
Abstract
Background:
The chondrolabral junction (CLJ) plays an important role in maintaining hip dynamics, and there is a paucity in the literature examining the effect of CLJ breakdown on long-term outcomes after hip arthroscopy.
Purpose:
To identify patient-reported outcomes (PROs), achievement of clinically significant outcomes, and reoperation rates at 10-year follow-up in patients with severe CLJ breakdown undergoing hip arthroscopy for femoroacetabular impingement.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
PROs were obtained preoperatively and at 10-year follow-up for patients undergoing surgery between January 2012 and June 2014. PROs included the Hip Outcome Score–Activities of Daily Living, Hip Outcome Score–Sports Subscale, modified Harris Hip Score, international Hip Outcome Tool-12, and visual analog scale for pain. Clinically significant outcomes included the minimal clinically important difference and Patient Acceptable Symptom State. Patients were categorized as having severe CLJ breakdown if their Beck classification was between 3 and 4 and mild if their classification was 1 to 2. Those with severe breakdown were propensity matched 1:1 to patients who had mild breakdown, controlling for age, sex, and body mass index (BMI). Independent t tests and Fisher exact tests were used to compare PROs and rates of hip arthroscopy revision and total hip arthroplasty conversion between groups, respectively.
Results:
In this study, 53 patients with severe CLJ breakdown (25 females; mean ± SD age, 38.6 ± 12.2 years; BMI, 25.9 ± 4.9 kg/m2) were matched successfully 1:1 by age, sex, and BMI to 53 patients with mild CLJ breakdown (27 females; age, 37.8 ± 11.3 years; BMI, 25.9 ± 4.9 kg/m2). Preoperatively, there were no differences in PROs between patients with severe and mild CLJ breakdown. At final 10-year follow-up, PRO scores were also similar between groups. However, at 10 years, patients with severe CLJ breakdown underwent conversion to total hip arthroplasty at significantly higher rates than those with mild breakdown (28.4% vs 5.7%; P = .003).
Conclusion:
Patients with severe CLJ junction breakdown undergoing hip arthroscopy for femoroacetabular impingement achieve similar PROs at long-term follow-up but undergo hip arthroplasty significantly more often when compared with patients with mild breakdown.
The acetabular labrum plays a vital role in maintaining hip stability within the joint.11,26,27 It is frequently torn as a result of femoroacetabular impingement (FAI), a condition marked by abnormal contact forces between the femoral head (cam) and the acetabulum (pincer). 16 If not addressed, these bony deformities and labral tears can disrupt hip mechanics and synovial fluid flow, leading to additional labral damage, cartilage delamination, and related hip symptoms such as groin pain, stiffness, and reduced range of motion.3,5,6,26 Nonoperative treatments, including activity modification, anti-inflammatory medications, and physical therapy, are typically the first line of management. 19 However, when these approaches fail to alleviate symptoms, hip arthroscopy may be considered to treat labral tears, relieve osseous impingement, and address other intra-articular issues. 16
The chondrolabral junction (CLJ) is defined as the intermediate zone between the acetabular cartilage and labrum and has been shown to be affected in patients with FAI.10,28 Specifically, it is thought that the asphericity of the femoral head in patients with cam morphology can lead to shearing forces during flexion phases of movement on the acetabular CLJ. 22 This can lead to labral tears and cartilage damage, ranging from delamination with an intact CLJ (wave or carpet sign) to delamination with a disrupted CLJ (pita sign).21,22 There have been various methods in grading cartilage damage intraoperatively, including the Beck classification, MAHORN classification, and the International Cartilage Repair Society score, which all consider the degree of cartilage roughening, carpeting, and thickness loss.2,15,18
Hip arthroscopy has been shown to be an effective treatment option for high-grade CLJ damage, with patients showing significantly improved patient-reported outcomes (PROs) postoperatively.4,7 Given that the status of the CLJ is important in determining outcomes after labral repair and hip arthroscopy, it is imperative to understand how cases of severe CLJ breakdown affect long-term PROs as well as rates of reoperation or conversion to total hip arthroplasty (THA). Previous studies investigating long-term PROs in patients with high-grade CLJ damage have shown favorable outcomes beyond 8 years, with a 10-year survivorship of 81.6%. 4
While studies such as these report on long-term PROs, few studies have compared outcomes and arthroplasty conversion survivorship after hip arthroscopy when stratifying by varying degrees of cartilage damage. Thus, this study has 2 primary purposes: (1) to examine PROs and achievement of clinically significant outcomes at 10-year follow-up between patients with mild and severe CLJ breakdown and (2) to compare reoperation-free survivorship between these sets of patient groups to determine how the degree of cartilage damage affects conversion to THA. We hypothesize that patients in both groups will have similar improvement of PROs and comparable achievement of clinically significant outcomes. However, we predict that the severe CLJ damage group will have a higher reoperation rate at long-term follow-up.
Methods
Selection Criteria
The study was approved by the local institutional review board (23092101-IRB01-AM03). A prospectively maintained, retrospectively analyzed surgical repository at a single institution was reviewed. Patients who underwent primary hip arthroscopy for labral repair by the senior author (S.J.N.) between January 1, 2012, and June 2014 were screened for inclusion. These patients provided preoperative consent for their data to be stored in the repository.
