
Abstract
Background:
Despite the clinical and functional improvements exhibited by ulnar collateral ligament (UCL) reconstruction (UCLR), there is little published in vivo information pertaining to how UCLR affects medial ulnohumeral joint space gapping seen on stress ultrasound (SUS), which has been used as a surrogate for quantifying clinical instability.
Purpose:
To determine if UCLR results in a decrease in ulnohumeral joint space gapping as measured on postoperative SUS examination.
Study Design:
Prospective cohort study; Level of evidence, 2.
Methods:
Overhead throwing athletes were identified within an existing institutional review board–approved single-blinded, prospective, randomized controlled trial designed to assess treatment outcomes after modified Jobe or docking UCLR. Patients underwent a uniform surgical approach with pre- and postoperative (minimum of 1 year) radiographic assessment with SUS. Postoperative SUS ulnohumeral joint space gapping (delta) of the affected extremity was compared with the ipsilateral and contralateral preoperative values.
Results:
SUS results were available for 41 of 80 (51.2%; 20 modified Jobe and 21 Docking) patients with a mean age of 19.2 ± 1.9 years, including 93% baseball players. Joint space gapping as a result of the stress examination (delta) was 0.83 ± 0.53 mm for the contralateral reference elbow, 2.28 ± 1.26 mm for preoperative affected elbow baseline, and 0.69 ± 0.44 mm for the postoperative elbow at a minimum of 1 year after UCLR. UCLR resulted in a 330% decrease in the magnitude of joint gapping measured on postoperative SUS, with a mean decrease of 1.55 mm, and significant improvement irrespective of modified Jobe or docking technique (P < .001).
Conclusion:
UCLR returned average ulnohumeral joint space gapping to normal values on postoperative SUS. UCLR results in a mean decrease of joint space gapping from 2.28 ± 1.26 mm to 0.69 ± 0.44 mm. Regardless of technique, UCLR restored delta values to those comparable to the contralateral, unaffected elbow (0.83 ± 0.53 mm). Both techniques yielded mean gapping values <1.0 mm. These findings provide surgeons with the expected change in joint space gapping after UCLR, as measured on SUS. By providing a reference, surgeons can better interpret SUS results in patients with concern for recurrent UCL injury after reconstruction where magnetic resonance studies alone may be challenging to interpret.
The ulnar collateral ligament (UCL) is the primary static soft tissue stabilizer to valgus force during the late cocking and early acceleration phases of the throwing motion.1,2,19,24,27 For many overhead athletes, this ligament is subject to overuse injury with regular exposures to stress that frequently exceed its tensile strength. 1 This may lead to repetitive, microscopic tearing and, ultimately, ligament attenuation and failure. When valgus instability of the elbow is suspected based on history and examination, it is typically confirmed with advanced imaging. The traditional modalities of magnetic resonance imaging (MRI) and magnetic resonance arthrography (MRA) have good sensitivity and specificity for detecting UCL tears. 6 However, these studies are limited by an inability to stress the joint during imaging, thus providing only a static snapshot of a pathology that is functionally dynamic. Furthermore, although MRA provides greater sensitivity for the recognition of subtle findings such as partial-thickness UCL tears, it requires intra-articular contrast, which many athletes may wish to avoid.6,12,33 The novel FEVER (flexed elbow valgus external rotation) view for MRI offers promise in that it allows for assessment of the ulnohumeral joint and UCL under weighted stress 25 ; however, this view has not yet been extensively compared with physical examination and other diagnostic modalities utilized for the diagnosis of UCL tears and ultimately still yields a static stress image. In contrast, stress ultrasound (SUS) offers both a static and dynamic assessment of the UCL and ulnohumeral joint.3,4 This dynamic imaging modality allows for the magnitude of instability to be quantified by measuring ulnohumeral joint space gapping, both before and after the application of a valgus stress.8,12 The dynamic assessment of ulnohumeral joint gapping using SUS has been validated and demonstrated to be reproducible and reliable for both partial and complete UCL tears.8,9,11,12,21,22
For overhead athletes, UCL reconstruction (UCLR) has yielded a relatively high rate of return to sport for high-performing patient populations.15,16 Despite the clinical and functional improvements exhibited by UCLR, there is scant published in vivo data demonstrating how UCLR affects postoperative ulnohumeral joint space gapping. Data on baseline values, presurgical values, and post-UCLR values for ulnohumeral joint gapping within a well-controlled population would add valuable, practical information regarding SUS examination, UCLR, and the effective change it produces regarding ulnohumeral joint space gapping. This information would be potentially invaluable when assessing for recurrent UCL injury after previous UCLR. We hypothesized that UCLR would result in a decrease in ulnohumeral joint space gapping seen on SUS examination at the 1-year follow-up compared with the preoperative, injured state.
Methods
The original study was a prospective, randomized controlled trial designed in accordance with the CONSORT (Consolidated Standards of Reporting Trials) statement. Postoperative imaging performed was a secondary outcome measure. The study was approved by our institutional review board (IRB) (TJUH IRB Control No.: 16D.028) on January 7, 2016. All patients, and their parents in the case of minors, were counseled and provided formal written informed consent.
