
Abstract
Background:
Total knee arthroplasty (TKA) provides pain relief and functional improvement for end-stage knee osteoarthritis patients. As TKA use increases in younger patients, return to sports (RTS) has become a key outcome measure. While RTS rates after TKA are generally high, they vary significantly across studies due to differences in study design, patient populations, and RTS definitions.
Purpose:
To determine RTS rates, evaluate return to preoperative sport levels, quantify time to RTS, and identify factors affecting RTS after TKA.
Study Design:
Cohort study; Level of evidence, 2.
Methods:
We analyzed 21,466 primary TKAs performed between 2016 and 2022. Of these, 1782 patients (8.3%) were athletes at baseline, with 1464 (82.2%) completing 1-year follow-up. We recorded demographic characteristics, comorbidities, baseline and 1-year RTS status, time to RTS, athlete type, and patient-reported outcomes. Analysis included descriptive statistics, Cox regression for time to RTS, and logistic regression for RTS-associated factors.
Results:
Of 1464 patients, 782 (53.4%) achieved RTS, while 676 (46.6%) did not; both contact and noncontact sports were included. Among those who returned, 62% resumed their previous sport at the same level, 34.5% at a reduced intensity, and 3.4% switched to a different sport. The median RTS time was 12 weeks, with 90% returning within 27 weeks. Medicaid patients had a delayed RTS compared with those with commercial insurance (hazard ratio [HR], 0.51). Overweight patients returned sooner than normal-weight patients (HR, 1.41). Female patients (odds ratio [OR], 0.76) and Black patients (OR, 2.34) had lower RTS odds, while recreational (OR, 0.06) and competitive athletes (OR, 0.10) had higher RTS odds versus those not participating in athletic activities.
Conclusion:
Over half of athletes returned to sports within 1 year of TKA, most within 27 weeks. RTS rates varied by preoperative competitive level, sex, race, body mass index, and comorbidity burden. These findings can guide patient expectations and shared decision-making regarding post-TKA sports participation. Future research should focus on improving RTS rates in high-risk groups, standardizing RTS criteria, and stratifying outcomes by sport type and impact level to enable more individualized patient recommendations.
Total knee arthroplasty (TKA) is a successful and increasingly common surgical procedure for end-stage knee osteoarthritis, providing significant improvements in pain, function, and quality of life.10,21,45 With an aging yet active population and expanding surgical indications, the demand for TKA is rapidly growing, especially among younger patients.14,19 It is projected that over half of patients receiving TKA will be <65 years by 2030.5,32 This demographic shift has important implications, as younger TKA patients often have higher expectations regarding postsurgical activity, including return to sports (RTS).15,49 Young patients often undergo TKA for posttraumatic osteoarthritis, inflammatory arthritis, or early end-stage osteoarthritis. 15
RTS is an important component of many patients' postoperative goals and plays a key role in quality of life and overall satisfaction after TKA.13,52 Participation in regular physical activity and sports can provide numerous physical and mental health benefits, facilitate recovery, and may even protect the replaced joint.6,7,8 However, the RTS rate after TKA varies widely in the literature from 36% to 89% depending on the study design, patient population, and definition of RTS used.2,3,24 The lack of standardized RTS criteria and significant heterogeneity between studies make it challenging to provide evidence-based guidance to patients on this topic.17,47 The absence of standardized definitions and criteria for RTS after TKA contributes to substantial heterogeneity in the published literature, making evidence synthesis and patient counseling challenging. Reported outcomes vary depending on whether RTS is defined as any postoperative sport participation, return to preoperative sport type and frequency, or thresholds on patient-reported activity scales. For example, pooled analyses demonstrate wide variability in reported RTS rates depending on timepoint, ranging from approximately 19% at 3 months to 70% at 6 months and 84% to 88% at 12 to 14 months, with individual prospective studies reporting mean RTS times between 16 and 24 weeks. 23 Similarly, pooled RTS rates differ significantly by sport intensity, with estimates of ~76% for low-impact sports compared with ~35% for high-impact sports. 34 Methodological variation further complicates interpretation, as many systematic reviews and cohort studies include mixed arthroplasty populations, apply retrospective and prospective designs, and utilize disparate outcome measures. 20 Moreover, surgeon recommendations themselves are inconsistent: while most endorse return to low-impact activities within 3 to 6 months, guidance regarding high-impact activities ranges from discouragement to conditional approval with training, reflecting a lack of consensus in clinical practice. 50
Furthermore, high-impact sports, such as running, basketball, and soccer, involve repetitive jumping, pivoting, and high joint loading. In contrast, low-impact activities, such as swimming, cycling, and walking, produce smoother, more controlled loading profiles and are generally considered safer for patients after TKA. 12 A systematic review found that RTS rates and activity levels seem to decline with longer-term follow-up after TKA, especially for high-impact sports.12,24 Even among patients who do RTS, many participate at a lower intensity or take up different, lower-impact activities than they did preoperatively.22,25 Multiple factors may influence the ability to RTS after TKA, including patient age, sex, preoperative sports participation, aerobic capacity, surgical factors, postoperative pain and function, and psychological readiness.9,33,35 However, the relative impact of these factors and how they can be optimized to facilitate RTS remains unclear.36,37
Reflecting these knowledge gaps, there is substantial variation in surgeon recommendations regarding RTS after TKA.39,48 Furthermore, the proportion of patients actually returning to sports remains unclear.38,43 To enable more personalized and evidence-based RTS guidance after TKA, detailed data are needed on the timeline, level, and determinants of sports resumption in a large contemporary patient cohort.29,44 Most previous studies on this topic have been limited by retrospective designs, small sample sizes, and insufficient adjustments for baseline patient characteristics.18,24,30 Also, they have often failed to distinguish the timing, frequency, and intensity of RTS relative to preoperative activity.20,40 Finally, very limited data exist on patient-reported outcome measures (PROMs) or objective functional tests as they relate to RTS after TKA.31,51
This study aimed to address these evidence gaps through a prospective, adequately powered analysis of RTS after primary TKA. The specific objectives are as follows: to (1) determine the rate of RTS 1 year after TKA; (2) evaluate the time to RTS and the degree of sports resumption relative to preoperative activity; and (3) identify which patient demographic and surgical factors are associated with the ability to RTS.
