
Abstract
Background:
Treatment decisions in patients with anterior cruciate ligament (ACL) injuries are influenced by multiple factors, such as the desire to return to sports or symptomatic instability. Identifying the differential treatment effect of ACL reconstruction (ACLR) compared with nonoperative management on a patient-specific level can inform surgical decision-making.
Hypothesis:
Unsupervised machine learning can identify distinct patient subgroups based on outcome achievement after ACL injury, and ACLR will exert a protective effect on the development of posttraumatic osteoarthritis (PTOA) over nonoperative management.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
A longitudinal populational registry identified patients with ACL injuries from 1990 to 2016 with a minimum 7.5-year follow-up. An unsupervised random forest algorithm was utilized to develop and validate patient subgroups. Treatment effects of ACLR on outcomes were analyzed using a machine learning causal inference estimator. Patient subgroup membership was incorporated into a multivariable logistic regression to identify factors predictive of optimal outcomes.
Results:
A total of 923 patients (785 primary ACLR, 138 nonoperative) were included. The random forest algorithm arrived at an optimal partition of 2 subgroups, with 653 patients in the optimal outcome subgroup (368 male [56.4%]; mean age, 26.0 ± 10.2 years; mean body mass index [BMI], 26.5 ± 4.30) and 270 patients in the suboptimal outcome subgroup (152 male [56.3%]; mean age, 35.0 ± 10.1 years; mean BMI, 30.5 ± 5.54). The latter group demonstrated significantly increased rates of secondary meniscal injury, development of symptomatic PTOA, and progression to total knee arthroplasty (TKA) at the final follow-up (all P < .01). In the optimal outcome subgroup, ACLR had significantly protective treatment effects on the risk of secondary meniscal injury (average treatment effect [ATE], 61%), contralateral ACL injury (ATE, 8%), symptomatic PTOA (ATE, 16%), and progression to TKA (ATE, 6%) (all P < .01). Conversely, in the suboptimal outcome subgroup, ACLR only protected against symptomatic PTOA (ATE, 11%) and progression to TKA (ATE, 8%) (both P < .01).
Conclusion:
Two clinically meaningful subgroups were identified from retrospectively collected data and found to experience differential treatment responses after ACL injuries. ACLR decreased the rate of development of PTOA and TKA in both subgroups but was not as effective in preventing secondary meniscal injuries or contralateral ACL injuries in patients who were older, heavier, or had concomitant medial meniscus injuries.
As greater proportions of the population become involved in athletics at a younger age,8,14,23,46 the incidence of anterior cruciate ligament (ACL) injuries in the United States has steadily increased, with estimates of between 100,000 and >200,000 injuries occurring annually.8,14,42,50 Factors that increase the risk of injury include being female, participation in high-risk cutting or pivoting sports, a quadriceps-dominant movement pattern, and a history of previous ACL injury.8,14,23 To restore the stability of the knee, active and younger patients are typically treated with ACL reconstruction (ACLR), whereas elderly or low-demand individuals may be indicated for nonoperative management. 27 Substantial evidence has highlighted the protective effect of ACLR against secondary meniscal injury.1,15,18,30 However, the role of reconstruction in delaying the development of long-term posttraumatic osteoarthritis (PTOA) is less firmly established, and PTOA after ACL injury remains a costly and clinically relevant sequela for both patients and surgeons.18,21 Furthermore, patient-specific risk factors that predict the development of PTOA despite successful reconstruction remain poorly described.
In the era of patient-centered decision-making, increasing emphasis must be placed on patient-specific goals and characteristics for determining surgical indications. Therefore, a thorough understanding of the patient and injury characteristics that predict optimal ACLR outcomes would be particularly salient. Previous research on this topic has been limited to parametric regression models.3,4 Recent machine learning approaches have combined unsupervised clustering with nonparametric inference models not only to identify but also to assess the subgroup-specific treatment effect of particular interventions with comparatively less bias. 28 This combined approach has 2 distinct advantages: First, the unsupervised clustering algorithm is a data-driven approach that identifies patient subgroups based on not a single stratifying variable (previously a human input made based on clinical intuition or previous literature) but instead a holistic measurement of the differences of all aggregate features. Second, the targeted inference models are “data adaptive” and have been shown to more closely simulate prospective study design compared with traditional causal estimators given its double-robust nature. Accordingly, the purpose of this study was to (1) utilize unsupervised clustering to identify clinically meaningful patient outcome subgroups after ACL injury, (2) use targeted maximum likelihood estimation (TMLE) to describe the treatment effect of reconstruction versus nonoperative management on these patient subgroups, and (3) identify patient-specific risk factors for optimal versus suboptimal outcomes. We hypothesized that while distinct patient subgroups exist with variable treatment responses on composite outcomes, reconstruction would demonstrate long-term protective effects against PTOA, highlighting the importance of intervention.
Methods
Study Design, Patient Selection, and Data Source
After institutional review board (IRB No. 14-005089) approval, a National Institutes of Health–sponsored established longitudinal geographic database (Rochester Epidemiology Project [REP] 34 ) was queried for patient inclusion. All patients who experienced an ACL injury between January 1, 1990, and July 31, 2016, were identified using the following International Classification of Diseases (ICD), 9th and 10th Revision diagnosis codes for ACL injury: ICD-9-CM 717.83, ICD-9-CM 844.2, ICD-10-CM S83.50, ICD-10-CM S83.51. The REP is an aggregate of >500,000 individual medical records collected from residents of Olmstead County as well as neighboring counties in southeast Minnesota and western Wisconsin. 22 After initial patient identification, patient charts were reviewed in a stepwise approach as follows: (1) confirmation of ACL injury diagnosis via arthroscopy or magnetic resonance imaging (MRI), (2) application of inclusion/exclusion criteria, and (3) chart review for data extraction. Patients were included if they (1) sustained a complete ACL rupture and subsequently underwent either nonoperative treatment or reconstruction, (2) had a minimum follow-up of 90 months (7.5 years), and (3) gave consent for research. Patients were excluded if they (1) sustained partial ACL tears, (2) underwent multiligament reconstructions (indications for concomitant ligamentous reconstruction included complete acute ruptures with no endpoint on stress examination or documented persistent instability after nonoperative treatment) or index revision ACLR, (3) had a history of previous ipsilateral arthroscopic knee surgery, or (4) were followed less than the minimum time of 90 months (Figure 1). Medical records were reviewed for the following variables: age, sex, body mass index (BMI), activity level, occupation, relevant comorbid diagnoses, number of arthroscopic surgeries on the index knee, treatment methods, concomitant radiographic findings, intraoperative findings in patients undergoing reconstruction, and clinical course after treatment. Additionally, primary outcomes of interest were also reviewed, which included (1) secondary meniscal injury identified on MRI; (2) contralateral ACL injury; (3) diagnosis of symptomatic PTOA, defined as documented radiographic osteoarthritis with accompanying symptoms in the index knee during follow-up by the treating physician; and (4) progression to total knee arthroplasty (TKA) at any time. A summary of the reviewed patient variables is provided in Table 1; however, only preoperative variables were utilized as covariates in the model to prevent target leakage.
