
Abstract
Background:
Anterior cruciate ligament (ACL) injuries are common, and ACL reconstruction (ACLR) restores stability and enables return to sport. To date, however, studies have failed to show that ACLR prevents long-term osteoarthritis, but the role of timing of ACLR in osteoarthritis has not been extensively examined in meta-analyses.
Purpose:
To compare the risk of long-term osteoarthritis after early versus delayed ACLR in the literature.
Study Design:
Systematic review and meta-analysis; Level of evidence, 4.
Methods:
The PubMed, Embase, and Cochrane Library databases were searched from 2000 to August 2024 for studies comparing osteoarthritis between early and delayed ACLR at a minimum 5-year follow-up. Outcomes are reported as risk reduction with 95% confidence interval for osteoarthritis incidence, and odds ratio with 95% confidence interval for difference in time from injury to surgery. Random-effects models were used.
Results:
Seventeen studies (3953 ACLRs) were included (mean age, 28.8 years; 67% male; mean follow-up, 13.3 years; 52% meniscectomy; 31% osteoarthritis incidence). The quality of the studies was rated as moderate, with a Methodological Index for Non-Randomized Studies score of 78% of maximum. Overall, earlier ACLR led to a 10% reduction in osteoarthritis compared with delayed ACLR (95% CI, 6%-14%; P < .001). Two studies (1474 patients) reported a 6% incidence reduction when ACLR was performed within versus after 1 month (95% CI, 2%-10%; P = .005). Similarly, 4 studies (349 patients) reported a 16% incidence reduction when ACLR was performed within versus after 6 months (95% CI, 5%-26%; P = .004), and 5 studies (2248 patients) showed a 13% osteoarthritis reduction with ACLR within versus after 12 months (95% CI, 6%-20%; P = .003). Six studies (685 patients) reported that patients without osteoarthritis were operated on a mean 15 months earlier than patients who developed osteoarthritis (95% CI, 2-29 months; P = .03).
Conclusion:
This systematic review with a 5-year minimum follow-up demonstrates that shorter time from injury to ACLR was associated with a decreased incidence of long-term osteoarthritis. This reduced risk was already seen when surgery was performed within 1 month but most pronounced within 6 months and 12 months.
Anterior cruciate ligament (ACL) injuries are common injuries with an estimated incidence between 37 and 79 per 100,000 person-years, corresponding to approximately 200,000 new injuries in the United States annually.30,37,54 ACL injuries can be either treated nonoperatively with potential delayed ACL reconstruction (ACLR) or addressed with direct (early) ACLR.28,41,48,49 Proponents of initial nonoperative treatment state that some patients might be copers and surgery is not required for all patients,29,41,48 whereas others have advocated that delayed ACLR leads to increased rates of intra-articular damage that might have consequences at long-term follow-up. Delaying surgery beyond 3 months has been shown to lead to increased meniscal tears,17,34,48 increased cartilage damage,33,34,42 and decreased repairability of meniscal tears. 43
Based on these studies and on the findings that meniscectomy at the time of ACLR increases the rates of osteoarthritis,5,54 one would expect that early ACLR would lead to decreased rates of osteoarthritis, but data in the literature are conflicting.4,7,51 Most of these studies have focused on comparing early ACLR with nonoperative treatment and potential delayed surgery1,7,14,40,50,55 and drawn conclusions based on this comparison. However, no systematic reviews or meta-analyses have specifically focused on the role of timing of surgery in the incidence of osteoarthritis when focusing on comparative studies.4,28,55
The goal of this study was therefore to assess the role of timing of ACLR in the incidence of osteoarthritis in the literature using comparative studies at a minimum 5-year follow-up. We hypothesized that ACLR within 3 months would lead to lower rates of osteoarthritis compared with delayed ACLR due to the increased risk of meniscal and cartilage damage from this time point.34,42,43,48
Methods
The PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines were used for this systematic review and meta-analysis, and the study was registered in PROSPERO (CRD42024584908). There was no funding or conflict of interest for this study.
Literature Search
A systematic search in the electronic databases of PubMed, Embase, and Cochrane Library for studies assessing the role of timing of ACLR in osteoarthritis was performed in August 2024. Search terms included “(anterior cruciate ligament OR ACL) AND (reconstruction OR repair) AND osteoarthritis AND (early OR delayed OR timing OR acute OR late).” The titles and abstracts of all identified studies were first assessed for potential inclusion, and then the full texts were reviewed for the inclusion and exclusion criteria by 2 reviewers (J.P.V.D.L. and C.M.) independently. In addition, potentially relevant references of the included studies were reviewed for inclusion, along with the references of all included studies in recent systematic reviews on general osteoarthritis after ACLR.4,28,50 Ultimately, agreement for inclusion was reached for all studies, and a third reviewer was not required.