Methods
Study Design and Patient Population
This study utilized data from a prospective cohort at a major integrated health care network, drawing from their Orthopaedic Minimal Data Set Episode of Care (OME) database.1,31 The OME system was established to facilitate efficient collection of PROMs through standardized protocols. The study examined patients who underwent primary unilateral TKA and completed initial OME surveys between January 2016 and December 2022 (Figure 1). Institutional review board approval was obtained before starting this study.
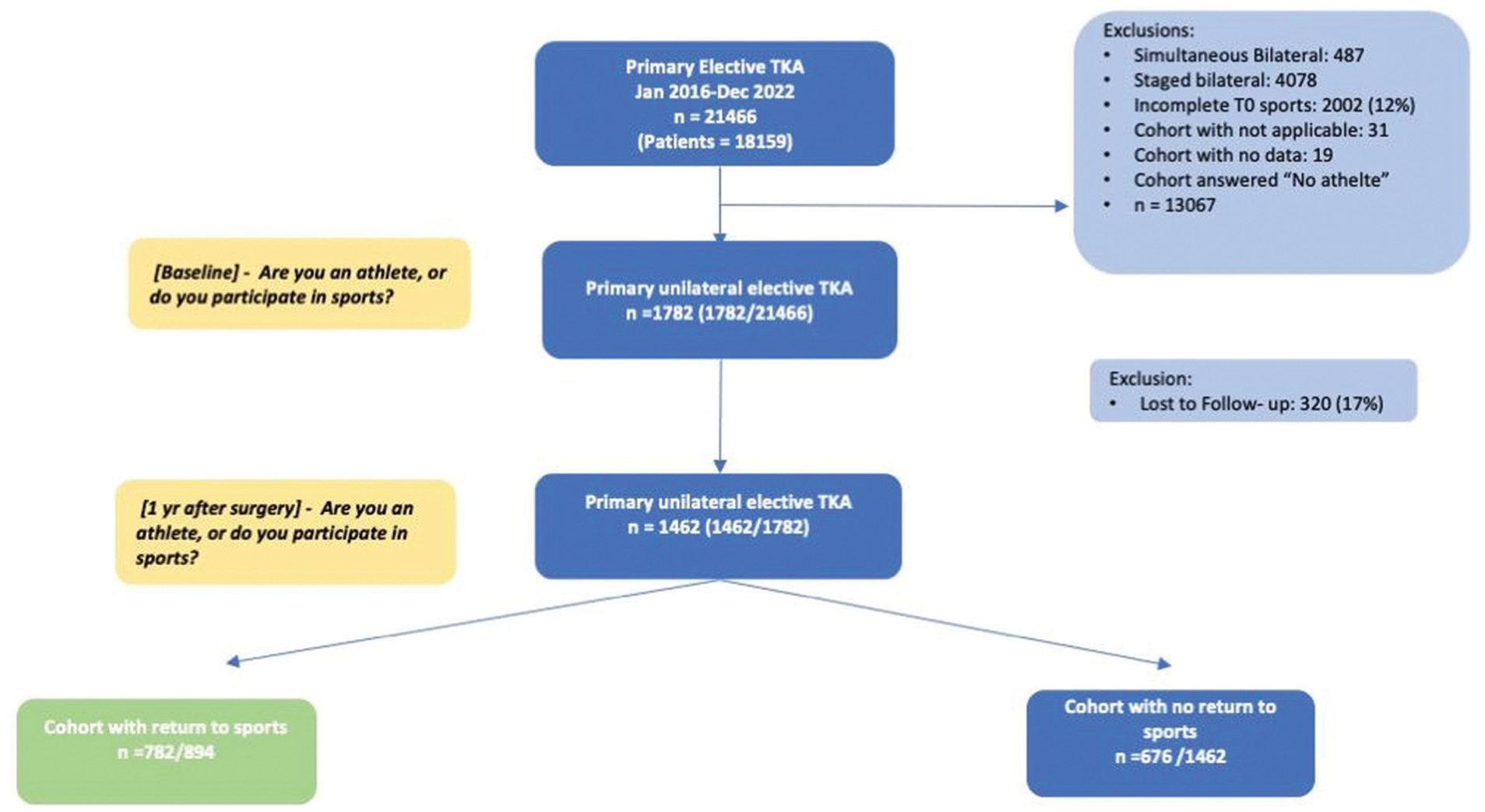
STROBE diagram. STROBE, Strengthening the Reporting of Observational Studies in Epidemiology; TKA, total knee arthroplasty.
