
Abstract
Background:
Nonoperative management versus medial patellofemoral ligament reconstruction (MPFLR) for first-time patellar dislocations remains controversial, and it is unclear whether the increased up-front costs from MPFLR are justified.
Purpose:
To compare the cost-effectiveness of an initial trial of physical therapy alone to that of early MPFLR to determine the preferred cost-effective treatment strategy for first-time patellar dislocations.
Study Design:
Economic and decision analysis; Level of evidence, 3.
Methods:
A Markov chain Monte Carlo probabilistic model was developed to evaluate the outcomes and costs (in US$) of 1000 simulated patients undergoing nonoperative management versus MPFLR for first-time patellar dislocations. Health utility values, transition probabilities, and costs were derived from published level 1/2 evidence in the literature. Outcome measures included costs, quality-adjusted life years (QALYs), and the incremental cost-effectiveness ratio (ICER). The 10-year cost for each patient in the microsimulation model was averaged by the initial treatment strategy to capture the costs of any subsequent treatment methods that the patient underwent as a result of recurrent dislocations. Cycle length was defined as 1 year, with all costs and utilities discounted at 3% annually.
Results:
Over the 10-year time horizon, mean total costs resulting from nonoperative management and MPFLR were $46,223 ± $9562 and $37,298 ± $14,130, respectively. On average, MPFLR was associated with 8.5 ± 0.6 QALYs, while nonoperative management was associated with 7.1 ± 0.5 QALYs. Overall, MPFLR was determined to be the preferred cost-effective strategy in 95.3% of patients included in the microsimulation, with nonoperative management predicted to be the preferred strategy in 4.7% of patients.
Conclusion:
MPFLR was shown to be the dominant cost-effective treatment strategy for first-time patellar dislocations based on the Monte Carlo microsimulation and probabilistic sensitivity analysis, and despite increased up-front costs, MPFLR was found to save costs in the long term. Patients who underwent an initial trial of nonoperative management experienced an increased risk of recurrent dislocations that ultimately resulted in an average cost for the nonoperative group that exceeded that of the MPFLR group because of the increased downstream costs incurred for recurrent dislocations. While this study supports the long-term cost-saving potential of MPFLR, these findings should be interpreted within the context of individual patient characteristics and clinical judgment.
A patellar dislocation is a prevalent injury among young, active patients, often resulting from sports-related trauma. Despite the high recurrence rate and association with subsequent joint degeneration, such as patellofemoral arthritis, the optimal management strategy for first-time patellar dislocations remains a subject of ongoing debate. Nonoperative management is commonly employed initially, offering simplicity and avoiding surgical risks. However, it is associated with recurrence rates as high as 45%, potentially leading to additional intra-articular damage and compromised knee function. 8 In contrast, medial patellofemoral ligament reconstruction (MPFLR) has been shown in multiple randomized controlled trials to demonstrate superior outcomes in preventing recurrent instability and normalizing knee function. 8 This superiority is particularly evident in young, active patients with high anatomic or biomechanical risk factors for recurrence.
While its clinical outcomes are well documented, the economic implications of MPFLR compared with nonoperative treatment for first-time dislocations remain underexplored, and it is unclear whether the increased up-front costs from MPFLR are justified. The cost-effectiveness of these approaches is particularly relevant in light of increasing health care expenditures and the need for value-driven decision-making. Thus, the purpose of this study was to compare the cost-effectiveness of an initial trial of physical therapy alone to that of early MPFLR to determine the preferred cost-effective treatment strategy for first-time patellar dislocations. The hypothesis was that MPFLR would be more cost-effective than nonoperative management via Markov model–based cost-effectiveness analyses for first-time patellar dislocations.
Methods
Markov Modeling Process
Markov models are decision trees used to represent clinical courses of treatment as transitions between discrete health states based on probabilistic events occurring over a specified period of time. 1 As summarized below, each state is associated with transition probabilities and costs that are determined from empirically derived or estimated data. According to the transition probabilities, experimental patients transition between health states through Markov cycles, accruing quality-adjusted life years (QALYs) and costs at each state.
The primary outcome of a Markov model is the incremental cost-effectiveness ratio (ICER), which is defined as the difference in costs between 2 treatment options divided by the difference in acquired QALYs for those treatment options. 7 For the present study, the treatment strategies were (1) nonoperative management and (2) MPFLR. A willingness-to-pay (WTP) threshold is defined as the maximum amount that society is willing to pay to achieve 1 additional QALY. A WTP of $50,000 is considered standard. 14 If a treatment method results in an ICER below the WTP threshold, it is considered cost-effective; as a result, the treatment with the most QALYs (lowest ICER) would be considered the optimal strategy. If a treatment method results in both lower costs and more QALYs, it is considered to be a “dominant” treatment. 3
Model Structure
The Markov decision tree model utilized in the current study was constructed from publicly available software (TreeAge Pro; TreeAge Software). A 20-year-old patient presenting with a first-time patellar dislocation served as the base case for our model. After each index treatment, patients followed the postoperative pathway as depicted in Figure 1.