Inclusion criteria consisted of studies (1) reporting on radiographic osteoarthritis after single-bundle ACLR; (2) reporting the incidence of radiographic osteoarthritis in early versus delayed ACLR, or time from injury to surgery in patients who ultimately did or did not develop radiographic osteoarthritis after ACLR; (3) published since 2000; and (4) with a minimum mean follow-up of 5 years. Exclusion criteria consisted of (1) concomitant bony procedures (eg, high tibial osteotomy, distal femoral osteotomy, and slope correction osteotomy); (2) concomitant ligament reconstruction procedures (ie, multiligamentous knee injuries); (3) case reports, animal studies, reviews, or biomechanical studies; and (4) non–English-language studies (Table 1). All studies were reviewed for authors, institution, and citations to assess duplicate studies, and if multiple studies of the same cohort were available, studies with the longest follow-up were used.10,29
Description of Included Studies a
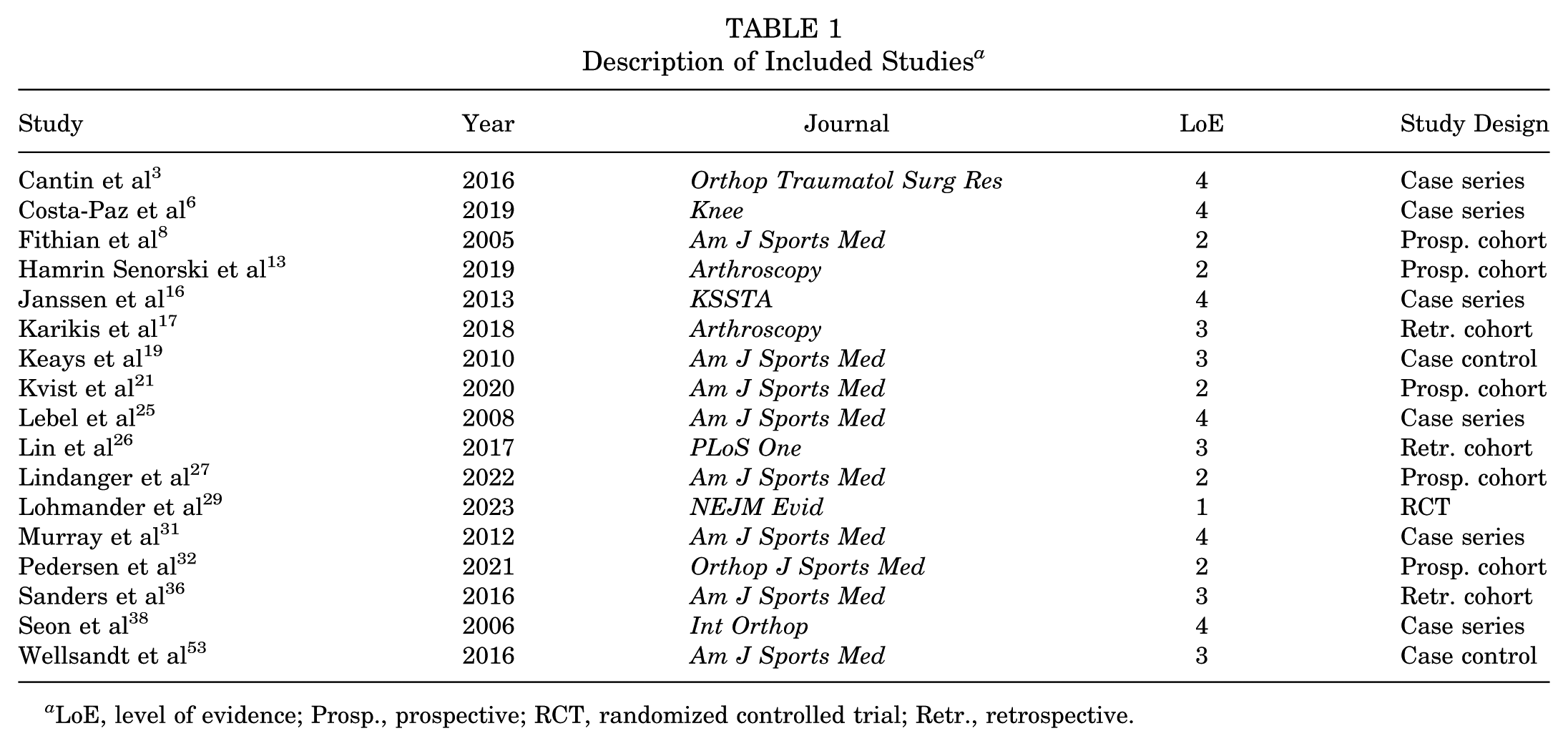
LoE, level of evidence; Prosp., prospective; RCT, randomized controlled trial; Retr., retrospective.
Quality Assessment
The level of evidence of included studies was graded using the adjusted Oxford Centre for Evidence-Based Medicine. 58 The Methodological Index for Non-Randomized Studies (MINORS) criteria were used to assess the methodological quality of studies. 39 The first 8 criteria were used for all studies, and all 12 criteria were used for comparative studies (Table 2). The Cochrane risk-of-bias tool for randomized trials Version 2 (RoB 2) was used for randomized controlled trials (RCTs). 44 Finally, the Grading of Recommendations Assessment, Development and Evaluation (GRADE) approach was used to grade quality of evidence. 11 Funnel plot analysis (RevMan Version 5.4; The Cochrane Collaboration) was performed to assess for potential publication bias.
