
Abstract
Background:
Meniscal allograft transplantation (MAT) is an emerging treatment for patients with symptomatic meniscal deficiency.
Purpose:
To systematically evaluate the long-term clinical outcomes and graft survivorship of MAT with a minimum follow-up of 10 years.
Study Design:
Systematic review and meta-analysis; Level of evidence, 4.
Methods:
A review was conducted following PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines and registered on Prospero. The PubMed, Cochrane Central Register of Controlled Trials, and Scopus databases were queried in January 2025. Studies assessing MAT patient-reported or objective outcomes with ≥10 years of follow-up were included. Non–English-language studies, case reports, non–peer-reviewed articles, editorials, commentaries, and reviews were excluded. The Lysholm score, Tegner Activity Scale score, visual analog scale (VAS) for pain score, Knee injury and Osteoarthritis Outcome Score (KOOS), and graft survivorship were extracted for analysis. MAT failure was defined by individual studies based on clinical, surgical, and/or radiographic criteria.
Results:
Thirteen studies, consisting of 619 patients and 632 MATs and performed from 1984 to 2012, met inclusion criteria. The mean patient age ranged from 24.5 to 43.5 years, with 47% to 87% males and a mean follow-up duration of 11.1 to 20.0 years. Fixation techniques included soft tissue (5 studies), bone plug (6 studies), and bone trough (4 studies). Statistically significant improvements were observed in the Lysholm score (7/9 studies), Tegner score (3/4 studies), VAS score (3/5 studies), and KOOS (1/1 studies). Two studies reported Patient Acceptable Symptom State rates ranging from 70.2% to 71% for Lysholm score and 58.5% to 82% for KOOS. Two studies also reported minimal clinically important difference rates, which ranged from 70.4% to 89.9% for the Lysholm score and 61% to 78.2% for the KOOS subscales. Ten-year MAT survival ranged from 45% to 100%. Most studies (5/9) demonstrated survivorship ≥73% at a minimum 10-year follow-up. MAT survival after ≥15 years ranged from 19% to 87%.
Conclusion:
MAT demonstrated favorable long-term clinical outcomes and variable graft survivorship beyond 10 years. Included studies varied based on graft type, fixation technique, and patient selection. Continued prospective, high-level studies are warranted to standardize surgical approaches, improve the durability of this joint-preserving intervention, and identify modifiable risk factors for inferior long-term outcomes.
The meniscus is a fibrocartilage structure within the tibiofemoral joint that plays a crucial role in knee joint stabilization and shock absorption. 23 Damage or deficiency of the meniscus can accelerate articular cartilage degeneration, leading to pain, mechanical symptoms, and early osteoarthritis.11,23 Injuries to the meniscus are among the most common orthopaedic pathologies, with an annual incidence of 13.2 tears per 10,000 individuals. 6 These injuries can occur as a result of sport, trauma, or degenerative processes, often severely limiting knee function and patient quality of life. 21 Effective management of meniscal injuries is vital to alleviate pain, restore function, and prevent long-term joint deterioration, especially in young and active patients.2,14
Meniscal allograft transplantation (MAT) is indicated in patients <50 years of age with symptomatic meniscal deficiency (usually after menisectomy), who have minimal to no existing osteoarthritis and correctable malalignment to optimize the success of the procedure.7,12,20 MAT involves the transplantation of a donor (allograft) meniscus to restore functional knee biomechanics and potentially delay the progression of osteoarthritis. While the native meniscus has a well-established protective effect against osteoarthritis, the degree to which MAT confers similar chondroprotective benefits remains less certain.2,20,31,37 Multiple fixation techniques for MAT have been described, including suture-only, bone plug, and/or bone bridge (trough) fixation. Recently, additional techniques such as meniscotibial ligament reconstruction have been increasingly used to secure the meniscal body to the tibia and reduce the risk of graft extrusion.3,9 While fixation modalities remain mixed across the literature, previous studies have suggested that bone plug fixation may encourage improved allograft stability, a lower risk of graft failure, and a decreased reoperation rate compared with suture-only and bone bridge fixation methods.1,20,28,44
Despite increasing utilization across specialized orthopaedic centers, MAT remains technically demanding and uncommon worldwide.7,12,36 Previous literature has suggested that MAT demonstrates promise as a modality associated with improved patient-reported outcomes and survivorship rates of >70% at 10 years.4,12,25,38,43 While short- and midterm studies report improved clinical and functional outcomes, limited high-quality evidence assesses the long-term efficacy of MAT.
∥
Understanding the long-term outcomes and graft survivorship of MAT is critical for guiding surgical decision-making and patient counseling. As such, the purpose of this study was to systematically evaluate the long-term clinical outcomes and graft survivorship of MAT with a minimum follow-up of 10 years. We hypothesized that MAT provides sustained improvements in pain and function
Methods
This systematic review was performed in accordance with PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines. 29 The protocol was prospectively registered in the PROSPERO database (registration ID: 42025640240), ensuring methodological transparency and adherence to established review standards.
Search Strategy
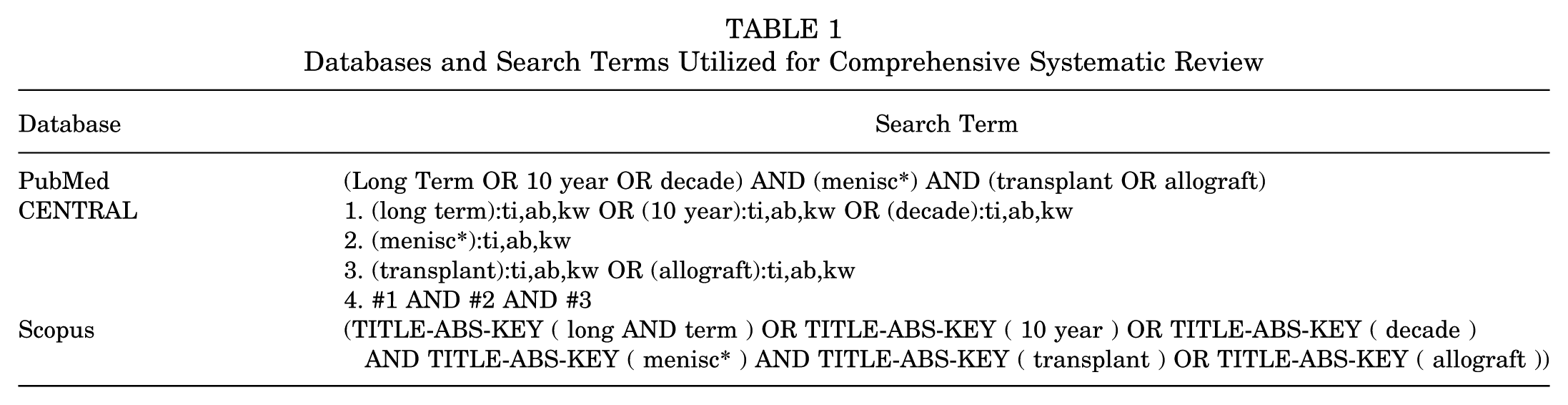
A systematic literature search was performed in January 2025 using the PubMed, Cochrane Central Register of Controlled Trials (CENTRAL), and Scopus databases. The search strategy combined terms related to MAT and long-term outcomes, including “meniscus,”“allograft,”“transplantation,”“minimum 10-year,” and “long-term.” Detailed search strings for each database are provided in Table 1.
Databases and Search Terms Utilized for Comprehensive Systematic Review
Eligibility Criteria
Included studies described patient-reported and functional outcomes associated with MAT at a minimum of 10 years after surgery. MAT failure was defined according to individual study criteria, including radiographic, surgical, or clinical endpoints. Studies were included if they involved human patients undergoing MAT for symptomatic meniscal deficiency. Exclusion criteria consisted of non–English-language publications, animal or cadaveric studies, case reports, editorials, commentaries, review articles, and studies lacking peer review. All studies that met inclusion and exclusion criteria were included regardless of year of publication, in order to maximize the capture of long-term outcomes after MAT.
Screening and Study Selection
All references were imported into Covidence (Veritas Health Innovation; www.covidence.org) for systematic screening. Two independent reviewers (J.D.K. and S.S.) screened titles and abstracts for relevance based on predefined inclusion and exclusion criteria. Full-text review was performed for studies meeting initial screening criteria. Discrepancies during study selection were resolved through consensus with a third reviewer (A.J.), a fellowship-trained orthopaedic sports medicine surgeon.
Data Extraction
A data extraction template was created in Microsoft Excel. Two blinded reviewers (J.D.K. and S.S.) independently performed data extraction. Information extracted included study design, level of evidence, sample size, study period, follow-up duration, patient demographics (age, sex, and body mass index [BMI]), surgical techniques, graft types, and concomitant cartilage procedures. Outcomes extracted included Lysholm score, Tegner Activity Scale score, Knee injury and Osteoarthritis Outcome Score (KOOS), visual analog scale (VAS) for pain score, MAT survival, and failure rates. Any discrepancies in the data extraction process were resolved by an independent third author (A.J.).