The inclusion criteria used were as follows:
Symptomatic FAI syndrome—for example, positive anterior impingement test result during examination, radiographic evidence of a cam deformity (90° Dunn radiograph with alpha angle >55°), or pincer deformity (anterior-posterior [AP] radiograph showing lateral center-edge angle [LCEA] >40°)8,21
Failure of nonoperative management—specifically, activity modification, anti-inflammatory drugs, a course of physical therapy, or intra-articular corticosteroid injection
Eligible for 10-year follow-up
The exclusion criteria were as follows: the surgical procedure in question was a revision hip arthroscopy, or patients had Tönnis grade >1, a history of developmental hip disorders (Legg Calvé-Perthes disease or slipped capital femoral epiphysis), a concomitant hip procedure, avascular necrosis, or hip dysplasia (LCEA <20°).
Patient Demographics
Patient demographic information, such as age, sex, and body mass index (BMI), was collected. Additional preoperative characteristics were collected, including participation in physical activity (regular activity ≥1 time per week), history of back pain, and preoperative symptom duration. Intraoperative cartilage grading with Beck classification was completed, and the types of procedures performed were recorded. 1
Preoperative Radiographic Findings
Radiographic parameters were assessed from a standard series of hip radiographs taken preoperatively and at the initial postoperative clinic visit, including a standing AP view, false profile view, and Dunn lateral view at 90° of hip flexion. The alpha angle was measured via the conventional technique on the Dunn lateral radiograph, while the LCEA and Tönnis grade were measured on the AP radiograph of the affected hip. 21 Additionally, the crossover sign, ischial spine sign, posterior wall sign, and coxa profunda were evaluated on the AP radiographs. All radiographic measurements were performed by an orthopaedic surgeon specializing in hip arthroscopy (S.J.N.).
Intraoperative Findings and Articular Cartilage Grading
Intraoperative findings were recorded, including the type of procedure performed and the presence of transitional zone acetabular cartilage damage according to Beck classification. 1 This classification grades articular cartilage between 0 and 4:
0: Normal—macroscopically sound cartilage
1: Malacia—roughening of surface
2: Debonding—loss of fixation to the subchondral bone with carpet phenomenon
3: Cleavage—loss of fixation to the subchondral bone with frayed edges and the presence of flaps
4: Defect—full-thickness defect
Severe breakdown was classified as between grades 3 and 4, while mild breakdown was classified as grades 1 and 2 in accordance with the previous literature. 4
Surgical Technique
All surgical procedures were carried out by the senior author (S.J.N.) following a previously described method. 16 In brief, patients were administered general endotracheal anesthesia and positioned in a modified supine position with traction applied by a well-padded perineal post. Anterolateral and modified midanterior portals were created, and the 2 portals were connected with an arthroscopic scalpel to perform the interportal (transverse) portion of the capsulotomy. A cuff of capsular tissue was preserved on the acetabular and femoral sides for later capsular plication or repair. Standard techniques were employed to address any central femoroacetabular compartment pathology, including pincer morphology and labral tear repair. Labral debridement was performed in cases of considerable labral degeneration where the tissue quality would not permit suture fixation. For cases requiring labral repair, a distal anterolateral accessory portal was added. In cases of cartilage damage, loose flaps were debrided with an arthroscopic shaver, and further treatment with microfracture was performed in select cases.
After the completion of central compartment work, traction was released. A T-type capsulotomy was then performed by extending the interportal capsulotomy distally along the femoral neck, allowing access to the peripheral compartment. Within the peripheral compartment, direct visualization of the cam deformity was achieved, and, if present, osteochondroplasty was performed until the cam resection was adequate and proper femoral head-neck offset was restored. Fluoroscopy was used to track resection progress. A dynamic examination of the leg was then performed to ensure cam impingement resolution. Capsular plication and closure were conducted using ultra-high molecular weight polyethylene sutures, beginning at the base of the vertical segment, followed by the interportal segment. Standard postoperative care and rehabilitation were administered in line with the institution’s previously described protocol. 12
PROs and Clinically Significant Outcomes
PROs included the Hip Outcome Score–Activities of Daily Living (HOS-ADL), Hip Outcome Score–Sports Subscale (HOS-SS), modified Harris Hip Score (mHHS), International Hip Outcome Tool–12 (iHOT-12), and visual analog scale (VAS) for pain and satisfaction. These PROs were collected preoperatively and at 2 and 10 years postoperatively. Rates of clinically significant outcomes were assessed, including the minimal clinically important difference (MCID) and Patient Acceptable Symptom State (PASS). Cohort-specific MCID thresholds were calculated utilizing the distribution method. 17 The threshold values were as follows: HOS-ADL, 11.3; HOS-SS, 15.7; mHHS, 9.0; and VAS pain, 13.5. PASS thresholds were calculated from the cohort by using receiver operative curve analysis with Youden index.9,14 Cohort-specific PASS thresholds were as follows: HOS-ADL, 75.2; HOS-SS, 53.5; mHHS, 67.5; and VAS pain, 28.1.
Secondary Surgery and Survivorship
Rates of secondary surgery were recorded, including revision hip arthroscopy and conversion to THA. At any follow-up after surgery, all patients were assessed for whether they had undergone a revision hip arthroscopy procedure or conversion to THA. If so, patients were asked the date that they underwent the secondary procedure. Those patients who underwent either a revision hip arthroscopy or THA conversion were included in gross survivorship analysis; however, their PRO data were excluded from any analyses performed after the date of their subsequent operation. Survivorship was calculated for both cohorts, and a Kaplan-Meier survivorship curve was used to compare gross survivorship between the groups.
Statistical Analysis
Patients with Beck classification >2 were propensity matched to patients with Beck classification ≤2 in a 1:1 ratio by age, sex, and BMI. Continuous variables were reported as means and standard deviations for parametric variables, and categorical variables were presented as counts and percentages. Normality of continuous variables was assessed with the Shapiro-Wilk test. Because outcomes were normally distributed, 2-tailed paired samples t tests were performed to evaluate within-group differences for significant improvements preoperatively to 10 years, whereas 2-tailed independent t tests were used to assess for significant differences between groups. Fisher exact tests were used to assess differences in categorical variables between groups.