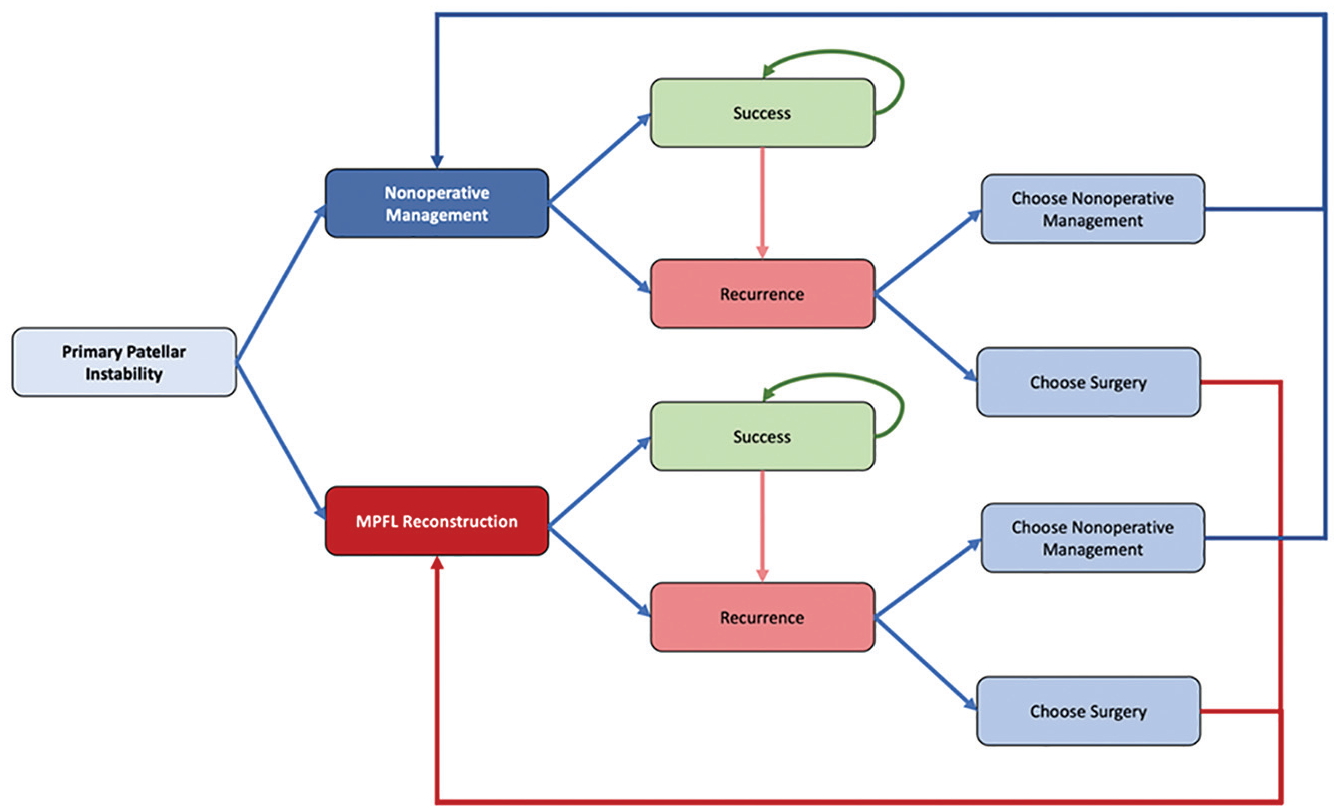
Markov model diagram depicting the flow of patients.
Model Parameters
To obtain outcomes and model inputs for patients with a first-time patellar dislocation, a targeted literature search was performed (Table 1). Recurrence rates were derived from a network meta-analysis of level 1/2 studies of patients who underwent either nonoperative management or MPFLR, while costs were derived from a report of raw up-front costs associated with nonoperative management or MPFLR from the 2014 State Ambulatory Surgery and Services Databases from 6 American states.8,11 Recurrence rates included both recurrent subluxations and dislocations.
