
Abstract
Background:
Injury to the medial ulnar collateral ligament (MUCL) is a common setback for throwing athletes, often requiring reconstruction with 12 to 18 months of rehabilitation. The authors previously described a more anatomic technique with improved mechanical strength as compared with the docking technique, which may allow for an accelerated return to sport.
Purpose:
To evaluate return-to-sport rates, time to return to sport, and the effect on the functional performance of amateur and professional throwing athletes who underwent anatomic MUCL reconstruction with suture tape augmentation.
Study Design:
Case series; Level of evidence, 4.
Methods:
A retrospective case series was performed including baseball players who underwent anatomic MUCL reconstruction with suture tape augmentation by a single surgeon from 2018 to 2022. Inclusion criteria consisted of a minimum 2-year follow-up, participation in baseball, and utilization of autograft (palmaris longus or gracilis). Patients who underwent previous MUCL reconstruction were excluded from the study. All patients initially followed an accelerated rehabilitation protocol. Outcome measures were collected, including Kerlan-Jobe Orthopaedic Clinic (KJOC), Single Assessment Numeric Evaluation (SANE), and Conway-Jobe scores, as well as throwing metrics such as ball velocity and spin rate.
Results:
Thirty-four baseball players (mean ± SD age, 21 ± 3 years) underwent primary MUCL reconstruction. Time of final follow-up was 36.1 ± 10.3 months. Of these, 16 were professional athletes and 18 were amateur. All throwers returned to live gameplay at a mean 10.1 ± 2.0 months after reconstruction (professional, 10.6 ± 2.3; amateur, 9.7 ± 1.8). Furthermore, 97% (94% professional, 100% amateur) advanced through the accelerated postoperative protocol without issues, and 91% (88% professional, 94% amateur) returned to the same role and 85% (75% professional, 94% amateur) to the same level of play. Professional postinjury KJOC scores improved from 42.6 ± 16 to 87.5 ± 8.3 and SANE scores from 25.0 ± 11.2 to 95.6 ± 4.2. Amateur postinjury KJOC scores improved from 35.6 ± 10.7 to 90.9 ± 8.6 and SANE scores from 57.5 ± 16.9 to 95.2 ± 7.2. No significant difference was identified in preinjury versus postreconstruction throwing velocity, ball spin rate, or horizontal/vertical ball movement. The overall failure rate was 2.9%, with 1 professional pitcher requiring revision for graft rupture at 3 years postoperatively.
Conclusion:
Anatomic reconstruction of the MUCL with suture tape is a viable option for MUCL injuries, allowing an expedited return to sport at 10.1 ± 2.0 months (professional, 10.6 ± 2.3; amateur, 9.7 ± 1.8) in baseball players, with a low failure rate.
Although our understanding of the risk factors for medial ulnar collateral ligament (MUCL) injuries has improved in recent years,18,22 the rate of MUCL injuries in baseball players and throwing athletes continues to climb steadily.4,5,7,12,19 This is true at the professional, collegiate, and even youth levels. As injury rates increase, the number of athletes undergoing surgery continues to rise, and a 2018 study recently demonstrated that 35% of Major League Baseball pitchers reported a history of MUCL surgery. 19 Historically, the gold standard for the surgical treatment of MUCL injuries has been ligament reconstruction, which is commonly referred to as Tommy John surgery, taking its namesake from the first professional baseball player to have ever undergone the procedure in 1974. 16 Although there have been several attempts to improve MUCL reconstruction surgical techniques, the docking technique (described in 2002) 23 and modified Jobe technique (described in 2001) 27 remain the most common methods for reconstructing the MUCL. 15 Over the last several decades, MUCL reconstruction has been a reliable surgical treatment option, with a mean 85% to 95% of players being able to return to competitive play.4,5,9,14,20,29 The primary issue with these historical techniques lies in the extended return-to-play times where most athletes require 12 to 18 months to return to full unrestricted baseball pitching.4,5,9,14,20,29 Accordingly, it is not uncommon that delayed treatment can result in a player missing 2 full seasons of competitive baseball.
In recent years, there has been growing interest in MUCL repair with suture tape augmentation.8,11 This technique relies on repair of the native MUCL back to the medial epicondyle or sublime tubercle, depending on the site of injury, and augmentation of the repair with a flat suture tape without utilization of a graft.11,17 This procedure is less disruptive to the native anatomy and biology of the medial elbow as compared with traditional reconstruction techniques, and accordingly, it has resulted in shorter return-to-play times that are generally in the 6- to 9-month range.10,25 The primary downsides of this surgical technique are that it may not be suitable for all tear types (chronic attrition, poor ligament quality, multisite injury, midsubstance tears, etc), and the long-term outcomes are less clear than they are for traditional reconstruction.2,13,28
In an attempt to retain the benefits of traditional MUCL reconstruction techniques (durability and broad applicability regardless of tear type) while expediting return-to-play times similar to that of augmented MUCL repair, new techniques have been developed that combine the concepts of native ligament repair, collagen reinforcement with a graft, and augmentation with a suture type.1,3,21,24 One such technique is the anatomic technique for MUCL reconstruction that was initially described in 2019. 3 This technique was designed to better replicate native ligament anatomy, minimize bone removal, decrease the biologic and vascular disruption, and maximize the tendon-to-bone contact area for the proximal and distal ends of the graft to increase healing potential. Without suture tape augmentation, this technique has demonstrated biomechanical strength superior to the docking technique and similar to the native MUCL, 3 but it was designed so that a suture tape augmentation could easily be added if desired. Although the biomechanical evidence for the anatomic technique is encouraging, clinical outcomes are lacking in the published literature. Accordingly, the primary purpose of this study was to report on the clinical outcomes of MUCL reconstruction using the anatomic technique with suture tape augmentation in competitive baseball players. Specifically, we sought to determine (1) return-to-sport rates; (2) time to return to sport after an accelerated rehabilitation protocol; and (3) the effect on functional and performance outcomes such as patient-reported outcomes (PROs), return to same level of play, and various ball-tracking metrics. We hypothesized that players would be able to return to high-level baseball at a high rate and would be able to do so faster than what has historically been observed for other MUCL reconstruction techniques.
Methods
Inclusion and Exclusion Criteria
After institutional board approval (Mayo Clinic IRB 22-003721), a retrospective review was performed consisting of baseball players who underwent anatomic MUCL reconstruction with suture tape augmentation by a single surgeon from 2018 to 2022. This resulted in 42 patients who were initially eligible for inclusion. Inclusion criteria consisted of a minimum 2-year follow-up, participation in baseball, and utilization of autograft (palmaris longus or gracilis). Patients who underwent previous MUCL reconstruction were excluded. In total 34 patients were included in this study.