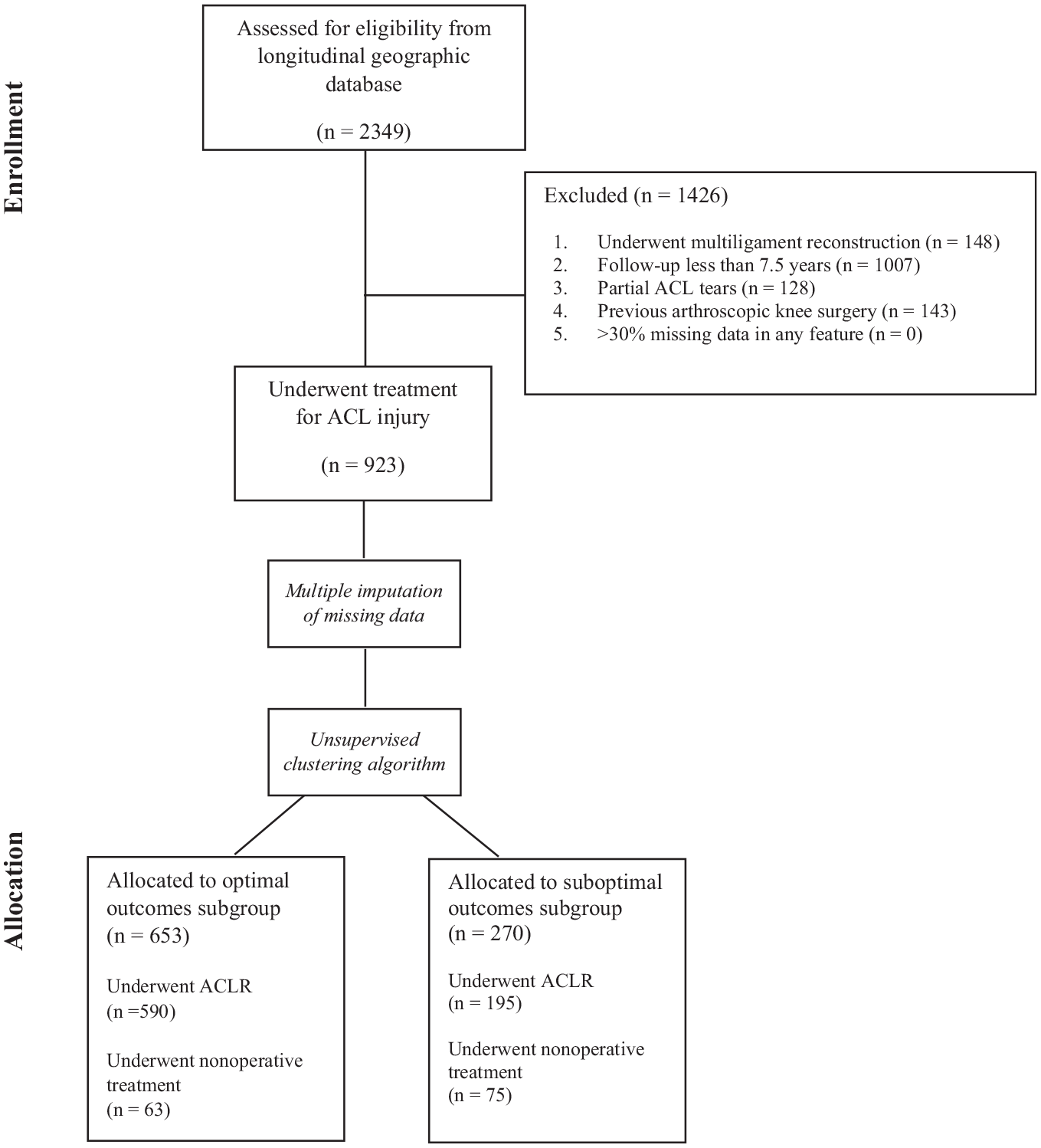
CONSORT (Consolidated Standards of Reporting Trials) flow diagram. ACL, anterior cruciate ligament; ACLR, anterior cruciate ligament reconstruction.