Results
Patient Characteristics
A total of 736 patients underwent hip arthroscopy for FAI syndrome between January 2012 and June 2014. After exclusion criteria, 619 patients remained. Of these patients, 184 were missing 10-year follow-up (compliance, 70.3%), and 297 had a normal Beck classification (grade 0). Thus, 138 patients remained with Beck classifications between 1 and 4. Of those, 63 had severe CLJ breakdown with a grade between 3 and 4, and 75 had mild CLJ breakdown with a grade between 1 and 2. Fifty-three patients with severe CLJ breakdown (25 females; mean ± SD age, 38.6 ± 12.2 years; BMI, 25.9 ± 4.9 kg/m2) were matched successfully 1:1 based on age, sex, and BMI to 53 patients with mild CLJ breakdown (27 females; age, 37.8 ± 11.3 years; BMI, 25.9 ± 4.9 kg/m2) (Figure 1). No significant differences were noted in any further preoperative characteristics between the groups (Table 1). Patients with severe breakdown had significantly higher preoperative alpha angles on Dunn lateral view (68.3° ± 12.0° vs 62.0° ± 13.4°; P = .021). They also had significantly smaller LCEAs preoperatively (28.9° ± 6.1° vs 31.2° ± 5.7°; P = .049) and postoperatively (27.1° ± 6.0° vs 30.0° ± 5.7°; P = .016). The groups had a similar Tönnis grade distribution and frequency of procedures performed, except for microfracture, with the severe breakdown group having a significantly higher amount of microfractures performed (5.7% vs 1.9%; P < .001). As expected, intraoperative grading revealed significantly higher proportions of grade 3 and 4 Beck classifications of acetabular cartilage in the severe CLJ breakdown group (P < .001) (Table 2). The severe group also had significantly higher proportions of International Cartilage Repair Society gradings of 3 and 4 as compared with the mild group (P = .005).
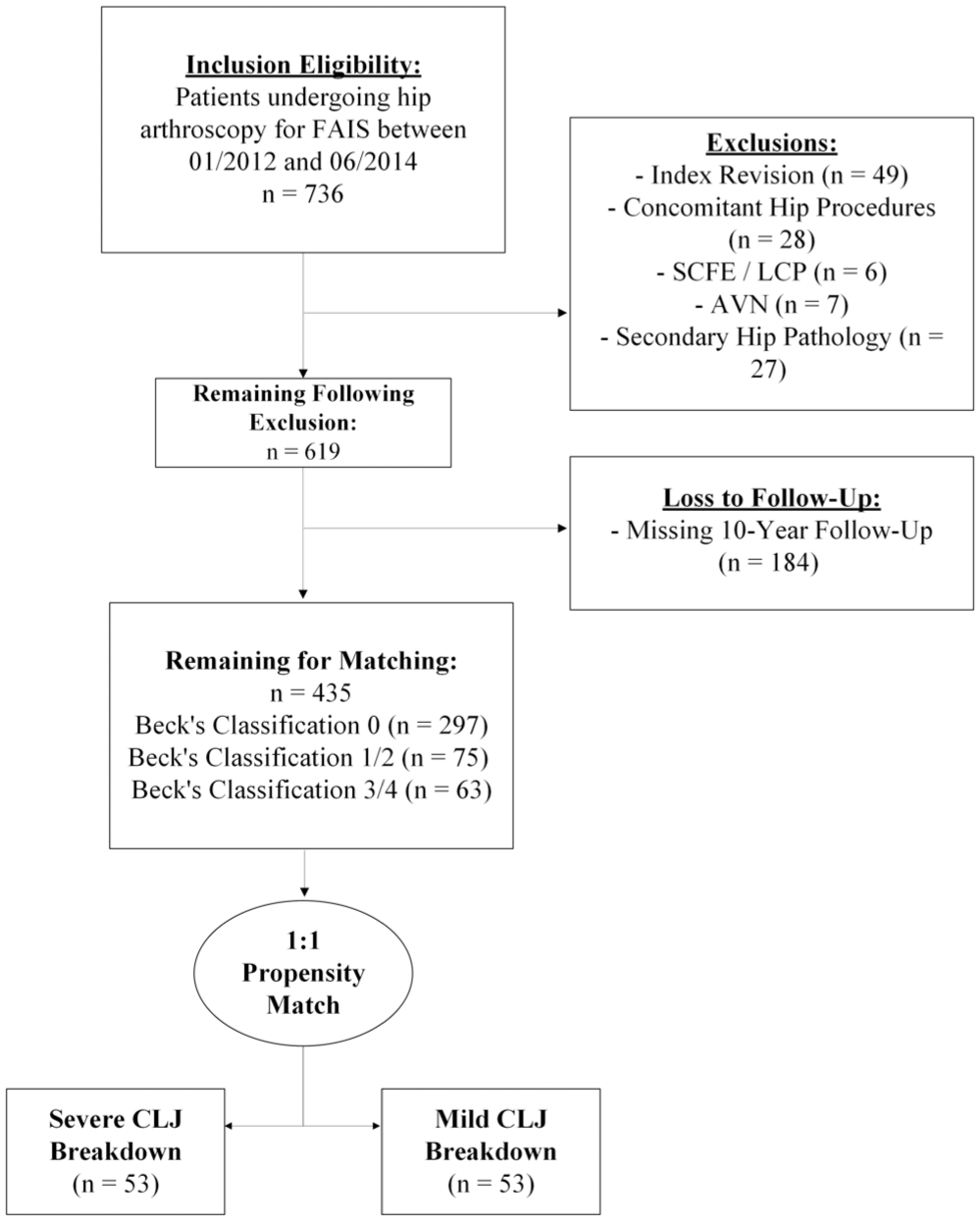
CONSORT (Consolidated Standards of Reporting Trials) diagram depicts patient selection methods after inclusion and exclusions. Patients were propensity matched by age, sex, and body mass index. AVN, avascular necrosis; CLJ, chondrolabral junction; FAIS, femoroacetabular impingement syndrome; LCP, Legg Calvé-Perthes; SCFE, slipped capital femoral epiphysis.