Surgical Technique
A video presentation of the surgical technique can be accessed at the following: https://doi.org/10.1177/26350254231212507. 6 The palmaris longus autograft was the preferred graft if present in the ipsilateral extremity; otherwise, the contralateral gracilis tendon was utilized. After graft harvest, a 6-cm incision is created over the medial epicondyle to expose the sublime tubercle and medial epicondyle. Sutures are placed using a No. 0 FiberWire suture in a running Krakow fashion through the torn ligament, which are eventually used to formally repair the native ligament at a later stage (Figure 1). Rather than splitting the native ligament, the tear is opened up to identify the joint line. A 4-mm socket is drilled to a depth of 15 mm in the MUCL origin of the medial epicondyle, and two 2-mm penetrating sockets are drilled toward the base of the 4-mm socket via a c-shaped guide. If the tear in the native ligament was proximal, the sutures in the native ligament are passed through the medial epicondyle sockets and later tied over the bone bridge to complete the native ligament repair; if the tear is distal, these repair sutures are loaded into the 3.5-mm SwiveLock anchor used to fix the graft distally (described later). A BTB TightRope (Arthrex) without a button is shuttled through the medial epicondyle socket. The long loop is passed from proximal to distal and then tagged. On the other side, the shuttling stitch and the remaining free suture are shuttled proximal to distal. The small shuttling stitch is tagged, and the longer suture is pulled and passed through the previously passed loop. This creates the tight rope that will contain the graft and suture tape on the distal side. The stitch is loaded back onto the shuttling suture and shuttled back through. It is then shuttled through the tight rope. This completes the creation of the tight rope over the bone bridge. The palmaris longus autograft and a suture tape internal brace (Arthrex) are loaded onto the tightrope and reduced into the humeral socket (Figure 2). On the ulna, knot-tying FiberTak anchors (Arthrex) are placed on either side of the sublime tubercle, 8 to 10 mm distal to the joint line. Both distal ends of the graft are then sutured with a FiberLoop (Arthrex). The graft is secured to the sublime tubercle by tying down the previously placed suture anchors at approximately 49° of flexion and neutral rotation while a varus load is applied. The FiberLoop sutures from the graft and the suture tape augmentation are loaded into a 3.5-mm SwiveLock suture anchor (Arthrex), which is fixed at the distal aspect of the sublime tubercle ridge creating an anatomic reconstruction (Figure 3). Then, the native ligament sutures and tight rope at the medial epicondyle are retensioned and tied across the humeral bone bridge for final fixation. The graft, suture tape, and native ligament are all sutured together to unitize the entire construct (Figures 4 and 5). For a complete technique video, please refer to the following: https://doi.org/10.1177/26350254231212507. 6
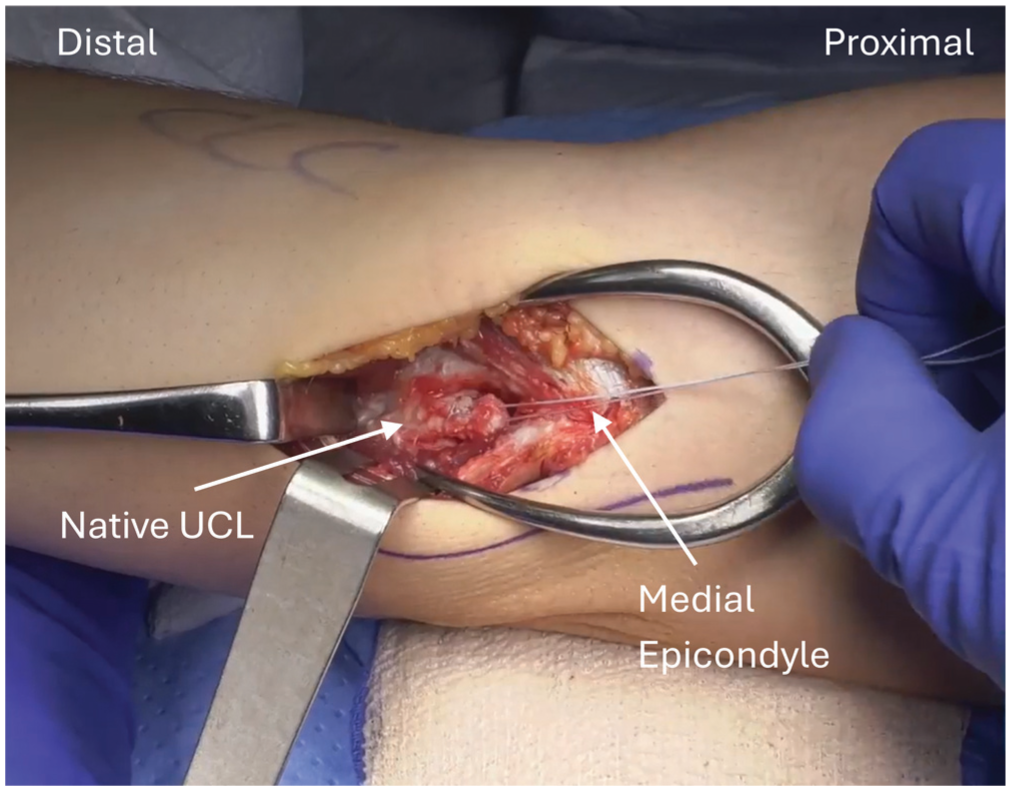
Right elbow with a No. 0 FiberWire suture in a running Krakow fashion within the native ligament, which will be used for repair. UCL, ulnar collateral ligament.
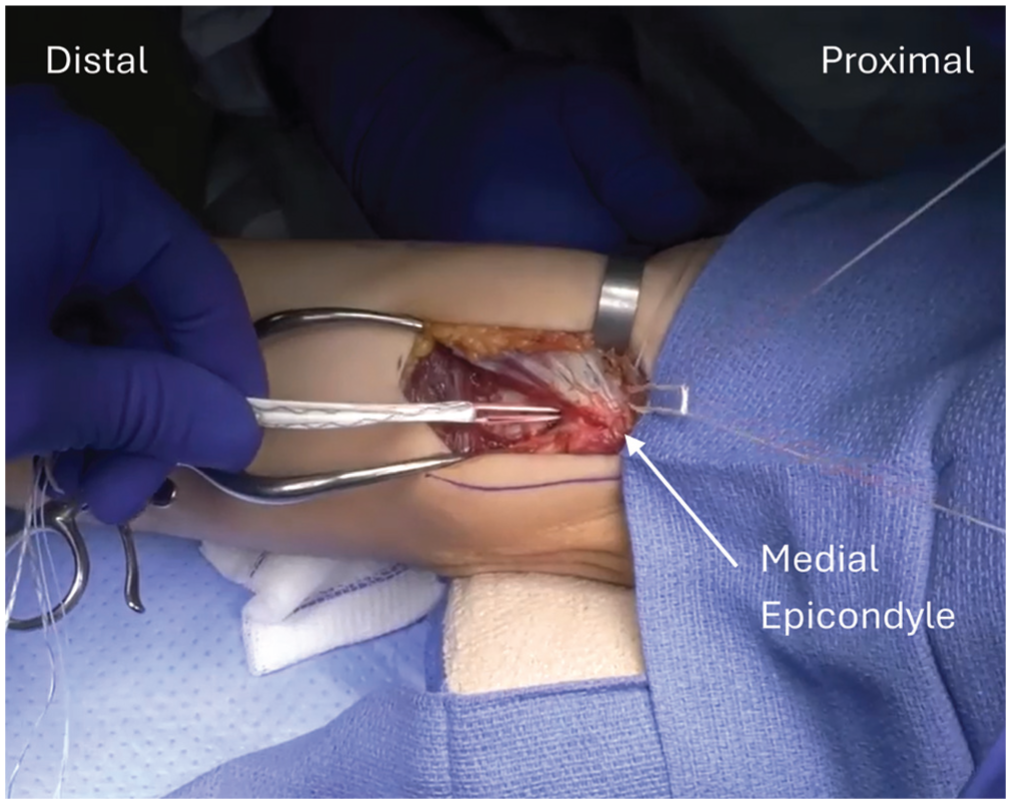
Right elbow with an Arthrex BTB TightRope without a button, assembled within medial epicondyle drill holes to reduce the graft and suture augment.