Comparison of Patient Characteristics Stratified by Subgroup Membership a
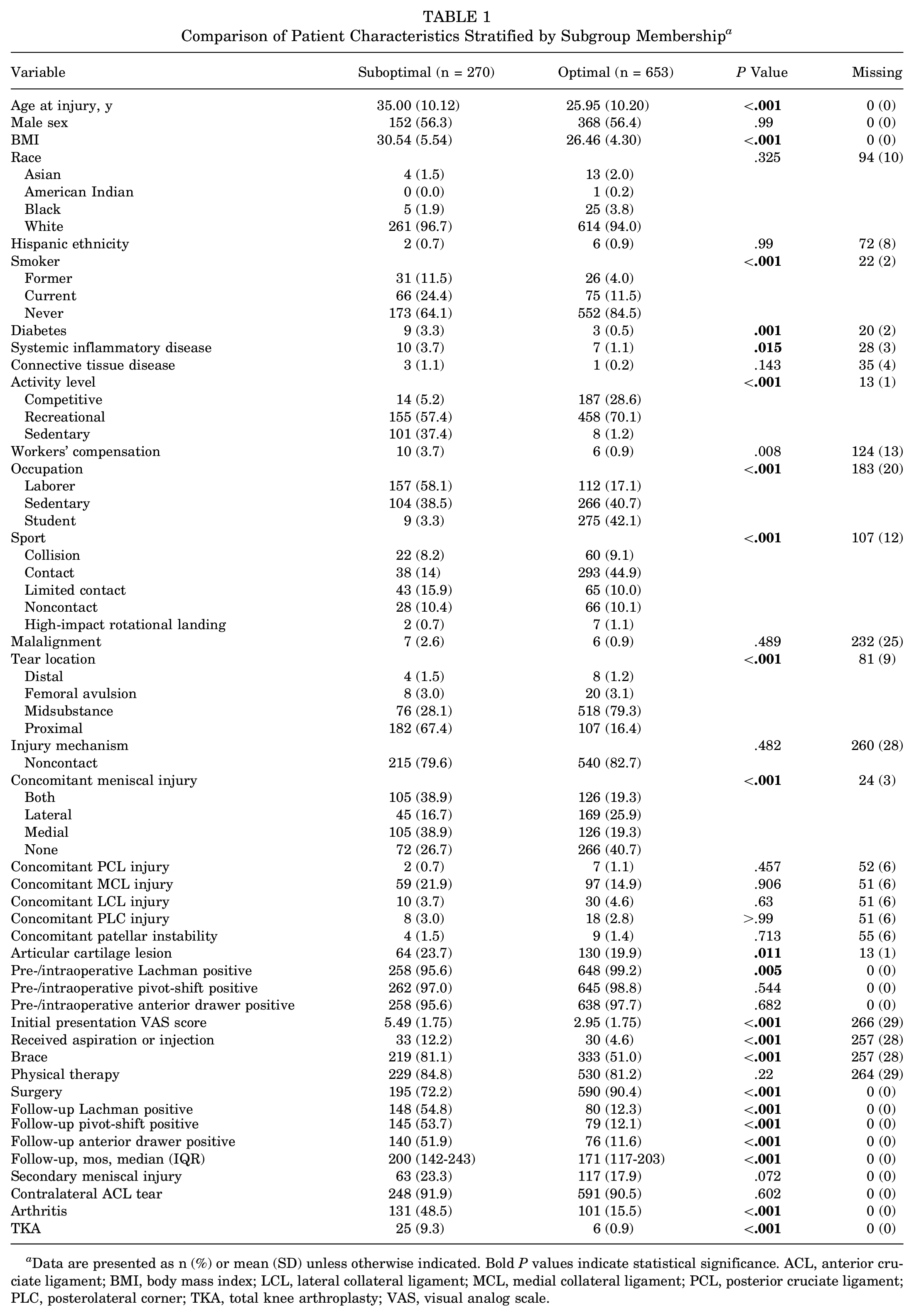
Data are presented as n (%) or mean (SD) unless otherwise indicated. Bold P values indicate statistical significance. ACL, anterior cruciate ligament; BMI, body mass index; LCL, lateral collateral ligament; MCL, medial collateral ligament; PCL, posterior cruciate ligament; PLC, posterolateral corner; TKA, total knee arthroplasty; VAS, visual analog scale.
Missing Data
Missing data were handled utilizing the following stepwise approach as previously described. 22 If a variable was considered important and missing in >30% of the study population, a complete case analysis was performed after exclusion of patients with incomplete data from the study cohort. The missForest multiple imputation method was used to impute remaining variables with <30% missing data.11,38 Variables were assumed to be missing at random (MAR) based on epidemiological convention.26,29 We considered both complete-case analysis and imputation for features with missing data and ultimately decided on imputation to reduce bias and improve statistical power 10 ; multiple imputation has been shown to be appropriate for the management of both MAR and missing completely at random data. 43 Confounding among features was controlled through filtering covariates with Spearman correlation coefficients >0.5 according to previously established guidelines. 22
Unsupervised Clustering
After imputation of missing variables, patients were partitioned into clinically distinct subgroups via unsupervised clustering with a random forest algorithm. Clustering is a machine learning technique that produces optimized nonoverlapping regions in the data space based on a specified distance measure. User input into the model in this instance is minimal, without a specified label (hence “unsupervised”). Distinct from supervised machine learning, this technique is often utilized for exploratory analysis, dimensionality reduction, and outlier removal, especially when there are manifold outcomes of interest in the data, such as in the present scenario. An ideal clustering assignment yields distinct subgroups with different likelihoods of achieving an outcome of interest.
Based on previously described methods, a random forest algorithm was leveraged to produce a proximity matrix characterizing the composite distances between each patient in the data space.28,36 The optimal number of clusters and cluster assignments was then determined using partitioning around medoids based on maximization of the average silhouette width (ASW). 16 Briefly, the ASW measures the proportion of the distance between objects in a cluster to the distance between neighboring clusters and can take on values between −1 and 1, with stronger clustering maximizing this number. 20 An ASW >0.7 is considered strong, while values >0.5 are considered acceptable. 25 Variable importance analysis was also performed to identify features that most strongly contributed to algorithm assignment of subgroup membership.
After generation and internal validation of the subgroups, both visual and descriptive comparisons were performed. For visual examination, we performed principal component analysis (PCA) 33 to reduce the >60 features associated with each patient into a 3-dimensional coordinate system that can be plotted. Patients were then plotted in the resulting coordinate system consisting of the 3 principal components with their subgroup labels. Descriptive comparisons between the subgroups were performed using Welch t tests for continuous variables and chi-square analyses for categorical variables.