Data Collection Process
Initial patient information was gathered electronically during preoperative consultations using tablet devices. The collected data encompassed demographic details (age, sex, and race), physical characteristics (body mass index), lifestyle factors (smoking status), health indicators (Charlson Comorbidity Index [CCI]), and educational background. Athletic participation was categorized into 3 groups: (1) nonparticipant; (2) recreational athlete; or (3) competitive athlete. All sports activities were included without restriction based on contact status or impact level. The assessment included baseline and 12-month measurements of the Knee injury and Osteoarthritis Outcome Score (KOOS), focusing on the pain and physical function short-form (PS) components. The 1-year evaluation also tracked RTS status and timing. RTS was defined as the resumption of any athletic or exercise activity after surgery. We predominantly used cemented fixation (88% cemented; 12% cementless in younger/good bone stock); implant constraint was mostly low-congruent: condylar-stabilized/medial-congruent in 52%, cruciate-retaining in 28%, posterior-stabilized in 17%, and varus-valgus constrained in 3%. After TKA, early pain and swelling are controlled, and mobilization is typically initiated within hours after surgery. Patients then undergo a structured course of supervised physical therapy, generally extending over 6 to 12 weeks, aimed at restoring range of motion, muscle strength, gait mechanics, and overall functional capacity. While recommendations for return to surgery depend on the surgeon and patient preferences, our institutions generally recommend an early return to activities as tolerated, starting with low-impact activities, followed by a gradual transition to higher-impact activities as tolerated. No agreement exists in our institutions. Patients undergoing cementless TKA are advised to be slightly more cautious regarding early RTS to allow for osseointegration. Still, long-term activity and RTS outcomes are comparable to those with cemented fixation and are heavily based on the patients’ tolerance.
After the initial assessment, patients selected their preferred contact method for follow-up communication. The 1-year postoperative surveys were distributed first through automated channels (email and patient portal) for 3 weeks. If patients did not respond, staff conducted manual outreach via phone or postal mail for an additional 4 weeks. Patients were classified as lost to follow-up if they failed to respond to at least 3 contact attempts through each communication channel (email, patient portal, and phone) during the 7-week postoperative period.
Statistical Methodology
The analysis began with calculating descriptive statistics for patient characteristics and PROMs. For categorical variables, results were presented as frequencies and percentages; continuous variables were expressed as means with standard deviations or medians with interquartile ranges, as appropriate. Comparisons between RTS and non-RTS groups were done using chi-square tests for categorical data and either 2-sample t tests or Wilcoxon rank-sum tests for continuous variables.
To examine factors influencing RTS timing, the study employed Cox proportional hazards regression models. The time to RTS was calculated as the weeks between surgery and first sports participation. Nonreturning patients were censored at 1 year. Model variables were selected in advance based on clinical relevance and prior research findings.
Multivariable logistic regression was used to analyze factors associated with inability to RTS at 1 year. Independent variables were selected using criteria similar to those for the Cox models. Model performance was assessed using the area under the receiver operating characteristic curve. Statistical significance was defined at α = .05. Analyses were conducted using R software Version 4.0.3 (R Foundation for Statistical Computing).
Results
Baseline Characteristics
The mean age of the cohort was 66.1 years, with no significant difference between the RTS and non-RTS groups (66 vs 66.2 years; P = .678). Sex distribution differed significantly, with men more likely to RTS (71.8% vs 65.5%; P = .012). Significant differences were observed in race, where White patients had higher RTS rates (92.1% vs 86.8%). The CCI was lower among patients who returned to sports (mean 0.8 vs 1.0; P = .005). Insurance status was also associated with RTS, with Medicaid patients being underrepresented among those who returned (1.3% vs 2.2%), while Medicare (49.4% vs 44.5%) and commercial insurance (39.2% vs 39.2%) distributions were similar between groups (P = .032) (Table 1).