Patient Population
As noted above, patients were identified within an existing IRB-approved single-blinded, prospective, randomized controlled trial designed to assess treatment outcomes after modified Jobe or docking UCLR. This population consisted of skeletally mature overhead throwing athletes (any level, ie, recreational, high school, collegiate, and professional) with a diagnosis of UCL injury involving either a complete UCL tear or a partial UCL tear that failed nonoperative management. Patients with a history of a previous ipsilateral elbow surgery (UCLR, ulnar nerve transposition, flexor-pronator debridement, posteromedial impingement debridement, or elbow fracture fixation), those who lacked clinical or imaging evidence of a UCL tear, or those who were nonthrowing athletes were all excluded.
Preoperative Evaluation
All patients underwent a thorough physical examination of the neck, shoulder, elbow, and kinetic chain preoperatively. A thorough assessment of elbow stability was conducted, including varus and valgus stress at 0° and 30° of elbow flexion, moving valgus stress, and milking maneuvers. Additionally, the function and stability of the ulnar nerve were evaluated by assessing for numbness and paresthesia in the ulnar nerve distribution at rest, with ulnar nerve compression testing, and Tinel testing at the elbow. Those patients who demonstrated significant ulnar nerve subluxation or reported ongoing ulnar nerve–related symptoms underwent concomitant subcutaneous ulnar nerve transposition at the discretion of the treating surgeon. All patients underwent preoperative imaging in the form of MRI or MRA and SUS to further characterize the integrity of the UCL.
UCL Surgical Technique
All UCLRs were performed by a single board-certified, sports medicine fellowship-trained orthopaedic surgeon (M.G.C.) who performs a high volume of UCLRs (50-70 procedures) each year, with ample clinical and research experience in both the modified Jobe and docking techniques. For all procedures, regardless of technique, a standardized gracilis tendon autograft was harvested from the contralateral leg to reduce sources of variability/confounding. This graft choice was chosen as some patients may lack a palmaris longus tendon. 36
The randomized, assigned surgical technique to be performed was disclosed to the surgeon on the morning of surgery, but the patient remained blinded throughout the study. The modified Jobe and docking techniques were performed as previously described with the use of contralateral gracilis autograft.7,10 For the modified Jobe technique, the graft was passed in a figure-of-8 configuration and sutured to itself while the elbow was maintained at 30° of flexion, neutral forearm rotation, and slight varus. For the docking technique, both ends of the graft were prepared with No. 2 FiberWire (Arthrex) passed in modified Krackow fashion (4-5 throws spanning 1 cm in length on each end of the graft) and subsequently docked into the humeral tunnel. Docking sutures were tied over a humeral bone bridge with the same elbow and arm positioning described above for the modified Jobe technique.
For both techniques, the anterior and posterior limbs of the native UCL were oversewn to the limbs of the graft using No. 1 Vicryl. Specifically, the No. 1 Vicryl suture was passed through the anterior limb of the native UCL, followed by the anterior and posterior limbs of the graft, and then carefully through the posterior limb of the native UCL in an interrupted figure-of-8 fashion spanning from the sublime tubercle to the medial epicondyle for both the modified Jobe and docking techniques. Identical layered closures were performed for both procedures, including closure of the flexor-pronator fascia. All patients were placed in a splint with 90° of elbow flexion and neutral forearm rotation at the conclusion of the procedure. All patients completed a standardized, previously published UCLR rehabilitation protocol, 1 including short toss beginning at 4 to 5 months with progression of long toss as tolerated. Pitchers began a mound program on completion of long toss, typically by 6 to 8 months. 10 All patients were followed for a minimum of 2 years after reconstruction. 20
Imaging
All patients underwent uniform preoperative radiographic assessment including MRI or MRA and SUS. Postoperative imaging included both MRI and SUS performed at a minimum of 1 year after surgery. Patients who lacked SUS data were excluded.