Targeted Maximum Likelihood Estimation
The treatment effect of ACLR on the primary outcomes of interest was evaluated using TMLE. As previously described, TMLE is a double-robust estimator that can simulate the conditions of a randomized controlled study in noncontrolled observational data, and represents a powerful method to obtain valid statistical inference using machine learning algorithms.44,45 In the absence of level 1 data, traditional methods for outcome regression and treatment assignment (eg, propensity scoring or matched cohort analysis) are reliant on correct causal assumptions regarding the underlying distribution of data. TMLE, however, utilizes a model-free, semiparametric approach through data-adaptive machine learning, which can accommodate high-dimensional data and nonlinear relationships better than classic statistical models, without any additional assumptions. 45 These double-robust methods have been shown to consistently outperform traditional causal estimators, especially given the sparsity of data and weak assumptions about the data distribution.9,31,40 We performed TMLE using a SuperLearner library that compiles the output from a diverse ensemble of algorithms (random forest, extreme gradient boosting, elastic net linear regression, and support vector machines) to approximate the treatment effect of ACLR compared with nonoperative management in each patient subgroup to identify whether these populations are truly clinically distinct.
Preoperative Predictors of Subgroup Membership
Subgroup membership, along with >30 preoperative demographic, comorbidity, and injury variables, was entered into a stepwise multivariable logistic regression to identify any features that may predict patient subgroup membership at the time of ACL injury. This can inform patient counseling and drive surgical indications. The regression model is optimized on the Akaike information criterion, which helps identify the combination of variables that best predict subgroup membership, even though not all individual predictors may show a significant association. Compared with the post hoc variable importance analysis from the clustering analysis, we utilized only preoperative variables in the regression model, which provides odds ratios as outputs to quantify the contribution of specific risk factors to subgroup membership. All statistical tests were 2-tailed, and the statistical difference was established with an alpha <.05.
All modeling and statistical analysis was performed through the R language for programming (Version 4.2.2; R Foundation for Statistical Computing) in RStudio software (Version 1.1.143; Posit).
Results
Population Characteristics
A total of 923 patients with ACL injury were included from the study period; 785 patients (85%) underwent primary ACLR, while 138 patients (15%) underwent nonoperative treatment. The median time to follow-up was 182.9 months (IQR, 123.4-222.9 months) (15.3 years [IQR, 10.3-18.6 years]). The clustering algorithm identified an ideal partition of 2 subgroups. Based on post hoc comparisons, one subgroup of 653 patients (71%) was designated the optimal outcome subgroup, while the other, with 270 patients (29%), was designated the suboptimal outcome subgroup. The overall ASW from the clustering was 0.64 (Figure 2). Visualization of the 2 subgroups in 3-dimensional feature space post-PCA is shown in Figure 2A. The variables identified and assigned importance by the unsupervised clustering algorithm for determining subgroup membership included occupation, age at injury, activity level, concomitant meniscal injury, and sports participation (Figure 2B).
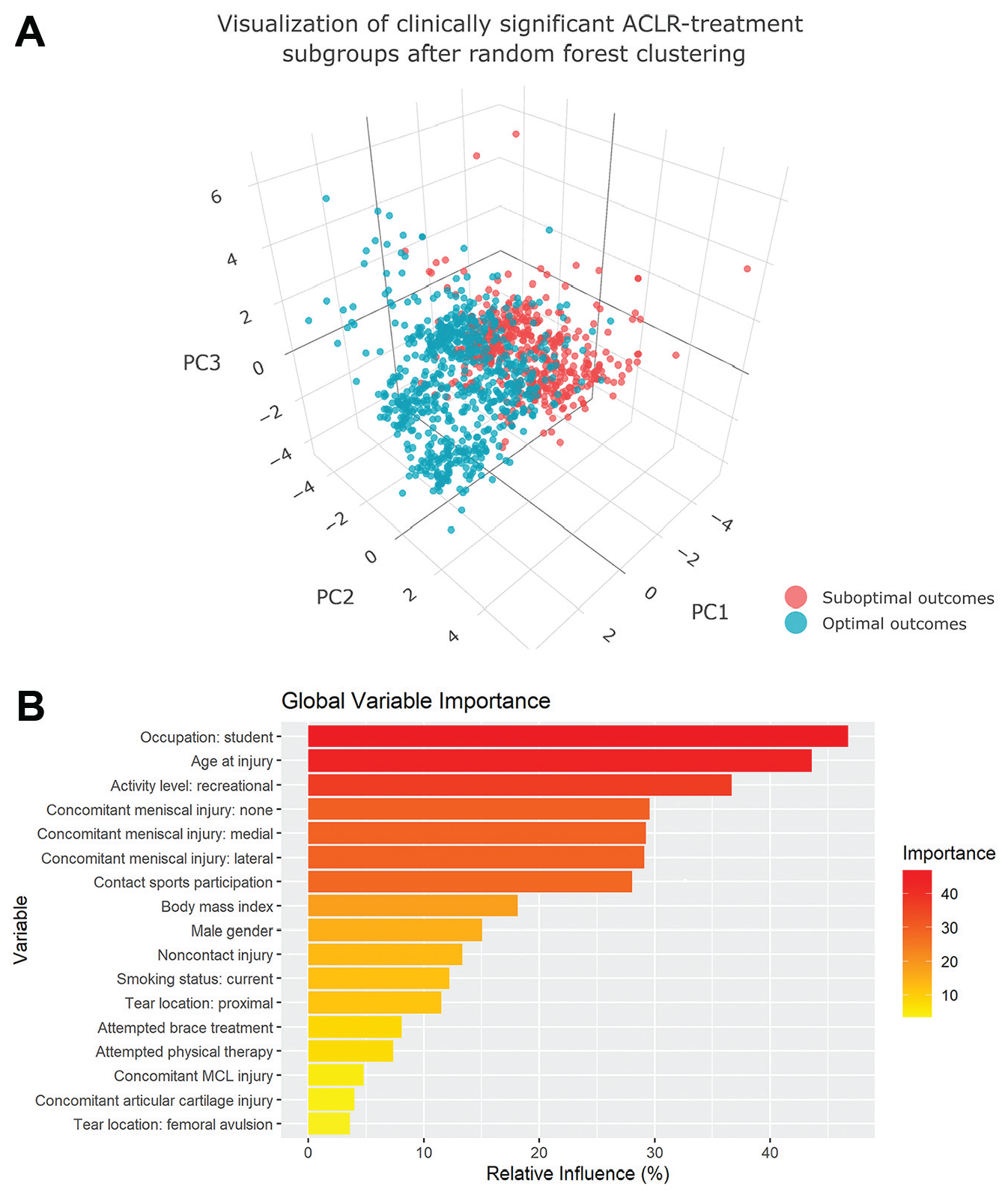
(A) Visualization of the 2 random-forest partitioned patient subgroups in 3-dimensional feature space; the axis is generated following principal component (PC) analysis to reduce the dimensionality of the dataset for ease of visualization. (B) Global variable importance of feature contributions to the performance of the random forest clustering algorithm. ACLR, anterior cruciate ligament reconstruction; MCL, medial collateral ligament.