Cohort Characteristics a
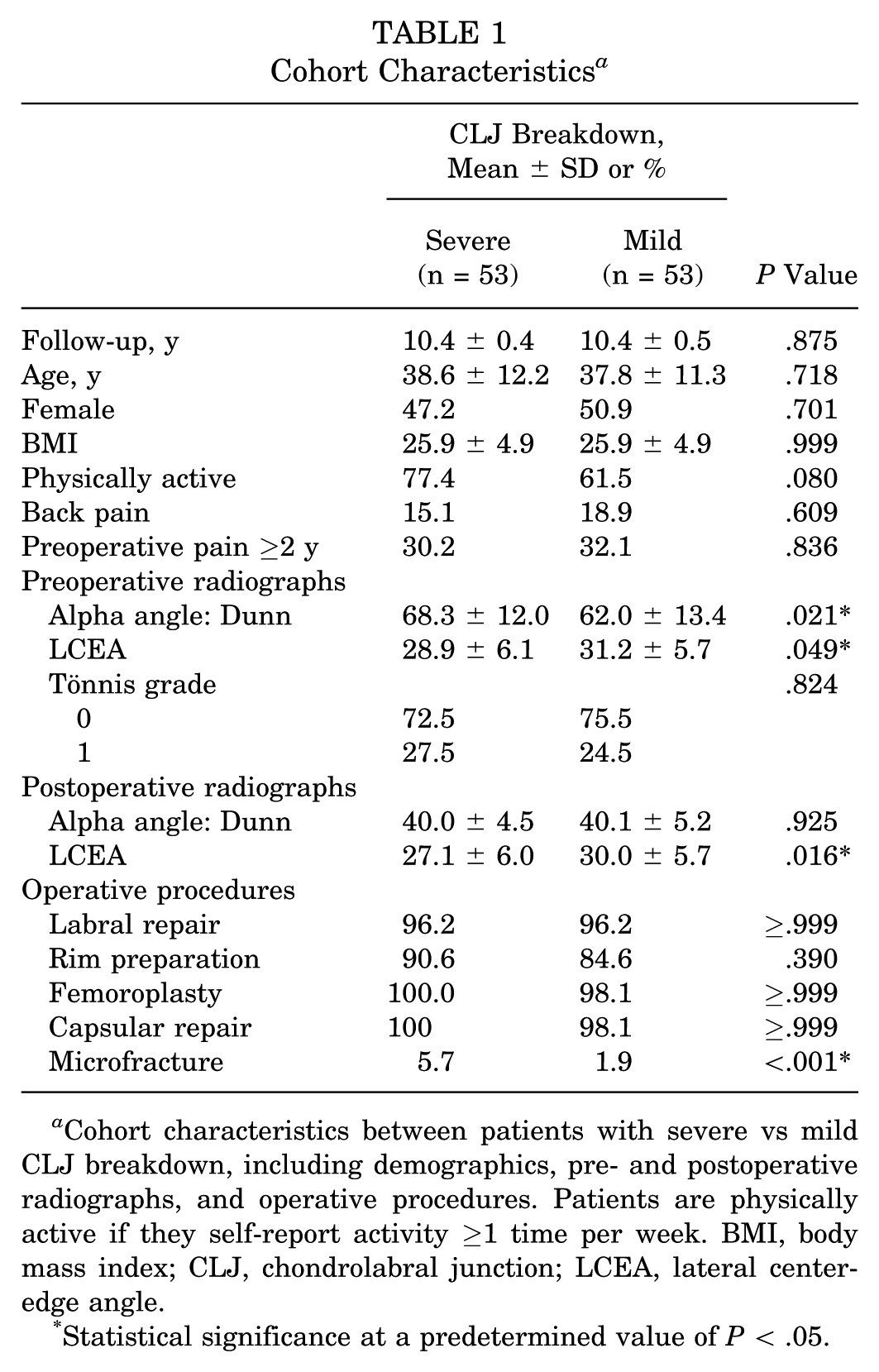
Cohort characteristics between patients with severe vs mild CLJ breakdown, including demographics, pre- and postoperative radiographs, and operative procedures. Patients are physically active if they self-report activity ≥1 time per week. BMI, body mass index; CLJ, chondrolabral junction; LCEA, lateral center-edge angle.
Statistical significance at a predetermined value of P < .05.
