
Abstract
Background:
The identification of the medial patellofemoral ligament (MPFL) insertion site relies heavily on the use of radiographic landmarks such as the Schöttle point. However, little is known on how the variation in condylar alignment and beam directionality affects this perceived location.
Purpose:
To quantify changes in the perceived MPFL insertion site when posterior proximal or posterior distal condylar alignment is optimized and when fluoroscopic beam directionality alters.
Study Design:
Controlled laboratory study.
Methods:
A total of 16 cadaveric knees were included. The femoral insertion of the MPFL was identified and fixed with a radiopaque metal marker after dissection. Fluoroscopic images in the medial-to-lateral (ML) direction were taken with the posterior proximal condyles aligned and then with the posterior distal condyles aligned. Beam directionality was flipped to the lateral-to-medial (LM) direction, and images with posterior proximal and posterior distal condylar alignment were taken. Images were then superimposed onto the reference image, with discrepancies between marker locations quantified in the x- and y-axis. The 2-tailed Student t test was performed on all obtained variations.
Results:
In the ML direction, proximal versus distal alignment resulted in a mean proximal displacement of 0.43 ± 1.86 mm (P = .37) and a mean posterior displacement of −0.11 ± 0.55 mm (P = .42). In the LM direction, proximal versus distal alignment resulted in a mean proximal displacement of 1.95 ± 2.37 mm (P = .005) and a mean anterior displacement of 0.22 ± 1.95 mm (P = .67). When comparing ML to LM beam directionality with optimized proximal condylar alignment, there was a mean distal displacement of −0.26 ± 1.73 mm (P = .56) and a mean anterior displacement of 2.22 ± 1.87 mm (P < .001). When comparing ML to LM beam directionality with optimized distal condylar alignment, there was a mean proximal displacement of 1.26 ± 2.53 mm (P = .07) and a mean anterior displacement of 2.55 ± 1.71 mm (P < .001).
Conclusion:
Beam directionality and condylar alignment affected the perceived location of the MPFL insertion. However, shooting in the ML direction and aligning the posterior proximal femoral condyles resulted in the least amount of total variation. Future studies are needed to determine the amount of variation in perceived MPFL insertion sites that are clinically significant.
Clinical Relevance:
This information provides surgeons with the insight that beam directionality and condylar alignment significantly affect the perceived location of the MPFL insertion site and that surgeons can use fluoroscopic imaging in the ML direction with posterior proximal condylar alignment to minimize image variation.
Keywords
The medial patellofemoral ligament (MPFL) is one of the most important soft tissue stabilizers of the patella.1,2,5,19,20 Connecting the medial aspect of the patella to the medial femoral condyle, the MPFL resists lateral displacement of the patella and helps to prevent patellar dislocations or subluxations.19,30 Patellar instability, which accounts for 3% of all knee injuries, can cause debilitating pain and functional impairment. The population most affected is adolescents, with an incidence rate of 29 per 100,000. 13
When nonoperative management is unsuccessful, a surgical intervention is considered. One of the most common surgical procedures performed for patellar instability is MPFL reconstruction (MPFLR).16,23,24,27,31,33 While additional methods and factors have been associated with improved outcomes, the success of this procedure largely depends on accurate femoral tunnel placement of the graft.23,24,33 Aberrant positioning of the femoral tunnel can lead to excessive graft anisometry, potentially resulting in persistent instability/dislocations, motion loss, graft failure, and patellar stiffness; technical errors have been described as a major contributor to the MPFLR failure rate, with reported values up to 46%.3,17,22,25 Intraoperative fluoroscopy is an important tool that is heavily relied on to ultimately determine and guide optimal positioning of the graft and hardware.6,9,10,12,15,29
One of the main radiographic concerns affecting fluoroscopy lies in standardizing alignment in the lateral view of the knee, which is essential for accurately assessing patellar height, patellar tilt, and variations in bony anatomy.9,10,15,26,35,36 The “perfect” lateral radiograph has been described as one in which the distal femoral condyles are superimposed on each other, indicating that the knee is in a true lateral position.1,7,9,11,35 Despite its importance in MPFLR, this view is not easy to achieve, with factors such as variability in patients’ native anatomy, body position, and angle of the fluoroscope all having a documented distortive influence on the perceived location of desired knee anatomy.4,6,9,10,35,36 Furthermore, there is no clarification as to whether proximal or distal condylar alignment should be prioritized in the “perfect” lateral radiograph, which can significantly alter the view in patients with discrepancies in femoral condylar size (Figure 1). Intraoperative beam directionality of the C-arm has also long been thought to be interchangeable, and its potential effect on fluoroscopic images has not been quantified. Thus, the purpose of this study was to quantify how variations in condylar alignment and beam directionality affect the perceived location of the MPFL insertion site.