Table 1 summarizes the baseline demographic and injury characteristics of patients in the optimal and suboptimal outcome subgroups. Compared with the optimal outcome subgroup, patients in the suboptimal outcome subgroup were characterized by significantly older age (35.0 ± 10.1 years vs 26.0 ± 10.2 years; P < .001), greater BMI (30.5 ± 5.5 kg/m2 vs 26.5 ± 4.3 kg/m2; P < .001), higher proportion of former (12% vs 4%) and current (24% vs 12%) smokers (P < .001), higher proportion of patients with diabetes (3% vs 0.5%; P = .001), and higher proportion of patients with systemic inflammatory disease (4% vs 1%; P = .015). Furthermore, the optimal outcome subgroup had a significantly higher percentage of students (42% vs 3%) and a lower percentage of laborers (17% vs 58%) (P < .001). In terms of activity level, there were more competitive (29% vs 5%) and recreational (70% vs 57%) athletes in the optimal outcome subgroup and fewer sedentary individuals (1% vs 37%) (P < .001). A significantly higher percentage of the optimal outcome subgroup participated in collision (9% vs 5%), contact (41% vs 8%), and noncontact sports (9% vs 6%) (all P < .001).
Comparison of injury characteristics showed no significant difference in the percentage of injury due to a noncontact mechanism in each group (optimal 83% vs suboptimal 80%; P = .482). The location of ACL tears was also significantly different, particularly for midsubstance tears (optimal 79% vs suboptimal 28%) and proximal tears (optimal 16% vs suboptimal 67%) (P < .001). Characterization of concomitant meniscal injury showed significant differences, with the optimal outcome subgroup having a higher percentage of no concomitant meniscal injury (39% vs 19%) and a lower percentage of medial meniscus injury (26% vs 17%) (P < .001). No significant differences were found for rates of nonoperatively treated concomitant ligamentous injury: posterior cruciate ligament (both 1%; P = .457), medial collateral ligament (optimal 15%, suboptimal 22%; P = .906), lateral collateral ligament (optimal 5%, suboptimal 4%; P = .63), and posterolateral corner (both 3%; P > .99).
On initial clinical presentation, the suboptimal outcome subgroup exhibited a significantly higher visual analog scale pain score (5.5 vs 3.0; P < .001). On physical examination, the suboptimal outcome subgroup had higher percentages of follow-up positive Lachman (31% vs 11%), positive pivot-shift (30% vs 11%), and positive anterior drawer (29% vs 11%) tests (all P < .001). Comparing treatment courses, the suboptimal group had significantly higher rates of aspiration or injection (12% vs 5%; P < .001) and bracing (81% vs 51%; P < .001), but lower rates of ACLR (69% vs 90%; P < .001). There was no difference in rates of physical therapy between the groups (optimal 81% vs suboptimal 85%; P = .22).
Differences Between Patients Who Underwent ACLR in the Optimal Outcome and Suboptimal Outcome Subgroups
Table 2 displays surgical characteristics and intraoperative findings for patients who underwent ACLR in each of the 2 subgroups. Among 653 patients in the optimal outcome subgroup, 590 (90%) underwent ACLR. Of the 270 patients with suboptimal outcomes, 195 (72%) underwent ACLR. Significantly fewer allografts (16% vs 29%) and more hamstring autografts (15% vs 11%) were used for graft type in the optimal outcome subgroup (P < .001). The most common graft type used across both groups was bone–patellar tendon–bone (BTB) autograft, comprising 69% of the optimal outcome subgroup and 60% of the suboptimal outcome subgroup. With respect to femoral fixation, both subgroups had similar rates of direct compression (optimal 77% vs suboptimal 77%), expansion (optimal 6% vs suboptimal 11%), and suspension (optimal 17% vs suboptimal 13%) (P = .058). For tibial fixation, the optimal group had higher rates of direct compression (optimal 88% vs suboptimal 79%), similar rates of suspension (optimal 5% vs suboptimal 4%), and lower rates of expansion (optimal 7% vs suboptimal 17%) (P < .001). The percentage of concomitant meniscectomies was significantly decreased in the optimal outcome subgroup (65% vs 53%; P = .004), but there were similar percentages of concomitant meniscal repairs (optimal 83% vs suboptimal 77%; P = .088).