Model Inputs for Probabilistic Sensitivity Analysis a
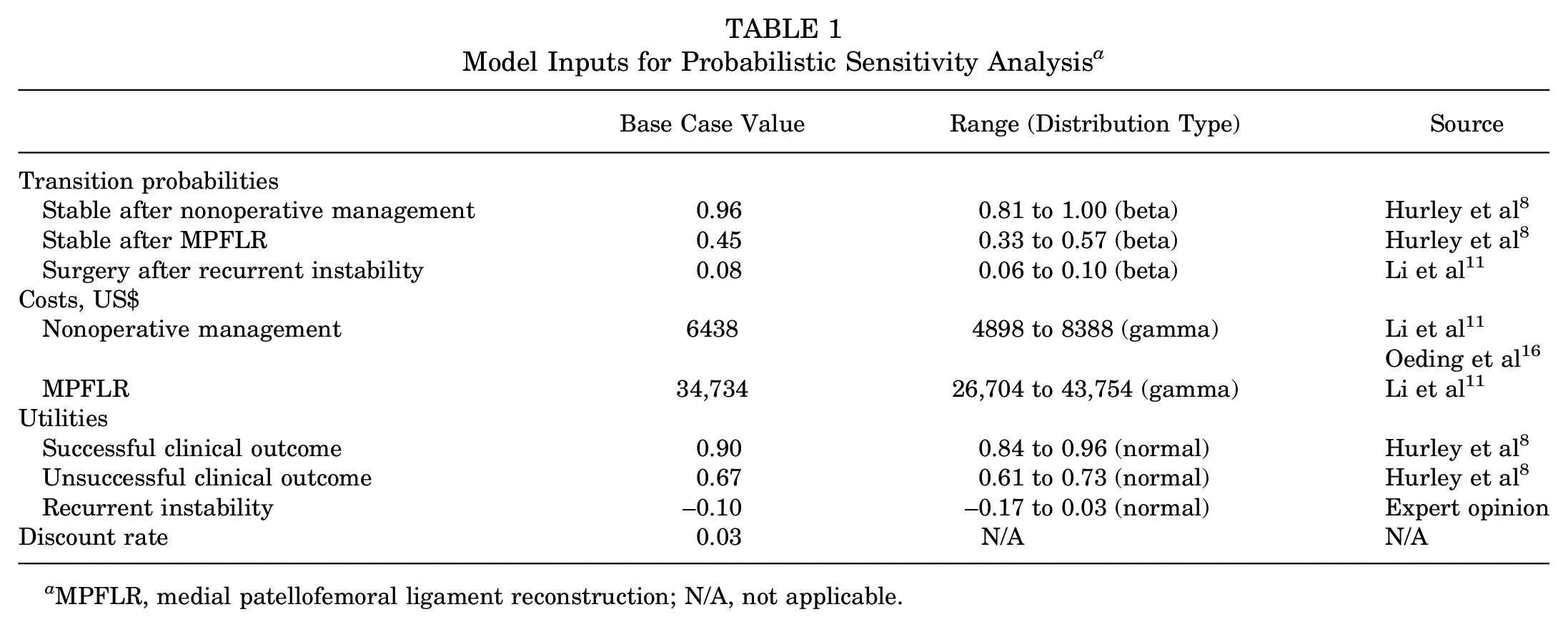
MPFLR, medial patellofemoral ligament reconstruction; N/A, not applicable.
Monte Carlo Microsimulation and Probabilistic Sensitivity Analysis (PSA)
In contrast to techniques used to create predictive models with fixed input values, the Monte Carlo simulation enables the construction of models that leverage probability distributions for variables with inherent uncertainty. In the present study, the Monte Carlo microsimulation was used to generate hypothetical patients who repeatedly traversed the model, each time with a set of different input parameters drawn from a corresponding probability distribution. For each microsimulation, patients accrued costs and utilities, and these were averaged and compared over many simulated cycles to produce more robust results that considered the uncertainty associated with estimated model inputs. A greater number of cycles that produce similar results corresponds to increased confidence that the result in question does in fact reflect reality, despite the inherent uncertainty associated with selected input parameters.
In this study, PSA was used to simultaneously vary all cost and transition probability input parameters in the model. PSA has been shown to better estimate uncertainty in the model compared with standard sensitivity analysis for microsimulations.2,6 There were 1000 patients simulated over 1000 cycles, with (1) cost parameters assigned gamma distributions based on their means and (2) transition probability parameters assigned beta distributions based on their means. 5 Standard deviations for transition probabilities and costs were assumed to be 20% of the mean based on previous analyses. 4 In this study, both costs and QALYs were discounted at a rate of 3% annually. 18 The ICER was used to evaluate the cost-effectiveness of each treatment arm by providing a measure of the cost per year incurred by undergoing the specific treatment arm that results in the highest number of QALYs. Cycle length was defined as 1 year, with an overall time horizon of 10 years.