Clinical example showing differences when the (A) posterior and distal condyles are aligned compared with when the (B) posterior and proximal condyles are aligned.
Methods
Specimen Dissection and Anatomic Identification
There were 16 fresh-frozen cadaveric knees utilized for this biomechanical radiographic analysis. Once thawed, specimens were carefully dissected down to bone, removing skin and subcutaneous fat and exposing the insertion of the MPFL along the medial aspect of the femur (Figure 2). Once identified, the approximate insertion point was marked, and a standardized 2.2 mm–diameter metal ball bearing was then hammered into the insertion point with a mallet.
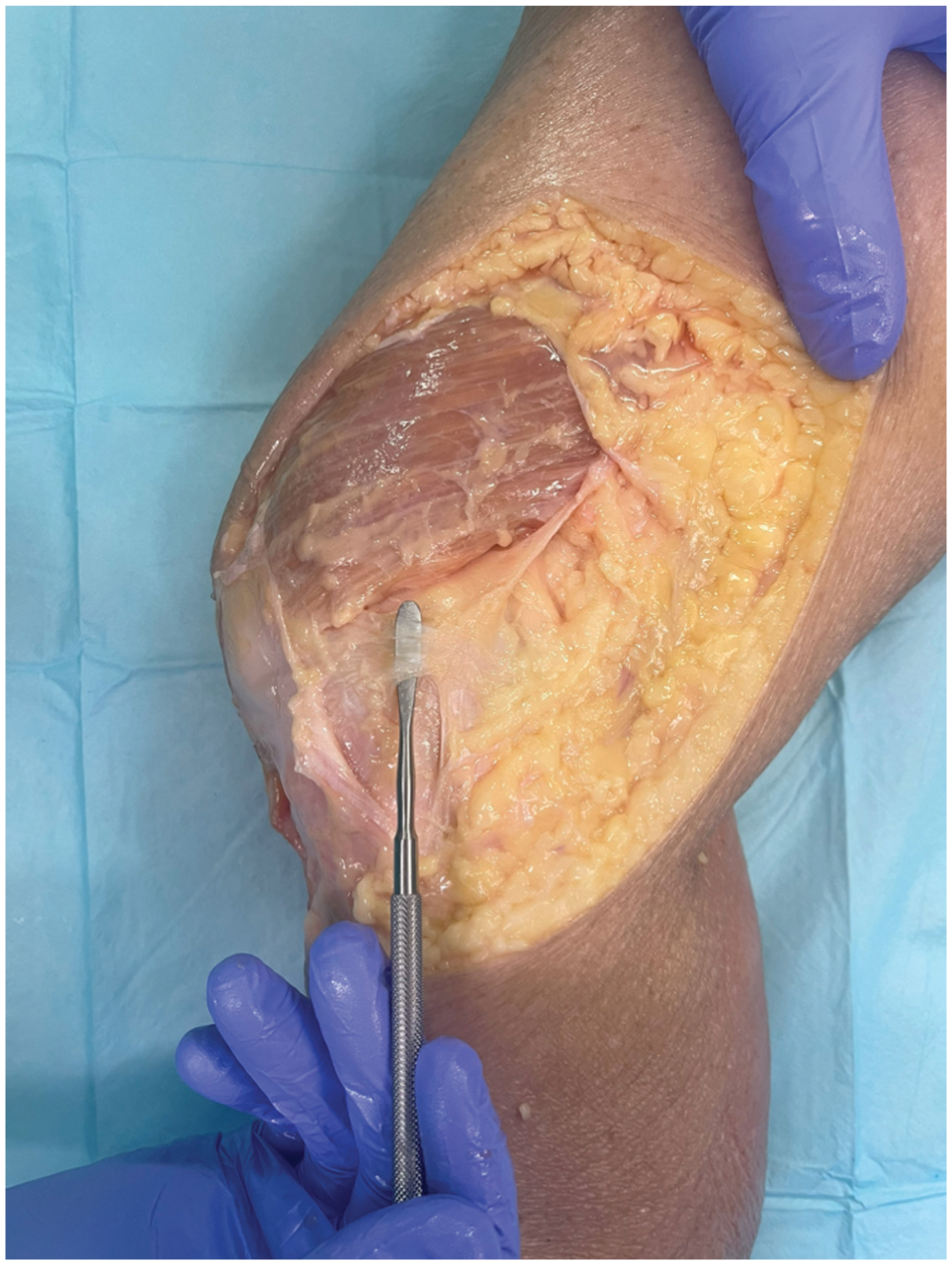
Cadaveric dissection of a right medial knee, with the medial patellofemoral ligament fibers raised.