Comparison of Surgical Characteristics and Intraoperative Findings Stratified by Subgroup Membership a
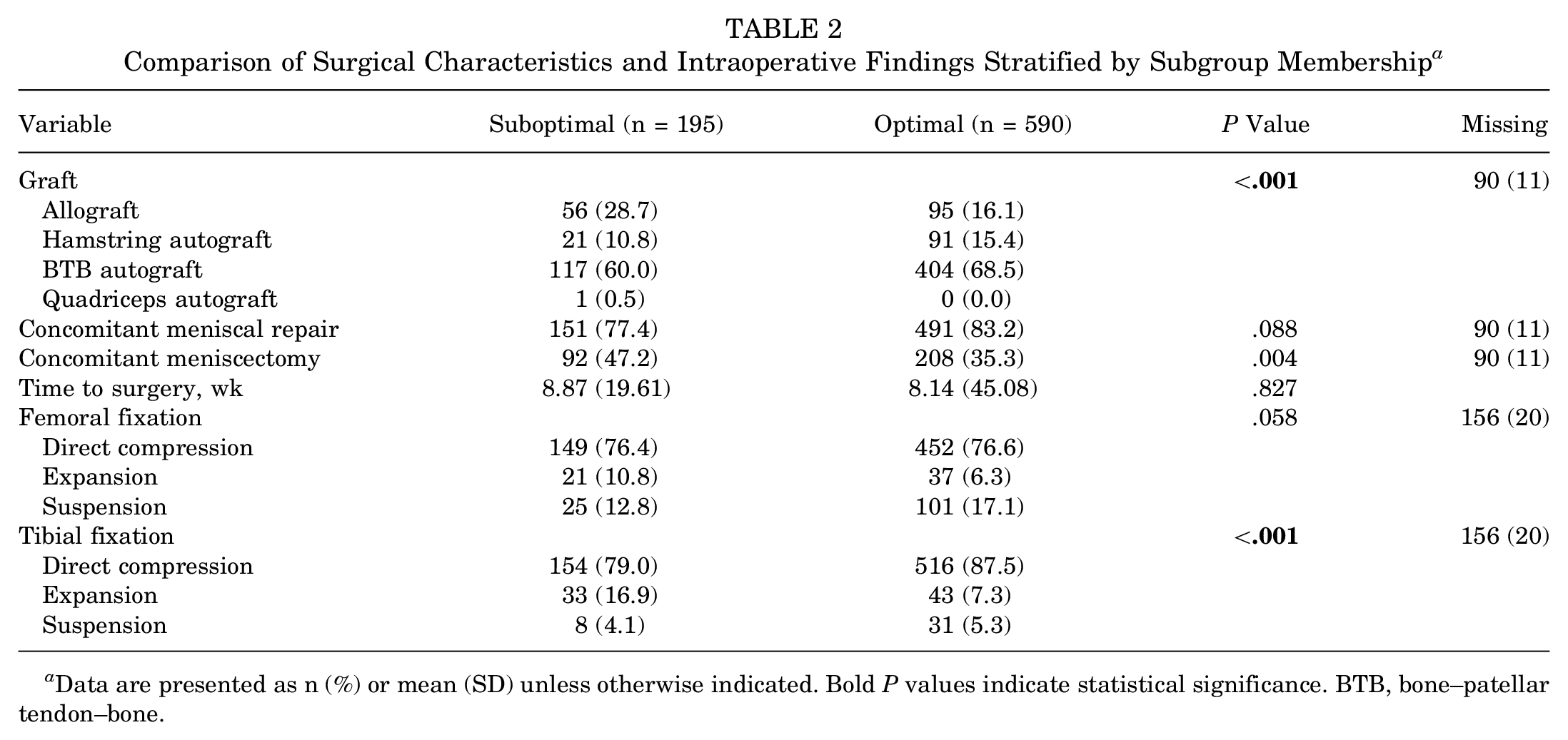
Data are presented as n (%) or mean (SD) unless otherwise indicated. Bold P values indicate statistical significance. BTB, bone–patellar tendon–bone.
Treatment Effect of ACLR on Outcomes for Optimal Outcome and Suboptimal Outcome Subgroups
The treatment effects of ACLR on the primary outcomes of interest in both subgroups are provided in Table 3. In the optimal outcome subgroup, ACLR demonstrated a significantly protective effect on the risk of secondary meniscal injury (average treatment effect [ATE], 61.0%; 95% CI, 59%-63%; OR, 0.06; 95% CI, 0.05-0.07; P < .01), contralateral ACL injury (ATE, 8.0%; 95% CI, 5%-10%; OR, 0.17; 95% CI, 0.07-0.42; P < .01), development of PTOA (ATE, 16%; 95% CI, 13%-19%; OR, 0.39; 95% CI, 0.31-0.47; P < .01), and progression to TKA (ATE, 6.0%; 95% CI, 5%-7%; OR, 0.05; 95% CI, 0.01-0.18; P < .01). In the suboptimal outcome subgroup, ACLR had a protective effect against the development of PTOA (ATE, 11%; 95% CI, 4%-17%; OR, 0.65; 95% CI, 0.5-0.85; P < .01) and progression to TKA (ATE, 8%; 95% CI, 4%-12%; OR, 0.48; 95% CI, 0.33-0.71; P < .01), but exerted no treatment effect on the risk of secondary meniscal injury or contralateral ACL injury.
Treatment Effect of ACL Reconstruction on Subgroup Outcomes via TMLE a
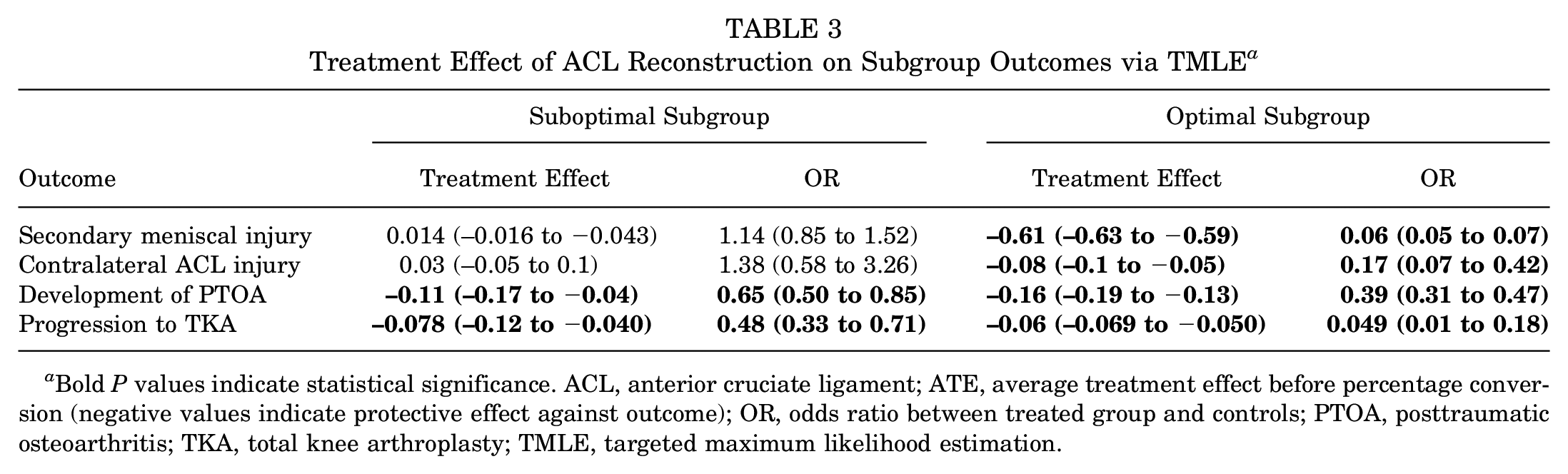
Bold P values indicate statistical significance. ACL, anterior cruciate ligament; ATE, average treatment effect before percentage conversion (negative values indicate protective effect against outcome); OR, odds ratio between treated group and controls; PTOA, posttraumatic osteoarthritis; TKA, total knee arthroplasty; TMLE, targeted maximum likelihood estimation.