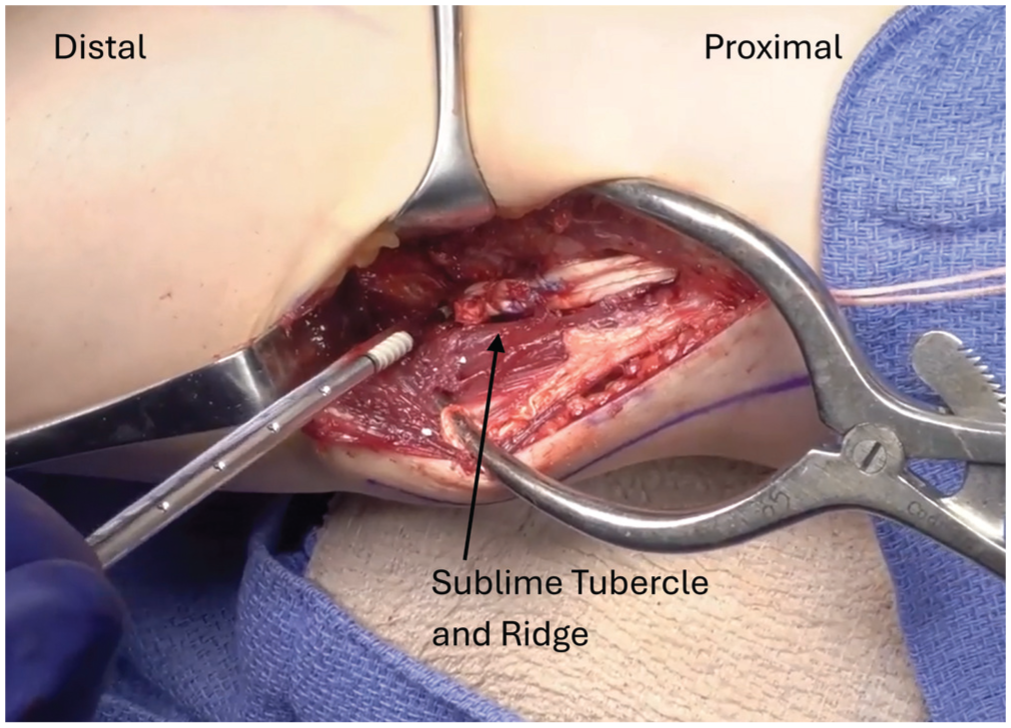
Right elbow: 2 knot-tying FiberTak anchors (Arthrex) on either side of the sublime tubercle are tied across the graft, and a 3.5-mm SwiveLock suture anchor (Arthrex) is fixed at the distal aspect of the sublime tubercle ridge to re-create the native footprint.
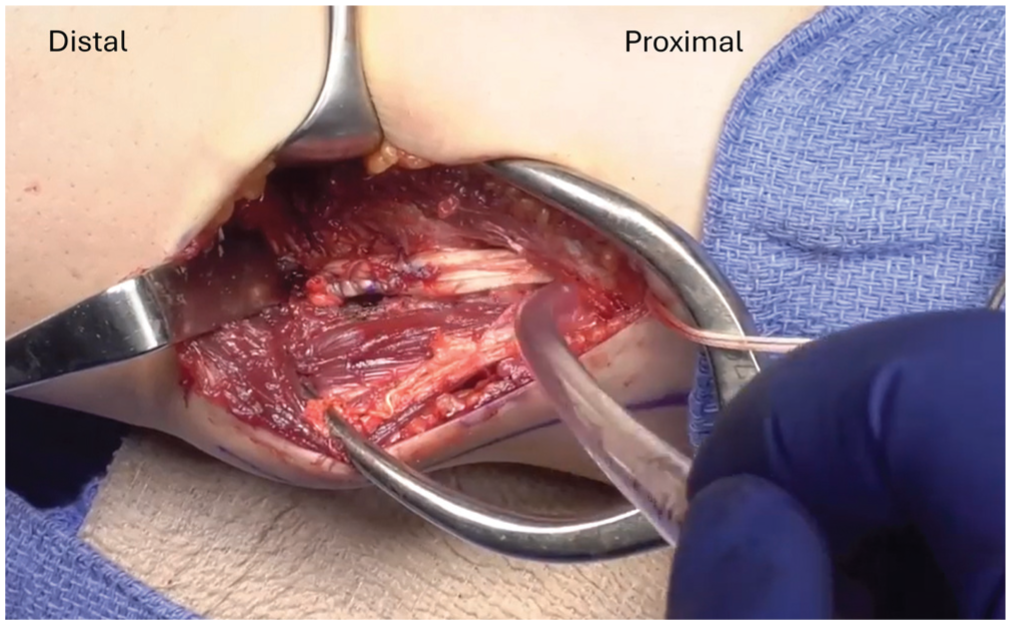
Right elbow demonstrates final graft reconstruction.