Radiographic Imaging Protocol
The specimens were examined by a team of 4 authors including an attending sports medicine physician, postgraduate year 5 resident, postgraduate year 1 resident, and third-year medical student (S.K.A., J.F., A.K.M., and A.Z.K., respectively). Once properly prepared, each knee was mounted to a stand to be visualized using a standard-size C-arm fluoroscopy machine (OEC 9900 Elite Mobile C-arm; GE HealthCare). Before beginning the imaging sequence, the distance between the fluoroscopic x-ray tube and intensifier was measured with a 3-ft ruler to ensure equidistant placement of the specimens at the same halfway point for each shot taken throughout the study. Furthermore, throughout the experiment, a 32 mm–diameter metal calibration sphere was placed in every shot to ensure a proper scale of the images. The fluoroscopic imaging sequence consisted of 4 shots, with the first 2 in the medial-to-lateral (ML) direction and the final 2 in the lateral-to-medial (LM) direction. The first image showed optimized alignment of the posterior proximal condyles (Figure 3A). The second shot had the posterior distal condyles aligned (Figure 3B). Then, the sample was flipped and recentered halfway between the x-ray tube and intensifier to obtain images in the LM direction (Figure 4). The third shot was taken again with the posterior proximal condyles aligned (Figure 3C) and the fourth shot with the posterior distal condyles aligned (Figure 3D). For every view in the sequence, multiple shots were taken until all present co-investigators agreed on optimal alignment, at which time the images were marked and uploaded to the institution’s picture archiving and communication system (IntelliSpace Radiology Enterprise 4.5; Philips).
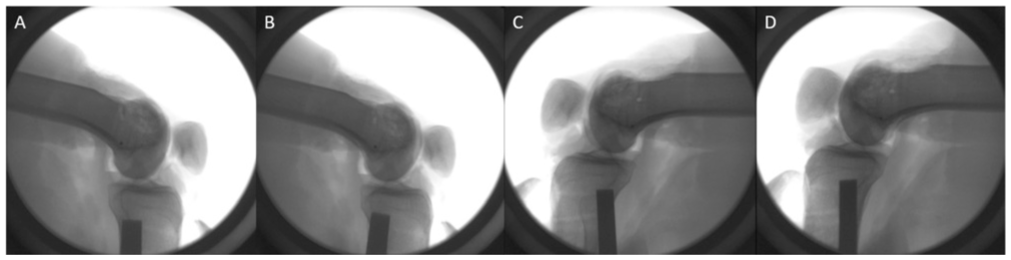
Imaging sequence: in the medial-to-lateral direction, alignment of the (A) posterior proximal condyles and (B) posterior distal condyles; in the lateral-to-medial direction, the flipped sample with alignment of the (C) posterior proximal condyles and (D) posterior distal condyles.