SUS Technique
SUS and ulnohumeral joint gapping measurements were performed by, or directly supervised by, 1 of 2 fellowship-trained musculoskeletal radiologists using a previously published technique.3,4,9-12,22,31 SUS was performed using a 5- to 15-MHz ultrasound transducer with a longitudinal orientation for imaging of the ulnohumeral joint. The patient was positioned with the arm resting comfortably at or slightly above waist height on a well-padded table and the elbow at approximately 30° of flexion with the forearm in supination and the shoulder relaxed. A rolled towel or “bump” was placed proximal to the elbow to provide support during the examination. During the initial measurement of ulnohumeral joint space, no stress was applied to the joint while images were captured. The distance from the trochlea to the sublime tubercle was measured using integrated electronic calipers. An instrumented valgus stress was then applied to the elbow via a Telos device, and an image of the stressed joint was captured with the joint space measured in the same manner as above. Instrumented stress allows a standardized force to be applied, and the authors prefer application of 15 daN of stress. Each measurement was repeated 3 times and mean values were calculated. The change in the joint space gapping due to stress application (delta) was then calculated by subtracting the mean joint space at rest from the mean joint space under valgus stress (Figure 1). It is customary for our radiologists to report the calculated delta values for a given elbow rather than each individual measurement. Interclass and intraclass correlation coefficients were not calculated in the present study in light of the previous establishment of high intraobserver and interobserver reliability of SUS.5,17,31,32,34
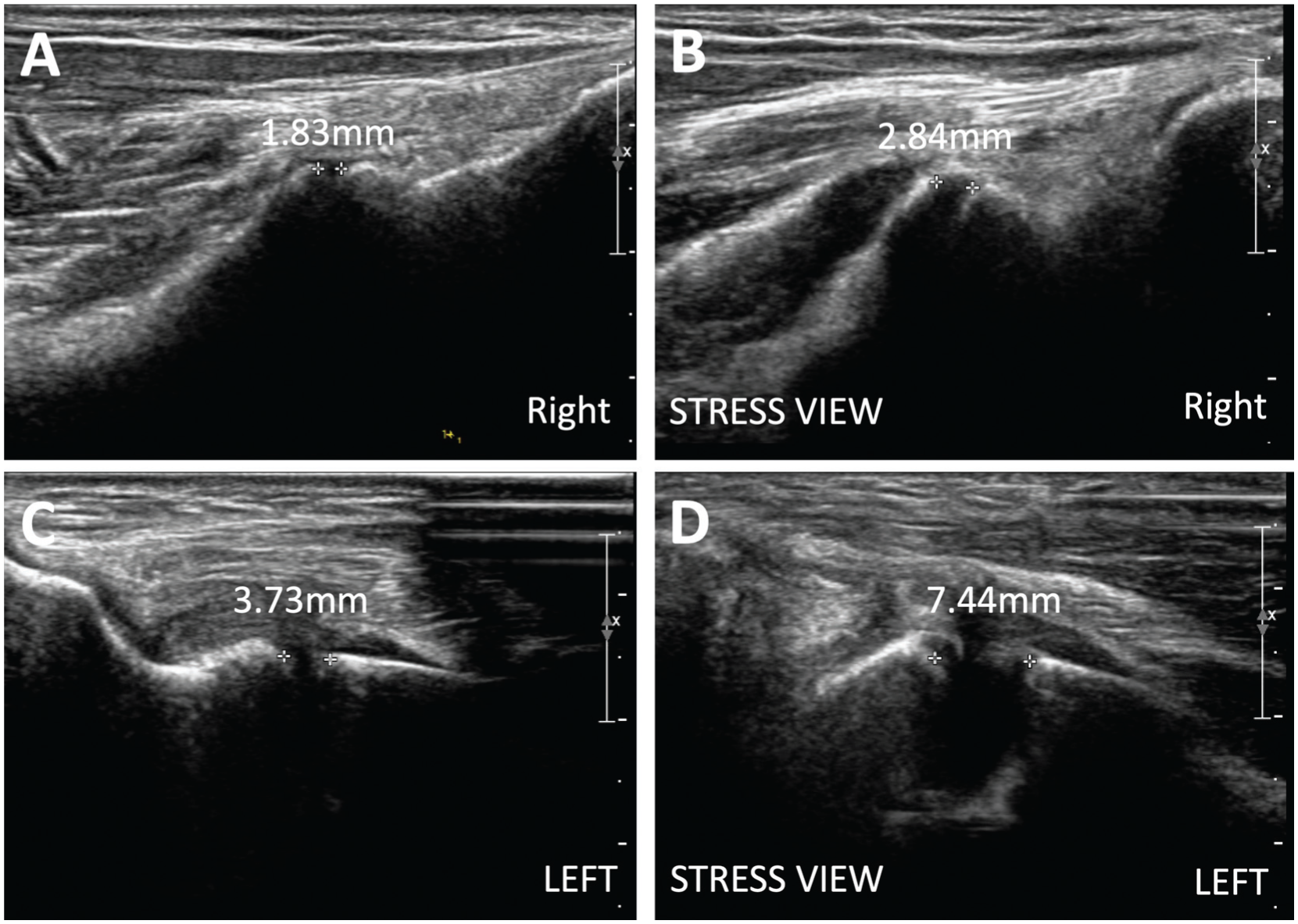
Assessment of ulnohumeral joint space gapping by stress ultrasound examination. Ulnohumeral joint space gapping is shown and measured for (A and B) the contralateral unaffected elbow and (C and D) the affected injured elbow. Images A and C show the ulnohumeral joint space in the resting state, while images B and D show a state when a standardized valgus force was applied. To determine the change in joint space, or delta, for a given elbow, both the resting and the stressed ulnohumeral joint space gap distance (the distance between the crosshairs) are repeated 3 times and the mean resting value is subtracted from the mean stressed value.
Statistical Analysis
Analysis was conducted using IBM SPSS Statistics (Version 29.0.1.0), utilizing 2-tailed independent t tests to compare population means, 2-tailed paired Student t tests for assessments of patients over 2 different time points, and 2-tailed 1-sample t tests to compare the effect of UCLR to a reference population mean. Receiver operating characteristic (ROC) analysis was conducted to determine the cutoff delta value(s) that discriminated between the injured elbow before UCLR and the contralateral reference elbow, and the area under the curve (AUC) was determined.