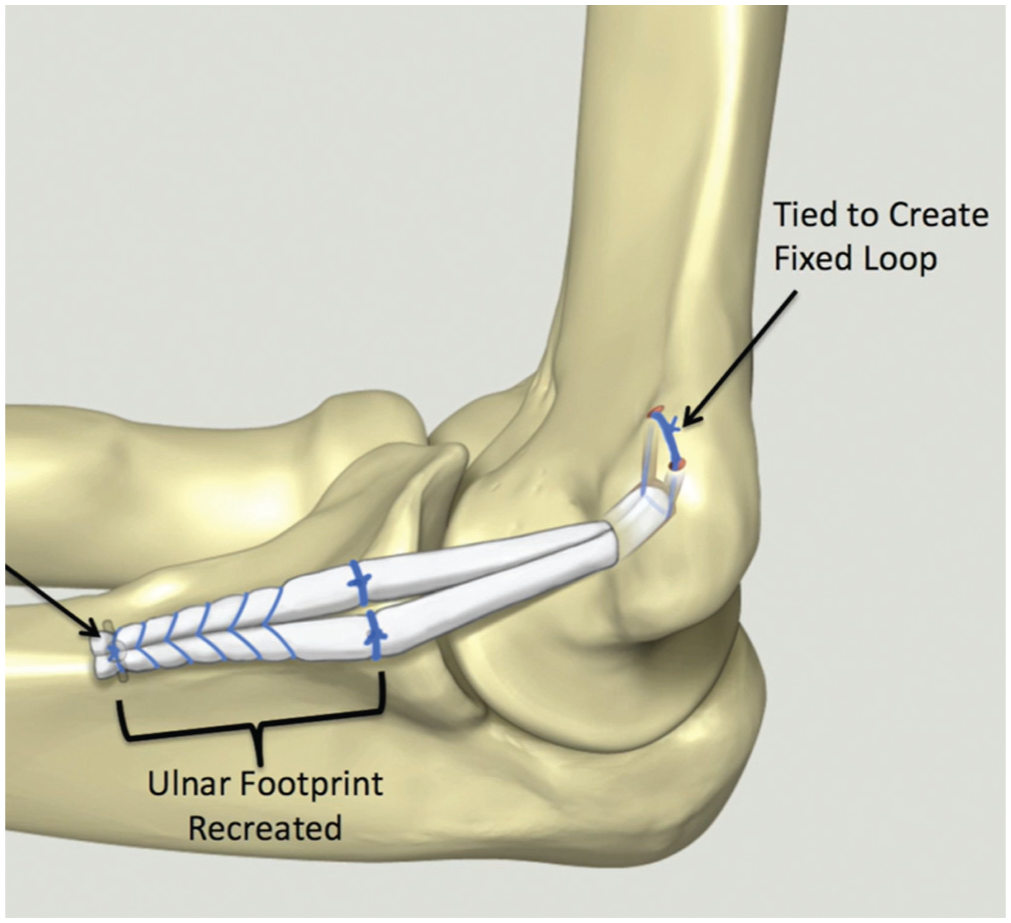
Illustration presents the anatomic reconstruction technique.
Postoperative Protocol
Postoperatively, all patients were started on the accelerated rehabilitation protocol. Upon completion of the procedure, patients were placed in a postoperative splint at neutral rotation and 49º of flexion with no elbow range of motion for 2 weeks. From weeks 2 to 6, they were placed in an unlocked hinged elbow brace and allowed to begin progressive pain-free passive range of motion with a goal of full active range of motion at 6 weeks as directed by pain. From weeks 6 to 12, a strength training protocol was initiated first with isometric exercises, progressing to 2 handed plyometrics. By month 3, patients began an interval throwing program and progressed to mound throwing at months 5 to 6. Overall, the return-to-play goal was 9 to 10 months postoperatively. If patients experienced any setbacks or were unable to tolerate the advanced protocol, their rehabilitation was slowed, and they transitioned to the standard MUCL rehabilitation protocol, which aims to return players to games by at least 12 months. A more in-depth view of the accelerated protocol can be seen in Figure 6.
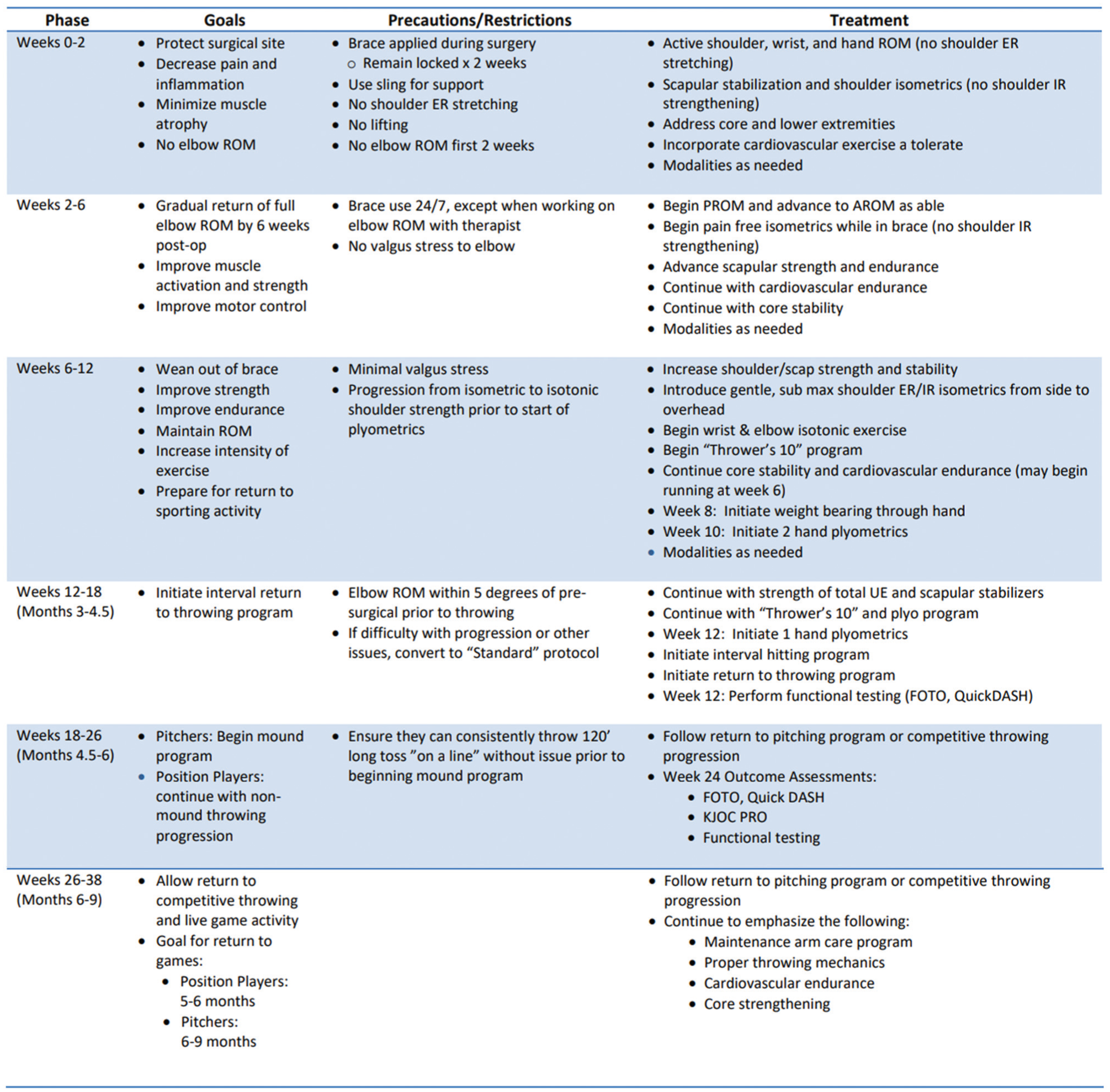
Accelerated rehabilitation protocol. AROM, active range of motion; ER, external rotation; FOTO, focus on therpeutic outcomes; IR, internal rotation; KJOC, Kerlan-Jobe Orthopaedic Clinic; PROM, patient-reported outcome measure; ROM, range of motion; UE, upper extremity.