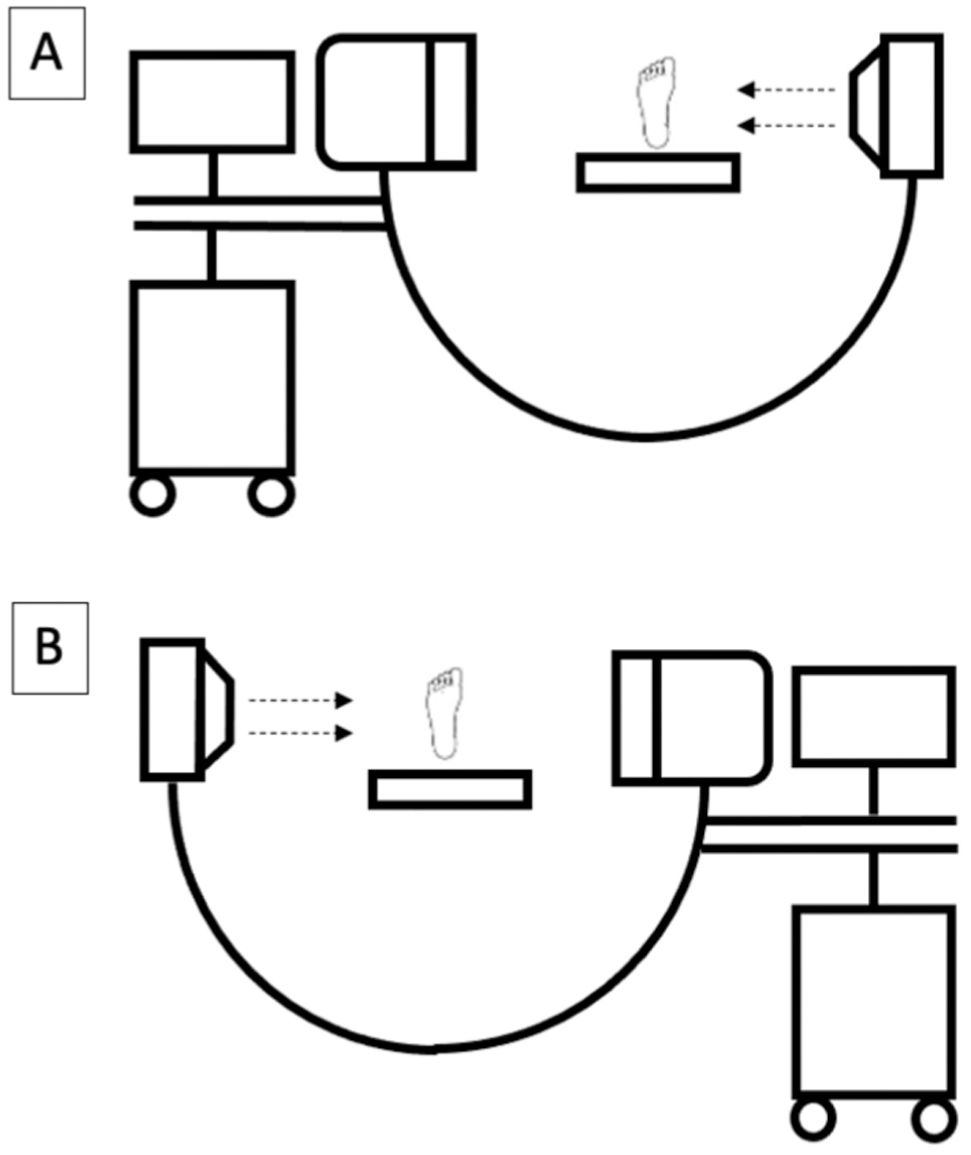
Diagram showing a beam shooting in the (A) medial-to-lateral direction and (B) lateral-to-medial direction to capture fluoroscopic images of a right leg.
Fluoroscopic Measurements
Once made accessible, all fluoroscopy shots were sorted by specimen. Using open-source image processing software ImageJ (National Institutes of Health), images from each sequence were individually uploaded alongside the “perfect” lateral image. Both images were calibrated and scaled to one another using the 32-mm sphere. Then, the 2 images were transposed and overlaid with matched orientation and transparency so that both MPFL markers could be clearly visualized. The overlaid images were thoroughly assessed to ensure the identical location of the femurs. To optimize alignment of the overlays, a scale-invariant feature transform algorithm was used to match the components of the overlay (location of the 2 femurs) to one another.
With the optimized overlays produced, the midpoint of each of the two 2.2-mm MPFL marker balls was identified, and a line was then drawn between them using the calibrated ruler function (Figure 5). The total distance, along with displacement in the x- and y-axis between the 2 markers, was recorded. This process was repeated for every view in each sequence by 2 medical students (B.T.J. and A.Z.K.).