Results
Of the 80 patients who were randomized in the prospective trial, 57 patients had SUS data available for inclusion in the present study. Sixteen patients were excluded who did not have contralateral measurements for the uninjured elbow available for a comparison control reference, leaving 41 patients for analysis. Of the 41 patients who received UCLR, 20 underwent the modified Jobe technique and 21 the docking technique (Figure 2). The mean age was 19.2 ± 1.9 years, and all patients were overhead athletes. Baseline patient characteristics for all patients and subgroups can be found in Table 1. SUS findings available for the 41 patients included 100% (41/41) preoperative baseline SUS examinations; 100% (41/41) reference preoperative SUS examinations on the contralateral, uninjured elbow; and 61.0% (25/41) with a minimum of 1 year after UCLR SUS examination.
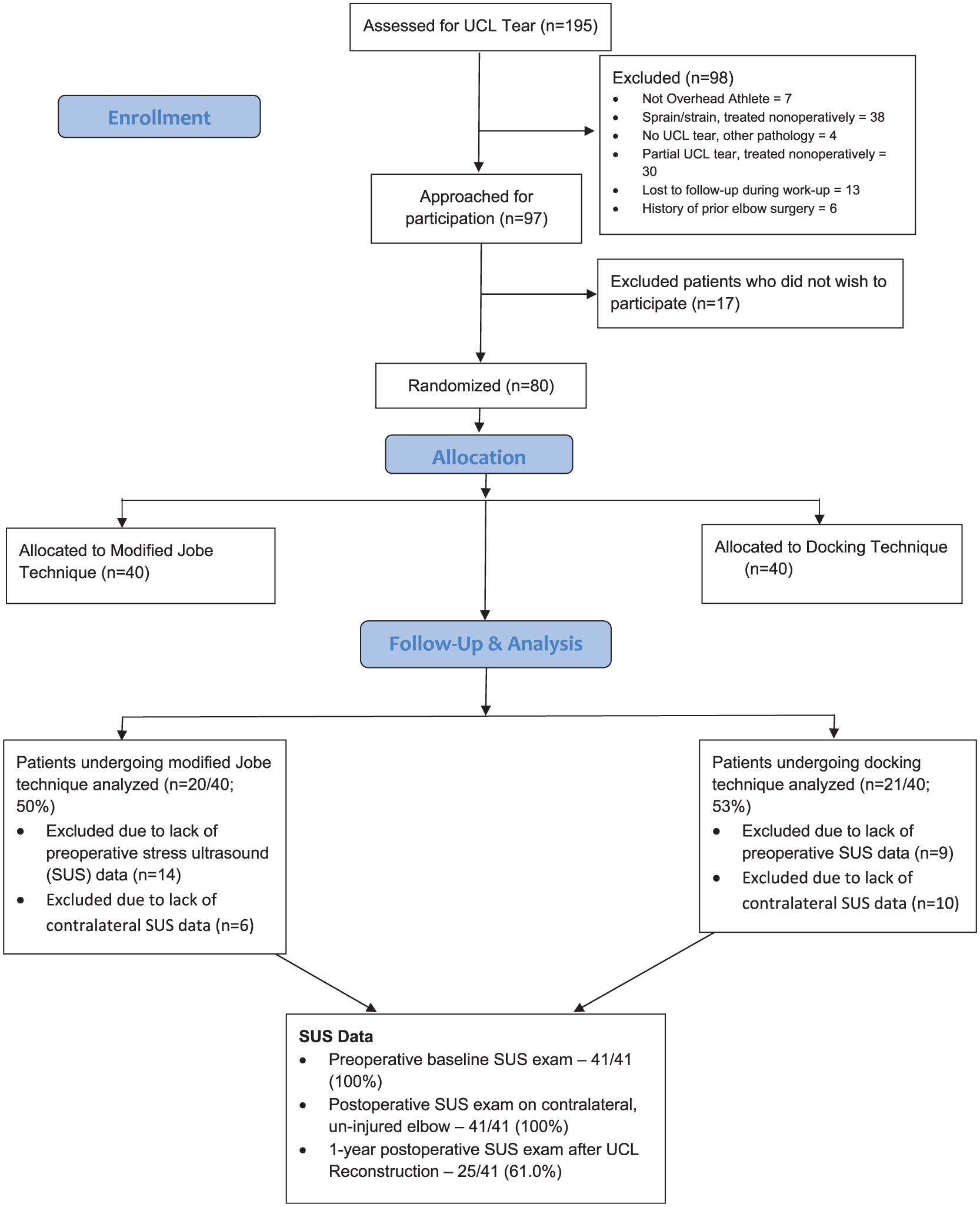
Study flow diagram. SUS, stress ultrasound; UCL, ulnar collateral ligament.
Baseline Characteristics for Patients a

Continuous data are reported as mean ± SD. Categorical data are reported as count (n). UCL, ulnar collateral ligament.