Significant Predictors of Membership in the Optimal Outcome Subgroup
Table 4 outlines predictors of membership in the optimal outcome subgroup using a multivariable stepwise regression model. Based on this analysis of retrospectively collected data, positive predictors of a patient being in the optimal outcome subgroup include student occupation (OR, 5.86; 95% CI, 2.66-12.88; P < .001), sports participation (OR, 8.71; 95% CI, 4.7-16.14; P < .002), and noncontact injury mechanism (OR, 1.77; 95% CI, 1.17-4.29; P < .001), whereas negative predictors of optimal outcome subgroup membership include older age at injury (OR, 0.89; 95% CI, 0.87-0.92; P < .001) or greater BMI (OR, 0.82; 95% CI, 0.78-0.86; P < .001). Regarding injury characteristics, concomitant injury to either the medial meniscus (OR, 0.07; 95% CI, 0.04-0.13; P < .001) or both the medial and lateral menisci (OR, 0.51; 95% CI, 0.28-0.93; P < .001) was a negative predictor of membership in the optimal outcome subgroup.
Predictors of Optimal Cluster Membership on Multivariable Stepwise Regression Model a
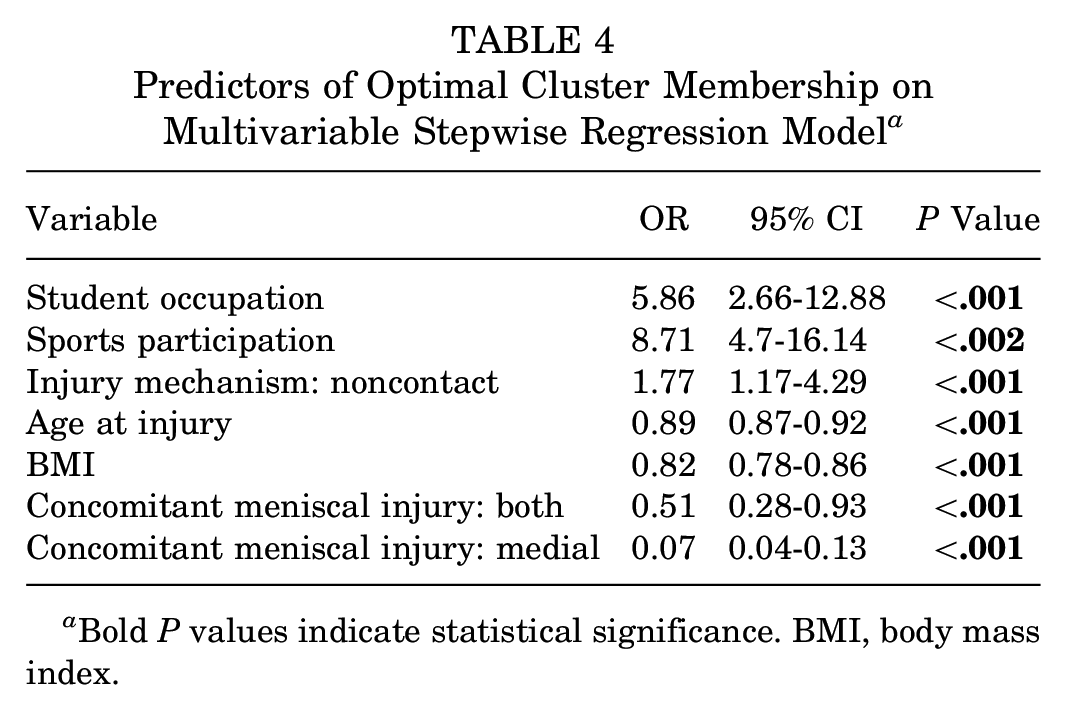
Bold P values indicate statistical significance. BMI, body mass index.
Discussion
This study identified 2 clinically meaningful patient subgroups with differential treatment responses to ACLR. Furthermore, while ACLR had a significant treatment effect on secondary meniscal injury and contralateral ACL disruption in the optimal subgroup only, it reduced the development of PTOA in all-comers. Finally, significant predictors for membership in the suboptimal subgroup included older age, greater BMI, and the presence of either a medial or bicompartmental meniscal injury, whereas sports participation, noncontact injury mechanism, and student occupation predicted membership in the optimal subgroup.
The epidemiology and predictors of PTOA after ACL injury are the subject of significant investigation, and despite advances in surgical technique, the treatment effect of reconstruction on preventing or delaying PTOA remains inconclusive. A recent systematic review with meta-regression identified a pooled PTOA incidence of 37.9% after reconstruction compared with 40.5% after nonoperative treatment, 21 while another meta-analysis of 29 studies, all with at least 10 years of follow-up, reported no significant difference in the radiographic progression of arthritis between patients undergoing ACLR and those treated nonoperatively. 1 They did report, however, that patients who underwent ACLR experienced fewer subsequent meniscal injuries. 47 Ferrero et al 6 conducted a meta-analysis exclusively of randomized controlled trials (RCTs) comparing ACLR with nonoperative treatment and reported a higher risk of osteoarthritis development after ACLR. However, the analysis was limited to only 3 studies, and the authors emphasized the need for further research. 6 In contrast, other studies suggested a protective role of ACLR in preventing PTOA.24,35 Interestingly, more substantial evidence exists for the protective effect of ACLR against secondary meniscal injury, likely because of the shorter follow-up needed.5,32 Given this as well as the increasingly apparent role of meniscal status on the natural history of the knee, 12 the protective effect of ACLR against PTOA in certain patient subgroups may be a foregone conclusion. Furthermore, RCTs directly comparing ACLR with nonoperative management are sparse. Frobell et al 7 compared early ACLR combined with structured rehabilitation to structured rehabilitation alone (with the option of delayed ACLR) and found no significant differences in radiographic PTOA at the 5-year follow-up. Similarly, Tsoukas et al 41 observed no differences in radiographic PTOA at the 10-year follow-up in a smaller RCT. Our study demonstrated that while clinically meaningful and distinct subgroups exist among ACL patients, ACLR exerted a significantly protective effect against the development of PTOA in both subgroups. This is likely consistent with the aforementioned protective effect of reconstruction on secondary meniscal injury evident from recent literature, 13 due to both the opportunity to arthroscopically identify and repair occult tears that escape detection on advanced imaging and the effect of restoring overall knee stability on future meniscal stress.