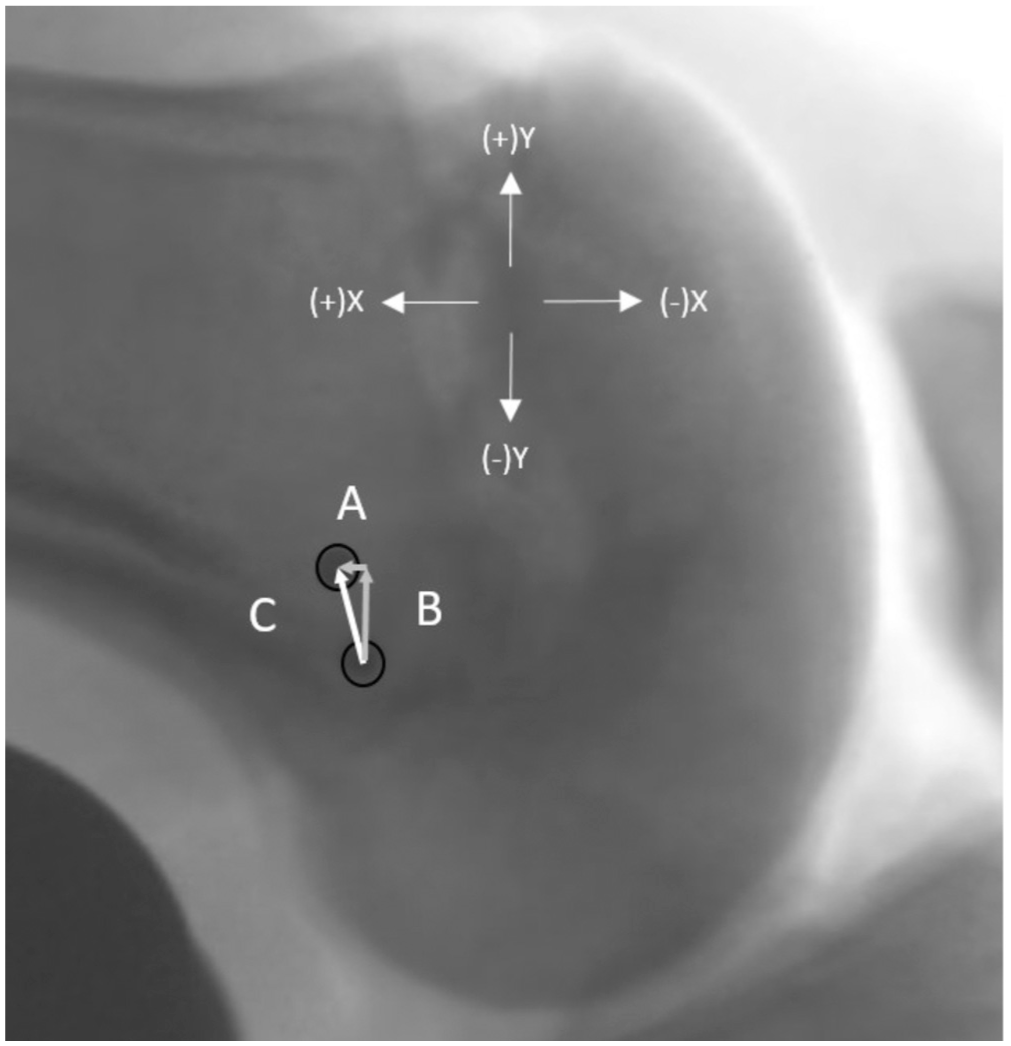
Example of the measurement process of 2 overlaid fluoroscopic images comparing optimized distal versus proximal condylar alignment in the medial-to-lateral direction in which the black circles represent the medial patellofemoral ligament marker. (A) The change in the x-axis, (B) the change in the y-axis, and (C) the Euclidean distance.
Statistical Analysis
All statistical analyses were performed using Excel (Version 16.54; Microsoft) and SPSS (Version 30.0; IBM). Once raw data were collected, means and standard deviations, along with Euclidean distances, were computed between all views, comparing both beam directionality (ML vs LM direction) and posterior condylar alignment (posterior proximal vs posterior distal). Interclass correlation coefficients were calculated via a consistency-type 2-way mixed model. The 2-tailed Student t test was performed to determine significance between alignment variations, with statistical significance defined as P < .05.