Delta SUS Descriptive Data
The mean amount of joint space gapping as a result of applied stress (delta) was 2.28 ± 1.26 mm for the preoperative injured elbow, 0.83 ± 0.53 mm for the contralateral uninjured reference elbow, and 0.69 ± 0.44 mm for the postoperative reconstructed elbow at a minimum of 1 year after UCLR. Table 2 shows postoperative delta values compared with the preoperative contralateral and ipsilateral values, respectively.
Postoperative Delta Values Compared With Preoperative Contralateral and Ipsilateral Values a
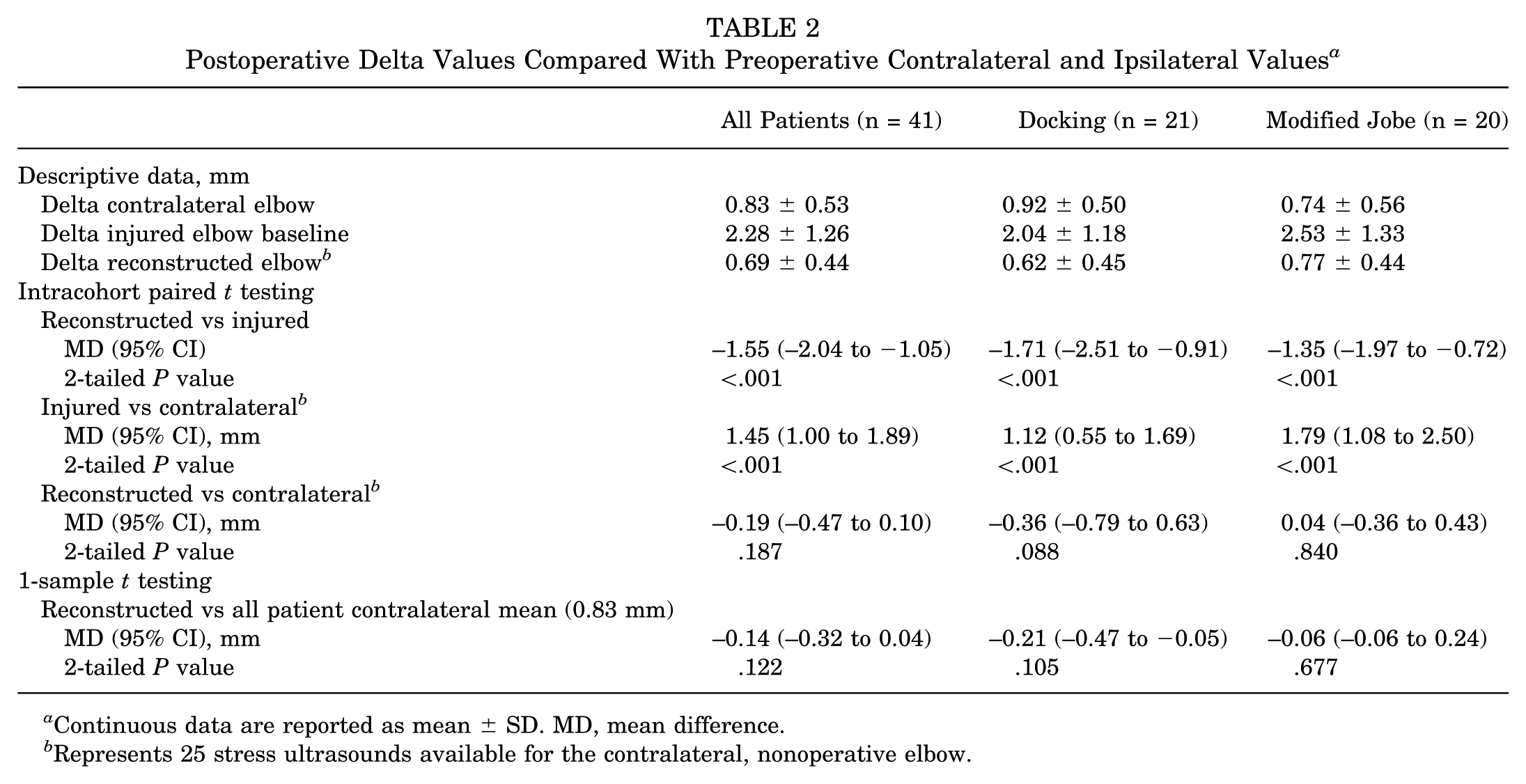
Continuous data are reported as mean ± SD. MD, mean difference.
Represents 25 stress ultrasounds available for the contralateral, nonoperative elbow.
Delta SUS: Preoperative and Postoperative Ipsilateral Comparisons
UCLR resulted in an approximately 330% decrease in the magnitude of joint space gapping measured on postoperative SUS, representing a mean decrease of 1.55 mm. UCLR restored ulnohumeral joint space gapping to values comparable to those of a native, uninjured elbow. There was significantly less joint gapping seen on SUS examination at time points ≥1 year after UCLR (0.69 ± 0.44 mm) compared with the preoperative SUS examination of the elbow (2.28 ± 1.26; P < .001). This was true irrespective of the procedure; the Docking technique resulted in a mean decrease in ulnohumeral gapping of 1.71 mm (95% CI, 0.91-2.51 mm; P < .001), and the modified Jobe technique decreased gapping by a mean of 1.35 mm (95% CI, 0.72-1.97 mm; P < .001) on paired analyses (Table 2).