Demographic and Clinical Characteristics of Patients Based on RTS Status After TKA a
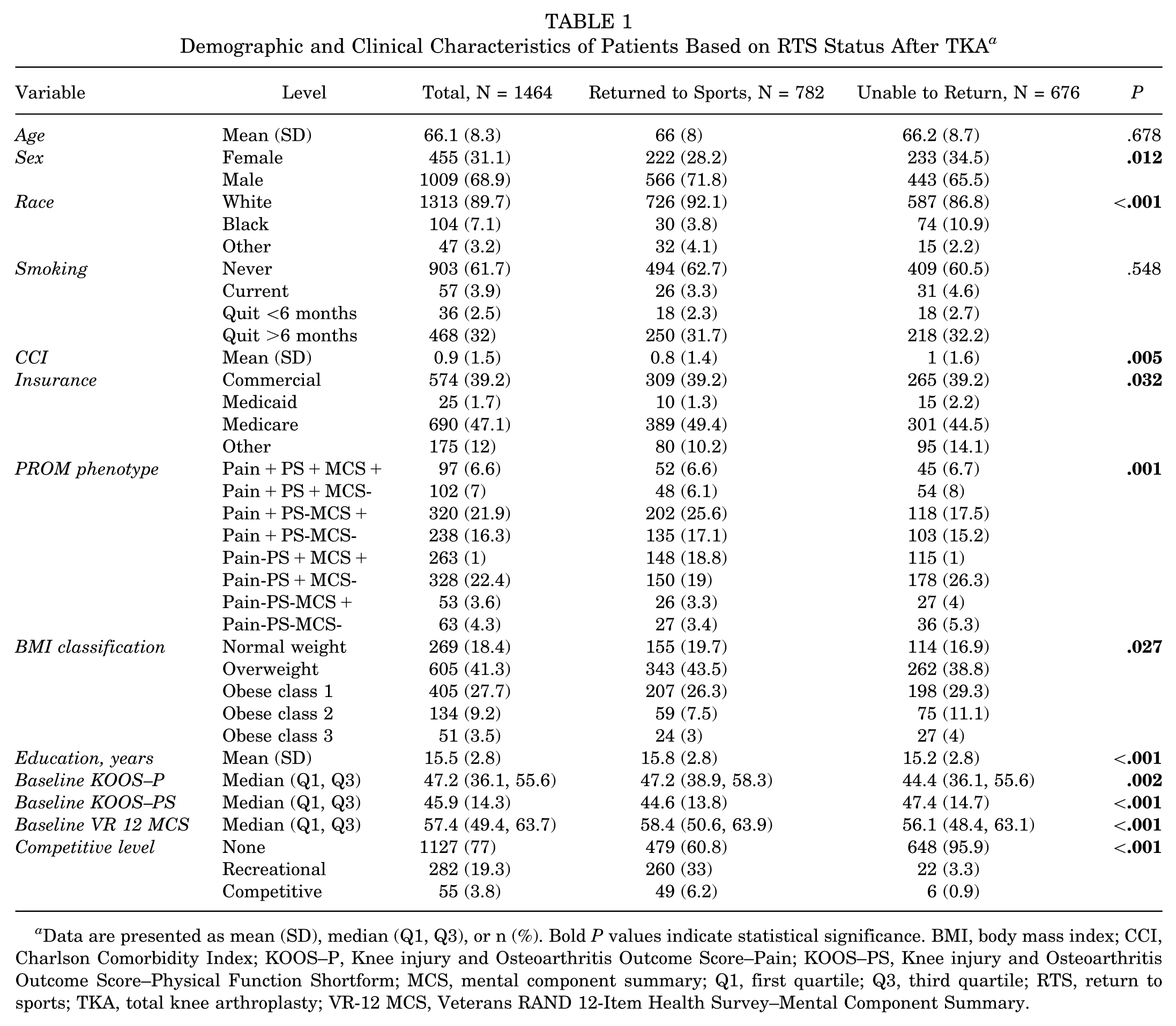
Data are presented as mean (SD), median (Q1, Q3), or n (%). Bold P values indicate statistical significance. BMI, body mass index; CCI, Charlson Comorbidity Index; KOOS–P, Knee injury and Osteoarthritis Outcome Score–Pain; KOOS–PS, Knee injury and Osteoarthritis Outcome Score–Physical Function Shortform; MCS, mental component summary; Q1, first quartile; Q3, third quartile; RTS, return to sports; TKA, total knee arthroplasty; VR-12 MCS, Veterans RAND 12-Item Health Survey–Mental Component Summary.
RTS Rates and Timelines
Of the 1464 patients who completed the 1-year follow-up, 782 (53.4%) were able to RTS, while 676 (46.6%) were unable to RTS (Table 1). Patients who were able to RTS had significantly higher preoperative KOOS–Pain scores (median, 47.2 [interquartile range, IQR, 38.9-58.3] vs 44.4 [IQR, 36.1-55.6]; P = .002), lower (better) preoperative KOOS–PS scores (median, 44.6 [IQR, 13.8] vs median, 47.4 [IQR, 14.7]; P < .001), and higher preoperative VR-12 MCS scores (median 58.4, [IQR, 50.6-63.9] vs median, 56.1 [IQR, 48.4-63.1]; P < .001) compared with those who did not RTS. They also had a higher proportion with post-high school education (mean 15.8 vs 15.2 years; P < .001) (Table 1).