Quality Assessment of the Included Studies Using the MINORS Criteria
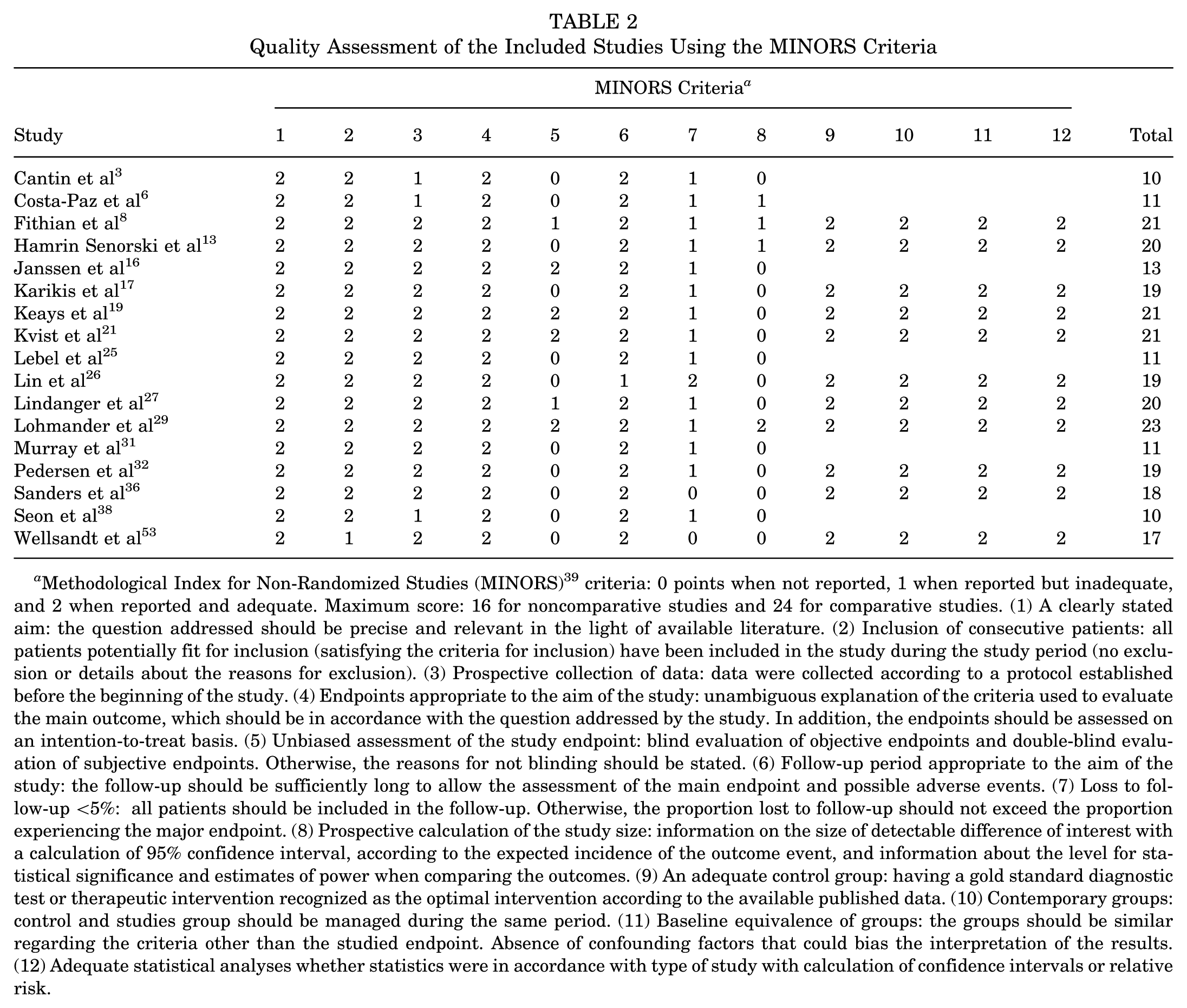
Methodological Index for Non-Randomized Studies (MINORS) 39 criteria: 0 points when not reported, 1 when reported but inadequate, and 2 when reported and adequate. Maximum score: 16 for noncomparative studies and 24 for comparative studies. (1) A clearly stated aim: the question addressed should be precise and relevant in the light of available literature. (2) Inclusion of consecutive patients: all patients potentially fit for inclusion (satisfying the criteria for inclusion) have been included in the study during the study period (no exclusion or details about the reasons for exclusion). (3) Prospective collection of data: data were collected according to a protocol established before the beginning of the study. (4) Endpoints appropriate to the aim of the study: unambiguous explanation of the criteria used to evaluate the main outcome, which should be in accordance with the question addressed by the study. In addition, the endpoints should be assessed on an intention-to-treat basis. (5) Unbiased assessment of the study endpoint: blind evaluation of objective endpoints and double-blind evaluation of subjective endpoints. Otherwise, the reasons for not blinding should be stated. (6) Follow-up period appropriate to the aim of the study: the follow-up should be sufficiently long to allow the assessment of the main endpoint and possible adverse events. (7) Loss to follow-up <5%: all patients should be included in the follow-up. Otherwise, the proportion lost to follow-up should not exceed the proportion experiencing the major endpoint. (8) Prospective calculation of the study size: information on the size of detectable difference of interest with a calculation of 95% confidence interval, according to the expected incidence of the outcome event, and information about the level for statistical significance and estimates of power when comparing the outcomes. (9) An adequate control group: having a gold standard diagnostic test or therapeutic intervention recognized as the optimal intervention according to the available published data. (10) Contemporary groups: control and studies group should be managed during the same period. (11) Baseline equivalence of groups: the groups should be similar regarding the criteria other than the studied endpoint. Absence of confounding factors that could bias the interpretation of the results. (12) Adequate statistical analyses whether statistics were in accordance with type of study with calculation of confidence intervals or relative risk.