Results
Over the 10-year time horizon, mean total costs resulting from nonoperative management and MPFLR were $46,223 ± $9562 and $37,298 ± $14,130, respectively (Table 2). On average, MPFLR was associated with 8.5 ± 0.6 QALYs, while nonoperative management was associated with 7.1 ± 0.5 QALYs. Results of the Monte Carlo microsimulation and PSA, demonstrating the predicted cost, effectiveness, and net monetary benefit associated with nonoperative management and MPFLR for patients with a first-time patellar dislocation, are also shown in Figure 2.
Results of Monte Carlo Microsimulation and Probabilistic Sensitivity Analysis a
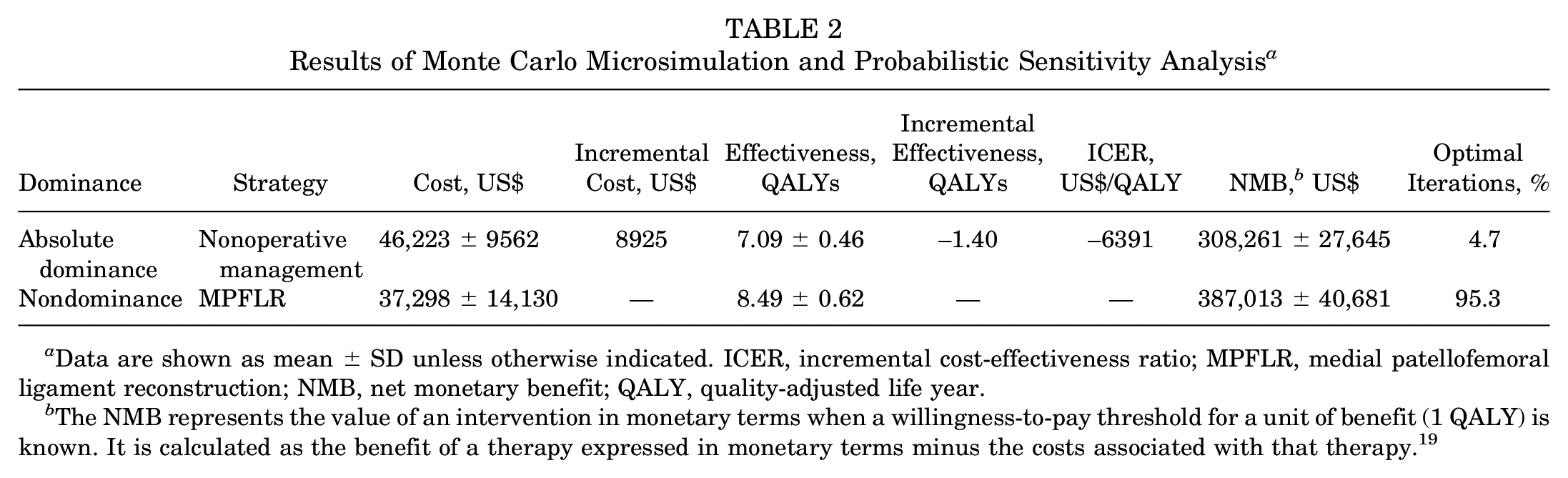
Data are shown as mean ± SD unless otherwise indicated. ICER, incremental cost-effectiveness ratio; MPFLR, medial patellofemoral ligament reconstruction; NMB, net monetary benefit; QALY, quality-adjusted life year.
The NMB represents the value of an intervention in monetary terms when a willingness-to-pay threshold for a unit of benefit (1 QALY) is known. It is calculated as the benefit of a therapy expressed in monetary terms minus the costs associated with that therapy. 19