Intraoperative Cartilage Grading a
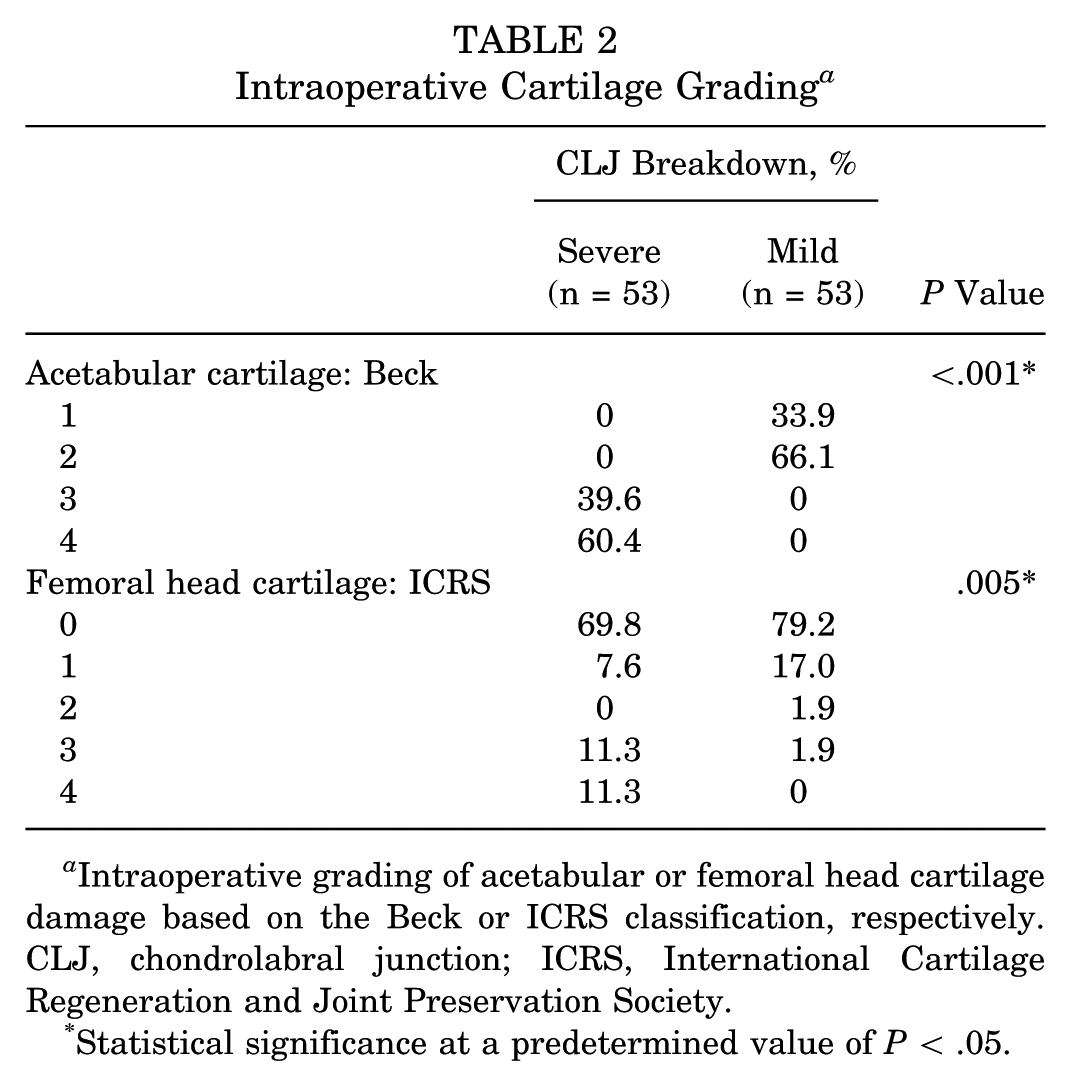
Intraoperative grading of acetabular or femoral head cartilage damage based on the Beck or ICRS classification, respectively. CLJ, chondrolabral junction; ICRS, International Cartilage Regeneration and Joint Preservation Society.
Statistical significance at a predetermined value of P < .05.
Patient-Reported Outcomes
All patients, regardless of CLJ breakdown, found significant improvement preoperatively to 10-year follow-up for all PROs measured (P < .001). Preoperatively, there were no significant differences for any PRO between groups. At 10 years, no significant differences were noted between groups for any PRO measure. The change in scores from preoperation to 10 years, or delta, was also similar between groups (Table 3).
Patient-Reported Outcomes a
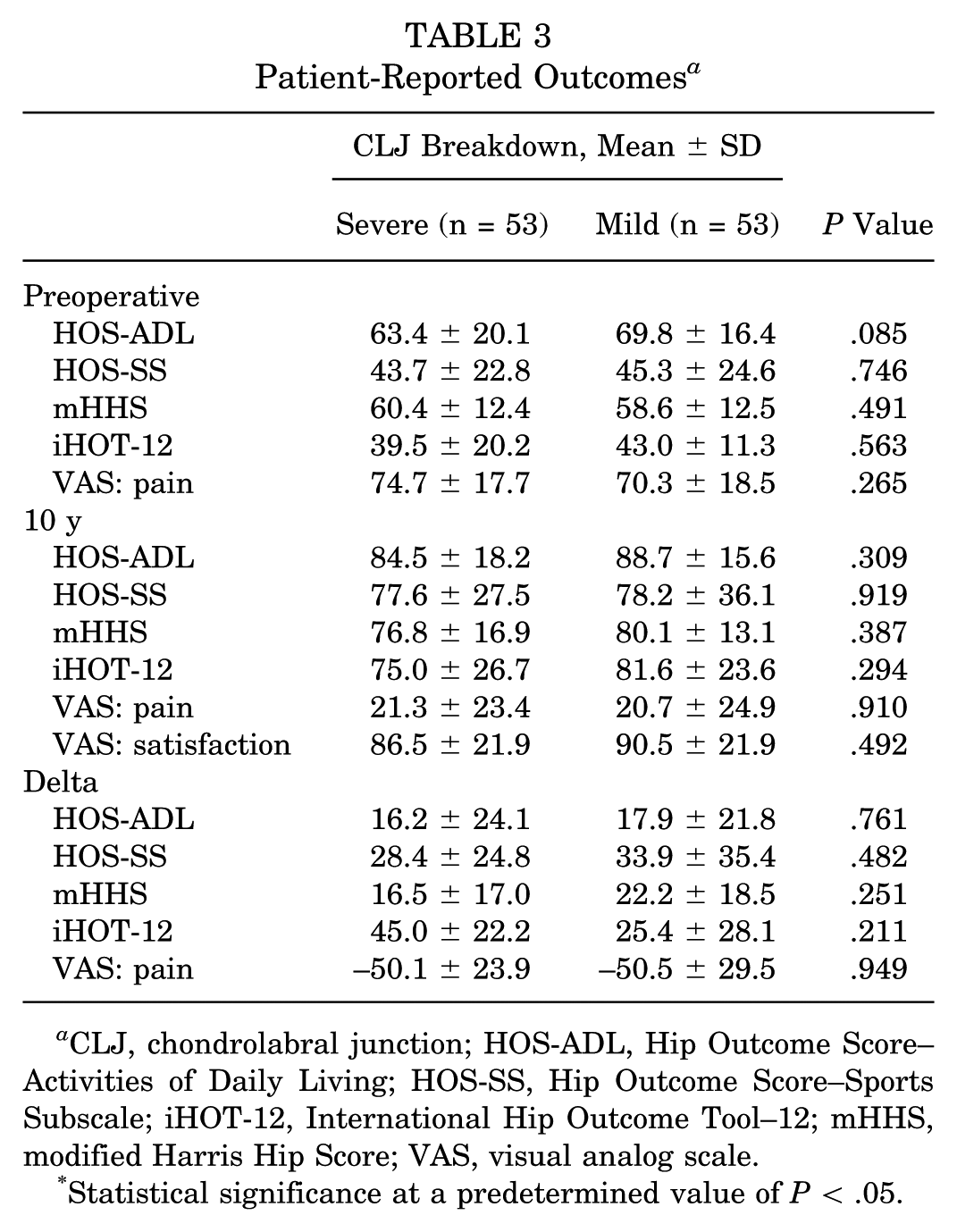