Results
A total of 16 female cadaveric knees (10 left, 6 right) with a mean age of 60.8 years and a mean body mass index of 27.5 kg/m2 were analyzed. The interclass correlation coefficient was 0.879 (range, 0.654-0.958) between reviewers, indicating strong agreement. 18
In the ML direction, proximal versus distal alignment resulted in a mean proximal displacement of 0.43 ± 1.86 mm and a mean posterior displacement of −0.11 ± 0.55 mm (Table 1); the mean Euclidean distance between markers for proximal versus distal condylar alignment was 1.65 ± 1.03 mm. In the LM direction, proximal versus distal alignment resulted in a mean proximal displacement of 1.95 ± 2.37 mm and a mean anterior displacement of 0.22 ± 1.95 mm; the mean Euclidean distance between markers for proximal versus distal condylar alignment was 2.91 ± 2.12 mm. When comparing ML to LM beam directionality with optimized proximal condylar alignment, there was a mean distal displacement of −0.26 ± 1.73 mm and a mean anterior displacement of 2.22 ± 1.87 mm. The mean Euclidean distance between proximal ML and LM beam changes was a 2.98 ± 1.55–mm anterior and distal alteration. When comparing ML to LM beam directionality with optimized distal condylar alignment, there was a mean proximal displacement of 1.26 ± 2.53 mm and a mean anterior displacement of 2.55 ± 1.71 mm. The mean Euclidean distance between distal ML and LM beam changes was a 3.94 ± 1.18–mm proximal and distal alteration.
Comparative Distances Between Alignment Variations a
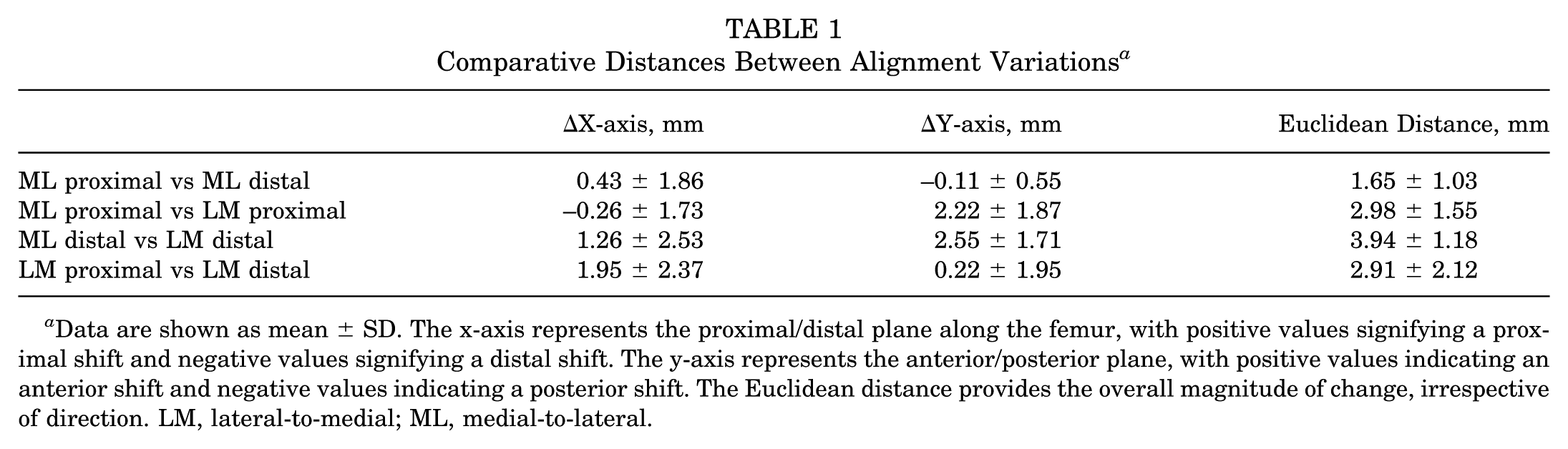
Data are shown as mean ± SD. The x-axis represents the proximal/distal plane along the femur, with positive values signifying a proximal shift and negative values signifying a distal shift. The y-axis represents the anterior/posterior plane, with positive values indicating an anterior shift and negative values indicating a posterior shift. The Euclidean distance provides the overall magnitude of change, irrespective of direction. LM, lateral-to-medial; ML, medial-to-lateral.