Among those who returned to sports, 62% did so at the same sport and level of intensity/performance as before surgery, 34.5% returned with reduced effort or performance, and 3.4% were able to RTS overall but not to the same sport they participated in before TKA (Figure 2).
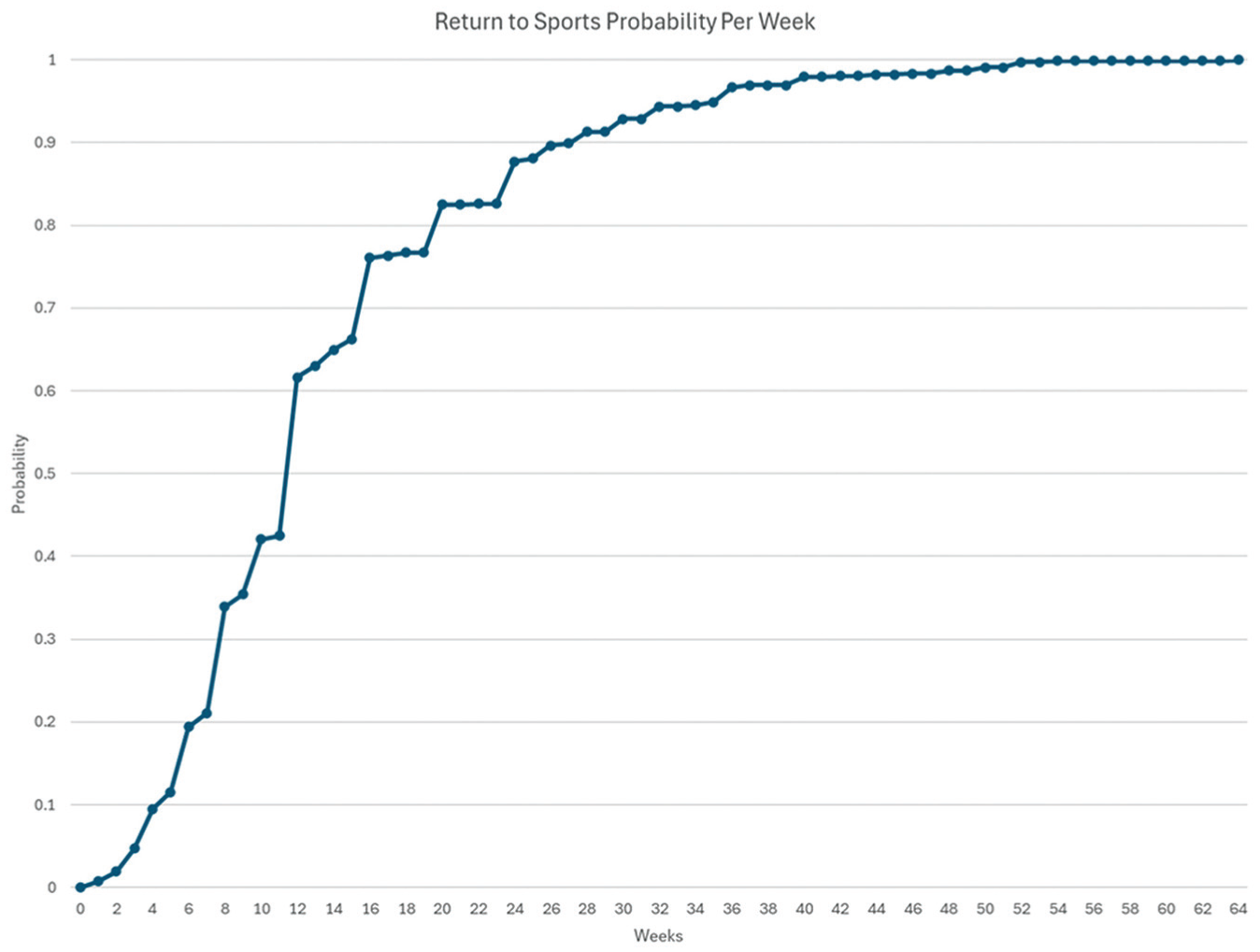
Cumulative probability of time to return to sports after total knee arthroplasty.
The median time to RTS was 12 weeks, with 90% of patients restarting sports participation within 27 weeks after surgery. Patients with Medicaid insurance experienced a delayed RTS compared with those with commercial insurance (hazard ratio [HR], 0.51 [95% CI, 0.26-0.99]). Overweight patients (body mass index [BMI], 25-29.9 kg/m2) returned to sports sooner than normal-weight patients (HR, 1.41 [95% CI, 1.14-1.74]). Recreational athletes had a longer time to RTS compared with competitive athletes (HR, 0.77 [95% CI, 0.66-0.90]) (Table 2).