CLJ, chondrolabral junction; HOS-ADL, Hip Outcome Score–Activities of Daily Living; HOS-SS, Hip Outcome Score–Sports Subscale; iHOT-12, International Hip Outcome Tool–12; mHHS, modified Harris Hip Score; VAS, visual analog scale.
Statistical significance at a predetermined value of P < .05.
Clinically Significant Outcomes
Most patients, regardless of CLJ status, achieved high MCID and PASS rates for all measured PROs. There were no significant differences noted between groups regarding MCID and PASS achievement rates at final follow-up (Figure 2).
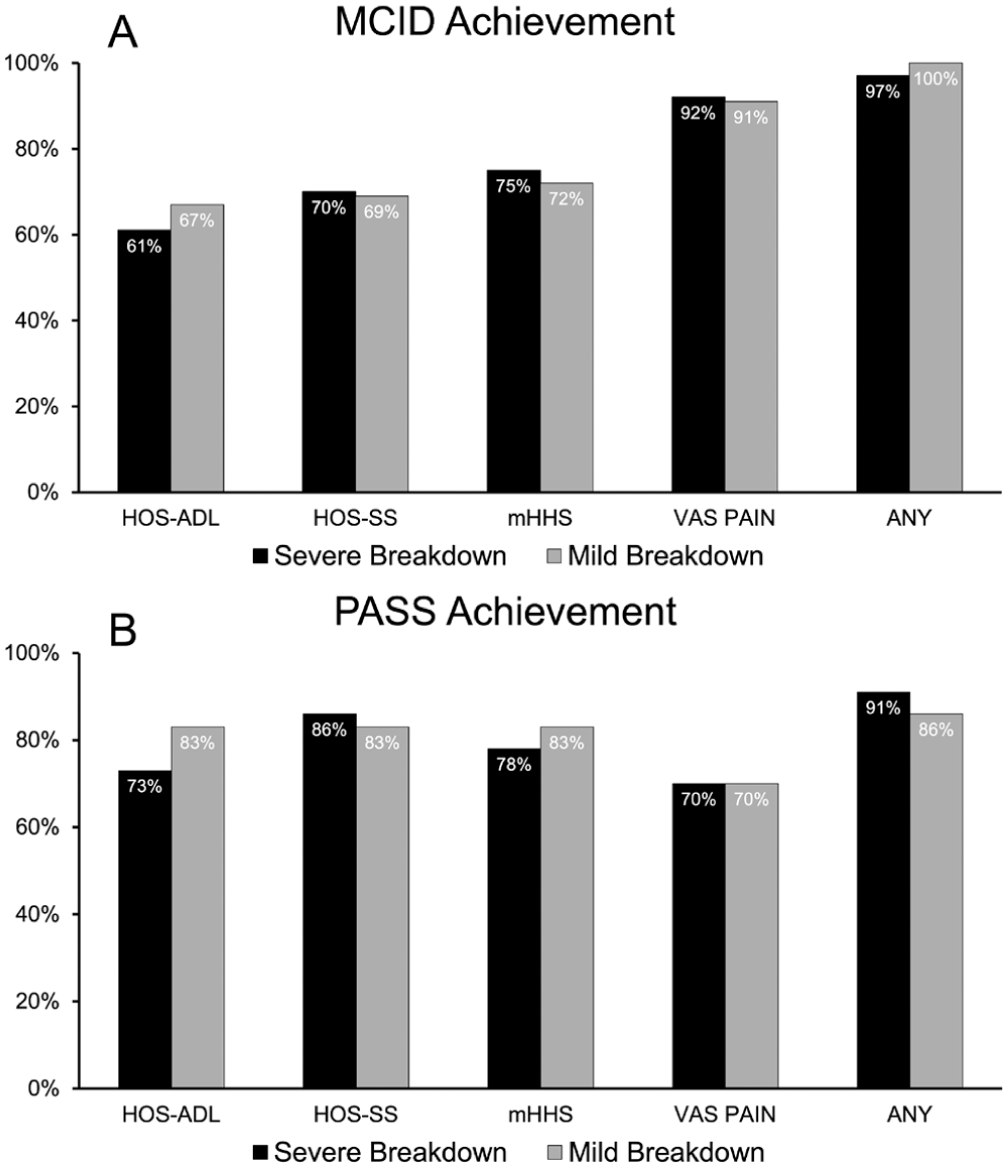
Clinically significant outcomes are compared at final 10-year follow-up between severe and mild CLJ breakdown groups. The patient-reported outcomes listed are the Hip Outcome Score–Activities of Daily Living (HOS-ADL), Hip Outcome Score–Sports Subscale (HOS-SS), modified Harris Hip Score (mHHS), and visual analog scale for pain (VAS PAIN). Also displayed is achievement of (A) the minimal clinically important difference (MCID) and (B) the Patient Acceptable Symptom State (PASS). CLJ, chondrolabral junction.