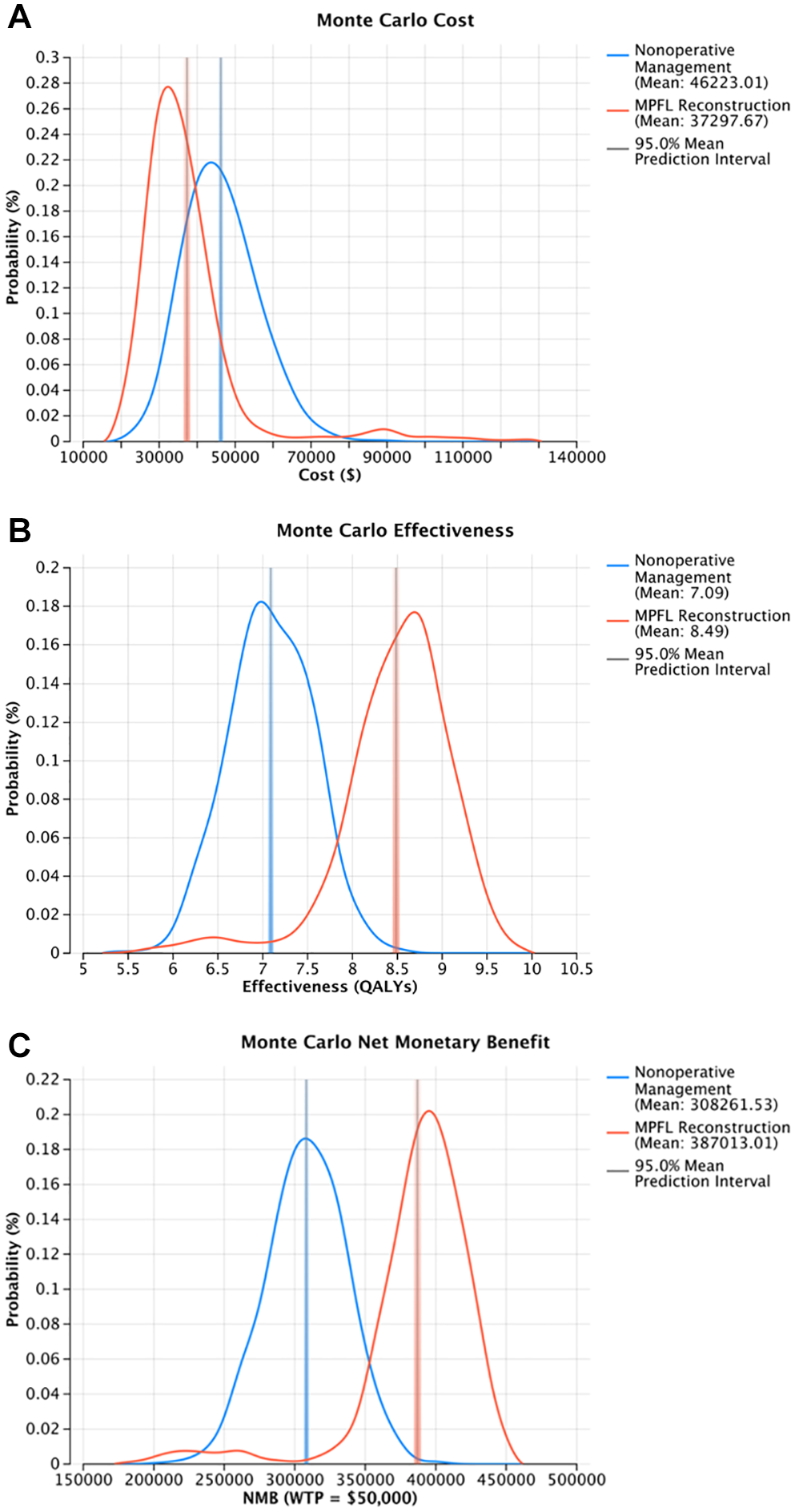
Results of the Monte Carlo microsimulation and probabilistic sensitivity analysis, demonstrating the predicted (A) cost, (B) effectiveness, and (C) net monetary benefit (NMB) associated with nonoperative management and medial patellofemoral ligament reconstruction (MPFLR) for patients with primary patellar instability. The NMB represents the value of an intervention in monetary terms when a willingness-to-pay (WTP) threshold for a unit of benefit (1 quality-adjusted life year [QALY]) is known. It is calculated as the benefit of a therapy expressed in monetary terms minus the costs associated with that therapy. 19
Cost-effectiveness acceptability curves for each treatment strategy at WTP thresholds from $0/QALY to $10,000/QALY are provided in Figure 3. The effectiveness scatterplot is depicted in Figure 4. Overall, MPFLR was determined to be the preferred cost-effective strategy in 95.3% of patients included in the microsimulation, with nonoperative management predicted to be the preferred strategy in 4.7% of patients.