Delta SUS: Contralateral Preoperative and Ipsilateral Postoperative Comparisons
Considering all patients with UCLR, 2-tailed 1-sample t testing found no difference in joint space gapping present in the minimum 1-year postoperative cohort (0.69 ± 0.44 mm; P = .122) compared with the selected mean of the contralateral reference (0.83 mm). Subanalysis via 2-tailed 1-sample t testing showed no statistical difference in gapping at 1 year postoperatively for the docking group (P = .105) or the modified Jobe group (P = .677) when compared with the reference mean of 0.83 ± 0.53 mm.
ROC Analysis
ROC analysis identified a cutoff delta value of 1.20 mm as having the best overall performance (Youden index, 0.61; AUC, 0.88; 95% CI, 0.80-0.95). This cutoff value of 1.20 mm had a sensitivity of 78% and a specificity of 83% for detecting injured UCL among contralateral controls. The nearest cutoff value to 1.0 mm greater than the contralateral reference mean was 1.95 mm, which had a specificity at 95% and a sensitivity of 59%.
Discussion
The current study utilized SUS results at a minimum of 1 year after surgery to confirm that UCLR, regardless of modified Jobe or docking technique, does reduce ulnohumeral joint space gapping (delta) compared with preoperative values. Both techniques were successful in at least restoring gapping to a range assumed to reflect the normal state. The present study affords surgeons with an objective, quantitative confirmation of the restoration of ulnohumeral joint stability after UCLR as detected by SUS. Evaluation at a minimum of 1 year after UCLR demonstrates that the reduction in joint space gapping produced by surgery was maintained throughout the rehabilitation period. Furthermore, one of the most challenging diagnostic scenarios among overhead throwing athletes is evaluation of possible reinjury after previous UCLR. In the setting of previous UCLR, MRI and MRA can be challenging to interpret given the presence of scar, graft, and suture material susceptibility. SUS continues to serve as an excellent adjunctive imaging evaluation. The current study provides surgeons with an invaluable method for establishing the diagnosis of recurrent UCL injury with substantially increased certainty. The current study suggests that if SUS reveals a delta >1.2 mm, the UCLR is potentially compromised; however, this cutoff value has only modest sensitivity (78%) and specificity (83%). However, for delta values that exceed the contralateral reference elbow by >1.0 mm, for which the nearest cutoff value in the present study was an absolute value of 1.95 mm, there was a much higher specificity (95%). An absolute cutoff delta value of 1.95 mm still exhibited a sensitivity of 59%.
There is scant published literature on the optimal postoperative imaging assessment of the reconstructed UCL. Wear et al 37 highlighted the utility of MR arthrograms when assessing symptomatic, reconstructed UCLs. However, the authors warned that non–contrast-enhanced imaging can be more limited in diagnostic value. The authors also stressed the notion that well-recognized indicators of abnormal native UCL injury, such as the “T-sign,” ligament thickening, and heterotopic ossification, may not confer the same diagnostic utility in the setting of previous UCLR. 37 As seen after anterior cruciate ligament reconstruction, signal uptake within the graft can vary based on timing after surgery, which can be misleading, often detracting from the utility of a postoperative MR study. 13 The FEVER view for MRI potentially offers a more comprehensive evaluation of the UCL and underlying ulnohumeral joint. The FEVER view has been correlated with level of play and endurance statistics in professional pitchers 30 and may prove to be a valuable addition to traditional MRI of the athlete’s elbow.3,4,25 While FEVER MRI offers promise, this imaging technique may be limited for the following reasons: the space constraints in an MRI system, its dependence on imaging variables such as slice selection and image angle, the inconsistent precision of the application of stress with weight compared with that of an instrumented device such as the Telos utilized with SUS, its provision of a single image without comparison with previous imaging or the contralateral elbow, and its potentially limited interpretation without inclusion of contralateral imaging or established thresholds for normal/abnormal. Ultimately, FEVER MRI has not yet been rigorously compared with SUS, physical examination, or other diagnostic modalities to determine its sensitivity or specificity for diagnosing UCL tears. Furthermore, traditional MRI or MRA and FEVER MRI provide only single static snapshots of the ligament that may be challenging to interpret due to the presence of scar, graft, and suture susceptibility and do not provide dynamic, functional data regarding the stability of the ulnohumeral joint.