Arthroplasty-Free Survivorship
In terms of reoperation rates, the group with high CLJ breakdown experienced significantly higher rates of conversion to THA as compared with the low CLJ breakdown group (28.4% vs 5.7%; P = .003) (Table 4).
Revision and Total Hip Arthroplasty Revision a
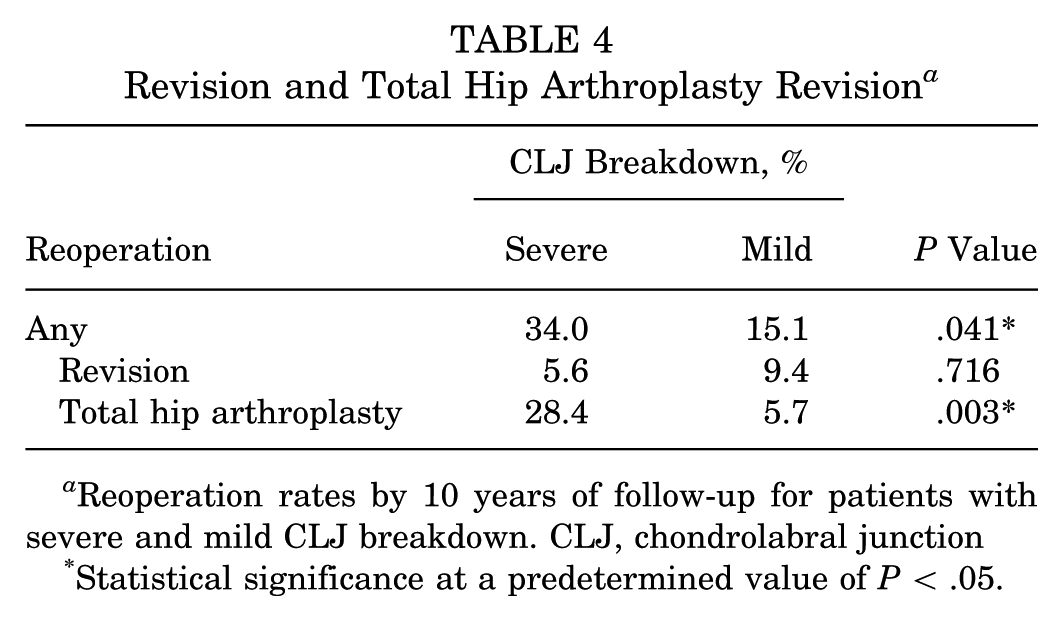
Reoperation rates by 10 years of follow-up for patients with severe and mild CLJ breakdown. CLJ, chondrolabral junction
Statistical significance at a predetermined value of P < .05.
When revision hip arthroscopy rates were compared, there were no significant differences between groups. On Kaplan-Meier survival analyses, there were significant differences in gross survivorship between the cohorts (P = .002) (Figure 3).
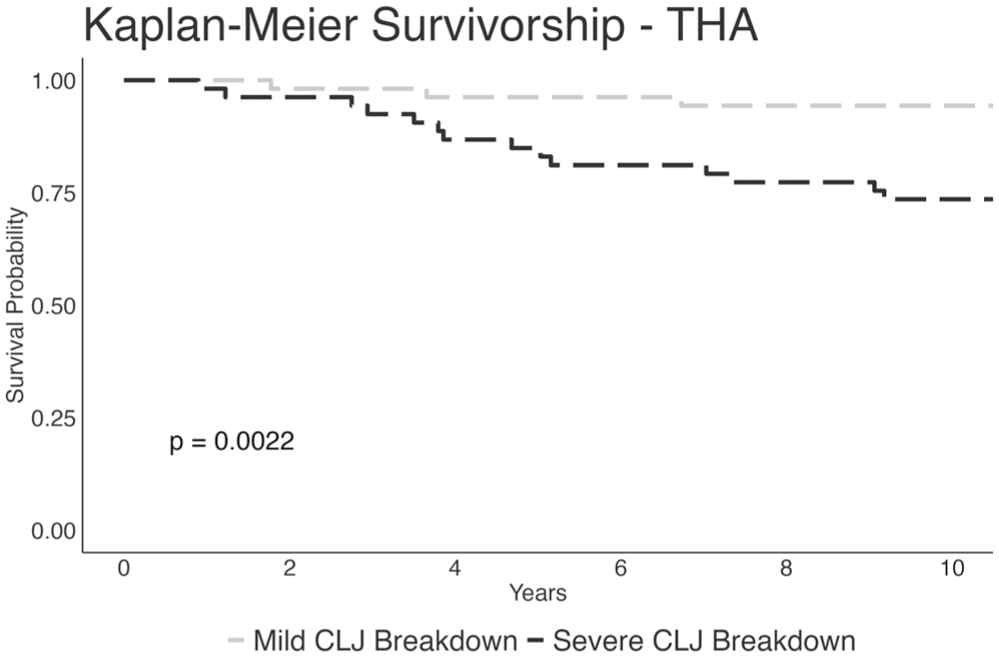
Kaplan-Meier survivorship analysis for those with severe and mild CLJ breakdown undergoing conversion to a total hip arthroplasty (THA). P value for the log-rank test is listed. CLJ, chondrolabral junction.