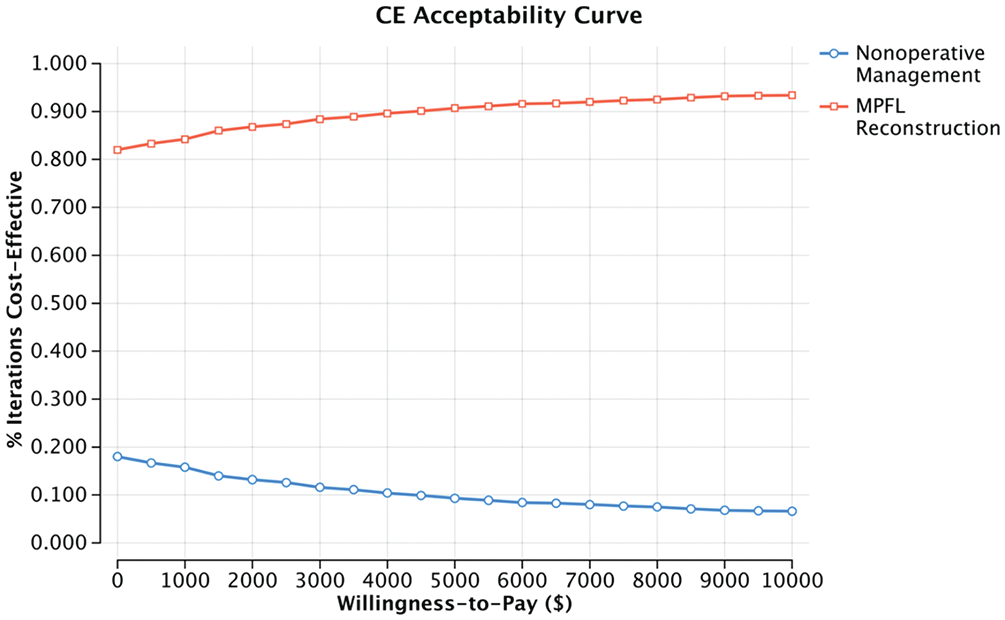
Cost-effectiveness acceptability curves for each treatment strategy at willingness-to-pay (WTP) thresholds from $0/quality-adjusted life year (QALY) to $10,000/QALY. Because medial patellofemoral ligament reconstruction (MPFLR) was determined to be the dominant treatment strategy, there was no WTP threshold beyond which nonoperative management became cost-effective.
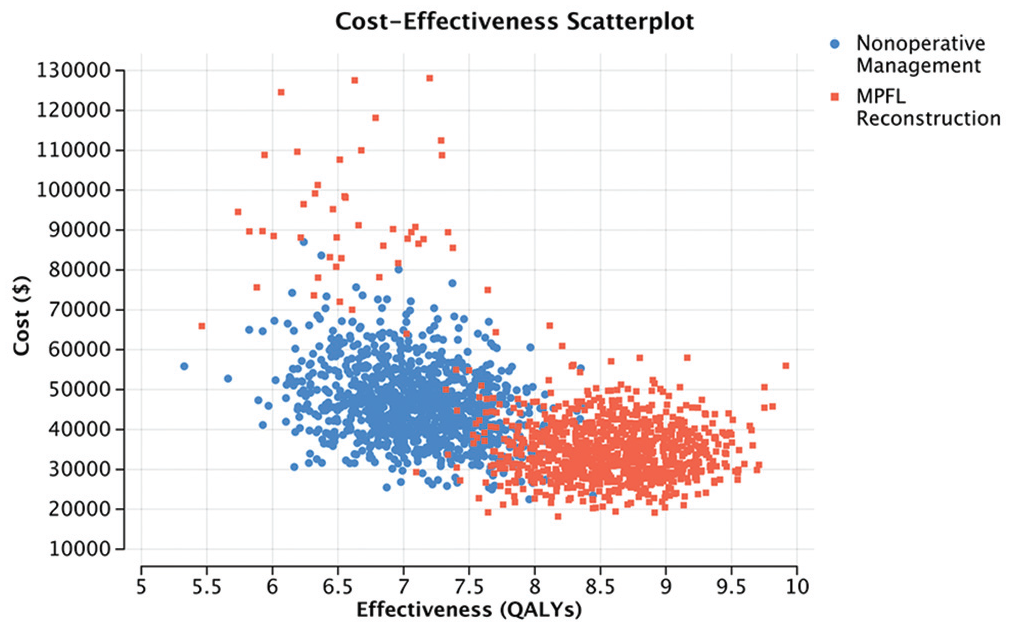
Costs and quality-adjusted life years (QALYs) per patient for each of the 1000 patients in the Monte Carlo microsimulation.
The incremental effectiveness scatterplot shown in Figure 5 illustrates the model’s predictions and confidence for patients faced with the decision of MPFLR versus nonoperative management. Dots in green correspond to patients for whom the model correctly predicted the most cost-effective treatment strategy (MPFLR over nonoperative management), while dots in red correspond to patients for whom the alternative would have been the most cost-effective treatment strategy. The model’s confidence is shown with a 95% confidence ellipse.