The ability to dynamically assess the integrity of a reconstructed graft and the valgus stability of the ulnohumeral joint makes SUS an adjunctive imaging study worth considering. 14 A small number of previous studies have utilized SUS in assessments after UCLR; however, none have quantitatively assessed the ulnohumeral joint. Merolla et al 26 performed postoperative radiographic imaging and ultrasound, including SUS, at a mean follow-up of 36 months after UCLR utilizing either the modified Jobe or docking technique. However, the reported results were strictly qualitative and fell short of providing clinicians with an expected reference range of ulnohumeral joint space gapping. 26 Regarding SUS, the authors’ reported findings were limited to qualitative assessments such as “all the grafts assessed appeared anatomically intact” and “dynamic ultrasonography assessment … demonstrates slight medial laxity with valgus stress maneuver without pain or other signs of medial instability.” The authors did not provide additional quantification of these results. 26 Park et al 29 performed sequential postoperative static ultrasonography and valgus stress radiographic imaging at 3 and 12 months postoperatively in 17 elite and professional baseball players after UCLR. The authors reported that the reconstructed grafts were well maintained on static US in all 17 players; however, 8 of 17 (47%) of these players could not return to their preinjury level of performance. This low rate of return to performance despite the appearance of an intact graft on static imaging suggests that dynamic imaging via SUS may offer some degree of additional utility compared with static ultrasound imaging in reliably assessing the postoperative restoration of ulnohumeral joint stability.
Dynamic assessment of ulnohumeral joint laxity in the injured state using SUS has been validated in cadaveric models in which transection of the anterior bundle of the UCL results in an increase in joint space gapping ranging from 1.7 to 3.4 mm compared with an uninjured ligament.9,21 The current study identified a mean preoperative delta for the injured elbow of 2.28 ± 1.26 mm, which is in agreement with the findings in the aforementioned studies. Several studies, including 2 cadaveric studies with sequential sectioning of the UCL and 1 in vivo study involving longitudinal analysis of professional baseball pitchers, have suggested that the clinically significant threshold for UCL injury is ipsilateral ulnohumeral joint space gapping >1 to 2 mm (presectioning vs postsectioning in cadaveric studies) on SUS.8,9,12 Furthermore, utilizing delta thresholds >1 mm compared with the uninjured contralateral elbow on SUS has been shown to be 96% sensitive, 81% specific, and 87% accurate for the diagnosis of UCL tear. 31 The present study found that uninjured contralateral control elbows demonstrated delta values of 0.83 ± 0.53 mm. With 1.95 mm being the nearest cutoff value ≥1.0 mm greater than the mean value for the uninjured elbows, we found this absolute threshold to be more suggestive of a higher specificity (95% vs 81%), but a reduced sensitivity (59% vs 96%). The additional 1.45 mm of gapping for the injured UCL elbow compared with the contralateral control elbow in the present study corroborates the findings of Roedl et al, 31 but demonstrates a more modest sensitivity. The increased sensitivity of the finding of Roedl et al could be related to an increased proportion of full-thickness (complete) UCL tears in their study population in comparison with ours (35% vs 29%). Based on previous cadaveric sectioning studies, it is plausible to conclude that complete UCL injury would result in a larger magnitude of ulnohumeral joint space widening with valgus stress than a partial-thickness injury, and thus the proportion of partial-thickness and full-thickness injuries in a given data set will then influence cutoff values. The present study adds to the current body of literature by providing sensitivity and specificity values for absolute delta values at 2 different thresholds based on the diagnostic needs of the examiner. Values >1.95 mm have a very high specificity for injury, and values above this threshold have a high probability of representing a definitive injury. Delta values >1.20 mm have a reasonable probability of identifying UCL injuries while also maintaining a pragmatic degree of specificity.
Despite the above listed thresholds proving beneficial for diagnostic purposes pre-UCLR, post-UCLR ulnohumeral gapping and the magnitude of quantitative restoration of ulnohumeral stability have not yet been thoroughly detailed. The present study is the first to demonstrate that ulnohumeral joint space delta decreases approximately 330% after UCLR (mean decrease of 1.55 mm) and is maintained at a minimum of 1 year after the procedure. This held true for both the docking and modified Jobe techniques, both of which exhibited a significant decrease in post-UCLR delta compared with the preoperative injured elbow. These findings, albeit intuitive, are now quantified and confirmed.
The current study found that post-UCLR delta (0.69 ± 0.44 mm) exhibited no statistical difference when compared with the contralateral, uninjured reference elbow (0.83 ± 0.53 mm) on both paired t testing (P = .187) and 1-sample t testing (P = .122). Applying rigorous exclusion criteria certainly limits the power of this assessment, and thus a lack of significance does not suggest that there is not a substantial difference or large effect size between the gapping of the reconstructed elbow and the contralateral uninjured elbow. All assessments and subgroup assessments trended toward reconstructed elbows approaching statistically less gapping than the contralateral reference elbow, but this was not significant, and we cannot draw any conclusions as to whether the reconstructed elbow should gap any less than the contralateral reference. This information does, however, suggest that reconstruction should result in ulnohumeral joint space gapping delta values that approximate those in the uninjured contralateral elbow, with values >1 mm after UCLR being considered as potentially abnormal, particularly in the clinical context where reinjury is being evaluated. Evaluating the delta value of the contralateral uninjured elbow could serve as a reference to compare values when there is concern for reinjury after reconstruction.