Discussion
This study demonstrates that patients undergoing hip arthroscopy with severe CLJ breakdown can achieve long-term PROs comparable to those with mild CLJ breakdown at 10-year follow-up. Despite presenting with more extensive preoperative deformities and radiographic evidence of greater joint damage, patients with severe CLJ breakdown exhibited similar improvements in HOS-ADL, HOS-SS, mHHS, iHOT-12, and VAS pain scores at final follow-up. Additionally, there was no significant difference in the proportion of patients achieving clinically significant outcomes between the groups. These findings underscore the potential for substantial functional recovery in patients with advanced FAI, particularly when managed appropriately by modern hip preservation techniques. In terms of long-term reoperation survivorship, rates of subsequent revision hip arthroscopy were similar regardless of CLJ status, but those with more severe grades underwent THA conversion at significantly higher rates, with an overall 10-year survivorship of 72%.
The preservation of the CLJ is crucial for long-term joint health, as it serves as the interface between the fibrocartilaginous labrum and the acetabular hyaline cartilage, ensuring smooth force transmission and joint stability.3,5,6 Cam deformities in particular exert abnormal shear forces on the CLJ, accelerating its breakdown and increasing the risk of osteoarthritis. 28 In this study, correcting alpha angles and LCEA played a key role in restoring hip function and reducing mechanical impingement. Preoperatively, patients with severe CLJ breakdown had significantly larger alpha angles than those with mild breakdown (69.8° ± 12.3° vs 60.6° ± 12.7°; P < .001), suggesting that greater cam deformity contributes to the risk of CLJ damage. Postoperative improvements in alpha angles across both groups highlight the efficacy of arthroscopic osteochondroplasty in reshaping the femoral head-neck junction.
Despite the success of arthroscopic intervention in the setting of advanced CLJ damage, the findings of the present study underscore the need for early recognition and intervention for FAI to address pathology before significant CLJ damage occurs. Specifically, the present study suggests that patients with severe CLJ damage require THA conversion after primary hip arthroscopy more frequently than patients with mild CLJ damage. Previous studies have shown that early surgical intervention and shorter symptom duration can limit CLJ damage, improve PROs, and decrease the risk of conversion to THA.23,24 In a recent meta-analysis, Martin et al 23 found that greater chondral damage, longer symptom duration (>1.5 years), and worse preoperative PROs significantly increased the likelihood of poorer postoperative outcomes and conversion to THA. Although no significant difference in revision arthroscopy rates was observed between patients with severe and mild CLJ breakdown (7.3% vs 10.9%; P = .742), the rate of THA conversion was notably higher in those with severe breakdown (25.5% vs 5.4%; P = .006). These findings suggest that although arthroscopy provides symptomatic and functional improvement, advanced articular damage increases the risk of osteoarthritis progression and eventual THA conversion.
The compromised healing capacity of the CLJ in adults, attributed to reduced vascular supply, likely contributes to this outcome.13,25,29 Philippon et al20 highlighted that while some fibrovascular ingrowth occurs after arthroscopic labral repair, complete restoration of the labrum’s structure is limited by diminished vascularity. However, whether earlier intervention in younger patients with a more robust blood supply leads to slower progression of CLJ damage and osteoarthritis remains an area for future research.
Limitations
The present study has several limitations. First, its retrospective nature may introduce selection bias, limiting the ability to establish causal relationships. Additionally, there is variability in follow-up duration, which could affect the consistency of long-term outcome assessments. Another significant limitation is the potential for variability in surgical techniques, which may influence the outcomes of chondrolabral repair. This study’s utilization of PROs is also prone to the ceiling effect, especially given the long-term follow-up period. Moreover, PROs were not collected after patients underwent reoperation. These PROs may further capture patient function, pain, and satisfaction in cases where hip arthroscopy alone was not sufficient. However, it would be difficult to isolate whether subjective reported outcomes would be related to the hip arthroscopy intervention or to the THA or revision surgery. Finally, the study may not account for variations in patient demographics, socioeconomic status, or preexisting comorbidities, all of which could affect healing and recovery outcomes.
Conclusion
Patients with severe CLJ breakdown can achieve significant improvement of clinical outcomes similar to those with mild CLJ breakdown at 10-year follow-up, despite their more advanced disease. However, these patients remain at a significantly higher risk of conversion to THA.
Footnotes
Submitted October 28, 2024; accepted September 2, 2025.
One or more of the authors has declared the following potential conflict of interest or source of funding: S.J.N. has received research support from AlloSource, Arthrex, Athletico, DJ Orthopaedics, Linvatec, Miomed, Smith & Nephew, and Stryker and consulting fees and royalties from Ossur, Stryker, and Springer. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.