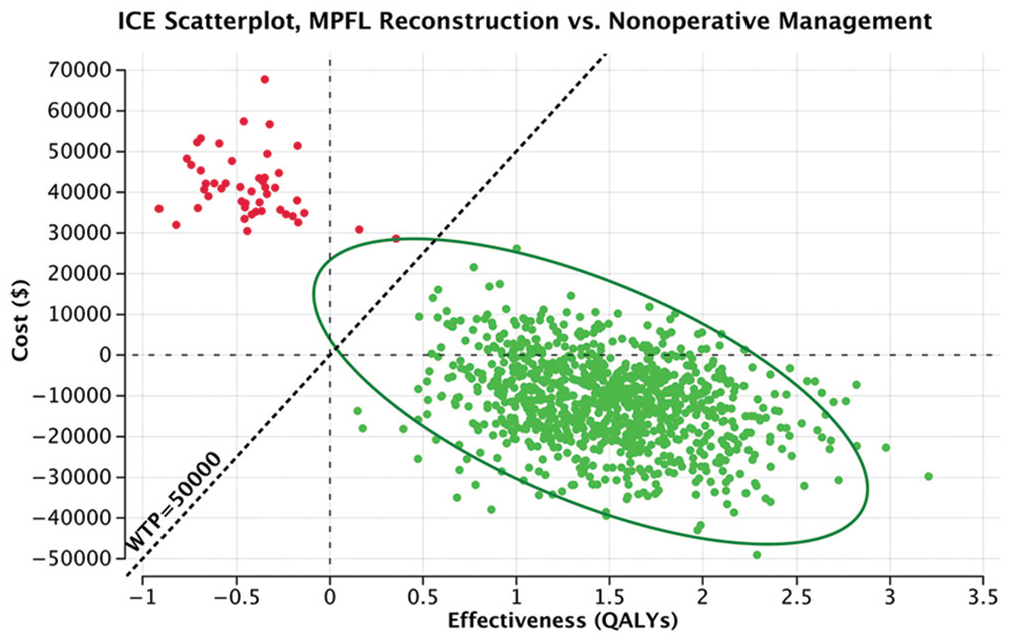
Incremental effectiveness scatterplot from probabilistic sensitivity analysis, shown with a 95% confidence ellipse. All dots to the right of the diagonal willingness-to-pay (WTP) line represent patients for whom the model predicted medial patellofemoral ligament reconstruction (MPFLR) as more cost-effective than nonoperative management at a WTP of $50,000/quality-adjusted life year (QALY) (green). Dots to the left of the WTP line correspond to patients for whom nonoperative management was the optimal strategy (red), and dots both below the $0 incremental cost line and to the right of the $50,000 WTP line correspond to patients for whom MPFLR was the dominant preferred treatment strategy.
Discussion
The most significant finding of this study is that within the constraints of our model, MPFLR emerged as the dominant cost-effective treatment strategy. MPFLR was found to save costs in the long term. Patients who underwent an initial trial of nonoperative management experienced an increased risk of recurrent dislocations that ultimately resulted in an average cost for the nonoperative group that exceeded that of the MPFLR group because of the increased downstream costs incurred for recurrent dislocations. While our study suggests a long-term economic advantage, it is important to recognize that cost-effectiveness alone should not dictate treatment recommendations, especially given the clinical variability and patient-specific factors inherent to patellar instability. Additionally, this model is not intended to suggest a universal recommendation for all first-time dislocations but rather to provide an economic perspective that may aid shared decision-making in appropriate candidates.
Cost-effectiveness analysis is an essential component in evaluating the economic impact of surgical procedures, especially as health care moves toward value-based decision-making.15-17 The cost-effectiveness of MPFLR versus nonoperative management was determined using a Markov model framework, which accounted for the costs of the procedure, reoperations, recurrence, and other clinical outcomes over a 10-year time horizon. The ICER was used to compare both treatment methods, with MPFLR emerging as the dominant strategy, resulting in better clinical outcomes in terms of QALYs gained. The model showed that over the 10-year time horizon, the mean cost of MPFLR was $8925 less than that of nonoperative management, but it resulted in 8.49 QALYs versus 7.09 QALYs for nonoperative management.
Both MPFLR and nonoperative management are commonly employed strategies for addressing patellar instability. Historically, nonoperative management has been the initial treatment choice, particularly for first-time dislocations, as it avoids surgical risks and offers a straightforward approach. However, recent studies, including a network meta-analysis of level 1/2 studies by Hurley et al, 8 have shown that MPFLR provides superior clinical outcomes, particularly in reducing the risk of recurrence. For example, they found that MPFLR significantly lowered the recurrence rate (2.7%) compared with nonoperative management (45.5%) and yielded better functional outcomes, as measured by the Kujala score (87.7 vs 84.8, respectively). These differences are critical in preventing long-term complications such as patellofemoral arthritis, which can arise from recurrent dislocations. Additionally, the reduced recurrence rate with MPFLR translates to a lower likelihood of secondary interventions, further enhancing its cost-effectiveness. While nonoperative management remains a viable option for certain patients, MPFLR appears particularly beneficial for young, active patients or those with anatomic risk factors such as an increased tibial tuberosity–trochlear groove distance or trochlear dysplasia.