Data Collection
Excel (Microsoft Corp) was used to collect the extracted data. Baseline data consisted of author names, year of publication, journal, number of patients and knees, age at procedure, length of follow-up (years), sex, type of graft used, percentage of meniscectomies performed, and overall incidence of osteoarthritis (Table 3). In case medians and ranges were reported, means and standard deviations were calculated using previously validated methods.15,52 The primary analysis involved the assessment of the incidence of osteoarthritis in patients operated on within versus after a certain time threshold (eg, within vs after 3 months). If studies were eligible for multiple time thresholds (eg, 3 months and 6 months), the study was included for all subgroup analyses but was only included once for the overall analysis. The secondary analysis involved the comparison of the time from injury to surgery between patients who did develop versus did not develop osteoarthritis at the final follow-up.
Baseline Characteristics of the Included Studies a
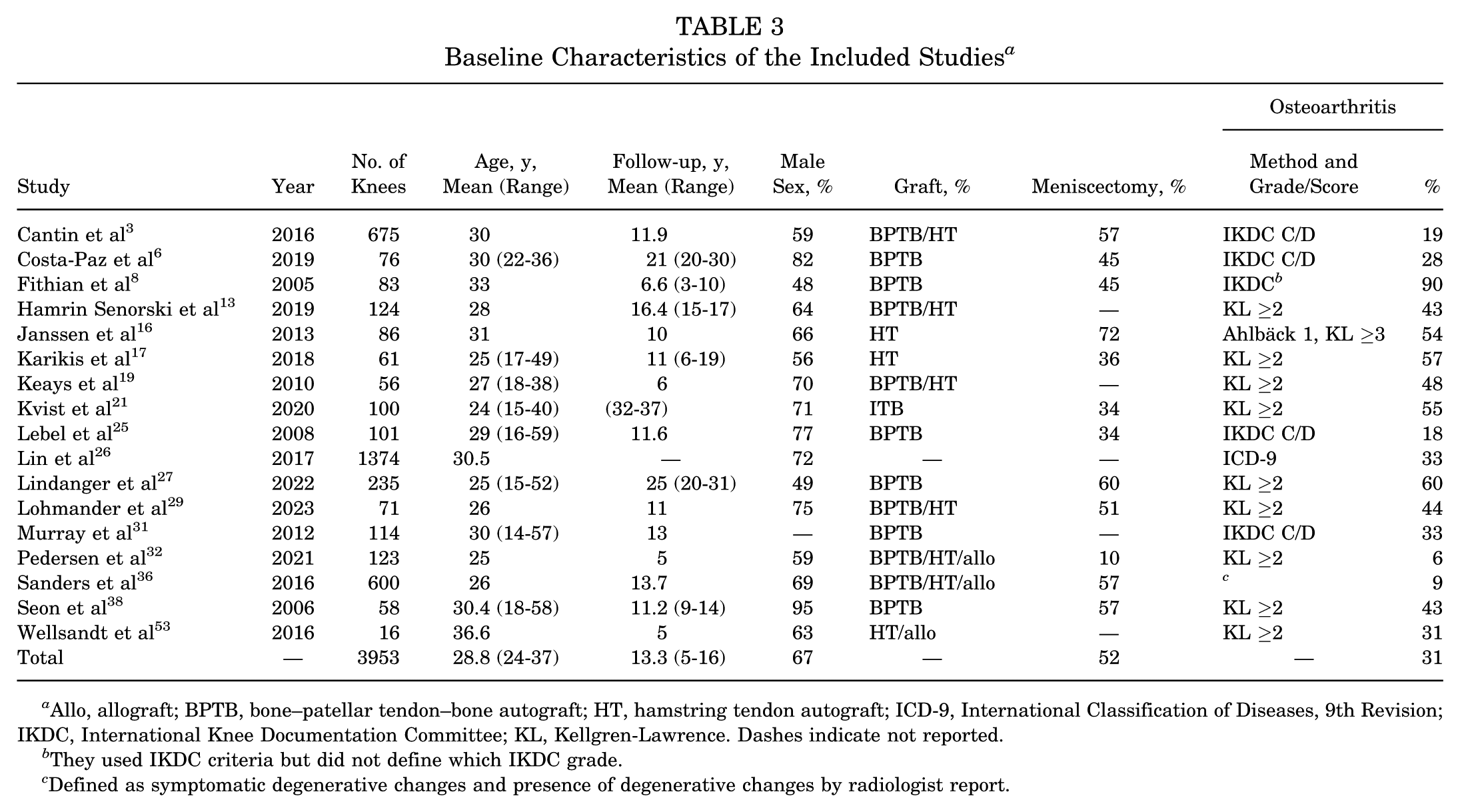
Allo, allograft; BPTB, bone–patellar tendon–bone autograft; HT, hamstring tendon autograft; ICD-9, International Classification of Diseases, 9th Revision; IKDC, International Knee Documentation Committee; KL, Kellgren-Lawrence. Dashes indicate not reported.
They used IKDC criteria but did not define which IKDC grade.
Defined as symptomatic degenerative changes and presence of degenerative changes by radiologist report.
Equity, Diversity, and Inclusion Statement
The author group consists of junior, midcareer, and senior researchers. Members of the author group are from different continents. Our study population included both male and female patients, although further specification of patient characteristics could not be made due to the study design of a systematic review and meta-analysis.