There were significant differences in the mean y-axis displacement when changing beam directionality from the ML to LM direction and when the proximal (P < .001) and distal (P < .001) condyles were aligned (Table 2). There was also a significant difference in the mean x-axis displacement when optimizing proximal versus distal condylar alignment in the LM direction (P = .005) but not in the ML direction (P = .37).
P Values for Statistical Significance a
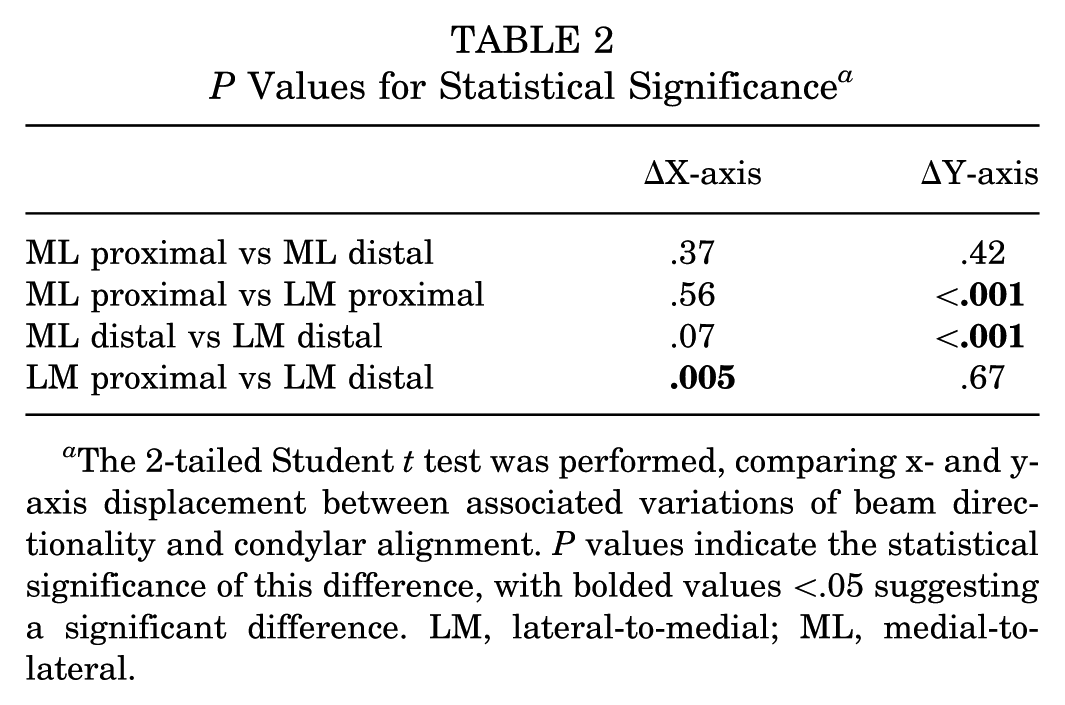
The 2-tailed Student t test was performed, comparing x- and y-axis displacement between associated variations of beam directionality and condylar alignment. P values indicate the statistical significance of this difference, with bolded values <.05 suggesting a significant difference. LM, lateral-to-medial; ML, medial-to-lateral.
Discussion
The findings of the present study suggest that fluoroscopic beam directionality and condylar alignment can affect the perceived location of the Schöttle point. Specifically, significant differences in the location of the MPFL insertion site were appreciated when shooting in the ML versus LM direction and when posterior proximal versus posterior distal condylar alignment was prioritized. These variations were smallest when utilizing a technique in the ML direction and with posterior proximal condylar alignment, indicating that this may be the most consistent method to obtain “perfect” lateral radiographs. Future studies are needed to determine the amount of variation that results in a clinically significant difference.
While the concept of the “perfect” lateral view is instrumental to orthopaedic diagnostic and surgical planning, the lack of consensus and defined specificity regarding condylar alignment remains. 7 Furthermore, multiple inherent variables make obtaining the perfect radiograph difficult, including natural asymmetry between the medial and lateral femoral condyles. 8 This asymmetry is further exaggerated in patients with patellar instability, who are thought to experience more significant lateral condylar hypoplasia compared with patients without instability. 14 Other factors such as sex also affect the variation in condylar anatomy. 34 Given that this study used skeletally mature and exclusively female cadaveric knees, this limits our findings compared with the standard patient population undergoing MPFLR. However, we believe that beam directionality and condylar alignment may play a larger role in the MPFLR population compared with our study population because of greater condylar asymmetry. Furthermore, we believe that the methodology utilized in this study would apply across other patient populations as well, but this may be the basis of future investigations.