The findings in this study are consistent with cost-effectiveness analyses in other areas of orthopaedics, such as anterior cruciate ligament reconstruction (ACLR) or shoulder stabilization, in which early operative interventions have been shown to be economically favorable in young, active patients.12,13 Similar to MPFLR, early ACLR prevents recurrent instability events that can lead to long-term joint degeneration and downstream health care costs. For instance, studies have demonstrated that delayed ACLR is associated with a higher risk of meniscal and chondral injuries, ultimately increasing long-term costs and reducing QALYs. 13 These parallels support the broader concept that in certain high-risk populations, earlier surgical stabilization may represent a value-based strategy.
From a clinical perspective, MPFLR demonstrates several advantages over nonoperative management. While nonoperative treatment relies on physical therapy and bracing to manage symptoms, MPFLR addresses the underlying instability by reconstructing the damaged ligament, providing a biomechanically stable patellofemoral joint. 8 This results in superior outcomes in terms of recurrence prevention and functional recovery. Moreover, MPFLR has been shown to be particularly effective in high-risk populations, such as adolescents and athletes, in whom physical demands and recurrence risks are higher. From an economic standpoint, MPFLR may also offer better long-term value. While the initial costs of surgery are higher, the reduced need for repeat medical interventions and associated rehabilitation improves the overall health care expenditure per QALY. For instance, preventing the high rates of recurrent instability seen with nonoperative management reduces downstream costs related to complications and additional procedures. These findings underscore MPFLR as a cost-effective strategy for optimizing patient outcomes and minimizing health care system burdens. However, treatment decisions should be tailored to the patient’s individual needs, considering factors such as age, activity level, and the presence of anatomic risk factors, as well as the potential benefits of an early surgical intervention in preventing long-term disability.9,10
Nonetheless, clinical decision making should consider not only economic models but also individual anatomy, patient preferences, and functional goals. While these findings support the economic value of MPFLR in terms of QALYs gained per dollar spent, we acknowledge that a modeled increase of 1.40 QALYs, although statistically meaningful, may not reflect a justifiable tradeoff for every patient. The up-front cost, potential surgical complications, and the loss of a noninvasive option with a generally favorable safety profile are important considerations. Furthermore, the QALY framework, while standard in cost-effectiveness analyses, may not fully account for the psychological resilience or quality-of-life adaptations experienced by patients managing patellar instability without surgery.
Limitations
The Markov model is a rigid model for an “average” patient undergoing a treatment option and must define definitive likelihoods of treatment failure, costs, and treatment pathways. While this limitation is minimized when applying the Monte Carlo microsimulation and PSA, this methodology did not capture the unique experience of every patient undergoing treatment for a first-time patellar dislocation. Accordingly, a shared decision-making discussion should be conducted regarding MPFLR versus nonoperative management based on individual patient factors. To conduct our analysis, assumptions were made about transition probabilities and outcomes using the current literature, including the studies from which model inputs were derived, despite the heterogeneity in patient populations. In addition, because there is variability in the costs of medical care based on practice setting and geographic location and because multiple factors contribute to an individual patient’s potential for healing, these results may not be applicable to all patients. This limitation is mitigated by performing sensitivity analyses that account for a spectrum of model inputs; however, it is not possible to remove all uncertainty from analyses.
Conclusion
MPFLR was shown to be the dominant cost-effective treatment strategy for first-time patellar dislocations based on the Monte Carlo microsimulation and PSA, and despite increased up-front costs, MPFLR was found to save costs in the long term. Patients who underwent an initial trial of nonoperative management experienced an increased risk of recurrent dislocations that ultimately resulted in an average cost for the nonoperative group that exceeded that of the MPFLR group because of the increased downstream costs incurred for recurrent dislocations. While this study supports the long-term cost-saving potential of MPFLR, these findings should be interpreted within the context of individual patient characteristics and clinical judgment.
Footnotes
Submitted December 31, 2024; accepted April 21, 2025.
One or more of the authors has declared the following potential conflict of interest or source of funding: J.F.D. has received research support from Arthrex, DePuy, the United States Department of Defense, the Orthopaedic Research and Education Foundation, and Smith & Nephew; has received intellectual property royalties from SLACK; and holds stock or stock options in Spartan Bioscience. J.R.W. has received consulting fees from Geistlich, has received speaking fees from Arthrex and Vericel, and holds stock and stock options in ViewFi. A.A. has received research support from Stryker, has received intellectual property royalties from Arthrex, has received publishing royalties from Springer and Wolters Kluwer–Lippincott Williams & Wilkins, and holds stock or stock options in Bone Solutions and Miach Orthopaedics. A.P.T. has received financial or material support from Arthrex, Breg, Mitek, Smith & Nephew, and Stryker. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.