Statistical Analysis
RevMan Version 5.4 was used for the meta-analysis. Forest plots with random-effects models were used, and data are presented as risk reduction with 95% confidence interval and as odds ratio with 95% confidence interval to report differences between the timing groups. Forest plots with random-effects models, presented as mean difference (MD) with 95% confidence interval, were used to assess the differences in time from injury to surgery in the cohorts that did or did not develop osteoarthritis after ACLR. A P value <.05 was considered statistically significant.
Results
Study Selection
After removal of duplicates, 1621 titles and abstracts were reviewed, and 101 studies were reviewed for their full text. Ultimately, 17 studies fulfilled the criteria and were included,3,6,8,13,16,17,19,21,25-27,29,31,32,36,38,53 of which 12 studies reported the incidence of osteoarthritis in early versus delayed groups6,8,13,17,21,25,26,29,31,32,36,38 and 6 studies reported the time from injury to surgery in cohorts that ultimately did develop versus did not develop osteoarthritis3,16,19,25,27,53 (Figure 1).
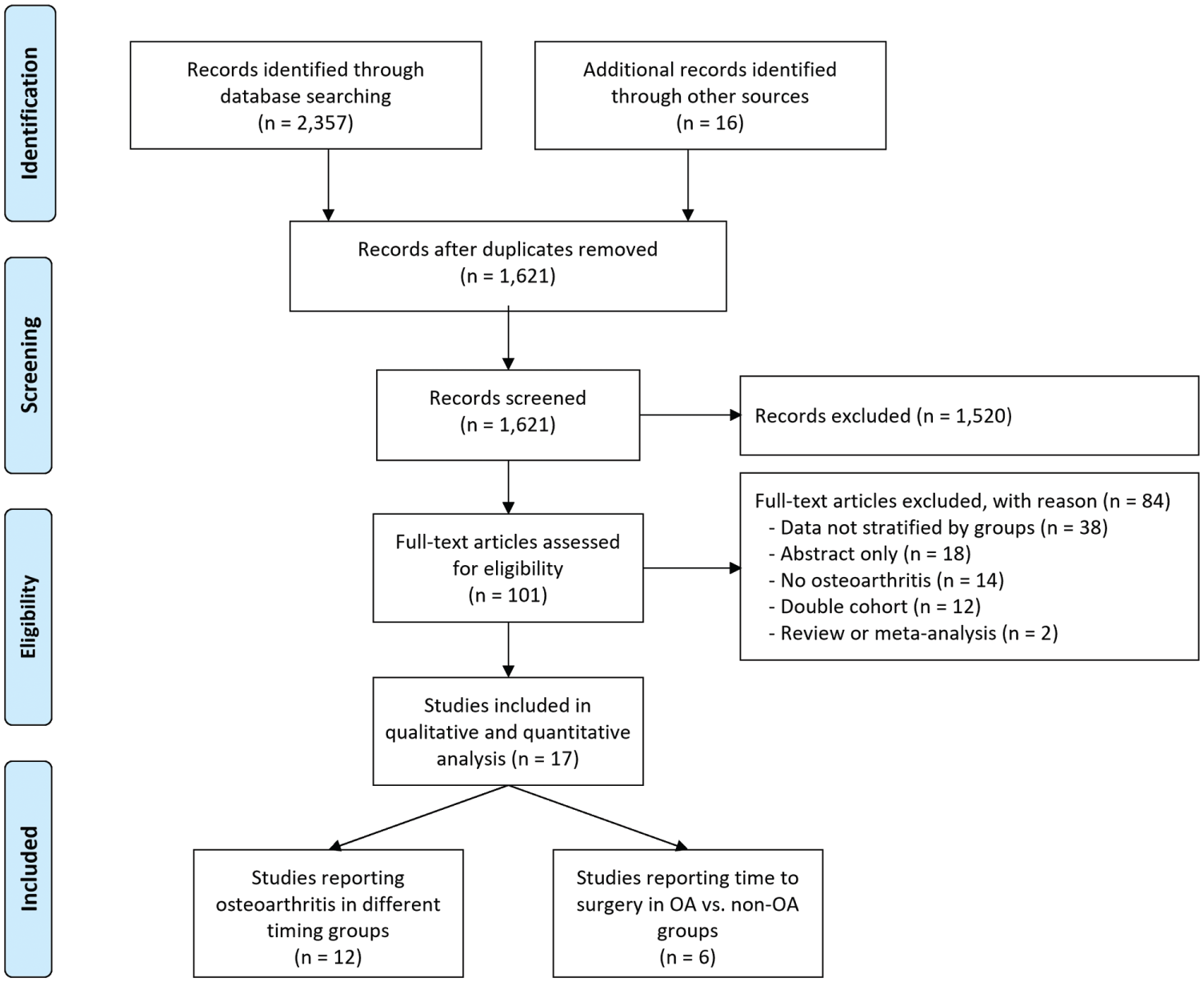
PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) flow diagram of study selection. OA, osteoarthritis.
Quality of Studies
One study consisted of level 1 evidence 29 ; 5 studies, level 2 evidence8,13,21,27,32; 5 studies, level 3 evidence17,19,26,36,53; and 6 studies, level 4 evidence.3,6,16,25,31,38 For noncomparative studies, the MINORS criteria score averaged 69% of the maximum score, and for comparative studies 83% (Table 2). The RoB 2 revealed a low risk of bias for the RCT study. 29 The level of evidence according to GRADE was classified as moderate. Funnel plot analysis showed that no large publication bias was present in this study (Figure 2).