Quality Assessment
Methodological quality was assessed using the Methodological Index for Non-Randomized Studies (MINORS) instrument. 35 This tool provides a maximum score of 16 for noncomparative studies and 24 for comparative studies. Studies scoring <14 were classified as poor quality, those scoring between 15 and 19 were considered moderate quality, and those scoring between 20 and 24 were categorized as high quality. 35 Two independent reviewers (J.D.K., S.S.) performed the scoring assessment, and discrepancies were resolved through consultation with a third reviewer (A.J.). A weighted Cohen kappa calculation was performed to assess the interrater reliability of MINORS scoring. 8
Statistical Analysis
Review Manager (RevMan; Version 5.4; The Cochrane Collaboration) was used to assess heterogeneity in patient-reported outcomes reported in ≥3 studies that included preoperative and postoperative values with standard deviations. Additionally, 10- and ≥15-year implant survival were assessed using RStudio (Posit) with R software Version 4.5.0 (R Foundation for Statistical Computing) with the ‘meta’ package (Version 8.1-0; Guido Schwarzer). Study proportions were pooled using inverse variance weighting. Heterogeneity was quantified using the I2 statistic, which measures the proportion of total variation across studies due to heterogeneity rather than chance. Between-study heterogeneity was assessed using the I2 statistic, with values of 25%, 50%, and 75% representing low, moderate, and high heterogeneity, respectively. 17 Statistical significance was defined as a P value <.05.
Results
Study Identification and Characteristics
A systematic search of the PubMed, Scopus, and CENTRAL databases identified a total of 1049 studies. After the removal of duplicates, titles and abstracts were screened for relevance. A total of 40 full-text articles were assessed for eligibility, of which 13 studies met the inclusion criteria and were included in the final analysis. ¶ The study selection process is detailed in the PRISMA flow diagram (Figure 1).
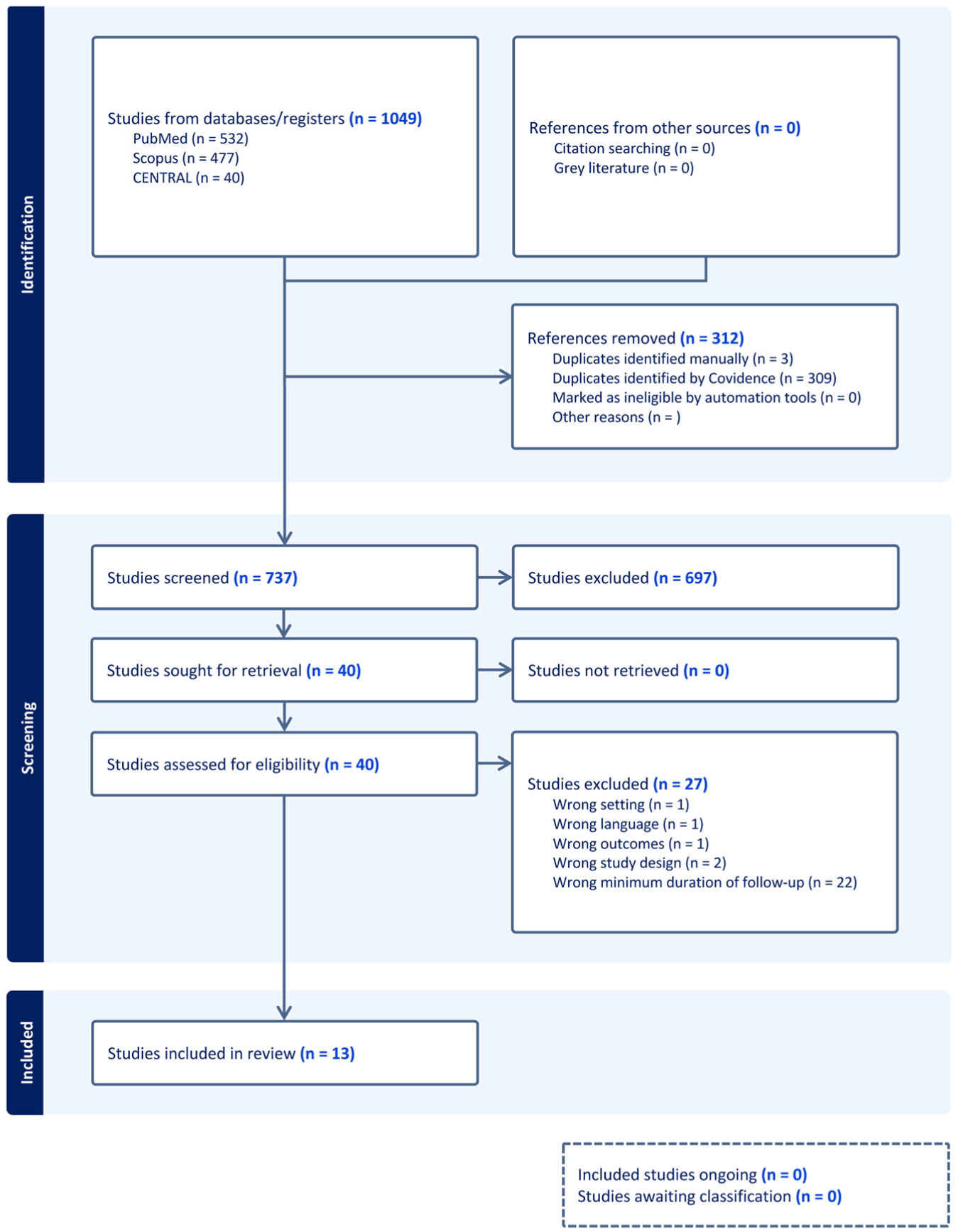
Flowchart according to PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines.
Study Characteristics and Demographics
Tables 2 and 3 summarize key study characteristics, including study design, level of evidence, study period, and patient demographics. Thirteen studies, consisting of 619 patients and 632 MATs, met inclusion criteria. # The analyzed studies included 9 case series, ** 2 retrospective cohort studies,40,43 and 2 prospective cohort study 31 ; all were classified as level 337,45 or 413,15,20,26,31,32,39-43 evidence. MINORS scores among included studies ranged from 9 20 to 19 45 (Figure 2). The weighted Cohen kappa demonstrated excellent interrater reliability of MINORS scoring (κ = 0.83).
Study Characteristics and Design a
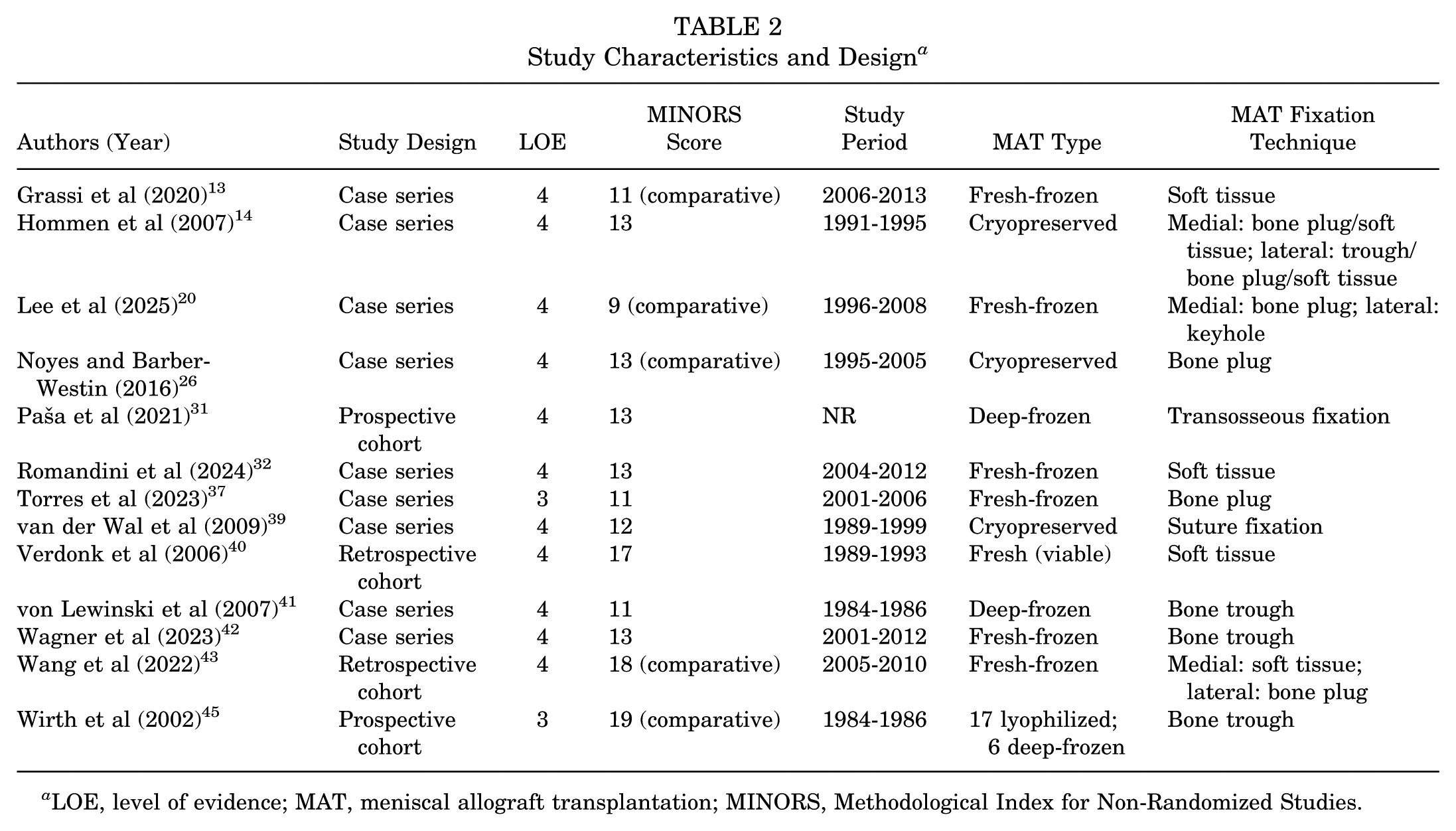
LOE, level of evidence; MAT, meniscal allograft transplantation; MINORS, Methodological Index for Non-Randomized Studies.