Outcome Collection
Electronic patient medical records were reviewed to collect demographics, sports participation, injury characteristics, and surgical details. Preoperative PROs were also collected, including the Kerlan-Jobe Orthopaedic Clinic (KJOC) shoulder and elbow scores and Single Assessment Numeric Evaluation (SANE) score. Preoperative magnetic resonance imaging and clinical records were reviewed to identify tear type, location, and concomitant pathologies, including flexor/pronator involvement, ulnar nerve involvement, posteromedial impingement, and medial epicondyle fractures. Nonoperative treatment time was calculated as the time from the onset of symptoms to the date of surgery. Follow-up was calculated as the time from the date of surgery to the last clinical follow-up or questionnaire completion. Time to return to play was calculated as the time from surgery to the first game participation. Preinjury throwing velocity, mean spin, and horizontal movement were available for all professional athletes and some amateur throwers. This was collected once again after the athlete returned to play. Nonprofessional patients were contacted by phone or clinic appointment to collect return-to-play information and postoperative PROs. Data for the professional athletes were collected by members of the Minnesota Twins medical team.
Statistical Analyses
PROs were organized and analyzed in Microsoft Excel (2010; Microsoft Corp). Continuous variables were reported as means with standard deviations while categorical variables were recorded with associated percentages. Pre- and postoperative scores were compared by paired t tests. All statistical tests were 2-sided, and P values <.05 were considered statistically significant.
Results
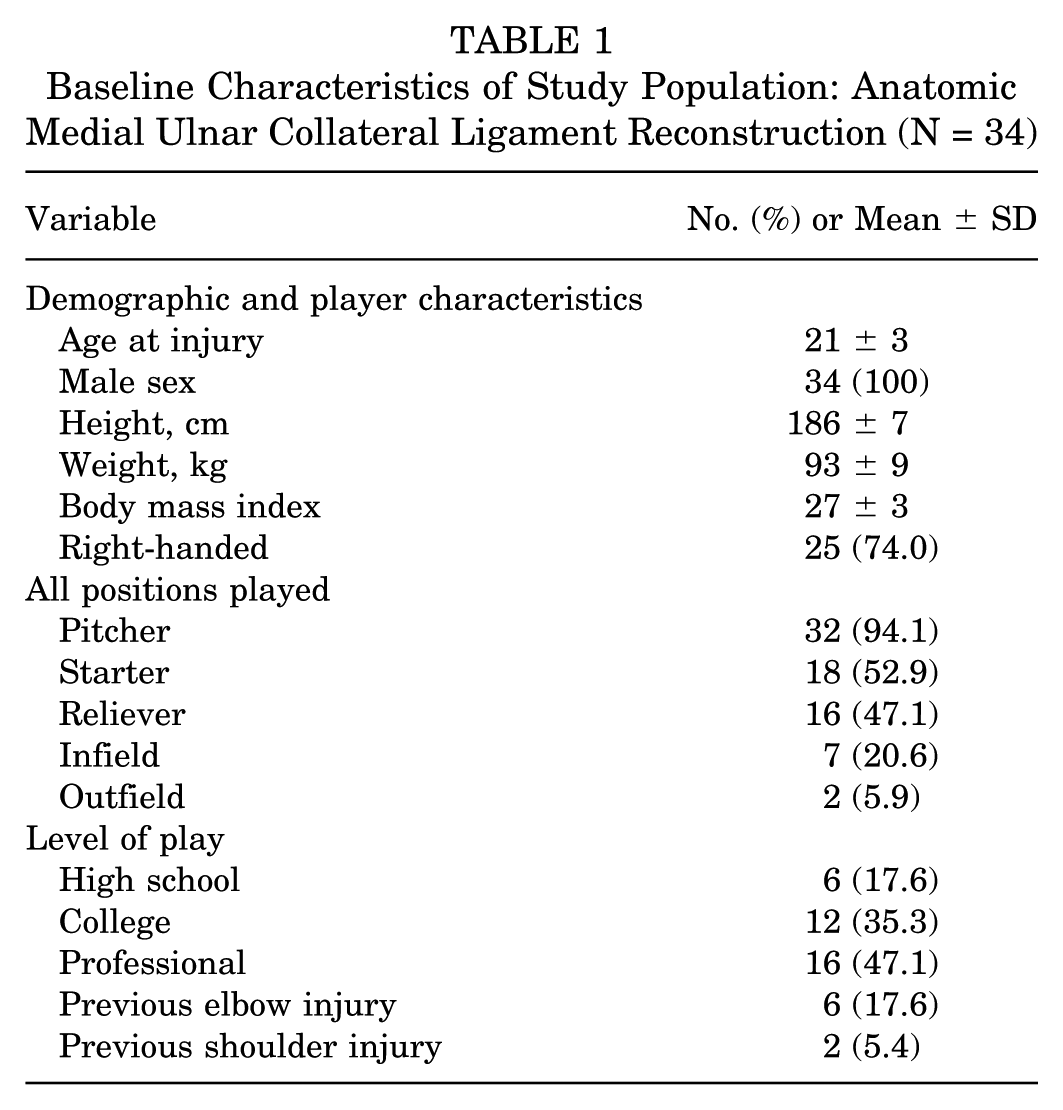
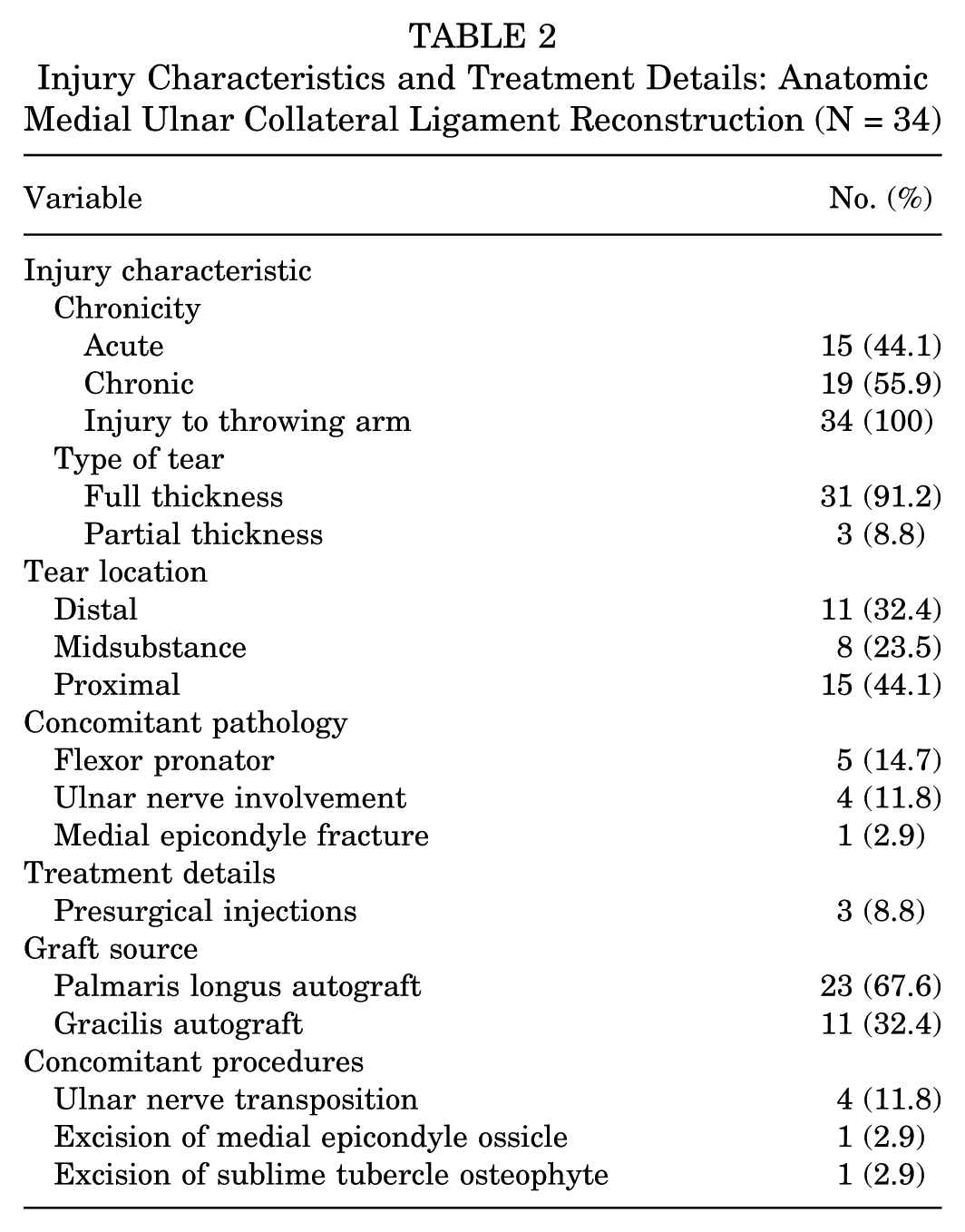