Funnel plot analysis enables visual inspection and shows no large publication bias in the included studies.
Baseline Characteristics
The 17 studies included 3953 ACLR procedures. Patients had a mean age of 28.8 years (range, 24-47 years), and 67% of patients were male. The mean follow-up was 13.3 years (range, 5-16 years). Meniscectomies were reported to be performed in 52% (range, 10%-72%) of cases, and the overall incidence of osteoarthritis (regardless of timing) was 31% (range, 6%-60%), with 1 outlier reporting a 90% incidence of osteoarthritis at 6.6 years of follow-up without defining how osteoarthritis was graded 8 (Table 3).
Timing and Osteoarthritis
Two studies (1474 patients) reported on the incidence of osteoarthritis when performing ACLR within versus after 1 month and noted a reduced incidence of osteoarthritis of 6% (95% CI, 2% to 10%; OR, 0.69; 95% CI, 0.54 to 0.89; P = .005). Three studies (274 patients) compared the incidence of osteoarthritis when performing ACLR within versus after 2.5 months and no significant reduction in osteoarthritis was noted with earlier surgery (RD, 7%; 95% CI, –5% to 18%; OR, 0.75; 95% CI, 0.45 to 1.26; P = .28). Four studies (343 patients) also found no significant difference when surgery was performed within 3 months compared with after 3 months (RD, 1%; 95% CI, –14% to 17%; OR, 0.98; 95% CI, 0.41 to 2.35; P = .97). Sensitivity analysis at 3 months was performed with the exclusion of the outlier study by Fithian et al 8 that reported a 90% osteoarthritis incidence at a 6.6-year follow-up, and 3 studies (250 patients) also showed no significant reduction in osteoarthritis when surgery was performed within 3 months (RD, 9%; 95% CI, –2% to 20%; OR, 0.65; 95% CI, 0.38 to 1.12; P = .12).
Four studies (349 patients) showed a significant reduction of 16% in long-term osteoarthritis when ACLR was performed within 6 months of injury compared with after 6 months (95% CI, 5% to 26%; OR, 0.44; 95% CI, 0.25 to 0.77; P = .004). Similarly, 5 studies (2248 patients) showed that performing ACLR within 12 months led to a 13% reduction in osteoarthritis when compared with ACLR after 12 months (95% CI, 6% to 20%; OR, 0.39; 95% CI, 0.21 to 0.72; P = .003). One study (58 patients) showed no statistically significant difference between surgery within 24 months compared with after 24 months after injury (RD, 17%; 95% CI, –7% to 42%; OR, 0.47; 95% CI, 0.16 to 1.40; P = .18), although the statistical analysis within the study itself found a significant difference between the groups (P < .01). 