bias and restricts the variables that could be analyzed or controlled for. Furthermore, PROs that were collected after a follow-up ipsilateral procedure were excluded, which may have introduced bias into the results. Finally, the classification of acute and chronic injuries was based on documented symptom duration, which generally corresponds to the injury time point but is not an absolute measure.
Conclusion
In patients with chronic meniscal injury, those with a more proinflammatory SF biomarker profile at the time of meniscectomy had worse outcomes than those with a less proinflammatory profile. In acute meniscal injuries, most patients demonstrate a high inflammatory profile, which was not associated with a difference in long-term outcomes.
Footnotes
Submitted January 7, 2025; accepted April 7, 2025.
One or more of the authors has declared the following potential conflict of interest or source of funding: D.J.K. has received hospitality payments from Arthrex, Exactech Inc, and Stryker; honoraria from Encore Medical; and support for education from Smith & Nephew and Gotham Surgical Solutions & Devices. E.S. has received consulting fees from Arthrex, Joint Restoration Foundation, Smith & Nephew, Vericel, DePuy Synthes Products, and Organogenesis; research support from Organogenesis, Cartiheal, and Fidia; support for education from Gotham Surgical Solutions & Devices; and publishing royalties from Jaypee Publishing and Springer. E.S. also holds stock or stock options in Better PT and Overture Orthopaedics. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.