Study Characteristics a
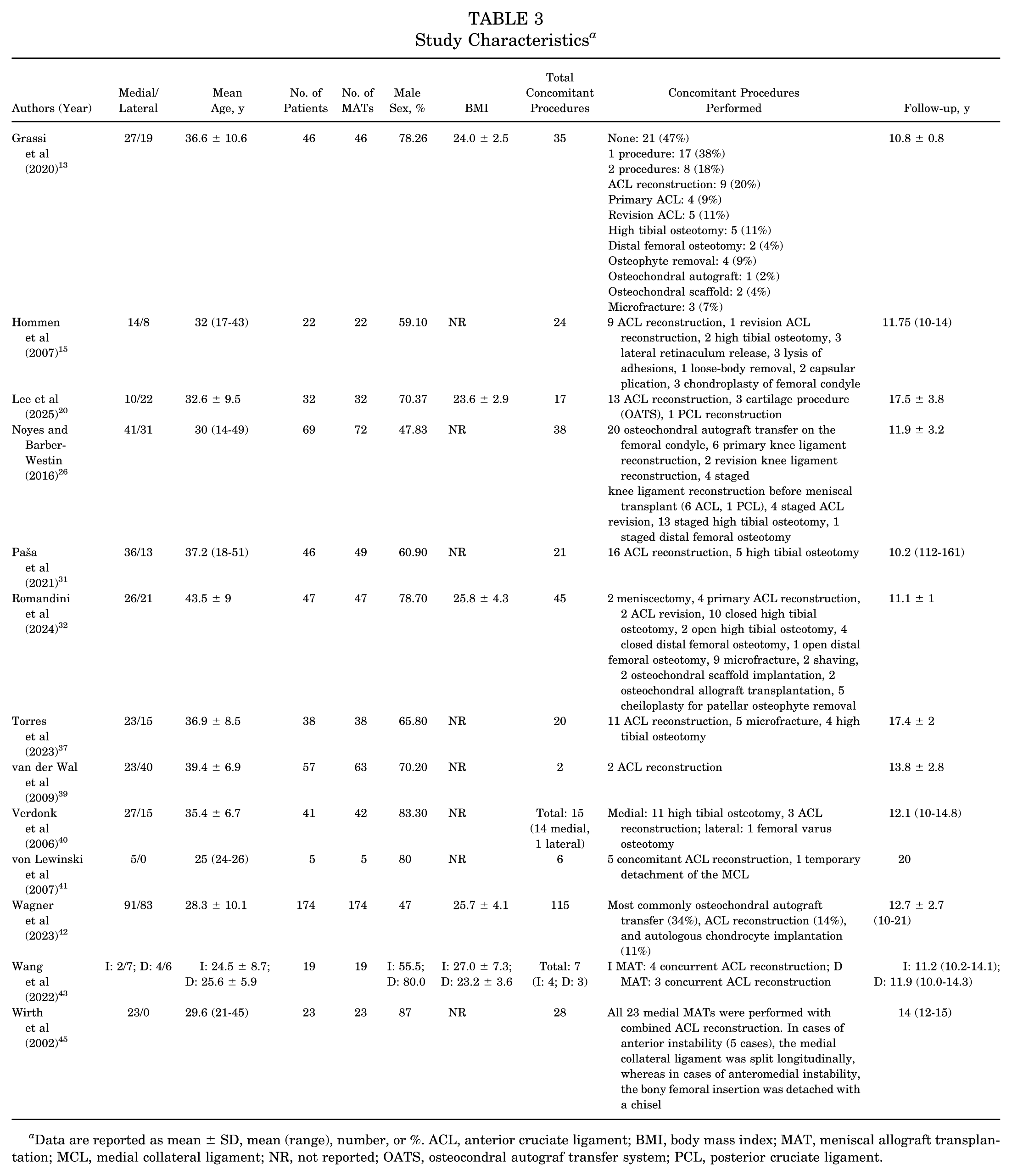
Data are reported as mean ± SD, mean (range), number, or %. ACL, anterior cruciate ligament; BMI, body mass index; MAT, meniscal allograft transplantation; MCL, medial collateral ligament; NR, not reported; OATS, osteocondral autograf transfer system; PCL, posterior cruciate ligament.
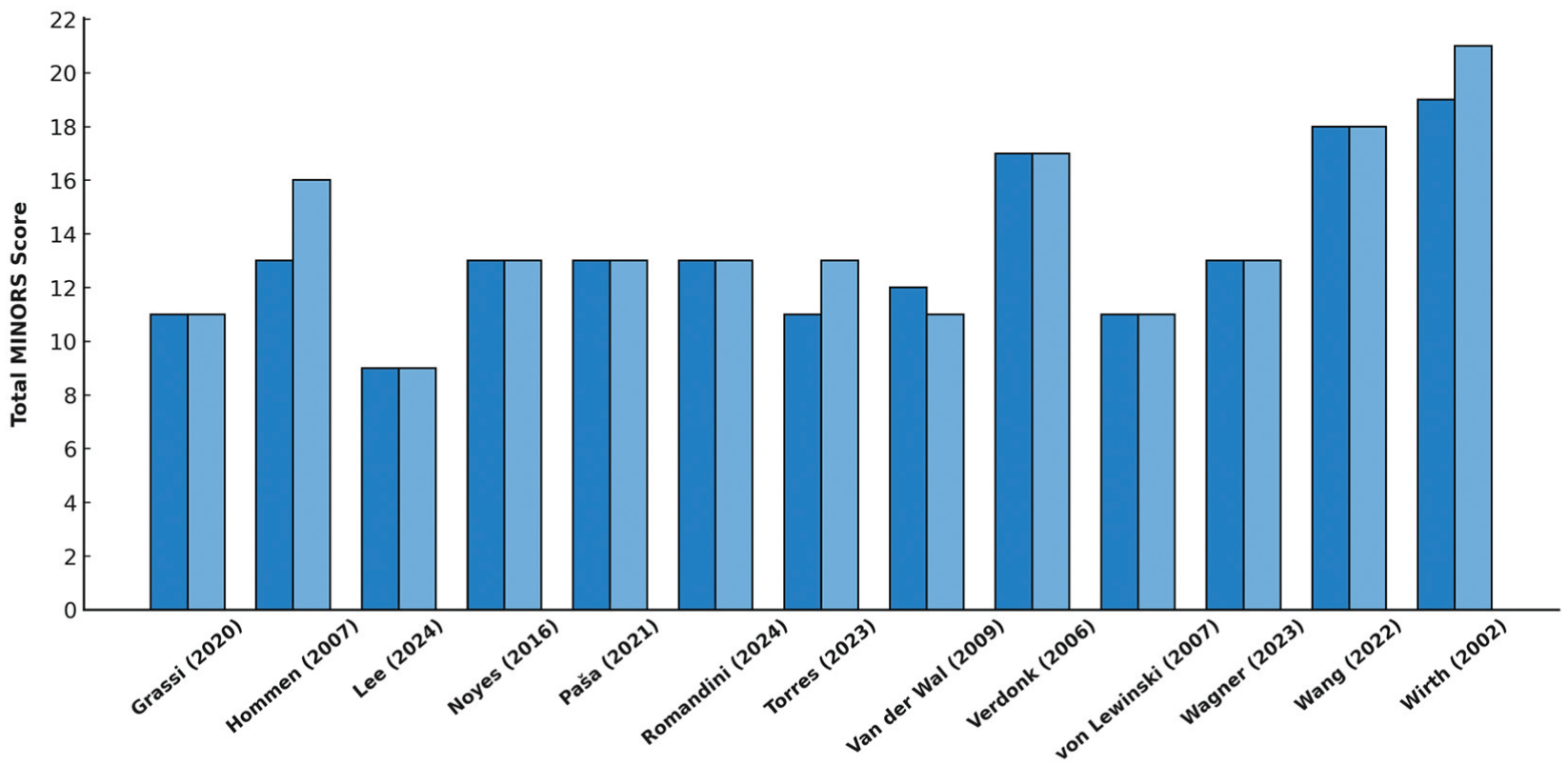
Comparison of initial Methodological Index for Non-Randomized Studies (MINORS) scoring and study quality assessment performed by Reviewer 1 (J.D.K; light blue) and Reviewer 2 (S.S.; dark blue). The weighted Cohen kappa demonstrated excellent interrater reliability of MINORS scoring between reviewers (κ = 0.83).