Among the 34 throwers included in our study, 16 (47%) played at the professional level and 32 (94%) were pitchers as their primary role. The mean age at injury was 21 ± 3 years with a mean follow-up of 36.1 ± 10.3 months. Fifteen (44%) throwers experienced an acute injury while the remainder had chronic pathology, which eventually required surgical management. Thirty-one (91%) injuries were full-thickness tears, 15 (44%) of which were proximal tears with 11 (32%) distal and 8 (24%) midsubstance. Concomitant pathology was seen in 10 (29%) throwers, with flexor/pronator injuries occurring in 5 (15%) and ulnar nerve involvement in 4 (12%). Of the patients included in the study, 6 (18%) had previous elbow injuries, 4 (12%) of which were partial MUCL tears treated nonoperatively and 2 (6%) were flexor/pronator tendonitis. Previous ipsilateral shoulder pathology was also reported in 2 (6%) athletes, which included a rotator cuff tear and biceps tendonitis.
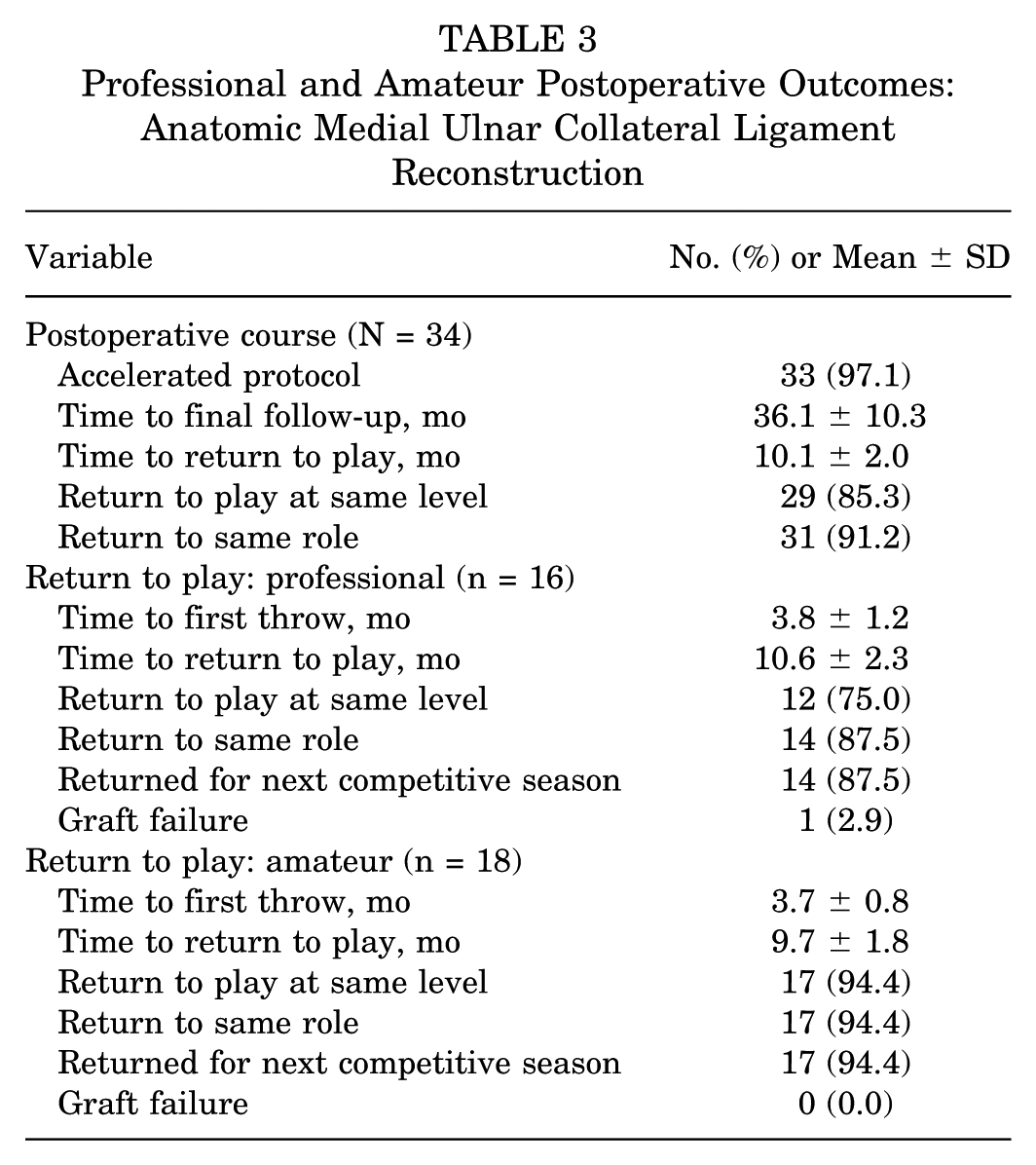
Palmaris longus autograft was used in 23 (68%) throwers and gracilis autograft in the remaining 11 (32%). Postoperatively, all patients were initially placed in the accelerated rehabilitation protocol, and 33 (97%) were able to complete it. Rehabilitation setbacks of some form were seen in 11 (32%) patients, with stiffness being the most common cause, which developed in 7 (21%) of the throwers. Postoperative ulnar neuropathy was seen in only 1 patient. These were all treated with continued physical therapy, and none required revision surgery for stiffness. The overall mean return to play was at 10.1 ± 2.0 months. On average, professional athletes’ first throw was 3.8 ± 1.2 months postoperatively with a mean time to return to play of 10.6 ± 2.3 months. Amateur throwers threw their first throw 3.7 ± 0.8 months postoperatively, returning to play at 9.7 ± 1.8 months. Twelve (75%) professional and 17 (94.4%) amateur throwers returned to the same or higher level. Fourteen (87.5%) professional and 17 (94.4%) amateur throwers returned to the same role (starter vs reliever). One of the professional pitchers required a revision MUCL reconstruction at 3 years postoperatively. For a complete evaluation of patient demographics, injury characteristics, treatment details, and postoperative course, see Tables 1 to 3.