17 One study (1374 patients) showed a significant reduction in osteoarthritis when surgery was performed within 36 months of injury compared with after 36 months of injury (RD, 14%; 95% CI, 4% to 24%; OR, 0.47; 95% CI, 0.29 to 0.77; P = .002). When combining all time thresholds and only including each study once, the overall reduction in osteoarthritis when performing ACLR early versus late after injury was 10% (95% CI, 6% to 14%; OR, 0.54; 95% CI, 0.35 to 0.82; P < .001) (Figure 3).
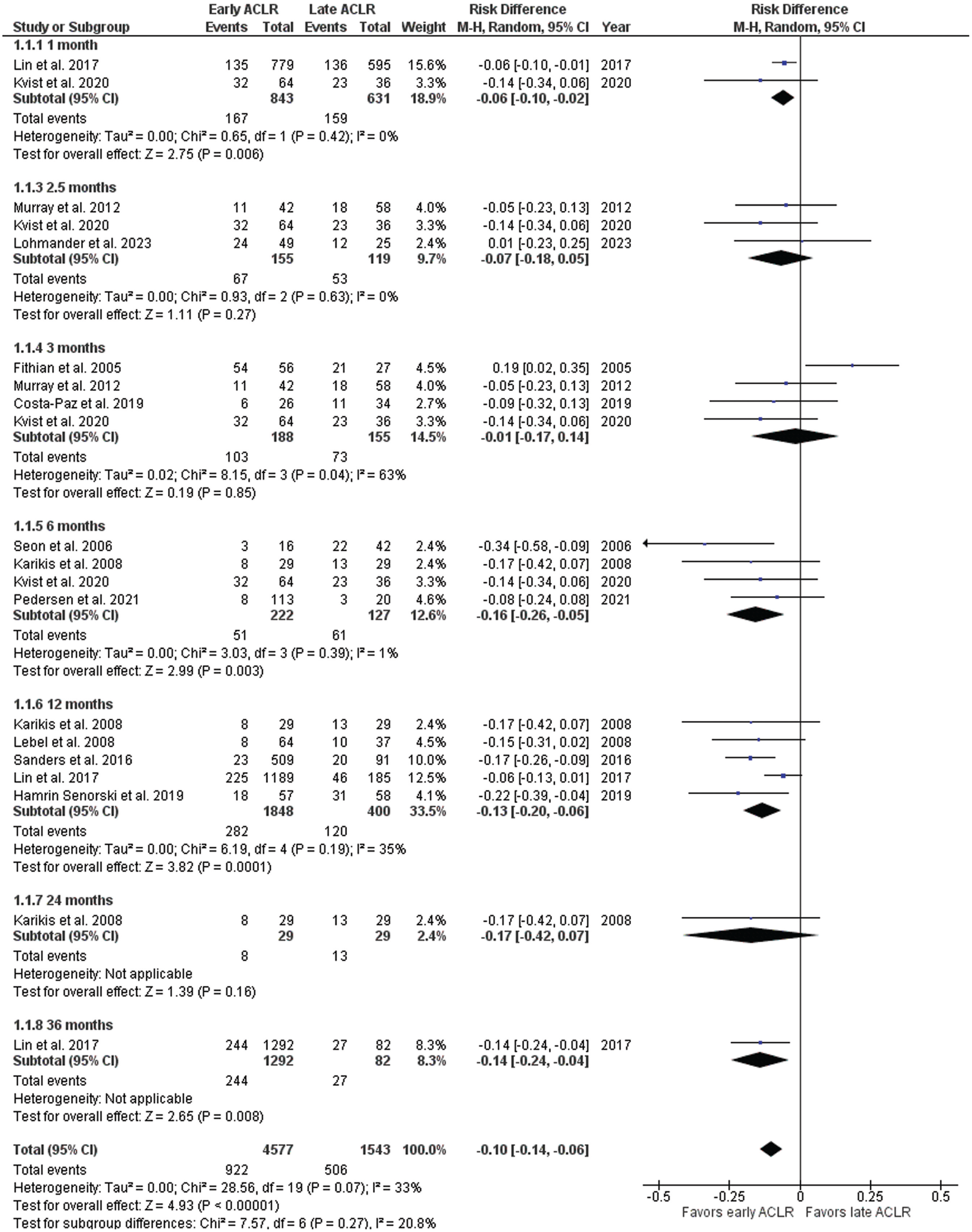
Forest plot of all studies with the different time thresholds comparing the incidence of osteoarthritis after early versus delayed anterior cruciate ligament reconstruction (ACLR) (reported as odds ratio).
Delay From Injury to Surgery
Six studies (685 patients) reported the time from injury to ACLR in the group that did versus did not develop osteoarthritis at the final follow-up. It was noted that patients who did not develop osteoarthritis underwent ACLR 15 months earlier after injury when compared with patients who ultimately developed osteoarthritis (MD, 15.4 months; 95% CI, 2-29 months; P = .03) (Figure 4).
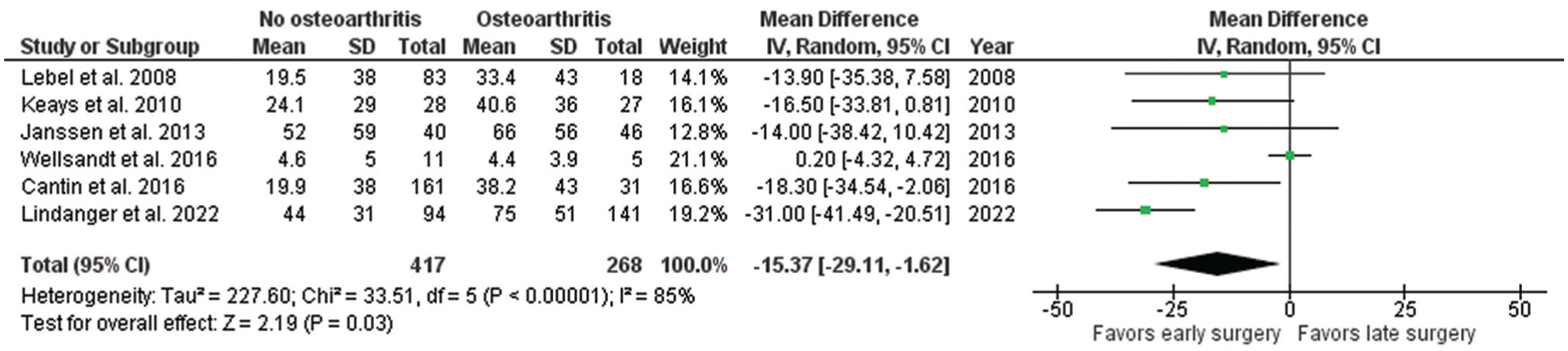
Forest plot of all studies comparing the time from injury to anterior cruciate ligament reconstruction in cohorts that did develop versus did not develop osteoarthritis at final follow-up (reported as mean difference).
Discussion
This study is, to the best of our knowledge, the first systematic review and comparative meta-analysis that assessed the role of timing of ACLR in the incidence of osteoarthritis at long-term follow-up. The main finding of this study was that increased time from injury to ACLR was associated with an overall 10% increased incidence of osteoarthritis when compared with early ACLR. This phenomenon was already noted at 1 month; the findings were most pronounced when surgery was performed within 6 and 12 months compared with delaying surgery beyond these thresholds.