Study periods ranged from 198441,45 to 2013, 13 with sample sizes varying from 5 41 to 174 42 total patients. The mean patient age ranged between 24.5 years 43 and 43.5 years, 32 with male patients comprising 47% 42 to 87% 45 of the study populations. BMI values were reported in 5 studies, ranging from 23.2 kg/m2 to 27.0 kg/m2. 43 The mean follow-up duration across all studies ranged from 11.1 years 32 to 20 years. 41
The meniscal allografts utilized varied in type and preservation method. Fresh-frozen allografts were most frequently reported and were used in 6 studies,13,20,32,37,42,43 whereas cryopreserved allografts were used in 3 studies.15,26,39 Deep-frozen allografts were documented in 3 studies,31,41,45 and lyophilized allografts were used in 1 study. 45 One study used fresh (viable) allografts. 40
The fixation techniques used exhibited considerable variability (Table 2). Soft tissue fixation was used in 5 studies,13,15,32,40,43 while bone plug fixation was reported in 5 studies,15,20,26,37,43 including 1 using a transosseous technique. 31 Four studies utilized bone trough (bridge-in-slot) fixation.15,41,42,45
Survivorship and Failure Rates
Graft survival was reported in 10 studies (Table 4). †† Among these, 4 of 10 studies (40.0%) demonstrated 10-year survivorship rates exceeding 73%.20,31,32,42 Reported 10-year MAT survival ranged from 45% to 100%, with the highest rates observed in lateral meniscus allograft cases. 31 Five studies reported survival rates with a minimum of 15 years of follow-up.20,26,37,39,42 The MAT survival rate after a mean follow-up of ≥15 years ranged from 19% to 87%, with Lee et al 20 reporting an 87% survival rate at 17.5 years, Torres et al 37 58% at 17.4 years, van der Wal et al 39 52.5% at 16 years, Wagner et al 42 72% at 15 years, and Noyes and Barber-Westin 26 demonstrating a decline in survival from 45% at 10 years to 19% at 15 years.
Survival and Failure Rates a
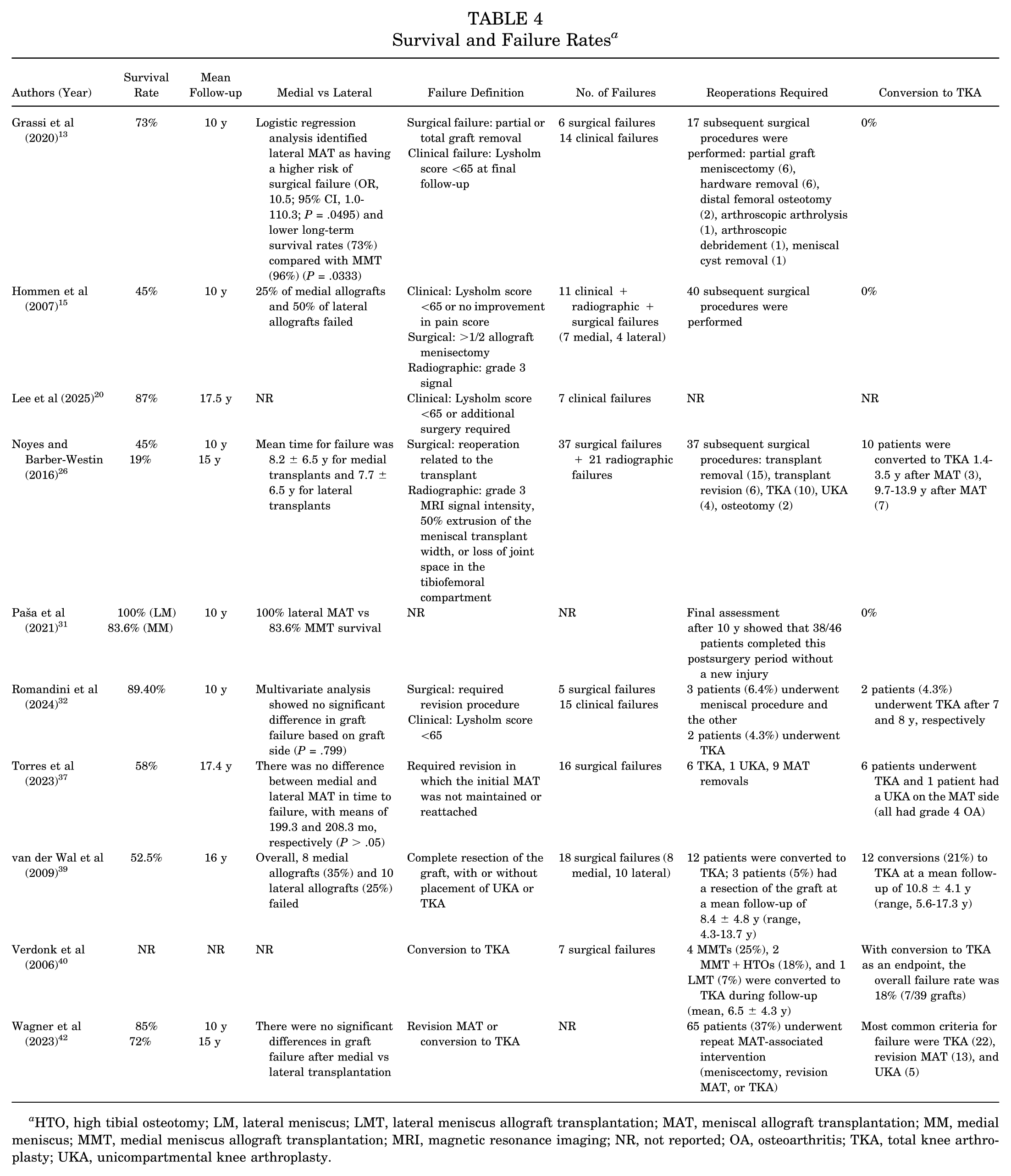
HTO, high tibial osteotomy; LM, lateral meniscus; LMT, lateral meniscus allograft transplantation; MAT, meniscal allograft transplantation; MM, medial meniscus; MMT, medial meniscus allograft transplantation; MRI, magnetic resonance imaging; NR, not reported; OA, osteoarthritis; TKA, total knee arthroplasty; UKA, unicompartmental knee arthroplasty.