The current study has several strengths. To our knowledge, this is the first study to quantitatively assess ulnohumeral joint space gapping via SUS after UCLR, and thus the first study to propose expected values for such joint gapping. The current study utilizes prospectively collected data. The 2 most common surgical techniques for UCLR, modified Jobe and docking, were both included, increasing applicability. All surgeries were performed by a single, highly experienced surgeon utilizing a uniform surgical approach, uniform autograft, and uniform postoperative rehabilitation. Utilization of in-office ultrasound is rising in popularity among orthopaedic surgeons,28,38 and the findings of the present study could help equip the trained orthopaedic surgeon with a validated, reliable means of efficiently diagnosing and stratifying a UCL injury. However, for the purposes of this study, all SUS examinations were performed or directly supervised by fellowship-trained musculoskeletal radiologists highly experienced in the technique. Finally, postoperative SUS was performed at a minimum of 1 year postoperatively. The mean time to return to full sport participation in this cohort was between 12 and 13 months, 10 suggesting that the reduction in joint space gapping achieved by UCLR is maintained throughout the early rehabilitation, tossing program, mound pitching, and even after initiation of full sport participation for some patients.
Limitations
The current study is not without limitations. First, SUS and US in general do not provide the high-level image quality to directly visualize a reconstructed graft when compared with traditional MRI and MRA or FEVER MRI and have historically been noted to be possibly technique and user dependent. 18 Some technical factors that must be accounted for when performing SUS include elbow flexion angle, magnitude of valgus stress applied, and consistency of measurement landmarks between baseline and stress measurements, 35 as all of these may influence the degree of ulnohumeral gapping found on SUS or any imaging modality assessing joint space gapping. All SUS evaluations in the present study were performed or directly supervised by 1 of 2 highly experienced musculoskeletal radiologists who are well versed in performing this diagnostic technique. While intraclass correlation coefficients were not specifically calculated in this study, high intrarater and interrater reliability have been demonstrated when these examinations are performed by experienced ultrasonographers.5,17,31,32,34 Radiologists or clinicians with a high level of experience may not be widely available at all institutions or practice settings, which may limit the generalizability of this study’s findings. However, in a cadaveric model Ferreira et al 18 found that UCL thickness measurements exhibited excellent and satisfactory agreement among radiology residents and with those acquired from an experienced radiologist who was well versed in ultrasound. Given the ideal location of the UCL with minimal overlying soft tissue and readily apparent bony landmarks, it is plausible that assessments in this anatomic region can be adequately performed by radiologists despite not necessarily having a robust background in clinical ultrasonography.
Second, the current study utilized a gracilis autograft in all patients. This was a conscious decision to reduce sources of variability for a prospective, randomized controlled trial since some patients lack a palmaris longus. 36 As a result, the findings of the current study may not be generalizable to all graft sources. While this may be a focus for future study, the authors would hypothesize that no clinically significant difference would be seen between gracilis and palmaris longus autografts regarding post-UCLR ulnohumeral joint gapping.
Additionally, while patients were clinically followed for a minimum of 2 years in this randomized controlled trial, not all patients received radiographic follow-up with SUS at 2 years. This was particularly impacted by the onset of the 2020-2021 COVID pandemic during the course of the trial. Therefore, patients with postoperative SUS performed at a minimum of 1 year postoperatively were included, and given the longest time to return to play occurring in pitchers, which frequently occurs between 12 and 18 months, 23 this follow-up period was believed to be sufficient to assess for the graft’s response to the stresses of rehabilitation and early return-to-sport participation. Furthermore, SUS assessment at a time point after at least 1 year of rehabilitation would likely adequately reflect restoration of a functional state similar to that expected at the time of release to full activity and potential subsequent reinjury. Finally, only 51.2% (41/80) of the initially enrolled patients received contralateral SUS, which resulted in only 61% (25/41) of these patients, specifically only 31% (25/80) of the originally enrolled cohort, additionally having both pre- and postoperative SUS values. This represents the challenges of coordinating long-term postoperative imaging of the affected extremity, let alone that of the contralateral extremity. However, the contralateral SUS performed and analyzed in the present study appropriately reflects the study cohort.
Conclusion
In the current study, UCLR returned average ulnohumeral joint space gapping to normal values on postoperative SUS. UCLR resulted in a mean decrease of joint space gapping from 2.28 ± 1.26 mm preoperatively to 0.69 ± 0.44 mm postoperatively. Regardless of technique, UCLR restored delta values comparable to those of the contralateral unaffected elbow (0.83 ± 0.53 mm). Both the modified Jobe and Docking reconstruction techniques yielded mean gapping values <1.0 mm. These findings provide surgeons with the expected change in joint space gapping (delta) after UCLR as measured on SUS. By providing a reference, surgeons can better assess patients with concern for recurrent injury after previous UCLR in situations where MR studies alone may be challenging to interpret.
Footnotes
Submitted November 15, 2024; accepted September 22, 2025.
Presented at the annual meeting of the AOSSM, Denver, Colorado, July 2024.
One or more of the authors has declared the following potential conflict of interest or source of funding: M.G.C. is a board member for Major League Baseball Team Physicians Association and Orthopaedic Learning Center. S.B.C. has received research support from Major League Baseball and Arthrex; consulting fees from CONMED Linvatec and Zimmer; and royalties from Zimmer. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.