In this study, an overall reduction in osteoarthritis incidence of 10% was seen when early versus delayed groups were compared, and these findings are likely at least partially explained by the status of the meniscus and cartilage at the time of ACLR. Several studies and meta-analyses have established clear correlations between an increased time from injury to surgery and the increased incidence of meniscal17,34,48 and cartilage injury.34,42 The increased incidence of osteoarthritis with increased time from injury to surgery might be explained by 3 potential mechanisms related to meniscal injuries: (1) an increased incidence of meniscal injuries at the time of ACLR,17,34,48 (2) a decreased likelihood of repairing torn menisci,34,43 and (3) an increased risk of failure of meniscal repair when performed later.18,20,22,28,45,57 These 3 factors increase the risk of meniscectomy during and after ACLR, and a clear correlation between meniscectomy and the development of osteoarthritis at follow-up has been previously established.5,12,55 Based on these mechanisms, the findings of the current study might not be surprising, but a correlation between delay of surgery and the increased risk of osteoarthritis had not been clearly identified previously. The findings in this study are supported by the systematic review by Cinque et al, 4 in which the authors performed an estimated meta-regression of case series and found a higher incidence of development of osteoarthritis when the mean time from injury to surgery was longer. Although they did not perform a formal meta-analysis and it is generally not recommended to compare incidences of different case series, the findings are similar to those of the current study. They found 12%, 22%, and 45% incidences of osteoarthritis with a delay of 6, 18, and 36 months, respectively.
Not all subgroup comparisons revealed statistical significance in this study, and this finding can most likely be explained by insufficient power in some of the subgroups. This limitation is shown by the fact that the nonsignificant comparisons (at 2.5, 3, and 24 months) had between 58 and 343 patients, whereas the significant comparisons had between 349 and 2248 patients. Furthermore, the odds ratios of the nonsignificant comparisons (range, 0.47-0.66 after sensitivity analysis) were not different from those of the significant comparisons (range, 0.39-0.69), indicating that the findings were consistent throughout the study with a reduced rate of osteoarthritis with earlier surgery, but that statistical significance was mostly determined by the number of patients in the subgroup analyses.
Most high-level evidence on the role of timing originates from 2 RCTs comparing early ACLR treatment with nonoperative treatment with potential delayed surgery,9,35 of which the long-term follow-up of one of these studies was included in this meta-analysis. 29 These studies found that between 39% and 50% of patients randomized to nonoperative treatment will require ACLR within 2 years,9,35 and that early ACLR prevents further meniscal damage at the 5-year follow-up. 41 However, the same study found no difference between both treatment strategies regarding cartilage thickness on magnetic resonance imaging at the 5-year follow-up 56 and on radiographic imaging at the 11-year follow-up. 29 The study designs of these RCTs are different from those of our included studies, and therefore the findings can not be directly compared with those of our study. However, the data in the current study suggest that, despite attempting nonoperative treatment as the initial treatment modality, one should consider not delaying surgery to prevent secondary damage and osteoarthritis. Interestingly, it has often been suggested that meniscal and chondral injury secondary to ACL instability becomes most pronounced when delaying surgery by >3 months,2,33,34,42 but the data in this study suggest that this effect might even occur earlier, with statistically significant findings at 1 month. This finding may be explained by the decreased success of meniscal repair at these time thresholds,18,20,22,45,47,57 and perhaps by the theory that earlier surgery might facilitate earlier return of knee function and normalization of synovial biomarkers.23,24,46
Limitations
Several limitations are present in this study. First, the level of evidence was rated as moderate using GRADE because one-third of the studies were level 4 evidence and not all studies had the main purpose to compare early versus late ACLR. Ideally, more prospective and preferably randomized studies will be performed on this topic to provide better data. Furthermore, because of the study design of a systematic review and meta-analysis, it is not possible to correct for potential confounders such as meniscectomy, length of follow-up, sex, or level of sports participation. However, meniscectomy is correlated with the delay between injury and surgery17,34,48 and is likely one of the drivers of the increased risk of osteoarthritis with delayed surgery.5,12,55 Also, the thresholds are arbitrary, as patients can be in different groups despite a small difference in delay between injury and surgery. The observed differences in osteoarthritis incidence were consistent throughout all time thresholds, indicating that the effect is based on a continuum rather than a threshold. Finally, several studies could not be included because of a lack of usable data for the meta-analysis, and it would be useful if future studies on osteoarthritis after ACLR would include the role of timing to increase our knowledge on this topic and enable more robust analysis and correction of potential confounders.
Conclusion
This systematic review with a 5-year minimum follow-up demonstrates that shorter time from injury to ACLR was associated with a decreased incidence of long-term osteoarthritis. This reduced risk was already seen when surgery was performed within 1 month, but it was most pronounced when surgery was performed within 6 months and 12 months after injury.
Footnotes
Submitted February 21, 2025; accepted May 5, 2025.
One or more of the authors has declared the following potential conflict of interest or source of funding: J.P.V.D.L. has received support for education from Smith & Nephew and hospitality payments from Arthrex. C.C.K. has received consulting fees from Arthrex. D.C.F. has received consulting fees from Verical Corp, Medical Device Business Services, Smith & Nephew, and Linvatec Corporation. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
An online CME course associated with this article is available for 1 AMA PRA Category 1 Credit™ at https://education.sportsmed.org/Public/Catalog/Home.aspx?CourseSearch=1&Criteria=9&Option=25. In accordance with the standards of the Accreditation Council for Continuing Medical Education (ACCME), it is the policy of The American Orthopaedic Society for Sports Medicine that authors, editors, and planners disclose to the learners all financial relationships during the past 12 months with any commercial interest (A ‘commercial interest’ is any entity producing, marketing, re-selling, or distributing health care goods or services consumed by, or used on, patients). Any and all disclosures are provided in the online journal CME area which is provided to all participants before they actually take the CME activity. In accordance with AOSSM policy, authors, editors, and planners’ participation in this educational activity will be predicated upon timely submission and review of AOSSM disclosure. Noncompliance will result in an author/editor or planner to be stricken from participating in this CME activity.