A pooled analysis of 10-year survival data across 5 studies demonstrated a survivorship rate of 70.9% (95% CI, 48.0%-86.5%) with notable between-study heterogeneity (I2 = 92.2%) (Figure 3).13,15,26,32,42 Similarly, pooled survival at ≥15 years was 58.4% (95% CI, 33.0%-80.0%) across a separate subset of 5 studies, again with substantial between-study heterogeneity (I2 = 93%) (Figure 4).20,26,37,39,42
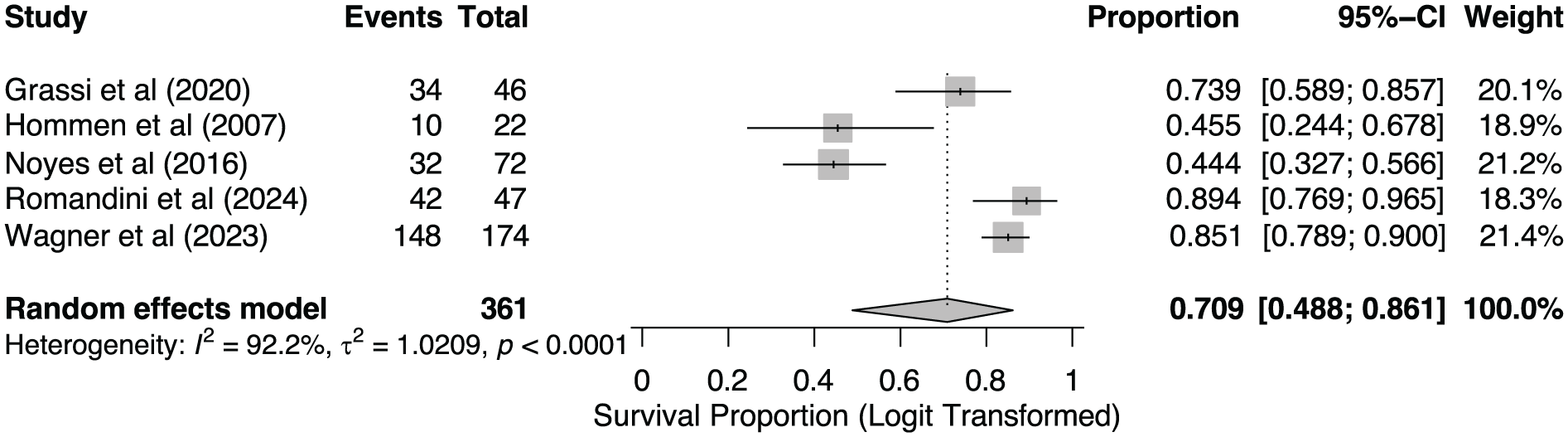
Forest plot of meniscal allograft survival proportions at 10 years postoperatively. Individual study survival estimates and 95% confidence intervals were calculated using a Wald-type method. The pooled survival proportion was 70.9% (95% CI, 48.0%-86.5%). Between-study heterogeneity was high (I2 = 92.2%).
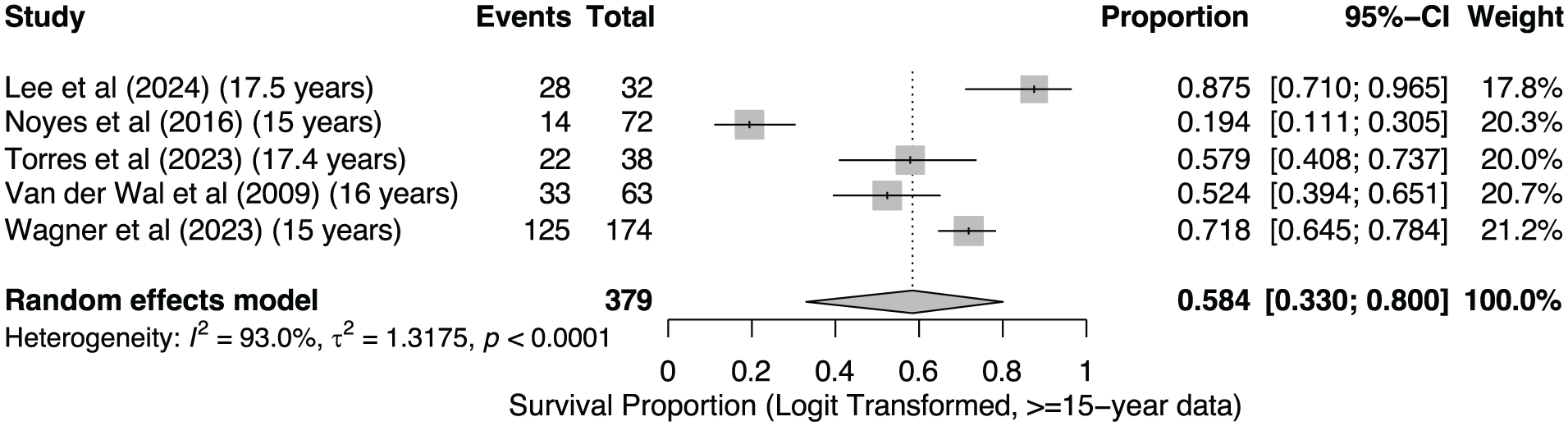
Forest plot of meniscal allograft survival proportions at ≥15 years postoperatively. Individual study survival estimates and 95% confidence intervals were calculated using a Wald-type method. The pooled survival proportion was 58.4% (95% CI, 33.0%-80.0%). Between-study heterogeneity was high (I2 = 93%).
Six studies assessing MAT survivorship before 2004 were found to have ≥10-year survival rates ranging from 45% to 87%.15,20,26,37,39,42 Alternatively, only 2 studies exclusively analyzed MATs performed from 2004 or later, reporting 73% to 89.4% survival.13,32
Among different allograft types, fresh-frozen meniscal grafts demonstrated a 58% to 89.4% ≥10-year survival rate across 5 studies (3/5 studies ≥85% survivorship).13,20,32,37,42 Alternatively, 3 studies using cryopreserved allografts demonstrated survivorship ranging from 45% to 52.5%.15,25,39 Only 1 study reported survivability in the context of deep-frozen allografts, underscoring an 83.6% survival rate for medial menisci and 100% survival for lateral menisci in a cohort of 49 total MATs. 31
Failure criteria varied across studies and included surgical failure,13,26,32,37,39,40 clinical failure,13,15,20,32 and radiographic failure.15,26 The incidence of surgical failure ranged from 5 cases 32 to 37 cases, 26 whereas clinical failure was observed in 7 20 to 15 cases, 32 and radiographic failure in 11 15 to 21 26 cases.
Graft survivorship and treatment failure rates among medial versus lateral MAT was analyzed among 8 reporting studies. The survivorship and failure rates associated with medial and lateral MAT were also notably variable. Studies from both Romandini 32 and Wagner et al 42 reported no significant differences in treatment failure based on graft laterality. Similarly, Torres et al 37 identified no significant difference in time to failure for medial or lateral MAT (199.3 vs 208.3 months, respectively). Inferior durability in lateral MAT was described by Noyes and Barber-Westin, 26 who reported a shorter time to failure (medial: 8.2 ± 6.5 years vs lateral: 7.7 ± 6.5 years), and Hommen et al, 15 who highlighted poorer overall survivorship in lateral MATs (50% failure rate lateral, 25% failure rate medial). Furthermore, Grassi et al 13 identified lateral MAT as having a higher risk of surgical failure (OR, 10.5; 95% CI, 1.0-110.3; P = .0495) and lower long-term survival rates (73%) compared with medial MAT (96%; P = .0333). In contrast, however, studies from van der Wal et al 39 (35% medial failure rate, 25% lateral failure rate) and Paša et al 31 (100% lateral MAT vs 83.6% medial MAT survival) underscored superior lateral MAT durability.
Graft survivorship also varied by fixation technique. Bone plug fixation was the most commonly reported method, with 10-year survival rates ranging from 45% to 87%.20,26,37 Two studies using soft tissue fixation reported survivorship between 73% and 89.4%.13,32 One study using a bone trough (bridge-in-slot) technique reported 85% survivorship at 10 years. 42 Suture-only fixation yielded a 52.5% survival rate at 10 years in 1 study, 39 while another using transosseous fixation demonstrated high survivorship, with 83.6% in medial and 100% in lateral allografts. 31
Functional Outcomes
Postoperative functional outcomes were assessed using validated patient-reported outcome measures, including the Lysholm score, Tegner Activity Scale score, VAS for pain score, and KOOS subscales (Table 5).