Ziegler et al 36 also performed a similar investigation to the current study, comparing the precision of the Schöttle point in 10 cadaveric knees in which they defined the “perfect” lateral radiograph as having the posterior condyles aligned. They changed the position of the fluoroscope by 2.5°, 5°, and 10° anteriorly, posteriorly, proximally, and distally and then superimposed the views with altered patellar tilt to track transposition of the MPFL insertion. While anterior, posterior, and distal translation of the beam were found to be statistically significant at 5°, proximal translation, which closely resembles posterior proximal condylar alignment in our study, was not found to be significantly different, even at 10° of error. 36 In the present study, deviations were also smallest when posterior proximal condyles were aligned, further suggesting that posterior proximal condylar alignment is an advantageous strategy to approximate the MPFL origin.
In 6 cadaveric femurs, Balcarek and Walde 4 investigated the effects of internal and external rotation, along with adduction and abduction, on displacement of the native MPFL site. They found that small degree changes in both internal and external rotation, as well as in abduction and adduction, significantly altered the perceived location of the MPFL insertion site with posterior distal condylar alignment. While the variation observed between approaches in these biomechanical studies and the current study may only be on the magnitude of millimeters, Stephen et al 32 determined that 5 mm of shift from the anatomic insertion point of the MPFL can cause significant changes in patellar tilt and tensile pressure. Furthermore, Rosenthal et al 28 found that only 5 mm of deviation from the standard MPFL insertion site across multiple directional planes changed functional biomechanical tension on the graft. While the observed variations approximated 2 mm, which falls below the 5 mm noted above, the millimetric differences between beam directionality and condylar alignment may be greater in the standard MPFLR population compared with the study population because of greater condylar asymmetry, as noted above. Furthermore, the millimetric amount of tunnel misplacement that correlates with changes in clinical outcomes or revision rates is unknown. The combination of data and questions highlights the sensitive nature of MPFLR and a need for more research into proper graft placement.
Overall, the “perfect” lateral radiograph is a highly sensitive and influential tool that requires further descriptive standardization. Patient anatomy, beam directionality, and condylar alignment significantly alter the perceived location of the MPFL insertion site, potentially affecting the accuracy of graft placement. The data presented here may be used to guide surgical decision-making and assist in our understanding of the subtleties of obtaining a “perfect” lateral radiograph. Further research is warranted to develop and validate standardized protocols, with the ultimate goal of improving the accuracy and safety of MPFLR.
Limitations
This study has several limitations. First, this experiment was performed on skeletally mature cadaveric knees, which may not accurately represent the average patient population undergoing MPFLR. The actual magnitude of changes may be larger in the clinical scenario, given the potential greater discrepancies in femoral condylar sizes in patients with patellar instability. 14 Second, all cadaveric knees were female, which may bias the results because some literature has reported differences in condylar anatomy between sexes. 21 Third, distances between alignment variations were measured manually, which inherently creates a risk for measurement bias. Our standardized calibration and scaling processes were consistently performed on every comparative view to minimize error, although, as with any manual process, a degree of potential user error always exists. Fourth, we did not systematically control for internal or external femoral rotation, which may affect measurements. Lastly, while we observed statistical significance with our findings, it is important to acknowledge that our results do not establish whether the variations noted are large enough to be clinically relevant when performing MPFLR.
Conclusion
When taking a “perfect” lateral radiograph, condylar alignment and fluoroscopic beam directionality play a significant role in the perceived location of the MPFL insertion site. Based on the current study, taking fluoroscopic images in the ML direction and aligning the posterior proximal femoral condyles resulted in the least amount of total variation.
Footnotes
Submitted April 15, 2025; accepted July 30, 2025.
One or more of the authors has declared the following potential conflict of interest or source of funding: J.J.E. has received consulting fees from Johnson & Johnson. S.K.A. has received consulting fees from Stryker. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.