Regression analysis of preoperative predictors of subgroup membership identified student occupation and noncontact injury to increase a patient's likelihood of being in the optimal subgroup, whereas advanced age, greater BMI, and concomitant meniscal injury negatively predicted optimal subgroup membership. We hypothesize that student occupation may lead to improved outcomes due to younger patient age at injury and, moreover, an unidentified effect likely related to patient motivation and resilience.37,49 The detrimental effect of demographic factors including advanced age, greater BMI, and injury characteristics such as concomitant meniscal pathology in exacerbating progressive knee degeneration after ACL disruption has been well documented.12,13,19 Both North American and European series have highlighted meniscal injury requiring surgical intervention (eg, meniscectomy or repair) as a significant risk factor for the development of PTOA.13,19 Lindanger et al 19 further stratified outcomes based on the compartment and found the risk to be near equivalent for lateral and medial meniscus injuries. Interestingly, the present data found isolated medial meniscus injuries to portend a greater risk of suboptimal outcomes compared with concomitant medial- and lateral-sided injuries. A possible explanation is the differences in patterns of meniscal injury as well as the repairability of tissue. Isolated medial-sided tears are more commonly degenerative in nature and associated with chronic ACL deficiency 2 ; conversely, concomitant bicompartmental meniscal pathology is more likely to be traumatic in nature and frequently represent medial meniscocapsular injuries with associated lateral meniscus tears, 17 and it may be more amenable to repair when identified. More granular data regarding the pattern of concomitant meniscal injury and management (resection vs repair) is crucial to further understanding PTOA after ACLR.
Our findings have interesting potential implications for patient selection and counseling. The benefits of reconstruction in patients within the optimal subgroup are consistent with the existing literature. These patients can be counseled that reconstruction can exert a significant treatment effect on future risk of meniscal injury, contralateral ACL disruption, and PTOA. Interestingly, while ACLR had no effect on the risk of secondary meniscal injury or contralateral ACL disruption for patients in the suboptimal subgroup, there remained a significant reduction in the risk of PTOA. While the importance of meniscal health on preventing the development of PTOA after ACL disruption cannot be understated, it is possible that despite the low repairability of degenerative meniscal tissue among those in the suboptimal subgroup, restoration of knee stability through ACLR can have a positive influence on the natural history of the knee. Indeed, there is some evidence to suggest that limited meniscectomy does not significantly alter tibiofemoral biomechanics in patients with irreparable meniscal tears who undergo isolated ACLR. 39 Overall, the findings of this study support ACLR not only for patients with a high likelihood of optimal outcomes (eg, younger, thinner patients with nonsedentary occupation or sports participation), but also for those in the suboptimal subgroup to mitigate the development of PTOA.
Limitations
This study has several limitations. First, given the retrospective nature of this study and the lengthy study period in question, heterogeneity in indications, surgical techniques (tunnel placement, drilling technique, graft size, etc), and rehabilitation is unavoidable; this includes evolution in the treatment of partial ACL injuries, nonoperative management of concomitant collateral or cruciate ligament injuries, and surgical management of concomitant meniscal injury. However, the patient subgroups are not temporally distinct based on length of follow-up, and additional steps were undertaken to methodologically mitigate confounding through both techniques in feature selection and targeted learning. Second, we did not have granular data on variables such as patient-reported outcomes or specific Kellgren-Lawrence grading of pre- or postoperative radiographic osteoarthritis, which can help more clearly establish disease baseline and progression. However, the outcomes reported in the present study, such as risk of secondary meniscal injury or contralateral ACL injury, may serve as meaningful surrogates. Third, while we set the minimum follow-up to 90 months to appropriately capture the mid- to long-term outcomes of PTOA, this criterion may potentially lead to the exclusion of patients who benefited from nonoperative treatment, as they are less likely to seek follow-up treatment if asymptomatic. Furthermore, data-adaptive algorithms have been criticized in specific use cases for biased identifications of patterns based on small perturbations that may be random due to positive feedback loops, although overfitting is relatively rare given the inborn mitigation strategies of TMLE such as ensemble learning and data augmentation. 48 Lastly, this study's conclusions are based on patient data queried from a single geographic registry, and care should be taken when applying findings to other populations, and while the study cohort included a large number of ACLRs, an increase in the sample size may help the model yield further insights.
Conclusion
Two clinically meaningful subgroups were identified from retrospectively collected data and found to experience differential treatment responses after ACL injuries. ACLR decreased the rate of development of PTOA and TKA in both subgroups but was not as effective in preventing secondary meniscal injuries or contralateral ACL injuries in patients who were older, heavier, or had concomitant medial meniscus injuries.
Footnotes
Submitted February 10, 2025; accepted June 12, 2025.
One or more of the authors has declared the following potential conflict of interest or source of funding: M.H. has received consulting fees from DJO/Enovis, Moximed, and Vericel. K.R.O. has received consulting fees from Arthrex and Smith & Nephew. D.B.F.S. has received support for professional activities from Relive Biotechnologies. A.J.K. has received consulting fees from Arthrex and research support from Aesculap/B. Braun. C.L.C. has received consulting fees from Arthrex, research support from Major League Baseball, publishing royalties and other financial support from Springer, and other fees from Zimmer Biomet Holdings and Gemini Medical. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.