Patient-Reported Outcomes a
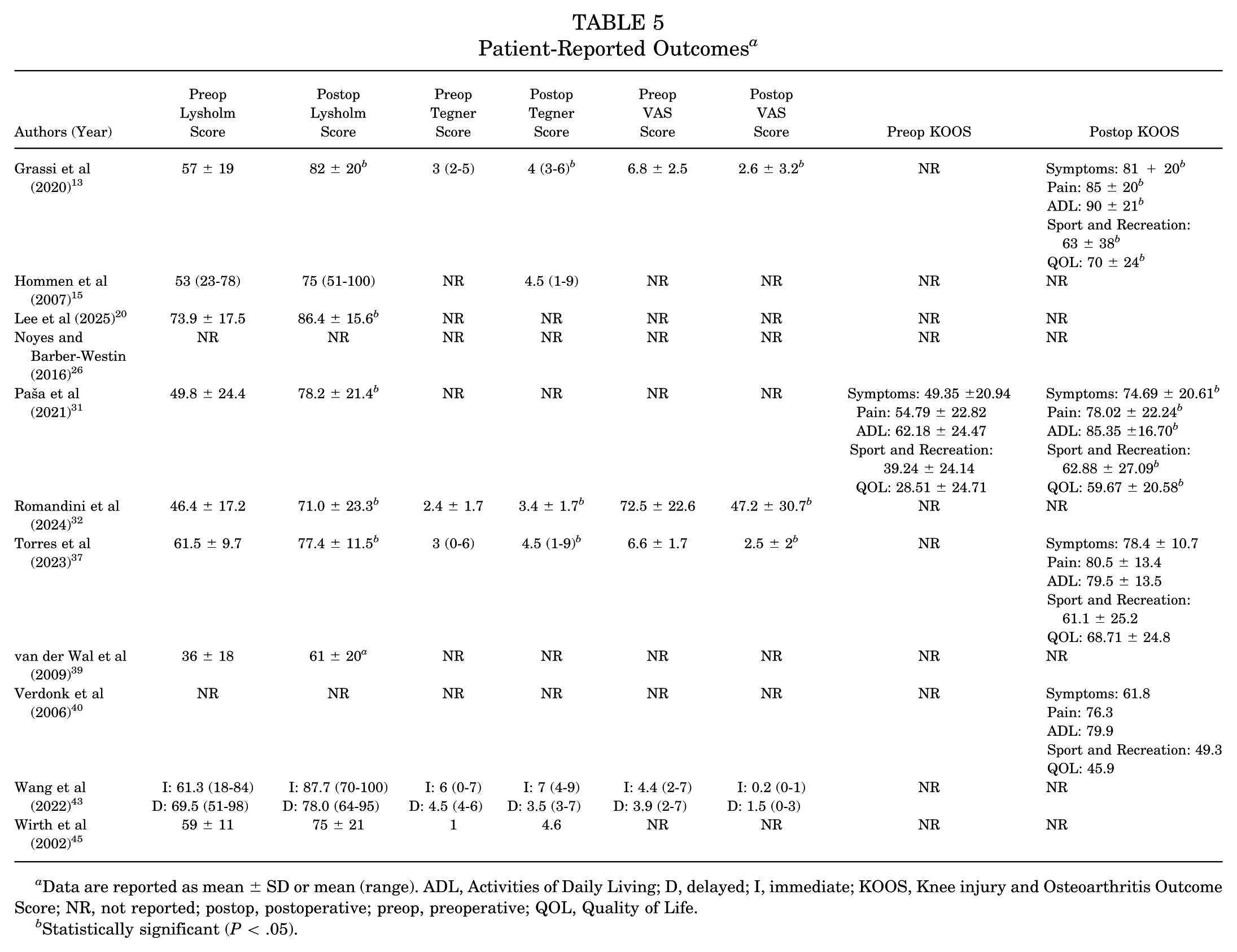
Data are reported as mean ± SD or mean (range). ADL, Activities of Daily Living; D, delayed; I, immediate; KOOS, Knee injury and Osteoarthritis Outcome Score; NR, not reported; postop, postoperative; preop, preoperative; QOL, Quality of Life.
Statistically significant (P < .05).
Lysholm scores were reported in 9 studies, ‡‡ with preoperative scores ranging from 36 39 to 73.9. 20 Postoperative scores ranged from 61.0 39 to 87.7. 43 Statistically significant improvements were reported in 7 of the 9 studies.13,15,20,31,32,37,39 The remaining studies showed numeric improvements but did not report P values.43,45 A pooled analysis of standardized mean differences (SMDs) across 7 studies demonstrated a significant overall improvement in Lysholm scores after MAT, with a pooled SMD of 1.32 (95% CI, 1.14-1.50) and no observed between-study heterogeneity (I2 = 0%) (Figure 5).
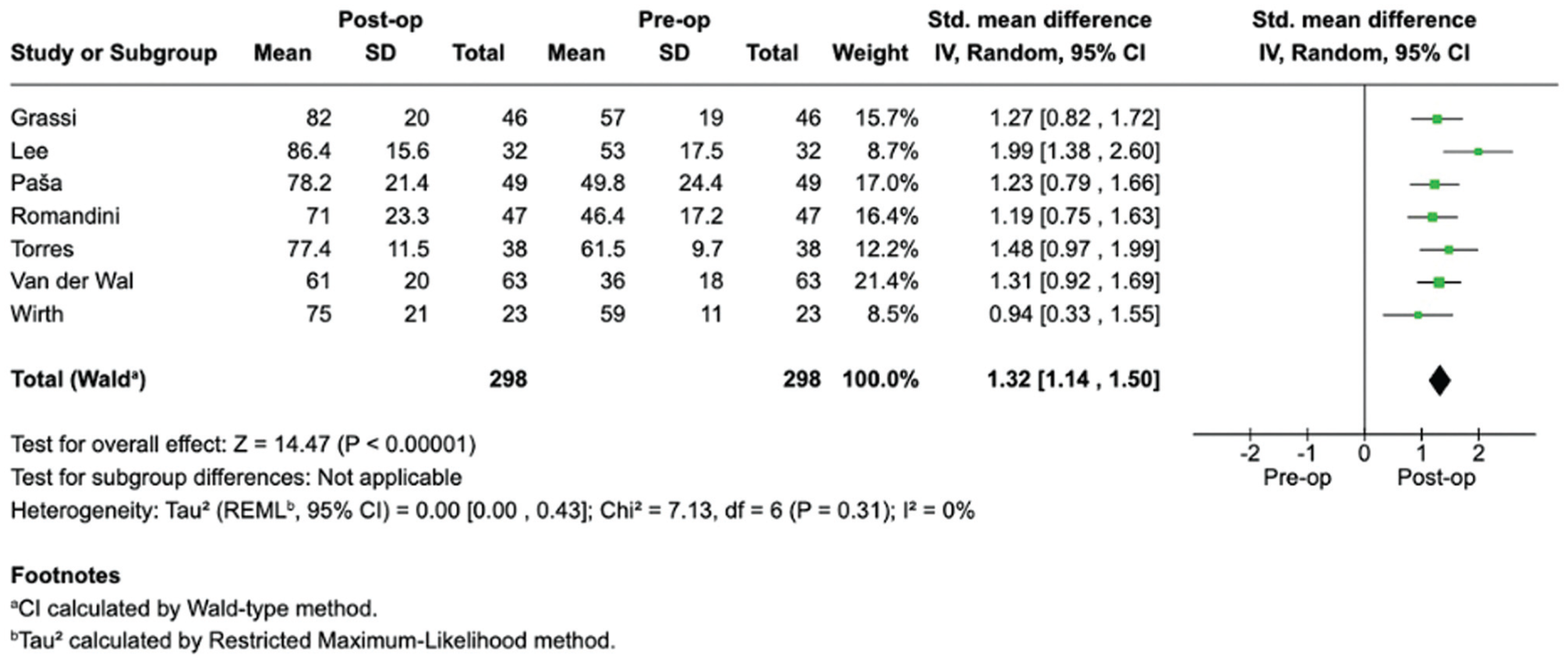
Forest plot of standardized mean differences in pre- and postoperative Lysholm scores. Study estimates were pooled using inverse variance weighting to calculate the overall effect. The pooled standardized mean difference (1.32; 95% CI, 1.14-1.50) was statistically significant (P < .001), with no observed between-study heterogeneity (I2 = 0%).
Tegner activity levels were assessed in 6 studies.13,15,32,37,43,45 Preoperative scores ranged from 1 45 to 6 (Wang et al, 43 immediate group), and postoperative scores ranged from 3.4 32 to 7 (Wang et al, 43 immediate group). Significant postoperative improvements were documented in 3 studies13,32,37; 2 studies did not report statistical significance.43,45
VAS pain scores were reported in 4 studies.13,32,37,43 Preoperative values ranged from 3.9 (Wang et al, 43 delayed group) to 7.25, 32 and postoperative values ranged from 0.2 (Wang et al, 43 immediate group) to 1.5 (Wang et al, 43 delayed group). Three studies reported statistically significant reductions in pain (P < .05).13,32,37 One study showed numeric improvements but did not report statistical significance. 43
Four studies reported postoperative KOOS values.13,31,37,40 The range of postoperative scores for each KOOS domain across these studies was as follows: Pain: 76.3 40 to 85.0 13 ; Symptoms: 61.8 40 to 81.0 13 ; Activities of Daily Living: 79.5 37 to 90.0 13 ; Sport and Recreation: 49.3 40 to 63.0 13 ; and Quality of Life: 45.9 40 to 70.0. 13 Of these, only Paša et al 31 reported both preoperative and postoperative values, demonstrating significant improvements in all 5 domains (P < .05).
Clinically Significant Outcomes
The Patient Acceptable Symptom State (PASS) and/or minimal clinically important difference (MCID) were reported in 3 studies (Table 6). Grassi et al 13 reported PASS achievement rates of 71% for Lysholm score and 60% to 82% for the KOOS subscales. Lee et al 20 found that 70.4% of patients met the MCID for Lysholm score. Furthermore, Wagner et al 42 reported MCID achievement rates of 86.5% (Lysholm score) and 61% to 78.2% (KOOS subscales), with corresponding PASS rates of 70.2% (Lysholm score) and 56.2% to 79% (KOOS subscales) and substantial clinical benefit (SCB) rates of 47.8% (Lysholm score) and 46.2% to 61.9% (KOOS subscales).