Baseline Characteristics of Study Population: Anatomic Medial Ulnar Collateral Ligament Reconstruction (N = 34)
Injury Characteristics and Treatment Details: Anatomic Medial Ulnar Collateral Ligament Reconstruction (N = 34)
Professional and Amateur Postoperative Outcomes: Anatomic Medial Ulnar Collateral Ligament Reconstruction
PROs were gathered in 13 (81%) professionals and 18 (100%) amateur throwers. Postoperative PROs were significantly higher, with professional postinjury KJOC scores improving 42.6 ± 16 to 87.5 ± 8.3 (P < .001) and SANE scores improving 25.0 ± 11.2 to 95.6 ± 4.2 (P < .001). Amateur postinjury KJOC scores improved from 35.6 ± 10.7 to 90.9 ± 8.6 (P < .001) and SANE scores from 57.5 ± 16.9 to 95.2 ± 7.2 (P = .005). At a mean 24 months postoperatively, 13 professional and 17 amateur throwers had excellent results via the Conway-Jobe scale (Tables 4 and 5). For professional athletes, mean fastball velocity, spin rate, and horizontal and vertical movement were maintained with no statistical difference when compared with preinjury throwing characteristics (Table 6).
Professional Patient-Reported Outcome Measures: Anatomic Medial Ulnar Collateral Ligament Reconstruction a
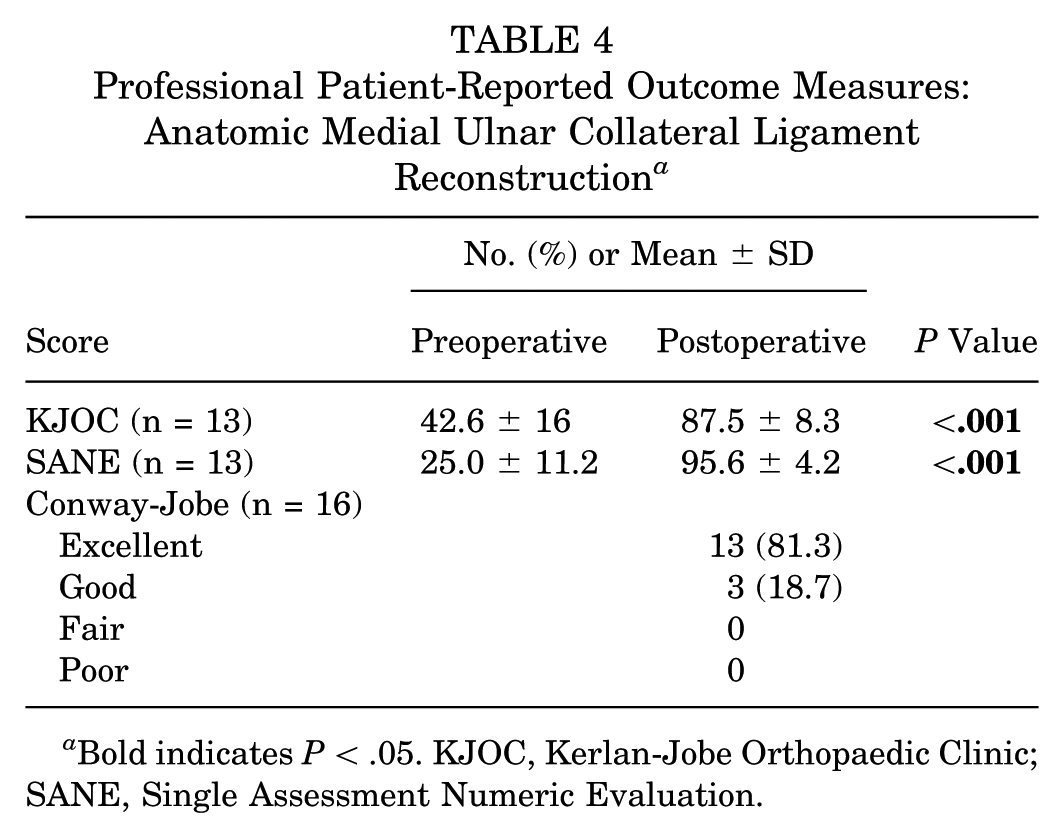
Bold indicates P < .05. KJOC, Kerlan-Jobe Orthopaedic Clinic; SANE, Single Assessment Numeric Evaluation.
Amateur Patient-Reported Outcome Measures: Anatomic Medial Ulnar Collateral Ligament Reconstruction (n = 18) a
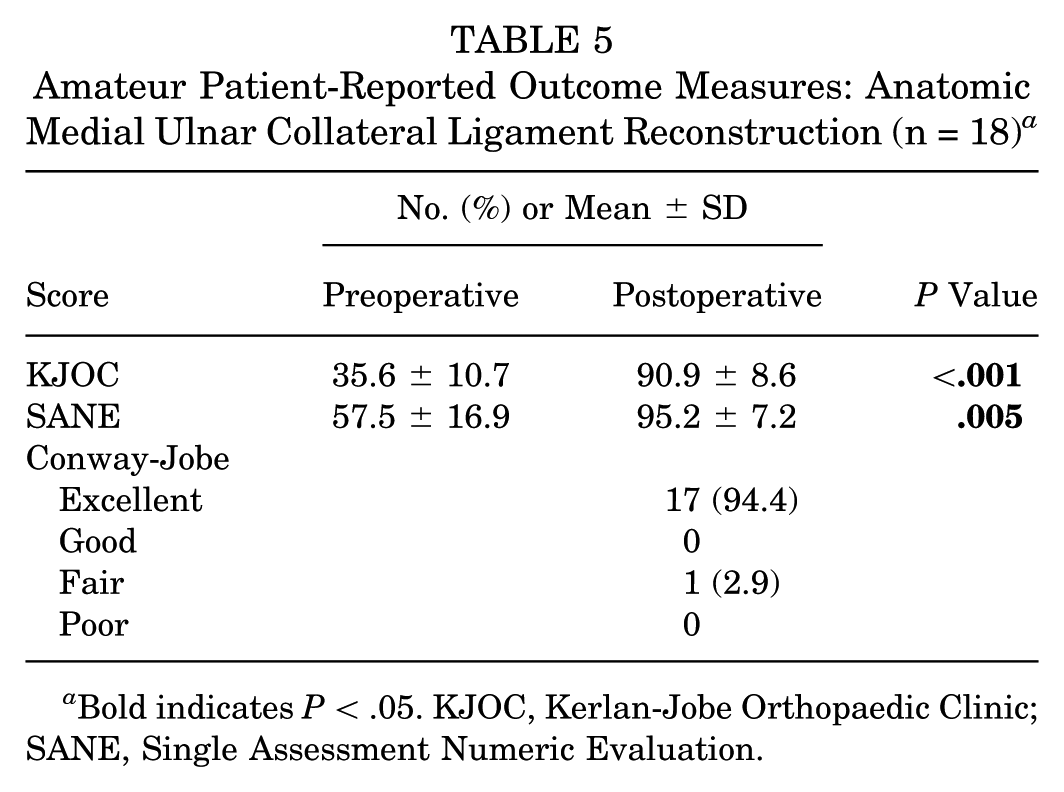
Bold indicates P < .05. KJOC, Kerlan-Jobe Orthopaedic Clinic; SANE, Single Assessment Numeric Evaluation.