Cox Regression Analysis for Time to RTS After TKA a
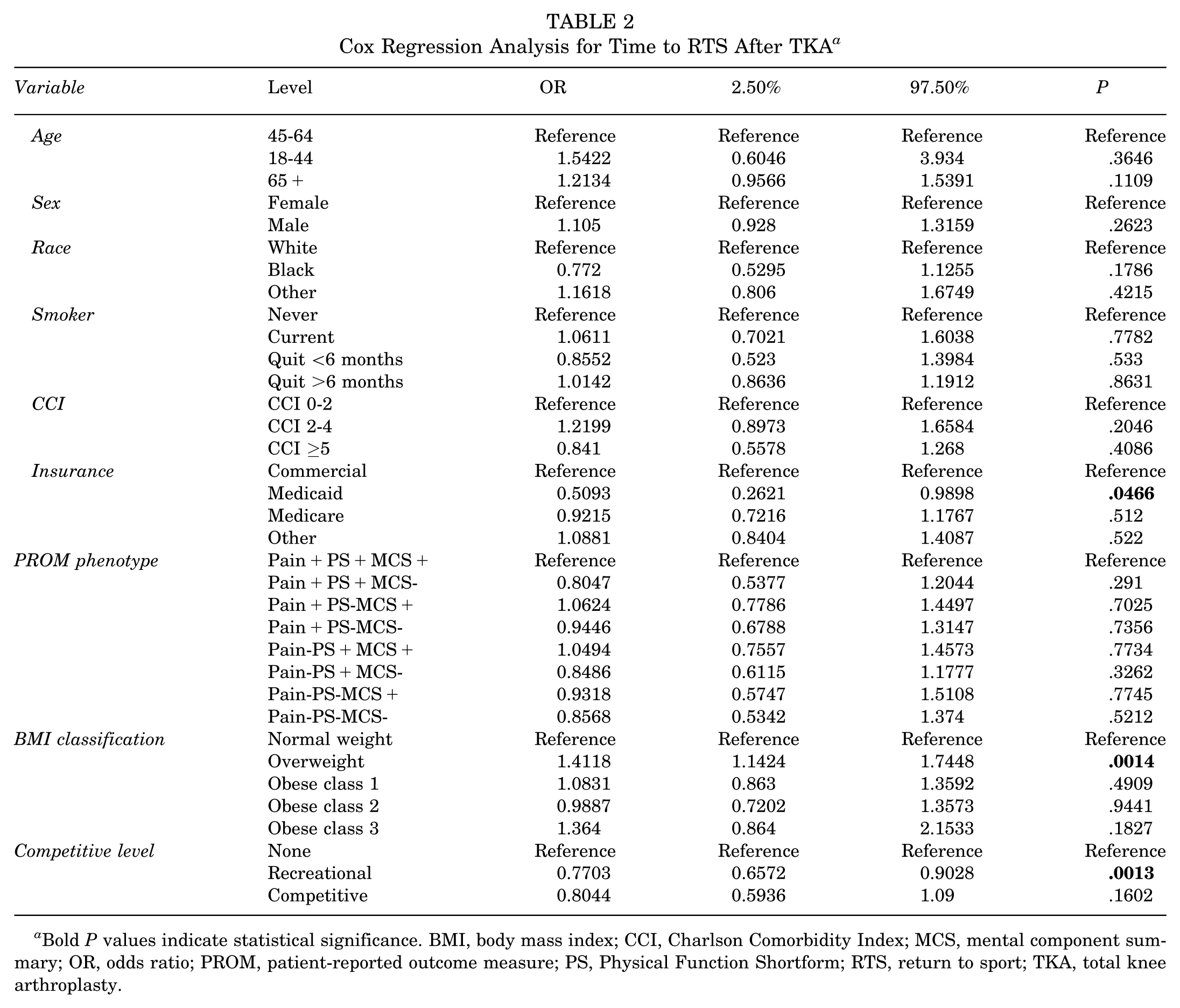
Bold P values indicate statistical significance. BMI, body mass index; CCI, Charlson Comorbidity Index; MCS, mental component summary; OR, odds ratio; PROM, patient-reported outcome measure; PS, Physical Function Shortform; RTS, return to sport; TKA, total knee arthroplasty.
Factors Associated with Inability to RTS
In the multivariable logistic regression analysis, female sex was associated with lower odds of RTS compared with male patients (odds ratio [OR], 0.76 [95% CI, 0.58-0.98]). The Black race was associated with a higher odds of not returning to sports than the White race (OR, 2.34 [95% CI, 1.43-3.93]). Patients with a CCI score of 2 to 4 had higher odds of not returning to sports compared with those with a CCI score of 0 to 2 (OR, 1.70 [95% CI, 1.09-2.70]).
Being a recreational athlete (OR, 0.06 [95% CI, 0.04-0.10]) or competitive athlete (OR, 0.10 [95% CI, 0.04-0.22]) was associated with significantly higher odds of RTS compared with being a nonathlete. Other factors, such as age, BMI category, smoking status, insurance type, and PROM phenotype, were not significantly associated with inability to RTS in the final model (Table 3).