Clinically Significant Outcomes a
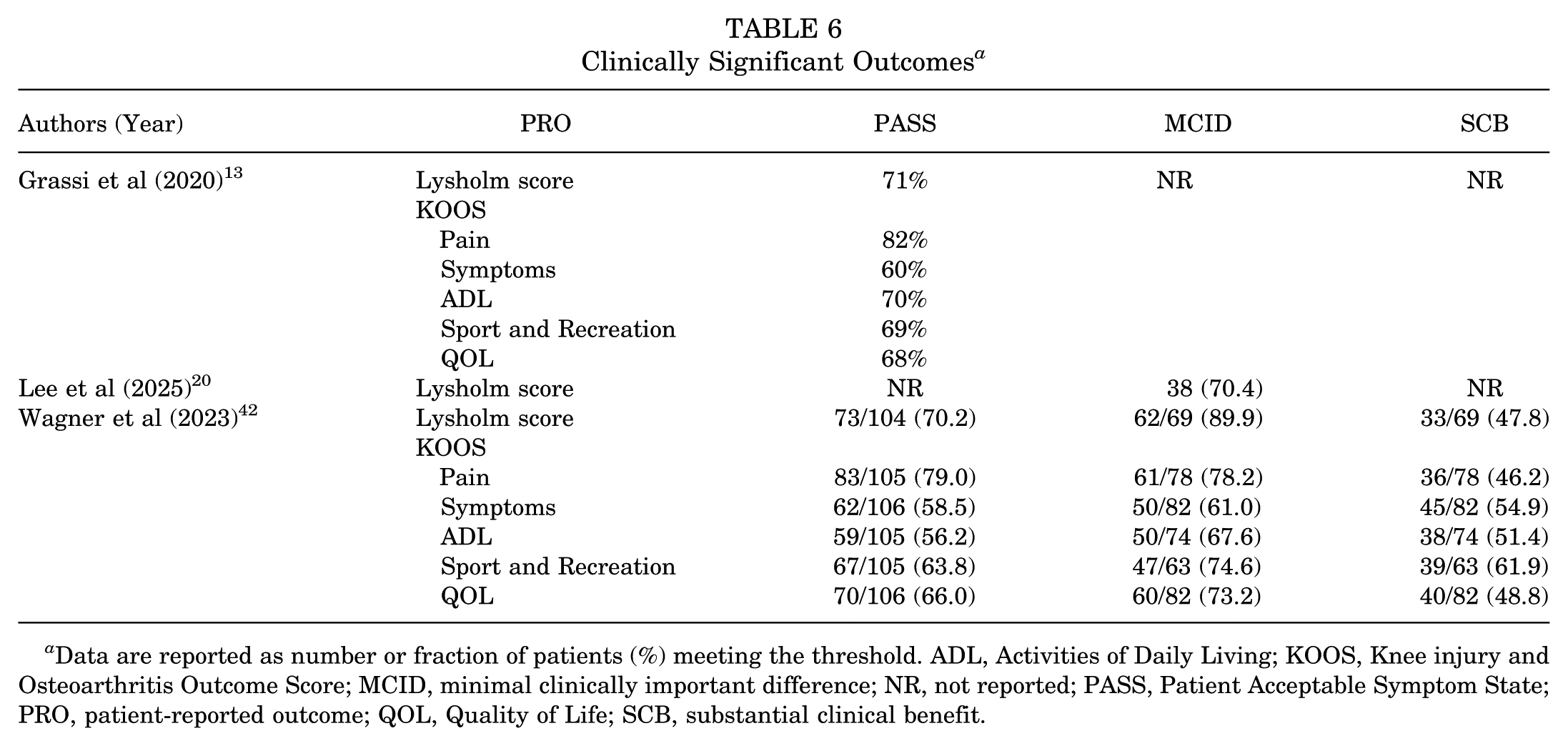
Data are reported as number or fraction of patients (%) meeting the threshold. ADL, Activities of Daily Living; KOOS, Knee injury and Osteoarthritis Outcome Score; MCID, minimal clinically important difference; NR, not reported; PASS, Patient Acceptable Symptom State; PRO, patient-reported outcome; QOL, Quality of Life; SCB, substantial clinical benefit.
Radiographic Progression of Osteoarthritis
Long-term progression of osteoarthritis after MAT was described variably across included studies (Table 7). Four studies measured the progression of preoperative joint space width (JSW) a decade after surgery. Lee et al 20 reported that the mean JSW narrowed from 4.96 ± 0.96 mm to 3.47 ± 1.62 mm, whereas Torres et al 37 reported a similar degree of narrowing from 3.3 ± 1.5 mm to 1.9 ± 1.5 mm. Changes in JSW were also analyzed by Verdonk et al, 40 who described a progression by 1 grade in 11 cases (34%), by 2 grades in 7 cases (22%), and by 3 grades in 1 case (3%). Similarly, Wang et al 43 identified a mean JSW narrowing of 0.35 ± 0.48 mm in immediate MATs and 0.71 ± 0.70 mm in delayed MATs.
Radiographic Progression of Osteoarthritis 10 Years After MAT a
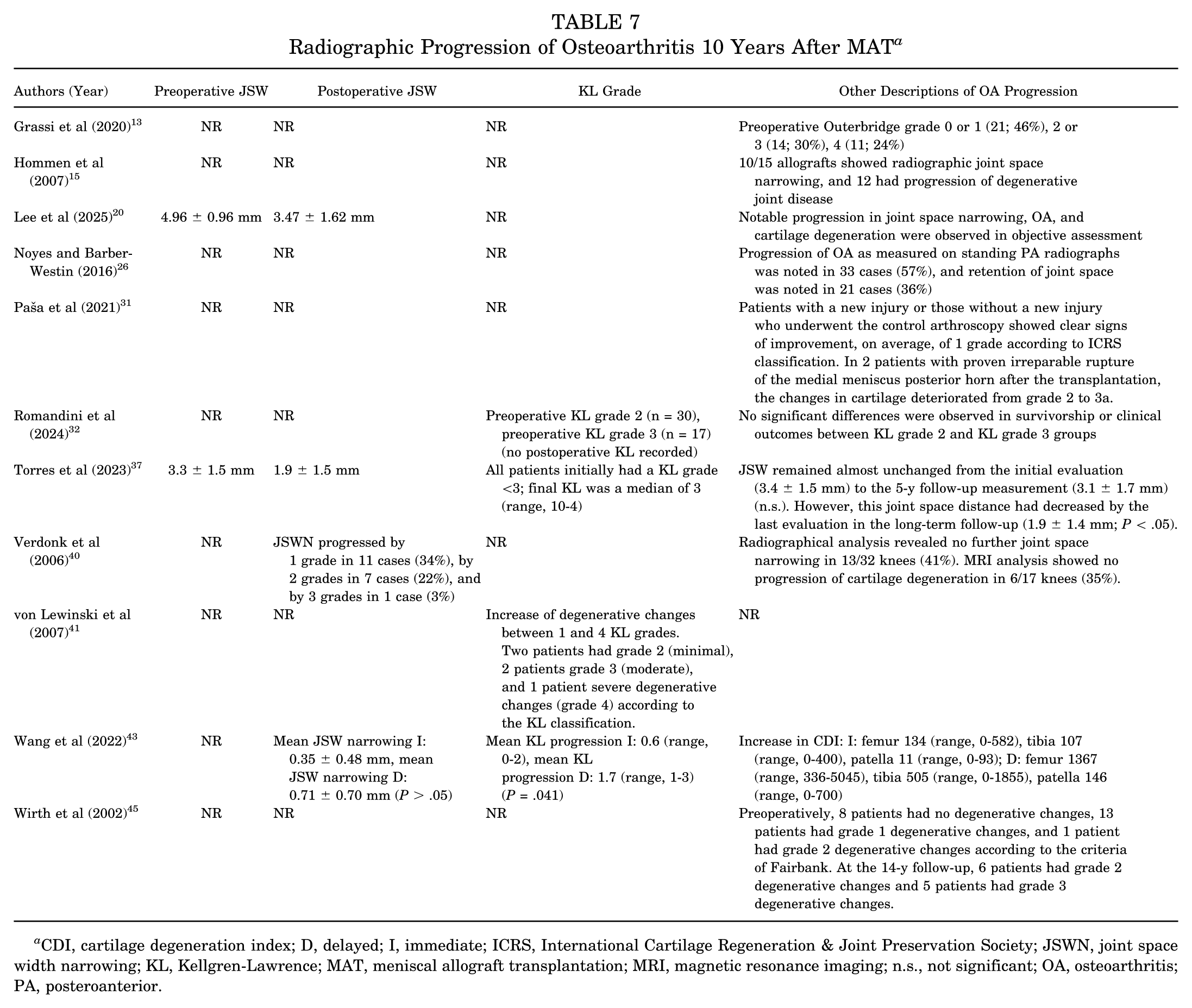
CDI, cartilage degeneration index; D, delayed; I, immediate; ICRS, International Cartilage Regeneration & Joint Preservation Society; JSWN, joint space width narrowing; KL, Kellgren-Lawrence; MAT, meniscal allograft transplantation; MRI, magnetic resonance imaging; n.s., not significant; OA, osteoarthritis; PA, posteroanterior.