Throwing Metrics for Professional Throwers: Anatomic Medial Ulnar Collateral Ligament Reconstruction (n = 11) a

Bold indicates P < .05. FB, fast ball.
Discussion
The current study is the first known study to provide clinical results for MUCL reconstruction using the anatomic technique with suture tape augmentation. Across these 34 players, 100% were able to return to play with 85% returning to the same or higher level of play. Only 1 (2.9%) player (professional pitcher) experienced a graft failure and required revision surgery. By utilizing this surgical technique in combination with an accelerated rehabilitation protocol, throwers at all levels were able to reliably return to play at a mean 10.1 ± 2.0 months after surgical management.
Despite multiple described techniques to reconstruct the MUCL, the majority experience similar return-to-play rates of 85% to 95%.4,5,8,13 In a systematic review of the modified Jobe versus docking technique, Looney et al 20 suggested that there was no significant difference in return-to-sport rate between the methods, reporting nearly a 75% return to the same level of play. The anatomic technique utilized in this cohort was first described in 2019 and seeks to re-create the native insertional footprint of the MUCL along the sublime tubercle and ridge and increase the overall amount of tendon-to-bone contact. Both of these are in an effort to maximize the biomechanical strength and the biologic healing potential. Biomechanically, this technique had superior strength and resistance to valgus torque when compared with the docking technique and similar strength to the native MUCL. 3 In our cohort, the anatomic technique with a suture tape augment resulted in all throwers returning to play, with 85% returning to the same level and 91% returning to the same position.
Although return-to-play rates have historically been reliable, timing of return to play remains a major barrier. Among professional baseball players, position players have been noted to return faster than pitchers, with a standard return to play of 11 to 12 months after surgery.5,26 Owing to the repetitive and increased force placed on the graft while pitching, historical return to play for pitchers can be delayed to 12 to 18 months postoperatively.5,26 Postoperative rehabilitation is a fine balance of progressing an athlete’s range of motion, strength, and function while giving the reconstructed ligament adequate time to heal. Ligament repair aims to utilize the body’s natural healing, often allowing for earlier return to play. However, in complete ruptures, especially among high-level throwers, reconstruction has been noted to provide more reliable outcomes, although return to play is often delayed as the body integrates the new tissue. 30 The anatomic technique seeks to utilize the native biology through ligament repair while providing an additional graft scaffold through ligament reconstruction. Additionally, suture tape augmentation has been noted to provide increased load to failure in the early stages of rehabilitation without overconstraining the elbow.1,21 Although a retensionable device was utilized in the anatomic technique, there is limited evidence demonstrating superior outcomes as compared with fixed-loop suture constructs, suggesting that a simple tied, nonretensionable loop may be equally effective. By improving the reconstructed ligament’s strength at time zero through the anatomic technique as well as suture brace augmentation, 97% of throwers were able to complete the accelerated rehabilitation protocol, initiating throwing on average 1 month faster than those in our standard rehabilitation protocol. Furthermore, as rehabilitation progressed, pitchers entered the mound throwing program at 4.5 months postoperatively as compared with 7 months in the standard protocol. The thrower who transitioned to the standard rehabilitation protocol returned to play 12 months after surgery. The 33 throwers who completed the accelerated protocol returned to play on average 10.1 ± 2.0 months after surgery.
While understanding the rate and timing of return to play is critical for throwers, functional outcomes after MUCL reconstruction remain the primary focus. In a systematic review of >1500 pitchers, Coughlin et al 9 reported that 79% to 87% of professional pitchers returned to preinjury levels; however, the majority of the studies reported a slight decrease in fastball velocity. Camp et al4 reported similar success in a systematic review of professional pitchers, finding an 80% rate of return to previous level of play and a 93% rate of survivorship at a mean follow-up of 4 years. Among our cohort, 85% reported a return to the same level of play and 91% were able to return to the same role. There were no statistically significant changes to pitch quality with regard to fast ball velocity, spin rate, horizontal movement, or vertical movement (Table 6). When compared with preoperative evaluation, all PRO measures significantly improved for professional and amateur throwers (Tables 4 and 5). Of the 34 throwers in our study, 1 did have a retear requiring revision surgery 3 years after primary reconstruction.
This study is not without limitations, which should be considered. Surgical procedures were performed by a single surgeon, which may limit the generalizability of the study. Additionally, performance data were not as readily available for amateur athletes; as such, it is not clear whether athletes earlier in their careers had similar progression in throwing performance as their peers with further maturation and training. Also, this study does provide insight into the short-term success of throwing athletes up to 3 years on average, but longer-term follow-up will be needed to determine the durability of the anatomic reconstruction technique with suture tape augmentation. Furthermore, with a cohort of 34 patients, larger studies will be valuable to better understand potential complications, delays in rehabilitation, and outcomes.
Conclusion
Anatomic reconstruction of the MUCL with suture tape augmentation is a viable option for MUCL injuries. This technique allowed an expedited return to sport (10.1 ± 2.0 months) for these baseball athletes with a low failure rate of 2.9%.
Footnotes
Submitted November 1, 2024; accepted September 5, 2025.
One or more of the authors has declared the following potential conflict of interest or source of funding: This study was partially funded by the National Institute of Arthritis and Musculoskeletal and Skin Diseases for the Musculoskeletal Research Training Program (T32AR56950). Its contents are solely the responsibility of the authors and do not necessarily represent the official views of the National Institutes of Health. Support was also received from the Foderaro-Quattrone Musculoskeletal-Orthopaedic Surgery Research Innovation Fund. C.L.C. receives consulting fees, hospitality, and education fees from Arthrex; other fees from Zimmer Biomet Holdings, Inc, and Gemini Medical LLC; publishing royalties, financial, or material support from Springer; and research support from Major League Baseball. J.S.D. receives consulting fees, hospitality, and education fees from Arthrex and other fees from Linvatec. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.