Multivariable Logistic Regression Analysis for Factors Associated With Inability to RTS at 1 Year After TKA a
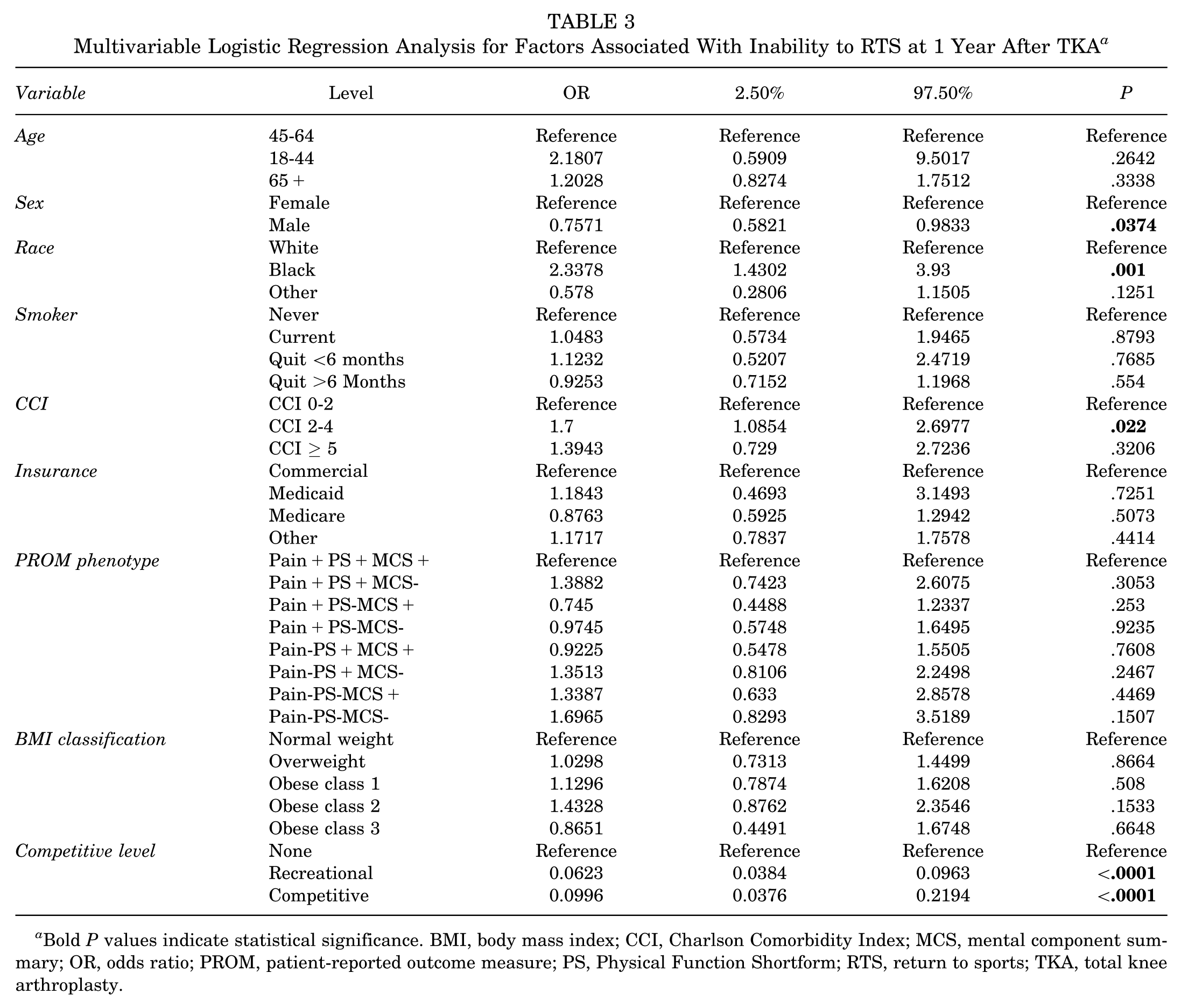
Bold P values indicate statistical significance. BMI, body mass index; CCI, Charlson Comorbidity Index; MCS, mental component summary; OR, odds ratio; PROM, patient-reported outcome measure; PS, Physical Function Shortform; RTS, return to sports; TKA, total knee arthroplasty.