Three studies evaluated long-term changes in Kellgren-Lawrence (KL) grading after MAT. Wang et al 43 also examined KL grade, reporting a significantly greater KL progression in delayed MATs (1.7; range, 1-3) compared with immediate MATs (0.6; range, 0-2) (P = .041). An increase of degenerative changes from 1 to 4 KL grades was reported by von Lewinski et al, 41 with 2 patients having grade 2 (minimal), 2 patients grade 3 (moderate), and 1 patient grade 4 (severe degenerative changes).
Discussion
The most important findings of this systematic review were as follows: (1) MAT led to sustained, meaningful improvements in patient-reported outcomes, including VAS pain scores, Lysholm scores, Tegner activity levels, and KOOS subscales; (2) survival rates were variable, ranging from 45% to 100% at 10 years and 17% to 87% at ≥15 years; and (3) failure rates increased over time, with declining survivorship beyond the 10-year mark. These findings suggest that while MAT is capable of providing significant improvements in pain and function for many patients, long-term graft survivorship is highly variable and may be influenced by a combination of patient selection, graft choice, and surgical technique.
While previous literature has established the short- and midterm efficacy of MAT, the present review demonstrates that MAT offers sustained, clinically meaningful improvements in pain and function after a decade.25,34 Preoperative Lysholm scores improved significantly in 78% (7/9) of studies a decade after surgery. Furthermore, a pooled analysis of 7 studies highlighted consistent improvements in Lysholm scores after MAT, indicating greater postoperative knee function.13,15,20,31,32,37,39 Preoperative VAS scores also significantly decreased in 60% (3/5) of the included studies,13,32,37 and Tegner activity levels improved in 75% (3/4).13,32,37 KOOS subscales also demonstrated improvement in pain, activities of daily living, and quality of life. 31 Given the sustained benefits across patient-reported outcomes, MAT remains a valuable joint-preserving treatment for young, active patients with significant meniscal deficiency. Nevertheless, future comparative studies should evaluate long-term MAT outcomes relative to the natural progression of untreated meniscal deficiency.11,20,24,30,33,37
Graft survivorship at 10 years demonstrated substantial variability, ranging from 45% to 100% across studies. §§ This review indicated that almost half the reporting articles demonstrated a survivability ≥83.6%,20,31,32,42 and pooled analysis demonstrated an overall 10-year survivorship rate of 70.9% (95% CI, 48.0%-86.5%) with substantial between-study heterogeneity. It is likely that differences in surgical technique, graft type, fixation methods, and patient selection contributed to this variability. Survivorship was also defined variably between studies, with most studies using a combination of clinical, surgical, or radiographic failure criteria.
As expected, graft failure rates increased with longer duration of follow-up. Common causes of failure included persistent pain, mechanical symptoms, and osteoarthritis progression. ∥∥ Beyond a decade from surgery, ≥15-year survival varied greatly, with MAT survivability ranging from 19% to 87%.20,26,37,39,42 This was reinforced by the findings of our pooled analysis (58.4%; 95% CI, 33.0%-80.0%), which was heterogeneous (I2 = 93%) and reinforced the inconsistencies in long-term MAT survivorship. Notable variability in implant survival supports the importance of patient counseling regarding the potential for long-term decline and additional revision surgery or conversion to arthroplasty. Furthermore, future investigations of MAT survivability at ≥15 years are warranted to maximize long-term outcomes and minimize osteoarthritis risk as patients age, especially considering the young age of MAT recipients.
Lydon et al 22 reported that fresh allografts may address common complications associated with fresh-frozen MAT, such as graft shrinkage and extrusion. This review found that fresh-frozen meniscal allografts had a 73% to 89.4% survival rate (5 studies), which was comparable to the 1 study that used deep-frozen allograft (83.6% survival medial menisci, 100% survival lateral menisci). However, these survivorship rates were superior to those observed across 3 studies using cryopreserved allografts (45%-52.5% survivorship). Additionally, patient-specific factors such as axial alignment, cartilage status, and concomitant procedures (eg, osteotomy) may significantly influence MAT outcomes.3,10,22,27
A recent meta-analysis examining different fixation techniques by Kakria et al 18 identified comparable short- to midterm outcomes between suture and bony fixation, although long-term data remain limited. Kakria et al initially hypothesized that osseous graft fixation would result in superior long-term survivorship; however, 3 studies using bone plug or trough fixation reported survivability rates of 58% or worse after 10 years.15,26,37 In contrast, Romandini et al 32 reported an 89.40% survival rate using soft tissue fixation, suggesting that fixation methodology alone may not be the sole determinant of long-term success. Another plausible explanation for this discrepancy may be that the bone plug studies date back to 1991-1996, before more recent advancements in surgical technique, graft preparation, and postoperative rehabilitation.
Medial versus lateral MAT fixation also remains a significant topic of debate among sports surgeons. This systematic review identified 8 studies comparing long-term failure rates or implant survivorship based on graft laterality. Although comprehensive, these findings were variable. Both medial and lateral MAT have been shown to provide significant improvements in pain and function; however, some meta-analyses and cohort studies have reported that lateral MAT may be associated with superior pain relief and functional scores in the mid- to long-term.5,19,46 Variability in cartilage status, concomitant procedures, and patient demographics may better explain differences in survival rather than graft laterality or the fixation method itself. Future studies directly comparing medial versus lateral fixation, surgical techniques, graft types, and biological augmentation strategies are warranted.
A prior systematic review by Novaretti et al 25 assessed long-term outcomes after MAT. While their work contributed important insights into survivorship and patient outcomes, their analysis included 3 studies with a mean follow-up period of <10 years. 25 In contrast, the present study focused exclusively on studies in which all patients had a minimum of 10 years of follow-up, offering a more homogeneous perspective on results after ≥10 years. This study also expands on the existing literature by incorporating clinically meaningful outcome measures such as the PASS, MCID, and SCB, providing greater context for evaluating patient-reported success. Finally, by including more recently published studies (2019-2025) and stratifying outcomes by graft type and fixation technique, our review offers a comprehensive update to the evolving body of literature surrounding MAT.
Limitations
This study has reportable limitations. First, the included studies were level 3 or 4 evidence, which carry risk of bias. It is also worth mentioning the significant heterogeneity in surgical techniques, patient populations, outcome measures, and definitions of failure; however, heterogeneity was shown to be zero for Lysholm score (I2 = 0.00%; 95% CI, 0.00-0.43). Another important consideration is that while SCB, PASS, and MCID data were useful contributions provided by this review, these values were only present in 3 studies. Furthermore, this investigation analyzed all studies with sufficient long-term MAT follow-up, which included surgeries performed ≥2 decades ago. This may not be representative of long-term outcomes observed with advancements and techniques of the modern surgeon.
Additionally, graft survivorship criteria were inconsistently defined, complicating cross-study comparison. Definitions of treatment failure varied widely across studies; while some authors characterized return to the operating room for procedures such as a partial meniscectomy or chondroplasty as failure, others limited failure to revision MAT or conversion to arthroplasty. These inconsistencies complicate interpretation of long-term survivorship and call for standardized failure definitions in future research.
Although data on concomitant procedures such as osteotomy and cartilage restoration were extracted, substantial heterogeneity in reporting and the limited availability of viable patient-level data across studies precluded meaningful subgroup analyses of mechanical axis alignment or the impact of additional procedures on MAT survivorship. As a result, this review was unable to provide quantitative insight into whether outcomes differ by alignment, presence of osteotomy, or isolated versus combined MAT procedures despite the recognized importance of these factors in long-term success and osteoarthritis prevention. Prospective, multicenter trials with standardized definitions of outcomes and failure, as well as consistent reporting of alignment, concomitant procedures, and patient-level variables, are needed to better inform evidence-based indications in MAT.
Conclusion
MAT demonstrated favorable long-term clinical outcomes and variable graft survivorship beyond 10 years. Included studies varied based on graft type, fixation technique, and patient selection. Continued prospective, high-level studies are warranted to standardize surgical approaches, improve the durability of this joint-preserving intervention, and identify modifiable risk factors for inferior long-term outcomes.
Footnotes
Submitted August 4, 2025; accepted September 2, 2025.
One or more of the authors has declared the following potential conflict of interest or source of funding: A.J. has received consulting fees from Smith ⩲ Nephew. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.