Discussion
This large prospective cohort study provides important insights into the RTS timeline, level, and determinants after TKA. We found that over half of patients who were involved in sports preoperatively successfully returned within 1 year, with a median time of 12 weeks. However, RTS rates and timelines varied based on patient characteristics, comorbidities, and preoperative sports participation level.27,54 With the rapid growth in TKAs performed in younger patients with higher expectations and physical demands, evidence-based recommendations for RTS are increasingly important.4,1
Our findings build on previous studies demonstrating that RTS is an achievable goal for many TKA patients. In a systematic review, Witjes et al 52 reported RTS rates ranging from 36% to 89% across 18 studies. Most recently, Magan et al 24 reported a pooled RTS rate of 87% among 1307 patients from 9 studies. We observed a lower 53% rate, which may reflect our larger sample size and adjustment for loss to follow-up.28,42 Hepperger et al, 13 using a similar methodology to our study, reported 76% sports participation at 2 years after TKA. Importantly, studies with longer-term follow-up suggest some attrition in sports participation over time 24 ; thus, our 1-year results likely represent a peak time point.
In terms of the RTS timeline, our cohort returned to sports at a median of 12 weeks, with 90% returning by 27 weeks, aligning with systematic reviews.3,33 An umbrella review by Lester et al 20 reported that across 10 studies, 70% to 100% of patients returned to their desired sport by 6 months after TKA. A survey study of 1792 patients by Peters et al. 41 found that a 3- to 6-month RTS timeframe was most common. While the literature supports our findings that a majority of patients RTS between 3 to 6 months post-TKA, the high variability between studies underscores the need for a personalized, criteria-based approach rather than a generic postoperative timeline.
Numerous patient factors influence the ability and timeline for RTS after TKA. Consistent with our findings, younger age, male sex, lower BMI, and less medical complexity have previously been associated with higher RTS rates.11,24 This likely reflects the better overall health, physical conditioning, and motivation of these patient subgroups. Notably, we found that preoperative sports participation level was the strongest predictor of postoperative RTS—with both recreational and competitive athletes having 10-fold greater odds of returning compared with nonathletes.16,53 This highlights the importance of understanding patients' prearthritic activity levels to manage postoperative expectations. Those who were sedentary before surgery are less likely to adopt active pursuits afterwards, regardless of knee-specific improvements. 26 Surgeons should thus consider not only the technical aspects of the procedure, but also ways to optimize patients' participation, such as presurgical exercise, weight loss, and pain coping skills. A key limitation in the RTS literature is the lack of a standardized, validated definition. Studies variably define RTS as any postoperative participation, return to the same sport, return at preoperative frequency, or achievement of activity-scale thresholds, resulting in wide heterogeneity and limited comparability. PROMs provide important complementary information, capturing pain, function, satisfaction, and quality of life. However, PROM selection is inconsistent, and many instruments demonstrate limited validity, responsiveness, or long-term sensitivity.41,46 Standardizing RTS definitions and incorporating rigorously validated PROMs are essential to enhance both research comparability and clinical utility.
This study has several limitations. This study lacked a clear, validated metric for defining sports resumption, making it difficult to compare results with existing research. RTS was defined as resumption of any athletic or exercise activity after surgery, which may lead to interpretive bias. Additionally, no specific criteria were established for what constituted sufficient athletic participation, potentially leading to classification errors, as the data were based on patients' self-identification. Such a distinction is highly relevant and should be addressed in further studies. Further studies may benefit from investigating sports participation and activity level using measures such as KOOS domains, Tegner, and Lysholm scores. The investigation did not document the specific factors that prevented individuals from resuming athletic activities, leaving uncertainty about whether knee conditions, shifting personal priorities, or other health concerns were responsible. The study's timeframe of 12 months may have been insufficient to fully document all relevant athletic outcomes, including delayed RTS, sustainability of sports activity, and long-term participation patterns. Also, the time to RTS was based on patients’ recall, which may lead to recall bias. Furthermore, our analysis did not stratify patients by sport type (e.g., contact vs. noncontact, high- vs. low-impact), limiting the ability to evaluate how different activity profiles influence RTS rates. Future studies should address this gap. Moreover, since the procedures were all conducted by skilled surgeons at a single specialized medical facility, these outcomes may not accurately reflect results from different health care settings or diverse patient groups.
Conclusion
Over half of athletes who were involved in sports before TKA returned to sports within 1 year of surgery, with a median time to return of 12 weeks, and 90% returned within 27 weeks. However, RTS rates varied based on preoperative competitive level, sex, race, BMI, and comorbidity burden. Providers should consider these factors when counseling patients on their postoperative goals and potential barriers to RTS. There is a need for studies stratifying outcomes by sport type and impact level to provide more individualized recommendations for patients.
Footnotes
Submitted October 20, 2025; accepted November 1, 2025.
Disclosure:
N.S.P. has received consulting fees from Stryker, Pacira, and Zimmer; holds stock or stock options in Osteal Therapeutics; and research support from Osteal Therapeutics, Peptilogics, RegenLab, Signature Orthopedics, Zimmer, and Stryker; serves on the editorial board of The Journal of Bone and Joint Surgery; and holds committee appointments with the American Association of Hip and Knee Surgeons and the Orthopaedic Research Society. M.E.D. has received royalties from Brasseler; holds stock in Romtech; and serves on the editorial board of the Journal of Knee Surgery. All other authors report no relevant financial relationships. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.